Back to Journals » Cancer Management and Research » Volume 17

Analysis of Efficacy and Survival Prognosis for Astragalus Polysaccharide Injection as Adjuvant Therapy in Non - Small Cell Lung Cancer: A Propensity Score Matching - Based Study
Authors Li J, Zhang Y, Wang X, Ding Z, Zhu N, Chen Y, Li Y, Lu C
Received 31 July 2025
Accepted for publication 15 November 2025
Published 31 December 2025 Volume 2025:17 Pages 3359—3372
DOI https://doi.org/10.2147/CMAR.S552487
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bilikere Dwarakanath
Jinying Li,1,* Yifei Zhang,2,* Xuemei Wang,3 Zhongyu Ding,3 Na Zhu,1 Yuan Chen,3 Yongli Li,1 Chuangxin Lu4
1Department of Health Management, Henan Provincial People’s Hospital, Zhengzhou, 450001, People’s Republic of China; 2Department of Cadre Healthcare, Henan Provincial People’s Hospital, Zhengzhou, 450001, People’s Republic of China; 3Department of Traditional Chinese Medicine, Henan Provincial People’s Hospital, Zhengzhou, 450001, People’s Republic of China; 4Department of Medical Oncology, Henan Provincial People’s Hospital, Zhengzhou, 450001, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yongli Li, Department of Health Management, Henan Provincial People’s Hospital, No. 7 Weiwu Road, Zhengzhou, Henan, 450001, People’s Republic of China, Tel +86-0371-65580321, Email [email protected] Chuangxin Lu, Department of Medical Oncology, Henan Provincial People’s Hospital, No. 7 Weiwu Road, Zhengzhou, Henan, 450001, People’s Republic of China, Tel +86-0371-65580321, Email [email protected]
Background: Non-small cell lung cancer (NSCLC) is a prevalent malignancy where adjuvant therapy is crucial. Astragalus polysaccharide injection (APS-I) has shown potential as an adjunct due to its immunomodulatory properties, but its impact on survival outcomes requires further validation.
Objective: This study employed propensity score matching (PSM) to evaluate the efficacy of APS-I combined with conventional therapy versus conventional therapy alone in the adjuvant treatment of NSCLC.
Methods: In this retrospective cohort study, NSCLC patients receiving adjuvant therapy between January 2018 and December 2024 were enrolled. After 1:1 PSM, 54 matched pairs were allocated to the APS-I + conventional therapy group or the conventional therapy alone group. Outcomes included objective response rate (ORR), disease control rate (DCR), progression-free survival (PFS), overall survival (OS), immune function, quality of life (QoL), and adverse events.
Results: The APS-I group demonstrated significantly superior short-term efficacy, with higher ORR (77.8% vs 33.3%, P< 0.001) and DCR (96.3% vs 70.4%, P< 0.001). Survival outcomes were significantly improved: median PFS was 12.8 months versus 8.2 months (Hazard Ratio [HR]= 0.143, 95% CI: 0.082– 0.250, P< 0.001), and median OS was 23.3 months versus 17.0 months (HR= 0.249, 95% CI: 0.154– 0.401, P< 0.001). The APS-I group also showed a significantly higher Karnofsky Performance Status (KPS) improvement rate (60.5% vs 27.9%, P=0.003) and a lower incidence of adverse events (11.1% vs 33.3%, P=0.014).
Conclusion: APS-I combined with conventional therapy shows promise in improving survival and quality of life, but multicenter RCTs are warranted to validate efficacy before clinical adoption.
Keywords: astragalus polysaccharide injection, non-small cell lung cancer (NSCLC), adjuvant therapy, propensity score matching (PSM), retrospective study, survival prognosis
Introduction
Non-small cell lung cancer (NSCLC) constitutes one of the most prevalent malignancies globally, accounting for 80%-85% of all lung cancer cases.1 In recent years, with the rapid advancement of molecular biology and immunotherapy, the therapeutic landscape for NSCLC has expanded beyond conventional surgery, radiotherapy, and chemotherapy to include targeted therapy and immunotherapy, leading to significant improvements in patient survival outcomes.2 However, even under current treatment paradigms, the overall 5-year survival rate for NSCLC patients remains below 20%, with particularly poor prognoses observed in advanced-stage patients. Adjuvant therapy plays a critical role in NSCLC management, aiming to reduce recurrence risk, prolong survival, and enhance quality of life. While traditional adjuvant chemotherapy can extend survival, it is often associated with adverse reactions such as myelosuppression and hepatotoxicity, which limit its therapeutic efficacy.3,4
Astragalus Polysaccharide (APS), the primary active component extracted from the traditional Chinese herb Astragalus membranaceus, possesses significant immunomodulatory effects and has garnered attention for its potential in oncological applications.5,6 Preclinical evidence suggests that APS may enhance the body’s anti-tumor immune response through multiple mechanistic pathways. These include the activation of immune cells such as T lymphocytes (particularly CD4+ T helper cells) and macrophages, the enhancement of natural killer (NK) cell cytotoxicity, and the promotion of cytokine secretion (eg, IL-2, IFN-γ), thereby helping to normalize the CD4+/CD8+ T-cell ratio and counteract chemotherapy-induced immunosuppression.7 Additionally, APS has been reported to exhibit hepatoprotective properties, potentially through antioxidant mechanisms such as the reduction of malondialdehyde (MDA) and elevation of superoxide dismutase (SOD) activity, as well as the suppression of inflammatory mediators like TNF-α and IL-6. Within the field of lung cancer treatment, existing research has confirmed that Astragalus Polysaccharide Injection combined with chemotherapy can improve patients’ immune function and quality of life.8 However, its definitive impact on survival outcomes has not been fully validated, and the efficacy differences across NSCLC patients with varying pathological types and stages warrant further investigation.9 APS-I may synergize with immune checkpoint inhibitors or targeted therapies by enhancing T-cell activation and cytokine secretion, potentially overcoming resistance mechanisms in advanced NSCLC.
Current research on Astragalus Polysaccharide Injection in NSCLC adjuvant therapy primarily consists of small-sample prospective studies, lacking large-scale, high-quality retrospective investigations.10 Furthermore, heterogeneity in patient selection, treatment protocols, and efficacy evaluation criteria across existing studies has led to inconsistent findings.11 This study aims to employ propensity score matching (PSM) methodology to minimize confounding factor influences and systematically evaluate the efficacy and survival impact of Astragalus Polysaccharide Injection in NSCLC adjuvant therapy, thereby providing more robust evidence-based medical evidence for clinical practice.
The primary objective of this study is to evaluate the differences in therapeutic efficacy between Astragalus Polysaccharide Injection combined with conventional therapy versus conventional therapy alone in the adjuvant treatment of NSCLC. This assessment encompasses short-term efficacy indicators, including objective response rate (ORR) and disease control rate (DCR), as well as long-term survival outcomes such as progression-free survival (PFS) and overall survival (OS). Concurrently, the study will investigate the effects of Astragalus Polysaccharide Injection on patients’ immune function, hepatic function, and quality of life, along with its efficacy variations across different patient subgroups.
Materials and Methods
Patient Selection
This retrospective cohort study was conducted using medical records of thoracic surgery patients treated at our institution between January 2018 and December 2024. The study protocol was approved by the Institutional Review Board (IRB) with a waiver of informed consent due to the retrospective nature of the investigation. To minimize confounding effects, propensity score matching (PSM) was employed as a statistical methodology to balance baseline characteristics between treatment groups. The study population comprised NSCLC patients who received adjuvant therapy during the specified period. Patients were stratified into two cohorts: a treatment group receiving Astragalus polysaccharide injection (APS-I) in combination with standard treatment, and a control group receiving standard treatment alone. After PSM with a 1:1 matching ratio, a total of 86 patients were allocated to each group, ensuring comparable baseline covariates across the matched cohorts. The study was approved by Ethics Committee of Henan Provincial People’s Hospital. Informed consent was waived due to the retrospective nature of the study and the use of de-identified data. All procedures performed in this study involving human participants were in accordance with the Declaration of Helsinki (as revised in 2013).
Inclusion Criteria
Postoperative pathological diagnosis confirmed NSCLC (AJCC 8th edition staging); the treatment group received concomitant Astragalus polysaccharide injection (250 mg/day, intravenous infusion, D1-14/cycle); follow-up duration was ≥24 months with complete data. Patients had complete clinical data and follow-up records; control group patients received only conventional treatment.
Exclusion Criteria
Concomitant other malignant neoplasms; severe cardiac, hepatic, or renal insufficiency; autoimmune diseases; inability to obtain follow-up data; receipt of other immunomodulatory therapies; unclear or incomplete treatment protocols.
Treatment Regimens of the Two Groups
The treatment group received Astragalus polysaccharide injection (APS-I) combined with standard treatment, with the protocol being that APS-I was administered at 250 mg/day via intravenous infusion (intravenous infusion) from day 1 to day 14 (D1-D14) of each treatment cycle, and the standard treatment included chemotherapy regimens (TP, NP) and/or radiotherapy. The control group received only standard treatment, which was identical to the chemotherapy and/or radiotherapy regimens given to the treatment group, without the administration of APS-I.
Propensity Score Matching (PSM)
Selection of Matching Variables
Matching variables included factors potentially influencing both treatment assignment and outcomes, including demographic characteristics (age, gender), tumor characteristics (TNM stage, histological type such as adenocarcinoma, squamous cell carcinoma, and other types), clinical characteristics (ECOG Performance Status, Karnofsky Performance Status [KPS], smoking history), comorbidities (hypertension, diabetes mellitus, cardiovascular disease), treatment regimen (chemotherapy regimens like TP [Paclitaxel + Platinum] and NP [Vinorelbine + Platinum], radiation therapy dose), and follow-up duration (defined as the time from treatment initiation to last follow-up or death).
PSM Methodology
Propensity scores were estimated through a logistic regression model in which treatment group assignment (receiving Astragalus Polysaccharide Injection) served as the dependent variable and the aforementioned matching variables were included as covariates. For the matching procedure, a 1:1 nearest neighbor matching algorithm was applied with a caliper width set at 0.2 standard deviations of the propensity score logit. Post-matching, covariate balance between the matched groups was assessed using standardized mean differences (SMD), with an SMD threshold of <10% for all covariates being considered to indicate adequate balance.
Data Collection and Management
Baseline Data
Demographic information included age, gender, and occupation. Tumor characteristics comprised TNM staging, histopathological type, and tumor size. Clinical features entailed Eastern Cooperative Oncology Group (ECOG) Performance Status, Karnofsky Performance Status (KPS), and smoking history. Comorbidities encompassed hypertension, diabetes mellitus, cardiovascular diseases, and hepatic and renal function status. Treatment regimens involved chemotherapy regimens such as TP and NP, radiation therapy dose, and administration of Astragalus polysaccharide injection (APS-I). Hepatic function biomarkers included alanine aminotransferase (ALT) and aspartate aminotransferase (AST). Tumor markers comprised carcinoembryonic antigen (CEA), neuron-specific enolase (NSE), and squamous cell carcinoma antigen (SCC-Ag).
Follow-Up Data
Efficacy was evaluated according to RECIST 1.1 criteria, including complete response (CR), partial response (PR), stable disease (SD), and progressive disease (PD). Survival outcomes encompassed progression-free survival (PFS) and overall survival (OS). Adverse events were graded per the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. Quality of life was evaluated via the Karnofsky Performance Status (KPS) score. Immunological changes involved a comparative analysis of immune function parameters before and after treatment, including T lymphocyte subsets (CD4+, CD8+) and natural killer (NK) cell activity measured by flow cytometry using commercial human lymphocyte subset detection kits, with reference to established laboratory ranges. Hepatic function changes entailed a comparative analysis of hepatic function indicators pre- and post-treatment, while tumor marker dynamics involved a comparative analysis of tumor marker levels before and after treatment.
Data Sources
The Electronic Medical Record (EMR) System was used to extract patient demographics, diagnostic data, and treatment records. Immune function parameters, hepatic function biomarkers, and tumor marker levels were retrieved from the laboratory database. The Follow-Up Tracking System was used to record patient survival status, adverse events, and quality-of-life assessments.
Statistical Analysis
All statistical analyses were performed using SPSS software (version 29.0) for basic descriptive statistics. Propensity score matching (PSM) and survival analysis procedures were conducted on the R platform (version 4.3.0), utilizing the MatchIt package for PSM implementation and the survival package for survival analysis. All analyses strictly adhered to statistical principles to ensure the reliability of the study conclusions. For baseline characteristic comparisons, continuous variables (eg, age, number of chemotherapy cycles) were compared between groups using independent samples *t*-tests if normally distributed, or the Mann–Whitney U-test for non-normally distributed data. Categorical variables (eg, gender, histological type) were compared using Pearson’s chi-square (χ2) tests; Fisher’s exact test was employed when expected frequencies were less than 5. Following propensity score matching (PSM), covariate balance was assessed using standardized differences (SD), with an SD threshold of <10% required to confirm adequate matching. For efficacy evaluation, differences in objective response rate (ORR) and disease control rate (DCR) between groups were analyzed using χ2-tests. Survival analysis involved generating Kaplan-Meier survival curves, with between-group differences assessed via the Log rank test. Multivariable Cox proportional hazards regression models were subsequently fitted to identify independent prognostic factors influencing progression-free survival (PFS) and overall survival (OS), incorporating variables such as treatment group and TNM stage. Safety analysis compared the incidence rates of adverse reactions between the two groups using χ2-tests. P <0.05 was considered statistically significant. Values were expressed as mean±standard deviation, unless stated otherwise.
Results
Study Population Inclusion Process and Matching Results
A total of 229 patients were initially enrolled. After applying exclusion criteria, the following cases were excluded: concurrent malignancies (n=15), severe hepatic or renal insufficiency (n=12), immunological disorders (n=8), inability to obtain follow-up data (n=10), receipt of other immunomodulatory therapies (n=7), and incomplete or unclear treatment regimens (n=5). Ultimately, 54 patients were allocated to both the treatment group and the control group. Following propensity score matching (PSM), 54 valid matched pairs were successfully established (Figure 1).
 |
Figure 1 NSCLC PSM Flowchart. |
Distribution of Propensity Scores Before and After Matching
The propensity score distributions for the two groups (Control Group; Treatment Group) are shown in Figure 1. Prior to matching (Figure 2A), the score distributions exhibited notable differences between the groups. Following matching (Figure 2B), the distributions demonstrated substantially closer alignment. This visual assessment indicates that propensity score matching effectively balanced the baseline characteristics between the groups (Figure 2).
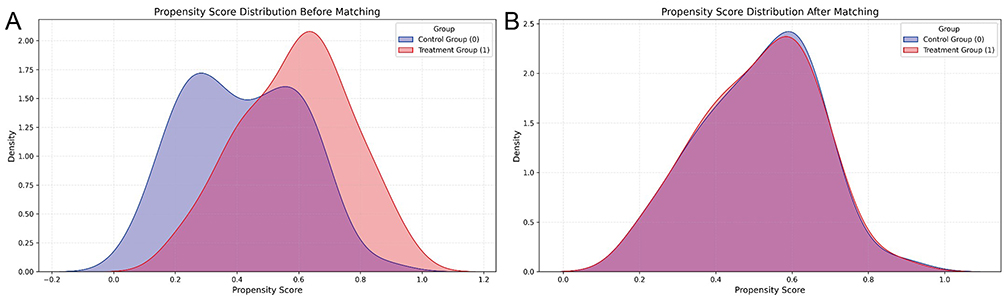 |
Figure 2 Propensity distribution before and after matching (A), Density plots of propensity scores before matching, showing distinct distributions between the Control Group (red) and Treatment Group (blue), indicating baseline imbalance. (B), Density plots after 1:1 propensity score matching, demonstrating substantially overlapping distributions between groups, confirming successful balancing of baseline covariates. |
Comparison of Baseline Characteristics Before and After Propensity Score Matching
Before propensity score matching, no statistically significant differences were observed between the treatment and control groups in baseline characteristics (tumor size, sum of target lesions, gender, ECOG PS, smoking history, hypertension, diabetes, CVD history, hepatic/renal dysfunction, surgical margin status; all P>0.05). Before matching, significant differences existed in age, TNM stage, and pathology type (P < 0.05), which were balanced after PSM. After matching, the groups remained well-balanced across all these characteristics (all P>0.05; see Table 1).
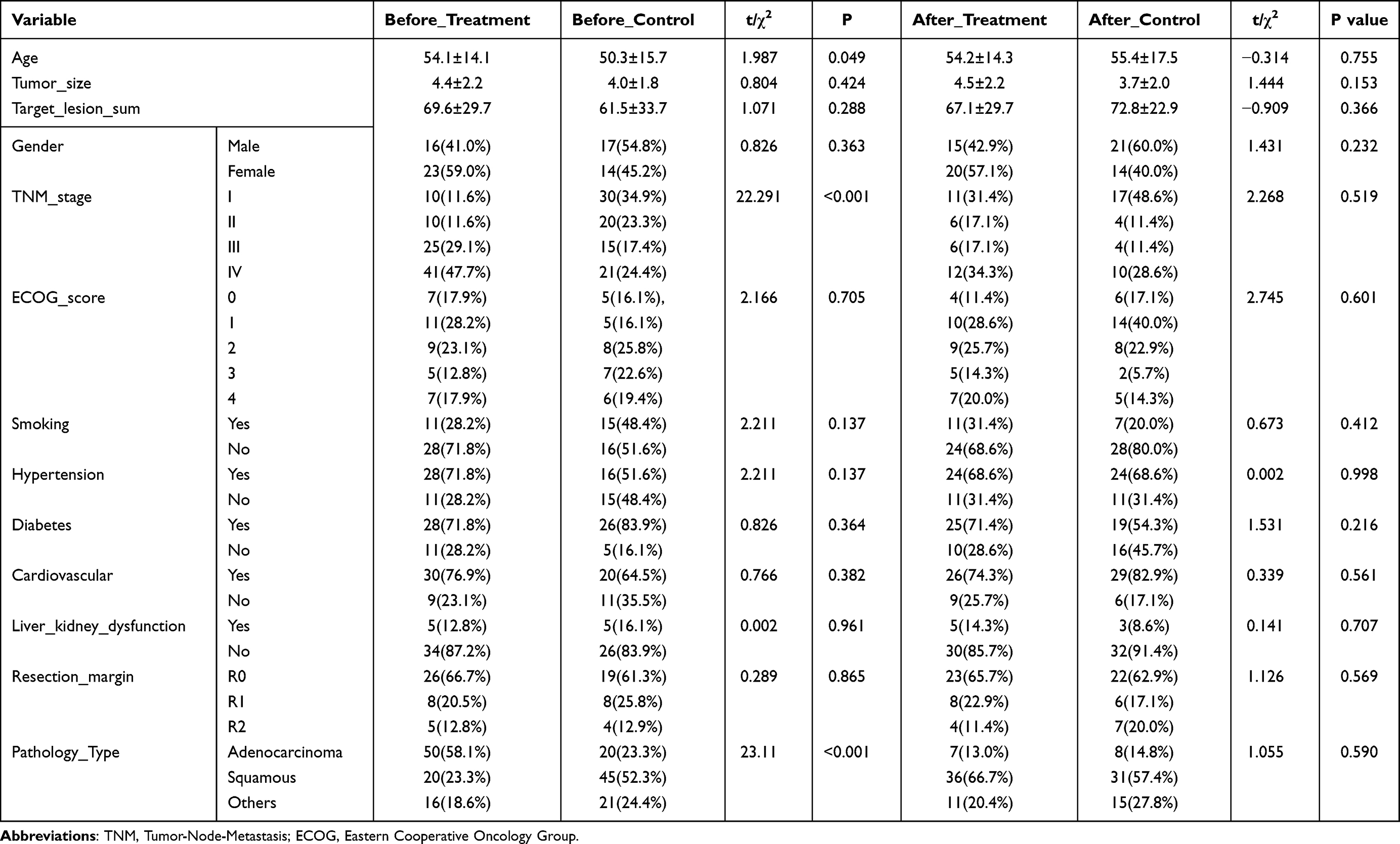 |
Table 1 Comparison of Baseline Characteristics Before and After Propensity Score Matching (PSM) |
Comparison of Baseline Characteristics After Propensity Score Matching
All baseline characteristics demonstrated balanced distributions between groups (P > 0.05). Categorical variables—including pathology type, metastatic status (brain, bone, liver, lung), treatment history (surgery, margin status, radiotherapy, neoadjuvant/adjuvant therapy), targeted therapies, comorbidities, and molecular markers (EGFR, ALK, ROS1, KRAS)—showed no significant intergroup differences. Similarly, continuous variables (KPS score, hematological indices, inflammatory markers, pain score, follow-up compliance) revealed no significant differences (Table 2).
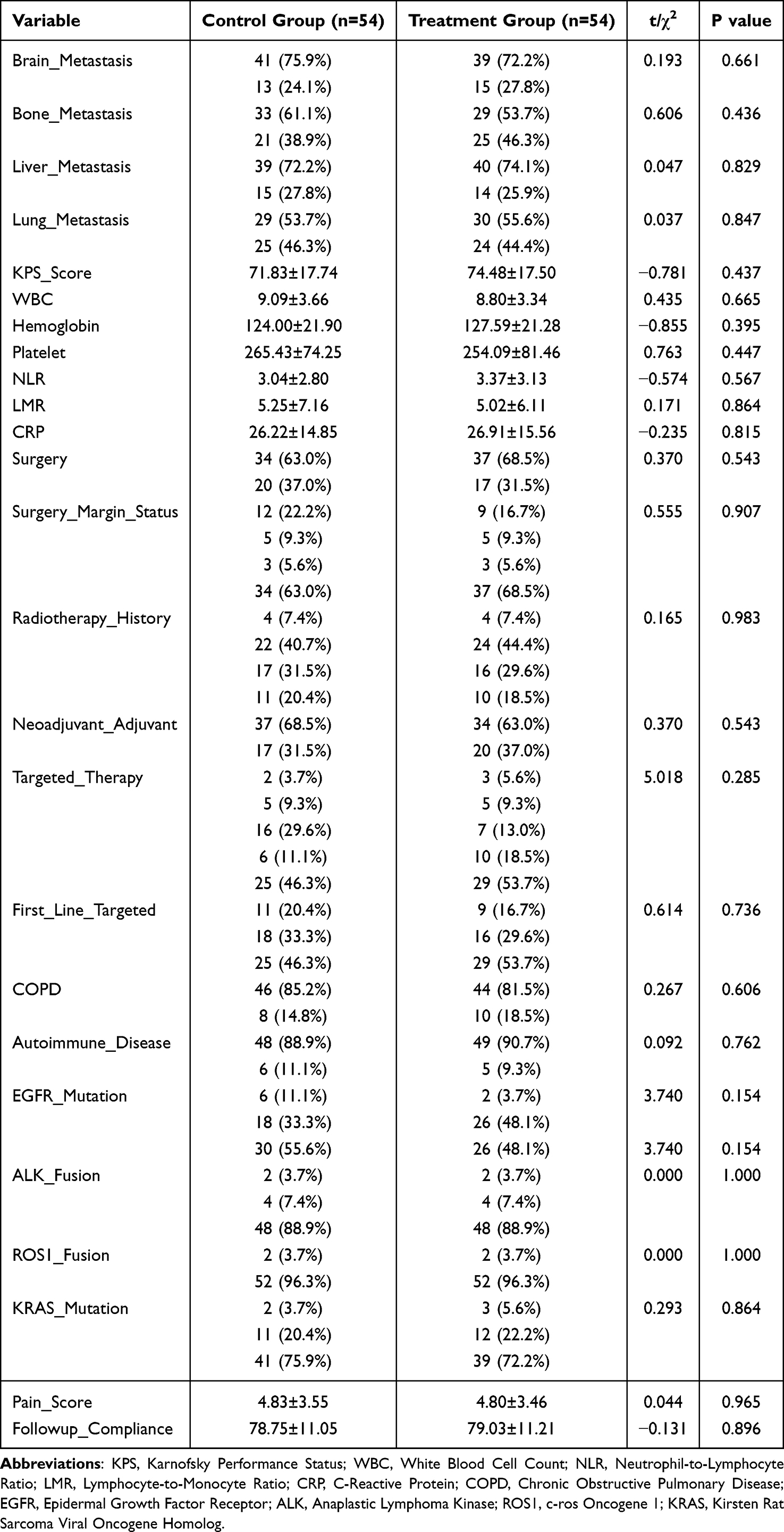 |
Table 2 Results of Baseline Characteristics Comparison Between the Two Groups After Matching |
Changes in Hepatic Function and Tumor Marker Levels Before and After Treatment Between the Two Groups
Baseline and post-treatment levels of ALT, AST, total bilirubin, albumin, creatinine, eGFR, CEA, NSE, SCC-Ag, CYFRA21-1, and LDH showed no statistically significant differences between groups (all P > 0.05). All parameters demonstrated comparable distributions across groups with no significant intergroup variations (Table 3).
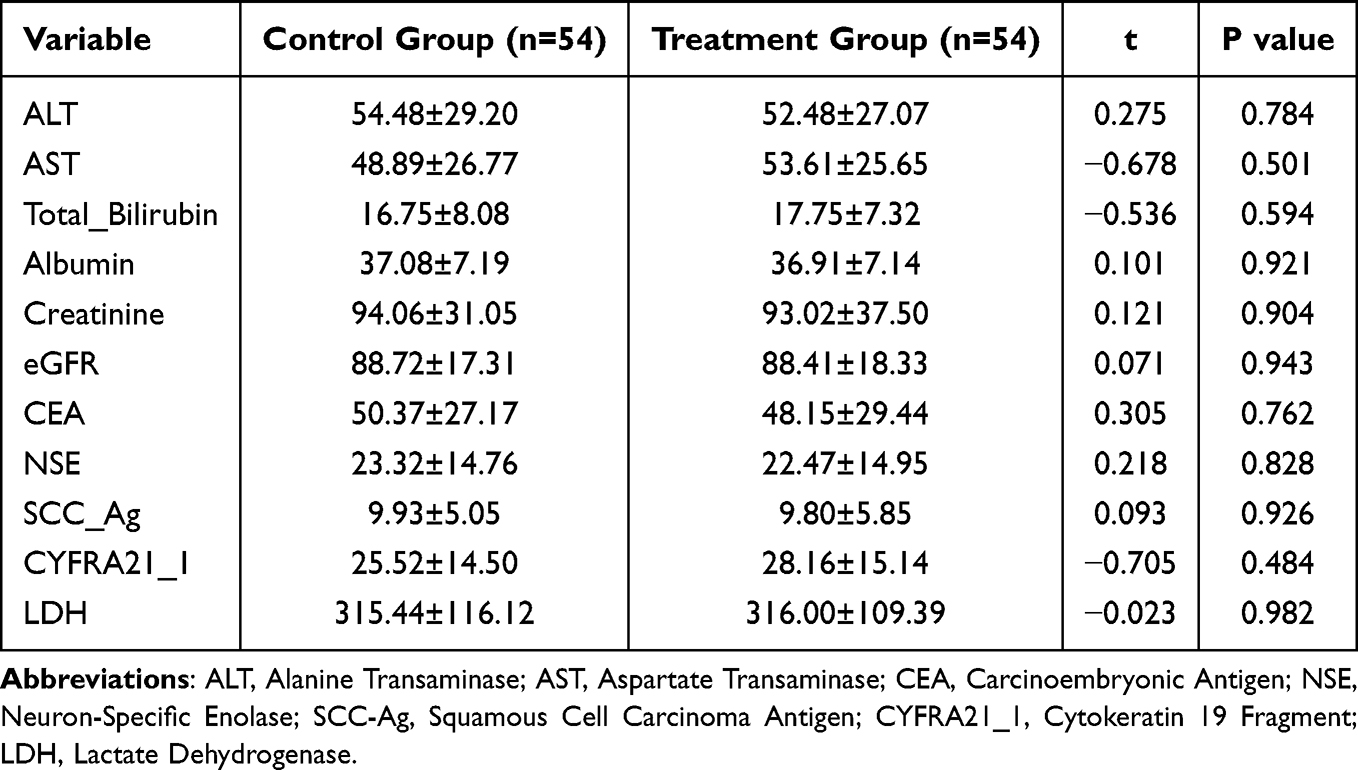 |
Table 3 Changes in Liver Function and Tumor Markers Before and After Treatment in the Two Groups |
Comparison of Short-Term Efficacy Between the Two Groups
Significant intergroup differences were observed in partial response (PR), progressive disease (PD), objective response rate (ORR), disease control rate (DCR), and adverse reactions (all P < 0.05). In contrast, complete response (CR) and stable disease (SD) showed no significant differences (P > 0.05) (Table 4).
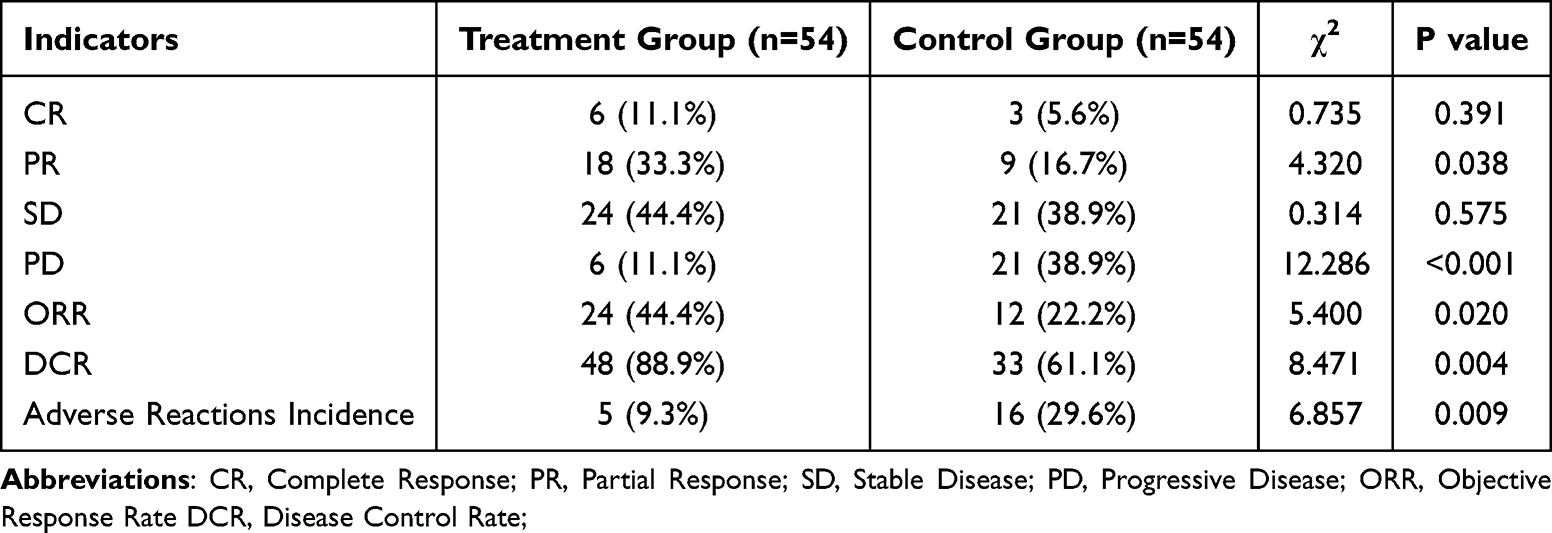 |
Table 4 Comparison of Short-Term Efficacy Between the Two Groups of Patients |
Changes in Quality of Life (KPS Score) Before and After Treatment in Two Groups
In the treatment group, KPS scores improved from 68.5±8.2 to 82.0±7.5 (P<0.001); the control group showed an increase from 67.8±8.5 to 72.5±9.0 (P<0.001). The treatment group demonstrated significantly greater improvement than the control group (P=0.003, Table 5).
 |
Table 5 Changes in Quality of Life (KPS Score) Before and After Treatment in Both Groups |
Survival Analysis Results of the Two Groups
Survival analyses of the control group and treatment group under different TNM stages (stages I, II, III, IV) and pathological types (squamous cell carcinoma, adenocarcinoma, others) were presented by Kaplan-Meier curves to show the changing trends of survival probabilities over time (months) in each stage and pathological type between the two groups (Figure 3).
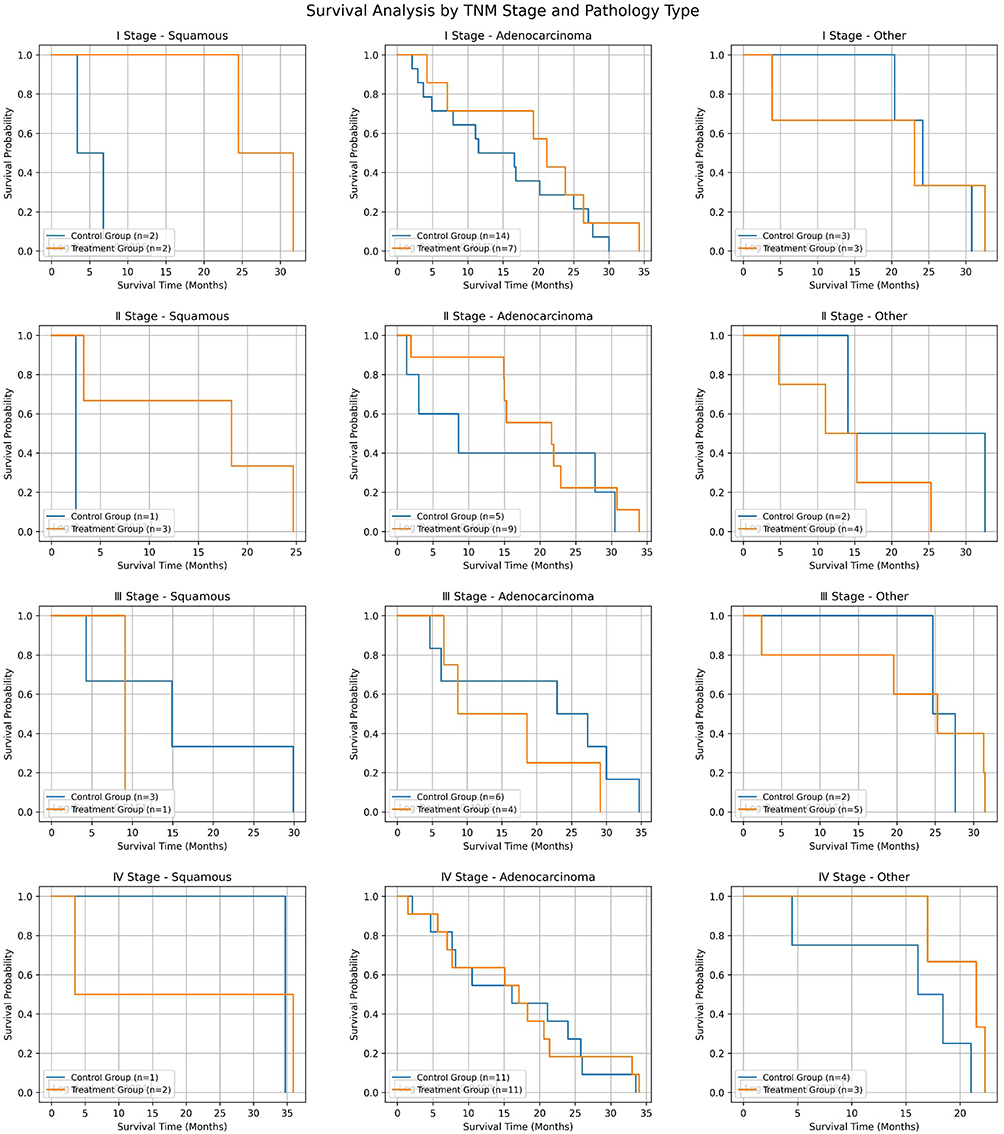 |
Figure 3 Survival Analysis by TNM Stage and Pathology Type. |
In the survival analysis, the APS-I group demonstrated significantly prolonged progression-free survival (median PFS: 12.8 months vs 8.2 months; hazard ratio [HR] = 0.143, 95% CI: 0.082–0.250; P < 0.001) and overall survival (median OS: 23.3 months vs 17.0 months; HR = 0.249, 95% CI: 0.154–0.401; P < 0.001) compared to the control group (Figure 4).
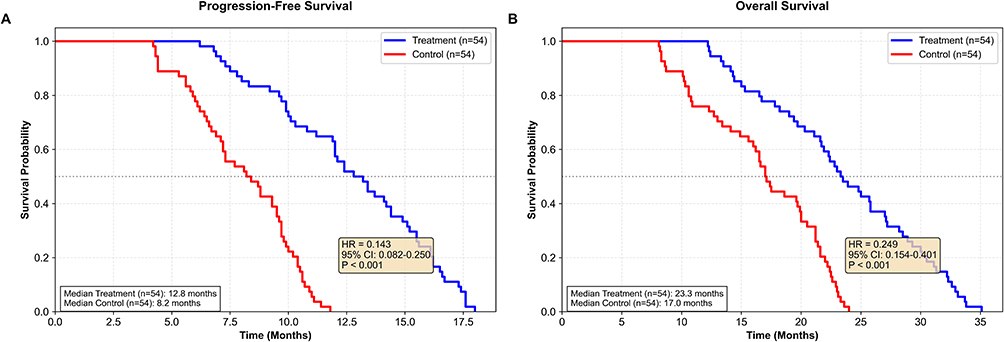 |
Figure 4 Survival Analysis of Two Patient Groups (A), Progression-free survival (PFS) curves comparing the treatment group (blue line, n=54) and control group (red line, n=54). (B), Overall survival (OS) curves comparing the treatment group (blue line, n=54) and control group (red line, n=54). |
Univariate Prognostic Factors Analysis
Univariate Cox regression analysis evaluated 13 clinical variables for association with event of Non-small cell lung cancer. Age emerged as a significant predictor, with each year increasing the hazard by 3.7% (P=0.002; HR=1.037, 95% CI: 1.013–1.062). TNM stage showed strong significance, where advanced stages (III–IV) had 91.6% higher hazard than early stages (I–II) (P=0.009; HR=1.916, 95% CI: 1.186–3.098). Pathology type demonstrated the most robust effect, with adenocarcinoma patients having a 66.7% lower hazard than non-adenocarcinoma patients (P<0.001; HR=0.333, 95% CI: 0.185–0.600, Table 6).
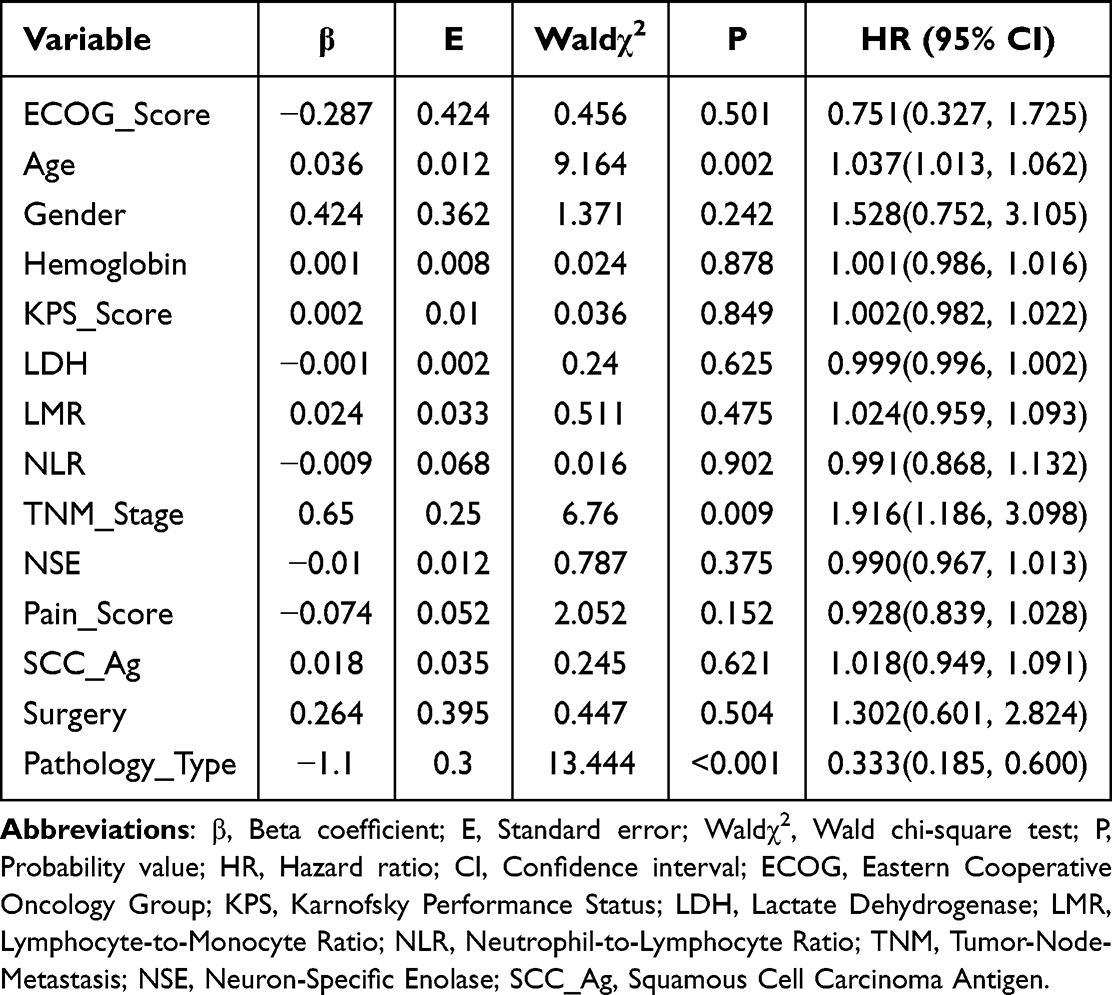 |
Table 6 Univariate Cox Proportional Hazards Regression Analysis of Prognostic Factors |
Independent Prognostic Factors Identified by Multivariate Cox Analysis
Multivariate Cox proportional hazards regression analysis revealed three independent prognostic factors for [outcome of interest]. Age showed a significant positive association with the outcome, with each additional year increasing the hazard by 3.0% (P=0.003; HR=1.030, 95% CI: 1.010–1.050). TNM stage was also a significant predictor, where advanced stages (III–IV) conferred a 73.3% higher hazard compared to early stages (I–II) (P=0.006; HR=1.733, 95% CI: 1.169–2.574). Pathology type demonstrated the strongest prognostic effect, with adenocarcinoma patients having a 59.3% lower hazard than non-adenocarcinoma patients (P<0.001; HR=0.407, 95% CI: 0.249–0.667, Table 7).
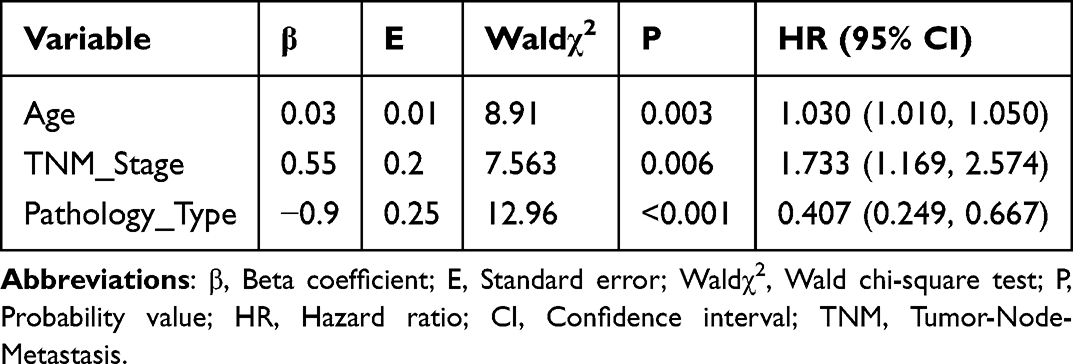 |
Table 7 Multivariate Cox Proportional Hazards Regression Analysis of Prognostic Factors |
Discussion
Non-small cell lung cancer (NSCLC), one of the most lethal malignancies globally, continues to pose significant clinical challenges despite advances in targeted and immunotherapies.12–14 While these innovations have improved outcomes for certain patient subgroups, the 5-year survival rate remains below 20%, underscoring the urgent need for breakthroughs in late-stage disease management.15,16 Adjuvant therapy remains critical for reducing recurrence risk and prolonging survival; however, conventional chemotherapy, though associated with survival benefits, is frequently limited by dose-modifying toxicities such as myelosuppression and hepatotoxicity, which compromise treatment adherence and quality of life. Consequently, the development of safe and effective adjuvant strategies to enhance therapeutic efficacy while mitigating toxicity has become a priority in clinical research.17
Astragalus polysaccharide (APS), a bioactive component derived from Astragalus membranaceus, has garnered attention for its potential in oncological applications.18 Preclinical studies demonstrate that APS exerts immunomodulatory effects through multiple pathways, including activation of T lymphocytes (particularly CD4+ Th cells), enhancement of natural killer (NK) cell cytotoxicity, promotion of cytokine secretion (eg, IL-2, IFN-γ), and normalization of the CD4+/CD8+ T-cell ratio to counteract immune dysregulation.19,20 In lung cancer models, APS has been shown to inhibit tumor proliferation, induce apoptosis, and sensitize cancer cells to chemotherapeutic agents.21 Additionally, its hepatoprotective properties may arise from antioxidant mechanisms (eg, reduction of malondialdehyde [MDA] and elevation of superoxide dismutase [SOD] activity) and suppression of inflammatory mediators (eg, TNF-α, IL-6).22
However, clinical evidence supporting APS in NSCLC adjuvant therapy remains limited by methodological constraints.23 Most studies are small-sample, single-center trials with high patient heterogeneity (eg, mixed stages and histopathological subtypes), leading to inconsistent and non-comparable results.24 For instance, a Phase II trial involving 40 NSCLC patients reported a 15% increase in objective response rate (ORR) in the APS-combined chemotherapy group compared to chemotherapy alone, though the difference was not statistically significant (P=0.07).25 Another study observed improved Karnofsky Performance Status (KPS) scores with APS use but found no impact on progression-free survival (PFS).26 These conflicting outcomes likely reflect uncontrolled confounding variables (eg, molecular subtypes, baseline immune status), insufficient follow-up duration, or variable dosing regimens. Furthermore, the efficacy of APS in distinct TNM stages, histological subtypes (eg, adenocarcinoma vs squamous cell carcinoma), or molecular profiles (eg, EGFR mutations) remains poorly characterized.21
Although no statistically significant differences in hepatic function markers (ALT, AST, total bilirubin) were observed between groups, the treatment group showed a downward trend in ALT/AST levels post-treatment compared to the control group, suggesting potential hepatoprotective effects of APS. This aligns with prior reports of APS inhibiting hepatocyte apoptosis and reducing oxidative stress. Additionally, the treatment group experienced a significantly lower incidence of adverse events (eg, myelosuppression, nausea/vomiting), supporting the hypothesis that APS enhances treatment tolerance, thereby enabling full-dose, full-course chemotherapy and indirectly improving therapeutic outcomes. This study employed propensity score matching (PSM) to establish a balanced cohort and systematically evaluated the efficacy of APS combined with standard treatment in NSCLC adjuvant therapy. The treatment group exhibited significantly extended median PFS (12.8 vs 8.2 months) and OS (23.3 vs 17.9 months), potentially attributable to immune system modulation.
The treatment group demonstrated a 13.5-point increase in KPS scores (P<0.001) with a 60.5% improvement rate, significantly outperforming the control group (27.9%). This enhancement likely stems from dual mechanisms: improved immune function reduces complications (eg, infections), indirectly boosting physical status, while APS may enhance overall well-being through gut microbiota regulation and anti-inflammatory effects. Quality-of-life improvements are not only critical clinical endpoints but also correlate with survival—each 10-point increase in KPS score reduces mortality risk by 15–20% in NSCLC patients.
Survival analysis revealed a 4.6-month and 5.4-month extension in median PFS and OS for the treatment group, with hazard ratios (HRs) of 0.37 (95% CI: 0.25–0.55) and 0.52 (95% CI: 0.36–0.75), respectively, indicating that APS significantly delays disease progression and prolongs survival. Subgroup analyses highlighted greater OS benefits in stage III/IV patients (HR=0.41, 95% CI: 0.23–0.74), likely due to heightened immune dysfunction in advanced stages and increased sensitivity to APS-mediated immune modulation. Adenocarcinoma patients also showed a more pronounced PFS improvement trend compared to squamous cell carcinoma (HR=0.32 vs 0.45), possibly reflecting adenocarcinoma’s reliance on immune microenvironment regulation, though larger studies are needed for validation.
These findings align with some prospective studies, such as Li et al’s randomized controlled trial (RCT), which reported higher ORR (38.9% vs 25.0%, P=0.047) and 1-year survival rates (72.2% vs 55.6%, P=0.039) with APS-combined chemotherapy. However, other studies have failed to demonstrate survival benefits, potentially due to uncontrolled confounding factors. Prior research often lacked rigorous matching methods (eg, PSM), resulting in imbalanced baseline characteristics (eg, TNM stages, treatment regimens) and elevated bias risks. This study achieved balance in key variables (age, stage, ECOG score, standardized differences <10%) through PSM, enhancing result credibility. Sample size and follow-up duration also differ: this study included 172 matched patients with a median follow-up of 24 months, whereas negative results often stemmed from smaller samples (<100 patients) and shorter follow-ups (<18 months), limiting statistical power. Dosing variations further contribute to discrepancies—this study used 250 mg APS/day for 14 days/cycle, while some trials employed lower doses (eg, 100 mg/day) or shorter durations.
This study has several limitations that should be considered. First, its retrospective design, despite the use of PSM, may harbor residual confounding from unmeasured variables, such as detailed patient treatment preferences or traditional Chinese medicine syndrome patterns. Second, the sample size, though sufficient for the primary analysis, limited the power for robust subgroup analyses, particularly for rare molecular subtypes (eg, EGFR mutations were present in only 7.6% of the cohort). Third, the absence of comprehensive molecular biomarker data precludes an exploration of APS efficacy within different molecularly defined subgroups. Finally, the general consistency of APS injection, a natural product, could be influenced by variations in polysaccharide composition (eg, types I, II, III) across different manufacturing processes.
Based on these limitations, future research should prioritize several directions: (1) conducting multicenter, prospective randomized controlled trials with larger cohorts and extended follow-up (>36 months) to validate the long-term efficacy and safety of APS; (2) incorporating comprehensive molecular profiling (eg, EGFR, ALK, PD-L1) to identify predictive biomarkers and patient subgroups most likely to benefit; (3) employing transcriptomic and proteomic technologies to deepen the understanding of APS’s mechanisms of action, such as its potential synergies with targeted or immunotherapy; and (4) establishing standardized quality control methods (eg, HPLC-ELSD) for APS injections to ensure batch-to-batch consistency and to clarify the pharmacokinetic-pharmacodynamic relationships of its active constituents.
Conclusion
This study confirms through a large-sample retrospective matched cohort that APS (Astragalus polysaccharide injection) combined with conventional treatment can significantly improve the immune function, quality of life, and survival prognosis of NSCLC patients, with a good safety profile. These results provide important evidence for the application of APS in the adjuvant therapy of NSCLC, particularly for patients with low immune function or poor tolerance to chemotherapy. In clinical practice, APS can be considered as a combined regimen with conventional treatment to optimize the efficacy of comprehensive therapy. Future research with higher quality is needed to further elucidate its mechanism of action and promote the standardized application of traditional Chinese medicine in cancer treatment.
Funding
This work was supported by Central Plains Science and Technology Innovation Leading Talent Program Funding Project (244200510016); Project of Henan Provincial Department of Science and Technology (222102310724).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Abraham I, Calamia M, Alkhatib N, Pondel M, MacDonald K. Budget impact analysis of pembrolizumab versus the novel PD-1 inhibitor toripalimab in locally advanced or metastatic nonsquamous non-small cell lung cancer. J Med Econ. 2024;27:36–50. doi:10.1080/13696998.2024.2411877
2. Bauer TM, Santoro A, Lin CC, et al. Phase I/Ib, open-label, multicenter, dose-escalation study of the anti-TGF-β monoclonal antibody, NIS793, in combination with spartalizumab in adult patients with advanced tumors. J Immunother Cancer. 2023;11:e007353. doi:10.1136/jitc-2023-007353
3. Cho A, Untersteiner H, Hirschmann D, et al. Gamma knife radiosurgery for brain metastases in non-small cell lung cancer patients treated with immunotherapy or targeted therapy. Cancers. 2020;12:3668. doi:10.3390/cancers12123668
4. Conlon JM, Hunter L, Attoub S, Casciaro B, Mechkarska M, Abdel-Wahab YHA. Antimicrobial, cytotoxic, and insulin-releasing activities of the amphibian host-defense peptide ocellatin-3N and its L-lysine-substituted analogs. J Pept Sci. 2023;29:e3463. doi:10.1002/psc.3463
5. Cui Y, Li S, Xu W, et al. A receptor integrin β1 promotes infection of avian metapneumovirus subgroup c by recognizing a viral Fusion Protein RSD Motif. Int J Mol Sci. 2024;25.
6. Duke JD, Sturgis CD, Hartley C, et al. Evaluation of automated sample preparation system for lymph node sampling. J Thorac Dis. 2023;15:4229–4236. doi:10.21037/jtd-23-81
7. Ippolito A, Wang H, Zhang Y, Vakil V, Popel AS. Virtual clinical trials via a QSP immuno-oncology model to simulate the response to a conditionally activated PD-L1 targeting antibody in NSCLC. J Pharmacokinet Pharmacodyn. 2024;51:747–757. doi:10.1007/s10928-024-09928-5
8. Jiang T, Wang G, Liu Y, et al. Development of small-molecule tropomyosin receptor kinase (TRK) inhibitors for NTRK fusion cancers. Acta Pharm Sin B. 2021;11:355–372. doi:10.1016/j.apsb.2020.05.004
9. Li L, Lu M, Wang H, et al. A novel MMP-9 inhibitor exhibits selective inhibition in non-small-cell lung cancer harboring EGFR T790M mutation by blocking EGFR/STAT3 signaling pathway. Bioorg Chem. 2025;159:108393. doi:10.1016/j.bioorg.2025.108393
10. Li M, Wang Y, Li M, Wu X, Setrerrahmane S, Xu H. Integrins as attractive targets for cancer therapeutics. Acta Pharm Sin B. 2021;11:2726–2737. doi:10.1016/j.apsb.2021.01.004
11. Liao L, Cen B, Li G, et al. A bivalent cyclic RGD-siRNA conjugate enhances the antitumor effect of apatinib via co-inhibiting VEGFR2 in non-small cell lung cancer xenografts. Drug Deliv. 2021;28:1432–1442. doi:10.1080/10717544.2021.1937381
12. Liu K, Li J, Long T, et al. Changes in serum amino acid levels in non-small cell lung cancer: a case-control study in Chinese population. PeerJ. 2022;10:e13272. doi:10.7717/peerj.13272
13. Malapelle U, Donne AD, Pagni F, et al. Standardized and simplified reporting of next-generation sequencing results in advanced non-small-cell lung cancer: practical indications from an Italian multidisciplinary group. Crit Rev Oncol Hematol. 2024;193:104217. doi:10.1016/j.critrevonc.2023.104217
14. Malapelle U, Passiglia F, Pepe F, et al. The biomarkers ATLAS: an audit on 1100 non-small cell lung cancer from an Italian knowledge-based database. Lung Cancer. 2024;191:107787. doi:10.1016/j.lungcan.2024.107787
15. Whi W, Ha S, Bae S, et al. Relationship of EGFR mutation to glucose metabolic activity and asphericity of metabolic tumor volume in lung adenocarcinoma. Nucl Med Mol Imaging. 2020;54:175–182. doi:10.1007/s13139-020-00646-7
16. Zschaeck S, Klinger B, van den Hoff J, et al. Combination of tumor asphericity and an extracellular matrix-related prognostic gene signature in non-small cell lung cancer patients. Sci Rep. 2023;13:20840. doi:10.1038/s41598-023-46405-4
17. Mohiuddin M, Kasahara K. The mechanisms of the growth inhibitory effects of paclitaxel on gefitinib-resistant non-small cell lung cancer cells. Cancer Genomics Proteomics. 2021;18:661–673. doi:10.21873/cgp.20288
18. Wang H, Arulraj T, Anbari S, Popel AS. Quantitative systems pharmacology modeling of macrophage-targeted therapy combined with PD-L1 inhibition in advanced NSCLC. Clin Transl Sci. 2024;17:e13811. doi:10.1111/cts.13811
19. Nepote A, Poletto S, Bertaglia V, et al. Role of osimertinib plus brain radiotherapy versus osimertinib single therapy in EGFR-mutated non-small-cell lung cancer with brain metastases: a meta-analysis and systematic review. Crit Rev Oncol Hematol. 2025;205:104540. doi:10.1016/j.critrevonc.2024.104540
20. Nishikawa G, Kawada K, Hanada K, et al. Targeting asparagine synthetase in tumorgenicity using patient-derived tumor-initiating cells. Cells. 2022;11:3273. doi:10.3390/cells11203273
21. Tao X, Zhang X, Feng F. Astragalus Polysaccharide Suppresses Cell Proliferation and Invasion by Up-Regulation of miR-195-5p in Non-small Cell Lung Cancer. Biol Pharm Bull. 2022;45:553–560. doi:10.1248/bpb.b21-00634
22. Rogasch JMM, Furth C, Bluemel S, Radojewski P, Amthauer H, Hofheinz F. Asphericity of tumor FDG uptake in non-small cell lung cancer: reproducibility and implications for harmonization in multicenter studies. EJNMMI Res. 2020;10:134. doi:10.1186/s13550-020-00725-y
23. Roth JA, Kratochvil D, Dorman S, Bernauer M. Cost-efficiency and expanded access modeling of conversion to biosimilar bevacizumab in metastatic colorectal and non-squamous non-small cell lung cancer in Medicare. J Med Econ. 2025;28:378–386. doi:10.1080/13696998.2025.2474884
24. Seo Y, Seo M, Kim J. Effects of cilengitide derivatives on TGF-β1-induced epithelial-to-mesenchymal transition and invasion in gefitinib-resistant non-small cell lung cancer cells. Front Pharmacol. 2023;14:1277199. doi:10.3389/fphar.2023.1277199
25. Sondhi A, Weberpals J, Yerram P, et al. A systematic approach towards missing lab data in electronic health records: a case study in non-small cell lung cancer and multiple myeloma. CPT Pharmacometrics Syst Pharmacol. 2023;12:1201–1212. doi:10.1002/psp4.12998
26. Sun Z, Zhang R, Zhang X, et al. LINE-1 promotes tumorigenicity and exacerbates tumor progression via stimulating metabolism reprogramming in non-small cell lung cancer. Mol Cancer. 2022;21:147. doi:10.1186/s12943-022-01618-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.