Back to Journals » Advances in Medical Education and Practice » Volume 17
Analysis of District Residency Program in Surgical Specialties at a University Teaching Hospital
Authors Ravi V, Ramachandran PI ![]() , Silambanan S
, Silambanan S
Received 10 June 2025
Accepted for publication 25 February 2026
Published 8 July 2026 Volume 2026:17 546051
DOI https://doi.org/10.2147/AMEP.S546051
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Sateesh Arja
Vaishnavi Ravi,1 Ponniah Iyyappan Ramachandran,2 Shanthi Silambanan3
1Department of Ophthalmology, Sri Ramachandra Institute of Higher Education and Research, Chennai, TN, India; 2Department of General Surgery, Sri Ramachandra Institute of Higher Education and Research, Chennai, TN, India; 3Department of Biochemistry, Sri Ramachandra Institute of Higher Education and Research, Chennai, TN, India
Correspondence: Ponniah Iyyappan Ramachandran, Email [email protected]
Background: The District Residency Programme (DRP) mandates three-month postings for postgraduate residents in district hospitals across India in various specialties to address healthcare disparities. While the programme demonstrates potential benefits in general medical specialties, its impact on surgical training requires critical evaluation.
Methods: This mixed-methods study involved 75 postgraduate surgical residents who completed mandatory DRP postings at a university teaching hospital in India. Data were collected through standardized questionnaires with Likert-scale items and qualitative open-ended questions, analyzed using descriptive statistics and thematic analysis.
Results: Quantitative findings revealed significant limitations in surgical exposure, with 72% of residents reporting limited clinical exposure and 64% experiencing reduced hands-on surgical training during DRP. However, 90% reported enhanced understanding of community healthcare needs, and 80% noted improved patient communication skills. Qualitative analysis identified three key themes: the tension between autonomy and supervision, enhanced community connection, and frustration with resource limitations. While residents valued the increased decision-making autonomy and community engagement, they expressed concerns about inadequate specialist supervision and infrastructure deficiencies impacting surgical skill development.
Conclusion: The DRP significantly contributes to residents’ professional identity formation and community health orientation but may compromise specialized surgical training. Recommendations include developing structured surgical curricula for district settings, implementing enhanced supervision models, integrating technology-enhanced learning, improving infrastructure, providing faculty development for district hospital staff, and establishing systematic programme evaluation to optimize the DRP for surgical specialties.
Keywords: district residency programme, surgical education, postgraduate medical training, rural healthcare, mixed-methods research, competency-based education, distributed medical education, community-oriented medical education, professional identity formation, healthcare disparities
Introduction
The Indian healthcare system grapples with a complex interplay of challenges, stemming from a vast and diverse population, a skewed distribution of healthcare professionals favoring urban centers, and a resultant disparity in access to quality medical services, particularly in rural and semi-urban areas according to Gupta et al1 This multifaceted problem necessitates innovative and strategic interventions to bridge the urban-rural healthcare gap and ensure equitable access to specialized medical care for all citizens according to Fedyanova.2 The National Medical Commission, recognizing the urgency of this situation, introduced the District Residency Program as a pivotal step towards addressing these systemic issues Shah.3 According to a report by MacQueen et al, the DRP, implemented in 2020, mandates a three-month posting for second-year postgraduate medical students in designated district hospitals, serving as a strategic deployment of medical expertise to underserved regions4 This initiative is conceived not only to augment healthcare delivery at the district level by providing much-needed manpower but as Rosa and Lopes et al points out, it aims to expose postgraduate students to the unique challenges and realities of healthcare practice in resource-constrained settings5 By immersing residents in these environments, the DRP aims to foster a deeper understanding of community health needs, improve their clinical acumen in diverse settings, and cultivate a sense of social responsibility towards underserved populations.
While the DRP has shown promise and reported successes in broad medical specialties such as general medicine, pediatrics, and community medicine, the program’s impact on surgical disciplines remains an area requiring deeper investigation and critical evaluation. Surgical training, by its very nature, demands consistent and immersive exposure to operative procedures, a meticulously maintained sterile environment, and access to advanced surgical equipment and technologies. These elements are crucial for the development of technical proficiency, surgical decision-making skills, and the ability to manage complex surgical cases effectively. Chu et al in his study emphasized that the success of surgical training hinges on a structured and supervised environment where residents can progressively hone their skills under the guidance of experienced surgeons6 Given the unique demands of surgical training and the potential variations in resource availability and surgical case mix across different district hospitals, according to Young et al, it is imperative to rigorously assess the effectiveness of the DRP in meeting the specific training needs of surgical residents7 A prior study by Abdulrahman et al investigated the integration of research into residency programs in Dubai, highlighting the need for systematic analysis to assess efficiency and outcomes, which underscores the importance of evaluating the DRP’s impact on surgical training8 Furthermore, trauma training programs in low- and middle-income countries face sustainability and ethical challenges according to Livergrant et al, highlighting the need for continuous knowledge and skill updates9 Therefore, a thorough evaluation of the DRP’s impact on surgical training is crucial to identify areas of strength, pinpoint potential shortcomings, and recommend evidence-based modifications to optimize the program for surgical specialties.
The present study endeavors to address this critical gap in understanding by conducting a comprehensive analysis of the DRP’s effectiveness in surgical postgraduate training within a university teaching hospital setting. The study will specifically focus on evaluating the impact of the DRP on the clinical and surgical skill development of surgical residents, as well as its influence on their professional behavior and attitudes towards community healthcare needs.
Literature Review
The implementation of the District Residency Program represents a significant policy intervention aimed at addressing the disparities in healthcare access and quality that persist between urban and rural areas in India. The DRP is designed to leverage the expertise and energy of postgraduate medical students to strengthen healthcare delivery systems at the grassroots level, while simultaneously providing these future specialists with invaluable exposure to the realities of medical practice in resource-constrained settings. While the core objectives of the DRP are broadly applicable across medical specialties, the specific challenges and opportunities presented by the program may vary considerably depending on the nature of the discipline. Surgical specialties, in particular, present a unique set of considerations due to the intensive technical training, specialized infrastructure, and consistent exposure to operative procedures required to achieve competence.
A study done by Atiyeh et al highlighted the critical shortage of surgeons and anesthesiologists in low- and middle-income countries, suggesting that task shifting and training of non-physician clinicians is the only viable option, particularly in developing countries10 The role of family physicians in delivering essential surgical care in underserved areas has gained recognition, with evidence by Kim et al suggesting that with appropriate training and support, family physicians can effectively perform a range of surgical procedures, thereby improving access to timely and life-saving interventions11 Furthermore, according to Sani et al, in rural settings where access to specialized surgical care is limited, general practitioners with additional surgical training can play a crucial role in providing essential surgical services, particularly in district hospitals.12
The assessment of surgical skills has evolved significantly, with the introduction of simulation-based training and objective assessment tools designed to evaluate technical competence and decision-making abilities in a standardized and reliable manner The integration of simulation into surgical training curricula has been shown to improve surgical skills, reduce errors, and enhance patient safety. According to a study by Gajewski et al, the implementation of surgical supervision models in district hospitals can significantly improve the quality of surgical care provided to rural populations13 By providing mentorship, guidance, and support to surgeons working in these settings, experienced specialists can help to ensure that patients receive safe and effective surgical treatment, even in resource-constrained environments Smith et al emphasizes the importance of development and implementation of standardized surgical training programs in low-resource settings to ensure that surgical residents receive consistent and high-quality training, regardless of their location.14
Methodology
Study Design and Setting
The present study was carried out as a mixed methods study among postgraduate surgical residents of a University medical college in Chennai.
Study Participants and Selection Criteria
All the postgraduate surgical residents pursuing post-graduation degree in general surgery, obstetrics and gynaecology, otorhinolaryngology and orthopedics of the University medical college who underwent DRP posting in various designated district hospitals during the period between October 2024 and January 2025 constituted the study participants. Residents who could not be contacted and/or refused to participate in the study were excluded.
Sample Size and Sampling
There were a total of 75 postgraduate surgical residents in the University medical college during the study period (4months). All the residents were selected for the study.
Ethical Approval and Informed Consent
The study protocol was reviewed and approved by the Institutional Ethics Committee of Sri Ramachandra Institute of Higher Education and Research, the university teaching hospital in which the study was undertaken (IEC No: SRIHER/PGS/2023/047). Informed consent was obtained from all participating residents prior to their inclusion in the study, with clear explanations of the study’s purpose, procedures, potential risks and benefits, and the right to withdraw at any time without penalty. Anonymity and confidentiality were maintained throughout the data collection and analysis process.
Data Collection
Data collection comprised of two components:
- A structured, self administered questionnaire was used to obtain qualitative data on perceptions of clinical and surgical skill development, behavioral changes, and overall satisfaction with the DRP experience. The questionnaire incorporated a Likert scale to assess residents’ agreement with statements related to various aspects of the DRP, such as the quality of surgical exposure, the adequacy of supervision, the availability of resources, and the impact on their attitudes towards rural healthcare.
- An open-ended section to to elicit qualitative data on residents’ experiences, challenges, and suggestions for improving the DRP. The qualitative data obtained from the open-ended questions were analyzed using thematic analysis to identify recurring themes and patterns in the residents’ narratives. The residents were contacted, and those who did not respond after three attempts or refused to participate were excluded from the study.15
Data Analysis
The quantitative data collected through the questionnaire were analyzed using descriptive statistics, such as means, standard deviations, and frequencies, to summarize the residents’ responses. The qualitative data obtained from the open-ended questions were analyzed using thematic analysis to identify recurring themes and patterns in the residents’ narratives. The analysis of qualitative data was conducted independently by two researchers to ensure inter-coder reliability and minimize bias.
Results
Demographics
A total of 75 postgraduate students across various surgical specialties participated in the study. Among them, 60% were male and 40% were female, with a mean age of 28.2 years. The distribution of respondents by specialty was as follows: General Surgery (38%), Orthopaedics (24%), Obstetrics and Gynaecology (20%), and ENT (18%) (Table 1 and Figure 1A).
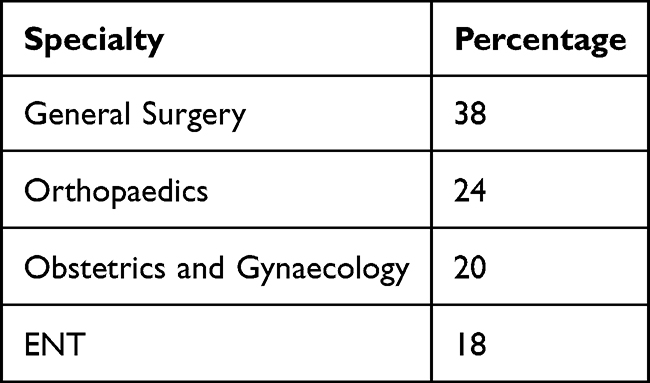 |
Table 1 Participant Demographics by Specialty (N=75) Mean Age: 28.2 Years | Gender: 60% Male, 40% Female |
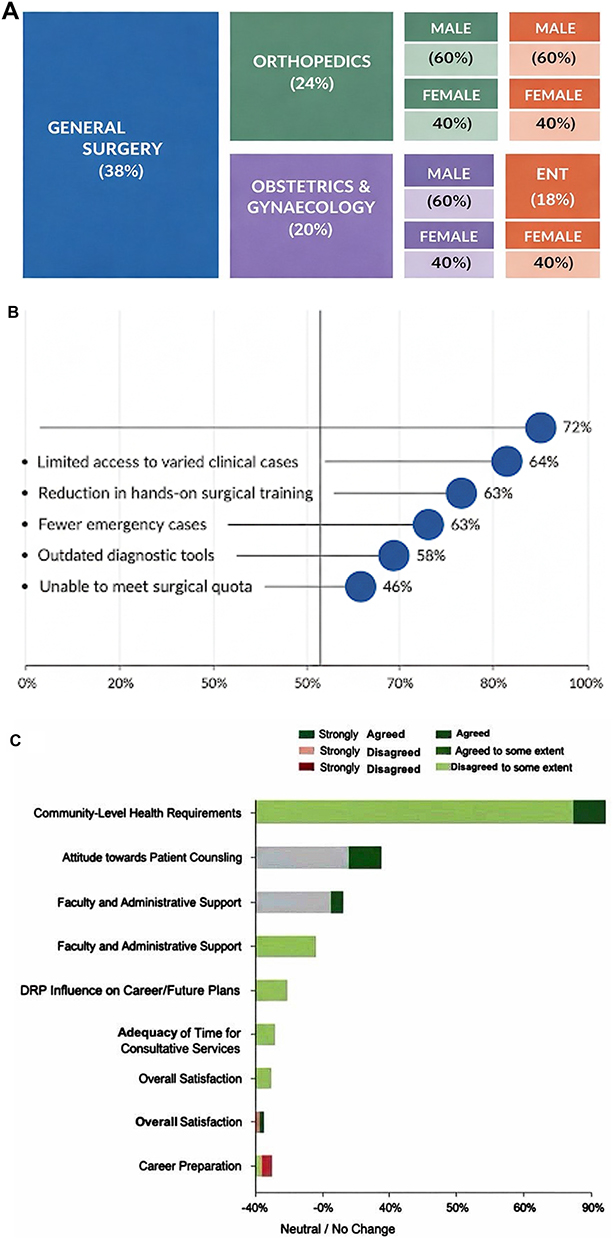 |
Figure 1 Summary of Participant Data and District Residency Program (DRP) Evaluation. (A) Nested treemap illustrates cohort demographics by specialty and gender. (B) Diverging dot plot shows the percentage of residents reporting specific clinical and surgical deficiencies; the 50% reference line indicates a majority experience. (C) Diverging stacked bar chart visualizes resident perceptions of program impact, with positive responses (Agree/Strongly Agree) shown in green and negative responses (Disagree/Strongly Disagree) in red, centered on a neutral/no change baseline. |
Clinical Exposure
Respondents reported notable limitations in their clinical exposure during the District Residency Program (DRP). Approximately 72% felt they had limited access to a variety of clinical cases, and 63% reported fewer opportunities to handle emergency cases compared to their parent institutions. Additionally, 58% indicated that they had to work with outdated or suboptimal diagnostic tools, which may have impeded effective clinical decision-making (Figure 1B).
Surgical Exposure
Surgical training during the DRP appeared constrained for many participants. Only 28% of residents reported being able to assist in major surgical procedures, while 64% noted a reduction in hands-on surgical skill training. Furthermore, 46% stated that they were unable to meet their monthly surgical quota during the three-month DRP period, highlighting a potential compromise in surgical competency development.
Perceptions of Program Impact
Analysis of Likert-scale responses revealed varied perceptions of the DRP across several educational and professional domains (Table 2 and Figure 1C):
- Overall satisfaction was moderate, with approximately 40–50% of participants indicating a neutral stance and 30–35% expressing agreement to some extent. Only a small proportion expressed strong satisfaction or dissatisfaction.
- Regarding faculty and administrative support, 45% of respondents agreed to some extent and 35% strongly agreed that they felt supported during their posting. However, 20% were neutral or disagreed, suggesting variability in mentorship quality.
- When asked if the DRP prepared them for their future careers, 30–40% disagreed, 30–35% agreed to some extent, and 20–25% agreed, indicating a divided perception on the program’s career-readiness impact.
- Concerning the DRP’s influence on career or future plans, a significant 80% of students acknowledged a positive impact (40% agreed, 40% agreed to some extent) (Table 3).
- On the adequacy of time for consultative services, 50% agreed to some extent, 30% agreed, and 20% disagreed, reflecting moderate satisfaction with time allocation.
- Regarding awareness of community-level health requirements, 60% agreed to some extent and 30% agreed, indicating that the DRP provided meaningful exposure to rural healthcare needs.
- In terms of attitude toward patient counseling and communication, 50% experienced a positive shift to some extent, while 30% strongly agreed. Nevertheless, 20% reported no significant change.
- When asked if the three-month duration of the DRP was sufficient, responses were split: 50% agreed to some extent, 30% agreed, and 20% found it inadequate, suggesting a need to reassess the duration or structure of the posting.
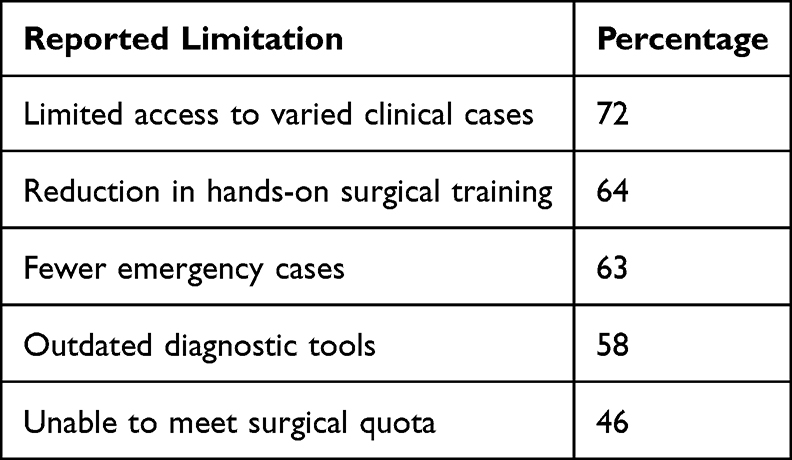 |
Table 2 Reported Deficiencies in Clinical & Surgical Exposure |
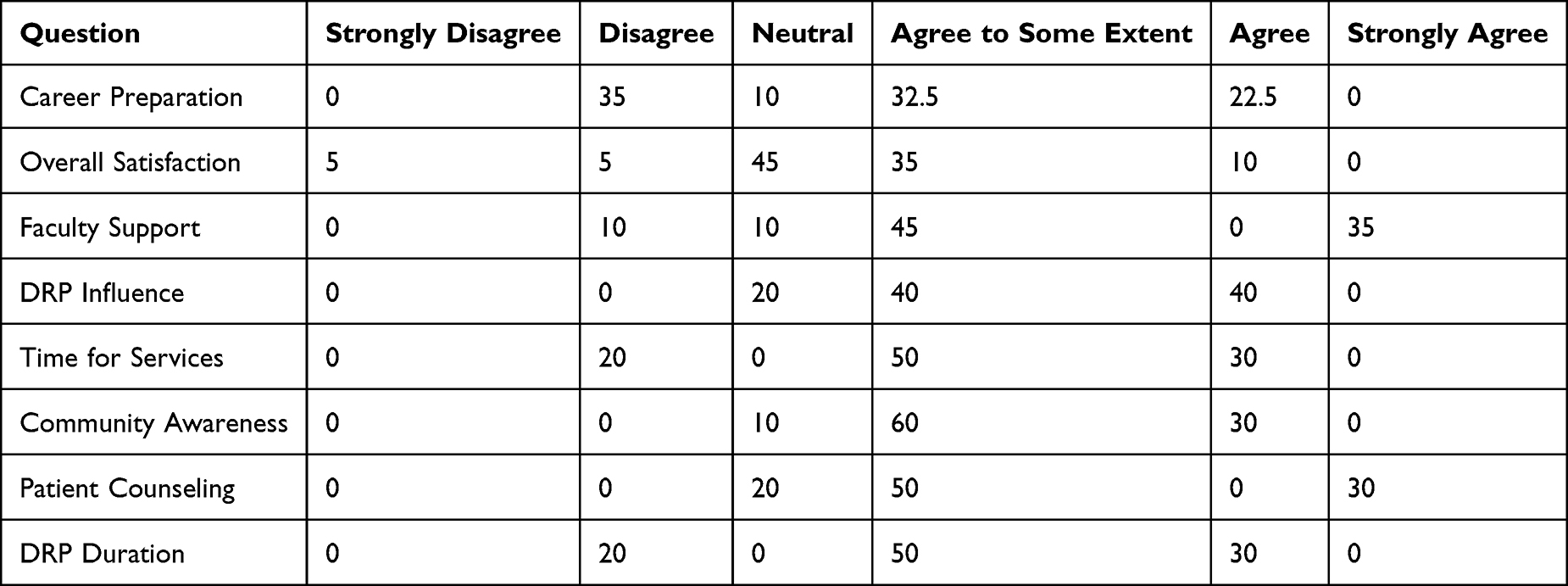 |
Table 3 Perceptions of Program Impact |
Qualitative Themes
Analysis of open-ended responses revealed three dominant themes:
- Autonomy vs. Supervision: Many residents appreciated the increased autonomy offered by district hospitals but simultaneously expressed concern over the lack of specialist supervision, which they felt was crucial for surgical learning and safety.
- Community Connection: Respondents highlighted a positive experience in dealing with diverse socio-cultural and economic backgrounds in rural populations. They viewed this as a valuable opportunity to enhance empathy and communication.
- Resource Limitation Frustration: There was widespread frustration regarding inadequate facilities, such as the lack of laparoscopic equipment, insufficient ICU support, and limited surgical infrastructure, which they believed hindered optimal learning and service delivery.
Discussion
The results of this study shed light on the multifaceted impact of the District Residency Program on surgical postgraduate training in a university teaching hospital. While the DRP aims to address healthcare disparities and enhance community health services, its effectiveness in surgical education is a subject of debate given the emphasis on hands-on experience and specialized supervision in surgical training. The results were comparable with studies done by Hatcher et al and Rourke et al.16,17
Clinical and Surgical Exposure
The study indicates that surgical residents face notable limitations in clinical and surgical exposure during their DRP postings, similar to a study done by Long and Sweeny et al18 The limited access to diverse clinical cases and hands-on surgical opportunities is a significant concern, particularly in surgical specialities where practical experience is essential for developing competency, similar to a study one by Malloy et al19 Surgical training necessitates consistent engagement in operative procedures within sterile environments, so the absence of these elements can impede skill acquisition, according to Stefanidis et al.20
This discrepancy in surgical exposure between parent institutions and district hospitals raises questions about the program’s design and implementation, which may inadvertently compromise surgical residents’ training quality. The study reveals the critical importance of adequate clinical material in medical education, noting that no single hospital provides sufficient opportunities to meet all curriculum learning objectives, similar to the study by Colquhoun et al21 This underscores the need for targeted interventions to augment clinical exposure during DRP postings to ensure residents meet the expected competency levels. Residents acknowledged that the DRP improved their understanding of healthcare challenges in resource-constrained settings and fostered a more patient-centered approach. However, these gains must be weighed against the potential loss of specialized surgical training. Furthermore, residents felt that they were better prepared to handle a variety of medical conditions with limited resources, which is a valuable skill for practice in diverse healthcare environments. Program satisfaction was moderate, and there were divisions on faculty and administrative support.
Behavioral and Attitudinal Changes
While surgical skill development is a primary focus of surgical residency, the DRP has shown promise in fostering important behavioral and attitudinal changes among residents. The program’s exposure to community-based healthcare delivery can significantly improve surgical residents’ communication skills, cultural sensitivity, and understanding of the socio-economic factors influencing patient care, similar to the findings of Petrushnko et al22 Residents also reported improved confidence in their clinical decision-making abilities and enhanced problem-solving skills when faced with limited resources. The increased autonomy during DRP postings allows residents to take on more responsibility, which can boost their self-assurance and preparedness for independent practice, as observed by Bisgaard et al23 According to a study by Kraus et al, the insights into palliative care education highlight the importance of communication skills, pain management, and ethical considerations in end-of-life care.24 These skills are highly relevant to surgical practice, where surgeons often encounter patients with advanced diseases requiring comprehensive care. The attitudinal and behavioral changes are particularly relevant, as residency is a formative period where values such as empathy, cultural competence, and humanism are either reinforced or eroded, according to Nivet and Berlin.25 Therefore, while surgical exposure may be limited, the DRP offers a unique opportunity to nurture well-rounded surgeons committed to addressing healthcare disparities.
Recommendations
To enhance the effectiveness of the District Residency Program in surgical specialties, several modifications and improvements are recommended. Recommendations to Improve the Effectiveness of the District Residency Program in Surgical Specialties.
Structured Surgical Curriculum
A standardized surgical training curriculum needs to be be implemented across all district hospitals participating in the DRP. This curriculum should outline specific learning objectives, competencies, and assessment methods to ensure that residents receive adequate surgical exposure and training during their DRP. It is essential that the curriculum is tailored to the resources and infrastructure available at each district hospital, focusing on essential surgical skills and procedures that are relevant to the local context. Consideration should be given to integrating virtual reality or simulation-based training to supplement the hands-on surgical experience, particularly in settings with limited resources. Ensuring that the learning environment adequately meets educational principles is crucial, irrespective of duty hours (Ulmer et al)26 For instance, implementing comprehensive andragogy, which focuses on tailoring education to the needs and experiences of adult learners, can significantly enhance the learning experience.
Mentorship and Supervision
Establishment of a mentorship program that connects surgical residents with experienced surgeons in both the parent institutes and the district hospitals could modify the perception of the overall programme among the residents. Mentors could provide guidance, support, and feedback to residents throughout their DRP, helping them to navigate the challenges of working in resource-limited settings and develop their surgical skills. Regular supervision by qualified surgeons is essential to ensure patient safety and provide residents with opportunities to learn from experienced practitioners. Allocation of additional resources to district hospitals to improve infrastructure, equipment, and supplies for surgical training could evade majority of the challenges faced by the residents.
Investing in telemedicine and remote consultation technologies can help to bridge the gap between specialist surgeons in parent institutes and residents in district hospitals. – may be contradictory as you have earlier mentioned that surgery requires in-person hands on practical training- suggest to remove this.
Community Engagement and Cultural Competence
Providing residents with training in community engagement and cultural competence could enhance their ability to communicate with patients from diverse backgrounds and understand the unique healthcare needs of rural communities. This training may cover topics such as cultural sensitivity, communication skills in regional languages, and strategies for addressing health disparities. This may include increasing capacity for surgical volume and workforce in these settings similar to the observations by Kamarajah and Alexander.27
Evaluation and Feedback
Implementing a robust evaluation system to assess the effectiveness of the DRP in achieving its objectives can go a long way in improving the outcomes it intends. This system could include regular feedback from residents, mentors, and patients, as well as objective measures of surgical skill development and knowledge acquisition. The feedback may be used to identify areas for improvement and refine the DRP curriculum and implementation strategies.
The introduction of the District Residency Program by the National Medical Commission represents a crucial step towards addressing the disparities in healthcare access and quality in India as highlighted by Bust and Chu.28 According to Monteleone, the experiences of residents during their training significantly influence their practices throughout their careers.29
Addressing Challenges Faced in Rural Postings
As highlighted by Thapa et al, Residents often face difficulties in rural postings due to the lack of guidance and senior support for handling varied medical situations30 The absence of specialist supervision, particularly in surgical disciplines, can lead to feelings of isolation and inadequacy among residents. Moreover, the infrastructure and resource limitations in district hospitals pose significant challenges to providing quality surgical care and achieving optimal learning outcomes. To address these challenges, the DRP should focus on providing adequate support and supervision to residents during their rural postings. This includes assigning experienced surgeons as mentors who can provide guidance and support remotely or through periodic visits to the district hospitals. Additionally, efforts should be made to improve the infrastructure and resource availability in district hospitals to create a more conducive environment for surgical training. According to Chu et al, the rural health workforce is essential to addressing disparities and improving health outcomes in underserved areas.6
Integration of Technology
The integration of technology can significantly enhance the educational experience and skill development of surgical residents during their DRP. Telemedicine platforms can facilitate remote consultations with specialists, providing residents with access to expert advice and guidance in complex cases. Surgical simulation tools can provide residents with opportunities to practice surgical skills in a safe and controlled environment, improving their confidence and competence. Mobile health applications can be used to deliver educational content, track resident progress, and facilitate communication between residents and mentors.
Financial and Logistical Support
Providing adequate financial and logistical support to residents during their DRP is essential to ensure their well-being and facilitate their participation in the program. This includes providing stipends to cover living expenses, transportation allowances, and accommodation facilities, as highlighted by Nielsen et al31 According to Totten et al, Inadequate internet access in rural areas poses a significant barrier to telehealth and remote training programs, which can reduce the utility of teleconsultations32 Therefore, providing residents with access to reliable internet connectivity is essential to enable them to participate in online learning activities and access online resources.
Addressing these multifaceted challenges through targeted interventions and policy reforms can transform the DRP into a robust platform for training competent and compassionate surgeons who are equipped to serve the diverse healthcare needs of the nation. As highlighted by Diaz-Navarro et al, cultivating support and ensuring consistent resourcing for healthcare simulation is vital, and leveraging virtual approaches can facilitate accessibility across various settings.33
Conclusion
The District Residency Program holds immense potential for transforming surgical training and improving healthcare delivery in India. Despite the success of such medical initiatives, as emphasized by Syed-Abdul et al, limited progress has been made in establishing sustained and significant improvements in surgical access on a broad scale.34 Also, as Alam et al pointed out, frequent evaluations of training programs ensure safe and productive environments for residents and affect performance and patient care.35
By addressing the challenges and implementing the recommendations outlined in this analysis, the DRP can be optimized to provide surgical residents with meaningful learning experiences, enhance their clinical and surgical skills, and instill in them a sense of commitment to serving underserved communities.
Acknowledgment
NMC nodal centre for faculty development, SRMC & RI.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gupta D, Yadav SK, Gupta NM, Piyush AR, Nath B. Perception of medical student regarding factors influencing the decision to serve in rural health services of Uttarakhand. J Prevent Med Holistic Health. 2020;6:37. doi:10.18231/j.jpmhh.2020.007
2. Fedyanova Y. Incentivizing young doctors to practise in underserved areas. CMAJ. 2018;190:E203–11. doi:10.1503/cmaj.109-5563
3. Shah JN. Taking Specialist Surgical Services to the Rural District Hospitals at One Forth Cost: a Sustainable ‘Return on Investment’ Public Health Initiative of Patan Hospital. Patan Acad Health Sci Nepal Kathmandu Univ Med J (KUMJ). 2015;13(50):186–192. PMID: 26643841. doi:10.3126/kumj.v13i2.16797
4. MacQueen IT, Maggard-Gibbons M, Capra G, et al. Recruiting rural healthcare providers today: a systematic review of training program success and determinants of geographic choices. J Gen Intern Med. 2018;33(2):191–199. PMID: 29181791; PMCID: PMC5789104. doi:10.1007/s11606-017-4210-z
5. Rosa SD, Lopes RE. Multiprofessional residency in healthcare and postgraduate education in Brazil: historical observations. Work Health Educ. 2009;7(3). doi:10.1590/S1981-77462009000300006
6. Chu K, Maine R, Duvenage R. We asked the experts: the role of rural hospitals in achieving equitable surgical access in low-resourced settings. World J Surg. 2021;45(10):3016–3018. PMID: 34338826; PMCID: PMC8327595. doi:10.1007/s00268-021-06271-5
7. Young L, Anderson E, Gurney T, et al. A comparative evaluation of quality and depth of learning by trainee doctors in regional, rural, and remote locations. BMC Med Educ. 2023;23(1):215. PMID: 37020284; PMCID: PMC10077336. doi:10.1186/s12909-023-04175-7
8. Abdulrahman M, Ahmed A, Carrick FR. Implementing resident research program to enhance physicians research in the United Arab Emirates. Int J Appl Basic Med Res. 2019;9(2):75–79. PMID: 31041168; PMCID: PMC6477951. doi:10.4103/ijabmr.IJABMR_183_18
9. Livergant RJ, Demetrick S, Cravetchi X, et al. Trauma training courses and programs in low- and lower middle-income countries: a scoping review. World J Surg. 2021;45(12):3543–3557. PMID: 34486080; PMCID: PMC8572832. doi:10.1007/s00268-021-06283-1
10. Atiyeh BS, Gunn SW, Hayek SN. Provision of essential surgery in remote and rural areas of developed as well as low and middle income countries. Int J Surg. 2010;8(8):581–585. PMID: 20659597. doi:10.1016/j.ijsu.2010.07.291
11. Kim EE, Araujo D, Dahlman B, et al. Delivery of essential surgery by family physicians. Bull World Health Organ. 2020;98(11):766–772. PMID: 33177773; PMCID: PMC7607462. doi:10.2471/BLT.20.252056
12. Sani R, Sanoussi S, Didier JL, Salifou GM, Abarchi H. Rural surgery in Niger: a multicentric study in 21 district hospitals. Indian J Surg. 2015;77(Suppl 3):822–826. PMID: 27011464; PMCID: PMC4775620. doi:10.1007/s12262-013-1015-0
13. Gajewski J, Monzer N, Pittalis C, et al. Supervision as a tool for building surgical capacity of district hospitals: the case of Zambia. Hum Resour Health. 2020;18(1):25. PMID: 32216789; PMCID: PMC7098155. doi:10.1186/s12960-020-00467-x
14. Smith JD, Poenaru D, Thompson DR, Phillips JD. Surgical residency training in the mission setting: current status and future directions. Christian J Global Health. 2016;3:160. doi:10.15566/cjgh.v3i2.135
15. Lum SK, Crisostomo AC. A comparative study of surgical training in South East Asia, Australia and the United Kingdom. Asian J Surg. 2009;32(3):137–142. PMID: 19656752. doi:10.1016/S1015-9584(09)60384-5
16. Hatcher AM, Onah M, Kornik S, Peacocke J, Reid S. Placement, support, and retention of health professionals: national, cross-sectional findings from medical and dental community service officers in South Africa. Hum Resour Health. 2014;12:14. PMID: 24571826; PMCID: PMC3975958. doi:10.1186/1478-4491-12-14
17. Rourke JT, Incitti F, Rourke LL, Kennard M. Relationship between practice location of Ontario family physicians and their rural background or amount of rural medical education experience. Can J Rural Med. 2005;10(4):231–240. PMID: 16356384.
18. Long BA, Sweeney MJ. Examining the growing demand for surgical care in rural communities and novel approaches to achieving a sustainable surgical workforce: a narrative review. Cureus. 2023;15(8):e43817. PMID: 37736467; PMCID: PMC10511206. doi:10.7759/cureus.43817
19. Malloy SM, Sanchez K, Cho J, Mulcahy SE, Labow BI. Hidden costs in resident training: financial cohort analysis of first assistants in reduction mammaplasty. Plast Reconstr Surg Glob Open. 2021;9(1):e3333. PMID: 33564574; PMCID: PMC7859249. doi:10.1097/GOX.0000000000003333
20. Stefanidis D, Grewal H, Paige JT, et al. Establishing technical performance norms for general surgery residents. Surg Endosc. 2014;28(11):3179–3185. PMID: 24939154. doi:10.1007/s00464-014-3582-y
21. Colquhoun C, Hafeez MR, Heath K, Hays R. Aligning clinical resources to curriculum needs: the utility of a group of teaching hospitals. Med Teach. 2009;31(12):1081–1085. doi:10.3109/01421590903199692
22. Petrushnko W, Perry W, Fraser-Kirk G, Ctercteko G, Adusumilli S, O’Grady G. The impact of fellowships on surgical resident training in a multispecialty cohort in Australia and New Zealand. Surgery. 2015;158(6):1468–1474. PMID: 26297054. doi:10.1016/j.surg.2015.07.013
23. Bisgaard CH, Rodt SA, Musaeus P, Petersen JAK, Rubak SLM. Early procedural training increases anesthesiology residents’ clinical production: a comparative pre-post study of the payoff in clinical training. BMC Med Educ. 2021;21(1):262. PMID: 33957915; PMCID: PMC8103582. doi:10.1186/s12909-021-02693-w
24. Kraus CK, Greenberg MR, Ray DE, Dy SM. Palliative care education in emergency medicine residency training: a survey of program directors, associate program directors, and assistant program directors. J Pain Symptom Manage. 2016;51(5):898–906. PMID: 26988848. doi:10.1016/j.jpainsymman.2015.12.334
25. Mason BS, Ross W, Ortega G, Chambers MC, Parks ML. Can a strategic pipeline initiative increase the number of women and underrepresented minorities in orthopaedic surgery? Clin Orthop Relat Res. 2016;474(9):1979–1985. PMID: 27113596; PMCID: PMC4965371. doi:10.1007/s11999-016-4846-8
26. Weaver MD, Landrigan CP, Sullivan JP, et al. The association between resident physician work-hour regulations and physician safety and health. Am J Med. 2020;133(7):e343–e354. PMID: 32061733; PMCID: PMC7469904. doi:10.1016/j.amjmed.2019.12.053
27. Kamarajah SK, Alexander P; NIHR Global Health Research Unit on Global Surgery. Structures, processes and outcomes between first referral and referral hospitals in low-income and middle-income countries: a secondary preplanned analysis of the FALCON and ChEETAh randomised trials. BMJ Glob Health. 2024;9(Suppl 4):e015599. PMID: 39510564; PMCID: PMC11552540. doi:10.1136/bmjgh-2024-015599
28. Bust L, Chu K. Improving district hospital surgical capacity in resource limited settings: challenges and lessons from South Africa Comment on “Improving access to surgery through surgical team mentoring - policy lessons from group model building with local stakeholders in Malawi”. Int J Health Policy Manag. 2022;11(10):2361–2364. PMID: 35184510; PMCID: PMC9808279. doi:10.34172/ijhpm.2022.6937
29. Monteleone RA. Innovations in residency training in community hospitals. Delaware J Public Health. 2020;6(1):54–55. doi:10.32481/djph.2020.04.012
30. Thapa KR, Shrestha BK, Bhattarai MD. Study of working experience in remote rural areas after medical graduation. Kathmandu Univ Med J KUMJ. 2014;12(46):121–125. PMID: 25552217. doi:10.3126/kumj.v12i2.13658
31. Nielsen M, D’Agostino D, Gregory P. Addressing Rural Health Challenges Head On. Mo Med. 2017;114(5):363–366. PMID: 30228634; PMCID: PMC6140198.
32. Totten AM, Womack DM, Griffin JC, et al. Telehealth-guided provider-to-provider communication to improve rural health: a systematic review. J Telemed Telecare. 2024;30(8):1209–1229. PMID: 36567431; PMCID: PMC11389081. doi:10.1177/1357633X221139892
33. Diaz-Navarro C, Armstrong R, Charnetski M, et al. Global consensus statement on simulation-based practice in healthcare. Adv Simul. 2024;9(1):19. PMID: 38769577; PMCID: PMC11106913. doi:10.1186/s41077-024-00288-1
34. Syed-Abdul S, Scholl J, Jian WS, Li YC. Challenges and opportunities for the adoption of telemedicine in India. J Telemed Telecare. 2011;17(6):336–337. PMID: 21844182. doi:10.1258/jtt.2011.101210
35. Alam L, Khan J, Alam M, Faraid V, Ajmal F, Bahadur L. Residents’ perspective on the quality of postgraduate training programs in Pakistan - the good, the bad and the ugly. Pak J Med Sci. 2021;37(7):1819–1825. PMID: 34912401; PMCID: PMC8613050. doi:10.12669/pjms.37.7.4297
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.