Back to Journals » Clinical Ophthalmology » Volume 17
Analysis of Asphericity and Corneal Longitudinal Spherical Aberration of 915 Chinese Myopic Adult Eyes
Authors Zhang J ![]() , Zheng L, Zhang Y, Wang K
, Zheng L, Zhang Y, Wang K
Received 11 January 2023
Accepted for publication 9 February 2023
Published 15 February 2023 Volume 2023:17 Pages 591—600
DOI https://doi.org/10.2147/OPTH.S404437
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jun Zhang, Li Zheng, Yixuan Zhang, Ke Wang
Department of Ophthalmology, Hangzhou MSK Eye Hospital, Hangzhou, People’s Republic of China
Correspondence: Jun Zhang, Department of Ophthalmology, Hangzhou MSK Eye Hospital, Hangzhou, People’s Republic of China, Tel +86-18667046602 ; +86-0571 85064148, Email [email protected]
Purpose: To analyze the corneal asphericity, longitudinal spherical aberration (LSA), and related factors in Chinese myopic adult eyes.
Methods: This was a retrospective study of myopic adult patients. The corneal asphericity and LSA were measured at 3.0, 4.0, 5.0, 6.0, and 7.0 mm diameter apertures using corneal tomography. Age and refractive power were recorded for correlation analysis.
Results: In total, 531 females and 384 males were included. At the above five diameter settings the corneal asphericity values (Q) of the anterior surface were − 0.09± 0.21, − 0.14± 0.16, − 0.15± 0.13, − 0.17± 0.11, and − 0.20± 0.11, and those of the posterior surface were 0.23± 0.49, 0.06± 0.29, − 0.01± 0.22, − 0.07± 0.16, and − 0.08± 0.15, respectively. The anterior corneal LSA values at these diameters were 0.39± 0.19, 0.63± 0.27, 0.97± 0.36, 0.90± 0.30, and 0.83± 0.29 D, respectively and the whole corneal values were 0.26± 0.20, 0.44± 0.27, 0.70± 0.36, 0.66± 0.30, and 0.59± 0.28 D, respectively. Corneal asphericity and peripheral LSA showed no or weak correlation with age or spherical equivalent (all r < 0.2).
Conclusion: Corneal anterior and posterior Q values in myopia patients are negatively correlated with corneal diameter. Corneal anterior and whole corneal LSA increased significantly with diameter up to 5 mm, then decreased slightly with diameter. Corneal asphericity and peripheral LSA showed very weak or no correlation with age or spherical equivalent.
Clinical Trial Registration Number: ChiCTR1800015985.
Keywords: wavefront aberration, asphericity, longitudinal spherical aberration, myopia
Introduction
In human eyes, the aspherical shape of the cornea and crystalline lens work together to optimize focus on the macula. Due to refractive index differences between the cornea and its surrounding refractive media, slight changes in corneal asphericity can modulate the focus of peripheral light significantly, while having little effect on focus of paraxial light. Changes in the spread of focal points may optimize visual quality or depth of field according to clinical needs.1–3 The Q value is a quantitative indicator of asphericity and is defined as the radius of curvature change from the apex to the periphery.4,5 Spherical-like aberration, which belongs to the category of transverse aberration, refers to the root mean square (RMS) of the zero-frequency Zernike coefficients above fourth-order.6 Longitudinal spherical aberration (LSA), which belongs to the category of longitudinal aberration, is a result of peripheral light rays being refracted more or less than those close to the axis, and may be measured as the difference between the points at which peripheral and more axial rays intersect with the axis, in diopter.4 Therefore, when the corneal Q value changes, the corneal spherical-like aberration and LSA will change accordingly, and the Q value can be used to modulate spherical-like aberration or LSA. Although both spherical-like aberration and LSA are characterized by the refraction of peripheral rays.1,7 LSA, the focal distance on the optical axis, is more closely associated with refractive error and may have implications for corneal refractive surgery strategies in presbyopia. In addition, few studies have been conducted on corneal LSA.
Presently, spherical-like aberration but no LSA can be obtained directly using standard ophthalmic equipment. The results of relevant studies between spherical-like aberrations with multifactor appear contradictory.8–10 With increasing attention on corneal refractive surgery for presbyopia, the potential for LSA-based estimation of near refractive error has attracted interest. For example, 1.00 D LSA allows peripheral light to provide 1.00 D near addition, while a similar effect can be achieved by 0.12 μm spherical-like aberration, but seems harder to understand. The main objective of the present study was to determine amplitude and range of corneal LSA in the Chinese myopic population, as a step toward a more accurate model of the Chinese eye.
Materials and Methods
Study Design and Patients
This was a retrospective study of patients planning to undergo therapeutic refractive surgery at Hangzhou MSK Eye Hospital between October 2018 and December 2018. The study was approved by the institutional review board at each participating site and by the ethics committee of Hangzhou MSK Eye Hospital. Since the data are anonymous, were stored confidentially and the study was compliant with the Declaration of Helsinki, the requirement for informed consent was waived.
The inclusion criteria were: (1) diagnosis of myopia; and (2) 18–40 years of age. Those with any history of ocular surgery (such as corneal refractive surgery, corneal traumatic repair, corneal transplantation, anterior chamber puncture, iris repair, and others), history of contact lens use within six months, or using any ocular medication were excluded from the study.
Ophthalmic Examination
Data from detailed ophthalmic assessments were extracted from the medical charts. These examinations were carried out before corneal refractive surgery and included a complete medical and ophthalmic history and a thorough ocular examination, including measurements of uncorrected visual acuity, refractive error (in diopters), best corrected visual acuity (BCVA), cycloplegic refraction, slit-lamp examination (to assess corneal status, any scarring, history of corneal transplantation, anterior chamber puncture, iris repair), axial length, gonioscopy (to look for peripheral retinal tears), fundoscopy (central retinal examination to screen for fundus diseases such as macular diseases and vasculopathy), and intraocular pressure. In addition, corneal topography, including parameters such as corneal central thickness (CCT) and Sim-K of anterior and posterior corneal surface, was conducted using a tomography system (CSO, Sirius, Florence, Italy). Spherical equivalent (SE) was obtained as spherical refractive error + 1/2 cylindrical refractive error based on manifest refraction.
Measurement of Vertex Curvature and the Q Value of Anterior and Posterior Corneal Surfaces
In the corneal tangential curvature map, the origin of the coordinate system is the corneal vertex curvature. The Q values of the anterior and posterior corneal surface at 3.0, 4.0, 5.0, 6.0, and 7.0 mm aperture diameters were obtained using tomography. All measurements were performed three times, and the mean was used for statistical analysis.
Calculation of LSA of the Anterior Corneal Surface and Whole Cornea
The LSAs of the anterior corneal surface and the whole cornea were calculated at 3.0, 4.0, 5.0, 6.0, and 7.0 mm aperture diameters.7 For the convenience of data collation, the LSA calculation process can be transformed as follows.
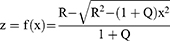
Corneal asphericity was calculated as follows11

Where x and y are the radii from the corneal apex, z is the distance from cornea to the XY plane, R is the radius of the curvature at corneal apex, and Q is the asphericity of the cornea.
A cross section of the corneal surface in the XOZ plane is shown in Figure 1. A single meridian on the corneal surface can be expressed as part of a conic curve.
 |
Figure 1 Corneal surface coordinate system. For a point moving along the curve, |


Because the corneal surface is only the front part of the quadric surface, the quadratic equation may be expressed as
Figures 2 and 3 show schematic diagrams of reflection by the anterior and posterior corneal surfaces.
 |
Figure 2 Refractive trajectory of light passing through the anterior surface of the cornea. The angle of motion α is also the angle of incidence, θ the angle of reflection; and n1 and n2 are the refractive indices of air and cornea respectively. |
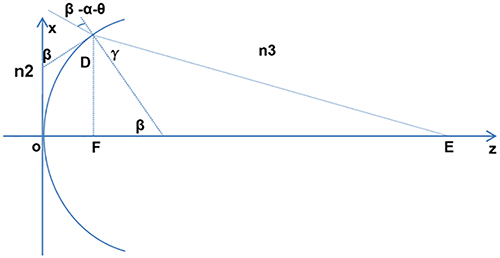 |
Figure 3 Refractive trajectory of light passing through the posterior surface of the cornea. β is the angle of motion; γ the angle of reflection; and n2 and n3 are the refractive indices of the cornea and aqueous humor, respectively. |
By calculating the first and second derivative of z to x, the angle of motion α, angle of motion β (posterior surface), speed v, and the acceleration in the direction of the z axis at the edge of the optical zone can be obtained.


According to the formula of centripetal acceleration in circular motion, the radius r of curvature at the edge of the optical zone can be obtained.

According to Figure 2, the LSA of the anterior corneal surface of the target optical zone can be calculated.

According to Figure 3, the LSA of the whole cornea at the target optical zone can be calculated.

Statistical Analysis
Continuous variables are expressed as means ± standard deviation (SD). Correlations between parameters were examined using the Pearson correlation. All statistical analyses were performed using SPSS 19.0 (IBM, SPSS, Armonk, NY, USA). Two-sided P values <0.05 were considered statistically significant.
Results
Characteristics of the Patients
This study included 915 eyes from 915 myopic patients, including 531 females with a mean age of 28.3±6.8 years and 384 males with a mean age of 24.1±6.9 years. In the total cohort, SE ranged from −13.00 to −0.50 D (mean: −6.5±2.2 D). The mean CCT and Sim-K of the anterior and posterior corneal surfaces were 536.0±91.2 μm, 43.0±1.4 D, and −6.0±0.2 D, respectively (Table 1). Slit-lamp examination, gonioscopy, and fundoscopy showed no significant lesions in these patients.
 |
Table 1 Characteristics of the Patients |
Corneal Q Values
The anterior surface corneal Q values were −0.09±0.21, −0.14±0.16, −0.15±0.13, −0.17±0.11, and −0.20±0.11 at 3.0, 4.0, 5.0, 6.0, and 7.0 mm diameters, respectively; those of the posterior surface were 0.23±0.49, 0.06±0.29, −0.01±0.22, −0.07±0.16, and −0.08±0.15, respectively. The distribution of corneal Q value at these aperture diameters is shown in Figure 4.
 |
Figure 4 Distribution of corneal Q value at 3.0, 4.0, 5.0, 6.0, and 7.0 mm aperture diameters, anteriorly and posteriorly, in 915 individuals. The corneal Q values of the anterior surface were: −0.09±0.21, −0.14±0.16, −0.15±0.13, −0.17±0.11, and −0.20±0.11, respectively, and those of posterior surface were 0.23±0.49, 0.06±0.29, −0.01±0.22, −0.07±0.16, and −0.08±0.15, respectively. |
Corneal LSA Values
The corneal LSA values of the anterior surface at these diameters were 0.39±0.19 D, 0.63±0.27 D, 0.97±0.36 D, 0.90±0.30 D, and 0.83±0.29 D, respectively; values for the whole cornea were 0.26±0.20 D, 0.44±0.27 D, 0.70±0.36 D, 0.66±0.30 D, and 0.59±0.28 D, respectively. Therefore, the corneal LSA values of the posterior surface were: −0.13±0.07 D, −0.19±0.09 D, −0.27±0.12 D, −0.24±0.10 D, and −0.24±0.09 D, respectively. The distribution of corneal LSA values at the range of aperture diameters is shown in Figure 5.
 |
Figure 5 Distribution of corneal longitudinal spherical aberration (LSA) values at 3.0, 4.0, 5.0, 6.0, and 7.0 mm aperture diameters, anteriorly and wholly, in 915 individuals. The corneal LSA values of the anterior surface were: 0.39±0.19 D, 0.63±0.27 D, 0.97±0.36 D, 0.90±0.30 D, and 0.83±0.29 D, respectively, and the mean whole corneal LSA values were 0.26±0.20 D, 0.44±0.27 D, 0.70±0.36 D, 0.66±0.30 D, and 0.59±0.28 D respectively. |
Correlations
Both corneal Q values and LSA at each of the aperture diameters showed very weak or no correlation with age and spherical equivalent (all r < 0.2) (Table 2).
 |
Table 2 Results of Correlation Analyses |
Discussion
Understanding of the human ocular refractive system is constantly improving with the rapid development of physical optics. In particular, higher order aberration (HOA) has enhanced the study of visual quality12–14 and has become an important index in research on refractive surgery. Spherical-like aberration or LSA is a higher order aberration with significant impact on visual quality.15 Previous studies have focused on its elimination16–18 or reduction to a level sufficient to meet clinical needs. However, as mentioned above, LSA has unique advantages. Understanding the distribution of corneal LSA in myopia may help to more accurately model the Chinese eye and provide guidance for custom corneal ablation treatment. In the case of extended focus presbyopia correction, LSA may enhance estimation of the near correction, a strategy which has attracted increasing attention.19–21 In addition, it is known that matching corneal asphericity with optical elements helps to establish an aberration balance or reduce spherical-like aberration,22,23 demonstrating that corneal asphericity Q value plays an important role in visual function.24 Therefore, the aim of this study was to report the distribution of corneal Q-value and LSA in patients with myopia.
We investigated the distribution of Q values in multiple regions on the myopic cornea, and the results are supported by previous studies. While those studies report different Q values (for example −0.08 for Horner,25 −0.20 for Fuller,2 −0.22 for Cheung14 and Scholz,26 −0.24 for Dubbelman,27 −0.30 for Zhang,1 −0.33 for Carney,24 and −0.35 for Davis)28 all are in the lower negative range, indicating that the corneal profile is prolate. Furthermore, we found that both anterior and posterior corneal Q values decreased with increasing diameter. From the apex of the cornea to the periphery of the cornea, the profile of the anterior corneal surface changes from spherical to prolate and the posterior surface from oblate to prolate. We also investigated the distribution of LSA at multiple corneal regions in myopia. Both corneal anterior and whole corneal LSA increased significantly up to 5 mm diameter, but beyond 5 mm they decreased slightly with increasing diameter. This may be related to eyelid compression and is not consistent with the previous assumption that all HOAs increases significantly with diameter. Both corneal Q values and LSA at all apertures showed very weak or no correlation with age or spherical equivalent. Similar conclusions were obtained by Fuller,2 Zhang,1 and Llorente.29
The present study has limitations. First, this was a single-center study with a relatively small sample size. Second, only myopic patients were included.
Conclusions
To summarize, the anterior and posterior corneal surface Q values in myopic patients were similar to those of previous studies, with Q values decreasing as diameter increased. From corneal apex to periphery, the profile of the anterior corneal surface changes from spherical to prolate, and that of the posterior surface changes from oblate to prolate. Both corneal anterior and whole corneal LSA increased significantly at diameters up to 5 mm, while beyond 5 mm both anterior and whole corneal LSA decreased slightly with diameter. Both corneal asphericity and LSA showed very weak or no correlation with age or spherical equivalent. These results may provide a useful reference for designing aspheric keratorefractive surgery, visual optical products, and future study of the optical properties of the human eye.
Abbreviations
LSA, longitudinal spherical aberration; ZZ IOL, Zhang & Zheng IOL; RMS, root mean square; BCVA, best corrected visual acuity; CCT, corneal central thickness; SE, spherical equivalent; HOA, higher order aberration.
Ethics Approval and Informed Consent
The study was approved by the institutional review board at each participating site and by the ethics committee of Hangzhou MSK Eye Hospital. The data are anonymous, confidential and the study was in compliance with the Declaration of Helsinki, so the requirement for informed consent was waived.
Acknowledgments
This work was supported by the Zhejiang Province Medical and Health Science and Technology Project (2018267858).
Disclosure
All authors declare that they have no conflicts of interest in this work.
References
1. Zhang Z, Wang J, Niu W, et al. Corneal asphericity and its related factors in 1052 Chinese subjects. Optomet Vision Sci. 2011;88(10):1232–1239. doi:10.1097/OPX.0b013e31822717ca
2. Fuller DG, Alperin D. Variations in corneal asphericity (Q Value) between African-Americans and whites. Optomet Vision Sci. 2013;90(7):667–673. doi:10.1097/OPX.0b013e318296befe
3. Zhang J, Zheng L, Zhao X, Sun Y, Feng W, Yuan M. Corneal aberrations after small-incision lenticule extraction versus Q value-guided laser-assisted in situ keratomileusis. Medicine. 2019;98(5):e14210–e. doi:10.1097/MD.0000000000014210
4. Calossi A. Corneal asphericity and spherical aberration. J Refract Surg. 2007;23(5):505–514. doi:10.3928/1081-597X-20070501-15
5. Hashemi H, Nabovati P, Aghamirsalim M, Mahboubipour H, Yekta A, Khabazkhoob M. Corneal asphericity and related factors in the geriatric population: a population‐based study. Ophthal Physiol Opt. 2021;41(4):691–701. doi:10.1111/opo.12831
6. Kiuchi G, Hiraoka T, Ueno Y, Mihashi T, Oshika T. Influence of refractive status and age on corneal higher-order aberration. Vision Res. 2021;181:32–37. doi:10.1016/j.visres.2020.12.007
7. El‐Nashar NF. Longitudinal spherical aberration and mass of bi‐aspheric aphakic rigid contact lenses. Ophthal Physiol Opt. 1999;19(5):441–445. doi:10.1046/j.1475-1313.1999.00467.x
8. Fernández J, Rodríguez-Vallejo M, Burguera N, Rocha-de-Lossada C, Piñero DP. Spherical aberration for expanding depth of focus. J Cataract Refract Surg. 2021;47(12):1587–1595. doi:10.1097/j.jcrs.0000000000000713
9. Du W, Lou W, Wu Q. Personalized aspheric intraocular lens implantation based on corneal spherical aberration: a review. Int J Ophthalmol. 2019;12(11):1788–1792. doi:10.18240/ijo.2019.11.19
10. Batres L, Peruzzo S, Serramito M, Carracedo G. Accommodation response and spherical aberration during orthokeratology. Graefes Archiv Clin Exp Ophthalmol. 2019;258(1):117–127. doi:10.1007/s00417-019-04504-x
11. Cheung SW, Cho P, Douthwaite W. Corneal shape of Hong Kong-Chinese. Ophthal Physiol Opt. 2000;20(2):119–125. doi:10.1046/j.1475-1313.2000.00488.x
12. Feng Z, Wang Q, Du C, Yang F, Li X. High-order aberration changes after femtosecond LASIK surgery in patients with high myopia. Ann Palliat Med. 2021;10(7):7689–7696. doi:10.21037/apm-21-1677
13. Zeng J, Lan G, Zhu M, et al. Factors associated with corneal high-order aberrations before and after femtosecond laser-assisted in situ keratomileusis. Ann Transl Med. 2021;9(12):989. doi:10.21037/atm-21-2367
14. Martins C, Amorim-De-Sousa A, Faria-Ribeiro M, Pauné J, González-Méijome JM, Queirós A. Visual performance and high-order aberrations with different contact lens prototypes with potential for myopia control. Curr Eye Res. 2019;45(1):24–30. doi:10.1080/02713683.2019.1645182
15. Kemraz D, Cheng X-Y, Shao X, et al. Age-related changes in corneal spherical aberration. J Refract Surg. 2018;34(11):760–767. doi:10.3928/1081597X-20181011-01
16. Faramarzi A, Moshirfar M, Karimian F, Delfazayebaher S, Kheiri B. Aspheric versus wavefront-guided aspheric photorefractive keratectomy in eyes with significant astigmatism. J Cataract Refract Surg. 2017;43(12):1534–1540. doi:10.1016/j.jcrs.2017.09.022
17. El-Mayah E, Anis M, Salem M, Pinero D, Hosny M. Comparison between Q-adjusted LASIK and small-incision lenticule extraction for correction of myopia and myopic astigmatism. Eye Contact Lens. 2018;44(2):S426–S32. doi:10.1097/ICL.0000000000000532
18. Manns F, Ho A, Parel J-M, Culbertson W. Ablation profiles for wavefront-guided correction of myopia and primary spherical aberration. J Cataract Refract Surg. 2002;28(5):766–774. doi:10.1016/S0886-3350(01)01322-0
19. Cantú R, Rosales MA, Tepichín E, Curioca A, Montes V, Ramirez-Zavaleta JG. Objective quality of vision in presbyopic and non-presbyopic patients after pseudoaccommodative advanced surface ablation. J Refract Surg. 2005;21(5). doi:10.3928/1081-597X-20050902-08
20. Koller T, Seiler T. Four corneal presbyopia corrections: simulations of optical consequences on retinal image quality. J Cataract Refract Surg. 2006;32(12):2118–2123. doi:10.1016/j.jcrs.2006.08.038
21. Alió JL, Amparo F, Ortiz D, Moreno L. Corneal multifocality with excimer laser for presbyopia correction. Curr Opin Ophthalmol. 2009;20(4):264–271. doi:10.1097/ICU.0b013e32832a7ded
22. Mrochen M, Donitzky C, Wüllner C, Löffler J. Wavefront-optimized ablation profiles. J Cataract Refract Surg. 2004;30(4):775–785. doi:10.1016/j.jcrs.2004.01.026
23. Ang R. What is the relevance of asphericity in today’s ophthalmic practice? Philipp J Ophthalmol. 2011;36(5–6):54.
24. Carney LG, Mainstone JC, Henderson BA. Corneal topography and myopia: a cross-sectional study. Invest Ophthalmol Vis Sci. 1997;38(2):311–320.
25. Horner DG, Soni PS, Vyas N, Himebaugh NL. Longitudinal changes in corneal asphericity in myopia. Optomet Vision Sci. 2000;77(4):198–203. doi:10.1097/00006324-200004000-00012
26. Scholz K, Messner A, Eppig T, Bruenner H, Langenbucher A. Topography-based assessment of anterior corneal curvature and asphericity as a function of age, sex, and refractive status. J Cataract Refract Surg. 2009;35(6):1046–1054. doi:10.1016/j.jcrs.2009.01.019
27. Dubbelman M, Sicam VA, Van der Heijde GL. The shape of the anterior and posterior surface of the aging human cornea. Vision Res. 2006;46(6–7):993–1001. doi:10.1016/j.visres.2005.09.021
28. Davis WR, Raasch TW, Mitchell GL, Mutti DO, Zadnik K. Corneal asphericity and apical curvature in children: a cross-sectional and longitudinal evaluation. Investig Ophthalmol Vis Sci. 2005;46(6):1899. doi:10.1167/iovs.04-0558
29. Llorente L, Barbero S, Cano D, Dorronsoro C, Marcos S. Myopic versus hyperopic eyes: axial length, corneal shape and optical aberrations. J Vis. 2004;4(4):5. doi:10.1167/4.4.5
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.