")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Analysis of Adverse Reactions of Cosmetics in Chinese Han Population in Recent Five Years
Authors Dong C, Liu F, Liao Z, Lin L, Wang R, Du J, Huang W
Received 18 May 2023
Accepted for publication 25 August 2023
Published 5 September 2023 Volume 2023:16 Pages 2419—2428
DOI https://doi.org/10.2147/CCID.S418591
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Video abstract presented by Wen Huang.
Views: 83
Canbin Dong,1,* Fang Liu,1,* Zuda Liao,2 Lanmei Lin,1 Runnan Wang,1 Juan Du,1 Wen Huang1
1Department of Dermatology, Huashan Hospital, Fudan University, Shanghai Institute of Dermatology, Shanghai, People’s Republic of China; 2Medical Insurance Office of Huashan Hospital Affiliated, Fudan University, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Juan Du; Wen Huang, Department of Dermatology, Huashan Hospital, Fudan University, Shanghai Institute of Dermatology, Shanghai, 200040, People’s Republic of China, Tel +86-21-52889999, Fax +86-21-52887782, Email [email protected]; [email protected]
Background: There are still some gaps in the summary and generalization of cosmetic-related adverse reaction reports.
Objective: The aim of this study is to summarize and analyze the occurrence of cosmetic adverse reactions in Shanghai Han population by using available survey data.
Materials and Methods: Collection, statistics and analysis of patients with cosmetic adverse reactions in Shanghai Huashan Hospital from 2017 to 2021.
Results: Among the 1004 patients, most of them (96.71%) were diagnosed as cosmetic contact dermatitis, which often occurred within 3 days of using cosmetics (51.79%). A total of 260 patients were tested with patch test, but the compliance rate was only 18.08%. Among them, 240 patients underwent additional European standard allergen tests, and positive allergens were detected in 210 cases (87.5%). Univariate analysis revealed that dosage form (emulsion and cream), age (≤ 25 years) and the allergic ingredients triethanolamine, rose oil, propylene glycol, thiomersal and musk ambrette are associated with the occurrence of cosmetic adverse reactions within seven days. A logit prediction model was also successfully constructed: Logit (P) = 1.710– 0.796× 1 + 1.185× 2 − 3.650X3-1.335X4.
Conclusion: This study complements the data reported on cosmetic adverse reactions in the Chinese Han population and suggests that in future clinical diagnosis and data collection, emphasis should be placed on patch testing, combining the patch test with cosmetic protoplast with the European standard allergen test to improve the detection rate.
Keywords: adverse reaction reporting, cosmetics, contact dermatitis, personal care products, patch tests
Introduction
Unlike the general population’s perception of cosmetics, the medical definition of “cosmetics” is any product that cleanses and beautifies the exterior of the body (hair, nails, skin, etc.).1–3 In this study, we used the US Food and Drug Administration (FDA)2 definition of cosmetic products, including skin care products, sunscreens, hair dyes, hair removal creams, etc.
With the increasing demand for cosmetics and the increasing variety of cosmetic products,4 adverse reactions caused by cosmetics are gaining more and more attention. Several studies have shown that the chemicals contained in some cosmetics and some naturally occurring toxic ingredients, such as snake venom, may pose a threat to the health of people with allergies.5–10 Some cosmetic products would interact with the skin microbiota and cause certain degree of disruption of the skin barrier.11 Mild symptoms include only mild allergic reactions, such as local itching and erythema, etc, while severe cases may even have physical symptoms such as headache and nausea.3,12,13
With the increasing frequency of cosmetic adverse reactions, more attention has been paid to the identification and monitoring of adverse cosmetic reactions.14 One of the most commonly used diagnostic methods is the patch test.15–17 The patch test is commonly used to evaluate allergic contact dermatitis. By making a reagent of the possible allergens and applying it to the skin, it is not only effective in assessing the severity of the allergic reaction, but also in helping the patient to detect the allergen.
The monitoring system for cosmetic adverse reactions is being gradually improved as the standard of living of the Chinese people continues to improve and the use of cosmetics becomes more widespread.14 The purpose of this study is to analyze the epidemiological characteristics of 1004 cases diagnosed and recorded in Huashan Hospital due to adverse reactions of cosmetics in the past five years (2017–2021), as well as the results of 260 patch test with cosmetic protoplasts and European allergen tests. The patch test, the European standardized allergen assay and related statistical methods follow international recommendations.18–20
Materials and Methods
Study Population
Data collection began in January 2017 and ended in December 2021. 1004 patients were those who went to Huashan Hospital of Fudan University in Shanghai for treatment due to adverse cosmetic reactions during the period, and were recorded at the permission of the patients.
Allocation of Cosmetic Allergens
In this study, cosmetic allergens were classified into two main groups: general and specific. The general category was subdivided into three groups: hair, skin care and cosmetic modifications (Supplementary Table 2). Classification is based on China’s New Cosmetics Regulation (CSAR) (intertek.com).
Interpretation of Patch-Test Reactions
Patch test with cosmetic protoplast to make the cosmetics suspected of sensitization into reagents, paste them on the skin for 48 hours, and then take them out to observe the reaction of patients for 48 hours and 72 hours respectively. The results and significance are as follows: negative reaction (no reaction), suspicious reaction (pale erythema), positive reaction (mild erythema and papules), strong positive reaction (edematous erythema and papules), and ultra-strong positive reaction (significant erythema, blisters, or maculopapular).19
The European standard allergen patch test (EUROIMMUN) follows the same procedure as the patch test, with the patch also being removed at 48 hours and the skin reaction evaluated at 48 and 72 hours, respectively. A total of 48 allergens are included in the European standard allergen test (Supplementary Table 1).
Photo-patch test were performed by applying the suspected photosensitizer to the patient’s back in three simultaneous patch tests, measuring the minimum erythema (MED) on the forearm or abdomen, and removing the three patch tests 24 hours later, with the first removed and protected from light, the second irradiated with UVB below the MED, and the third irradiated with UVA for 20 to 30 times the MED. The results were evaluated in the same way as the patch test with cosmetic protoplast.
Statistical Analysis
The analysis is presented below. Continuous variables are represented by mean ± standard deviation (SD), and categorical variables are represented by frequency (%). Continuous variables were compared using t-test and Wilcoxon rank sum test; categorical variables were compared using Pearson chi-square test. Logistic regression models were used to detect the relationship between allergens and the two groups (≤7 days group and >7 days group). The area under the curve (AUC) was used to evaluate the predictive power of the forecasting model and the Hosmer-Lemeshow (HL) test was used to estimate the goodness-of-fit of the logistic regression model. Bilateral P < 0.05 was considered a statistically significant difference. Statistical analysis and graph production were performed using SPSS software (version 22).
Results
Characteristics of the Study Participants
As shown in Table 1, a total of 1004 patients were included in this study, of which 49 were males (4.88%) and 955 were females (95.12%). The age distribution was unknown in 52 of the 1004 patients. Of the remaining 952 patients, the mean age was 34.66 years, the median age was 33 years, the youngest age was only 11 years. The largest number of patients, approximately 70%, were between 19 and 40 years of age. The 25th and 75th percentiles were 26 and 41 years, respectively.
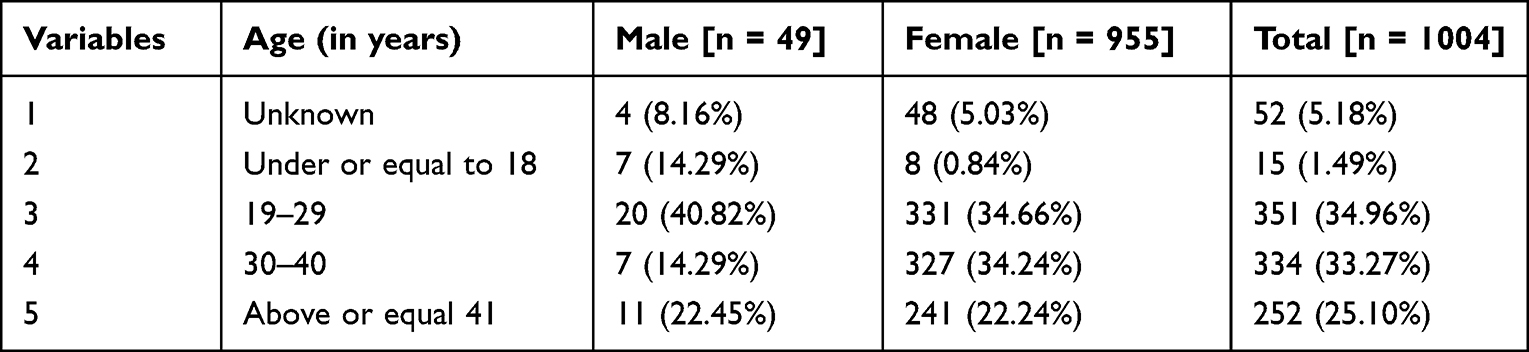 |
Table 1 Population Distribution |
Cosmetic Categories and Sources
Among the classification of cosmetic products, the most cases were caused by the common category of cosmetics, with 927 cases (92.33%) and only 77 cases (7.67%) in the special category of cosmetics. Among them, the highest percentage of the common cosmetics category was skin care, with 819 cases, accounting for more than 80% of all cases, with cosmetic water (150 cases, 14.94%), masks (161 cases, 16.04%), cosmetic lotion (239 cases, 23.80%) and cosmetic cream (231 cases, 23.00%) being the most common.
Over half of the cosmetics were sourced from online purchases (520 cases, 51.79%), and shopping malls (259 cases, 25.80%) and beauty salons (78 cases, 7.77%) were also common purchase channels, which are shown in Table 2.
 |
Table 2 Product Sources |
Preliminary Diagnosis
Cosmetic contact dermatitis was the most common diagnosis, with 971 cases (96.71%) diagnosed in this study, while other diagnoses included cosmetic skin pigmentation abnormalities (1.39%) and cosmetic photosensitive dermatitis (0.90%). The other detailed diagnoses are shown in Figure 1. Of these, acne specifically refers to acne-like rashes on the face caused by cosmetics. Lipitis is contact lipitis, which specifically refers to allergic reactions on the lips caused by cosmetics.
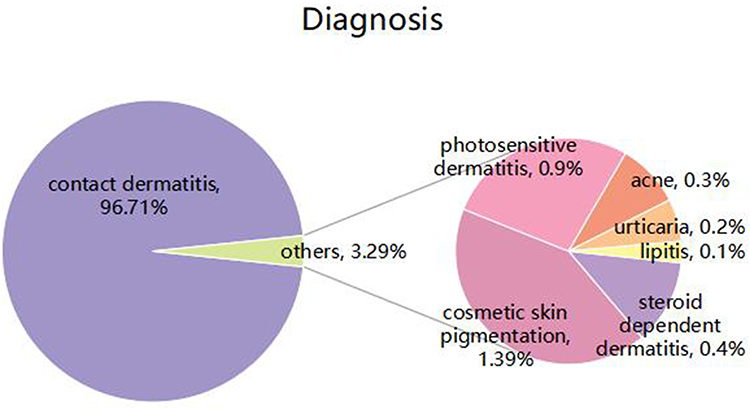 |
Figure 1 Demonstration of the results of the preliminary diagnosis through pie charts. |
Onset Time
As in Table 3, more than a quarter of the patients (25.70%) developed the disease within one day after using cosmetics, and more than half of the patients (51.79%) developed the disease within three days. More than eighty percent (80.28%) of all cases developed within two weeks of application of cosmetics.
 |
Table 3 Onset Time |
Lesion Site, Conscious Symptoms, Lesion Pattern
The lesions occurred almost exclusively on the face (99.30%), with other sites such as the neck (1.99%), scalp (0.60%), and the external auricle (0.30%) also having a few sites. Other rare sites of lesions are shown in Figure 2A.
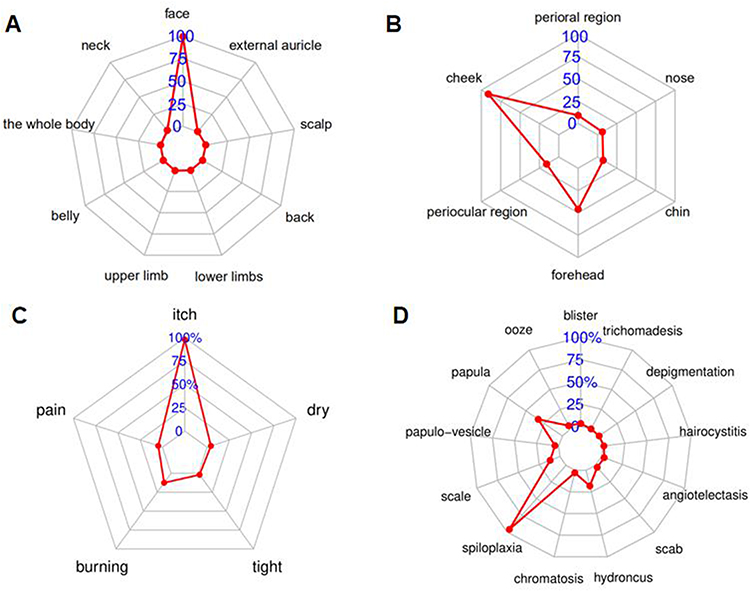 |
Figure 2 Lesion site, conscious symptoms, lesion pattern. (A) Demonstration of body sites of disease by radar diagram (B) Demonstration of facial onset by radar diagram (C) Demonstrating symptoms of consciousness through radar diagram (D) Demonstration of lesion type by radar diagram. |
In the face, the most predominant occurrence was on the cheek (91.04%), and lesions were also found on the forehead in nearly half of the cases (46.02%), while other common lesion sites were around the periocular region (15.74%), perioral region (9.06%), chin (7.37%), and nose (6.27%). The respective percentages are shown in Figure 2B.
Almost all patients suffer from itching as a conscious symptom (98.01%) and about one in eight patients also experience a burning sensation (12.45%). This is followed by symptoms of pain, tightness, and dryness (Figure 2C).
In Figure 2D, a variety of lesion patterns were observed, 95.92% of the patients would have erythema. Papules and edema were also relatively common lesion patterns (33.07% and 18.03%, respectively).
It is not uncommon for a patient to have multiple lesions with multiple sites at the same time, or to have multiple spontaneous symptoms with multiple lesion patterns. A total of 507 patients had more than 2 lesion sites, accounting for 50.50% of the cases. There were 176 cases (17.53%) with multiple self-perceived symptoms, and 56.37% of patients had multiple lesion patterns (566 cases).
Patch Test with Cosmetic Protoplast, European Standard Allergen Series, Photo-Patch Test
A total of 260 patients underwent patch testing for cosmetic allergens, of which 47 had positive results associated with adverse reactions, a compliance rate of 18.08%. Of these 260 patients, 240 underwent additional patch testing for European standard allergens, of which 210 were detected, with a positivity rate of 87.5%.
Including the 240 patients noted above, a total of 266 of the 1004 patients in this study underwent patch testing for European standard allergens, and 218 patients had allergens detected, a detection rate of 81.95%. The most common allergen/irritant was sodium dodecyl sulfate (107 cases, 49.08%), followed by Thiomersal (85 cases, 38.99%).
There were also 88 patients who underwent the photo-patch test in all cases, of which 17 were positive, with a positivity rate of 19.32%.
Correlation Analysis of the Time of Onset of Cosmetic Adverse Reactions
To explore the potential factors associated with the time to onset of allergic reactions to cosmetics. We screened 218 patients who were able to check for allergic components. As shown in Supplementary Table 3, dosage form (emulsion and cream), triethanolamine, rose oil, and propylene glycol were negatively associated with the presence of allergic reactions within 7 days (r < 0, P < 0.05), and age (≤ 25 y), thiomersal, and musk ambrette were positively associated (r > 0, P < 0.05). While bronopol, sodium dodecyl sulfate, vanillin, triclosan, and salicylic acid did not seem to be associated.
To further explore independent factors associated with time to onset, indicators that were statistically significant (p < 0.05) in the univariate analysis such as dosage form (emulsion and cream), thiomersal, propylene glycol, and triethanolamine were included in the regression analysis model. As shown in Table 4, based on the independent predictors determined by unconditional logistic regression, we developed the logit model as follows: Logit (P) = 1.710–0.796×1 + 1.185×2 −3.650X3-1.335X4, where X1 is represented as the dosage form (emulsion and cream), X2 is thiomersal, X3 is propylene glycol and X4 is triethanolamine. To estimate the goodness of fit of the logistic regression model, a Hosmer-Lemeshow (HL) test was performed. The HL test showed that the model fitted well with an HL statistic = 4.978 (p= 0.419). Therefore, the risk of onset within seven days score was calculated for the entire study group using the model and plotted on a ROC curve.
 |
Table 4 Independent Factors |
The ROC curve using the model to predict onset within seven days are shown in Figure 3. The area under the receiver operating characteristic curve were 0.743 (95% CI 0.673–0.813). Based on the ROC curve, the optimal cut-off point for predicting the risk score for onset within seven days of the event is 0.836 (sensitivity 53.9%, specificity 81.1%).
 |
Figure 3 Use the ROC curve to evaluate the performance of the model. |
Discussion
As the construction of China’s cosmetic adverse reaction monitoring system becomes more and more well established, we recorded and analyzed 1004 patients who went to Huashan Hospital for cosmetic adverse reactions during a total of five years from 2017 to 2021, using the method of hospital targeted monitoring and recording. Due to the different definitions of the term “cosmetic”, and in order to be as comparable as possible to previous studies, we have adopted a broader definition in medicine, ie all skin care and beauty products are defined as cosmetics.
Among the participants in our study, the 19- to 29-year-olds made up the highest percentage, about 35%, followed by the 30- to 40-year-olds, about one-third. This data is consistent with previous studies.13,21,22 This age group is more conscious of self-care as well as beautification and uses cosmetics significantly more frequently than other age groups. More than 90% of the population of patients attending the clinic were women, probably due to the fact that women use cosmetics much more frequently than men, in line with the pattern shown in previous studies.21,22
In this study, online shopping was the most predominant source of cosmetic purchases, accounting for more than half of all sources, which may be related to the rise of online shopping in recent years and people’s increased trust in online shopping.
Consistent with previous studies, skin care cosmetics have the highest correlation with the occurrence of contact dermatitis. There is literature demonstrating that many skin care products incorporate a variety of chemical additives in order to increase their effectiveness, and these chemical additives are often the main culprit of contact dermatitis,1,6 and there have even been reports of products such as soap causing aberrant respiratory distress syndrome.17 Additionally, daily skin care products are used more frequently in life and may be the reason why skin care products account for the highest percentage of adverse cosmetic reactions.
Cosmetics may cause a wide range of adverse reactions, such as pigmentation disorders, acne, and urticaria,1 and may even lead to endocrine disruption.6 Of these 1004 cases we recorded, almost all of them occurred as cosmetic contact dermatitis, 971 cases (96.71%). More than half of the patients self-reported onset within three days of cosmetic use, but the accuracy of this data may be diminished due to recall bias. Itching, followed by pain and tightness are the main symptoms. Most of the sites of onset are on the face, consistent with the site of contact with the skin care products used. The above data are consistent with the clinical features of cosmetic contact dermatitis.1,21,23
Allergic patch test for suspected cosmetics was performed in 260 patients out of the total number of cases, but the compliance rate was only 18%. This reflects the necessity of adding the European standard series of allergy tests, which is also mentioned in the guidelines related to patch testing.20 Cosmetic contact dermatitis can be classified as cosmetic irritant contact dermatitis and cosmetic allergic contact dermatitis depending on the pathogenesis.13 In this clinical test, we did not enforce a distinction between irritant and allergic reactions. If the patch test with cosmetic protoplast shows a positive result and the patient’s history and clinical presentation are consistent, we consider a correlation between the adverse reaction and the cosmetic product. However, the compliance rate of the original object patch test was relatively low. Possible reasons are as follows: First, most patients often have acute contact dermatitis, with severe symptoms such as itching and pain, and some of them may have taken oral antihistamines before the tests to relieve symptoms, which may interfere with the accuracy of the patch test; Second, some patients use a variety of cosmetics at the same time, therefore, the adverse reaction may not be caused by the cosmetics brought by the patient for the patch test with cosmetic protoplast, or it may be caused by the combined use of several cosmetics; Third, the negligence of long-term cosmetic use. The cosmetics that patients carry for patch test are often the latest purchased and used, and different allergens cause adverse reactions for different lengths of time, causing this adverse reaction to occur may also be the cosmetics that have been used for a period of time before; Fourth, the results of the patch test are influenced by the subjective judgment of the physician. Patch test results may be ignored because the allergic reaction is relatively mild. Finally, possible deterioration, dilution, or loss of cosmetics during the period prior to the clinic attendance, due to factors such as preservation or the quality of the product itself, may also result in a false negative patch test.
In the present study, the compliance rate of the photopatch test was also low, only 19.32%, and the number of patients who underwent the photopatch test was also low, only 88. The possible reason for this is that photosensitizing substances are not the main factor causing cosmetic adverse reactions, which has been reported in the previous literature.24
As early as the early 21st century, a modified European standard series of allergen tests has been used in China and its usefulness has been confirmed.25 In this study, a total of 266 patients participated in European standard allergen patch test examination, and 218 cases were positive. More than 80% of the patients were able to detect allergens through European standard patch test. A total of 48 antigens were positive, most notably sodium dodecyl sulfate and thiomersal, and the remaining 46 antigens were sporadically distributed, in agreement with previous studies.7 The European standard patch test can compensate to a certain extent for the low detection rate of the patch test with cosmetic protoplast, which enables patients to recognize their allergens more clearly and avoid buying related products when purchasing cosmetics in the future, thus reducing the risk of adverse reactions. The detection rate can be increased to 86% with the addition of European standard allergens, although the compliance rate of the patch test with cosmetic protoplast is low (18%). Therefore, we recommend that the patch test with cosmetic protoplast be performed in conjunction with the European standard allergen patch test to improve the detection rate. Even if the patch test with cosmetic protoplast is positive, more specific allergens can be screened using the European standard allergen patch test, which will guide patients in their future product purchases. But it should be supplemented that with the increasing variety of cosmetic products in recent years, there may be some potential allergens that are hard to be detected by the European standard allergens. As well, the results of the patch test are subjectively judged by physicians, and thus there are limitations to the interpretation of their results in this study.
Acute allergic reactions have more severe clinical symptoms,26 so in order to better help the group, especially the allergic group, we did an analysis of the correlation between each indicator and the occurrence of allergic reactions within seven days. We found that dosage form (emulsion and cream), triethanolamine, rose oil, and propylene glycol were independent risk factors for the occurrence of anaphylactic reactions within seven days, and used this to develop a predictive model for the occurrence of anaphylactic reactions within seven days. Allergic individuals can be screened according to this model when choosing cosmetics to reduce the probability of acute allergic reactions.
In recent years, the advancement of nanotechnology may well improve the appealing adverse effects of cosmetics. Nanomaterials have the advantages of small size, high safety and stability, easy dose control, and high bioavailability.27 They have been reported in the field of atopic dermatitis and psoriasis.28,29 However, they are currently limited to laboratory studies. With the maturity and popularization of nanotechnology, it would have a broad application prospect in the field of cosmetics.
Besides, there are the following limitations in this study: First, there are certain limitations in the whole study process. Among the allergens we statistically identified, some of them are also found in non-care products (eg industrial products),30,31 and the source of potential allergens is not fully confirmed to originate from make-up products. Furthermore, since the definition of “cosmetic” in medicine is not fully standardized, there may be some bias in comparing the data with other literature.
Second, when accounting for the initial time of cosmetic use to the time of distance from onset, the collection of medical history relied on patients’ memories of their condition, and hence a certain amount of recall bias may lead to incomplete accuracy of the data. Moreover, many patients no longer suffer from the onset of the disease as a result of their first exposure to the allergen, but may have a second or even a third onset. In contact dermatitis, the time of onset and the severity of the second and third immunizations are different relative to the first immunization, but this is not distinguished in our data.
Despite these shortcomings, this study describes the epidemiological characteristics, cosmetic classifications, diagnostic types, onset times, as well as the characteristics of lesions, self-perceived symptoms, and patch test results of cosmetic adverse reactions in Han Chinese population in Shanghai and even in East China based on a large amount of data. The study also suggested a combined patch test with cosmetic protoplast with a European standard allergen series, which has positive implications for general dermatologists in identifying and diagnosing cosmetic adverse reactions. It also provides guidance to the general population on how to properly use and purchase cosmetics and how to perceive adverse reactions to cosmetics.
Conclusion
In conclusion, this study complements the data on reported adverse cosmetic reactions in the Chinese Han population and elucidates the need to improve the detection rate of patients with allergens in combination with European standardized allergen testing. Using correlates and allergens/irritants, we established a prediction model for the occurrence of allergic reactions within seven days to provide a reference for the selection of skin care products for allergic people. We suggest that people with allergies actively screen for allergens and choose appropriate skincare products. In addition, the use of nanotechnology in cosmetics is likely to be an important way to reduce their adverse effects in the future.
Data Sharing Statement
The data is not publicly available due to the contain information that could compromise confidentiality of the patients.
Ethics and Consent Statements
This study was conducted in accordance with the Declaration of Helsinki. The studies involving human participants were reviewed and approved by the Institutional Review Board of Huashan Hospital, Fudan University (2020-139). Written informed consent for participation was not required for this study in accordance with China Cosmetic Supervision and Administration Regulation and institutional requirements.
Acknowledgments
This study was funded by Huashan Hospital of Fudan University in Shanghai.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Alani JI, Davis MD, Yiannias JA. Allergy to cosmetics: a literature review. Dermatitis. 2013;24(6):283–290. doi:10.1097/DER.0b013e3182a5d8bc
2. U.S. Food and Drug Administration. Cosmetics | FDA [WWW Document]; 2018. Available from: https://www.fda.gov/cosmetics.
3. Lucca JM, Joseph R, Hussain Al Kubaish Z, Mohammad Al-Maskeen S, Ali Alokaili Z. An observational study on adverse reactions of cosmetics: the need of practice the Cosmetovigilance system. Saudi Pharm J. 2020;28(6):746–753. doi:10.1016/j.jsps.2020.04.017
4. Statista. Annual growth of the global cosmetics market from 2004 to 2021; 2021. Available from: https://www.statista.com/statistics/297070/growth-rate-of-The-global-cosmetics-market.
5. Panico A, Serio F, Bagordo F, et al. Skin safety and health prevention: an overview of chemicals in cosmetic products. J Prev Med Hyg. 2019;60(1):E50–E57. doi:10.15167/2421-4248/jpmh2019.60.1.1080
6. Nicolopoulou-Stamati P, Hens L, Sasco AJ. Cosmetics as endocrine disruptors: are they a health risk? Rev Endocr Metab Disord. 2015;16(4):373–383. doi:10.1007/s11154-016-9329-4
7. Morris SAV, Bobbitt JR, Ananthapadmanabhan KP, Kasting GB. The effect of prolonged exposure on sodium dodecyl sulfate penetration into human skin. Toxicol in Vitro. 2021;77:105246. doi:10.1016/j.tiv.2021.105246
8. Herman A, Aerts O, de Montjoye L, Tromme I, Goossens A, Baeck M. Isothiazolinone derivatives and allergic contact dermatitis: a review and update. J Eur Acad Dermatol Venereol. 2019;33(2):267–276. doi:10.1111/jdv.15267
9. Fransway AF, Fransway PJ, Belsito DV, et al. Parabens. Dermatitis. 2019;30(1):3–31. doi:10.1097/DER.0000000000000429
10. Di Nicola MR, Pontara A, Kass GEN, et al. Vipers of Major clinical relevance in Europe: taxonomy, venom composition, toxicology and clinical management of human bites. Toxicology. 2021;453:152724. doi:10.1016/j.tox.2021.152724
11. Hammond M, Gamal A, Mukherjee PK, et al. Cutaneous dysbiosis may amplify barrier dysfunction in patients with atopic dermatitis. Front Microbiol. 2022;13:944365. doi:10.3389/fmicb.2022.944365
12. Husain K. A survey on usage of personal care products especially cosmetics among university students in Saudi Arabia. J Cosmet Dermatol. 2019;18(1):271–277. doi:10.1111/jocd.12773
13. Salverda JG, Bragt PJ, de Wit-Bos L, et al. Results of a cosmetovigilance survey in The Netherlands. Contact Dermatitis. 2013;68(3):139–148. doi:10.1111/cod.12005
14. Guo X, Chen M, Meng X, et al. [Research progress in sample pretreatment and analytical techniques for cosmetics]. Se Pu. 2020;38(2):151–161. Chinese. doi:10.3724/SP.J.1123.2019.06031
15. Wetter DA, Yiannias JA, Prakash AV, Davis MD, Farmer SA, el-Azhary RA. Results of patch testing to personal care product allergens in a standard series and a supplemental cosmetic series: an analysis of 945 patients from the Mayo Clinic Contact Dermatitis Group, 2000-2007. J Am Acad Dermatol. 2010;63(5):789–798. doi:10.1016/j.jaad.2009.11.033
16. Warshaw EM, Buonomo M, DeKoven JG, et al. Importance of Supplemental Patch Testing Beyond a Screening Series for Patients With Dermatitis: the North American Contact Dermatitis Group Experience. JAMA Dermatol. 2021;157(12):1456–1465. doi:10.1001/jamadermatol.2021.4314
17. Zhu TH, Suresh R, Warshaw E, et al. The Medical Necessity of Comprehensive Patch Testing. Dermatitis. 2018;29(3):107–111. doi:10.1097/DER.0000000000000362
18. Johansen JD, Aalto-Korte K, Agner T, et al. European Society of Contact Dermatitis guideline for diagnostic patch testing - recommendations on best practice. Contact Dermatitis. 2015;73(4):195–221. doi:10.1111/cod.12432
19. Gefeller O, Pfahlberg AB, Uter W. What can be learnt from nothing? - A statistical perspective. Contact Dermatitis. 2013;69(6):350–354. doi:10.1111/cod.12112
20. Mahler V, Nast A, Bauer A, et al. S3 guidelines: epicutaneous patch testing with contact allergens and drugs - Short version, Part 1. J Dtsch Dermatol Ges. 2019;17(10):1076–1093. doi:10.1111/ddg.13956
21. Zaragoza-Ninet V, Blasco Encinas R, Vilata-Corell JJ, et al. Allergic contact dermatitis due to cosmetics: a clinical and epidemiological study in a tertiary hospital. Actas Dermosifiliogr. 2016;107(4):329–336. doi:10.1016/j.ad.2015.12.007.7
22. Zhao J, Li LF. Contact sensitization to cosmetic series of allergens in a general population in Beijing. J Cosmet Dermatol. 2014;13(1):68–71. doi:10.1111/jocd.12078
23. Hafner MFS, Rodrigues AC, Lazzarini R. Allergic contact dermatitis to cosmetics: retrospective analysis of a population subjected to patch tests between 2004 and 2017. An Bras Dermatol. 2020;95(6):696–701. doi:10.1016/j.abd.2020.04.011
24. Shao Y, Hu Y, Wang D, et al. Photopatch testing in Chinese patients: a 5-year experience. Contact Dermatitis. 2021;85(1):78–84. doi:10.1111/cod.13808
25. Wang WH, Li LF, Lu XY, Wang J. Cosmetic dermatitis in Chinese eczema patients patch tested with a modified European standard series of allergens. Contact Dermatitis. 2005;53(6):314–319. doi:10.1111/j.0105-1873.2005.00717.x
26. Simons FE. Anaphylaxis. J Allergy Clin Immunol. 2010;125(2 Suppl 2):S161–81. doi:10.1016/j.jaci.2009.12.981
27. Pan S, Goudoulas TB, Jeevanandam J, Tan KX, Chowdhury S, Danquah MK. Therapeutic Applications of Metal and Metal-Oxide Nanoparticles: dermato-Cosmetic Perspectives. Front Bioeng Biotechnol. 2021;9:724499. doi:10.3389/fbioe.2021.724499
28. Damiani G, Eggenhöffner R, Pigatto PDM, Bragazzi NL. Nanotechnology meets atopic dermatitis: current solutions, challenges and future prospects. Insights and implications from a systematic review of the literature. Bioact Mater. 2019;4:380–386. doi:10.1016/j.bioactmat.2019.11.003
29. Damiani G, Pacifico A, Linder DM, et al. Nanodermatology-based solutions for psoriasis: state-of-The art and future prospects. Dermatol Ther. 2019;32(6):e13113. doi:10.1111/dth.13113
30. Orton F, Ermler S, Kugathas S, Rosivatz E, Scholze M, Kortenkamp A. Mixture effects at very low doses with combinations of anti-androgenic pesticides, antioxidants, industrial pollutant and chemicals used in personal care products. Toxicol Appl Pharmacol. 2014;278(3):201–208. doi:10.1016/j.taap.2013.09.008
31. De Groot AC, White IR, Flyvholm MA, Lensen G, Coenraads PJ. Formaldehyde-releasers in cosmetics: relationship to formaldehyde contact allergy. Part 1. Characterization, frequency and relevance of sensitization, and frequency of use in cosmetics. Contact Dermatitis. 2010;62(1):2–17. doi:10.1111/j.1600-0536.2009.01615.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.