")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Analysis of a Case of Facial Nerve Injury Caused by Bee Sting in a Child
Received 21 July 2022
Accepted for publication 23 December 2022
Published 20 February 2023 Volume 2023:16 Pages 247—253
DOI https://doi.org/10.2147/RMHP.S381303
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Tang-Jiang Li,1,2 Min Xiang,3 Xin Lv1,2
1Department of Pediatric Surgery, Affiliated Hospital of Zunyi Medical University, Zunyi, 563000, People’s Republic of China; 2Department of Pediatric Surgery, Guizhou Children’s Hospital, Zunyi, 563000, People’s Republic of China; 3Department of Electrocardiogram Room, Affiliated Hospital of Zunyi Medical University, Zunyi, 563000, People’s Republic of China
Correspondence: Tang-Jiang Li, Department of Pediatric Surgery, Affiliated Hospital of Zunyi Medical University, Zunyi, 563000, People’s Republic of China, Tel +86 13984277525, Email [email protected]
Background: Bee sting injuries in children are accidental and occur in rural areas in summer and autumn. They have the characteristics of rapid onset, rapid change, many complications, complex treatment, and high disability rate. Patients experience various symptoms, such as vomiting, diarrhea, dyspnea, angioedema, multiple neuritis, myocardial infarction, acute renal failure, hypotension, and collapse. Systemic complications of the nervous system are rare. However, some cases of stroke, optic neuritis, and acute disseminated encephalomyelitis are related to bee stings. There are many cases of systemic multiple organ dysfunctions after bee sting injury, but there are few reports of facial nerve injury. The case presented here was caused by bee venom. This report is important because there are few instances of facial paralysis in the large number of notified bee sting cases. After active treatment, the facial paralysis of the child recovered gradually.
Case Presentation: The patient was a 6-year-old boy. The bee stings by bee swarm induced pain in many parts of the body for 8 h. After the injury, he had skin itching, rash, swelling, and pain in the head and face. The boy had soy sauce-colored urine later and was transferred to the Affiliated Hospital of Zunyi Medical University from a lower-level hospital for treatment. On the seventh day after transfer, the child suddenly suffered from deviated mouth, which was considered a delayed facial nerve injury. After active treatment, he recovered from facial paralysis and was discharged from the hospital.
Conclusion: This case report adds the clinical manifestation of facial paralysis after bee stings. They require close observation and being alert to possible clinical manifestations, as well as carrying out active intervention treatment.
Keywords: children, bee sting, facial nerve injury, combined treatment
Introduction
Summer and autumn are the most common seasons for bee stings. Bee sting injuries in children are accidental and occur in rural areas in summer and autumn. They have the characteristics of rapid onset, rapid change, many complications, complex treatment, and high disability rate. After bee stings, patients experience various local symptoms, such as vomiting, diarrhea, dyspnea, angioedema, multiple neuritis, myocardial infarction, acute renal failure, hypotension, and collapse. Systemic complications of the nervous system are rare in these patients. However, some cases of stroke, optic neuritis, and acute disseminated encephalomyelitis are related to bee stings.1–6 Bee stings may cause skin redness, swelling, and pain in mild cases, or multiple organ dysfunction7 or even anaphylactic shock in severe cases, which need timely treatment. There are many cases of systemic multiple organ dysfunctions after bee sting injuries, but there are very few reports of facial nerve injuries. This case presentation discusses a child with multiple organ dysfunction and facial nerve injury after bee stings who was successfully cured in the subject hospital.
Clinical Data
The patient was a 6-year-old boy. The patient was hospitalized for 8 h for multiple body aches caused by bee stings. The child was treated in local hospital because of skin itching, rash, swelling, and pain on the head and face after stabbing hornets’ nest and being stung by a swarm of hornets. The child was transferred to the Affiliated Hospital of Zunyi Medical University from a lower-level hospital for further treatment due to obvious head swelling, severe stings, and soy sauce-colored urine. Legal guardian of the patient provided informed consent for the case details and images to be published.
A physical examination showed temperature 36.8°C, pulse 112 beats/min, respiratory rate 24 times/min, blood pressure 100/60 mmHg, and the child was depressed and sleepy. Scattered needle-like wounds caused by bee stings could be seen on the top of the head, both upper limbs, both knees, and both feet. The wounds on the top of the head were the densest. Local redness and swelling were obvious, white needle-like pus spots were seen on some wounds, and no residual bee stings were found. The respiratory sounds of both lungs were clear without dry and wet rales, the heart rhythm was regular, and there was no murmur in either valve area. An abdominal physical examination showed no special findings. There was no history of difficulty in swallowing and no deviation in the angle of the mouth. Neurological examination showed that the patient was well oriented. There was no evidence of central and peripheral facial nerve palsy.
Supplementary examination results showed leukocyte 18.50 × 109/L, neutrophil absolute value 15.61 × 109/L, hemoglobin 124 g/L, and total platelet count 204 × 109/L. A routine urine test showed occult blood +3 and urinary protein +2. Liver function showed alanine aminotransferase 863 U/L and glutamic oxaloacetic transaminase 3190 U/L. Renal function was normal. Myocardial enzymes were creatine kinase 19,030 U/L, creatine kinase isoenzyme 500 U/L, lactate dehydrogenase 2317 U/L, and α-hydroxybutyrate dehydrogenase 1230 U/L. Myoglobin was 1239 ng/mL, and high-sensitivity troponin was 18.40 ng/L. Coagulation function activated partial thromboplastin time was 62.70 s. Electrolytes were in the normal range.
The diagnoses were bee stings and multiple organ dysfunction syndromes (MODS). The patient was immediately given cefazolin to fight against infection and allergy, accelerate toxin discharge, and neutralize free toxins. Treatments for protecting the liver, nourishing myocardium, and alkalizing urine were given. Jidesheng snake medicine was applied externally and taken orally. Water electrolyte balance and acid–base balance were maintained. Symptomatic supportive therapy was administered.
After active treatment, the symptoms improved significantly. The patient’s mental state improved, the head and face swelling subsided significantly, and the myocardial enzymes, liver function, coagulation function, hematuria, urine protein and so on improved gradually. On the seventh day after admission, the family members of the child found that the left corner of his mouth was crooked, especially when talking and smiling. This was considered as facial paralysis caused by nerve injury from the bee venom. Acupuncture physiotherapy, oral vitamin C, and compound vitamin B were given to promote nerve recovery. After 16 d of hospitalization, all the indexes returned to normal levels, the facial paralysis was significantly improved, and the child was discharged (Figures 1–4).
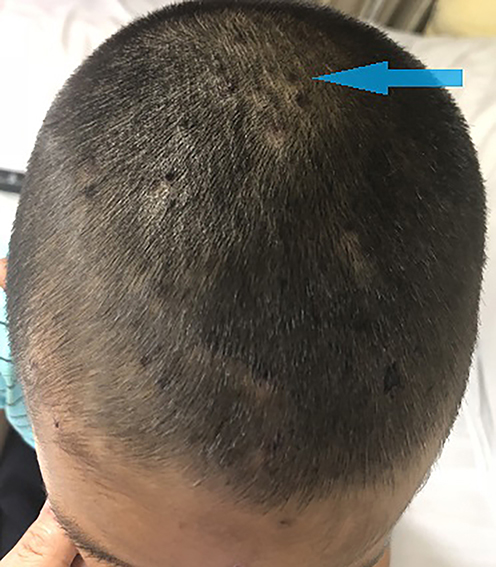 |
Figure 1 Bee stings on the head and face (The arrow shows scattered needle-like wounds from bee stings on the top of the head). |
 |
Figure 2 Before facial paralysis treatment (The arrow here indicate facial nerve injury, as shown by the crooked corners of the mouth). |
 |
Figure 3 After facial paralysis treatment (The arrow shows a marked improvement symptoms of crooked mouth after treatment). |
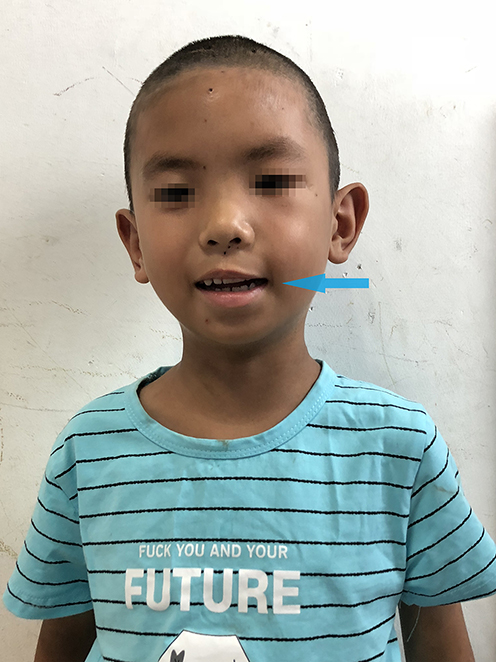 |
Figure 4 The boy is smiling after facial paralysis treatment (The arrow shows a significantly improvement of crooked mouth after treatment). |
Discussion
Bees belong to hymenoptera, and those which sting are mainly honey bees, wasps, and hornets.8 Bee tail stings are connected to the venomous glands. When person is stung, the toxins in the venomous glands are injected into the skin through the stings, causing local or systemic reactions. The clinical manifestations of bee stings are closely related to the volume of bee venom and can cause death in severe cases. Different kinds of bees have varying venom chemical properties. Honey bee venom is acidic, while hornet venom is alkaline. After hornet stabs, the tail sting is recovered; while after honey bee stabs, the tail sting is left behind in the human body. Bee venom has complex components, mainly including histamine, various enzymes, formic acid, neurotoxin, and hemolytic toxin. When the bee sting enters the skin, the venom in the venomous gland enters the human body, causing symptoms of poisoning. The toxic reaction caused by bee venom is related to the amount of bee venom entering the human body, the site of the sting, and whether there is an allergic reaction.9 A single bee sting only causes local redness, itching, pain, and urticaria and can often heal itself without residual dysfunction. But if multiple sites are stung, systemic toxic reactions will occur, resulting in liver and kidney function damage, myocardial toxicity, arrhythmia, and heart failure.10,11 When hemolytic reaction occurs, hemoglobinuria and even acute renal failure may be induced, resulting in multiple organ dysfunction.
Bee venom has neurotoxicity; whole bee venom, melittin, apamin, and tropine have significant neutrophilic properties. The neurotoxin of bee venom is mainly exerted by melittin, which is peptide composed of 18 amino acids, with two disulfide bonds between the first and the eleventh amino acids and between the first and the fifteenth amino acids. It has toxic effects on both the central and peripheral nervous systems. Bee venom can selectively block the nerve cholinergic receptor, block the nicotinic cholinergic receptor in the central nerve, induce encephalitis and immune response, and cause brain tissue damage. It can inhibit the nerve-muscle synaptic transmission, cause weak curare-like effect, and impede the transmission of ganglion to inhibit the peripheral nerve. In this case, the child suffered from facial paralysis after being stung by bees, the exact pathogenesis of the development of neurological symptoms following bee sting is unknown. The postulated mechanisms include 1) These were in the distribution area of the facial nerve, and the volume of bee venom was large. Melittin might inhibit the activity of Na+-K+-ATPase on the nerve synapse through the above mechanism,12 resulting in facial nerve paralysis. 2) Bee venom is composed of proteins like hyaluronidase, phospholipase, peptides like secapin, apamin, procamine, and active amines like histamine and apamin. Apamin is a potent neurotoxin known to inhibit calcium-dependent potassium channel in brain and spinal code, impede the transmission of neural signal to inhibit the peripheral nerve. 3) Honey bee venom contains certain allergenic proteins that induce the production of IgE antibodies. These antibodies can cross-react with myelin basic proteins and cause various neurological symptoms. Together with the fact that most of the reported cases are second bites, they are in a pre-sensitive state and thus aggravate the hypersensitivity reaction.5 Most of the reactions are caused by IgE-mediated type I hypersensitivity. Delayed/late reactions include serum sickness, nephritic syndrome, vasculitis, neuritis or encephalopathy. Just as the patient developed facial paralysis on the seventh day. The pathogenesis of late reactions is not clear, but it is perceived to be a non-IgE-mediated immunological response (type III hypersensitivity) to hymenoptera venom involving deposition of immune complexes and complement activation. However, the specific mechanism of peripheral nerve injury is not fully understood.13 If one is allergic to bee venom, it will also induce skin rash, laryngeal edema, bronchospasm, slow heart rate, decreased blood pressure, and even anaphylactic shock. The child in this case was stung by a swarm of bees over wide area of the body introducing a large volume of bee venom. Therefore, liver dysfunction, myocardial damage, hemoglobinuria, and secondary coagulation dysfunction occurred successively.
At present, there is no specific drug for bee sting injuries. Treatment may be local or systemic.
(1) Local treatment: For patients with bee stings, the wound surface should be fully exposed. The head and face are the most vulnerable areas for bee stings. Hair on the top of the head can be cut short or shaved to fully expose the wound surface. Residual bee stings should be found and picked out as far as possible. Furthermore, the species of bee should be determined if possible, and appropriate liquid should be chosen to treat the wound according to the acidity and alkalinity of the venom. Honey bee venom is acidic and can be washed with weak alkaline solution, such as soapy water and low-concentration sodium bicarbonate to neutralize the toxin. Hornet venom is weakly alkaline and common vinegar can be used to clean up the wound and neutralize the toxin. For patients who cannot identify the type of bee sting, normal saline is usually used to clean the wound surface.
(2) Systemic treatment is as follows:
(i) Jidesheng snake medicine is the most conventional medicine for the treatment of snake bite. Its effective ingredients include Paris polyphylla, centipede, toad skin, creeping euphorbia, and other ingredients. It can relieve fever, improve microcirculation, promote the recovery of liver and kidney functions, enhance the detoxification function of the body, and has a significant and lasting role in relieving stools, protecting the liver, and promoting the recovery of toxic liver cells.14 It is also widely used in patients with bee stings. The initial dose is 20 tablets, then 10 tablets every 6 h until the symptoms are relieved and the swelling subsides. Meanwhile, white vinegar should be used to make a thin paste for external application on the affected area and to ensure that the Jidesheng snake medicine is in a wet state to facilitate drug absorption.
(ii) Early, massive, and short-term use of glucocorticoids can prevent adrenal hypofunction, inhibit and reduce the allergic reaction and necrosis of tissues, enhance the detoxification ability of the body, and relieve the stress response to bee venom. In routine situations, 10 mg of dexamethasone mixed with 5% glucose saline is injected intravenously for 4–5 d, and generally for not more than 7 d.
(iii) Bee stings are often accompanied by local infection. Semi-synthetic penicillin or the first generation of cephalosporins with less toxicity to the liver and kidneys can be used to avoid damaging liver and kidney function and aggravating renal load.
(iv) In case of shock, the patient is treated with active anti-shock therapy. In the case of anemia, the patient is treated with the timely transfusion of red blood cells. When there is a tendency to gastrointestinal bleeding, the patient is treated with acid production, protection of gastric mucosa, and liquid diet. In the case of dyspnea or paralysis of respiratory muscles, the patient is treated with timely tracheotomy to assist breathing. When the myocardium is damaged, the patient is treated with nutrition to the myocardium. When renal function is severely damaged, the patient is treated for strengthening diuresis, alkalizing urine, protecting kidney function, promoting toxin excretion, and performing timely blood purification. At present, it is considered that blood purification is an effective treatment for acute renal failure or MODS after bee stings.15
(v) In foreign countries, bee venom immunotherapy has been adopted as a conventional method for the treatment of bee stings, and its efficacy and safety have been verified.16 The incidence of adverse reactions from immunotherapy is low, and these are mostly manifested as local skin redness and swelling, so it can be used for both adults and children.17 However, the immunotherapy of bee venom has not been carried out in China at present. If bee venom immunotherapy can be gradually carried out in China, it will greatly improve the survival rate of patients with bee stings, reduce the disability rate, and improve the effects of treatment.
Summary
Summer and autumn are the seasons with high incidence of bee stings for children, especially those in rural areas. Children are curious about things around them. They like to play in the wild and also like to take risks, like to catch bees or like to poke hornets’ nests. They have no safety awareness and life experience and lack self-preservation ability, so they are susceptible to bee stings. After being stung by a swarm of bees, the onset of symptoms is acute, and the progress is rapid. If the treatment is not timely, serious complications and even death may occur. Therefore, early detection, diagnosis, and treatment are the keys to the successful treatment of bee stings. Furthermore, because children’s tissues and organs are not fully developed, their tolerance to bee venom is less than that of adults, and bee venom has more serious impact on them. Due to immature physical and psychological development and poor adaptability, children lack judgment when they experience discomfort, such as pain and swelling after being stung. They are often anxious, irritable, will cry and have other emotions, and may not cooperate with medical staff to treat the disease. Therefore, psychological comfort and counseling for injured children is also one of the key measures for successful treatment.
Due to lack of safety awareness and self-protection ability, after children are stung by bees, especially by bee swarm, they have severe symptoms, many complications, and high mortality. Therefore, it is particularly important to strengthen parental supervision of children and to improve the knowledge about bee sting protection in rural areas. Early, timely, correct, and effective treatment after bee stings is an effective measure to reduce death and complications.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). The study was approved by Ethics Committee of the Affiliated Hospital of Zunyi Medical University (KLL-2022-609). Legal guardian of the patient provided informed consent for the case details and images to be published.
Acknowledgments
We are particularly grateful to all the people who have given us help on our article.
Funding
No external funding was received to conduct this study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Jain J, Banait S, Srivastava AK, Lodhe R. Stroke intracerebral multiple infarcts: rare neurological presentation of honey bee bite. Ann Indian Acad Neurol. 2012;15(2):163–166. doi:10.4103/0972-2327.95008
2. Kahilogullari G, Ugur HC, Tatli M, Kanpolat Y. Trigeminal neuropathic pain following honeybee sting: a case report. Turk Neurosurg. 2010;20(2):261–264. doi:10.5137/1019-5149.JTN.1761-09.1
3. Choi MY, Cho SH. Optic neuritis after bee sting. Korean J Ophthalmol. 2000;14(1):49–52. doi:10.3341/kjo.2000.14.1.49
4. Boz C, Velioglu S, Ozmenoglu M. Acute disseminated encephalomyelitis after bee sting. Neurol Sci. 2003;23(6):313–315. doi:10.1007/s100720300007
5. Poddar K, Poddar SK, Singh A. Acute polyradiculoneuropathy following honey bee sting. Ann Indian Acad Neurol. 2012;15(2):137–138. doi:10.4103/0972-2327.95000
6. Pirasath S, Senthan V, Seneviratne MH. Kounis syndrome: acute myocardial infarction following multiple bee stings. SAGE Open Med Case Rep. 2021;9:2050313X21999206. doi:10.1177/2050313X21999206
7. Navaradnam P, Suganthan N, Kumanan T, Sujanitha V, Mayorathan U. Kounis syndrome and multiorgan failure following multiple wasp stings. Cureus. 2021;13(4):e14606. doi:10.7759/cureus.14606
8. Badiadka KK, Amir S, Prarnod KL. Wasp sting envenomation a case report. Int J Med Toxicol Leg Med. 2017;20(1):40–43. doi:10.15406/frcij.2017.04.00135
9. Smits JH, van der Linden J, Blankestijn PJ, Rabelink TJ. Coagulation and haemodialysis access thrombosis. Nephrol Dial Transplant. 2000;15(11):1755–1760. doi:10.1093/ndt/15.11.1755
10. Yan N, Zhang SX, Liu SY. A case of anaphylactic shock with severe arrhythmia caused by wasp sting. Chin J Crit Care Med. 2000;3:45. Chinese.
11. Liu KY, Liu Y. Clinical analysis of 12 cases of bee sting poisoning. Chin J Coal Industry Med. 2000;10:1064. Chinese.
12. Yang S, Zhang XM, Jiang MH. Inhibitory effect of melittin on Na+,K+-ATPase from Guinea pig myocardial mitochondria. Acta Pharmacol Sin. 2001;22(3):279–282.
13. Bánovcin P, Havlíceková Z, Jesenák M, et al. Severe quadriparesis caused by wasp sting. Turk J Pediatr. 2009;51(5):485–488.
14. Rao M, Gan YP. Early comprehensive treatment of 52 cases of snake bite. People Mil Surg. 2013;56(12):1442–1443. Chinese.
15. Wang T, Zhang F, Wei M, et al. Clinical effects of different blood purification methods in the treatment of acute renal failure caused by wasp sting. J Chongqing Med Univ. 2014;39(06):828–831. Chinese.
16. Zhao Y, Zhang F, Cao LH, et al. The research progress of venom immunotherapy for bee stings. Med Recapitulate. 2016;22(13):2582–2585. Chinese.
17. Goldberg A, Confino-Cohen R. Bee venom immunotherapy - how early is it effective? Allergy. 2010;65(3):391–395. doi:10.1111/j.1398-9995.2009.02198.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.