Back to Journals » Local and Regional Anesthesia » Volume 16
Analgesic Effects of Different Local Infiltration Anesthesia Techniques Combined with Femoral Nerve Block in Patients Undergoing Total Knee Arthroplasty: A Randomized Controlled Clinical Trial
Authors Gui YK ![]() , Xiao R
, Xiao R ![]() , Luo YR
, Luo YR ![]() , Liu Y, Da X
, Liu Y, Da X ![]() , Zhu SH
, Zhu SH ![]() , Shi DW, Hu XD, Xu GH
, Shi DW, Hu XD, Xu GH
Received 23 August 2023
Accepted for publication 29 November 2023
Published 22 December 2023 Volume 2023:16 Pages 183—192
DOI https://doi.org/10.2147/LRA.S436767
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Yong-Kang Gui,1,2,* Rui Xiao,3,* Ya-Ru Luo,1,2,* Yang Liu,1,2 Xin Da,1,2 Si-Hui Zhu,1,2 De-Wen Shi,1,2 Xu-Dong Hu,1,2 Guang-Hong Xu1,2
1Department of Anesthesiology, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, 230022, People’s Republic of China; 2Key Laboratory of Anesthesia and Perioperative Medicine of Anhui Higher Education Institutes, Hefei, Anhui, 230022, People’s Republic of China; 3Fuyang Hospital of Anhui Medical University, Fuyang, Anhui, 230022, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guang-Hong Xu, Department of Anesthesiology, The First Affiliated Hospital of Anhui Medical University, Hefei, Anhui, 230022, People’s Republic of China, Tel +86-13856949535, Fax +86 551 62923704, Email [email protected]
Objective: Pain after total knee arthroplasty (TKA) remains an unresolved problem. Femoral nerve block (FNB) could relieve pain; however, it alone is insufficient. The local infiltration anesthesia technique (LIA) has been suggested as a supplement to FNB. This study aimed to evaluate the analgesic effects of different LIA combined with FNB in TKA patients.
Methods: The femoral nerve was blocked with 0.375% ropivacaine 20mL, and all patients routinely received general anesthesia. The primary indicator was the proportion of patients who did not receive post-operative remedial analgesia. Seventy-eight patients were randomly assigned to PAI (periarticular injection combined with FNB), IAI (intra-articular injection combined with FNB), or control (FNB alone) groups. All patients underwent FNB under general anesthesia. The primary outcome was the proportion of patients who did not receive additional postoperative analgesia within the first 48 h after surgery.
Results: Compared with the PAI and control groups, the IAI group had a higher proportion (69.23%) of patients who did not receive remedial analgesia within 48 hours after surgery (P = 0.009; P = 0.009), a lower consumption of diclofenac sodium lidocaine (P = 0.021; P < 0.001), and an earlier time of walking with a walker (P < 0.001; P < 0.001). The time of first need for remedial analgesia postoperatively in IAI group was longer than the PAI group (P = 0.008) and IAI group has a shorter hospital stay than the control group (P = 0.008). The maximum NRS during the first 48 hours postoperatively and NRS 24 hours after surgery in the IAI group were lower than those in the control and PAI groups. The incidences of POD and PONV were similar among the three groups (P = 0.610; P = 0.264).
Conclusion: When combined with FNB, intra-articular injection offers a superior analgesic effect and favorable recovery compared to periarticular injection and separate application of FNB.
Keywords: analgesia, local infiltration anesthesia, nerve block, total knee arthroplasty
Introduction
Total knee catheterization is a severe traumatic operation.1,2 The uncontrollable postoperative pain will significantly affect the early postoperative activities of patients, prolong the length of hospital stay, increase the consumption of opioids and increase the economic burden of patients.3–5 Pain management is key to enhanced recovery after surgery (ERAS) in TKA.6 However, pain after TKA remains an urgent problem, and the optimal analgesic regimen remains controversial.7–9
In recent years, with the popularization of ultrasound technology in clinical anesthesia, the application of peripheral nerve block (PNB) in major orthopedic surgeries, such as joint arthroplasty, has gradually become favored by more clinicians.10 Femoral nerve and sciatic nerve are the main innervating nerves of the lower limbs, and their combined block has also been widely used in TKA.11 However, due to the deep location of sciatic nerve and its unclear ultrasonic imaging, irreversible injury of the sciatic nerve after sciatic nerve block have been reported, which is undesirable.12,13 However, if TKA patients only received FNB, a large number of them will still experience severe postoperative pain.14
The local infiltration anesthesia technique (LIA) has been introduced into clinical practice15 and provides effective analgesia after TKA, even when combined with multimodal systemic analgesia.16 Related studies have suggested LIA as a supplement to conventional pain control modalities including FNB.14,17 There are commonly used after TKA: periarticular injection (PAI) and intra-articular injection (IAI).18
However, the effect of FNB combined with different LIA on postoperative analgesia after TKA is still unclear. Therefore, we designed this randomized controlled trial (RCT) to observe the effect of different LIA combined with FNB on postoperative analgesia after TKA, so as to provide reference for clinical application.
Methods
The randomized controlled trial (RCT) was registered with the Clinical Trials Registry (ChiCTR1900028425, website: www.chictr.org.cn/) on December 21, 2019, and approved by the First Affiliated Hospital of Anhui Medical University Clinical Medical Research Ethics Committee (PJ2020-03-04) on February 5, 2020. All the patients provided written informed consent to participate in the study. This clinical trial was performed between February 2020 and October 2020.
Study Participants
Patients aged 50–80 years undergoing elective TKA under general anesthesia were eligible for participation. All participants were classified as American Society of Anesthesiologists (ASA) physical status classes I–III and had normal communication skills. The exclusion criteria were as follows: TKA resulting from trauma, allergy to medicines used in the research, contraindications for peripheral nerve block (PNB), arrhythmia that affects hemodynamic stability, history of heart failure, neurological or psychiatric diseases such as cerebral infarction associated with sequelae or dementia, failed preoperative screening of Montreal cognitive assessment (MoCA), history of opioid use, or failed cooperation with researchers. Participants who met the following criteria were excluded from the study: serious complications, sent to the Intensive Care Unit (ICU), and incomplete data.
After excluding 19 ineligible patients, 78 patients were randomly assigned to one of the three study groups, all of whom completed the experiment and were followed up until discharge (Figure 1). The demographic characteristics were similar among the three groups (Table 1).
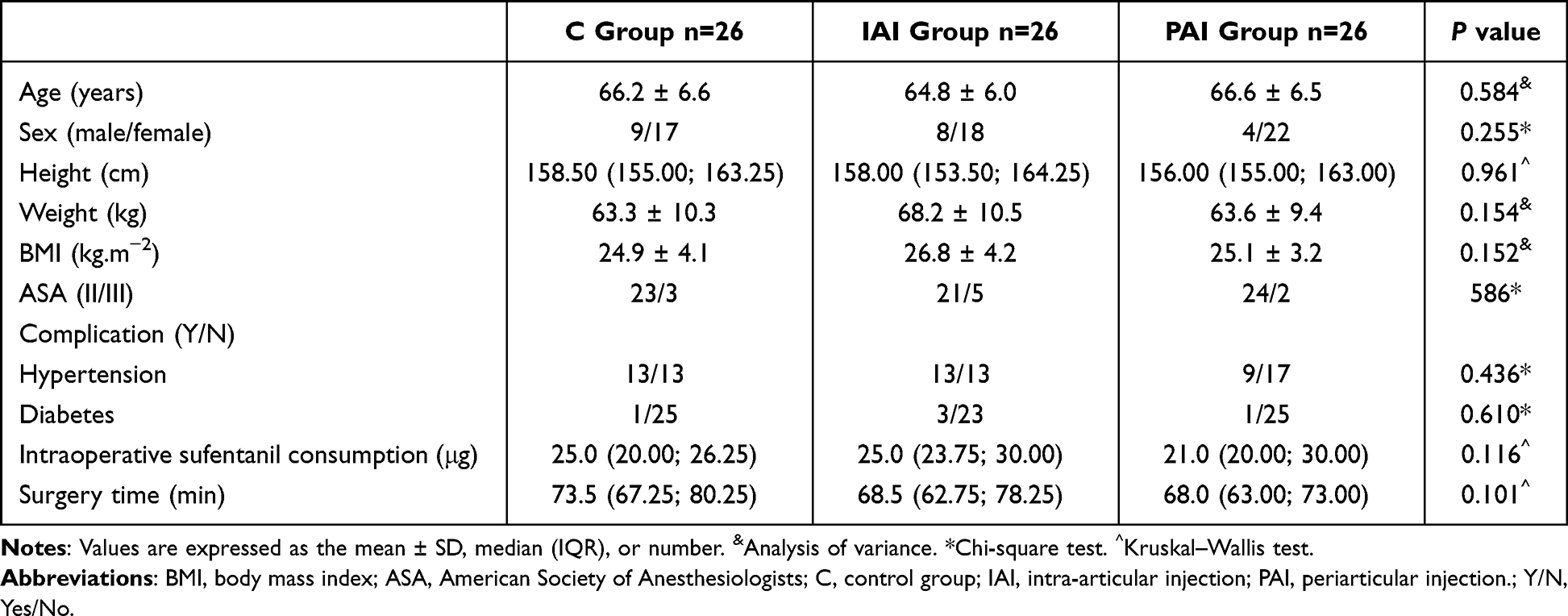 |
Table 1 Demographic Characteristics and Operation Details |
 |
Figure 1 Consolidated standards of reporting trials flow diagram through study. Abbreviations: C, control group; IAI, intra-articular injection; PAI, periarticular injection; FNB, Femoral nerve block; TKA, total knee arthroplasty; MoCA, Montreal cognitive assessment. |
Randomization and Blinding
Patients were assigned to the PAI group (periarticular injection combined with FNB), IAI group (intra-articular injection combined with FNB), or control group (FNB alone) using a computer-generated randomization sequence, which was sealed in sequentially numbered, opaque, and sealed envelopes. Before the surgery, the specialist nurse opened a consecutively numbered envelope and prepared a solution for the LIA. Anesthesiologists, physicians, and other nurses were unaware of the group assignment. A researcher who was not aware of the group status and only specialized in postoperative visit was responsible for the postoperative visit and related information collection, and the number of patients with no remedial analgesia within 48 hours after surgery was recorded (patients were instructed to self-measure their pain degree using NRS score before surgery, and nurses in the ward were responsible for pain assessment every 6 hours postoperatively).
Nerve Block and General Anesthesia Procedure
All patients were routinely monitored in the operating room using electrocardiogram (ECG), pulse, pulse oxygen saturation (SpO2), and blood pressure (BP). Patients were also open for peripheral venous access for the delivery of sodium lactate ringer solution 5 mL/kg/h and received masked oxygen. A bispectral index monitor (BIS) was used to adjust the appropriate depth of anesthesia.
The patient was in a supine position with both lower limbs slightly abducted and the affected limb slightly externally rotated. After intravenous administration of 5μg sufentanil to relieve anxiety and pain, FNB was performed in the operated limb. Under ultrasound guidance, the needle was inserted into the lateral side of the femoral artery, close to the femoral nerve, to avoid injury to the femoral artery. A nerve stimulator was used to look inward towards the femoral nerve. When the quadriceps muscle, especially the rectus femoris muscle, is split, the needle tip is located at the level of the femoral nerve. Subsequently, local anesthetic was injected into the lateral femoral nerve. Under ultrasound, a dark liquid area was observed to spread around the femoral nerve to ensure the safety of the femoral nerve block. The FNB was completed using 0.375% ropivacaine 20mL.
After completion of FNB, all patients received general anesthesia. For anesthesia induction, etomidate at 0.2–0.3 mg/kg according to the systemic conditions of patients, sufentanil at 0.2–0.5µg/kg, and cis-atracurium at 0.15–0.2 mg/kg were injected, followed by laryngeal mask airway insertion when the eyelash reflex disappeared. Mechanical ventilation parameters were set to maintain the end-tidal carbon dioxide (PETCO2) at 35–45 mmHg and SpO2 at 99–100%. Intravenous-inhalation balanced anesthesia (propofol and 0.5–0.7 MAC sevoflurane for avoiding intraoperative awareness) was used to maintain BIS at 40–60 during the whole operation. Sufentanil and cis-atracurium were administered intravenously as needed. Intraoperative BP and heart rate were maintained at ± 20% of the baseline values. All patients received 50 mg flurbiprofen before surgery and 50 mg flurbiprofen near the end of surgery. To prevent postoperative nausea and vomiting (PONV), 10 mg metoclopramide was administered intravenously to all patients 30 minutes before the end of surgery.
Local Infiltration Anesthesia Technique and Tourniquet
All local infiltration anesthesia procedures were performed by the same group of experienced surgeons to eliminate any potential bias due to differences in technique, and the drug solution was prepared by a specialist nurse to ensure that the others were blinded to the grouping. There are two types of solutions for periarticular injections: (1) a total of 20 mL of the drug solution composed of 5 mL 1% ropivacaine, 1 mL compound betamethasone and 14mL normal saline, and (2) 20 mL saline alone. Periarticular injections were performed several times in sequence along the perimeter of the incision, approximately at 25-mm intervals, before the incision was closed. The needle was inserted perpendicular to the edge of the incision and injected at the same time as the needle was withdrawn.
There are two types of solutions for intra-articular injections: (1) a total of 50 mL of the drug solution composed of 5 mL 1% ropivacaine, 1 mL compound betamethasone and 44mL normal saline; (2) 50 mL saline alone. At the end of surgery, after sealing of the joint cavity and before the joint cavity drainage tube was connected to the drainage bottle, the above solutions were injected into the joint cavity through the drainage tube. After IAI, the joint cavity drainage tube was clamped for 2 hours and then opened, and the tube was removed on the second postoperative day.
Patients in the control group received a periarticular injection of 20 mL saline and an intra-articular injection of 50 mL saline. Patients in the IAI group received a periarticular injection of 20 mL saline and an intra-articular injection of 50 mL drug solution. Patients in the PAI group received a periarticular injection of 20 mL of drug solution and an intra-articular injection of 50mL saline.
The tourniquet was inflated at the start of the procedure and deflated after the skin closure. Tourniquet pressure setting: Systolic blood pressure (SBP) + 100 mm Hg.
Analgesia Scheme
All patients received celecoxib 200 mg orally before entering the operating room.
In the post-anesthesia care unit (PACU), 5–10 µg sufentanil was administered intravenously when the numerical rating scale (NRS; 10 cm scale, where 0 = no pain and 10 = worst pain) score was ≥ 3/10. In the ward, postoperative conventional analgesia was achieved with scheduled oral celecoxib 200 mg every 12 h. When the patient’s NRS score was ≥ 3/10, or when the patient required it, diclofenac sodium was mainly used for analgesia. If the patient’s NRS score was still ≥ 3/10 or the patient requested it, opioids were used to provide remedial analgesia. For example, patients received oral oxycodone (10 mg) and intramuscular injection of tramadol (100 mg).
The nurses assessed the intensity of pain every 6 h. The type of remedial analgesic used was based on the patient’s condition.
Study Outcomes
The primary outcome was the proportion of patients who did not receive additional postoperative analgesia within the first 48 h after surgery.
The duration of analgesia (the duration from the completion of FNB to the first postoperative remedial analgesia, patients who did not receive remedial analgesia within 48 hours were included in the analysis with 48 hours as the maximum cutoff time of remedial analgesia); resting NRS at postoperative 6h, 12h, 24h, 48h; motorial NRS at postoperative 12h, 24h, 48h; maximum NRS; dosage of postoperative remedial analgesics during the postoperative 48 h; occurrence of postoperative nausea and vomiting (PONV) and postoperative delirium (POD) assessed by the CAM-ICU scale during postoperative 72 h; first time to walk with a walker (the patient could press the leg and extend the knee by himself, perform terminal extension training moderately, press the knee joint to the bed surface with the assistance of others, and then try to get out of bed with the assistance of a walking aid); and length of hospital stay (LOHS) were recorded as secondary outcomes.
Statistical Analysis
Statistical analysis of the data was performed using Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL, USA) V26.0. Normality of distribution was assessed using Shapiro–Wilk test. Quantitative data were expressed as mean ± standard deviation (SD) or median (interquartile range, IQR) according to their distribution. Normally distributed age and Body Mass Index (BMI) data were assessed using analysis of variance, while other quantitative data were analyzed using the Kruskal–Wallis test and pairwise multiple comparisons. Qualitative data were expressed as numbers and analyzed using the chi-square (χ2) test. The duration of analgesia was analyzed using Kaplan-Meier survival analysis and compared between the groups using the Log rank test. P < 0.05 in Pairwise multiple comparisons were considered to be statistically significant at P < 0.05. All other tests were performed at the 5% level bilaterally.
Sample Size Calculation
The sample size was calculated as the proportion of patients without additional postoperative analgesia during postoperative 48 hours according to the preliminary experimental data. In the preliminary experiment including 27 patients, the number of patients without postoperative additional analgesia was respectively 3 (33%) in control group:7 (78%) in IAI group: and 3 (33%) in PAI group. When α was 0.05 and 1-β was 0.9, the calculated sample size was 72. A dropout rate of 20% was considered; 97 patients were screened, and 78 participants completed the study.
Results
In the present study, none of the patients required remedial analgesia in the PACU. In the IAI group, 18 patients (69.23%) did not receive remedial analgesia within 48 hours after surgery, which was significantly higher than that in the PAI group (26.92%) and the control group (26.92%) (P = 0.002 and P = 0.002, respectively), however, there was no difference between the PAI and control groups (P >0.999). The time of first remedial analgesia within 48 days after operation in IAI group was significantly longer than that in PAI group (P = 0.008), there was no difference between the PAI and control groups (P >0.999). The consumption of diclofenac sodium was lower in the IAI group than in the control and PAI groups (P < 0.001 and P = 0.021, respectively), meanwhile, PAI group was lower than that in the control group (P = 0.049). When tramadol and oxycodone were converted to equivalent doses of morphine, the dosage of morphine in the PAI group was higher than that in the control group (P = 0.001), whereas there was no difference in the dosage of morphine between the IAI and control groups (P = 0.519) or between the IAI and PAI group (P = 0.070). The IAI group had the shortest LOHS (P = 0.008), whereas there was no significant difference between the PAI and control groups (P > 0.999). Patients in the IAI group had the earliest postoperative walk after surgery with the help of a walker earlier than those in the PAI and control groups (P < 0.001), whereas the time of walking was comparable between the control and PAI groups (P = 0.510) (Table 2).
 |
Table 2 Postoperative Medication Details and Postoperative Rehabilitation |
Kaplan-Meier survival analysis (Figure 2) showed that the duration of analgesia for patients without remedial analgesia was 48 h, and the duration of analgesia was comparable between the control and PAI groups (P = 0.483). However, the median duration of remedial analgesia was lower in the IAI group than in the control and PAI groups (P =0.006 and P = 0.003, respectively).
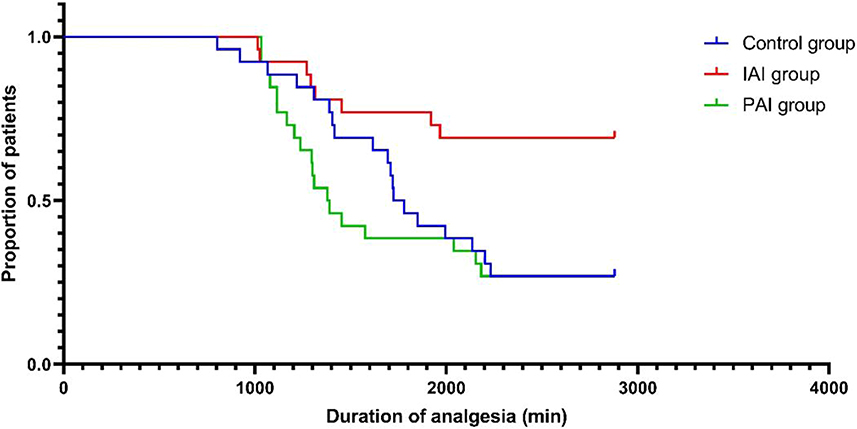 |
Figure 2 Kaplan-Meier survival plot for the duration of analgesia. Notes: Log rank test (P=0.004 comparison among three groups; P = 0.483 comparison between the control group and PAI group; P=0.006 comparison between the control group and IAI group; P=0.003 comparison between the IAI group and PAI group). |
The resting pain score of the IAI group at 12 hours postoperatively was significantly lower than that of the control group (P = 0.014) (Table 3); however, there was no difference between the IAI and PAI groups (P = 0.922). The resting and motor NRSs 24 h after surgery and the maximum NRSs within 48 h after surgery were significantly lower in the IAI group than in the PAI and control groups, while there was no significant difference between the PAI and control groups. In addition, the NRS scores were similar among the three groups at the other time points.
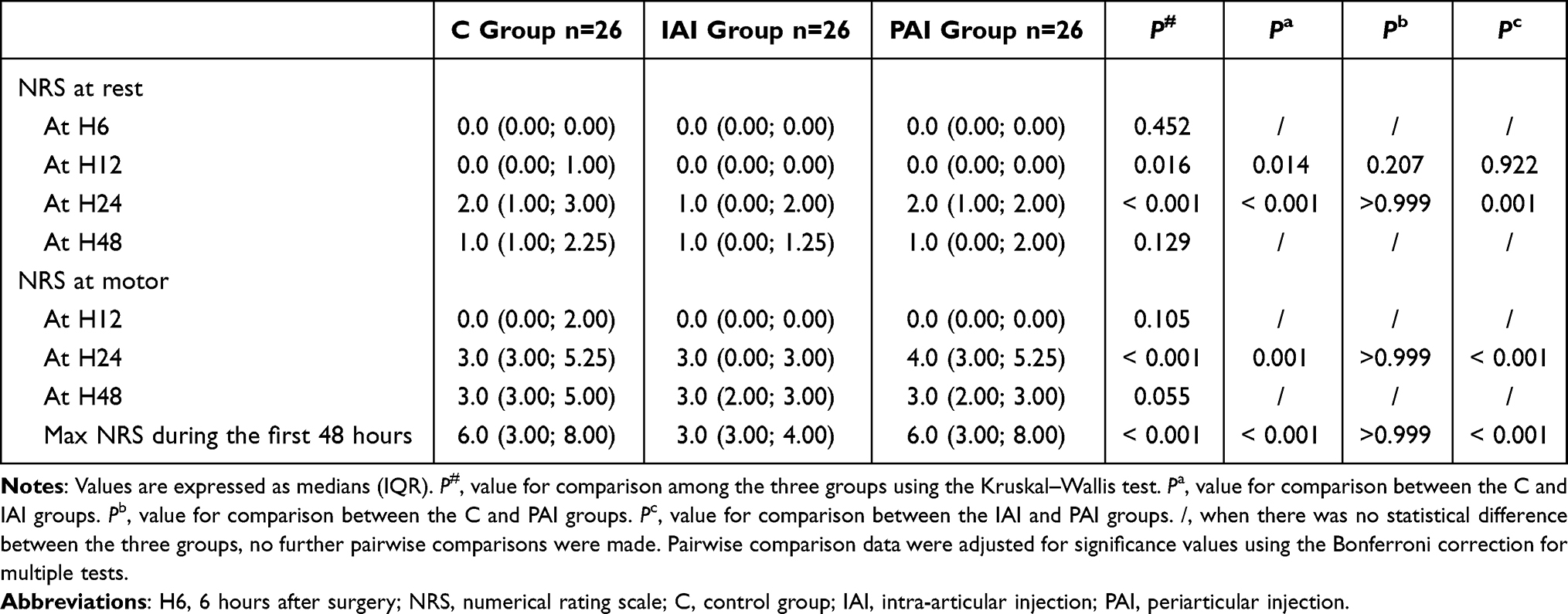 |
Table 3 Postoperative NRS Pain Score |
The incidences of POD and PONV were similar among the three groups (P = 0.610 and P = 0.264, respectively) (Table 4). None of the three groups reported the occurrence of common peroneal nerve injury, deep vein thrombosis, or falls after getting out of bed.
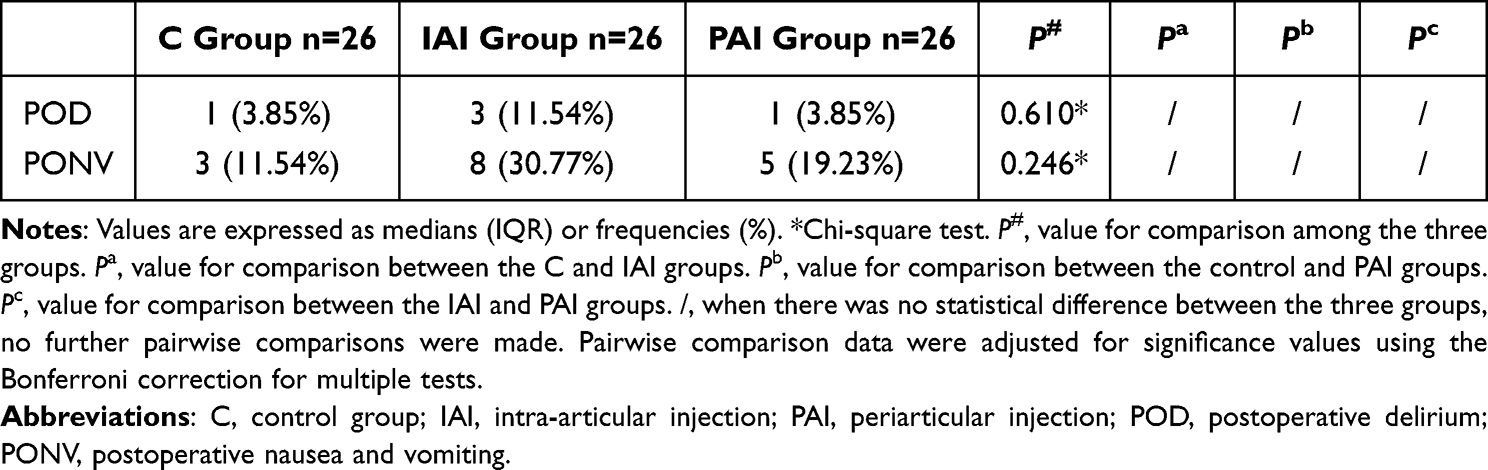 |
Table 4 Incidence of Adverse Events |
Discussions
Our study showed that a combination of FNB with PAI does not relieve postoperative pain better than FNB alone in TKA, and that a combination of FNB with IAI could provide stronger pain relief, prolong the time of first need for remedial analgesia postoperatively, reduce the demand rate of remedial analgesia and postoperative NRS score, facilitate patients to perform functional exercise early after surgery, enhance recovery after surgery (ERAS), and shorten LOHS.
Opinions on the comparison of analgesic effects of different local infiltration anesthetics in TKA remain inconsistent. A meta-analysis showed that PAI does not offer superior effects on pain control and discharge compared to IAI in TKA.18 A single-blinded prospective randomized study also found that intra-articular injections of bupivacaine and morphine were as effective as periarticular injections for postoperative analgesia in TKA.2 All of these studies acknowledged the effectiveness and feasibility of intra-articular infiltration for analgesia. Cheng et al concluded the opposite; they suggested that PAI has superior performance in pain relief and improvement of motion range compared to IAI.6 These adverse results may be related to the method of administration, type and dosage of medication, operative time, and patient status. Wang et al suggested that single-injection FNB provided effective analgesia, facilitated early ambulation, and reduced LOHS19 However, previous research has shown that FNB alone may not be sufficient to provide adequate analgesia.20 Some studies mentioned that both methods of LIA and FNB provide excellent pain relief.21,22 However, the current research on the combined application of LIA and FNB in TKA is limited. To this end, we compared two methods for combining LIA with FNB.
The main finding of our study was that IAI had a better analgesic effect than PAI, when combined with FNB. Because 69% of the patients treated with IAI and FNB did not require postoperative remedial analgesia and had a lower NRS 24 h after surgery and a lower maximum NRS at 48 h postoperatively. This is probably because the analgesic effect of incision-based peripheral infiltration anesthesia coincided with the femoral nerve block area, while intra-articular injection can play a good anesthetic effect on the intra-articular structure, which may well explain the advantages of intra-articular injection in postoperative pain control. Overall, IAI combined with FNB had a broader blocked range.
No patient required remedial analgesia in the PACU. This also suggests that FNB alone, even without combined IAI or PAI, can provide adequate short-term postoperative analgesia.
When Kaplan-Meier survival analysis was used to compare the duration of analgesia, there was no statistical difference between periarticular local infiltration combined with FNB and FNB alone (P = 0.483). We assumed that this inconsistency with the results of previous studies was due to the additional performance of FNB.2,6 The sensation at the incision site is innervated by the femoral nerve,23 and the analgesic effect of periarticular local infiltration is obscured by FNB. The effect of the LIA becomes apparent only when the analgesic effect of the femoral nerve block wears off. Further, it is also reported that periarticular infiltration anesthesia could provide a similar analgesic effect to FNB.22,24 The implementation of PAI consumes more time, while IAI is easy to operate and has no increased risks.6 First-time walking with a walker in the IAI group was much earlier than that of the rest of the participants (P < 0.001). This was because both the pain scores at 24 h postoperatively and the maximum pain scores in the first 48 h were lower in the IAI group than those in the other groups. Lower levels of postoperative pain and fewer postoperative remedial analgesic needs will prompt patients to resume exercise later in the post-operative period. The LOHS in the IAI group was lower than that in the control and PAI groups (P = 0.007). Considering these factors, we cannot conclude that IAI might be a better choice for postoperative analgesia and recovery than PAI.
Five participants developing POD (6.4%) were observed among the three groups, similar to the study by Wang et al,25 who observed 6–41% of total joint arthroplasty patients with delirium. PONV occurred in 16 patients. There was no statistically significant difference in the incidence of POD or PONV, which may be due to the small sample size.
This study has some limitations. First, the composition and capacity of the liquids used in LIA vary, and the location of the PAI varies in different countries and hospitals. Analgesic effects vary according to these factors. In our study, local infiltration was observed only using the usual administration method and drug composition at our hospital. Second, we only observed short-term effects. The trial would be more convincing if it included a measure of the long-term quality of life. In addition, the quality of postoperative rehabilitation was limited to pain score, first ambulation time, and LOHS. Postoperative rehabilitation indicators, such as joint range of motion, lower limb muscle weakness, and postoperative complications, were not evaluated in this study. These observations may help improve postoperative analgesia. Further studies should be conducted in the future.
Conclusion
When combined with FNB, IAI offers a superior analgesic effect and favorable recovery compared to PAI. Further studies are required to determine the differences in long-term quality of life.
Data Sharing Statement Indicating
The individual participant data will be available. The data specifically includes individual participant data that underlie the results reported in this article, after de-identification (text, tables, figures). No other documents will be available. Under reasonable requirements, the data of this study can be obtained from the corresponding author and the data will be available beginning 9 months and ending 36 months following article publication.
Acknowledgments
The research team greatly appreciated funding support and research participants for their cooperation and support.
Funding
This study was supported by the National Natural Science Foundation of China (No. 81870837).
Disclosure
None of the authors have any conflicts of interest to declare.
References
1. Jain RK, Porat MD, Klingenstein GG, Reid JJ, Post RE, Schoifet SD. The AAHKS clinical research award: liposomal bupivacaine and periarticular injection are not superior to single-shot intra-articular injection for pain control in total knee arthroplasty. J Arthroplasty. 2016;31(9 Suppl):22–25. doi:10.1016/j.arth.2016.03.036
2. Rice DA, Kluger MT, McNair PJ, et al. Persistent postoperative pain after total knee arthroplasty: a prospective cohort study of potential risk factors. Br J Anaesth. 2018;121(4):804–812. doi:10.1016/j.bja.2018.05.070
3. Kelley TC, Adams MJ, Mulliken BD, Dalury DF. Efficacy of multimodal perioperative analgesia protocol with periarticular medication injection in total knee arthroplasty: a randomized, double-blinded study. J Arthroplasty. 2013;28(8):1274–1277. doi:10.1016/j.arth.2013.03.008
4. Macrinici GI, Murphy C, Christman L, et al. Prospective, double-blind, randomized study to evaluate single-injection adductor canal nerve block versus femoral nerve block: postoperative functional outcomes after total knee arthroplasty. Reg Anesth Pain Med. 2017;42(1):10–16. doi:10.1097/AAP.0000000000000507
5. Wu CL, Naqibuddin M, Rowlingson AJ, Lietman SA, Jermyn RM, Fleisher LA. The effect of pain on health-related quality of life in the immediate postoperative period. Anesth Analg. 2003;97(4):1078–1085. doi:10.1213/01.ANE.0000081722.09164.D5
6. Cheng KY, Feng B, Peng HM, et al. The analgesic efficacy and safety of peri-articular injection versus intra-articular injection in one-stage bilateral total knee arthroplasty: a randomized controlled trial. BMC Anesthesiol. 2020;20(1):2. doi:10.1186/s12871-019-0922-4
7. Grosu I, Lavand’homme P, Thienpont E. Pain after knee arthroplasty: an unresolved issue. Knee Surg Sports Traumatol Arthrosc. 2014;22(8):1744–1758. doi:10.1007/s00167-013-2750-2
8. Kastelik J, Fuchs M, Kramer M, et al. Local infiltration anaesthesia versus sciatic nerve and adductor canal block for fast-track knee arthroplasty: a randomised controlled clinical trial. Eur J Anaesthesiol. 2019;36(4):255–263. doi:10.1097/EJA.0000000000000929
9. Lutzner J, Gehring R, Beyer F. Slightly better pain relief but more frequently motor blockade with combined nerve block analgesia compared to continuous intraarticular analgesia after total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. 2020;28(4):1169–1176. doi:10.1007/s00167-019-05843-2
10. Fowler SJ, Symons J, Sabato S, Myles PS. Epidural analgesia compared with peripheral nerve blockade after major knee surgery: a systematic review and meta-analysis of randomized trials. Br J Anaesth. 2008;100(2):154–164. doi:10.1093/bja/aem373
11. Grape S, Kirkham KR, Baeriswyl M, Albrecht E. The analgesic efficacy of sciatic nerve block in addition to femoral nerve block in patients undergoing total knee arthroplasty: a systematic review and meta-analysis. Aenaesthesia. 2016;71(10):1198–1209. doi:10.1111/anae.13568
12. Kinghorn K, Ellinas H, Barboi AC, Dolinski SY, Riou B. Case scenario: nerve injury after knee arthroplasty and sciatic nerve block. Anesthesiology. 2012;116(4):918–923. doi:10.1097/ALN.0b013e31824bdfab
13. Shah S, Hadzic A, Vloka JD, Cafferty MS, Moucha CS, Santos AC. Neurologic complication after anterior sciatic nerve block. Anesth Analg. 2005;100(5):1515–1517. doi:10.1213/01.ANE.0000150613.23987.92
14. Tanikawa H, Harato K, Ogawa R, et al. Local infiltration of analgesia and sciatic nerve block provide similar pain relief after total knee arthroplasty. J Orthop Surg Res. 2017;12(1):109. doi:10.1186/s13018-017-0616-x
15. Ranawat AS, Ranawat CS. Pain management and accelerated rehabilitation for total hip and total knee arthroplasty. J Arthroplasty. 2007;22(7 Suppl 3):12–15. doi:10.1016/j.arth.2007.05.040
16. Andersen LO, Kehlet H. Analgesic efficacy of local infiltration analgesia in hip and knee arthroplasty: a systematic review. Br J Anaesth. 2014;113(3):360–374. doi:10.1093/bja/aeu155
17. Parvataneni HK, Shah VP, Howard H, Cole N, Ranawat AS, Ranawat CS. Controlling pain after total hip and knee arthroplasty using a multimodal protocol with local periarticular injections: a prospective randomized study. J Arthroplasty. 2007;22(6 Suppl 2):33–38. doi:10.1016/j.arth.2007.03.034
18. Deng W, Chen J, Li Q, et al. Comparison of periarticular injection and intra-articular injection for pain management after total knee arthroplasty: a systematic review and meta-analysis. J Perianesth Nurs. 2021;36(4):406–412. doi:10.1016/j.jopan.2020.10.015
19. Chan EY, Fransen M, Parker DA, Assam PN, Chua N. Femoral nerve blocks for acute postoperative pain after knee replacement surgery. Cochrane Database Syst Rev. 2014;2014(5):CD009941. doi:10.1002/14651858.CD009941.pub2
20. Tierney E, Lewis G, Hurtig JB, Johnson D. Femoral nerve block with bupivacaine 0.25 per cent for postoperative analgesia after open knee surgery. Can J Anaesth. 1987;34(5):455–458. doi:10.1007/BF03014348
21. Albrecht E, Guyen O, Jacot-Guillarmod A, Kirkham KR. The analgesic efficacy of local infiltration analgesia vs femoral nerve block after total knee arthroplasty: a systematic review and meta-analysis. Br J Anaesth. 2016;116(5):597–609. doi:10.1093/bja/aew099
22. Moghtadaei M, Farahini H, Faiz SH, Mokarami F, Safari S. Pain management for total knee arthroplasty: single-injection femoral nerve block versus local infiltration analgesia. Iran Red Crescent Med J. 2014;16(1):e13247. doi:10.5812/ircmj.13247
23. Xu J, Chen XM, Ma CK, Wang XR. Peripheral nerve blocks for postoperative pain after major knee surgery. Cochrane Database Syst Rev. 2014;12:CD010937. doi:10.1002/14651858.CD010937.pub2
24. Fan L, Yu X, Zan P, Liu J, Ji T, Li G. Comparison of local infiltration analgesia with femoral nerve block for total knee arthroplasty: a prospective, randomized clinical trial. J Arthroplasty. 2016;31(6):1361–1365. doi:10.1016/j.arth.2015.12.028
25. Wang L, Seok S, Kim S, Kim K, Lee S, Lee K. The risk factors of postoperative delirium after total knee arthroplasty. J Knee Surg. 2017;30(6):600–605. doi:10.1055/s-0036-1593872
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Analgesic Efficacy of an Ultrasound-Guided Transversus Thoracis Plane Block Combined with an Intermediate Cervical Plexus Block on Postoperative Pain Relief After Trans-Areolar Endoscopic Thyroidectomy: A Single Center Prospective Randomized Controlled Study
Zhong R, Zou Y, Bao S, Chen Y, Huang G, Wang L, Chen L, Zhong M, Liang W
Journal of Pain Research 2023, 16:1059-1067
Published Date: 24 March 2023
Sufentanil Improves the Analgesia Effect of Continuous Femoral Nerve Block After Total Knee Arthroplasty

Dong J, Jin Z, Chen H, Bao N, Xia F
Journal of Pain Research 2023, 16:4209-4216
Published Date: 7 December 2023
S-Ketamine Reduces the Risk of Rebound Pain in Patients Following Total Knee Arthroplasty: A Randomized Controlled Trial
Li Q, Tian S, Zhang L, Chai D, Liu J, Sheng F, Jiang X, Feng W, Zhao Y, Zhu Y
Drug Design, Development and Therapy 2025, 19:2315-2327
Published Date: 27 March 2025
Noninferiority of 0.25% versus 0.375% Ropivacaine in Popliteal Sciatic and Saphenous Nerve Blocks for Analgesia After Foot and Ankle Surgery: A Randomized Self-Paired Noninferiority Trial
Wu L, Xi C, Lei G, Li H, Yin Y, Wan M, Wu H, Wang Y, Hu C, Wang G
Drug Design, Development and Therapy 2025, 19:4093-4104
Published Date: 19 May 2025
The Analgesic Efficacy of Liposomal Bupivacaine in Adductor Canal Block Following Knee Arthroplasty: A Single-Center, Prospective, Randomized and Controlled Clinical Trial
Xu M, Wang S, Meng Y, Gao C, Liu L, Yuan J, Ding S, Chai X, He K
Drug Design, Development and Therapy 2025, 19:7591-7601
Published Date: 2 September 2025