Back to Journals » Journal of Pain Research » Volume 19
Analgesic and Sedative Effects of Virtual Reality on Children with Acute Pulpitis: A Study Protocol for a Randomised Controlled Trial
Authors Cao W, Liu C, Yang Z, Wang Y, Dou J, Qiu X, Zhang L, Lv A, Tang L ![]()
Received 3 December 2025
Accepted for publication 27 March 2026
Published 14 April 2026 Volume 2026:19 586296
DOI https://doi.org/10.2147/JPR.S586296
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Helen Koechlin
Wenjuan Cao,1,* Chunpeng Liu,2,* Zaiyong Yang,3,* Yuchen Wang,2,4 Jiayi Dou,1,2 Xueling Qiu,2,5 Liting Zhang,2,6 Aiqin Lv,7 Lu Tang2
1School of Nursing, Shandong Second Medical University, Weifang, Shandong, People’s Republic of China; 2Department of Stomatology, 960th Hospital of the Chinese People’s Liberation Army, Jinan, Shandong, People’s Republic of China; 3Oral Medicine Teaching and Research Office, War Rescue Medical Department, Non-Commissioned Officer School, Army Medical University, Shijiazhuang, Hebei, People’s Republic of China; 4School of Nursing, Jinzhou Medical University, Jinzhou, Liaoning, People’s Republic of China; 5School of Nursing, Shandong First Medical University (Shandong Academy of Medical Sciences), Taian, Shandong, People’s Republic of China; 6School of Nursing, Shandong University of Traditional Chinese Medicine, Jinan, Shandong, People’s Republic of China; 7Department of Medical Services, Shandong University Stomatological Hospital, Jinan, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Aiqin Lv, Email [email protected] Lu Tang, Email [email protected]
Background: Root canal treatment is common in dentistry. Pulp exposure and drainage during the procedure cause significant discomfort in children, triggering fear and anxiety that reduce their physical comfort and treatment compliance. Virtual reality (VR) glasses divert patients’ attention from pain, alleviate anxiety, and feature simple operation and high safety. This study aims to investigate the safety and efficacy of virtual reality technology during pulp chamber open for drainage, providing empirical evidence for alleviating pain and reducing anxiety in pediatric patients undergoing the procedure.
Methods: This study is designed as a single-center, randomized, controlled trial. This study will recruit 100 patients aged 6 to 12 years undergoing pulp chamber open for drainage. Participants will be randomly assigned to either the intervention or control group in a 1:1 ratio. Data collectors will be blinded to the study. The experimental group will receive conventional local anesthesia combined with VR glasses, while the control group will receive conventional local anesthesia alone. Assessments will be conducted at baseline collection (in the dental chair) (T0), during local anesthesia (T1), at pulp exposure (T2), and immediately after treatment completion (T3). Primary outcomes are pain scores (Wong-Baker FACES Pain Scale) and anxiety scores (Visual Analog Scale for Anxiety). Secondary outcomes include treatment compliance (Frankl Behavior Rating Scale), physiological parameters, adverse effects, and physician-patient satisfaction and acceptance.
Trial Registration Number: ChiCTR2500111920.
Keywords: virtual reality, children, pulpitis, root canal treatment, pain, anxiety
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Zhao has been published for this article.
Introduction
Oral health is a universal concern that affects every individual worldwide. The World Health Organization’s 2025 Global Oral Health Status Report estimates that approximately 3.7 billion people worldwide suffer from oral diseases, including over 530 million children with primary tooth caries and as many as 2 billion individuals with permanent tooth caries.1 Primary tooth pulpitis is a highly prevalent oral disease among children. Failure to initiate standardized treatment promptly can adversely affect the normal replacement of primary teeth and the healthy development of permanent teeth. Currently, root canal therapy is the clinically recognized effective treatment for primary tooth pulpitis.2 However, its complex procedure, multiple required visits, and invasive steps involving pulp exposure and drainage often cause significant physical and psychological distress in children, triggering fear, anxiety, and even treatment resistance.3 Dental anxiety refers to the tension and fear children experience during dental procedures,4 with prevalence rates ranging from 5.7% to 46.8% across different pediatric populations. Dental fears unresolved during childhood often persist into adulthood, underscoring the critical importance of timely intervention.5 Even with local anesthesia, the pulp exposure and drainage process involves uncomfortable stimuli (eg., needles, drill sounds, stinging sensations) that exacerbate anxiety, reduce treatment compliance, and compromise oral health.6,7 Therefore, alleviating pain and anxiety in children undergoing pulp exposure and drainage is crucial for enhancing treatment compliance and improving quality of life.
Pain management strategies fall into pharmacological and non-pharmacological categories. Pharmacological approaches center on local anesthesia, with preoperative nerve block or infiltration anesthesia using lidocaine, bupivacaine, or other epinephrine-containing agents. Though these relieve procedural pain, individual anesthetic response variability means some pediatric patients may still experience pain.8 Inhaled nitrous oxide can supplement analgesia, yet excessive concentrations or improper oxygen-nitrogen ratios may cause dizziness and chest tightness, increasing risks for children with impaired respiratory function.9 For highly pain-sensitive children, oral NSAIDs or opioid analgesics may be used adjunctively, but these carry risks of drug dependence and adverse effects.10,11 Among non-pharmacological methods, the conventional “explanation-demonstration-procedure” approach has limited efficacy in younger or easily distracted children.12 Thus, there is an urgent need to develop novel, highly effective adjunctive analgesic strategies tailored to pediatric patients undergoing open pulp drainage.
VR is an emerging technology that immerses users in a computer-generated virtual 3D environment. Integrating head-mounted displays, motion sensors, headphones and joysticks, it stimulates users’ visual, auditory, proprioceptive and sometimes tactile/olfactory senses, replacing real-world sensory input.13 Due to its safety, simplicity and non-invasiveness,14,15 VR has been widely used in international clinical practice, including dental procedures such as pediatric deciduous tooth extraction, dental implant placement, supragingival scaling, special patient oral treatment, and periodontal scaling and root planing.16–20 Virtual reality achieves analgesia through distraction mechanisms by engaging the brain’s audiovisual information processing pathways with immersive 3D content, thereby reducing cognitive resources allocated to pain perception.13,14 However, the role of VR in root canal therapy, especially in pulp chamber open for drainage procedures, remains unknown for both adults and children, with no relevant reports in the current literature. Given these characteristics, VR appears to be a potential analgesic method for children undergoing access preparation for pulpitis.
This study hypothesized that VR would provide analgesic effects during open pulp chamber drainage procedures, as these procedures involve dental drills and pulp exposure, which can trigger intense somatosensory and emotional responses in children. The null hypothesis was that combining VR goggles with conventional local anesthesia would not significantly reduce pain or anxiety in pediatric patients undergoing such procedures, nor would it improve treatment compliance, compared to using conventional local anesthesia alone. Therefore, the primary objective of this study is to evaluate the safety and efficacy of VR-assisted interventions in these children, providing evidence-based support for optimizing pain and anxiety management during pediatric dental procedures.
Method
Study Design
This study protocol has been registered with the China Clinical Trial Registry (ChiCTR2500111920) and approved by the Ethics Committee at the 960th Hospital of the Chinese People’s Liberation Army (approval number: 2025–130), approval Date: 15/ 7/ 2025. The ethical approval of the present trial was based on the overall ethical evaluation of a larger research project that combines qualitative research and retrospective case studies to investigate the current status of pain control in pediatric acute pulpitis treatment, with the randomized controlled trial as a key component of this larger project. The study will be scheduled to commence in 25/ 2/ 2026. The trial protocol will be reported in accordance with the Standard Protocol Items Recommendations for Interventional Trials (SPIRIT 2025) (Supplementary S1 file). A single-center, randomized, controlled interventional study will be conducted to evaluate the efficacy and safety of using VR glasses for analgesia and sedation during pulp chamber open for drainage. Eligible participants will be randomly assigned in a 1:1 ratio to either the intervention group (conventional local anesthesia + VR glasses) or the control group (conventional local anesthesia). Table 1 summarises the schedule for enrolment, interventions and assessments. It is shown in Figure 1 for the entire study design.
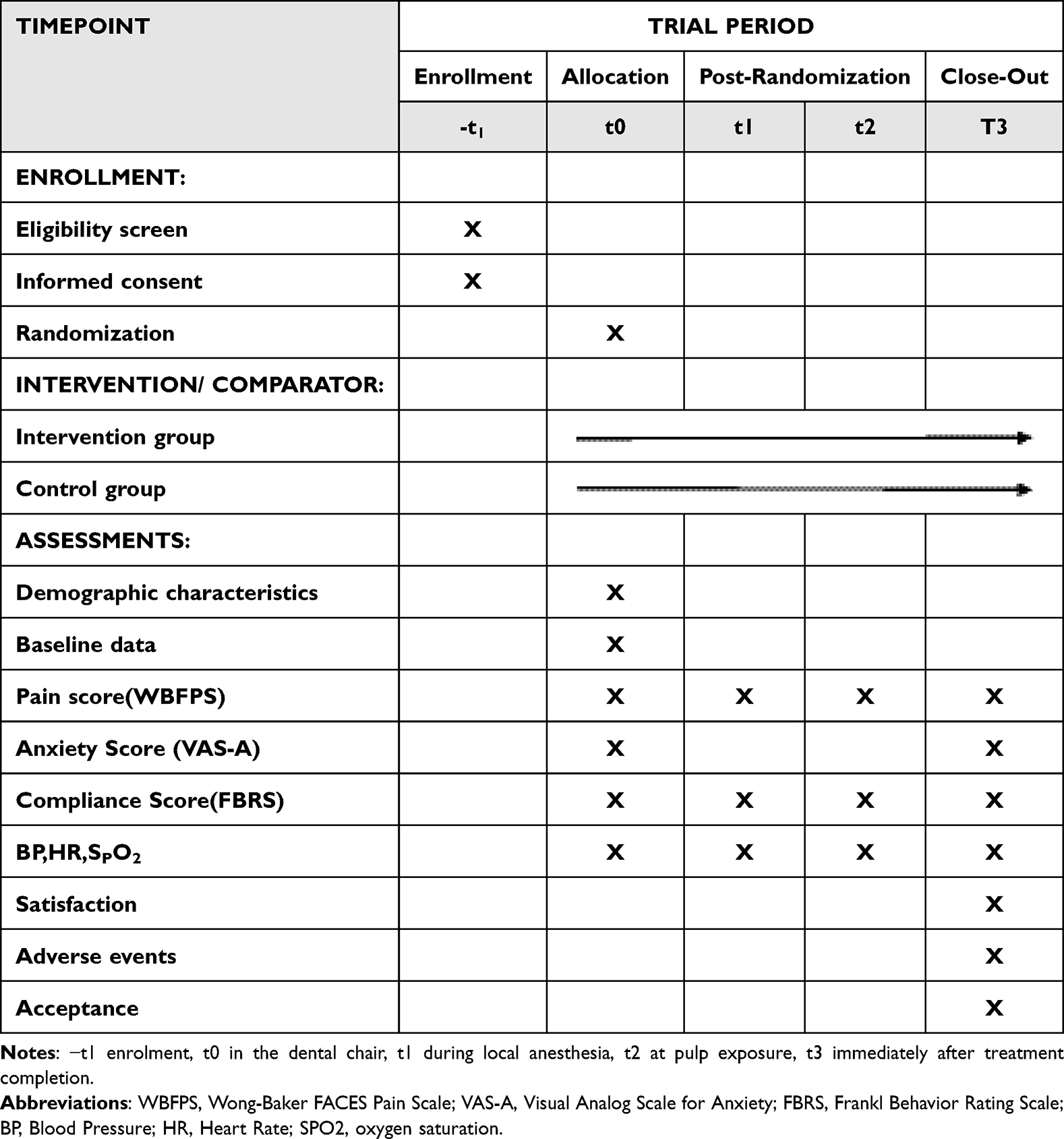 |
Table 1 SPIRIT Diagram of Enrolment, Interventions and Assessment for the Study |
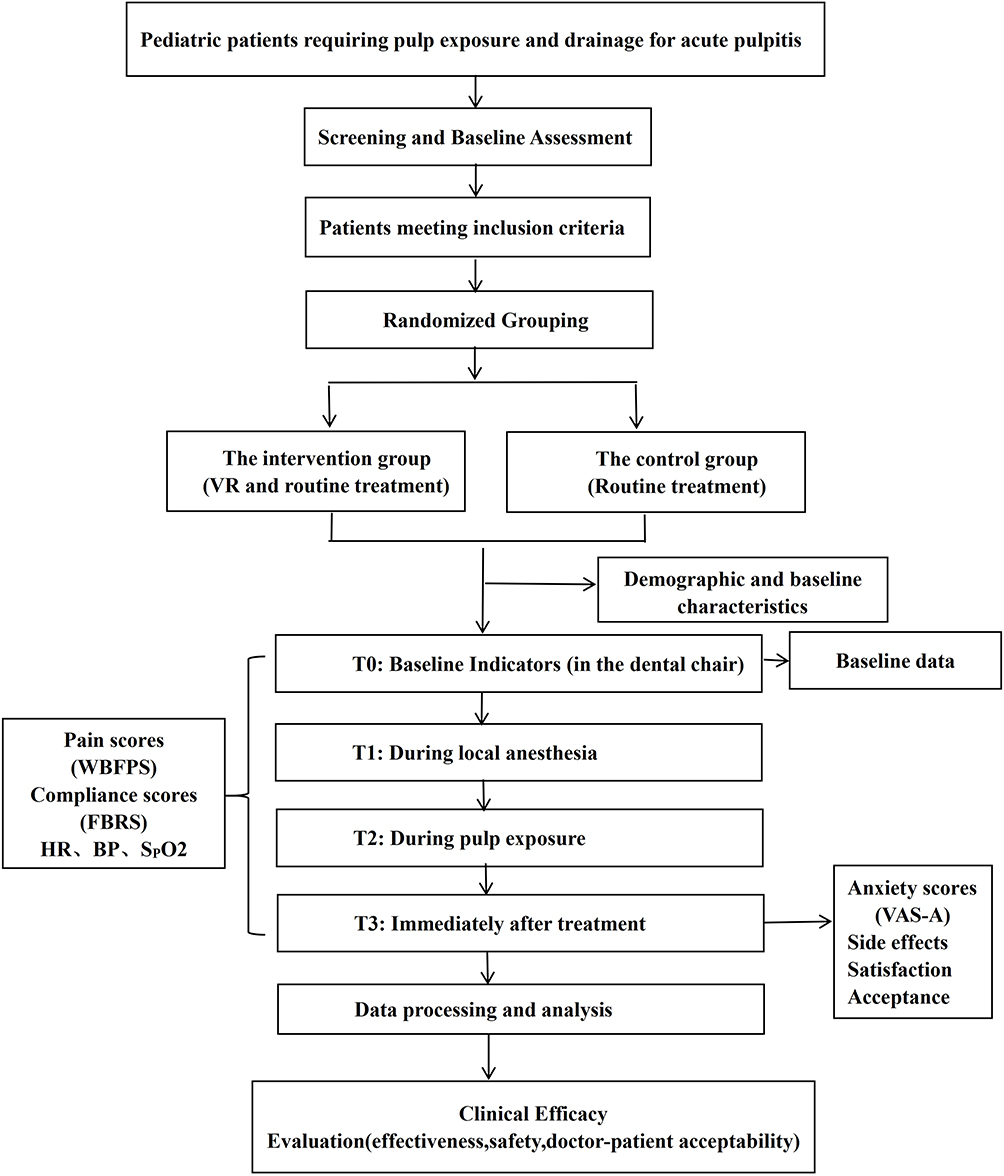 |
Figure 1 Research design roadmap. |
The trial has been officially recorded in the Chinese Clinical Trials Registry and will strictly comply with the ethical standards outlined in the Declaration of Helsinki, as well as the principles of Good Clinical Practice. The recruitment plan will be implemented at the Dental Clinic of the 960th Hospital of the Chinese People’s Liberation Army in February 2026. The trial will be conducted at the Pediatric Dentistry Department of the 960th Hospital of the Chinese People’s Liberation Army.
Eligibility Criteria
All pediatric patients aged 6–12 years requiring pulp chamber open drainage will be potential study participants. The research team will screen participants by reviewing medical records according to predefined inclusion and exclusion criteria and will design a specialized informed assent procedure tailored to children’s cognitive level. This procedure will be conducted in a quiet, non-intimidating setting at the initial visit, prior to any study-related operations. The research team, trained in pediatric communication, will first explain the study details to the children using simple, age-appropriate language (avoiding medical jargon), including the study purpose, key procedures (eg., wearing VR glasses, routine local anesthesia), potential slight discomfort, and the right to refuse or withdraw at any time. Sufficient time will be allocated for the children to ask questions, and responses will be provided truthfully and clearly.
Only after a child demonstrates understanding and willingness to participate will the research team inform the guardians of the details and obtain written informed consent. Written informed consent for all children aged 6–12 in this study will be signed by their legal guardians. The form confirms voluntary participation, permits regulated data disclosure, and ensures privacy protection. Free VR-assisted treatment will be provided by a professional team: root canal therapy will be performed by physicians with ≥2 years of experience, and VR operation will be managed by trained nurses.
The inclusion criteria for this trial will be established prior to the trial as follows: Age 6–12 years; Patients diagnosed by a pediatric dentist with acute pulpitis requiring pulp chamber open for drainage; No cognitive impairment and capable of independent expression; Participants with or without prior dental treatment history; Willingness to participate in the trial and signing of an informed consent form.
Exclusion criteria include: children or families who decline participation; patients with visual or auditory impairments; children with epilepsy or a history of seizures; individuals experiencing motion sickness from virtual reality imagery; patients with communication barriers preventing cooperation with VR equipment; children who have recently taken analgesic medications; and patients who withdraw from treatment during the study period. The primary inclusion and exclusion criteria for this study are shown in the table below. (Table 2)
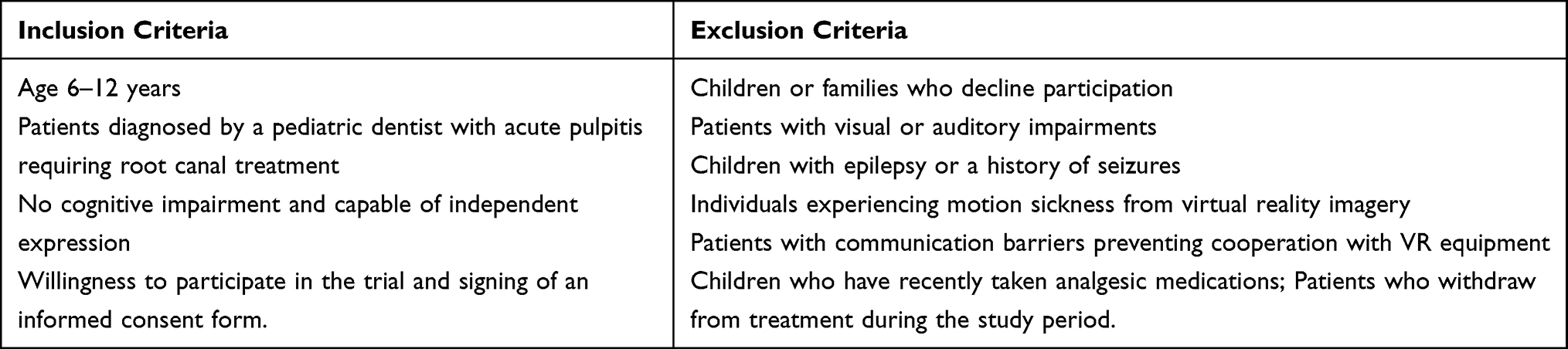 |
Table 2 Main Inclusion and Exclusion Criteria |
Intervention and Comparator
Participants in this trial will be randomly assigned to either the intervention group or the control group, and all trial procedures will be conducted in the Department of Pediatric Dentistry. In accordance with standard pediatric dentistry protocols, local infiltration anesthesia will be administered using articaine hydrochloride and epinephrine injection (containing 68 mg of articaine hydrochloride and 17 μg of epinephrine bitartrate per 1.7 mL). Prior to injection, aspiration is required to confirm no intravascular placement, and the injection rate must not exceed 1 mL per minute. The dentist will perform pulp exposure only after verifying the effectiveness of anesthesia via a pinprick test, and researchers will collect all observational indicators at four time points (T0, T1, T2, and T3).
Rokid Max AR Smart Glasses will be adopted for VR-assisted interventions in this study. All selected VR content will be non-violent, age-appropriate for 6–12 years old children, and sourced from popular animated series with positive themes. The research team will pre-screen the content to ensure it contains no scary or distressing elements. On the basis of receiving the same routine treatment as the control group, children in the intervention group will additionally receive complimentary VR-assisted therapy services: researchers will pre-download video content according to each child’s age and preferences, mainly including popular animated series such as “My Little Pony, SpongeBob SquarePants, and Doraemon.” After a child sits in the dental treatment chair and wears the glasses properly, the VR experience will be initiated immediately and will last throughout the entire diagnosis and treatment process. This VR intervention will adopt a passive immersive mode, which will not require children to make large-scale limb or head movements. The slight head movements made by children while watching VR content will not interfere with the normal conduct of diagnostic and therapeutic procedures.
During the use of VR glasses, researchers will closely monitor the children’s reactions and body postures, providing gentle guidance when necessary to maintain the standard operative posture. Throughout the entire process, the children’s blood pressure, heart rate, and blood oxygen saturation will be continuously monitored to ensure their safety. Upon the completion of diagnosis and treatment, researchers will assist the children in removing the VR glasses and promptly disinfect the devices with sterile wipes to prevent cross-infection.
Randomisation, Allocation Concealment and Blinding
To minimize selection bias, members of our research team will not participate in any other aspects of the study. All participants will complete a standardized baseline assessment using a uniform evaluation tool administered by researchers unaware of the study hypotheses. During the baseline assessment, the dental office will maintain a quiet environment with a distraction-free setting (eg., soft lighting, no exposure of sharp instruments) to minimize anxiety triggers.
Eligible patients will be randomly assigned in a 1:1 ratio to either the intervention group or the control group. The intervention group will receive VR intervention combined with conventional local anesthesia, while the control group will receive conventional local anesthesia alone. Patients participating in this experiment will be randomly assigned to the control or intervention group by a statistician using Microsoft Excel. The assignments will be confirmed and stored by an administrator not involved in the experiment. Prior to trial commencement, a series of sealed envelopes or containers will be prepared, each containing a card indicating the treatment assignment (“VR Analgesia Group” or “Control Group”). Upon meeting inclusion criteria and providing informed consent, the investigator randomly selected one numbered sealed envelope or container from the series. The patient’s treatment assignment will be determined based on the card’s content. The selection process must be conducted free from external interference, and the envelope or container is immediately destroyed afterward to ensure allocation concealment. Given the distinct visual characteristics and user experience of the VR glasses used in this study, which clearly differentiate them from the conventional control intervention, blinding of patients and researchers is not feasible.
Baseline Data
Demographic data (gender, age, height, weight, nationality, ethnicity, etc)., anxiety levels, pain levels, and treatment compliance scores will be recorded at baseline (T0, while seated on the dental chair) using internally designed forms. Physiological parameters such as blood pressure (BP), heart rate (HR), and oxygen saturation (SPO2) will also be measured at baseline.
Outcomes
Primary Outcome
The primary outcome measures will be pain and anxiety levels, assessed using the Wong-Baker FACES Pain Scale (WBFPS) and the Visual Analog Scale for Anxiety (VAS-A). Pain levels will be assessed at baseline collection (in the dental chair) (T0), during local anesthesia (T1), at pulp exposure (T2), and immediately after treatment completion (T3). Anxiety levels will be evaluated at T0 and T3. The WBFPS will be selected for its simplicity and intuitiveness, allowing rapid assessment of the child’s current facial expression. This scale comprises six distinct facial expressions, arranged from left to right to represent increasing pain intensity, ranging from happy to extremely sad. Each expression corresponds to a score from 0 to 10;21 0 = no pain, 2 = mild pain, 4 = moderate pain, 6 = moderately severe pain, 8 = severe pain, 10 = worst possible pain; validity confirmed in pediatric emergency and dental settings. VAS-A is a simple, sensitive, rapid, and reliable tool for assessing dental anxiety.22 The scale ranges from 0 to 10 points; 0 = no anxiety, 1–3 = mild anxiety, 4–6 = moderate anxiety, 7–10 = severe anxiety. Assessment time points: Pain levels (WBFPS) at T0, T1, T2, T3; anxiety levels (VAS-A) at T0 and T3.
Secondary Outcome
Secondary outcome measures include Frankl treatment compliance scores and physiological parameters at T0, T1, T2, and T3 to observe the effects of pain, anxiety, and intervention measures on patients’ physiological indicators;23 FBRS: 1 = definitely negative, 2 = negative, 3 = positive, 4 = definitely positive; Used to assess treatment compliance. The patient’s blood pressure, heart rate, and oxygen saturation will be monitored throughout the pulp chamber opening and drainage procedure and recorded at T0, T1, T2, and T3. During the procedure, if patients experience nausea, vomiting, dizziness, or headache, the VR device will be immediately removed, appropriate measures taken, and the incident promptly documented.At the conclusion of the procedure, patient and medical staff satisfaction (Satisfied = 1; Dissatisfied = 0) and acceptance will be assessed and documented. Finally, the total duration of the pulp chamber open for drainage surgery will be recorded.
Sample Size Estimate
In the protocol development stage, a senior statistician will conduct prospective sample size calculation via the GPower 3.1 software. The objective of this computation will be to identify the target sample size that will ensure 80% statistical power for two-tailed tests, with a Type I error rate (α) set at 5% for each measurement. Referring to a prior study investigating the impact of virtual reality on pain experienced by children during short-term dental treatments,24 a moderate effect size (Cohen’s d = 0.5) will be adopted as the expected effect size for this study. Based on this parameter, the initial estimated sample size per group will be determined to be 12 cases. To account for a potential 20% dropout rate, a total target sample size of 100 cases (50 cases per group) will be proposed, ensuring adequate statistical power to detect the expected intervention effect.
Data Management and Analysis
To ensure the security of research data and protect participant privacy, all relevant information will be managed under strict confidentiality protocols: All research-related materials (such as data collection forms) and electronic data will be archived in designated files and stored in encrypted format. Paper-based data must be placed in Ziploc sealable bags and securely archived in locked office drawers. Data entry will be conducted by two professionally trained researchers. Data loss prevention measures include daily inspections, validity checks, and creation of backup files (using the same backup method as source files). Throughout the study, participants’ personal data will be replaced with numerical codes and kept confidential at all times. Only the research project manager or designated physicians will have access to original personal information, further restricting access to safeguard privacy.
This study will employ SPSS 25.0 software (IBM Corporation, Armonk, NY, USA) for statistical analyses, with the initial quantitative evaluation following the intention-to-treat principle. The detailed analysis procedures are outlined below: For quantitative data, the statistician will compute the mean (standard deviation, SD), median (interquartile range, IQR), minimum value, maximum value, and proportion (95% confidence interval, 95% CI). For qualitative data, frequency and percentage will be used for descriptive presentation.
For intergroup comparisons, the appropriate statistical test will be selected based on the distribution characteristics of the mean anxiety and pain scores between the two patient groups: a t-test (parametric test) will be used if data are normally distributed, while a two-sample Mann–Whitney U-test (nonparametric test) will be employed if data are non-normally distributed. For vital signs during treatment (primarily blood pressure, heart rate, and oxygen saturation), repeated measures analysis of variance (ANOVA) will be performed. Patient satisfaction will be analyzed using the rank-sum test. We will perform Pearson or Spearman correlation analyses (based on data distribution) to explore the relationship between VR engagement (duration of immersion, reported enjoyment) and primary outcomes (pain/anxiety scores) in the intervention group. Additionally, the study will report adverse event rates and corresponding safety measures for each group, comparing differences between groups using the chi-square (χ2) test. In this study, a P value < 0.05 is defined as statistically significant.
Safety Assessment and Adverse Event Monitoring
Potential side effects encompass dizziness, headache, nausea, vomiting, and other forms of discomfort. All adverse reactions will be evaluated and recorded both during and following the procedure. If any of these occur, immediately remove the VR glasses and rest to alleviate symptoms. It is recommended that children become familiar with the VR equipment beforehand (eg., through a 5–10 minute preview session) to reduce anxiety or discomfort caused by unfamiliarity with the device.
Quality Control
Pain management specialists, dentists, nurses, and senior statisticians will jointly undertake the coordination and oversight of this study. To guarantee research quality, the project manager and team members will formulate detailed implementation schemes and contingency plans for unexpected situations before the official launch of the study. Throughout the trial, all research staff will receive standardized and targeted professional training to ensure the smooth and orderly progress of the study. Concurrently, the research funder will conduct regular audits to comprehensively verify the authenticity of data sources, accuracy of information, completeness of content, reliability of results, and security of storage.
Protocol Amendments
Any modifications to the protocol adopted in clinical trials must strictly comply with the relevant regulations and requirements for ethical review. Additionally, the roles and responsibilities of the ethics committee must be fully fulfilled to enhance the safety risk control of protocol changes during the clinical trial period.
Discussion
Maintaining oral health in early childhood is crucial for lifestyle and social development. Reports indicate that the prevalence of dental phobia among preschoolers, school-age children, and adolescents ranges from 13.3% to 36.5%.25 Compared to other children, those with higher levels of dental anxiety exhibit greater tooth decay rates and lower dental visitation rates, leading to reduced dental care-seeking behavior.26 Memories stemming from painful experiences and repeated similar encounters during past dental visits may exert an impact on future dental appointments. These recollections can linger into adolescence and adulthood, compromising oral and dental health. Moreover, childhood experiences involving intense anxiety, negative feelings, and pain are a key contributor to the emergence of dental anxiety.27,28 Therefore, it is reasonable to infer that effective pain management has the potential to enhance treatment satisfaction for both children and parents while simultaneously reducing the burden on healthcare providers.
VR constructs a computer-generated, adjusted three-dimensional (3D) setting and functions as an audiovisual distraction technique. It creates an immersive 3D realm that shields children’s vision and hearing throughout dental appointments. This virtual space engages and amuses them, diverting their attention from the dental office’s visual and auditory stimuli. As a result, it may alleviate pain and anxiety, rendering the dental experience more favorable.29 Multiple studies report that VR glasses, as a passive distraction tool, prove more effective than traditional strategies such as singing, watching television, controlled breathing, and relaxation techniques.30 Currently, virtual reality is not only employed in pediatric dental procedures such as primary tooth extraction, teeth cleaning, and dental examinations,16–20 but also widely applied in other clinical settings including burn care, oncology care, and venous access.31 VR exerts effective analgesic effects in various fields and is an effective, relatively safe adjunct in pediatric dentistry. It needs no specialized team support and is easily operable by dental nurses; adverse reactions are extremely rare and mild, with nausea only seen when combined with opioid analgesics, not when used alone or with other distraction techniques.32,33
This study is the first randomized controlled trial in China to date that evaluates the safety, analgesic, and sedative effects of VR in pediatric patients undergoing pulp opening and drainage, and it will fill the gap in clinical evidence for non-pharmacological pain management in pediatric dentistry. The VR intervention is safe and child-friendly, serving as a non-pharmacological, non-invasive approach that avoids medication-related risks while being simple to operate and standardized for nursing implementation. This solution demonstrates strong clinical feasibility for widespread adoption, requiring no complex supporting infrastructure and adapting to routine pediatric clinical settings. If proven effective, it will become a safer, more convenient adjunctive solution for alleviating pain and anxiety during pediatric dental procedures, offering a new, easily disseminated option for pediatric dental pain management.
Limitation
This study has certain limitations: its single-center design aimed to ensure standardization of VR intervention and assessment procedures, minimize inter-institutional operational bias, and serve as an exploratory trial to validate the feasibility of the research protocol, laying the groundwork for subsequent multicenter studies. However, the demographic characteristics of participants may be relatively homogeneous, necessitating cautious interpretation when extrapolating findings to other populations or clinical settings. Although pain and anxiety scores are subjective measures, standardized and validated scales were used for consistent assessment across all participants to mitigate potential bias. Nevertheless, significant individual differences exist in how children of varying ages perceive and express pain and anxiety, which may introduce subtle variations in outcome measurement that should be considered when interpreting the results.
Conclusion
If effective, VR can serve as a non-pharmacological, child-friendly adjunct to alleviate pain and anxiety in children undergoing pulp drainage, improve treatment compliance, and reduce the development of dental phobia. Future studies should be conducted in multi-center settings to further explore the efficacy of VR in pediatric patients of different age groups, as well as its long-term impacts on children’s dental care-seeking behaviors.
Abbreviations
WBFPS Wong-Baker FACES Pain Scale, VAS-A Visual Analog Scale for Anxiety, FBRS Frankl Behavior Rating Scale, BP Blood Pressure, HR Heart Rate, SPO2 oxygen saturation, −t1 enrolment, t0 in the dental chair, t1 during local anesthesia, t2 at pulp exposure, t3 immediately after treatment completion.
Data Sharing Statement
Data and materials are available from the corresponding author Lu Tang (Email: [email protected]) upon reasonable request.
Ethics Approval and Informed Consent
This protocol has been approved by the Ethics Committee (2025-130). A brief description of the study protocol and the informed consent form are available in the supplementary file (S2 File). Participants’ rights and safety will be protected through full compliance with the Declaration of Helsinki and Good Clinical Practice (GCP) guidelines. Written informed consent will be obtained from participants. Appropriate measures will be taken to ensure the confidentiality of data collected in this study.
Consent for Publication
All authors granted permission for the material to be published.
Acknowledgments
We appreciate all the authors of included studies.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study did not receive external funding.
Disclosure
The authors declare no competing interests in this work.
References
1. World Health Organization, 2025. Oral health, 2025. Available from: https://www.who.int/news-room/fact-sheets/detail/oral-health.
2. León-López M, Cabanillas-Balsera D, Martín-González J, Montero-Miralles P, Saúco-Márquez JJ, Segura-Egea JJ. Prevalence of root canal treatment worldwide: a systematic review and meta-analysis. Int Endodontic J. 2022;55:1105–11. doi:10.1111/iej.13822
3. Zhou XW, Wang LX, Liu XY. Clinical trail on the effect of nitrous oxide/oxygen inhalation sedation on the treatment of acute pulpitis. Shanghai J Stomatol. 2013;22:702.
4. Berggren U, Meynert G. Dental fear and avoidance: causes, symp⁃ toms, and consequences. J Am Dent Assoc. 1984;109(247):251. doi:10.14219/jada.archive.1984.0328
5. Alsadat FA, El-Housseiny AA, Alamoudi NM, Elderwi DA, Ainosa AM, Dardeer FM. Dental fear in primary school children and its relation to dental caries. Niger J Clin Pract. 2018;21:1454–1460. doi:10.4103/njcp.njcp_160_18
6. Hmud R, J WL. Dental anxiety: causes, complications and management approaches. J Minim Interv Dent. 2009;2:67–78.
7. Razavian H, Mazaheri M, Shiri A. Effect of lavender oral drops in reducing dental anxiety among patients requiring endodontic treatment: a randomised clinical trial. Eur Endod J. 2025;10:66–72. doi:10.14744/eej.2024.06641
8. Zhao JJ, Cui J. The role of nurses in pain management. Chin J Nurs. 2009;44:383–384.
9. Miroshnychenko A, Ibrahim S, Azab M, et al. Injectable and topical local anesthetics for acute dental pain: 2 systematic reviews. J Am Dent Assoc. 2023;53–64.e14. doi:10.1016/j.adaj.2022.10.014
10. Stanley W, Drum M, Nusstein J, Reader A, Beck M. Effect of nitrous oxide on the efficacy of the inferior alveolar nerve block in patients with symptomatic irreversible pulpitis. J Endod. 2012;38:5659. doi:10.1016/j.joen.2012.02.010
11. Lader M. Benzodiazepine harm: how can it be reduced? Br J Clin Pharmacol. 2014;77:295–301. doi:10.1111/j.1365-2125.2012.04418.x
12. Yazar M, Aydınoğlu S, Günaçar DN. Are technological contributions in behavior guidance techniques superior to conventional methods?: effects on dental anxiety and pain perception. BMC Oral Health. 2025;25:735. doi:10.1186/s12903-025-06139-3
13. Barros Padilha DX, Veiga NJ, Mello-Moura ACV, Nunes Correia P. Virtual reality and behaviour management in paediatric dentistry: a systematic review. BMC Oral Health. 2023;23:995. doi:10.1186/s12903-023-03595-7
14. Indovina P, Barone D, Gallo L, et al. Virtual reality as a distraction intervention to relieve pain and distress during medical procedures:a comprehensive literature review. Clin J Pain. 2018;34:858–8774. doi:10.1097/ajp.0000000000000599
15. De Rooij IJ, Van de Port IG, Meijer JG. Effect of virtual reality training on balance and gait ability in patients with stroke: sys tematic review and meta- analysis. Phys Ther. 2016;96:1905–1918. doi:10.2522/ptj.20160054
16. Du Q, Ma X, Wang S, et al. A digital intervention using virtual reality helmets to reduce dental anxiety of children under local anesthesia and primary teeth extraction: a randomized clinical trial. Brain Behav. 2022;12:e2600. doi:10.1002/brb3.2600
17. Ghobadi A, Moradpoor H, Sharini H, Khazaie H, Moradpoor P. The effect of virtual reality on reducing patients’ anxiety and pain during dental implant surgery. BMC Oral Health. 2024;24:186. doi:10.1186/s12903-024-03904-8
18. Yi X, Mao J. Effect of virtual reality technology applied to ultrasonic supragingival scaling on patient pain. General Nursing. 2019;17:3428–3430.
19. Al Kheraif AA, Adam TR, Wasi A, Alhassoun RK, Haddadi RM, Alnamlah M. Impact of virtual reality intervention on anxiety and level of cooperation in children and adolescents with autism spectrum disorder during the dental examination. J Clin Med. 2024;13:6093. doi:10.3390/jcm13206093
20. Hoffman HG, Garcia-Palacios A, Patterson DR, Jensen M, Furness T, Ammons WF. The effectiveness of virtual reality for dental pain control: a case study. Cyberpsychol Behav. 2001;4:527–535. doi:10.1089/109493101750527088
21. Garra G, Singer AJ, Taira BR, et al. Validation of the Wong-Baker FACES pain rating scale in pediatric emergency department patients. Acad Emerg Med. 2010;17:50–54. doi:10.1111/j.1553-2712.2009.00620.x
22. Facco E, Zanette G, Favero L, et al. Toward the validation of visual analogue scale for anxiety. Anesth Prog. 2011;58:8–13. doi:10.2344/0003-3006-58.1.8
23. Frankl SN. Should the parent remain with the child in the dental operatory. J Dentistry Child. 1962;(2):150–163.
24. Ran L, Zhao N, Fan L, Zhou P, Zhang C, Yu C. Application of virtual reality on non-drug behavioral management of short-term dental procedure in children. Trials. 2021;22:562. doi:10.1186/s13063-021-05540-x
25. Grisolia BM, Dos Santos APP, Dhyppolito IM, Buchanan H, Hill K, Oliveira BH. Prevalence of dental anxiety in children and adolescents globally: a systematic review with meta-analyses. Int J Paediatr Dent. 2021;31:168–183. doi:10.1111/ipd.12712
26. Prado IM, Carcavalli L, Abreu LG, Serra-Negra JM, Paiva SM, Martins CC. Use of distraction techniques for the management of anxiety and fear in paediatric dental practice: a systematic review of randomized controlled trials. Int J Paediatr Dent. 2019;29:650–668. doi:10.1111/ipd.12499
27. Bagattoni S, Nascimben F, Biondi E, et al. Preparing children for their first dental visit: a guide for parents. Healthcare. 2022;10:2321. doi:10.3390/healthcare10112321
28. Ram D, Shapira J, Holan G, Magora F, Cohen S, Davidovich E. Audiovisual video eyeglass distraction during dental treatment in children. Quintessence Int. 2010;41:673–679.
29. Garrocho-Rangel A, Ibarra-Gutiérrez E, Rosales-Bérber M, Esquivel-Hernández R, Esparza-Villalpando V, Pozos-Guillén A. A video eyeglasses/earphones system as distracting method during dental treatment in children: a crossover randomised and controlled clinical trial.Eur. J Paediatr Dent. 2018;19:74–79. doi:10.23804/ejpd.2018.19.01.14
30. Delgado A, Ok SM, Ho D, Lynd T, Cheon K. Evaluation of children’s pain expression and behavior using audio visual distraction. Clin Exp Dent Res. 2021;7(12021):795–802. doi:10.1002/cre2.407
31. Eijlers R, Utens EMWJ, Staals LM, et al. Systematic review and meta-analysis of virtual reality in pediatrics:effects on pain and anxiety. Anesth Analg. 2019;129:1344–1353. doi:10.1213/ANE.0000000000004165
32. Sharar SR, Carrougher GJ, Nakamura D, Hoffman HG, Blough DK, Patterson DR. Factors influenc⁃ ing the efficacy of virtual reality distraction analgesia during postburn physical therapy:preliminary results from 3 ongoing studies. Arc Phys Med Rehabil. 2007;88:S43–S49. doi:10.1016/j.apmr.2007.09.004
33. Schmitt YS, Hoffman HG, Blough DK, et al. A randomized, con ⁃ trolled trial of immersive virtual reality analgesia, during physi ⁃ cal therapy for pediatric burns. Burns. 2011;37:61–68.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.