Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 12
An Update on the Prevention and Management of Bronchopulmonary Dysplasia
Authors Hennelly M, Greenberg RG, Aleem S
Received 24 May 2021
Accepted for publication 23 July 2021
Published 11 August 2021 Volume 2021:12 Pages 405—419
DOI https://doi.org/10.2147/PHMT.S287693
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Roosy Aulakh
Marissa Hennelly,1 Rachel G Greenberg,1,2 Samia Aleem1,2
1Department of Pediatrics, Duke University, Durham, NC, USA; 2Duke Clinical Research Institute, Durham, NC, USA
Correspondence: Rachel G Greenberg
Department of Pediatrics, Duke University, 300 W. Morgan St, Suite 800, Durham, NC, 27701, USA
Tel +1 919-668-4725
Email [email protected]
Abstract: Bronchopulmonary dysplasia (BPD) is a common morbidity affecting preterm infants and is associated with substantial long-term disabilities. There has been no change in the incidence of BPD over the past 20 years, despite improvements in survival and other outcomes. The preterm lung is vulnerable to injuries occurring as a result of invasive ventilation, hyperoxia, and infections that contribute to the development of BPD. Clinicians caring for infants in the neonatal intensive care unit use multiple therapies for the prevention and management of BPD. Non-invasive ventilation strategies and surfactant administration via thin catheters are treatment approaches that aim to avoid volutrauma and barotrauma to the preterm developing lung. Identifying high-risk infants to receive postnatal corticosteroids and undergo patent ductus arteriosus closure may help to individualize care and promote improved lung outcomes. In infants with established BPD, outpatient management is complex and requires coordination from several specialists and therapists. However, most current therapies used to prevent and manage BPD lack solid evidence to support their effectiveness. Further research is needed with appropriately defined outcomes to develop effective therapies and impact the incidence of BPD.
Keywords: bronchopulmonary dysplasia, neonate, preterm infant, chronic lung disease
Introduction
Bronchopulmonary dysplasia (BPD) is a syndrome of aberrant alveolar and vascular development of the lungs resulting in impaired gas exchange.1,2 Infants with BPD often have substantial long-term respiratory and neurodevelopmental morbidities, in addition to increased likelihood of re-hospitalization, asthma, and chest wall deformities.3–9 BPD is a common morbidity in preterm infants; and depending on which definition is used (Table 1), the incidence ranges from 32% to 59%.10 Even though the incidence of other neonatal morbidities has decreased in recent years, the incidence of BPD has been relatively unchanged.3 While this is in part a reflection of improved survival of infants predisposed for developing BPD, there is also limited evidence suggesting the effectiveness of current preventive interventions.2,4,10,11 Most pharmacologic agents that are prescribed in an effort to prevent BPD are also used for the management of established BPD.11 In this review, we summarize current evidence behind strategies used for the prevention and management of BPD (Table 2), and the evolving research of new therapeutic targets.
 |
Table 1 Definitions of Bronchopulmonary Dysplasia (BPD) |
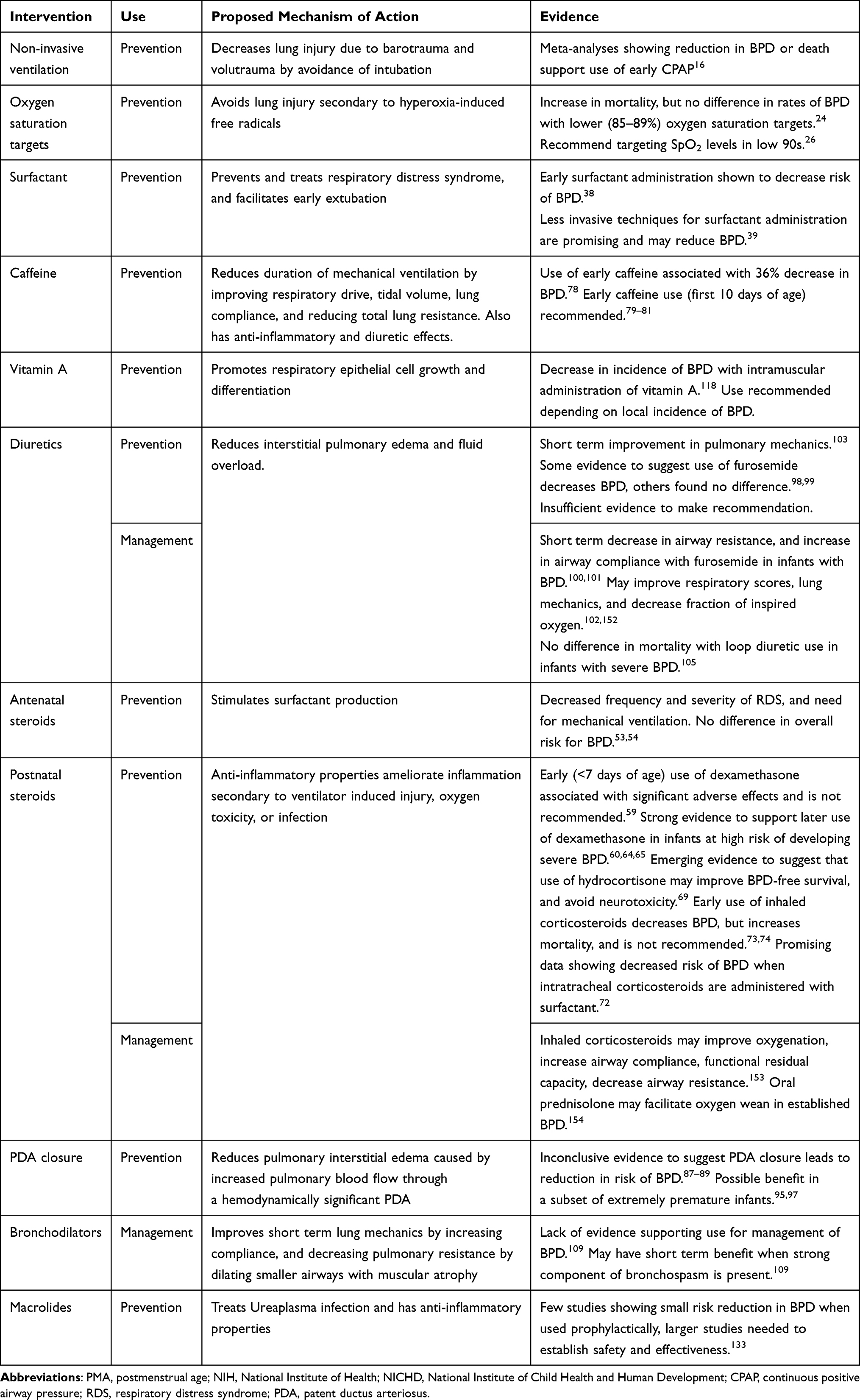 |
Table 2 Summary of Interventions for the Prevention and Management of Bronchopulmonary Dysplasia (BPD) |
Lung Protective Ventilation Strategies
Mechanical ventilation via an endotracheal tube exposes the developing lung to volutrauma and barotrauma. These insults contribute to lung fibrosis and inflammation, which are both important factors in the development of BPD.12 Non-invasive management strategies, in which infants receive respiratory support without the need for an endotracheal tube, have been studied as a strategy to avoid direct trauma to the developing lung, and potentially reduce the risk of developing BPD.13–15
Delivery Room Stabilization
Three of the largest randomized controlled trials (RCTs) that compared delivery room stabilization with early nasal continuous positive airway pressure (CPAP) to intubation and surfactant found a small, but non-statistically significant reduction in the rates of death or BPD at 36 weeks postmenstrual age (PMA).13–15 The Surfactant, Positive Pressure, and Pulse Oximetry Randomized Trial was a multicenter RCT that examined early treatment with CPAP compared to early intubation, followed by surfactant administration within one hour of birth in 1316 extremely low birth weight (ELBW) infants.13 The study found no significant difference between the two groups in the rate of death or BPD, both when analyzed with the physiological definition of BPD (p=0.59) and when defined by the need for supplemental oxygen at 36 weeks PMA (p=0.53). The study also found that when compared to the surfactant group, the CPAP group had lower prevalence of corticosteroid use for treatment of BPD (p<0.001), fewer days of ventilation (p=0.03), and greater survival free of mechanical ventilation at day 7 (p=0.01).13 Similarly, the Continuous Positive Airway Pressure or Intubation at Birth trial compared nasal CPAP with intubation and ventilation at 5 minutes after birth in 610 ELBW infants, and found no statistically significant reduction in the rate of death or BPD.14 Finally, the Vermont Oxford Network DRM Study Group compared three study groups: prophylactic surfactant treatment followed by brief mechanical ventilation, prophylactic surfactant followed by rapid extubation to nasal CPAP, and CPAP with selective surfactant treatment.15 The study found no statistically significant difference in death or BPD between the groups.15 A Cochrane meta-analysis comparing prophylactic CPAP with intubation and mechanical ventilation noted a small but significant reduction in the incidence of BPD at 36 weeks [relative risk (RR) 0.89, 95% confidence interval (CI) 0.79–0.99].16 Based on current evidence, delivery room stabilization with CPAP in spontaneously breathing ELBW infants results in improved short-term outcomes, but a reduction in BPD has not been seen consistently.
Non-Invasive Ventilation
Other studies have compared the effectiveness of various techniques of non-invasive ventilator support in reducing BPD. Nasal intermittent positive pressure ventilation (NIPPV) is a form of non-invasive ventilation that delivers a baseline distending pressure similar to CPAP, but with the addition of superimposed peak inspiratory pressures at intervals.17 A Cochrane analysis of ten studies including 1061 infants comparing early NIPPV and early CPAP use determined that even though infants randomized to early NIPPV had reduced risk of requiring intubation (RR 0.78 CI 0.64–0.94) and respiratory failure (RR 0.65 CI 0.51–0.82), there was no reduction in the risk of BPD among infants who received NIPPV.18 Another meta-analysis of the use of NIPPV versus CPAP in preterm infants after extubation found a reduction in BPD associated with synchronized NIPPV (RR 0.64, 95% CI 0.44–0.95) on subgroup analysis, but in the overall cohort no difference was found in the rates of BPD between the two groups (RR 0.94, 95% CI 0.80–1.10).19
High Frequency Ventilation
The use of high-frequency ventilation has been proposed as a way to prevent ventilator associated lung injury, but the evidence is scarce. In centers reporting high survival rates of infants born at <23 weeks gestation, first-intention high-frequency ventilation is used as a method to limit barotrauma and volutrauma.20 An RCT of 797 infants born 23–28 weeks gestation that randomized infants to either high-frequency oscillatory ventilation or conventional ventilation, found no significant difference in the outcome of death or BPD between the two groups.21 A Cochrane review of 19 studies including 4096 infants explored high frequency oscillatory ventilation compared with conventional ventilation on the incidence of BPD. The meta-analysis found a small but inconsistent reduction in the risk of BPD with the use of high frequency oscillatory ventilation compared with conventional ventilation.22 Advantages of high-frequency ventilation over conventional ventilation have not been clearly demonstrated.
Oxygen Saturation Targets
Exposure to supraphysiological oxygen has been associated with BPD, thus defining optimal oxygen saturation targets has been well studied. Infants born at <30 weeks randomized to high-saturation target (95–98%) have a significantly higher risk of needing supplemental oxygen at 36 weeks compared to infants randomized to 92–94% [odds ratio (OR) 1.40, 95% CI 1.15–1.70].23 An individual patient meta-analysis of the five RCTs of the Neonatal Oxygen Prospective Meta-Analysis (NeOProM) Collaboration examined restricted (85–89%) versus liberal (91–95%) oxygen saturation targets in infants less than 28 weeks gestation, and found no significant difference in the composite outcome of death or major neurodevelopmental outcomes, or severe visual problems at 18–24 months between the two groups (RR 1.04, 95% CI 0.98–1.09).24 Significantly fewer infants in the restricted oxygen saturation target group received supplemental oxygen at 36 weeks PMA (RR 0.81, 95% CI 0.74–0.90) but there was also an increase in the risk of death (RR 1.17, 95% CI 1.04–1.31) and NEC (RR 1.33, 95% CI 1.10–1.61) in this group.25 While further studies are needed to make definitive conclusions, some authors suggest maintaining oxygen saturation targets between 88% and 92%, and a higher alarm limit of 96%.26
Surfactant Administration
Endogenous surfactant production by type II pneumocytes begins at approximately 20 weeks gestation, and is insufficient in infants born prematurely.27 This deficiency of surfactant leads to respiratory distress syndrome (RDS), characterized by increased surface tension and a reduction in pulmonary compliance.28,29 Exogenous surfactant replacement therapy decreases surface tension within the alveoli, improves ease of inflation of the lung, thereby treating RDS.30–32 Early studies done prior to the routine use of antenatal corticosteroids, found that exogenous surfactant administration reduced mortality and BPD.31–35 However, subsequent meta-analyses have failed to show exogenous surfactant leading to a consistent reduction in BPD.36–37 Timing of surfactant administration appears to play a role in the development of BPD. A Cochrane analysis of six RCTs that compared early surfactant administration with delayed in infants with RDS concluded that early administration of surfactant was associated with a decreased the risk of BPD.38
While surfactant has multiple benefits, its administration traditionally involves intubation with subsequent mechanical ventilation, which can lead to ventilator-associated lung injury and higher risk for BPD. The INSURE (Intubation Surfactant Extubation) technique of surfactant administration by transient intubation, surfactant administration, and immediate extubation has allowed for a method of medication delivery that may mitigate lung trauma associated with prolonged ventilation.39 A systematic review and meta-analysis of nine trials (1551 infants) comparing INSURE with CPAP found no statistically significant difference between the two, though the RR favors INSURE in regard to reduction in BPD and death in BPD (RR 0.88, 95% CI 0.76–1.02), with a 14% decrease in BPD.39 Existing data suggests that the INSURE method is not universally successful in all preterm infants with RDS, with failure rates ranging from 19% to 49%.40,41 A possible cause of failure of INSURE is the inability of preterm lung with RDS to maintain adequate functional residual capacity that would allow for equal and homogenous exogenous surfactant distribution.42 In an effort to overcome this, the IN-REC-SURE (INtubate, RECruit-SURfactant-Extubate) trial was recently published which compared surfactant administration after alveoli recruitment using high frequency oscillatory ventilation, followed by extubation with the traditional INSURE method in preterm infants who failed nasal CPAP.42 Although there was a reduced requirement for mechanical ventilation during the first 72 hours of age in the IN-REC-SUR-E (40%) group compared to the IN-SUR-E (54%) group (p=0.037), no difference was found between the two groups in the incidence of moderate to severe BPD.43 The decreased need for mechanical ventilation is promising, but adequately powered studies are needed to determine any benefits for BPD.
As a way to circumvent the need for mechanical ventilation entirely, administration of surfactant via a thin catheter has been evaluated.44 A RCT of 200 infants less than 36 weeks gestation compared surfactant administration through tracheal instillation of a catheter during CPAP in a method called the Take Care technique. When compared with INSURE, the authors found a significantly lower rate of mechanical ventilation and BPD.45 Less invasive surfactant therapies (LIST) through a thin tracheal catheter were compared to standard administration of surfactant through an endotracheal tube in a meta-analysis of six RCTs. LIST was found to be associated with decreased risk of BPD (RR 0.71, 95% CI 0.52–0.99), BPD or death (RR 0.74, 95% CI 0.58–0.94), and need for invasive ventilation (RR 0.67, 95% CI 0.53–0.84).46 The role of aerosolized surfactant has also been evaluated as a less invasive alternate route of surfactant administration. A recent RCT of 457 infants born between 23 and 41 weeks gestation found that infants who received aerosolized surfactant within the first 12 hours of age were less likely to require later intubation and surfactant administration.47 In a recent meta-analysis comparing various non-invasive ventilation strategies (including INSURE, LISA, and nebulized surfactant), the use of LISA was associated with the lowest likelihood of BPD at 36 weeks PMA [OR 0.53, 95% credible interval (CrI) 0.27–0.96].48 While the combination of less invasive surfactant delivery and non-invasive ventilation may be beneficial in treating RDS and reducing the need for mechanical ventilation, more robust data is needed to establish the effect on BPD.
Synthetic Surfactant
A wide variety of surfactant preparations have been developed, including synthetic surfactant, which may contain protein or be protein-free; and animal-derived surfactant that is derived from both porcine or bovine sources.49 Animal-derived surfactant is not only expensive to produce, but is also in limited supply, thus leading to the development of synthetic preparations.50 Comparisons of animal-derived surfactant with early generations of synthetic surfactant found a shorter duration of invasive ventilation, quicker weaning off of respiratory support, and decreased mortality with animal-derived preparations.49 A later meta-analysis comparing animal-derived surfactant with protein-free synthetic surfactant found no effect of surfactant preparation on the risk of BPD at 36 weeks adjusted age (RR 0.99, 95% CI 0.91–1.09), or the composite outcome of BPD or death (RR 0.97, 95% CI 0.90–1.04).49 A recent randomized trial comparing poractant alfa (porcine surfactant) with the synthetic surfactant CHF5633 (first fully synthetic surfactant enriched with surfactant proteins, SP-B and SP-C peptide analogues) found no difference in BPD between the two preparations (RR 1.03, 95% CI 0.81–1.32), and otherwise had a similar safety and efficacy profile.51 Thus, while newer generations of protein-containing surfactant preparations may be used in place animal-derived preparations, they have not shown additional benefit in prevention of BPD.
Corticosteroids
Antenatal Corticosteroids
Antenatal corticosteroids are routinely administered to mothers at risk for preterm delivery for its known benefit in lung maturation and decreasing RDS in the newborn.11,52 In a recent Cochrane review of 1368 infants analyzing the effect of antenatal corticosteroids on the development of BPD there was a reported decrease in the need for mechanical ventilation (RR 0.68, CI 0.56 to 0.84) and moderate/severe RDS (RR 0.59, 95% CI 0.38–0.91).53 Despite this, six of the studies examining antenatal corticosteroid use and BPD found inconclusive evidence of antenatal corticosteroids and the development of BPD (RR 0.86, 95% CI 0.42 to 1.79).53 Other observational studies have found that a full course of antenatal steroids was associated with a small but statistically significant reduction in the composite outcome of BPD or death in lower gestational age infants.54–56 Thus, while a universal decrease in BPD has not been established, antenatal steroids reduce the severity of RDS and other serious morbidities (including death and longer term neurodevelopmental impairment), and may also have a role in reducing BPD in the lowest gestational age group of infants.54,56
Postnatal Systemic Corticosteroids
Corticosteroids are commonly used as a component of BPD prevention and management due to their anti-inflammatory effects.44 However, clinicians considering use of corticosteroids, particularly dexamethasone, must weigh benefit to the lung against established side effects that include increased risk for neurodevelopmental impairment, intestinal perforation and impaired growth.11,57 In 2002, concerns about these risks led to a statement by American Academy of Pediatrics Committee on the Fetus and Newborn recommending against the use of systemic dexamethasone in the prevention or treatment of BPD in very low birth weight (VLBW) infants.58
The side effect profile is especially pronounced when systemic dexamethasone is used early after birth.59 The most recent Cochrane review examining the use of early (<8 days) systemic corticosteroids in the prevention of BPD found improvement in the rates of BPD and a composite of BPD and death.59 The review also noted an increase in the risk of adverse effects including intestinal perforation, hypertrophic cardiomyopathy, cerebral palsy, and major neurosensory disability. Given this side effect profile, early dexamethasone use for prevention of BPD is not recommended.59 An alternate strategy is to administer postnatal steroids in ventilator-dependent infants, who are at highest risk of developing BPD.60 This was initially studied in the Dexamethasone: A Randomized Trial study, which included 70 infants who were ventilator dependent after the first week of age. This study found that treatment with dexamethasone improved ventilator and oxygen requirements, and decreased duration of intubation. However, there was no effect seen at later mortality (OR 0.52, 95% CI: 0.14–1.95; p=0.33) or rates of BPD (OR 0.58, 95% CI 0.08–0.32, p=0.71).61 A subsequent Cochrane review of late (>7 days) corticosteroids of 21 RCTs reported improvement in development of BPD, but with increased short-term side effects and a trend towards cerebral palsy.62 In another meta-analysis of 47 RCTs including 6747 infants treatment with high and low-dose dexamethasone was associated with decreased risk of BPD (high dose OR 0.11, 95% CrI 0.02–0.4; low dose OR 0.37 CrI 0.16–0.67).63 A recent systematic review and meta-analysis suggests that moderately early initiated (8–14 days of age) systemic dexamethasone at a medium cumulative dose of 2–4 mg/kg may be the most appropriate regimen for preventing BPD.64 An important consideration is the association of neurodevelopmental impairment with BPD itself, and factoring in individual patient risks and benefits.60 In infants with >60% risk for BPD, postnatal steroids reduce the risk of death and cerebral palsy, thus it is reasonable to administer steroids to such infants.60 Administration between weeks 2–7 of age may minimize the risk of severe BPD in infants with evolving lung disease, with the lowest unadjusted rate of severe BPD seen with administration at 22–28 days (Table 2).60,65
As an alternate strategy without the neurotoxic risk profile, hydrocortisone has been evaluated for its efficacy in prevention of BPD.66 In an RCT of low-dose hydrocortisone for ELBW infants requiring mechanical ventilation, rates of survival without BPD were similar between the groups, however, there was improved survival without BPD among chorioamnionitis exposed infants.67 This study was stopped early due to concern for increased spontaneous gastrointestinal perforation in the hydrocortisone group, with a heightened effect among infants treated with hydrocortisone and indomethacin.67 Thereafter, the PREMILOC study of infants born between 24 and 27 weeks gestation randomized to low-dose hydrocortisone or placebo for the first 10 days of age, found that the hydrocortisone group had significantly improved survival without BPD at 36 weeks (p=0.04). This particular study did not show any increased rate of gastrointestinal perforation between the two groups, but did note a nearly twofold increase in the rate of late-onset sepsis in infants between 24 and 25 weeks gestation who received hydrocortisone.68 A recent individual patient meta-analysis including 4 studies and 982 infants examined low-dose hydrocortisone used as prophylaxis for adrenal insufficiency, and found that treatment with low-dose hydrocortisone for 10–15 days significantly increased survival without BPD (p=0.007).69 The study also found increased risk for gastrointestinal perforation when indomethacin and hydrocortisone were used (p=0.004), and increased incidence of late onset sepsis (p=0.04).69 The recently published STOP-BPD study that randomized 372 infants to receive either a 22-day course of systemic hydrocortisone or placebo found no difference in the rates of death or BPD (aOR 0.87, 95% CI 0.54–1.38).70 With conflicting data, further studies regarding the dosage, safety, efficacy and long-term effects of hydrocortisone are needed.
Inhaled Corticosteroids
Inhaled corticosteroids have been an area of interest for management of BPD, as the targeted delivery allows for the anti-inflammatory benefit in the lungs without the systemic side effects.57 Small studies have found short-term benefits in oxygenation with inhaled corticosteroids in infants with BPD, but no long-term effect.71 Others have evaluated treatment with budesonide and surfactant compared to surfactant alone in management of infants at high risk for BPD, who required mechanical ventilation.72 There was a significantly lower incidence of BPD or death in the group managed with budesonide (p<0.001), with no increase in adverse events between the two groups.72 The NEUROSIS trial that randomized infants to either inhaled budesonide or placebo until they no longer required supplemental oxygen and positive pressure ventilation found a statistically significant decrease in BPD (RR 0.74, 95% CI 0.60–0.91), although an increase in mortality was seen at 36 weeks PMA (RR 1.24, 95% CI 0.91–1.69) and at 2 years (RR 1.37, 95% CI 1.01–1.86).73,74 There are other trials currently ongoing examining intratracheal budesonide, including the PLUSS trial and others.75–77
Caffeine
Caffeine is used routinely for the treatment of apnea of prematurity, and is one of the few drugs known to reduce the risk of BPD at 36 weeks PMA.78 The Caffeine for Apnea of Prematurity Trial examined 2006 infants with birth weights between 500 and 1250 g, who were randomly assigned to either the caffeine or placebo. It was found that treatment with caffeine led to a 36% decrease in BPD (aOR 0.63, p<0.001).78 Infants treated with caffeine also had earlier successful extubations (median PMA of 29.1 weeks vs 30.0 weeks, p<0.001), discontinuation of positive airway pressure (31.0 weeks vs 32.0 weeks, p<0.001), and were weaned to room air earlier (33.6 weeks vs 35.1 weeks, p<0.001).78 A post hoc analysis of this trial found a greater reduction in the duration of respiratory support among infants who received early caffeine therapy (<3 days of age), compared to later on (>3 days).79
Other studies have evaluated the timing of caffeine initiation and the effect on BPD. A retrospective data analysis of 2951 infants found that early initiation of caffeine (0–2 days) compared with delayed initiation (3–10 days) was associated with reduction in BPD (OR 0.69, p<0.001) or BPD and death (OR 0.77, p=0.01).80 The initiation of early (<3 days of age) compared to late (≥ to 3 days of age) caffeine therapy was studied in a retrospective cohort study of 140 infants with birth weight less than 1250g.81 The study demonstrated improved outcomes with early caffeine therapy, with 25% of infants who received early caffeine developing the outcome of death or BPD compared to 53% of infants in the late caffeine group (aOR 0.26, p<0.01).81 Another retrospective cohort study of 5517 infants born less than 31 weeks’ gestation examined early (<3 days) compared to late (≥ 3 days) caffeine administration. Again, this study showed decreased odds of development of the outcome of death or BPD in the early caffeine group (aOR 0.81).82 Current evidence thus supports the use of caffeine, especially when initiated within the first 10 days of age, as one of the few pharmacological therapies proven to prevent the development of BPD (Table 2).
Patent Ductus Arteriosus (PDA) Closure
Left-to-right shunting across a PDA can lead to increased pulmonary congestion and worsen pulmonary edema resulting in impaired alveolar development and increased need for mechanical ventilation.83 Observational studies have shown an association between the presence of PDA and development of BPD in premature infants, but this does not necessarily imply causation.84–86 Multiple RCTs designed to evaluate pharmacological ductal closure have failed to show a reduction in risk of BPD.87–89
A randomized controlled non-inferiority trial examining ibuprofen treatment compared with non-intervention for PDA closure found that the non-intervention group was not inferior to the treatment group with regards to the incidence of BPD or death (non-inferiority margin −0.2, p=0.51). This may in part due to the low efficacy of ibuprofen closure particularly in infants born at 23–26 weeks.90 Another study evaluating PDA closure with either indomethacin or surgical ligation compared to non-intervention found lower rates of BPD in the non-intervention group (p<0.05) and no statistically significant difference in mortality and morbidities including necrotizing enterocolitis (NEC), intraventricular hemorrhage, and periventricular leukomalacia.91 It is important to note that most modern day RCTs have been designed to determine the efficacy of several pharmacologic therapies to close the PDA, and may be underpowered in estimating the impact on preventing BPD.92 A recent meta-analysis of RCTs and observational studies found no difference in the morbidities or mortality related to various medical treatment options (ibuprofen, indomethacin, acetaminophen) for PDA closure.93
Other studies have investigated the timing of PDA closure and its effect on BPD. The PDA-TOLERATE Trial compared early with later conservative pharmacologic treatment of moderate-to-large PDA.94 In infants who had ongoing respiratory support needs and had a moderate-to-large PDA, there was a higher incidence of BPD in those intubated >10 days (75%) compared to infants intubated <10 days (27%, p<0.0001). However, among the infants intubated greater than 10 days, prolonged exposure to moderate-to-large PDA was associated with increased risk of BPD (p=0.04). These findings suggest that an increased risk of BPD among infants with exposure to moderate-to-large PDA and receiving prolonged mechanical ventilation >10 days.94
With the lack of conclusive evidence surrounding PDA closure to prevent BPD, and adverse effects of all available management strategies, there is an increase in a more conservative approach of “watchful waiting” across centers.95 A threshold of 7–13 days of exposure to a moderate to severe PDA has been found to lead to a significant increase in the incidence of BPD or death (OR 2.12, 95% CI 1.04–4.32) in infants <28 weeks gestation.96 These data suggest that while expectant management may be prudent in a majority of cases, there is likely a subset of infants who benefit from PDA closure, such as those who are extremely premature (in whom spontaneous closure is delayed)97 or those with hemodynamically significant PDAs.95
Diuretics
In premature infants, clinicians often use diuretics with the goal of decreasing pulmonary edema and the amount of respiratory support needed, thereby improving risk factors leading to the development of BPD. In a large retrospective cohort study of 37,693 infants born at 23–29 weeks gestational age and who were exposed to diuretics between postnatal day 7 and 36, an increase in the number of days of furosemide therapy by 10% was associated with decreased incidence of BPD (4.6%, p=0.001) and BPD or death (3.7%, p=0.01).98 In this study, 51% of all extremely preterm infants were treated with furosemide during hospitalization.98 However, in 835 infants in the Prematurity and Respiratory Outcomes Program observational cohort, no temporal association between administration of diuretics and change in respiratory status was noted between diuretic exposed and unexposed infants.99
Diuretics are also commonly used in the management of established BPD. In small studies, diuretics have been shown to improve pulmonary mechanics by increasing airway compliance and decreasing airway resistance in infants with BPD.100–102 A Cochrane review aimed to evaluate loop diuretic use in infants with or developing BPD. The review included six RCTs involving diuretic use in infants less than 37 weeks gestation with either oxygen or ventilator dependency beyond five days of age. The review found a decreased risk of failure to extubate within a week of furosemide usage and improvement in pulmonary compliance with a one-to-two-day course of furosemide. Overall, the authors concluded there was not enough evidence to recommend loop diuretics in patients with or developing BPD.103 There is currently no standard practice in the chronic diuretic treatment of ELBW infants with a diagnosis of BPD, and nearly 20% of infants discharged home are treated with diuretics.104 There is also significant variability in loop diuretic use, suspected to be due to a lack of consensus in evidence-based practice.105 A retrospective cohort study of 3252 infants less than 32 weeks gestation with severe BPD examined between-center variation in loop diuretic use for treatment of bronchopulmonary dysplasia, with an adjusted mean range of 7.3–49.4% of days.105 The study found similar mortality rates at high-use centers compared with low-use centers (aOR 0.98, p=0.98), and similar discharge age between both the low-use and high-use centers (47.3 weeks vs 47.4 weeks, p=0.96).105 The variation in use across centers, and conflicting evidence regarding long-term benefits, coupled with side effects of chronic diuretic use, highlight the need for future studies designed to understand which infants are best suited for diuretic therapy.
Bronchodilators
Inhaled bronchodilators, such as albuterol and ipratropium, are used in the management of bronchospasm associated with established BPD.106 Their use may be beneficial in managing acute symptoms by decreasing airway resistance and increasing lung compliance following administration.107,108 However, randomized trials have not shown any benefit in the management or improvement in the severity of BPD.109 Despite this, nearly half of hospitalized infants with severe BPD are prescribed bronchodilators, with exposure higher in infants with more serious illness, and varying greatly across hospitals (0–59%).110 This marked variability in inhaled bronchodilator use in the absence of supporting evidence demonstrates a need for future studies in this population.
Nutritional Interventions
Intrauterine growth and postnatal nutrition management play a critical role in the development and management of BPD in extremely premature infants. Small for gestational age (SGA) preterm infants have higher rates of adverse pulmonary outcomes when compared with those grown appropriately.111 A case-control study of 2255 infants born before 33 weeks gestation found SGA infants have higher risk of later development of BPD, indicating that growth restriction may be a risk factor.111 Furthermore, infants with established BPD have been shown to have postnatal growth failure as a result of their higher energy expenditures, and potentially as a side effects of medications used for treatment.112,113 Optimizing nutrition has been recognized as an area for both prevention and treatment of BPD.
Breast milk is well known for its protective effect against NEC, and has also been studied for its role in preventing BPD.114–116 In a multicenter cohort study of 1587 preterm infants who received an exclusively human breast milk-based diet, the incidence of BPD was significantly lower compared to infants who received either preterm formula or maternal breast milk with bovine fortifier (56.3% vs 47.7%, p = 0.0015).116 A pooled meta-analysis of eight observational studies showed a BPD protective effect of donor human milk compared to formula when used as supplement to mother’s own milk (RR 0.78, 95% CI 0.67–0.90).116 However, meta-analysis of three RCTs found no statistically significant difference in BPD between infants receiving donor human milk compared to preterm formula when mother’s own milk was unavailable (RR 0.89, 95% CI 0.60–1.32).115
Vitamin A
Vitamin A is involved in lung growth and the development of the epithelial cells of the respiratory tract, making it an attractive agent for supplementation.117 A Cochrane review of eleven trials found a small benefit in the risk of BPD at 36 weeks PMA with intramuscular vitamin A supplementation in VLBW infants.118 During a vitamin A shortage in the United States, a large observational study found similar rates of BPD in infants who received vitamin A, compared to those who did not.119 Given these data, and the need for frequent intramuscular administration, vitamin A is not being universally administered. As an exploration for alternate routes of administration, a recent RCT of 188 infants born less than 28 weeks gestation evaluated enterally administered vitamin A compared to intramuscular. While it was found that following enteral treatment plasma retinol levels increased, there was no improvement in severity of BPD.120 The ongoing NeoVitA trial is a multicenter, double-blind RCT comparing high-dose oral vitamin A vs placebo. The study aims to evaluate the effect of enteral vitamin A supplementation on the outcome of BPD or death in ELBW infants.121 The results of this study will further guide the efficacy of oral vitamin A use.
Infants with BPD have increased energy requirements as compared to those without.122 It has been estimated that infants with BPD have 15–25% increased energy expenditure compared to controls.122 A Cochrane analysis to evaluate the effects of increased energy intake compared to standard intake on infants with BPD could not identify any eligible trials.123 Increased protein and calorie intake is needed to meet the metabolic needs of these infants, and many require up to 30 calorie fortified breast milk or formulas to achieve intakes of >130 kCal/kg/day.124–126 Along with enriched formula, calcium, phosphorous, zinc and other micronutrients and vitamins help infants with BPD to have improved lung growth and bone mass.127 Ultimately, the nutritional management post-hospital discharge requires an interdisciplinary team approach.
Infection Prevention and Antibiotic Stewardship
Multiple infectious organisms have been implicated in the development of BPD.128–131 Ureaplasma is one such organism, and given the anti-inflammatory properties of macrolides used to treat Ureaplasma, they have been proposed as a potential therapy for both prevention and management of BPD.132 A meta-analysis evaluating the use of prophylactic azithromycin therapy for BPD in 3 small trials found a small reduction in BPD (RR 0.83, 95% CI 0.71–0.91).133 However, a more recent RCT of a three-day course of IV azithromycin therapy in infants born 24–28 weeks gestation demonstrated that although this treatment regimen is effective in eradication of respiratory tract Ureaplasma colonization, there was no difference in the incidence of BPD between the two groups.134 Some centers report screening extremely premature infants for Ureaplasma soon after birth, and selectively treating those infants requiring prolonged mechanical ventilation with azithromycin.135 Larger trials are needed to establish the safety and effectiveness of prophylactic azithromycin, and must balance out the risk of BPD associated with antibiotic use.
Nosocomial infections contribute to BPD, likely related to persistent inflammatory mediators that contribute to the development of BPD.136 A retrospective cohort study using the California Perinatal Quality Care Collaborative database noted that nosocomial infection significantly increased the risk of BPD (OR 2.74, 95% CI 2.54–2.94).137 The study also found that as the rates of nosocomial infection decreased from 24.7% to 15% as a result of quality improvement efforts, the rates of BPD decreased by 8%.137 This is of particular importance because antibiotics used to treat infections may in fact increase the risk of developing BPD. In ELBW infants, early empiric antibiotic therapy of 4–7 days is associated with increased adjusted odds of BPD, and each additional day of antibiotics in the first 2 weeks of age significantly increases the risk of severe BPD (OR 1.15, 95% CI 1.08–1.27).138,139 Other studies have found an association between total antibiotic exposure in the neonatal intensive care unit and an increased risk for BPD.140 Ultimately, prevention of nosocomial infections by implementation of strict hand hygiene policies and central-line care bundles are identifiable strategies to reduce the component of increasing BPD risk caused by infection and antibiotic exposure.
Emerging Areas of Research
Stem Cells
Mesenchymal stem cells (MSCs) have emerged as a potential new therapeutic target in both the prevention and treatment in BPD. In animal models, treatment with MSCs was shown to reverse alveolar injury and improve lung functioning.141 These results have motivated research evaluating the safety of MSC treatment in humans. Placental derived human amnion epithelial cells (hAECs) infusion was evaluated for safety in a small scale first in human study. The authors determined that hAECs were safe and well tolerated by their study population.142 Results from a recently concluded Phase II trial demonstrated safety and feasibility of MSCs in preterm infants between 23 and 28 weeks gestation, although it was underpowered to detect therapeutic efficacy towards preventing BPD, and larger clinical trials are underway.143 MSC-derived extracellular vesicles have pro-regenerative and immune modulating effects and have been shown to improve lung morphology, pulmonary function and suppress inflammation in animal models.144 While these findings are promising, their clinical implications are yet to be established.
IGF-1
Insulin-like growth factor (IGF-1) is a growth factor involved in vascular development.11 IGF-1 levels typically rise in the third trimester and are important in tissue growth. IGF-1 levels are lower in infants born prematurely than those age matched fetal in utero levels due to loss of maternal source of IGF-1 and postnatal factors such as poor nutrition which account for a slow rise in IGF-1 following delivery. It has been shown that in infants who develop BPD, these low serum IGF-1 levels are persistent after birth. This identifies IGF-1 as a potential therapeutic target for BPD through improving vascular development.145
Conclusion
While there has been tremendous progress in the understanding of the pathophysiology and progression of BPD, its prevention and management continue to be major challenges for neonatologists, especially with the increasing survival of extremely premature infants. Strategies that are theoretically effective have failed to translate to clinical settings. Most strategies to prevent and treat BPD lack evidence and have long-term adverse effects. Additionally, none of the current medications in practice are labeled by the US Food and Drug Administration to prevent or treat BPD in infants, and yet are being used widely. There is continued need for future meta-analyses and prospective randomized controlled studies designed to measure clinically meaningful outcomes, and an even greater need to design trials evaluating the safety, efficacy, and dosing of pharmacologic agents in this population.
Funding
No funding was secured for this study.
Disclosure
Dr Rachel G Greenberg is a consultant for Tellus Therapeutics, outside the submitted work. The authors have no other conflicts of interest to disclose in this work.
References
1. Northway WH
2. Thébaud B, Goss KN, Laughon M, et al. Bronchopulmonary dysplasia. Nat Rev Dis Primers. 2019;5(1):78.
3. Stoll BJ, Hansen NI, Bell EF, et al. Trends in care practices, morbidity, and mortality of extremely preterm neonates, 1993–2012. JAMA. 2015;314(10):1039–1051.
4. Schmidt B, Roberts RS, Davis PG, et al. Prediction of late death or disability at age 5 years using a count of 3 neonatal morbidities in very low birth weight infants. J Pediatr. 2015;167(5):982–986e982.
5. Vohr BR, Wright LL, Dusick AM, et al. Neurodevelopmental and functional outcomes of extremely low birth weight infants in the National Institute of Child Health and Human Development Neonatal Research Network, 1993-1994. Pediatrics. 2000;105(6):1216–1226.
6. Natarajan G, Pappas A, Shankaran S, et al. Outcomes of extremely low birth weight infants with bronchopulmonary dysplasia: impact of the physiologic definition. Early Hum Dev. 2012;88(7):509–515.
7. Keller RL, Feng R, DeMauro SB, et al. Bronchopulmonary dysplasia and perinatal characteristics predict 1-year respiratory outcomes in newborns born at extremely low gestational age: a prospective cohort study. J Pediatr. 2017;187(89–97):e83.
8. Greenough A, Cox S, Alexander J, et al. Health care utilisation of infants with chronic lung disease, related to hospitalisation for RSV infection. Arch Dis Child. 2001;85(6):463–468.
9. Fawke J, Lum S, Kirkby J, et al. Lung function and respiratory symptoms at 11 years in children born extremely preterm: the EPICure study. Am J Respir Crit Care Med. 2010;182(2):237–245.
10. Poindexter BB, Feng R, Schmidt B, et al. Comparisons and limitations of current definitions of bronchopulmonary dysplasia for the prematurity and respiratory outcomes program. Ann Am Thorac Soc. 2015;12(12):1822–1830. doi:10.1513/AnnalsATS.201504-218OC
11. Mandell EW, Kratimenos P, Abman SH, Steinhorn RH. Drugs for the prevention and treatment of bronchopulmonary dysplasia. Clin Perinatol. 2019;46(2):291–310.
12. Mosca F, Colnaghi M, Fumagalli M. BPD: old and new problems. J Matern Fetal Neonatal Med. 2011;24(Suppl 1):80–82.
13. SUPPORT Study Group of the Eunice Kennedy Shriver NICHD Neonatal Research Network; Finer NN, Carlo WA, et al. Early CPAP versus surfactant in extremely preterm infants. N Engl J Med. 2010;362(21):1970–1979.
14. Morley CJ, Davis PG, Doyle LW, Brion LP, Hascoet JM, Carlin JB. Nasal CPAP or intubation at birth for very preterm infants. N Engl J Med. 2008;358(7):700–708.
15. Dunn MS, Kaempf J, de Klerk A, et al. Randomized trial comparing 3 approaches to the initial respiratory management of preterm neonates. Pediatrics. 2011;128(5):e1069–1076.
16. Subramaniam P, Ho JJ, Davis PG. Prophylactic nasal continuous positive airway pressure for preventing morbidity and mortality in very preterm infants. Cochrane Database Syst Rev. 2016;6:CD001243.
17. Courtney SE, Barrington KJ. Continuous positive airway pressure and noninvasive ventilation. Clin Perinatol. 2007;34(1):73–92, vi.
18. Lemyre B, Laughon M, Bose C, Davis PG. Early nasal intermittent positive pressure ventilation (NIPPV) versus early nasal continuous positive airway pressure (NCPAP) for preterm infants. Cochrane Database Syst Rev. 2016;12(12):Cd005384.
19. Lemyre B, Davis PG, De Paoli AG, Kirpalani H. Nasal intermittent positive pressure ventilation (NIPPV) versus nasal continuous positive airway pressure (NCPAP) for preterm neonates after extubation. Cochrane Database Syst Rev. 2017;2:CD003212.
20. Rysavy MA, Mehler K, Oberthur A, et al. An immature science: intensive care for infants born at</=23 weeks of gestation. J Pediatr. 2021;233:16–25.
21. Johnson AH, Peacock JL, Greenough A, et al. High-frequency oscillatory ventilation for the prevention of chronic lung disease of prematurity. N Engl J Med. 2002;347(9):633–642.
22. Cools F, Offringa M, Askie LM. Elective high frequency oscillatory ventilation versus conventional ventilation for acute pulmonary dysfunction in preterm infants. Cochrane Database Syst Rev. 2015;3:Cd000104.
23. Askie LM, Henderson-Smart DJ, Irwig L, Simpson JM. Oxygen-saturation targets and outcomes in extremely preterm infants. N Engl J Med. 2003;349(10):959–967.
24. Manja V, Lakshminrusimha S, Cook DJ. Oxygen saturation target range for extremely preterm infants: a systematic review and meta-analysis. JAMA Pediatr. 2015;169(4):332–340.
25. Askie LM, Darlow BA, Davis PG, et al. Effects of targeting lower versus higher arterial oxygen saturations on death or disability in preterm infants. Cochrane Database Syst Rev. 2017;4(4):Cd011190.
26. Nelin LD, Bhandari V. How to decrease bronchopulmonary dysplasia in your neonatal intensive care unit today and “tomorrow”. F1000Res. 2017;6:539.
27. Burri PH. Fetal and postnatal development of the lung. Annu Rev Physiol. 1984;46:617–628.
28. Avery ME, Mead J. Surface properties in relation to atelectasis and hyaline membrane disease. AMA J Dis Child. 1959;97(5,Part 1):517–523.
29. Reynolds EO, Roberton NR, Wigglesworth JS. Hyaline membrane disease, respiratory distress, and surfactant deficiency. Pediatrics. 1968;42(5):758–768.
30. Fujiwara T, Maeta H, Chida S, Morita T, Watabe Y, Abe T. Artificial surfactant therapy in hyaline-membrane disease. Lancet. 1980;1(8159):55–59.
31. Soll RF. Prophylactic natural surfactant extract for preventing morbidity and mortality in preterm infants. Cochrane Database Syst Rev. 2000;1997(2):CD000511.
32. Soll RF. Prophylactic synthetic surfactant for preventing morbidity and mortality in preterm infants. Cochrane Database Syst Rev. 2010;2010(1):CD001079. https://pubmed.ncbi.nlm.nih.gov/20091513/
33. Stevenson D, Walther F, Long W, et al. Controlled trial of a single dose of synthetic surfactant at birth in premature infants weighing 500 to 699 grams. The American Exosurf Neonatal Study Group I. J Pediatr. 1992;120(2 Pt 2):S3–12.
34. McMillan D, Chernick V, Finer N, et al. Effects of two rescue doses of synthetic surfactant in 344 infants with respiratory distress syndrome weighing 750 to 1249 grams: a double-blind, placebo-controlled multicenter Canadian trial. Canadian Exosurf Neonatal Study Group. J Pediatr. 1995;126(5 Pt 2):S90–98.
35. Konishi M, Fujiwara T, Chida S, et al. A prospective, randomized trial of early versus late administration of a single dose of surfactant-TA. Early Hum Dev. 1992;29(1–3):275–282.
36. Seger N, Soll R. Animal derived surfactant extract for treatment of respiratory distress syndrome. Cochrane Database Syst Rev. 2009;(2):CD007836.
37. Beam KS, Aliaga S, Ahlfeld SK, Cohen-Wolkowiez M, Smith PB, Laughon MM. A systematic review of randomized controlled trials for the prevention of bronchopulmonary dysplasia in infants. J Perinatol. 2014;34(9):705–710.
38. Bahadue FL, Soll R. Early versus delayed selective surfactant treatment for neonatal respiratory distress syndrome. Cochrane Database Syst Rev. 2012;11(11):Cd001456.
39. Isayama T, Chai-Adisaksopha C, McDonald SD. Noninvasive ventilation with vs without early surfactant to prevent chronic lung disease in preterm infants: a systematic review and meta-analysis. JAMA Pediatr. 2015;169(8):731–739.
40. Lakkundi A, Wright I, de Waal K. Transitional hemodynamics in preterm infants with a respiratory management strategy directed at avoidance of mechanical ventilation. Early Hum Dev. 2014;90(8):409–412.
41. Brix N, Sellmer A, Jensen MS, Pedersen LV, Henriksen TB. Predictors for an unsuccessful INtubation-SURfactant-Extubation procedure: a cohort study. BMC Pediatr. 2014;14:155.
42. Vento G, Pastorino R, Boni L, et al. Efficacy of a new technique - INtubate-RECruit-SURfactant-Extubate - “IN-REC-SUR-E” - in preterm neonates with respiratory distress syndrome: study protocol for a randomized controlled trial. Trials. 2016;17:414.
43. Vento G, Ventura ML, Pastorino R, et al. Lung recruitment before surfactant administration in extremely preterm neonates with respiratory distress syndrome (IN-REC-SUR-E): a randomised, unblinded, controlled trial. Lancet Respir Med. 2021;9(2):159–166.
44. Jensen EA. Prevention of bronchopulmonary dysplasia: a summary of evidence-based strategies. Neoreviews. 2019;20(4):e189–e201.
45. Kanmaz HG, Erdeve O, Canpolat FE, Mutlu B, Dilmen U. Surfactant administration via thin catheter during spontaneous breathing: randomized controlled trial. Pediatrics. 2013;131(2):e502–509.
46. Rigo V, Lefebvre C, Broux I. Surfactant instillation in spontaneously breathing preterm infants: a systematic review and meta-analysis. Eur J Pediatr. 2016;175(12):1933–1942.
47. Cummings JJ, Gerday E, Minton S, et al. Aerosolized calfactant for newborns with respiratory distress: a randomized trial. Pediatrics. 2020;146:5.
48. Isayama T, Iwami H, McDonald S, Beyene J. Association of noninvasive ventilation strategies with mortality and bronchopulmonary dysplasia among preterm infants: a systematic review and meta-analysis. JAMA. 2016;316(6):611–624.
49. Ardell S, Pfister RH, Soll R. Animal derived surfactant extract versus protein free synthetic surfactant for the prevention and treatment of respiratory distress syndrome. Cochrane Database Syst Rev. 2015;8:CD000144.
50. Principi N, Di Pietro GM, Esposito S. Bronchopulmonary dysplasia: clinical aspects and preventive and therapeutic strategies. J Transl Med. 2018;16(1):36.
51. Ramanathan R, Biniwale M, Sekar K, et al. Synthetic surfactant CHF5633 compared with poractant alfa in the treatment of neonatal respiratory distress syndrome: a multicenter, double-blind, randomized, controlled clinical trial. J Pediatr. 2020;225(90–96):e91.
52. Effect of corticosteroids for fetal maturation on perinatal outcomes. NIH consensus development panel on the effect of corticosteroids for fetal maturation on perinatal outcomes. JAMA. 1995;273(5):413–418.
53. Roberts D, Brown J, Medley N, Dalziel SR. Antenatal corticosteroids for accelerating fetal lung maturation for women at risk of preterm birth. Cochrane Database Syst Rev. 2017;3(3):Cd004454.
54. Travers CP, Carlo WA, McDonald SA, et al. Mortality and pulmonary outcomes of extremely preterm infants exposed to antenatal corticosteroids. Am J Obstet Gynecol. 2018;218(1):130e131–130 e113.
55. Chawla S, Natarajan G, Shankaran S, et al. Association of neurodevelopmental outcomes and neonatal morbidities of extremely premature infants with differential exposure to antenatal steroids. JAMA Pediatr. 2016;170(12):1164–1172.
56. Carlo WA, McDonald SA, Fanaroff AA, et al. Association of antenatal corticosteroids with mortality and neurodevelopmental outcomes among infants born at 22 to 25 weeks’ gestation. JAMA. 2011;306(21):2348–2358.
57. Filippone M, Nardo D, Bonadies L, Salvadori S, Baraldi E. Update on postnatal corticosteroids to prevent or treat bronchopulmonary dysplasia. Am J Perinatol. 2019;36(S 02):S58–s62.
58. Jefferies AL. Postnatal corticosteroids to treat or prevent chronic lung disease in preterm infants. Pediatrics. 2002;109(2):330–338.
59. Doyle LW, Cheong JL, Ehrenkranz RA, Halliday HL. Early (< 8 days) systemic postnatal corticosteroids for prevention of bronchopulmonary dysplasia in preterm infants. Cochrane Database Syst Rev. 2017;10(10):Cd001146.
60. Doyle LW, Halliday HL, Ehrenkranz RA, Davis PG, Sinclair JC. An update on the impact of postnatal systemic corticosteroids on mortality and cerebral palsy in preterm infants: effect modification by risk of bronchopulmonary dysplasia. J Pediatr. 2014;165(6):1258–1260.
61. Doyle LW, Davis PG, Morley CJ, McPhee A, Carlin JB. Low-dose dexamethasone facilitates extubation among chronically ventilator-dependent infants: a multicenter, international, randomized, controlled trial. Pediatrics. 2006;117(1):75–83.
62. Doyle LW, Cheong JL, Ehrenkranz RA, Halliday HL. Late (> 7 days) systemic postnatal corticosteroids for prevention of bronchopulmonary dysplasia in preterm infants. Cochrane Database Syst Rev. 2017;10(10):Cd001145.
63. Zeng L, Tian J, Song F, et al. Corticosteroids for the prevention of bronchopulmonary dysplasia in preterm infants: a network meta-analysis. Arch Dis Child Fetal Neonatal Ed. 2018;103(6):F506–f511.
64. Ramaswamy VV, Bandyopadhyay T, Nanda D, et al. Assessment of postnatal corticosteroids for the prevention of bronchopulmonary dysplasia in preterm neonates: a systematic review and network meta-analysis. JAMA Pediatr. 2021;175:e206826.
65. Harmon HM, Jensen EA, Tan S, et al. Timing of postnatal steroids for bronchopulmonary dysplasia: association with pulmonary and neurodevelopmental outcomes. J Perinatol. 2020;40(4):616–627.
66. Watterberg KL. American Academy of Pediatrics. Committee on F, Newborn. Policy statement–postnatal corticosteroids to prevent or treat bronchopulmonary dysplasia. Pediatrics. 2010;126(4):800–808.
67. Watterberg KL, Gerdes JS, Cole CH, et al. Prophylaxis of early adrenal insufficiency to prevent bronchopulmonary dysplasia: a multicenter trial. Pediatrics. 2004;114(6):1649–1657.
68. Baud O, Maury L, Lebail F, et al. Effect of early low-dose hydrocortisone on survival without bronchopulmonary dysplasia in extremely preterm infants (PREMILOC): a double-blind, placebo-controlled, multicentre, randomised trial. Lancet. 2016;387(10030):1827–1836.
69. Shaffer ML, Baud O, Lacaze-Masmonteil T, Peltoniemi OM, Bonsante F, Watterberg KL. Effect of prophylaxis for early adrenal insufficiency using low-dose hydrocortisone in very preterm infants: an individual patient data meta-analysis. J Pediatr. 2019;207:136–142.e135.
70. Onland W, Cools F, Kroon A, et al. Effect of hydrocortisone therapy initiated 7 to 14 days after birth on mortality or bronchopulmonary dysplasia among very preterm infants receiving mechanical ventilation: a randomized clinical trial. JAMA. 2019;321(4):354–363.
71. Nelin LD, Logan JW. The use of inhaled corticosteroids in chronically ventilated preterm infants. Semin Fetal Neonatal Med. 2017;22(5):296–301.
72. Yeh TF, Chen CM, Wu SY, et al. Intratracheal administration of budesonide/surfactant to prevent bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2016;193(1):86–95.
73. Bassler D, Plavka R, Shinwell ES, et al. Early inhaled budesonide for the prevention of bronchopulmonary dysplasia. N Engl J Med. 2015;373(16):1497–1506.
74. Bassler D, Shinwell ES, Hallman M, et al. Long-term effects of inhaled budesonide for bronchopulmonary dysplasia. N Engl J Med. 2018;378(2):148–157.
75. ClinicalTrialsgov. Intratrachel budesonide/surfactant prevents BPD. Available from: https://clinicaltrials.gov/ct2/show/NCT03275415.
76. ANZCTR. Multicentre Randomised Controlled Trial of Surfactant Plus Budesonide to Improve Survival Free of Bronchopulmonary Dysplasia in Extremely Preterm Infants. Available from: https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=372110. Accessed August 03, 2021.
77. The Budesonide in Babies (BiB) Trial (BiB). Available from: https://clinicaltrials.gov/ct2/show/NCT04545866.
78. Schmidt B, Roberts RS, Davis P, et al. Caffeine therapy for apnea of prematurity. N Engl J Med. 2006;354(20):2112–2121.
79. Davis PG, Schmidt B, Roberts RS, et al. Caffeine for apnea of prematurity trial: benefits may vary in subgroups. J Pediatr. 2010;156(3):382–387.
80. Taha D, Kirkby S, Nawab U, et al. Early caffeine therapy for prevention of bronchopulmonary dysplasia in preterm infants. J Matern Fetal Neonatal Med. 2014;27(16):1698–1702.
81. Patel RM, Leong T, Carlton DP, Vyas-Read S. Early caffeine therapy and clinical outcomes in extremely preterm infants. J Perinatol. 2013;33(2):134–140.
82. Lodha A, Seshia M, McMillan DD, et al. Association of early caffeine administration and neonatal outcomes in very preterm neonates. JAMA Pediatr. 2015;169(1):33–38.
83. Clyman RI. Patent ductus arteriosus, its treatments, and the risks of pulmonary morbidity. Semin Perinatol. 2018;42(4):235–242.
84. Gonzalez A, Sosenko IR, Chandar J, Hummler H, Claure N, Bancalari E. Influence of infection on patent ductus arteriosus and chronic lung disease in premature infants weighing 1000 grams or less. J Pediatr. 1996;128(4):470–478.
85. Marshall DD, Kotelchuck M, Young TE, Bose CL, Kruyer L, O’Shea TM. Risk factors for chronic lung disease in the surfactant era: a North Carolina population-based study of very low birth weight infants. North Carolina Neonatologists Association. Pediatrics. 1999;104(6):1345–1350.
86. Oh W, Poindexter BB, Perritt R, et al. Association between fluid intake and weight loss during the first ten days of life and risk of bronchopulmonary dysplasia in extremely low birth weight infants. J Pediatr. 2005;147(6):786–790.
87. Evans P, O’Reilly D, Flyer JN, Soll R, Mitra S. Indomethacin for symptomatic patent ductus arteriosus in preterm infants. Cochrane Database Syst Rev. 2021;1:CD013133.
88. Mitra S, Scrivens A, von Kursell AM, Disher T. Early treatment versus expectant management of hemodynamically significant patent ductus arteriosus for preterm infants. Cochrane Database Syst Rev. 2020;12:CD013278.
89. Ohlsson A, Shah SS. Ibuprofen for the prevention of patent ductus arteriosus in preterm and/or low birth weight infants. Cochrane Database Syst Rev. 2020;1:CD004213.
90. Sung SI, Lee MH, Ahn SY, Chang YS, Park WS. Effect of nonintervention vs oral ibuprofen in patent ductus arteriosus in preterm infants: a randomized clinical trial. JAMA Pediatr. 2020;174(8):755–763.
91. Sung SI, Chang YS, Chun JY, et al. Mandatory closure versus nonintervention for patent ductus arteriosus in very preterm infants. J Pediatr. 2016;177:66–71.e61.
92. Mitra S, McNamara PJ. Patent ductus arteriosus-time for a definitive trial. Clin Perinatol. 2020;47(3):617–639.
93. Marconi E, Bettiol A, Ambrosio G, et al. Efficacy and safety of pharmacological treatments for patent ductus arteriosus closure: a systematic review and network meta-analysis of clinical trials and observational studies. Pharmacol Res. 2019;148:104418.
94. Clyman RI, Kaempf J, Liebowitz M, et al. Prolonged tracheal intubation and the association between patent ductus arteriosus and bronchopulmonary dysplasia: a secondary analysis of the PDA-TOLERATE trial. J Pediatr. 2021;229:283–288.e282.
95. Sankar MN, Bhombal S, Benitz WE. PDA: to treat or not to treat. Congenit Heart Dis. 2019;14(1):46–51.
96. Clyman RI, Hills NK, Liebowitz M, Johng S. Relationship between duration of infant exposure to a moderate-to-large patent ductus arteriosus shunt and the risk of developing bronchopulmonary dysplasia or death before 36 weeks. Am J Perinatol. 2020;37(2):216–223.
97. Semberova J, Sirc J, Miletin J, et al. Spontaneous closure of patent ductus arteriosus in infants</=1500 g. Pediatrics. 2017;140:2.
98. Greenberg RG, Gayam S, Savage D, et al. Furosemide exposure and prevention of bronchopulmonary dysplasia in premature infants. J Pediatr. 2019;208:134–140.e132. doi:10.1016/j.jpeds.2018.11.043
99. Blaisdell CJ, Troendle J, Zajicek A. Acute responses to diuretic therapy in extremely low gestational age newborns: results from the prematurity and respiratory outcomes program cohort study. J Pediatr. 2018;197:42–47.e41. doi:10.1016/j.jpeds.2018.01.066
100. Kao LC, Warburton D, Sargent CW, Platzker AC, Keens TG. Furosemide acutely decreases airways resistance in chronic bronchopulmonary dysplasia. J Pediatr. 1983;103(4):624–629.
101. Engelhardt B, Elliott S, Hazinski TA. Short- and long-term effects of furosemide on lung function in infants with bronchopulmonary dysplasia. J Pediatr. 1986;109(6):1034–1039.
102. Kao LC, Durand DJ, McCrea RC, Birch M, Powers RJ, Nickerson BG. Randomized trial of long-term diuretic therapy for infants with oxygen-dependent bronchopulmonary dysplasia. J Pediatr. 1994;124(5 Pt 1):772–781.
103. Stewart A, Brion LP. Intravenous or enteral loop diuretics for preterm infants with (or developing) chronic lung disease. Cochrane Database Syst Rev. 2011;2011(9):Cd001453.
104. Ryan RM, Keller RL, Poindexter BB, et al. Respiratory medications in infants <29 weeks during the first year postdischarge: the Prematurity and Respiratory Outcomes Program (PROP) consortium. J Pediatr. 2019;208(148–155):e143.
105. Bamat NA, Nelin TD, Eichenwald EC, et al. Loop diuretics in severe bronchopulmonary dysplasia: cumulative use and associations with mortality and age at discharge. J Pediatr. 2021;231:43–49.e43.
106. Slaughter JL, Stenger MR, Reagan PB, Jadcherla SR. Inhaled bronchodilator use for infants with bronchopulmonary dysplasia. J Perinatol. 2015;35(1):61–66.
107. Wilkie RA, Bryan MH. Effect of bronchodilators on airway resistance in ventilator-dependent neonates with chronic lung disease. J Pediatr. 1987;111(2):278–282.
108. Morrow DK, Schilling D, McEvoy CT. Response to bronchodilators in very preterm infants with evolving bronchopulmonary dysplasia. Res Rep Neonatol. 2015;5:113–117.
109. Ng G, da Silva O, Ohlsson A. Bronchodilators for the prevention and treatment of chronic lung disease in preterm infants. Cochrane Database Syst Rev. 2016;12:CD003214.
110. Euteneuer JC, Kerns E, Leiting C, McCulloh RJ, Peeples ES. Inhaled bronchodilator exposure in the management of bronchopulmonary dysplasia in hospitalized infants. J Perinatol. 2021;41(1):53–61.
111. Eriksson L, Haglund B, Odlind V, Altman M, Ewald U, Kieler H. Perinatal conditions related to growth restriction and inflammation are associated with an increased risk of bronchopulmonary dysplasia. Acta Paediatr. 2015;104(3):259–263.
112. Poindexter BB, Martin CR. Impact of nutrition on bronchopulmonary dysplasia. Clin Perinatol. 2015;42(4):797–806.
113. Natarajan G, Johnson YR, Brozanski B, et al. Postnatal weight gain in preterm infants with severe bronchopulmonary dysplasia. Am J Perinatol. 2014;31(3):223–230.
114. Moschino L, Duci M, Fascetti Leon F, et al. Optimizing nutritional strategies to prevent necrotizing enterocolitis and growth failure after bowel resection. Nutrients. 2021;13:2.
115. Villamor-Martínez E, Pierro M, Cavallaro G, Mosca F, Kramer BW, Villamor E. Donor human milk protects against bronchopulmonary dysplasia: a systematic review and meta-analysis. Nutrients. 2018;10:2.
116. Hair AB, Peluso AM, Hawthorne KM, et al. Beyond necrotizing enterocolitis prevention: improving outcomes with an exclusive human milk-based diet. Breastfeed Med. 2016;11(2):70–74.
117. Biesalski HK, Nohr D. Importance of vitamin-A for lung function and development. Mol Aspects Med. 2003;24(6):431–440.
118. Darlow BA, Graham PJ, Rojas-Reyes MX. Vitamin A supplementation to prevent mortality and short- and long-term morbidity in very low birth weight infants. Cochrane Database Syst Rev. 2016;2016(8):Cd000501.
119. Tolia VN, Murthy K, McKinley PS, Bennett MM, Clark RH. The effect of the national shortage of vitamin A on death or chronic lung disease in extremely low-birth-weight infants. JAMA Pediatr. 2014;168(11):1039–1044.
120. Rakshasbhuvankar AA, Simmer K, Patole SK, et al. Enteral Vitamin A for reducing severity of bronchopulmonary dysplasia: a randomized trial. Pediatrics. 2021;147:1.
121. Meyer S, Gortner L. Early postnatal additional high-dose oral vitamin A supplementation versus placebo for 28 days for preventing bronchopulmonary dysplasia or death in extremely low birth weight infants. Neonatology. 2014;105(3):182–188.
122. Denne SC. Energy expenditure in infants with pulmonary insufficiency: is there evidence for increased energy needs? J Nutr. 2001;131(3):935s–937s.
123. Lai NM, Rajadurai SV, Tan KH. Increased energy intake for preterm infants with (or developing) bronchopulmonary dysplasia/ chronic lung disease. Cochrane Database Syst Rev. 2006;3:CD005093.
124. Groothuis JR, Makari D. Definition and outpatient management of the very low-birth-weight infant with bronchopulmonary dysplasia. Adv Ther. 2012;29(4):297–311.
125. Anderson C, Hillman NH. Bronchopulmonary dysplasia: when the very preterm baby comes home. Mo Med. 2019;116(2):117–122.
126. Abman SH, Collaco JM, Shepherd EG, et al. Interdisciplinary care of children with severe bronchopulmonary dysplasia. J Pediatr. 2017;181(12–28):e11.
127. Brunton JA, Saigal S, Atkinson SA. Growth and body composition in infants with bronchopulmonary dysplasia up to 3 months corrected age: a randomized trial of a high-energy nutrient-enriched formula fed after hospital discharge. J Pediatr. 1998;133(3):340–345.
128. Van Marter LJ, Dammann O, Allred EN, et al. Chorioamnionitis, mechanical ventilation, and postnatal sepsis as modulators of chronic lung disease in preterm infants. J Pediatr. 2002;140(2):171–176.
129. Liljedahl M, Bodin L, Schollin J. Coagulase-negative staphylococcal sepsis as a predictor of bronchopulmonary dysplasia. Acta Paediatr. 2004;93(2):211–215.
130. Lahra MM, Beeby PJ, Jeffery HE. Intrauterine inflammation, neonatal sepsis, and chronic lung disease: a 13-year hospital cohort study. Pediatrics. 2009;123(5):1314–1319.
131. Weimer KED, Kelly MS, Permar SR, Clark RH, Greenberg RG. Association of adverse hearing, growth, and discharge age outcomes with postnatal cytomegalovirus infection in infants with very low birth weight. JAMA Pediatr. 2020;174(2):133–140.
132. Viscardi RM, Kallapur SG. Role of ureaplasma respiratory tract colonization in bronchopulmonary dysplasia pathogenesis: current concepts and update. Clin Perinatol. 2015;42(4):719–738.
133. Nair V, Loganathan P, Soraisham AS. Azithromycin and other macrolides for prevention of bronchopulmonary dysplasia: a systematic review and meta-analysis. Neonatology. 2014;106(4):337–347.
134. Viscardi RM, Terrin ML, Magder LS, et al. Randomised trial of azithromycin to eradicate Ureaplasma in preterm infants. Arch Dis Child Fetal Neonatal Ed. 2020;105(6):615–622.
135. Poets CF, Lorenz L. Prevention of bronchopulmonary dysplasia in extremely low gestational age neonates: current evidence. Arch Dis Child Fetal Neonatal Ed. 2018;103(3):F285–F291.
136. Balany J, Bhandari V. Understanding the impact of infection, inflammation, and their persistence in the pathogenesis of bronchopulmonary dysplasia. Front Med (Lausanne). 2015;2:90.
137. Lapcharoensap W, Kan P, Powers RJ, et al. The relationship of nosocomial infection reduction to changes in neonatal intensive care unit rates of bronchopulmonary dysplasia. J Pediatr. 2017;180:105–109.e101.
138. Ting JY, Roberts A, Sherlock R, et al. Duration of initial empirical antibiotic therapy and outcomes in very low birth weight infants. Pediatrics. 2019;143:3.
139. Cantey JB, Huffman LW, Subramanian A, et al. Antibiotic exposure and risk for death or bronchopulmonary dysplasia in very low birth weight infants. J Pediatr. 2017;181(289–293):e281.
140. Ting JY, Synnes A, Roberts A, et al. Association between antibiotic use and neonatal mortality and morbidities in very low-birth-weight infants without culture-proven sepsis or necrotizing enterocolitis. JAMA Pediatr. 2016;170(12):1181–1187.
141. Hansmann G, Fernandez-Gonzalez A, Aslam M, et al. Mesenchymal stem cell-mediated reversal of bronchopulmonary dysplasia and associated pulmonary hypertension. Pulm Circ. 2012;2(2):170–181.
142. Lim R, Malhotra A, Tan J, et al. First-in-human administration of allogeneic amnion cells in premature infants with bronchopulmonary dysplasia: a safety study. Stem Cells Transl Med. 2018;7(9):628–635.
143. Ahn SY, Chang YS, Lee MH, et al. Stem cells for bronchopulmonary dysplasia in preterm infants: a randomized controlled phase II trial. Stem Cells Transl Med. 2021. Available from: https://stemcellsjournals.onlinelibrary.wiley.com/doi/10.1002/sctm.20-0330. Accessed August 03, 2021.
144. Willis GR, Fernandez-Gonzalez A, Anastas J, et al. Mesenchymal stromal cell exosomes ameliorate experimental bronchopulmonary dysplasia and restore lung function through macrophage immunomodulation. Am J Respir Crit Care Med. 2018;197(1):104–116.
145. Hellström A, Engström E, Hård AL, et al. Postnatal serum insulin-like growth factor I deficiency is associated with retinopathy of prematurity and other complications of premature birth. Pediatrics. 2003;112(5):1016–1020.
146. Shennan AT, Dunn MS, Ohlsson A, Lennox K, Hoskins EM. Abnormal pulmonary outcomes in premature infants: prediction from oxygen requirement in the neonatal period. Pediatrics. 1988;82(4):527–532.
147. Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2001;163(7):1723–1729.
148. Walsh MC, Yao Q, Gettner P, et al. Impact of a physiologic definition on bronchopulmonary dysplasia rates. Pediatrics. 2004;114(5):1305–1311.
149. Isayama T, Lee SK, Yang J, et al. Revisiting the definition of bronchopulmonary dysplasia: effect of changing panoply of respiratory support for preterm neonates. JAMA Pediatr. 2017;171(3):271–279.
150. Higgins RD, Jobe AH, Koso-Thomas M, et al. Bronchopulmonary dysplasia: executive summary of a workshop. J Pediatr. 2018;197:300–308.
151. Jensen EA, Dysart K, Gantz MG, et al. The diagnosis of bronchopulmonary dysplasia in very preterm infants: an evidence-based approach. Am J Respir Crit Care Med. 2019;200(6):751-759.
152. Stewart A, Brion LP, Ambrosio-Perez I. Diuretics acting on the distal renal tubule for preterm infants with (or developing) chronic lung disease. Cochrane Database Syst Rev. 2011;2011(9):CD001817.
153. Yuksel B, Greenough A. Randomised trial of inhaled steroids in preterm infants with respiratory symptoms at follow up. Thorax. 1992;47(11):910–913.
154. Bhandari A, Schramm CM, Kimble C, Pappagallo M, Hussain N. Effect of a short course of prednisolone in infants with oxygen-dependent bronchopulmonary dysplasia. Pediatrics. 2008;121(2):e344–349.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.