Back to Journals » Neuropsychiatric Disease and Treatment » Volume 15
An intervention targeting social, communication and daily activity skills in children and adolescents with Down syndrome and autism: a pilot study
Authors Wester Oxelgren U ![]() , Westerlund J, Myrelid Å
, Westerlund J, Myrelid Å ![]() , Annerén G, Johansson L, Åberg M, Gustafsson J, Fernell E
, Annerén G, Johansson L, Åberg M, Gustafsson J, Fernell E ![]()
Received 17 February 2019
Accepted for publication 23 May 2019
Published 18 July 2019 Volume 2019:15 Pages 2049—2056
DOI https://doi.org/10.2147/NDT.S205721
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Ulrika Wester Oxelgren,1 Joakim Westerlund,2,3 Åsa Myrelid,1 Göran Annerén,4 Lotta Johansson,5 Marie Åberg,5 Jan Gustafsson,1 Elisabeth Fernell3
1Department of Women’s and Children’s Health, Uppsala University, Uppsala, Sweden; 2Department of Psychology, Stockholm University, Stockholm, Sweden; 3Gillberg Neuropsychiatry Centre, Department of Neuroscience and Physiology, Gothenburg University, Gothenburg, Sweden; 4Department of Immunology, Genetics, and Pathology, Science for Life Laboratory, Uppsala University, Uppsala, Sweden; 5Department of Health and Rehabilitation, Uppsala County, Kungsgärdet Center, Uppsala, Sweden
Purpose: To evaluate whether an intervention, targeting deficits in social communication, interaction and restricted activities in children and adolescents with Down syndrome and autism could lead to enhanced participation in family and school activities.
Methods: The intervention included education for parents and school staff about autism, and workshops to identify social-communication and daily living activities that would be meaningful for the child to practice at home and at school. Thereafter, a three-month period of training for the child followed. Outcome measures comprised evaluation of goal achievement for each child, the “Family Strain Index” questionnaire and a visual scale pertaining to the parents’ general opinion about the intervention.
Results: On average, more than 90% of the goals were (to some extent or completely) achieved at home and at school. The mean scores of the “Family Strain Index” were almost identical at the follow-up to those before intervention. The evaluation supported that the use of strategies, intended to facilitate activities and communication, remained largely 18 months after start of the intervention.
Conclusion: Despite the group involved in this study being composed of older children and adolescents, most of whom had severe and profound intellectual disability, the goal achievements and parents’ views on the intervention were encouraging.
Keywords: Down syndrome, intellectual disability, autism, psychoeducational intervention
Introduction
Down syndrome (DS), ie, trisomy 21, is the single most commonly identified etiology of intellectual disability (ID)1 and has a worldwide incidence of about 1:800–1:1,000 live births.2 Down syndrome was previously considered as an autism “contrast syndrome”, but this view has changed.3 The level of intellectual disability varies from mild to profound and, in addition to ID, coexisting autism spectrum disorder, attention-deficit/hyperactivity disorder (ADHD) and other developmental/neuropsychiatric disorders have been increasingly reported.4–8 Prevalence estimates of these neurobehavioral and psychiatric disorders range from 20% to 40% in children with DS.4
Autism spectrum disorder (ASD) occurs in approximately 1% of the children in the general population9 and in up to 40% of the individuals with ID.10 Greater severity of one of these two disorders appears to have effects on the other disorder, ie, as IQ goes down the severity of ASD and challenging behaviors goes up.11
The prevalence of ASD in children with DS has been reported to be 17–40%6,7 and is particularly high in those with severe ID.12 There is evidence from several studies that individuals with DS and ASD, in addition to ID, show more cognitive, social and behavioral difficulties than those with ‘typical’ DS.5
Social and communicative deficits combined with specific behavioral abnormalities constitute the core impairments in ASD.13 Walton and Ingersoll14 reviewed specific interventions with the aim of improving social skills in adolescents with ASD combined with severe or profound ID. They reported that studies in the field were associated with significant challenges regarding research design and methodology. The differences in challenging behaviors between individuals with ASD and ID and those with ID only demonstrate that the former have unique needs. Consequently, they may not be well served by existing programs designed for individuals with ID or for ASD only.14
Techniques based on Applied Behavior Analysis (ABA), ie, to analyze antecedents and consequences of specific behaviors to decrease severely challenging behaviors in children with autism were developed by Lovaas in the 1960s.15,16 ABAis a teaching method that applies the principles of learning theory to “improve socially significant behaviors to a meaningful degree” that is specific to the needs of the individual. Common strategies used are reinforcement, prompting and fading with the goal of either improving or decreasing targeted behaviors.
This operant learning treatment technique to teach a variety of skills in children with autism has now increasingly been modified and implemented in the child’s natural settings, using a variety of behavioral strategies to teach developmentally appropriate and prerequisite skills, often referred to as naturalistic developmental behavioral intervention. Thus, ABA and developmental sciences have gradually been merged.17–22
Several studies have shown a high prevalence of problem behaviors in individuals with ID. Wachtel and Hagopian23 discussed how problem behavior in individuals with ID may emerge from a combination of factors including deficits in communication and adaptive behavior. Their three cases illustrated children with severe problem behaviors that responded well to psychopharmacological treatment combined with ABA.
Children with ASD constitute a highly heterogeneous group – etiologically, biologically and clinically.3 Children with ASD and higher cognitive levels have been found to have better acquisition of skills and better adaptive functioning outcome than those with a low cognitive level.24
In this study, we present experiences and results from the use of a comprehensive psychoeducational program, based on ABA and adapted for individuals with DS and ID combined with ASD. The study group was diagnosed with ASD in a previous, population-based study.7 The program represents a naturalistic approach adapted to the cognitive and adaptive impairments of these individuals. To our knowledge, such an intervention has not previously been implemented and evaluated in children and adolescents with DS and ID combined with ASD.
The aim of the study was to evaluate whether a targeted educational program for parents and teachers, and a training period for the children and adolescents with DS and autism, could improve the situation at home and at school.
Methods
Original study cohort
The study was performed in the county of Uppsala, an area with around 350 000 inhabitants.
The parents of all children with DS born in the period 1994–2006 had been invited with their child to participate in a study concerning the prevalence of ASD and ADHD and assessment of ID.7 In total, 60 children (41 M, 19 F) met the age criterion (age range 5–17 years). All subjects attended special classes for children with ID located in mainstream schools. Education was in accordance with the special national educational curriculum for pupils with ID.
Of the 60 subjects, 41 had been assessed within the previously reported ASD and ADHD prevalence study, which revealed that 17 had ASD, 9 of them had combined ASD and ADHD. Diagnosis of ASD was based on DSM-IV criteria25 and included the ADOS and ADI-R in addition to clinical assessments.26–28
Cognitive test,29 an adaptive assessment30,31 and a clinical examination were or had been performed within a former ASD/ADHD study or less than three years prior to the intervention. The patients with DS and ASD generally had more severe ID; 2 children had mild, 4 moderate and 11 severe/profound ID.7
Patients included in the study
Fourteen of the 17 patients with DS and ASD (age range 6–18 years, median 13.0 years) participated in the intervention. Three subjects could not participate, one due to severe behavioral problems for which an individualized intervention had already been initiated, one family moved from the county during the period of the investigation and the parents of the third patient did not respond to the invitation. The sex and ID levels of the 14 children with newly established ASD diagnosis are presented in Table 1. Eleven of the 14 participants had severe/profound, 2 had moderate and 1 had mild ID. Seven of the 14 individuals had no verbal speech, the remaining 7 had major communication difficulties and used picture communication aids as alternative means of expressing themselves. All participants had very few activities outside school.
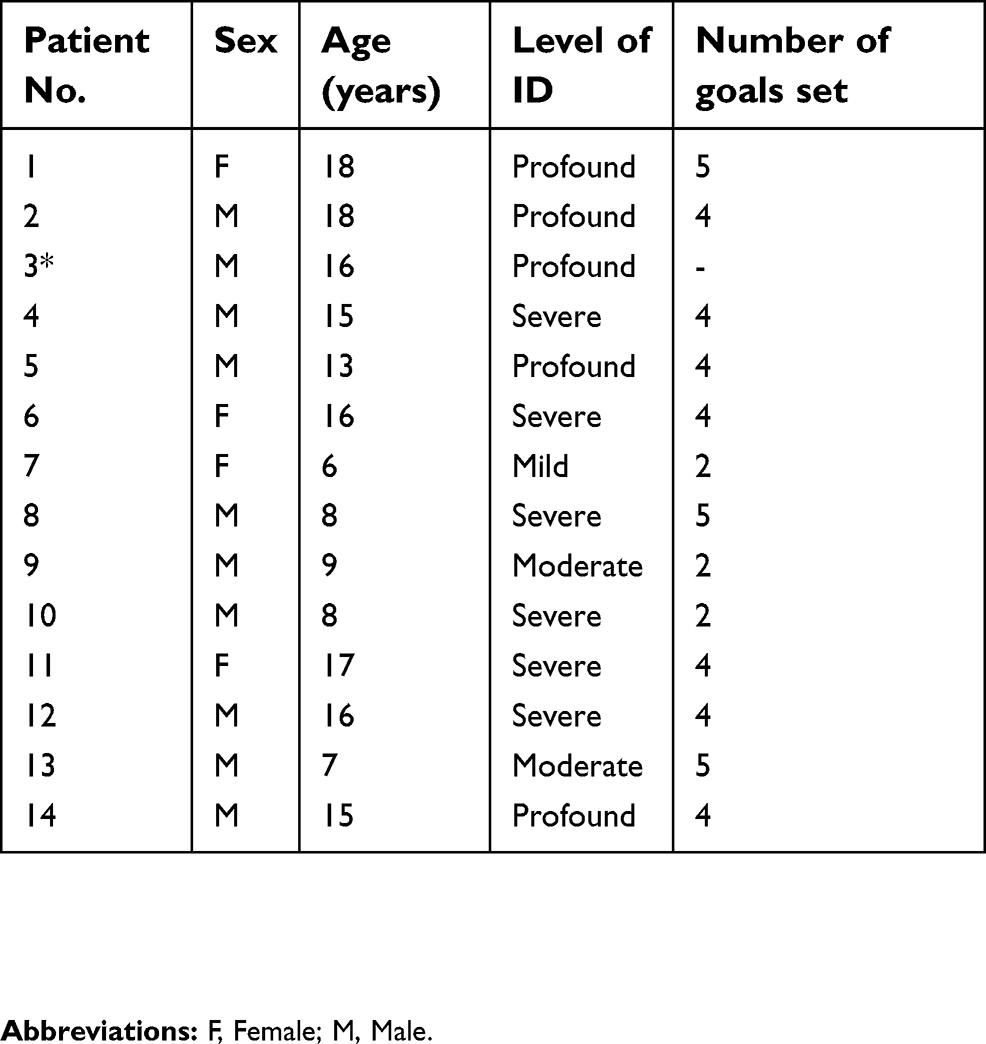 |
Table 1 Background data for children with Down syndrome and autism spectrum disorder and the goals set |
Intervention
A comprehensive psychoeducational intervention program adapted to the specific needs of families with a child with DS and ASD was used. The program was based on the principles of ABA, modified according to the child’s ID level. The intervention was implemented in the child’s natural settings using behavioral strategies to teach developmentally appropriate skills.20–22
All professionals in the research team had considerable experience of working with children with ID and ASD in children with DS. The team included a physiotherapist, a neuropediatrician, a neuropsychologist, a special needs teacher, a speech and language pathologist, and a youth worker.
The intervention encompassed several parts as illustrated in Figure 1.
 |
Figure 1 The intervention time schedule. |
- An educational program was provided for parents and school staff. The program focused on providing general information about DS, ASD and on how to improve communication and daily/leisure activities, taking into account the children’s cognitive and adaptive functioning. A three-week long educational program, comprising approximately three hours every week for parents and school staff was provided, respectively.
- Workshops about communication and daily activities pertaining to each child were organized for parents and school staff. The purpose was to identify what specific aspects should be practiced regarding social and communication skills and to daily-living and leisure activities – at school and at home. At a subsequent meeting, the specific goals for each child were established and agreed upon by parents and school staff. The research-team guided and supervised with making these decisions.
- A medical assessment was performed by the neuropediatrician. Two of the children had pharmacological treatment for ADHD, three for obsessive-compulsive disorder and eight for sleep-disorder. No corrections in medication were made for ADHD, sleep-disorder or psychiatric problems before or during the intervention.
- Five meetings with the parents were organized and led by the neuropsychologist. In these group discussions, parents could raise questions about the consequences the implementation of the new strategies would have on the children’s specific behavioral problems in daily life. The discussions took place every second week during the intervention period.
Individual goals
The parents and school staff chose one to five communication tasks and one to five activity tasks for their child to practice and perform. The goals were set with guidance from the professionals in the research team. Some of the goals defined were more suitable for practice at home and others were more relevant for school. The school staff had extensive experience of working with the children in the study and were motivated to work with the intervention program. The intervention was specifically adapted for this target group.
The goals that the parents, school staff and research team had agreed upon reflected the level of daily functioning of the participants. Most children had three to five goals set in each domain, ie, activity and communication (Table 1). These two types of goals overlapped to a great extent and were merged in the statistical calculation. The research team advised the parents and school staff to set reasonable levels for the goals. The majority of the children had a very low level of functioning and the goals were adapted accordingly. The tasks chosen represented activities that the children had not been able to manage previously. Most children had no activities with other family members or planned activities outside home or school and they could not communicate their views and wishes. An important issue was to find ways for the children to participate with their family and at school. The goal of an activity could therefore be to participate in a social game or by making the table before dinner with an adult every day. A communication goal could, for instance, be to ask and respond to questions using a communication application in a tablet or computer.
Intervention in practice
The period of the intervention was started simultaneously at home and at school and continued for three months. The research-team guided the families and school staff in introducing the activities, eg, helping with domestic activities. For some children, computer programs were introduced to enable communication through images. The research team had contact with both parents and school staff during the three-month period of the intervention with visits at and/or phone-contacts with the Habilitation center to provide advice when required. The ABA behavioral principles – here adapted to children also with severe to profound ID – were applied in everyday situations in order to increase or decrease targeted behaviors.
Outcome measures
Evaluation of goals achieved after the three-month intervention
The goals were evaluated according to whether the goal was achieved completely (1), achieved to some extent (0.5) or not achieved at all (0). A completely achieved goal meant that the goal was met to 100% and a goal achieved to some extent meant 50–100%. Numbers of goals set (2–5), differed between the children due to parents’ and teachers’ preferences. A total score for each child was calculated. The mean value for the goals achieved to some extent or completely was calculated. Goal attainment at home and at school was evaluated by the parents and teachers, respectively.
Family Strain Index questionnaire before and 18 months after the intervention
The questionnaire Family Strain Index (FSI),32,33 a six-item questionnaire, was completed by parents (Table 2). The items describe situations of stress and in which demands were imposed. The items are scored from 0 (never) to 4 (always) yielding a maximum score of 24. Factor analysis in the sample reported by Riley et al indicated that the FSI scale reflects an overall experience of worry, disruption and demand on parents of children with ADHD. In the present sample, the FSI demonstrated satisfactory internal consistency before (Cronbach’s alpha =0.84) as well as after (Cronbach’s alpha =0.83) the intervention.
 |
Table 2 “Family Strain Index” questionnaire |
Parents’ perception of the intervention 18 months after completion
Six items were used by the research team to measure parents’ opinions and attitudes to the given intervention at a meeting that took place with a neuropsychologist who was not a member of the research team. The parents indicated their opinion by marking each question on a 120 mm horizontal line with 0 indicating not at all/no positive effect and 120 indicating very much/very positive effect. The questions pertained to the parents themselves and their child with DS (Table 3).
 |
Table 3 Parents’ perception of the intervention 18 months after completion |
Ethics
The Regional Ethical Review Board of Uppsala approved the study. All parents gave their written informed consent to participate.
Statistics
The mean number of goals either completely or only to some extent achieved was computed for home and for school, respectively. For the 11 parents who completed the “Family Strain Index” both before and after the intervention, a paired sample t-test was used to compare the mean score before, with the mean score after the intervention, using a 5% alpha level. Mean scores and 95% confidence intervals on the 6 items measuring parent’s perception of the intervention 18 months after completion were computed.
Results
Evaluation of goals achieved, after the three-month intervention period
The parents of one child did not complete the intervention period and could not be evaluated. Nine children had evaluations both from home and school, whereas for four children, results could only be obtained from home. The number of goals set varied from 2 to 5 (M=3.77, SD=1.09). On average, 92.31% (SD=18.78%) of the goals were (to some extent or completely) achieved at home and 95.56% (SD=13.33%) of the goals were (to some extent or completely) achieved at school.
Family Strain Index questionnaire before and 18 months after the intervention
Parents of 11 of the 14 children completed the “Family Strain Index” both before the intervention and at the follow-up held 18 months after the intervention had been completed. Parents of three children declined this part of the follow-up for various reasons that were unrelated to their child’s disability. The mean scores were almost identical at the follow-up (M=10.91, SD=4.78) to those before intervention (M=11.27, SD=5.02); t10=0.48, p=0.640, Cohens’ d=0.07.
Parent’s perception of the intervention 18 months after its completion
Parents of 10 of the 14 children completed the 6 items using the 120 mm horizontal line. Parents of four children declined this part of the follow-up for various reasons, including severe medical disorders in two children. The 95% confidence intervals for the mean ratings on the six items are presented in the visual scale in Figure 2. During the interview, the parents of these 10 children made several comments, eg,
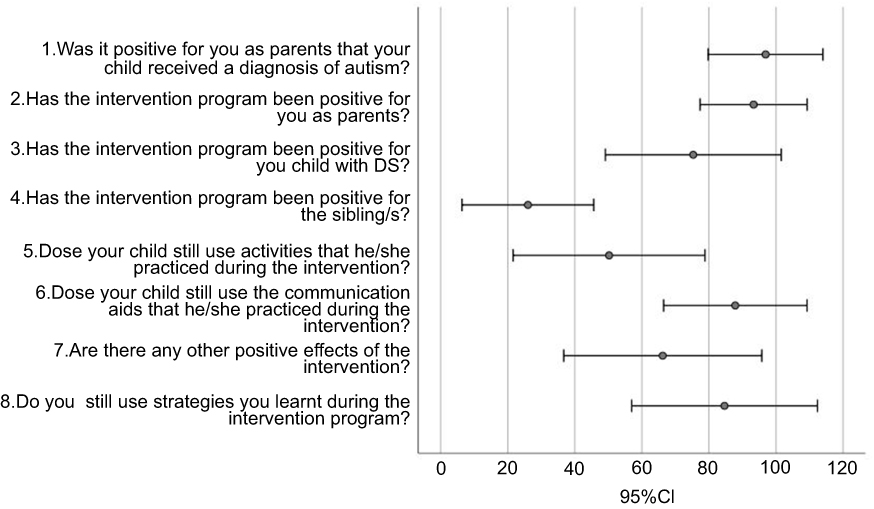 |
Figure 2 Parents’ perception of the intervention 18 months after completion. Scoring: 0= No, not at all/no positive effect; 120= Yes, very much/very positive effect. |
We suspected autism long ago; we are relieved to have it confirmed. Now we can get appropriate help and support”. “Our son is treated in another way now, we understand his behavior better.” “We prepare more before activities. We have a changed mind-set, we don’t have to do things that don’t work, eg, travel while on vacation.” “My worries and stress concerning my child’s behavior and my own short-comings were reduced by the intervention.
Discussion
There are several reports on the effects of behavior modification programs, including ABA, in children with ASD. These have demonstrated positive effects in groups of children, particularly with regard to the reductions of major behavioral problems.14,20 However, IQ and basic autism dysfunctions often remain unchanged or are only marginally positively affected.3,34 The role of intellectual level on the outcome in children with ASD has been pointed out and children with higher initial cognitive levels have been found to have better acquisition of skills and better adaptive functioning outcome.18
The present study aimed at creating an adapted intervention based on ABA for children and adolescents with DS and ASD in addition to ID. A further aim was to analyze the possibility of enhancing performance, communication, participation and well-being in these children, as well as diminishing the family burden.
Clinical experience and research support the value of identifying developmental disorders including autism early on in order to inform parents and staff in the preschool setting about the basic cognitive problems of the child.35 It has also been pointed out that intervention should be performed to improve the situation of the individual and family rather than to cure the underlying disorder.3
The most important finding in the present study was that the children could achieve goals and skills they had not previously managed. Our results demonstrated some improvements in all children. Most children achieved the goals that had been set either fully or to some extent.
The results of the “Family Strain Index” demonstrated that the parents rated the stress and burden of illness correspondingly high at the follow-up to that before the intervention. The FSI score before the intervention was unexpectedly low considering that the children were multi-impaired and therefore substantial improvements were unlikely to be achieved. The parents were aware of their children’s severe disability including ID and had consequently adapted their daily life to the situation in many ways. FSI has mostly been used in studies of intervention in subjects with ADHD. Our results are in agreement with those of Silva et al33 who could not demonstrate any difference in parental scores before and after an intervention in children with ADHD and ASD.
The parents’ perception of the intervention 18 months after study start was generally positive. Almost all parents expressed a sense of relief when they received confirmation that their children also had ASD. Many of the parents had experienced that their child for many years had not been understood. Their child had additional difficulties compared to other children with DS and the parents had felt lonely and insufficient to meet their child’s needs. The evaluation also supported that the use of strategies intended to facilitate activities and communication remained largely 18 months after completion of the intervention.
The results demonstrated that a psychoeducational program can be adapted for schoolchildren with DS and severe or profound ID. We used an approach with a comprehensive psychoeducational program, based on ABA, but to a large extent adapted for older children and teenagers (6–18 years) with DS, ID and ASD. All children had been diagnosed with autism recently. No formal education had been given previously to the parents about autism. The use of a psychoeducational program, adapted to the severity of ID of each child, made it possible to address specific problems of communication and daily activities. To our knowledge no similar research using modified ABA approaches in this patient group of schoolchildren, of whom the majority was teenagers with severe ID, has been reported.
In a review, Moss and Howlin36 highlighted that recognition of ASD-like characteristics (even where a true diagnosis of ASD may not be relevant) in individuals with genetic syndromes is crucial in ensuring appropriate behavioral management and educational placement.
Limitations of the study include the open design in which each child was his or her own control. The small study group and the difficulty in finding appropriate evaluation instruments also represent limitations. Strengths of the study were that the patient group was derived from a population-based cohort of children with DS, that the goals set were adapted to the severity of ID and that the activities were relevant for the daily life of the children and their families.
Conclusion and clinical implications
We conclude that it is possible to create an adapted intervention program based on ABA for older children and adolescents with Down syndrome with coexisting ASD, in the case of severe or profound ID. An intervention, adapted individually and taking the severity of ID into account, seems to be beneficial both for the children and for the parents. Future studies are needed to confirm these results. The study highlights the importance of identifying coexisting ASD in children with DS. An ASD screening program already implemented during preschool age would enable further clinical assessment to be carried out, appropriate information to be given and interventions put in place. It is likely that it would be possible to implement similar adapted intervention programs also for other patient groups with ASD and severe ID.
Acknowledgments
We are grateful to the children and parents who participated in this research. The Sävstaholm Foundation, the Gillberg Foundation and the Uppsala University Hospital Research Fund supported the study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Delabar JM, Allinquant B, Bianchi D, et al. Changing paradigms in down syndrome: the first international conference of the trisomy 21 research society. Mol Syndromol. 2016;7(5):251–261. doi:10.1159/000449049
2. Englund A, Jonsson B, Zander CS, Gustafsson J, Annerén G. Changes in mortality and causes of death in the Swedish Down syndrome population. Am J Med Genet A. 2013;161A(4):642–649. doi:10.1002/ajmg.a.35706
3. Coleman M, Gillberg C. The Autisms.
4. Visootsak J, Sherman S. Neuropsychiatric and behavioral aspects of trisomy 21. Curr Psychiatry Rep. 2007;9(2):135–140.
5. Channell MM, Phillips BA, Loveall SJ, Conners FA, Bussanich PM, Klinger LG. Patterns of autism spectrum symptomatology in individuals with Down syndrome without comorbid autism spectrum disorder. J Neurodev Disord. 2015;7(1):5. doi:10.1186/1866-1955-7-5
6. Warner G, Howlin P, Salomone E, Moss J, Charman T. Profiles of children with Down syndrome who meet screening criteria for autism spectrum disorder (ASD): a comparison with children diagnosed with ASD attending specialist schools. J Intellect Disabil Res. 2017;61(1):75–82. doi:10.1111/jir.12344
7. Oxelgren UW, Myrelid Å, Annerén G, et al. Prevalence of autism and attention-deficit-hyperactivity disorder in Down syndrome: a population-based study. Dev Med Child Neurol. 2017;59(3):276–283. doi:10.1111/dmcn.13217
8. Moss JF. Autism spectrum disorder and attention-deficit-hyperactivity disorder in Down syndrome. Dev Med Child Neurol. 2017;59(3):240. doi:10.1111/dmcn.13261
9. Baird G, Simonoff E, Pickles A, Chandler S, Loucas T, Meldrum D. Prevalence of disorders of the autism spectrum in a population cohort of children in South Thames: the Special Needs and Autism Project (SNAP). Lancet. 2006;368:210–215. doi:10.1016/S0140-6736(06)69041-7
10. La Malfa G, Lassi S, Bertelli M, Salvini R, Placidi GF. Autism and intellectual disabilityt: a study of prevalence on a sample of the Italian population. J Intellect Disabil Res. 2004;48:262–267. doi:10.1111/j.1365-2788.2003.00567.x
11. Matson JL, Shoemaker M. Intellectual disability and its relationship to autism spectrum disorders. Res Dev Disabil. 2009;30(6):1107–1114. doi:10.1016/j.ridd.2009.06.003
12. Wester Oxelgren U, Myrelid Å, Annerén G, Westerlund J, Gustafsson J, Fernell E. More severe intellectual disability found in teenagers compared to younger children with Down syndrome. Acta Paediatr. 2019;108:961–966.
13. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: (DSM-5).
14. Walton KM, Ingersoll BR. Improving social skills in adolescents and adults with autism and severe to profound intellectual disability: a review of the literature. J Autism Dev Disord. 2013;43:594–615. doi:10.1007/s10803-012-1601-1
15. Lovaas O. Behavioral treatment and normal educational and intellectual functioning in young autistic children. J Consult Clin Psychol. 1987;55(1):3–9.
16. Smith T, Eikeseth SO. Ivar Lovaas: pioneer of applied behavior analysis and intervention for children with autism. J Autism Dev Disord. 2011;41(3):375–378. doi:10.1007/s10803-010-1162-0
17. Stevens MC, Fein DA, Dunn M, et al. Subgroups of children with autism by cluster analysis: a longitudinal examination. J Am Acad Child Adolesc Psychiatry. 2000;39(3):346–352. doi:10.1097/00004583-200003000-00017
18. Ben-Itzchak E, Zachor DA. The effects of intellectual functioning and autism severity on outcome of early behavioral intervention for children with autism. Res Dev Disabil. 2007;28(3):287–303. doi:10.1016/j.ridd.2006.03.002
19. Panerai S, Ferrante L, Zingale M. Benefits of the treatment and education of autistic and communication handicapped children (TEACCH) program as compared with a non-specific approach. J Intellect Disabil Res. 2002;46:318–327.
20. Dawson G, Rogers S, Munson J, et al. Randomized, controlled trial of an intervention for toddlers with autism: the Early Start Denver Model. Pediatrics. 2010;125(1):e17–e23. doi:10.1542/peds.2009-0958
21. Schreibman L, Dawson G, Stahmer AC, et al. Naturalistic Developmental Behavioral Interventions: empirically Validated Treatments for Autism Spectrum Disorder. J Autism Dev Disord. 2015;45(8):2411–2428. doi:10.1007/s10803-015-2407-8
22. Vivanti G, Kasari C, Green J, Mandell D, Maye M, Hudry K. Implementing and evaluating early intervention for children with autism: where are the gaps and what should we do? Autism Res. 2018;11(1):16–23. doi:10.1002/aur.1900
23. Wachtel LE, Hagopian LP. Psychopharmacology and Applied Behavioral Analysis: tandem treatment of Severe Problem Behaviors in Intellectual Disability and a Case Series. Isr J Psychiatry Relat Sci. 2006;43(4):265–274.
24. Hedvall Å, Westerlund J, Fernell E, et al. Preschoolers with Autism Spectrum Disorder Followed for 2 Years: those Who Gained and Those Who Lost the Most in Terms of Adaptive Functioning Outcome. J Autism Dev Disord. 2015;45(11):3624–3633. doi:10.1007/s10803-015-2509-3
25. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: (DSM-IV).
26. Gotham K, Risi S, Pickles A, Lord C. The Autism Diagnostic Observation Schedule: revised algorithms for improved diagnostic validity. J Autism Dev Disord. 2007;37(4):613–627. doi:10.1007/s10803-006-0280-1
27. Lord C, Rutter M, Le Couteur A. Autism Diagnostic Interview-Revised: a revised version of a diagnostic interview for caregivers of individuals with possible pervasive developmental disorders. J Autism Dev Disord. 1994;24(5):659–685.
28. Cicchetti DV, Lord C, Koenig K, Klin A, Volkmar FR. Reliability of the ADI-R: multiple examiners evaluate a single case. J Autism Dev Disord. 2008;38(4):764–770. doi:10.1007/s10803-007-0448-3
29. Wechsler D. WPPSI-III. Wechsler Preschool and Primary Scale of Intelligence. Manual, Stockholm: Psykologiförlaget AB; 2005. In Swedish.
30. Harrison PL, Oakland T. ABAS, Adaptive Behavior Assessment System. Manual, San Antonio: Psychological Corporation; 2000.
31. Sparrow SS, Cicchetti DV, Balla DA. Vineland Adaptive Behavior Scales.
32. Riley AW, Lyman LM, Spiel G, et al; ADORE Study Group. The Family Strain Index (FSI). Reliability, validity, and factor structure of a brief questionnaire for families of children with ADHD. Eur Child Adolesc Psychiatry. 2006;15(Supplement 1):i72–i78. doi:10.1007/s00787-006-1010-0
33. Silva D, Houghton S, Jacoby P, Jongeling B, Bower C. Child attention deficit hyperactive disorder co morbidities on family stress: effect of medication. Community Ment Health J. 2015;51(3):347–353. doi:10.1007/s10597-014-9770-3
34. Howlin P, Magiati I, Charman T. Systematic review of early intensive behavioral interventions for children with autism. Am J Intellect Dev Disabil. 2009;114(1):23–41. doi:10.1352/2009.114:23;nd41
35. Sacrey LA, Bennett JA, Zwaigenbaum L. Early infant development and intervention for autism spectrum disorder. J Child Neurol. 2015;30(14):1921–1929. doi:10.1177/0883073815601500
36. Moss J, Howlin P. Autism spectrum disorders in genetic syndromes: implications for diagnosis, intervention and understanding the wider autism spectrum disorder population. J Intellect Disabil Res. 2009;53(1):852–873. doi:10.1111/j.1365-2788.2009.01197.x
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.