Back to Journals » Open Access Journal of Contraception » Volume 14
An Interpretative Study of LARCs Discontinuation in Ethiopia: The Experiences of Women Accessing Contraceptives in Selected Public Health Facilities
Authors Mihretie GS ![]() , Abebe SM
, Abebe SM ![]() , Abera M, Assefa DT
, Abera M, Assefa DT
Received 23 October 2022
Accepted for publication 4 February 2023
Published 17 February 2023 Volume 2023:14 Pages 41—51
DOI https://doi.org/10.2147/OAJC.S394590
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Igal Wolman
Getasew Sisay Mihretie,1 Solomon Mekonnen Abebe,2 Mikyas Abera,3 Daniel Tadesse Assefa4
1Department of Obstetrics and Gynecology, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Sociology, College of Social Sciences and the Humanities, University of Gondar, Gondar, Ethiopia; 4Monitoring Evaluation Research and Quality(MERQ) Consultancy PLC, Addis Ababa, Ethiopia
Correspondence: Solomon Mekonnen Abebe, University of Gondar, P.O.Box 196, Gondar, Ethiopia, Email [email protected]
Background: Discontinuation of contraception for reasons other than wanting to become pregnant is a public health concern as it affects women’s autonomy in sexual and reproductive health decision making as well as gender equality. Studies identified various factors, including community perception and users’ dissatisfaction that limited the reach and impact of contraceptives, primarily LARCs, on women’s wellbeing. In Ethiopia, however, the reasons for early discontinuation of LARCCs are not adequately explored. Against this backdrop, this study explores the main reasons for the early discontinuation of LARCs among Ethiopian women in selected public health facilities.
Methods: This study used an institution-based qualitative study design and covered selected university hospitals and health centers in Addis Ababa, Gondar, Mekelle, and Jimma. It involved in-depth interviews with 29 women aged 15– 49 to gather data and explore the decision-making processes involved in the early discontinuation of LARCs. It used description, narration and thematic interpretation as data analysis procedures.
Results: Interviewees reported several reasons for early discontinuation of LARCs, including side effects (eg, weight gain/loss, heavy menses, tiredness, and reduced libido), desire to conceive, and husbands’ disapproval. This study found that women were sufficiently aware of alternative contraceptives, including LARCs. Many reported experimenting before deciding on an option. Conversely, others’ reports reveal the influences of gender roles and community misconceptions on women’s decisions to discontinue LARCs.
Discussion and Implications: The common threads in interviewees’ narratives highlight the significance of traditional values, gender roles, community perception, and experience with side effects to women’s early discontinuation of LARCs. This study concludes with remarks on how to improve the effectiveness of family planning programming by adopting the gender transformative approach (GTA) in their design and implementation.
Keywords: contraceptive, LARCs, early discontinuation, institution-based qualitative study
Introduction
Globally, 90% of abortions happen due to unintended pregnancy, and in the remaining cases, it results in increased adverse maternal and infant health and socioeconomic outcomes.1,2 Increasing access to effective contraceptives could mitigate this pressing global public health problem to a greater extent.3–8
In 2019, 76% of women of reproductive age (15–49) met their family planning needs with modern contraceptive methods.9 Amongst these, almost equal percentages use Long-Acting (45.2%) and Short-Acting (46.1%) contraceptives, while the remaining (8.7%) use traditional methods. Sub-Saharan Africa has a general contraceptive prevalence rate of 28%, with injectables being the dominant method (9.6%) and IUDs and Implants accounting for less than 5% - even though LARCs are arguably the most effective method against unwanted pregnancy and their possible bad outcomes.2,7,10,11
Authorities argued these advantages of LARCs should make them clear favorites among women with family planning needs. On the back of this, multilateral organizations (eg, WHO) and governments of developing countries promote LARCs as effective strategies to implement family planning programs in the context of their unmet contraceptive needs, limited resources, and high fertility rates.10,12
Using LARCs reduces users’ visits to health providers to restock supplies, and implants and IUDs are usable for almost all women, though this does not mean these methods are first choices for all women.13,14 A woman could eliminate adherence and user dependence from the contraceptive effectiveness equation with a single act of motivation for long-term use.14,15 Though the availability of LARCs has improved significantly over the years, their adoption has only improved slightly while their early discontinuation remains consistently high.5,9,14–24 Studies show early discontinuation is specifically high among users who practice contraception without sufficient knowledge that may result in considerable misinformation and, in turn, dissatisfaction.25,26 And, the discontinuation of LARCS for reasons other than wanting to become pregnant is a public health concern as it contributes to unplanned pregnancies, unwanted births, and unsafe abortions.27–29 On the other hand, comprehensive information about contraception shapes women’s contraceptive decision making abilities and behaviors.30 It is critical for users to consult with healthcare providers in choosing suitable contraception to ensure their successful adoption.18,31–34 Conversely, poor interactions with healthcare providers may increase users’ dissatisfaction with and discontinuation of services.35–38
In 2019, the prevalence of modern contraceptive use among Ethiopian women of reproductive age (15–49) was 41.4%.31,39 There is significant variation among regions and localities (urban versus rural) and women’s characteristics, including age, partner’s education, household wealth, number of children, and exposure to family planning information.40 Injectables are the most popular choice among these women (27%). Implants and IUDs account for 9% and 2% of contraceptives used with 11% and 9% discontinuation rate over 12 months, respectively.41,42 The Ethiopian government stresses improving LARCs accessibility as a strategy to improve maternal health and achieve the Sustainable Development Goals.43 Though health promotion programs advocate LARCs for their efficacy with little demand for strict user compliance, studies reported the tendency among health providers to force LARCs on users has been criticized to contradict the right based family planning approach.44,45 Family planning service providers should focus on the fertility intention of women and LARC side effects when counseling women for choice of contraceptives.46,47 Health promotion programs and agents should target the promotion of gender equality and improving women’s autonomy in sexual and reproductive health decision making, which arguably increase their access to proper and effective contraceptives and other health services thereby increasing their social, economic, and political roles, and personal development.48–51
With few and fragmented studies,32,52,53 relevant, empirical and nuanced discussions on Ethiopian women’s personal experiences with LARCs in the context of cultural, structural and institutional factors remain insufficient and insignificant. It is against this backdrop that this study explores the lived experiences of 29 women from four major urban centers of Ethiopia who discontinued LARCs within 12 months of initial use and interprets their developing narratives on contextual factors.
Methods and Procedures
Study Design
This study is part of a broader study that employed an institution-based, multi-centered follow-up study design. It employed a phenomenological approach to explore and interpret the lived experiences of women who discontinued LARCs within 12 months following method initiation. The authors conducted the fieldwork between March 2017 and December 2018.
Study Area, Population, Sampling Procedure
This study involved 29 women in the reproductive age (15–49) who access family planning services in health centers located in four urban centers of Ethiopia: Addis Ababa (St. Paul’s Hospital, and four health centers), Gondar (Comprehensive Specialized Hospital of the University of Gondar, and four health centers), Mekelle (Ayder Referral Hospital and four health centers) and Jimma (The Teaching Hospital of Jimma University, and four health centers).
It specifically focused on users who, after initiation, discontinued LARCs within 12 months. The actual interviewees were identified from the health facilities’ registers of users who discontinue LARCs during the follow-up period. After excluding women who still use LARCs, 32 potential participants were purposefully selected for an in-depth interview, representing evenly the four urban centers. During data collection, authors found that while 2 potential participants could not avail themselves, 1 provided a faulty or obsolete contact address. After 3 attempts, interviews with the 3 were abandoned. As a result, the data that informs this article drew on transcripts of 29 in-depth interviews.
Data Collection, Management, and Analyses
The authors conducted all in-depth interviews using a guide with unstructured question items. It contains sections with informed consent, introduction, research questions on interviewees’ experiences with LARCs and discontinuation, and wrap-up. The guide was developed in English first, and competent language experts translated it into three local languages, ie, Amharic, Oromiffa, and Tigrigna.
Interview settings were identified in consultation with – at the convenience of interviewees – to promote rapport, freedom of expression, and privacy. All interviews were conducted within one week following user discontinuation. All interviews were conducted in the selected health facilities. All interviewees provided written consent to participate in the study, and their conversations were audio-recorded. For each interview session, an assistant accompanied the interviewer to take note of interviewees’ remarks, anecdotal expressions, and gestures that fed into a thick description of women’s lived experiences.
At the end of each interview, interviewers and assistants discussed the session and complete an interview schedule with reflections on its completeness, consistency, and recommendations for subsequent sessions. Audio recordings were transcribed verbatim in the language used for the interview and translated into English by competent language experts.
The English transcripts were imported to NVivo (v.12) software. The authors read and coded the transcripts using a combination of research questions and core themes that emerged from interview schedules. The coding process was iterative, whereby the authors discussed and refined codes from the initial seven transcripts. The coding of the remaining 22 transcripts used the coding template. A series of iterative and inductive coding produced a final list of codes, which the authors organized under five main abiding concerns: knowledge, preference, attitude, early discontinuation, myths, and realities.
Using these themes, authors conducted detailed descriptive write-ups with extended quotations and moderated code synthesis, which they frequently verified through recursive readings of transcripts, codes, and interview schedules.
Results
This section presents the results of the qualitative descriptive analyses of 29 in-depth interviews with women aged 15–49 under two subsections: (a) awareness and use of contraceptive use, as contraceptive behavior may largely reflect knowledge on it; (b) reasons for discontinuation of LARCs. Table 1 presents details on the interviewees’ age, location, and type of LARCs discontinued.
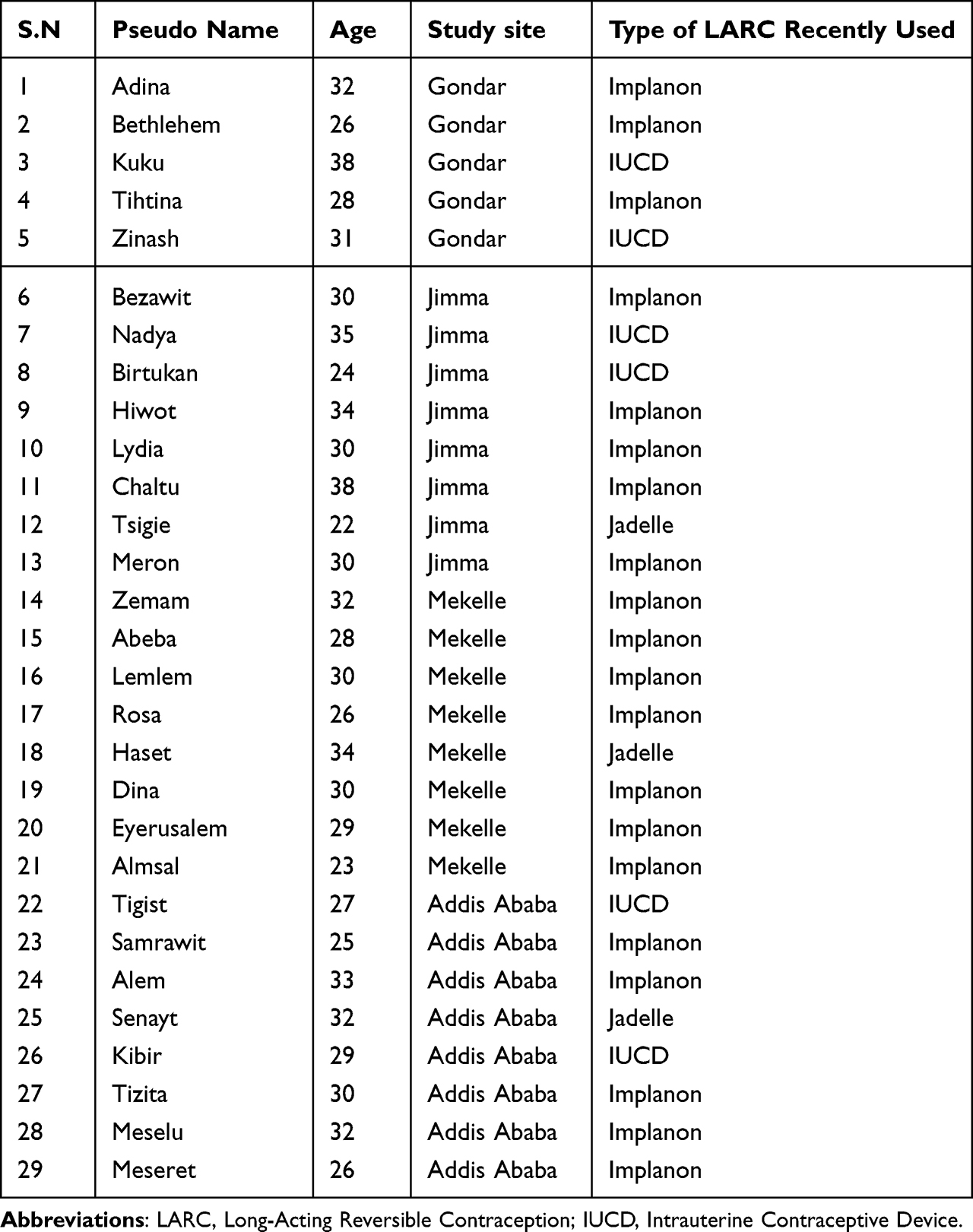 |
Table 1 Interviewees’ Sociodemographic Profiles |
Awareness and Use of Contraceptive Methods
Study participants were reportedly aware of the uses and options of various family planning methods. All could identify at least one contraceptive method, and most could describe the duration of action/efficacy or mode of administration of several modern contraceptive methods. For instance, Meseret (26, Addis Ababa) states,
To prevent unwanted pregnancy, women can choose among several family planning methods. I know loop [Copper IUD], and I do not specifically know their names, but others can be used for three months or three years. The ones used for three months and three years are spacing methods, and loop [Copper IUD] is the best option if women do not want to have babies anymore.
While injectables (which interviewees refer to variously as “the one used for three months”, “injectable” or “Depo”) are the most frequently mentioned contraceptive, a few interviewees identified Copper IUD, implant, oral contraceptives, and condoms as family planning methods available for use.
Some interviewees were able to identify as well as classify contraceptive methods in terms of their primary purposes:
If a mother wants to take good care of her children, the spacing contraceptive method is advisable. If she does not want a child or has enough children and wants to avoid pregnancy, tubal ligation is the best option. But she has other options in the loop [Copper IUD] or implant. For example, from my experience, I have been using implants after I gave birth to my child…. Now my child has grown, and I am removing it to get pregnant (Abeba. 28, Mekelle).
Lemlem (30, Mekelle) concurs with Abeba (28, Mekelle):
If a mother plans to space pregnancy, she can use loop [Copper IUD] and that of 5 years Jadelle implant. For a mother who would like to stop giving birth, tubal ligation is her best option.
But a few interviewees expressed mistaken views about specific contraceptive methods. For example, Meseret (26, Addis Ababa) identified Copper IUD as preferable for women who want a contraceptive with a permanent effect. Others thought implants limit childbirth and IUD avoid pregnancy permanently (eg, Birtukan. 24, Jimma), and Depo Provera closes the cervix and causes infertility. For instance, Hiwot (34, Jimma) explains,
To space pregnancies, a woman can use contraceptives. To avoid pregnancy, she should use Depo. But if taken for an extended period, Depo will close the cervix. I gave birth ten years ago, and I started using Depo. But my friends told me it causes infertility. Then, I immediately shifted to implant.
Interviewees were variedly aware of LARCs. Meseret (26, Addis Ababa) described LARCs as “the methods that do not require checking with health professionals for an extended time after use.” Informed about the advantages and disadvantages, many consider LARCs a reliable and trusted method to avoid unwanted pregnancy. Samrawit (25, Addis Ababa) elaborates,
LARCs have several advantages. For example, loop [Copper IUD] does not have hormonal effects. If I want to conceive, I can remove it and conceive immediately. I do not see any disadvantage except a few irregular menses, which accumulate blood. I do have concerns about this…. [Conversely,] you may forget to use short-acting methods, and unwanted pregnancy may occur. But with implants, there is no such worry…. Previously, I used to take Depo/injection. I experienced difficulty in conceiving after I stopped it.
Eyerusalem (29, Mekelle) compares LARCs with Depo (injection) and says,
I used Depo (injection) before and gained 5kg within three months. My menses were irregular, and I was usually a nervous wreck. I used to fight a lot with my husband as well. Implanon has been comfortable for me…. I hear from friends that Depo will cause infertility. It has not been my personal experience. Overall, I think it’s better to consult health professionals about [options and] concerns.
Several reports also show interviewees’ awareness of when and why to use LARCs. For instance, Adina (32, Gondar) says, “Couples should use these methods if they want to stay for a long period, or if they want to complete certain tasks and they think having a child may be difficult before doing the task. The task can be business, education, building a house.” She identifies Copper IUD as advisable for couples who plan to limit childbirth.
About implants, for instance, Meseret (26, Addis Ababa) comments, “One of my friends has been using it for about ten years now. And implants prevent pregnancy for 3 or 5 years.” Comparatively, interviewees’ awareness of IUDs was relatively poor. Most interviewees could describe the correct site of administration and duration of action of implants, but when it comes to IUDs, they struggle:
I do not know about IUDs. But I know about a contraceptive inserted under the arm. And that’s what I have been using for one year now. It had side effects like menstrual disorders and headaches. Implants can serve for three years, but I do not know for how long IUDs can be used (Zinash. 5, Gondar).
There are observable variations in interviewees’ awareness and knowledge of different contraceptive methods and their uses, administration, and duration, on the one hand, and access to adequate and effective family planning education and messaging, personal experimentation, and community awareness. Several interviewees shared misgivings, including, for instance, that implants serve only for three years, Copper IUDs serve for a lifetime, etc. A few other interviewees misunderstood the duration of action of LARCs, especially IUD: “The one [Copper IUD] inserted under the arm serves for three- or five years”, says Bethlehem (26, Gondar). Chaltu (38, Jimma) adds, “[implant] under the arm and inside the uterus are LARCs. Implant under the arm can serve for up to five years. I do not know about [implant] in the uterus and for how long it serves.”
Many interviewees based their contraceptive choices on personal experimentations, information from health professionals, or opinions from friends and acquaintances’ personal experiences. For instance, Tigist (27, Addis Ababa) decided on an option after consulting with “health providers [who] informed me about many available options.” Alem (33, Addis Ababa) tells how she “had misgivings about IUD because people were talking about its difficulty. It was frightening.” Birtukan (24, Jimma) experimented with IUD, though she discontinued it early as her husband disliked the discomfort it created during sexual intercourse. Before she opted for IUD, Senayt (32, Addis Ababa) experimented with various options:
I have two children…. After my firstborn, I started using Depo/injection. It caused massive vaginal bleeding. After 3 months, I stopped it and started using pills instead. The main side-effect of pills was the severe stomachache. Finally, providers advised me to use IUD.
With LARCs, though interviewees appreciate their stress-free use, their lengthy duration has caused marital discord, which, for Abeba, resulted in “my separation from my husband.” Abeba and Hiwot experienced health problems related to LARCs, which led to their decision to discontinue. When asked if they will ever use LARCs, Hiwot (34, Jimma) says, “Yes, if my condition improves”, and Abeba (28, Mekelle) retorts, “It threatened my health. I give priority to my health. I don’t plan to use it again”. And then she implored, “Are you joking?! I will never use it again!”
Reasons for Early Discontinuation of LARCs
Women could discontinue LARCs early for various reasons, ranging from weight gain/loss, heavy menses, tiredness, reduced libido, and marital discord to the desire to conceive. A combination of these factors could induce early discontinuation, as Rosa’s case illustrates: “Many discontinue [LARCs] when they experience uncomfortable side effects like weight gain, weight loss, and heavy menses. I decided to discontinue because I was feeling tired at work. [I] wanted to conceive too” (Rosa. 26, Mekelle)
Senayt (32, Addis Ababa) situates early LARCs discontinuation within the context of many more others who did the same:
Women discontinue contraceptives if they feel uncomfortable I mean, if they experience melanism, acne, or weight change, they will not keep using it…. I decided [to discontinue LARCs] when I could not have menses for a very long time. It felt uncomfortable to the extent that I did not feel like a woman. Moreover, I wanted to have a baby too.
Chaltu (38, Jimma) explained the health effects of implants that forced her to discontinue early:
I was sick while using it [implant]. My frequency and urgency to urinate increased. I also felt inflammation when I release myself. I gradually grew febrile. I am a daily laborer, and it was not comfortable for me. The implant used to make me nervous. The pain in that part of the arm was unbearable, especially when trying to lift heavy objects at work.
Hiwot (34, Jimma) discussed how her neighbor discontinued implants as she started “losing hair and weight and displaying abnormal behaviors” while using them. She continues,
She was glad to discontinue it…. [As to me,] I decided to remove the implant when I felt its side-effects – numbness in my upper extremities, headache, fatigue, and increased blood pressure.
Bezawit (30, Jimma) was very elaborate on the decision-making and early LARCs discontinuation processes:
[Some] contraceptives might not be suitable for some women. Their body weight might change significantly, or menstrual bleeding may be frequent. When this happens, they may discontinue its use. I knew a woman who used insertion [implant] under the arm. She removed it, for, she said, it caused frequent menstrual bleeding. Then she shifted to injection [Depo Vera] immediately. Since the injection, none of the side-effects of insertion [implant] occurred…. I decided to remove it due to its side effects – loss of appetite and change of behavior. After I started using injections, there were improvements, and my body recovered.
Though many interviewees stressed side effects as the main reasons for their early discontinuation of LARCs, not too few others ended their exposition with an “I also wanted a baby” remark. Several women who discontinued LARCs early claim to obtain superficial information on the use, duration, and requirements of LARCs from health providers. For instance, Chaltu (38, Jimma) was not cautioned against heavy lifting during the few days following the implants. Chaltu (38, Jimma) and other interviewees claim health centers usually advocate LARCs to all women with family planning needs without detailing the side effects and precautions users must take. Interviewees (eg, Bethlehem (26, Gondar), Haset (34, Mekelle), Dina (30, Mekelle), and Hiwot (34, Jimma)) were also critical of LARCs users who do not genuinely engage with counselors to evaluate and match their contraceptive needs with available options and soon discontinue or switch.
Many women experimented with different contraceptive methods before settling for the most convenient option.
Several interviewees stressed the impact husbands could have when and if they were involved in the discussion on family planning with providers – which could reduce the prevalence of early discontinuation of LARCs due to external pressures. Lemlem (30, Mekelle) explains,
My husband did not know that I began using implants. I was comfortable with the implant. He found out after four months. He got angry and started nagging me to remove it, which continued until I finally gave in. I had to remove it because of my husband. He came with me to the health facility. He complained that he does not know anything about the implant, and threatened to sue them if they do not remove it immediately.
Lemlem’s husband forced the early removal because “he wanted a child.” Her remark that she may use implants in the future “if I can convince my husband” (Lemlem. 30, Mekelle) taps into the patriarchal values that undermine women’s independence and control over their bodies and reproductive health rights.
Underlying these findings are community values, myths, and beliefs that affect contraceptive use or discontinuation. Senayt (32, Addis Ababa) says there are rumors “that implants make a woman weak and unattractive to her husband [due to excessive acne on the face], and most users will end up divorcing.” Hiwot (34, Jimma) adds, “people say it can cause permanent baldness. Implants may be lost in the arm, leading to infertility.” Dina (30, Mekelle) elaborates on the sources and impacts of community myths and beliefs about contraceptives:
People in our area have concerns about LARCs. Some people believe that IUDs may migrate to the abdomen - and even to the brain - due to sexual activity. Others say IUDs may dislodge if a woman engages in sex multiple times a night. The popular opinion about implants is they will be lost in the arm if done immediately after delivery.
These myths and beliefs also link contraceptive displacement with infertility, breast cancer, etc. The myth that LARCs could cause infertility creates, Adina (32, Gondar) comments, “community misconceptions that lower contraceptives use.” She continues, “[My] community values children as gifts of God”, and using contraceptives implies refusing God. Whenever a woman struggles to conceive, Bethlehem (26, Gondar) comments, community myths associate it with her history of contraceptive use. For Zemam (32, Mekelle), the interaction between religion and myths creates a powerful barrier to contraceptive use, especially of LARCs: “My religion forbids contraceptives, and there are also myths that once you use them, you will remain sterile (infertile) forever.”
Access to quality and relevant health information has helped many interviewees to dispel their community fears and myths about contraceptive use. For instance, Samrawit (25, Addis Ababa) reiterates,
Some of my friends advised me against using an implant. They say it causes breast cancer, and I should remove it. I consulted health providers who assured me these claims are unfounded….
In other words, evidenced information on family planning, framed in culturally sensitive formats, could improve how women and their significant others view and use contraceptives. But as myths and beliefs are embedded in people’s cultures and psyches, they may prove resistant to dramatic changes. Community health education and practices must be relevant to the people for impact.
Discussion
The results of the qualitative study underlined the relevance of cultural and institutional factors as well as user experience, desire to conceive, and partner opposition in the use, compliance, or discontinuation of contraceptives in general and LARCs in particular among sexually active women in Ethiopian urban centers. It explored the lived experiences of women who discontinue LARCs to document how contraceptives’ actual or perceived side effects affect women’s choices and experiences. In this regard, the results confirm several studies.17,18,23
Women base their contraceptive choices on personal experiments, family and friends, religious and community values, and health providers. Partners reportedly play significant roles in women’s decision to discontinue LARCs. At times, health professionals encouraged women to consult with their partners regarding contraceptive use. Living in a patriarchal society with conservative values about their sexuality, women might find it difficult to decide unilaterally on childrearing or contraceptive use. Marriage is the union of a man and a woman in husband-and-wife roles – with the man’s roles defined in broader terms of household management and decision-making. A patriarchal culture also treats a childless marriage as an incomplete family. The purpose of family is procreation, whereby virility and fertility are stressed, and sexual satisfaction is only secondary to this social role. Children are gifts of God, and more children mean more grace – and improved status and prestige in the eyes of the community. In light of this, health providers and family planning counselors should intentionally engage husbands and partners to critically reflect, challenge, and transform unbalanced gender roles and empower women over their reproductive rights. Their intervention should incorporate an explicit gender transformative approach while involving women and their partners in the decisions over family planning choices and harnessing men’s agency towards gender equality. This approach involves examining the roles of patriarchal relations in women’s and men’s health, reshaping men’s values, attitudes, and practices, and constituting men as part of the solution rather than the problem. Otherwise, as interviewees’ experiences show, in a largely patriarchal society like Ethiopia, where women’s sexuality is defined primarily in their ability to procreate, a unilateral decision to use contraceptives could cause intimacy discord, family instability, disorganization, and dissolution.
Contraceptives hinder this traditional goal for marriage and family, and husbands could easily see them as undermining – and this is due to the prevailing unbalanced gender roles and entrenched patriarchy. Health service and family planning interventions should integrate a gender-transformative approach to their programming. Gender transformative health programming focuses on transforming the power dynamics and structures that serve to reinforce gendered inequalities in access to health services – rather than singularly targeting individualized self-improvement services to women.54–57 It involves gender-based analysis of communities to understand how health behaviors reflect cultural differences between men and women, especially regarding power and decision-making. Based on this understanding, it delivers appropriate gender sensitivity training to health providers and builds the capacity of health centers to encourage contraceptive users, partners, and communities to reflect critically on how gender norms and harmful gender stereotypes affect the well-being of women, children, partners, families, and communities. Gender transformative programming in family health specifically challenges and transforms unequal gender and power relations and promotes gender equality, in addition to their specific health outcomes of empowering women on their reproductive rights and improving maternal and child health.
Gender transformative programming typically involves participatory processes whereby individuals and communities participate and promote positive, more equitable behaviors and norms. It aims, when possible, to transform the underlying norms, structures, and policies that sustain inequality in reproductive health rights and women women’s access to effective family planning services.58 More importantly, the success of this approach requires effective intersectoral collaborations at higher government (between the Ministry of Health, Ministry of Women and Child Affairs, and Ministry of Education) and programming (between family health providers and gender equality and women’s rights projects) levels. Entrenched patriarchal gender norms, myths, and misconceptions about contraceptives require the broader and more effective dissemination of evidence-based, culturally appropriate, and accessible family planning information. Program planning and implementation could face resistance as advocacy for gender-transformative change threaten existing power structures and dynamics from some corners.54
Early discontinuation of LARCs could partially relate to health providers’ advocacy for LARCs that did not match their family planning needs. Health centers and providers should consult users on their family planning options, benefits, side effects, duration of use, compliance requirements, etc. In the current study and other studies (e.g,18,24 prior consultation with health providers has improved user decision-making and compliance. The GATHER approach to counseling--Greet, Ask, Tell, Help, Explain, and Return—which has documented effectiveness in family planning programs, is associated with more satisfied clients who are more likely to use contraception.59 Health counseling may not automatically empower women about their reproductive health rights and choices, though these outcomes should drive its processes. It primarily creates a safe and engaging platform for women to discuss their needs and concerns with professionals and to dispel and replace their worries and fears with assurances and reliable information. As such, it should be participatory and informed by women’s needs rather than the availability of methods or, as the national health policy alludes, strategic priorities.43 Their aim, thus, should be improving users’ awareness and knowledge of their options, uses, side effects, etc. Practice makes a habit, and both depend on attitude, and appropriate and scientific messaging to dispel misperceptions and myths about contraceptives. In a society with a strong sense of community, knowledge gaps about contraceptives are not always filled with scientific information but also rumors and gossip.
Strengths and Limitations
Both the strengths and limitations of this study are mainly related to the qualitative method it employed. The strengths lay in the in-depth and contextual information the study gathered on women that enriched the understanding and interpretation of circumstances and decision-making processes on the use and/or discontinuation of LARCs. With its scope delimited to the women in the selected urban centers, the findings could not represent the experiences of women in rural areas and other urban centers on their choices related to contraceptives in general and LARCs in particular.
Data Sharing Statement
We have to abide by the data sharing policy of the University of Gondar; nonetheless, we have included all important information regarding the data presented (No additional data are available).
Ethics Approval and Consent to Participate
The Institutional Ethics Board of the University of Gondar reviewed and declared the study to meet the required ethical standards involving humans. Before commencing each interview, interviewers informed study participants about the study’s purpose and their participation and solicited their informed written consent. Interviewers obtained informed consent for participants under 18 from themselves (verbal assent) and their parents or legal guardians (written consent). Interviewers informed participants that they will not face harm or be publicly identified. They clarified the terms of confidentiality in data management and publications, the use of pseudonyms and passcode to participants. The study complies with the Declaration of Helsinki.
Acknowledgments
The authors are very grateful for the funding provided by CIHRT to conduct this study with full support which included the training of every study participant at each step of the study, for this, we have no words to thank this organization. We would like to acknowledge the study participants.
Author Contributions
All authors (GSM, SMA, MA, and DTA) had contributed to the ideation, design and execution of the study as well as the acquisition, analysis and interpretation of data. All had been involved in drafting, revising and reviewing this manuscript. All had agreed on the journal to which the article will be submitted as well as its versions before submission, and during revisions. They all agree on the final version of the article accepted for publication and, if any changes are introduced at the proofing stage, to take responsibility after approval and be accountable for its contents.
Funding
CIHRT and the University of Gondar.
Disclosure
The authors have stated explicitly that there are no conflicts of interest in connection with this article.
References
1. Hellerstedt WL, Pirie PL, Lando HA., et al. Differences in Preconceptional and Prenatal Behaviors in Women with Intended and Unintended Pregnancies. Am J Public Health. 1998;88(4):663–666.
2. Yazdkhasti M, Pourreza A, Pirak A, Abdi F. Unintended Pregnancy and Its Adverse Social and Economic Consequences on Health System: a Narrative Review Article. Iran J Public Health. 2015;44(1):12–21.
3. Say L, Chou D, Gemmill A, et al. Global causes of maternal death: a WHO systematic analysis. Lancet Global Health. 2014;2(6):e323–33.
4. Blanc AK, Curtis SL, Croft TN. Monitoring Contraceptive Continuation: links to Fertility Outcomes and Quality of Care. Stud Fam Plann. 2002;33(2):127–140.
5. Cleland J, Ali MM. Reproductive Consequences of Contraceptive Failure in 19 Developing Countries. Obstet Gynecol. 2004;104(2):314–320.
6. Gipson JD, Koenig MA, Hindin MJ. The Effects of Unintended Pregnancy on Infant, Child, and Parental Health: a Review of the Literature. Stud Fam Plann. 2008;39(1):18–38.
7. Winner B, Peipert JF, Zhao Q, et al. Effectiveness of Long-Acting Reversible Contraception. N Engl J Med. 2012;366(21):1998–2007.
8. Saleem S, Bobak M. Women’s autonomy, education and contraception use in Pakistan: a national study. Reprod Health. 2005;2(1):1–8.
9. UNDESA. Contraceptives Use by Method. New York: UUnited Nations Department of Economic and Social Affairs, Population Division, Division P;2019. Report No.: 2019: Data Booklet (ST/ESA/SER.A/435).
10. Peterson HB, Curtis KM. Clinical Practice. Long-Acting Methods of Contraception. N Engl J Med. 2005;353(20):2169–2175.
11. Hogberg U. The World Health Report 2005: ‘Make Every Mother and Child Count’ - including Africans. Scand J Public Health. 2005;33(6):409–411.
12. Samuel M, Fetters T, Desta D. Strengthening Postabortion Family Planning Services in Ethiopia: expanding Contraceptive Choice and Improving Access to Long-Acting Reversible Contraception. Global Health Sci Practice. 2016;4:S60–72.
13. Potter JE, Stevenson AJ, Coleman-Minahan K, et al. Challenging unintended pregnancy as an indicator of reproductive autonomy. Contraception. 2019;100(1):1–4.
14. Law A, Pilon D, Lynen R, et al. Retrospective analysis of the impact of increasing access to long acting reversible contraceptives in a commercially insured population. Reprod Health. 2016;13(1):1–12.
15. Law A, Pilon D, Lynen R, et al. Retrospective Analysis of the Impact of Increasing Access to Long Acting Reversible Contraceptives in a Commercially Insured Population. Reprod Health. 2016;13(1):96.
16. Moreau C, Cleland K, Trussell J. Contraceptive Discontinuation Attributed to Method Dissatisfaction in the United States. Contraception. 2007;76(4):267–272.
17. Harvey C, Seib C, Lucke J. Continuation Rates and Reasons for Removal among Implanon Users Accessing Two Family Planning Clinics in Queensland, Australia. Contraception. 2009;80(6):527–532.
18. Garbers S, Haines-Stephan J, Lipton Y, Meserve A, Spieler L, Chiasson MA. Continuation of Copper-Containing Intrauterine Devices at 6 months. Contraception. 2013;87(1):101–106.
19. Mansour D, Bahamondes L, Critchley H, Darney P, Fraser IS. The Management of Unacceptable Bleeding Patterns in Etonogestrel-releasing Contraceptive Implant Users. Contraception. 2011;83(3):202–210.
20. Andersson K, Odlind V, Rybo G. Levonorgestrel-releasing and Copper-releasing (Nova T) IUDs During Five Years of Use: a Randomized Comparative Trial. Contraception. 1994;49(1):56–72.
21. Sznajder KK, Tomaszewski KS, Burke AE, Trent M. Incidence of Discontinuation of Long-Acting Reversible Contraception among Adolescent and Young Adult Women Served by an Urban Primary Care Clinic. J Pediatr Adolesc Gynecol. 2017;30(1):53–57.
22. Peipert JF, Zhao Q, Allsworth JE, et al. Continuation and Satisfaction of Reversible Contraception. Obstet Gynecol. 2011;117(5):1105–1113.
23. O’Neil ME, Peipert JF, Zhao Q, Madden T, Secura G. Twenty-Four-Month Continuation of Reversible Contraception. Obstet Gynecol. 2013;122(5):1083–1091.
24. Modesto W, Bahamondes MV, Bahamondes L, Randomized Clinical A. Trial of the Effect of Intensive versus Non-intensive Counselling on Discontinuation Rates due to Bleeding Disturbances of Three Long-Acting Reversible Contraceptives. Human Reproduction. 2014;29(7):1393–1399.
25. Valente TW, Paredes P, Poppe PR. Matching the message to the process: the relative ordering of knowledge, attitudes, and practices in behavior change research. Hum Commun Res. 1998;24(3):366–385.
26. Hall KS, Castaño PM, Westhoff CL. The influence of oral contraceptive knowledge on oral contraceptive continuation among young women. J Womens Health. 2014;23(7):596–601.
27. Starbird E, Norton M, Marcus R. Investing in family planning: key to achieving the sustainable development goals. Global Health. 2016;4(2):191–210.
28. Blumenthal PD, Voedisch A, Gemzell-Danielsson K. Strategies to prevent unintended pregnancy: increasing use of long-acting reversible contraception. Hum Reprod Update. 2011;17(1):121–137.
29. Blanc AK, Curtis SL, Croft TN. Monitoring contraceptive continuation: links to fertility outcomes and quality of care. Stud Fam Plann. 2002;33(2):127–140.
30. Lopez LM, Tolley EE, Grimes DA, Chen-Mok M. Theory-based strategies for improving contraceptive use: a systematic review. Contraception. 2009;79(6):411–417.
31. GebreMedhin T, GebreKidan KG, Nerea MK, Gerezgiher H, Haftu M. Early Implanon Discontinuation Rate and its Associated Factors in Health Institutions of Mekelle City, Tigray, Ethiopia 2016/17. BMC Res Notes. 2019;12(1):8.
32. Hrusa G, Spigt M, Dejene T, Shiferaw S. Quality of Family Planning Counseling in Ethiopia: trends and Determinants of Information Received by Female Modern Contraceptive Users, Evidence from National Survey Data, (2014-2018). PLoS One. 2020;15(2):e0228714.
33. Dehlendorf C, Krajewski C, Borrero S. Contraceptive counseling: best practices to ensure quality communication and enable effective contraceptive use. Clin Obstet Gynecol. 2014;57(4):659.
34. Schivone GB, Glish LL. Contraceptive counseling for continuation and satisfaction. Curr Opin Obstet Gynecol. 2017;29(6):443–448.
35. Evaluation M. Quick investigation of quality (QIQ): a user’s guide for monitoring quality of care in family planning. Stud Fam Plann. 2016;1:878.
36. Mack N, Crawford TJ, Guise JM, et al. Strategies to improve adherence and continuation of shorter‐term hormonal methods of contraception. Cochrane Database Sys Rev. 2019;4:548.
37. Diamond-Smith N, Warnock R, Sudhinaraset M. Interventions to improve the person-centered quality of family planning services: a narrative review. Reprod Health. 2018;15(1):1–17.
38. Yirgu R, Wood SN, Karp C, Tsui A, Moreau C. ”You better use the safer one. leave this one”: the role of health providers in women’s pursuit of their preferred family planning methods. BMC Womens Health. 2020;20(1):170.
39. Ethiopian Mini EDHS. Demographic and Health Survey 2019: Key Indicators Rockville. Maryland, USA: Ethiopian Demographic and Health Survey: Ethiopian Public Health Institute (EPHI) and ICF; 2019.
40. Tegegne TK, Chojenta C, Forder PM, Getachew T, Smith R, Loxton D. Spatial Variations and Associated Factors of Modern Contraceptive use in Ethiopia: a Spatial and Multilevel Analysis. BMJ Open. 2020;10(10):1–10.
41. Central Statistical Agency - CSA/Ethiopia, ICF. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia: CSA and ICF; 2017.
42. Ethiopian Public Health Institute - EPHI, Federal Ministry of Health - FMoH, ICF. Ethiopia Mini Demographic and Health Survey 2019. Addis Ababa, Ethiopia: EPHI/FMoH/ICF; 2021.
43. MoH. National Guideline for Family Planning Services in Ethiopia. Vol. 2019. Addis Ababa: Ministry of Health of the Federal Democratic Republic of Ethiopia; 2020.
44. Corley A, Sprockett A, Montagu D, Chakraborty N. Exploring and Monitoring Privacy, Confidentiality and Provider Bias in Sexual and Reproductive Health Service Provision to Young People: a Narrative Review. Int J Enviorn Res Public Health. 2022;19(6576):1–22.
45. Rouncivell L, Takuva S, Ledibane N, Musekiwa A, Leong T. Knowledge, Attitudes, and Perceptions of Long-Acting Reversible Contraceptive Methods among Healthcare Workers in Sub-Saharan Africa. Tropical Med Int Health. 2021;26(8):840–861.
46. Fekadu GA, Omigbodun AO, Roberts OA, Yalew AW. Factors associated with early long-acting reversible contraceptives discontinuation in Ethiopia: evidence from the 2016 Ethiopian demographic and health survey. Arch Public Health. 2020;78(1):1–10.
47. Bereku T, Habtu Y, Abreham B, Ayele M, Eliso M. Magnitude and factors for method discontinuation and switching among long acting reversible contraceptive users in health facilities of Southern Ethiopia. Reprod Health. 2022;19(1):1–10.
48. Federation IPP. Sexual and Reproductive Health and Rights–the Key to Gender Equality and Women’s Empowerment. London: International Planned Parenthood Federation (IPPF); 2015.
49. Blanc AK. The Effect of Power in Sexual Relationships on Sexual and Reproductive Health: an Examination of the Evidence. Stud Fam Plann. 2001;32(3):189–213.
50. Kavanaugh ML, Anderson RM. Contraception and Beyond: The Health Benefits of Services Provided at Family Planning Centers. New York: Guttmacher Institute; 2013.
51. Cleland J, Conde-Agudelo A, Peterson H, Ross J, Tsui A. Contraception and health. Lancet. 2012;380(9837):149–156.
52. Asaye MM, Nigussie TS, Ambaw WM. Early Implanon Discontinuation and Associated Factors among Implanon User Women in Debre Tabor Town, Public Health Facilities, Northwest Ethiopia, 2016. Int J Reproductive Med. 2018;2018(3597487):1–10.
53. Wong RC, Bell RJ, Thunuguntla K, McNamee K, Vollenhoven B. Implanon Users are Less Likely to be Satisfied with their Contraception after 6 months than IUD Users. Contraception. 2009;80(5):452–456.
54. Hillenbrand E, Karim N, Mohanraj P, Wu D. Measuring Gender-Transformative Change: A Review of Literature and Promising Practices. USA: CARE USA. Working Paper; 2015.
55. Hay K, McDougal L, Percival V, et al. Disrupting Gender Norms in Health Systems: making the Case for Change. Lancet. 2019;393(10190):2535–2549.
56. WHO. Delivered by Women, Led by Men: A Gender and Equity Analysis of the Global Health and Social Workforce. Geneva: World Health Organization;2019. Report No.: Human Resources for Health Observer Series No. 24.
57. Morgan R, Ayiasi RM, Barman D, et al. Gendered Health Systems: evidence from Low- and Middle-Income Countries. Health Research Policy Sys. 2018;16(1):1–12.
58. Aventin Á, Rabieb S, Skeen S, et al. Adaptation of a Gender-Transformative Sexual and Reproductive Health Intervention for Adolescent Boys in South Africa and Lesotho Using Intervention Mapping. Glob Health Action. 2021;14(1):1–18.
59. Rinehart W, Rudy S, Drennan M. GATHER guide to counseling. Popul Rep J. 1998;48:1–31.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.