Back to Journals » Clinical Interventions in Aging » Volume 20
An Interdisciplinary Approach to Assistive Technology for Parkinson’s Disease Dementia
Authors Munzesheimer S, Siu TWT, Yacinthe D, Garcia-Casals M, Haq IU, Shpiner DS
Received 10 January 2025
Accepted for publication 10 July 2025
Published 15 August 2025 Volume 2025:20 Pages 1253—1265
DOI https://doi.org/10.2147/CIA.S516786
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Maddalena Illario
Video abstract of “Assistive Technology for Parkinson’s Disease” [516786].
Views: 293
Sara Munzesheimer,1,* Tin Wai Tiffany Siu,2,* Dudley Yacinthe,1 Michelle Garcia-Casals,1 Ihtsham ul Haq,3 Danielle S Shpiner3
1Department of Physical Therapy, University of Miami Miller School of Medicine, Miami, FL, USA; 2Department of Otolaryngology, Division of Speech Pathology, University of Miami Miller School of Medicine, Miami, FL, USA; 3Department of Neurology, University of Miami Miller School of Medicine, Miami, FL, USA
*These authors contributed equally to this work
Correspondence: Tin Wai Tiffany Siu, Email [email protected]
Abstract: Parkinson’s Disease Dementia (PDD) and Parkinson’s Disease-Mild Cognitive Impairment (PD-MCI) are common non-motor complications that can manifest as Parkinson’s disease (PD) progresses. Cognitive impairment associated with PDD/PD-MCI can degrade patients’ functional communication, safety, independence in activities of daily living, relationships with others, and increase caregivers’ burden. Assistive Technology (AT) can help the PDD/PD-MCI population and their families to improve daily functioning, safety, and quality of life. This review highlights the breadth, functionality, effectiveness, and utilization of currently available AT in PDD and PD-MCI from an interdisciplinary rehabilitative perspective, including insights from physical therapy, occupational therapy, and speech-language pathology. Some larger AT studies that were reviewed offer meaningful perspectives on realistic patient implementation; however, other AT studies had limitations including small sample sizes, insufficient focus on PDD/PD-MCI population needs, and underrepresentation of patients with cognitive deficits. Nevertheless, this review aims to serve as one of the first interdisciplinary clinical guides for determining appropriate use, timing, and individualized adaptation of AT, allowing clinicians to maximize functional outcomes in the PDD/PD-MCI population. Additional studies are required to gain a deeper understanding of practical application, training, and implementation of AT for individuals with PDD/PD-MCI from an interdisciplinary perspective.
Keywords: mild cognitive impairment, physical therapy, occupational therapy, speech therapy
Introduction
Parkinson’s Disease (PD) is the second most common neurodegenerative disorder in the United States. Early PD is characterized by motor symptoms including rigidity, bradykinesia, resting tremor, and changes in posture and gait.1 The incidence of PD diagnosis is rapidly increasing. In 2010, approximately 680,000 individuals in the United States aged ≥45 years were diagnosed with PD; projections for 2030 are almost double this number.2 A 2022 study revealed that approximately 90,000 people in the United States are newly diagnosed with PD annually, which is 50% higher than previous estimates.3
Parkinson’s Disease Dementia (PDD) is one of the most common non-motor manifestations of advanced PD. It is distinguished mainly by cognitive-linguistic deficits including executive and visuospatial function, attention, and memory.4 Behavioral symptoms including apathy, visual hallucinations and delusions are also common. Dementia with Lewy bodies presents similarly though it has a quicker onset of cognitive symptoms and a lower motor symptom burden.5,6 It is estimated that around 50% of the PD population will develop PDD over their lifetimes, usually later in the disease course.7–10 The risk for developing dementia overall is sixfold higher in people with PD when compared to the general population.11 Dementia in PD is associated with an increase in mortality rates over a ten-year period when compared to control groups without PD.12 PDD commonly results in reduced quality of life, increased caregiver distress, higher risk of falls, and a larger incidence of nursing home placement.13 Milder forms of cognitive impairment are frequently seen in patients with PD. In studies of patients with new PD diagnosis, the prevalence of mild cognitive impairment (MCI) ranges from about 15–40%.14,15 This can be a potential early indicator for the development of PDD and is also associated with diminished quality of life.14
While there is currently no known cure for PD or PDD, therapeutic interventions can assist with improving quality of life, safety, and dignity throughout the disease process. Cognitive deficits are typically not responsive to dopaminergic medications used to treat motor symptoms and may even worsen with such treatment. Pharmacological therapies, such as acetylcholinesterase inhibitors, for cognitive symptoms in PD typically provide only modest benefits and carry risk of side effects.16 Hence, non-pharmacological interventions are of practical relevance for patients and their families, including assistive technology (AT).5 AT emerges in recent literature as a cutting-edge treatment option which can address safety concerns, maximize independence in persons with PDD/PD-MCI and minimize caregiver burden.17
AT can be classified into low-tech, mid-tech, and high-tech products, based on complexity, cost, and required training level. Low-tech ATs have simple mechanical or electric parts. They are typically more affordable and require low levels of training. Examples include walkers, pen or pencil grips, grabbers, nonslip mats, and handheld magnifiers. Mid-tech ATs tend to have electronic or complex features, are more expensive, and may require some additional training. Examples include personal hearing amplifiers, adaptive keyboards or computer mice, reminder alarm clocks, talking calculators, and manual wheelchairs. High-tech ATs are the most complex and costly among all AT devices. They are often computerized and require training for successful utilization. Robotic exoskeletons, power wheelchairs and scooters, digital hearing aids, remote-control devices, voice activated environmental controls, home automation, and dedicated speech generating devices are all examples of high-tech ATs.18
There is widespread consensus that interdisciplinary care is essential for the most effective treatment of PD.19–21 However, PDD can significantly complicate patient access to interdisciplinary care due to a range of factors: caregiver burden, difficulty employing and maintaining intervention strategies, and psychiatric comorbidities such as depression and apathy.22,23 Despite variable terminologies used to represent the different care models, the term “interdisciplinary” will be used in this review to represent the integration of knowledge and methods from different disciplines working together as a unified team.21 Studies support both inpatient and outpatient applications of interdisciplinary care in the PD population for improved quality of life, motor function, balance, and performance in activities of daily living (ADLs) and instrumental activities of daily living (IADLs).19–21 Given the complex interaction of motor, cognitive, and behavioral symptoms in PDD and PD-MCI, an interdisciplinary approach to assistive technology implementation is critical. Our review highlights how such an approach ensures that AT solutions are clinically relevant to caregivers, practitioners, and patients alike.
AT for Exercise, Mobility, and Fall Reduction in PDD and PD-MCI
Patient-specific AT can be instrumental in working towards exercise and mobility goals, while also contributing to reducing fall risk.24 This can be integral in the PDD/PD-MCI populations by reducing mental load, increasing participation and engagement in physical activity, and reducing risk of secondary impairment.25 Physical Therapy (PT) practitioners can prescribe AT to assist with these goals. A comprehensive PT program is often recommended to address PD-related motor and non-motor symptoms, educate patients/caregivers throughout the disease process, and reduce the risk of secondary complications or functional decline.26
Regular participation in exercise is incredibly important within the PD population due to its beneficial effects on neuroplasticity.27 Current research has shown that exercise has the potential to slow the progression of PD, though the mechanism is not yet fully understood.28 The use of monitoring devices and smart phone applications can serve as an exercise reminder and way of tracking fitness goals in patients with memory and attentional impairments. One way to track physical activity using AT is through counting an individual’s number of steps. Applications such as GoogleFIT (Google, Mountainview, CA, USA), STEPZ (Easy Tiger Apps, LLC, Brooklyn, NY, USA), Pacer (Pacer Health, Inc., Hialead, FL, USA), and Health (Apple, Cupertino, CA, USA) as well as an activity monitor, FitBit INC (Google, Mountainview, CA, USA), were found to be valid tools to measure the number of steps in individuals with PD. These tools can promote increased daily physical activity.28 Another study found that patient participation in an 8-week home-based training program using the smart phone exercise application, Parkinson Rehab (Rune Labs, San Francisco, CA, USA), was feasible, safe, and improved participants’ PD-related symptoms, mobility, and cognition.29
AT with visual, auditory, and proprioceptive cues can assist persons with PDD/PD-MCI in combating common motor complications such as freezing of gait (FOG) and difficulty with turns, facilitating patient exercise participation, and decreasing fall risk.30–33 FOG is a brief arrest in forward motion arising from dysfunction of higher-order cortical processing and is therefore more common in people with cognitive impairment.34,35 FOG occurs more often with complex motor tasks including gait initiation, rotation, or walking through narrow spaces. It also worsens with dual tasking, increased stress, and in crowded environments.36 AT with visual cues have shown promising results when compared to AT with other cueing methods such as the sound metronome, vibrating metronome, or walking stick. For instance, the use of a laser cane reduced episodes of freezing and improved walking parameters in persons with PD.30 Another study found that the use of a laser light beam from a cane or walker (ie Ustep (In Step Mobility, Skokie, IL, USA)) contributed to a significant decrease in FOG episodes and frequency of falls as compared to using assistive devices without visual cues. However, it should be noted that participants with cognitive impairment were excluded from the study and benefit among patients with cognitive issues cannot be assumed.31 It is likely that AT requires a certain level of baseline cognitive and motor processing to provide benefit. Additional study will be required to establish such prerequisites during AT use.
Gait speed is an important walking parameter that can predict risk for falls in community dwelling adults.37 However, utilization of AT does not uniformly improve gait speed or stride length in the PD population.38,39 It is the addition of visual and auditory cues that can significantly improve gait speed.39,40 One study found that patients using canes with visual cues (ie laser) or an auditory pacer showed increased gait speed compared to patients using standard canes during the “off” state.38 Please refer to Table 1 for a summary of AT addressing gait parameters and fall risk.39–41 Additional research will be required to delineate the impact of cognitive impairment on AT’s capacity for assistance in PDD/PD-MCI.
 |
Table 1 AT for Mobility and Decreased Fall Risk |
Remote monitoring devices aimed at addressing fall risk within the home also exist. This can be especially beneficial for both individuals with cognitive impairment and their caregivers. These monitoring ATs may allow some individuals with dementia to live in their homes and communities for longer.25 Currently available high-tech AT tools for monitoring vitals, tracking falls, assessing fall risk, and alerting in case of falls include smartwatches, smart phones, belts, pagers, and wristbands.42
Overall, appropriately selected AT can be helpful in improving walking parameters, reducing fall risk, and tracking and promoting exercise. Nonetheless, these technologies should be a supplement to in-person caregiving.25 The choice and application of AT should be tailored to each patient individually. Consultation with a qualified healthcare professional, such as a PT, can guide proper AT selection and use.39
AT for ADLs, IADLs, and Patient Safety Interventions in PDD and PD-MCI
PD often leads to dysfunction in daily roles and routines,43 which cognitive impairment can exacerbate. Occupational Therapy Practitioners (OTPs) are experts in task analysis and curators of solutions for ADLs that promote participation despite the impact of disease. Interventions are grounded on the ability to facilitate independence, safety, participation, and dignity during ADLs and IADLs.44 Motor symptoms including tremors, bradykinesia, and rigidity may lead to a noticeable increase in time spent performing ADL tasks.45 Fine motor control can especially worsen with cognitive impairment.46 Implementing low- to mid-tech AT can assist in performing functional tasks safely and reduce frustration due to symptom interference.47 When considering AT to mitigate the magnitude of hand tremors during self-care tasks, weighted wrist cuffs provide more support during tasks when compared to weighted utensils.48,49 Larger handles can be implemented on commonly used items that require fine motor focus (ie, toothbrushes and utensils) for increased ease and participation with ADL/IADL tasks.50 It is worth noting that the evidence supporting the use of many low-tech items, including weighted utensils, is limited and mostly anecdotal.49 More research is needed to fully evaluate the optimal use and benefits of these items.
Toileting, dressing, and bathing tasks tend to be more challenging when patients with PD experience executive functioning deficits.43 ADL bathroom tasks including transfers, peritoneal hygiene, and bathing pose an increased safety risk for patients with PDD. Current literature identifies mechanical falls as frequently occurring in the bathroom during transfers, leading to high risk of injury for patients and caregivers.51 AT that may help with tasks in the bathroom environment includes bidet attachments, elevated commodes, shower chairs/benches, grab bars, and contrast sensitivity implementation to allow those with PDD to better distinguish objects from their background. Examples of contrast sensitivity implementation include replacing toilet seats with an opposing color to the toilet bowl to increase safety when transferring onto the seat. Additional home modifications promoting safe participation in bathroom tasks include motion sensors, color contrasting steps, nonslip mats, and pathway lighting.52
Transfers in and out of various environments can also present challenges for patients with akinesia and bradykinesia.45 Vehicle transfer can be especially challenging. Available vehicle transfer aids include portable vehicle support handles, wheelchair transfer boards, and a swivel seat. Additionally, floor-to-ceiling grab bars and repositioned bed railings can increase participation and safety when transferring in and out of bed.53
Executive function serves as a critical component of ADL and IADL performance. The capacity to perform tasks relies on sensory processing, reasoning, motor abilities, planning skills, and an individual awareness of the task’s necessity without external cues.54 The executive dysfunction associated with PDD, including skills related to motor planning and cognitive processing, can impact the ability to perform functional tasks successfully. AT can assist in promoting participation in functional tasks, however the effectiveness of the AT will depend on the individual’s capacity, and caregiver assistance may be needed.55 Examples of AT for dressing include button hooks, magnetic buttons, reachers, and shoehorns.47 IADLs are complex tasks that require higher-level cognitive functions to be implemented and carried out successfully.56 One example of a common IADL is medication management, which requires the ability to obtain a prescription, fill/refill at the pharmacy, interpret medical information, take the medications correctly, and monitor outcomes.57 OTPs help clients manage medications by promoting routines that support adherence, modifying the environment, and addressing impairments (eg, strength, dexterity, cognition) that hinder medication management.57 New literature supports mobile applications for multiple purposes for those with PD, including medication management assistance and journaling capabilities for symptom monitoring.58 AT can assist with medication management and may include voice alarm notifications, simple traditional pill-sorters or more advanced high-tech devices that aid in medication dispensing.59
Occupational dysfunction and decreased engagement are common in advanced PD stages. Some of the primary therapy goals in these stages focus on equipping patients and family members with the appropriate tools to preserve dignity and safety.24 High-tech equipment, including hydraulic hospital beds, hydraulic pump or electric transfer lifts, remote monitoring, and location trackers, facilitates interdependence for patients with PDD.24 Likewise, bladder dysfunction is not uncommon among patients with mid- to advanced-stage PDD.60 This is due to diminished fluid intake, inadequate peritoneal hygiene, and pharmacological effects on the bladder system. Bladder dysfunction can subsequently lead to urinary tract infections, causing a high risk of hospitalization, delirium, mood disruptions, falls, and sepsis.60 Suction urination systems may be helpful for monitoring fluid output and urinary tract infections in patients with advanced stages of PDD.61 Ensuring that caregivers have access to appropriate AT when providing care for those with advanced stages of PDD is paramount, as PDD patients often require total assistance with ADL and IADL tasks from their caregivers. The heightened assistance needs increase the risk for caregiver burnout and injury.
While PD often leads to dysfunction in daily roles and routines, AT provides many options for interventions that can help facilitate patient independence, safety, participation, and dignity during ADLs and IADLs, as well as reduce caregiver burden. A summary of some commonly used AT for ADLs and IADLs can be found in Table 2.
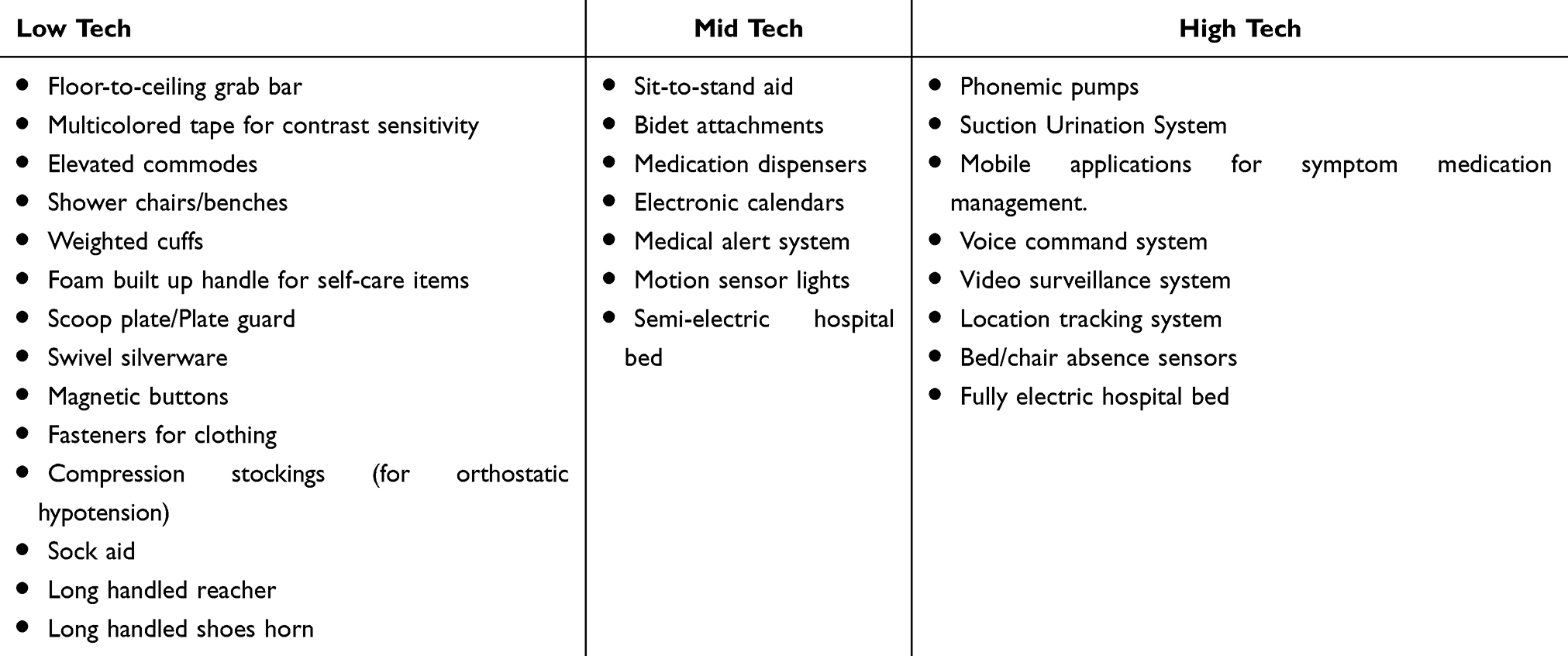 |
Table 2 AT for ADL and IADL Management |
AT for Cognitive-Linguistic and Swallowing Interventions in PDD and PD-MCI
PDD negatively affects motor speech, receptive and expressive language skills, cognitive-linguistic functions, and swallowing abilities.62 As ATs rapidly evolve, speech-language pathologists (SLPs) play a crucial role in selecting effective assessment and therapy tools. By targeting these deficits SLPs can maximize patients’ functionality and elevate quality of life.63
Hypokinetic dysarthria, characterized by hypophonia, imprecise articulation, and reduced prosody is common in patients with PD,64 and those with PDD, complicating functional communication, especially in noisy environments.65 Tools such as portable and stationary voice amplifiers, speakers, and other communication systems can improve voice projection and improve speech intelligibility and endurance even in these challenging conditions.66 Clinical guidance from SLPs is crucial during intervention to improve perceptual intelligibility, sound pressure level, and semitone standard deviation.67
Augmentative and alternative communication (AAC) attempts to compensate individuals with severe disorders of speech-language production and comprehension in both spoken and written modes of communication.68 There are two primary types of AAC: aided or unaided. Vocalizations, speech approximations, signs and gestures, as well as eye blink codes for yes and no indications are all examples of unaided AAC. Aided AAC includes computer-based speech generating technologies and mobile technologies such as tablets and phones with a vast range of digital communication media and applications.68 Aided AAC can be further divided into two major categories: low-tech and high-tech. Examples of low-tech AAC include communication boards, remnant books, drawing, photographs, written messages, and choices.69 High-tech AAC typically refers to speech-generating devices which allow patients with different severity levels of communication deficits to select visually presented icons to express their needs, wants, thoughts and opinions.69 PDD patients can benefit from speech-generating devices to improve functional communication.70 Many factors, including the individual’s motor and cognitive deficits and variable levels of caretaker support, can affect the successful implementation of AAC71 and an individualized approach is often necessary.72
Cognitive-linguistic AT software, often available as electronic device applications, target impairment in attention, memory, executive functions, language and visuo-spatial skills, and may be helpful in addressing the broad spectrum of cognitive-linguistic deficits faced by PDD patients. While not specifically designed for PDD, these technologies target a wide range of disorders resulting in varied levels of cognitive impairment.73 Home-based electronic cognitive therapy programs74 have shown benefits in mild dementia, and studies suggest that motor-focused interventions may yield comparable cognitive benefits.75
Memory aids, including prospective memory aids (PMAs) and retrospective memory aids (RMAs), may also help patients with cognitive and memory skills.76 PMAs aid information recognition and recall as well as task sequencing. Some can even record activities in sequential order,77 helping those with PDD in effectively organizing tasks and improving information retrieval. Unlike traditional external memory aids such as notebooks, cards, and timers that act as scheduling and reminder tools to strengthen information recall.63 PMAs focus on improving daily performance of multiple tasks, while RMAs aim to improve remembrance of events, words, and people encountered in the past. Advanced memory aids need further development and research for consistent use in PDD.76
Positive outcomes on AT use to address communication and cognitive deficits are likely influenced by a motivated focus on external aids utilization, a systematic approach to external aids instruction, and emphasis on individualized goals.78 Caregivers play a crucial role during AT utilization,55 with tasks including products identification, installation, ongoing management, and daily routine implementation and support. Nevertheless, there seems to be a lack of standardized protocols and guidelines in how to effectively utilize AT in cognitive-linguistic interventions among the PDD population as well as insufficient education and caretaker training on AT from healthcare professionals.55
AT also plays an essential role in managing dysphagia, a common issue in PDD compounded by cognitive and motor impairments.79 Motor problems as well as sensory and behavioral factors, can further complicate known swallowing problems, leading to choking episodes, aspiration pneumonia, weight loss, dehydration, and malnutrition.80
Similar to common practices of dysphagia management, suspected swallowing problems in the PDD population are often identified through comprehensive diagnostic examination. This can include completion of validated quality of life measures or questionnaires such as EAT-1081 and PILL-5,82 oral trials of foods and liquid boluses with varied viscosities, clinician observations of clinical signs and symptoms of aspiration, and objective swallowing assessments such as videofluoroscopic swallow studies. Videofluoroscopic swallow studies involve real-time X-ray technique, allowing SLPs to visualize the entire swallowing process in the bolus flow tract, from lips to the stomach to identify any abnormalities.83 Once dysphagia is confirmed, SLPs determine optimal intervention approaches to address these deficits.
Dysphagia management is often diverse and individualized. Adaptive feeding devices play an important role in improving independence in feeding among those with neurodegenerative diagnoses,84,85 including PDD. Bendable utensils with easy grip handles, plate guards, cups with weight base and non-slip mats are all useful feeding tools that can help reduce spillage, secure feeding process and improve mealtime enjoyment despite existing rigidity and cognitive deficits.
Patients with neurodegenerative diseases such as PDD tend to experience muscular changes affecting overall swallowing functions. One of the hallmarks of oral motor changes is reduced lingual strength.86 Current available devices such as the Tongueometer, are used for lingual strength measuring and strengthening, aiming for better muscular coordination, strength and endurance with real-time visual biofeedback.87 Pharyngeal swallowing changes can be detected via use of surface electromyography (sEMG). sEMG is often used during swallowing therapies given its benefits of providing realistic biofeedback to both SLPs and patients.88,89 Available sEMG products such as Mobili-T have been studied among other patient populations. The sEMG products aim at monitoring muscular and activities and functions to track therapy progress with real-time visual biofeedback.90 One recent study showed that high-density surface electromyography (HD-sEMG) targeting suprahyoid muscles demonstrated positive muscular changes among PD patients after electrical stimulation intervention.91 Future studies targeting the PDD population are needed to explore candidacy and effectiveness.
Patients with chronic and progressive cognitive-linguistic deficits such as PDD may not always be the most appropriate population to utilize AT in swallowing management, given the possibility of difficulty understanding intervention rationales and inability to follow multistep directions consistently to participate in swallowing therapies. For instance, patients may not be able to simply complete a swallow with a recommended strategy or maneuver such as a chin tuck posture or supraglottic swallow, resulting in suboptimal outcomes.80 The use of video-assisted swallowing therapy can improve quality of life and increase pleasure from eating, in addition to improving swallowing functions and reducing pharyngeal residue utilizing flexible fiberoptic evaluation of swallowing (FEES).92 This is administered by SLPs inserting a flexible endoscope through the nose to view the pharynx with use of food dye during scoping to assess swallowing functions in mostly the pharyngeal stage of swallowing.
In addition to available ATs to address communication, cognitive-linguistic impairments, and swallowing difficulties, the modality of speech therapy has also transformed with increased implementation of telemedicine during and after the COVID-19 pandemic. Multiple factors contribute to successful tele practice when addressing speech and swallowing deficits in patients with chronic cognitive deficits, especially those with PDD, including internet connection stability, presence of dedicated and supportive caretakers, motivation of patients and families, access to insurance with reimbursement benefits and consistent access to telemedicine services.93
Table 3 lists some commonly available AT targeting communication, cognition and swallowing functions.
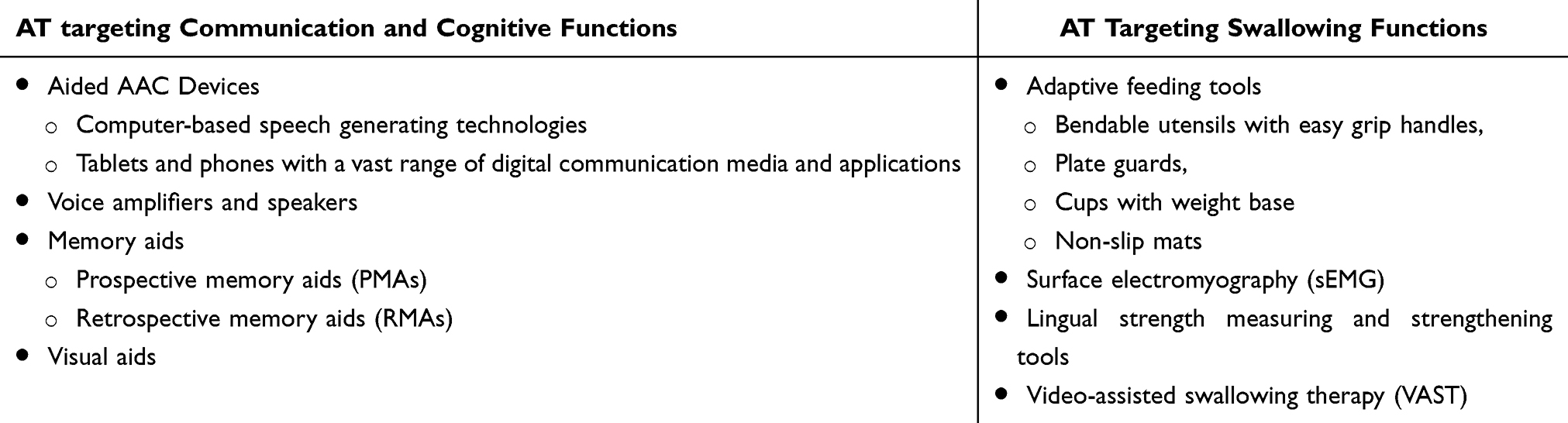 |
Table 3 AT for Communication, Cognitive, and Swallow Functions |
Discussion
Assistive technology (AT) has many potential applications for improving daily functioning and quality of life for patients with PDD or PD-MCI and their caregivers. AT can mitigate fall risk, track exercise goals, improve independence, reduce caregiver burden, and ameliorate cognitive communication and swallow deficits.25,44,55 However, the impact of AT depends on thoughtful implementation. While AT can empower caregivers and patients, it may inadvertently increase caregiver burden due to the reliance on caregivers for operation and support.55
The mental health and cognitive capacity of the individual with PDD/PD-MCI must be considered when prescribing AT. Some common neuropsychiatric symptoms amongst people with PDD are depression, apathy, anxiety, and hallucinations.94 These symptoms, along with cognitive symptoms such as executive dysfunction and social dysfunction,95 can negatively affect acceptance or successful use of AT. Incorporation of interdisciplinary team experts in this area, such as neuropsychology, physical therapy,96 occupational therapy, or speech therapy, can help address these deficits and improve the benefit of AT.97
AT recommendations should further take into account the requirements and views of both caregivers and patients, while also considering patient and caregivers’ current abilities and future needs. The level of support and perception of caregivers can greatly affect the successful use of AT.98 It is crucial to consider the environmental, financial, educational, and cultural contexts of all persons involved in AT use. A holistic and individualized approach is essential to foster adoption and ongoing utilization. Some social barriers to AT adoption can include stigma associated with visible devices which may be perceived as signs of disability or weakness, lack of awareness and access to clinical education, and resistance to change. Different cultural attitudes towards disability and cultural insensitivity in AT design can also potentially make AT less functional and appealing to patients and families. Potential economic obstacles can include inadequate insurance or funding support and higher maintenance costs for repairs and software updates, especially for those from low-income communities. Collaboration with different members of the interdisciplinary team such as social workers can be key in the successful acquisition of AT items.99
The timing of AT introduction is critical, as patients’ needs evolve throughout the disease course. High-tech AT options may be more appropriate for those with PD-MCI or with more caregiver support.55 Lack of technical literacy and navigating more complex AT interfaces are some of the primary barriers to AT use in an older population with significant cognitive deficits.39
All barriers must be addressed through structured training, education, and professional support. Healthcare practitioners can incorporate recommended AT into patient education by providing demonstrational videos, visual and written instructions, or hands-on learning. They may also, as needed, provide the patient and caregivers with the contact information for vendors that can support acquisition of recommended AT.100 Input from healthcare professionals can be particularly vital as some studies have shown negative consequences when using the incorrect device.39
To date, there has been no established clinical algorithm or framework to guide AT selection, training, and evaluation tailored to PDD progression. Individual prescription and intermittent follow-up with a healthcare clinician is key in assessing appropriateness and effectiveness of AT throughout the PDD and PD-MCI journey. In Table 4, we propose a framework for AT selection, implementation, follow-up, and assessment in this population. One study suggested a formal program for AT integration including identification and removal of barriers, education and structured training on AT use in different contexts, and regular follow-up support.18 The effectiveness of AT use can be measured informally through subjective patient or caregiver report or formally through questionnaires for the patient (Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST)) or caregiver (Caregiver Assistive Technology Outcome Measure (CATOM)). The Canadian Occupational Performance Measure (COPM) may be appropriate for use in the PD-MCI population.101
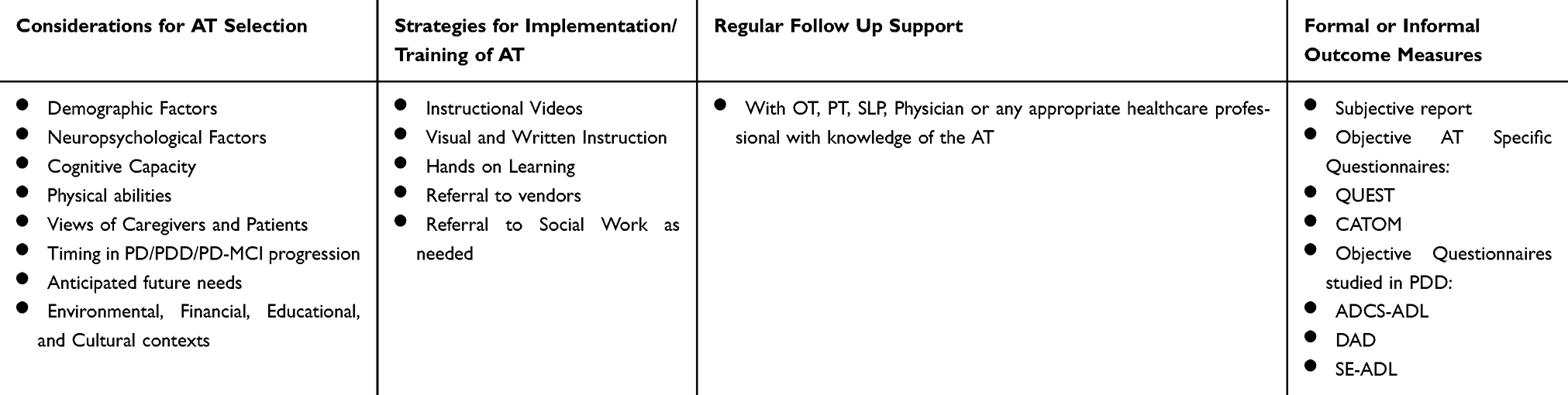 |
Table 4 Proposed Framework for AT Selection, Implementation, Follow-Up, and Assessment |
However, these objective assessments have not been formally studied in the PDD/PD-MCI populations. Some alternative ADL and QoL outcome measures studied in the PDD/PD-MCI populations include the Alzheimer’s Disease Cooperative Study‐Activities of Daily Living Scale (ADCS-ADL), the Disability Assessment for Dementia (DAD), or the Schwab and England‐ADL scale (SE-ADL). The use of these assessments before and after AT introduction, acquisition, and training can give healthcare practitioners a better understanding of the success or failure of AT use.102
Although research on AT in PDD and PD-MCI populations is limited, existing studies demonstrate some promising outcomes. For instance, home monitoring devices, including voice-activated technology and home automation, have been associated with significant improvements in walking, especially in freezing of gait. However, AT use appears to not affect broader outcomes such as risk of nursing home admissions for persons with dementia.24 Certain ATs such as motion sensing nightlights, remote intercoms, and wearable fall detection bracelets can reduce fall risk and improve overall safety.41 Patient feedback also suggests that cognitive stimulation devices were the most preferred among ATs in the dementia population, followed by social robots.103
AT adoption and successful implementation depends on individual and demographic factors. Female sex, higher education, higher annual income, more frequent use of social networking services, and willingness to live in a nursing home when needed were all positively associated with the acceptance of AT for ADLs. Nevertheless, widespread use of AT was not found in long-term care facilities.104
While larger studies and recent advancements36,64,73 provide valuable insights, many studies in this paper have small sample sizes38,55,76,84,92 or lack PDD-specific focus, thus limiting generalizability.55,76,84,89,92 Other articles were dated31,48 or excluded persons with severe cognitive deficits.28,31 Some AT discussed in this review (eg weighted utensils) had little research supporting their use.48,50 Other ATs have stronger evidence, such as the use of laser canes and metronomes to improve gait parameters; computer based cognitive rehabilitation programs to influence working memory, language comprehension, and executive function; weighted cuffs for tremor management; and mobile apps for motor and nonmotor symptom tracking.37,38,47,55,70 Despite a confluence of existing limitations and strengths, these studies still provide a beneficial guide from an interdisciplinary team perspective when implementing care for individuals with PDD/PD-MCI.
Future directions include wearable and non-wearable technologies using artificial intelligence (AI) for telehealth or remote assessments of patients’ conditions in their natural home environment and shows potential in helping patients to better manage their conditions.105 This is especially relevant after the COVID-19 pandemic. Novel algorithms and multi-modal sensors show high accuracy (97.4%) and speed (within 0.5 seconds) in predicting intended movements in the PD population.106 Classification algorithms can assist in better prescribing AT for persons with PD and potentially automatically incorporate the range of factors impacting AT adoption likelihood.107 One recent paper envisions the combined use of wearable physical and chemical sensors that track levodopa measurements with a control algorithm and drug delivery system. Although such autonomous systems are in the early stages of development, the impact of such a device could change the landscape of medication management for persons with PD.108 However, special consideration must be given to the PDD population when implementing high-tech AT such as wearable sensors or use of AI. Such technologies may be difficult to navigate for patients with PDD, creating increased confusion or agitation. Nevertheless, it could also serve as a helpful monitoring aid to the caregiver when patient reporting becomes less reliable due to cognitive impairment. Individualized prescription and ongoing reassessment with a healthcare professional is necessary.
Further research is needed to better understand the real-world recommendation, training, and use of AT for persons with PDD and PD-MCI from an interdisciplinary perspective. The needs of both patients and caregivers during each stage of the disease must be considered. There is a gap of knowledge especially regarding interdependence during the advanced stages of PD, and methods in which AT can be applied to maintain dignity and safety while supporting caregivers.
Conclusion
Multiple previous articles have discussed the advantages and limitations of AT with PD, dementia, and general older adult populations. Nevertheless, this is one of the first to examine the use of currently available AT for persons with PDD and PD-MCI through an interdisciplinary lens. The diversity of currently available AT can serve in assisting people with PDD/PD-MCI in avoiding falls, tracking exercise goals, improving ability to perform ADL and IADL, and enhancing communication and swallow functions; thereby improving patients’ independence and maximizing overall quality of life.
Abbreviations
ADL, Activities of Daily Living; ADCS-ADL, Alzheimer’s Disease Cooperative Study‐Activities of Daily Living Scale; AI, Artificial Intelligence; AT, Assistive Technology; CATOM, Caregiver Assistive Technology Outcome Measure; COPM, Canadian Occupational Performance Measure; DAD, Disability Assessment for Dementia; FEES, Flexible Fiberoptic Evaluation of Swallowing; FOG, Freezing of Gait; IADL, Instrumental Activities of Daily Living; OTP, Occupational Therapy Practitioners; PD, Parkinson’s Disease; PDD, Parkinson’s Disease Dementia; PD-MCI, Parkinson’s Disease- Mild Cognitive Impairment; PMAs, Prospective Memory Aids; QUEST, Quebec User Evaluation of Satisfaction with Assistive Technology; PT, Physical Therapy/Physical Therapist; RMAs, Retrospective Memory Aids; SE-ADL, Schwab and England‐ADL scale; EMG, Surface Electromyography; SLP, Speech Language Pathologist; VAST, Video-Assisted Swallowing Therapy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tolosa E, Garrido A, Scholz SW, Poewe W. Challenges in the diagnosis of Parkinson’s disease. Lancet Neurol. 2021;20(5):385–397. doi:10.1016/S1474-4422(21)00030-2
2. Marras C, Beck JC, Bower JH, et al. Prevalence of Parkinson’s disease across North America. NPJ Parkinson’s Dis. 2018;4(1):21–27. doi:10.1038/s41531-018-0058-0
3. Willis AW, Roberts E, Beck JC, et al. Incidence of Parkinson disease in North America. NPJ Parkinson’s Dis. 2022;8(1):170–177. doi:10.1038/s41531-022-00410-y
4. Yu R-L, Wu R-M. Mild cognitive impairment in patients with Parkinson’s disease: an updated mini-review and future outlook. Front Aging Neurosci. 2022;14:943438. doi:10.3389/fnagi.2022.943438
5. Emre M. Cognitive Impairment and Dementia in Parkinson’s Disease.
6. Gomperts SN. Lewy body dementias: dementia with Lewy bodies and Parkinson disease dementia. Continuum. 2016;22(2, Dementia):435–463. doi:10.1212/CON.0000000000000309
7. Aarsland D, Zaccai J, Brayne C. A systematic review of prevalence studies of dementia in Parkinson’s disease. Mov Disord. 2005;20(10):1255–1263. doi:10.1002/mds.20527
8. Anang JBM, Gagnon J-F, Bertrand J-A, et al. Predictors of dementia in Parkinson disease: a prospective cohort study. Neurology. 2014;83(14):1253–1260. doi:10.1212/WNL.0000000000000842
9. Gallagher J, Gochanour C, Caspell-Garcia C, et al. Long-term dementia risk in Parkinson disease. Neurology. 2024;103(5):e209699. doi:10.1212/WNL.0000000000209699
10. Gibson LLWD, Lemmen RPG, Chaudhuri KR, Svenningsson P, Aarsland D. Risk of dementia in Parkinson’s disease: a systematic review and meta-analysis. Mov Disord. 2024;39(10):1697–1709. doi:10.1002/mds.29918
11. Aarsland D, Kurz MW. The epidemiology of dementia associated with Parkinson’s disease. Brain Pathol. 2010;20(3):633–639. doi:10.1111/j.1750-3639.2009.00369.x
12. Gonzalez MC, Dalen I, Maple-Grødem J, Tysnes O-B, Alves G. Parkinson’s disease clinical milestones and mortality. NPJ Parkinson’s Dis. 2022;8(1):58. doi:10.1038/s41531-022-00320-z
13. Sawires M, Sampaio C, Seppi K, Costa J, Poewe W. Treatment of dementia in Parkinson’s disease. Cochrane Database Syst Rev. 2019;2019(5). doi:10.1002/14651858.CD005358.pub2
14. Lawson RA, Yarnall AJ, Duncan GW, et al. Severity of mild cognitive impairment in early Parkinson’s disease contributes to poorer quality of life. Parkinsonism Related Disord. 2014;20(10):1071–1075. doi:10.1016/j.parkreldis.2014.07.004
15. Wallace ER, Segerstrom SC, van Horne CG, Schmitt FA, Koehl LM. Meta-analysis of cognition in Parkinson’s disease mild cognitive impairment and dementia progression. Neuropsychol Rev. 2022;32(1):149–160. doi:10.1007/s11065-021-09502-7
16. Weintraub D, Aarsland D, Chaudhuri KR, et al. The neuropsychiatry of Parkinson’s disease: advances and challenges. Lancet Neurol. 2022;21(1):89–102. doi:10.1016/S1474-4422(21)00330-6
17. Kim -H-H, Jung N-H. Effects of assistive technology application in dementia intervention for people with mild cognitive impairment & mild Alzheimer type dementia and caregiver. Alternat Ther Health Med. 2023;29(2):104–111.
18. Widehammar C, Lidström H, Hermansson L. Environmental barriers to participation and facilitators for use of three types of assistive technology devices. Assistive Technol. 2019;31(2):82. doi:10.1080/10400435.2017.1363828
19. Ferrazzoli D, Ortelli P, Zivi I, et al. Efficacy of intensive multidisciplinary rehabilitation in Parkinson’s disease: a randomised controlled study. J Neurol Neurosurg. 2018;89(8):828–835. doi:10.1136/jnnp-2017-316437
20. Monticone M, Ambrosini E, Laurini A, Rocca B, Foti C. In-patient multidisciplinary rehabilitation for Parkinson’s disease: a randomized controlled trial. Mov Disord. 2015;30(8):1050–1058. doi:10.1002/mds.26256
21. Rajan R, Brennan L, Bloem BR, et al. Integrated care in Parkinson’s disease: a systematic review and meta‐analysis. Mov Disord. 2020;35(9):1509–1531. doi:10.1002/mds.28097
22. Aarsland D, Ballard CG, Halliday G. Are Parkinson’s disease with dementia and dementia with Lewy bodies the same entity?: Psychiatric aspects of Parkinson’s disease, Parkinson’s disease with dementia and dementia with Lewy bodies. J Geriatric Psychiatry Neurol. 2004;17(3):137–145. doi:10.1177/0891988704267470
23. Vatter S, Stanmore E, Clare L, McDonald KR, McCormick SA, Leroi I. Care burden and mental ill health in spouses of people with Parkinson disease dementia and Lewy body dementia. J Geriatric Psychiatry Neurol. 2020;33(1):3–14. doi:10.1177/0891988719853043
24. Collins TL, Cardella A, Gordon S. The impact of assistive technology on quality of life of home-dwelling people with Parkinson’s disease. Home Healthcare Now. 2023;41(4):214–220. doi:10.1097/NHH.0000000000001187
25. Clark M, Mierzwinski-Urban M, Mason J, Hao Q. Technologies to increase freedom for people living with dementia. Can J Health Technol. 2023;3(12). doi:10.51731/cjht.2023.797
26. Mak MK, Wong-Yu IS, Shen X, Chung CL. Long-term effects of exercise and physical therapy in people with Parkinson disease. Nat Rev Neurol. 2017;13(11):689–703. doi:10.1038/nrneurol.2017.128
27. Petzinger GMD, Fisher BEP, McEwen SP, Beeler JAP, Walsh JPP, Jakowec MWP. Exercise-enhanced neuroplasticity targeting motor and cognitive circuitry in Parkinson’s disease. Lancet Neurol. 2013;12(7):716–726. doi:10.1016/S1474-4422(13)70123-6
28. de Carvalho Lana R, Ribeiro de Paula A, Souza Silva AF, Vieira Costa PH, Polese JC. Validity of mHealth devices for counting steps in individuals with Parkinson’s disease. J Bodyw Mov Ther. 2021;28:496–501. doi:10.1016/j.jbmt.2021.06.018
29. Putzolu M, Manzini V, Gambaro M, et al. Home-based exercise training by using a smartphone app in patients with Parkinson’s disease: a feasibility study. Front Neurol. 2023;14:1205386. doi:10.3389/fneur.2023.1205386
30. McCandless PJ, Evans BJ, Janssen J, Selfe J, Churchill A, Richards J. Effect of three cueing devices for people with Parkinson’s disease with gait initiation difficulties. Gait Posture. 2016;44:7–11. doi:10.1016/j.gaitpost.2015.11.006
31. Donovan S, Lim C, Diaz N, et al. Laserlight cues for gait freezing in Parkinson’s disease: an open-label study. Parkinsonism Related Disord. 2011;17(4):240–245. doi:10.1016/j.parkreldis.2010.08.010
32. Bryant MS, Rintala DH, Lai EC, Protas EJ. A pilot study: influence of visual cue color on freezing of gait in persons with Parkinson’s disease. Disability Rehabil. 2010;5(6):456–461. doi:10.3109/17483107.2010.495815
33. Chen PH, Yang YY, Liao YY, Cheng SJ, Wang PN, Cheng FY. Factors associated with fear of falling in individuals with different types of mild cognitive impairment. Brain Sciences. 2022;12(8):990. doi:10.3390/brainsci12080990
34. Gao C, Liu J, Tan Y, Chen S. Freezing of gait in Parkinson’s disease: pathophysiology, risk factors and treatments. Transl Neurodegener. 2020;9(1):12. doi:10.1186/s40035-020-00191-5
35. Hashimoto T. Speculation on the responsible sites and pathophysiology of freezing of gait. Parkinsonism Related Disord. 2006;12(2):S55–S62. doi:10.1016/j.parkreldis.2006.05.017
36. Salari M, Rashedi R, Momenilandi F, Shirin MB, Etemadifar M. The effects of laser cane cues on the freezing of gait of Parkinson’s disease patients: can increasing the laser light beam width play a role? Acta Neurol Belg. 2024;124(5):1647–1653. doi:10.1007/s13760-024-02592-z
37. Kyrdalen IL, Thingstad P, Sandvik L, Ormstad H. Associations between gait speed and well‐known fall risk factors among community‐dwelling older adults. Physiother Res Int. 2019;24(1):e1743–n/a. doi:10.1002/pri.1743
38. Bryant MS, Pourmoghaddam A, Thrasher A. Gait changes with walking devices in persons with Parkinson’s disease. Disability Rehabil. 2012;7(2):149–152. doi:10.3109/17483107.2011.602461
39. García‐Bustillo Á, Valiñas‐Sieiro F, Allende‐Río M, González‐Santos J, Cubo E. Assistive devices for personal mobility in Parkinson’s disease: a systematic review of the literature. Mov Disord Clin Pract. 2022;9(8):1040–1046. doi:10.1002/mdc3.13568
40. Rocha PA, Porfírio GM, Ferraz HB, Trevisani VFM. Effects of external cues on gait parameters of Parkinson’s disease patients: a systematic review. Clin Neurol Neurosurg. 2014;124:127–134. doi:10.1016/j.clineuro.2014.06.026
41. Brims L, Oliver K. Effectiveness of assistive technology in improving the safety of people with dementia: a systematic review and meta-analysis. Aging Mental Health. 2018;23(8):942–951. doi:10.1080/13607863.2018.1455805
42. Prieto-Avalos G, Sánchez-Morales LN, Alor-Hernández G, Sánchez-Cervantes JL. A Review of commercial and non-commercial wearables devices for monitoring motor impairments caused by neurodegenerative diseases. Biosensors. 2022;13(1):72. doi:10.3390/bios13010072
43. Wood J, Henderson W, Foster ER. Occupational therapy practice guidelines for people with Parkinson’s disease. Am J Occup Ther. 2022;76(3). doi:10.5014/ajot.2022.763001
44. Smith EM. The Global report on assistive technology: a new era in assistive technology. Assistive Technol. 2022;34(3):255. doi:10.1080/10400435.2022.2077596
45. Poewe W. 115Global scales to stage disability in pd: the Hoehn and Yahr scale. In: Sampaio C, Goetz CG, Schrag A, editors. Rating Scales in Parkinson’s Disease: Clinical Practice and Research. Oxford University Press; 2012.
46. Tan S, Hong CT, Chen JH, et al. Hand fine motor skill disability correlates with cognition in patients with moderate-to-advanced Parkinson’s disease. Brain Sci. 2020;10(6):337. doi:10.3390/brainsci10060337
47. Yau Y, Hsiao C-H. The technology acceptance model and older adults’ exercise intentions—a systematic literature review. Geriatrics. 2022;7(6):124. doi:10.3390/geriatrics7060124
48. McGruder J, Cors D, Tiernan AM, Tomlin G. Weighted wrist cuffs for tremor reduction during eating in adults with static brain lesions. Am J Occup Ther. 2003;57(5):507–516. doi:10.5014/ajot.57.5.507
49. Sabari J, Stefanov DG, Chan J, Goed L, Starr J. Adapted feeding utensils for people with Parkinson’s-related or essential tremor. Am J Occup Ther. 2019;73(2):7302205120p1–7302205120p9. doi:10.5014/ajot.2019.030759
50. Ma H-I, Hwang W-J, Tsai P-L, Hsu Y-W. The effect of eating utensil weight on functional arm movement in people with Parkinson’s disease: a controlled clinical trial. Clin rehabilitat. 2009;23(12):1086–1092. doi:10.1177/0269215509342334
51. Edwards NC. Preventing falls among seniors: the way forward. J Safety Res. 2011;42(6):537–541. doi:10.1016/j.jsr.2011.11.001
52. Riazi A, Ying Boon M, Bridge C, Dain SJ. Home modification guidelines as recommended by visually impaired people. J Assist Technol. 2012;6(4):270–284. doi:10.1108/17549451211285762
53. Ainsworth E, De Jonge D. Measuring the person and the home environment. In: An Occupational Therapist’s Guide to Home Modification Practice. Routledge; 2024:145–174.
54. Mlinac ME, Feng MC. Assessment of activities of daily living, self-care, and independence. Arch Clin Neuropsychol. 2016;31(6):506–516. doi:10.1093/arclin/acw049
55. Gibson G, Dickinson C, Brittain K, Robinson L. The everyday use of assistive technology by people with dementia and their family carers: a qualitative study. BMC Geriatr. 2015;15(1):89. doi:10.1186/s12877-015-0091-3
56. Spalla G, Yaddaden A, Kenfack Ngankam H, Gouin-Vallerand C, Bier N. Assistive technologies designed to support executive function impairments while promoting Independence: a scoping review. J Rehabil Assist Technol Eng. 2024;11:20556683241268658. doi:10.1177/20556683241268658
57. Association AOT. Occupational therapy’s role in medication management. Am J Occup Ther. 2017;71(Supplement_2):7112410025p1–7112410025p20. doi:10.5014/ajot.2017.716S02
58. Lee J, Yeom I, Chung ML, Kim Y, Yoo S, Kim E. Use of mobile apps for self-care in people with Parkinson disease: systematic review. JMIR Mhealth Uhealth. 2022;10(1):e33944. doi:10.2196/33944
59. Vaish A. Automated pill dispenser to improve medication compliance, efficiency, and accuracy. 2024;192–196.
60. Jesudasan A. Urinary bladder problems in Parkinson’s disease. J Park Restless Legs Syndrome. 2012;30. doi:10.2147/JPRLS.S37080
61. Hogg E, Frank S, Oft J, Benway B, Rashid MH, Lahiri S. Urinary tract infection in Parkinson’s disease. J Parkinsons Dis. 2022;12(3):743–757. doi:10.3233/jpd-213103
62. Verny M, Blanc F. Lewy body dementia: therapeutic propositions according to evidence based medicine and practice. Gériatrie et psychologie neuropsychiatrie du vieillissement. 2019;17(2):189. doi:10.1684/pnv.2019.0803
63. Klimova B, Maresova P, Kuca K. Assistive technologies for managing language disorders in dementia. Neuropsychiatr Dis Treat. 2016;12(Issue 1):533–540. doi:10.2147/NDT.S95903
64. Umer S, Rout RK. Descriptive and inferential analysis of features for Dysphonia and dysarthria Parkinson’s disease symptoms. Health Services Outcomes Res Methodol. 2024;24(3):304–326. doi:10.1007/s10742-023-00316-z
65. Adams S, Moon B-H, Dykstra A, Abrams K, Jenkins M, Jog M. Effects of multitalker noise on conversational speech intensity in Parkinson’s disease. J Med Speech Lang Pathol. 2006;14(4):221–228.
66. Knowles T, Adams SG, Page A, Cushnie-Sparrow D, Jog M. A comparison of speech amplification and personal communication devices for hypophonia. J Speech Lang Hear Res. 2020;63(8):2695–2712. doi:10.1044/2020_JSLHR-20-00085
67. Muñoz-Vigueras N, Prados-Román E, Valenza MC, et al. Speech and language therapy treatment on hypokinetic dysarthria in Parkinson disease: systematic review and meta-analysis. Clin rehabilitat. 2021;35(5):639–655. doi:10.1177/0269215520976267
68. Beukelman DR, Yorkston KM, Reichle J. Augmentative and Alternative Communication for Adults with Acquired Neurologic Disorders. AAC series. Paul H. Brookes Pub. Co.; 2000.
69. Beukelman DR, Fager S, Ball L, Dietz A. AAC for adults with acquired neurological conditions: a review. Augment Altern Commun. 2007;23(3):230–242. doi:10.1080/07434610701553668
70. Creer S, Enderby P, Judge S, John A. Prevalence of people who could benefit from augmentative and alternative communicationAAC) in the UK: determining the need. Int J Lang Communicat Disorder. 2016;51(6):639–653. doi:10.1111/1460-6984.12235
71. Armstrong L, Jans D, MacDonald A. Parkinson’s disease and aided AAC: some evidence from practice. Int J Lang Communicat Disorder. 2000;35(3):377–389. doi:10.1080/136828200410636
72. May AA, Dada S, Murray J. Review of AAC interventions in persons with dementia. Int J Lang Communicat Disorder. 2019;54(6):857–874. doi:10.1111/1460-6984.12491
73. Irazoki E, Contreras-Somoza LM, Toribio-Guzmán JM, Jenaro-Río C, van der Roest H, Franco-Martín MA. Technologies for cognitive training and cognitive rehabilitation for people with mild cognitive impairment and dementia. a systematic review. Front Psychol. 2020;11:648. doi:10.3389/fpsyg.2020.00648
74. Marin A, DeCaro R, Schiloski K, et al. Home-based electronic cognitive therapy in patients with Alzheimer disease: feasibility randomized controlled trial. JMIR Format Res. 2022;6(9):e34450–e34450. doi:10.2196/34450
75. Zimmermann R, Gschwandtner U, Benz N, et al. Cognitive training in Parkinson disease: cognition-specific vs nonspecific computer training. Neurology. 2014;82(14):1219–1226. doi:10.1212/WNL.0000000000000287
76. King AC, Dwan C. Electronic memory aids for people with dementia experiencing prospective memory loss: a review of empirical studies. Dementia. 2019;18(6):1994–2007. doi:10.1177/1471301217735180
77. Berry E, Kapur N, Williams L, et al. The use of a wearable camera, SenseCam, as a pictorial diary to improve autobiographical memory in a patient with limbic encephalitis: a preliminary report. Neuropsychological Rehabilitat. 2007;17(4–5):582–601. doi:10.1080/09602010601029780
78. Spencer KA, Paul J, Brown KA, Ellerbrock T, Sohlberg MM. Cognitive rehabilitation for individuals with Parkinson’s disease: developing and piloting an external aids treatment program. Am J Speech Lang Pathol. 2020;29(1):1–19. doi:10.1044/2019_AJSLP-19-0078
79. Bine JE, Frank EM, McDade HL. Dysphagia and dementia in subjects with Parkinson’s disease. Dysphagia. 1995;10(3):160–164. doi:10.1007/bf00260970
80. Easterling CS, Robbins E. Dementia and Dysphagia. Geriatric Nurs. 2008;29(4):275–285. doi:10.1016/j.gerinurse.2007.10.015
81. Belafsky PC, Mouadeb DA, Rees CJ, et al. Validity and reliability of the eating assessment toolEAT-10). Ann Otol Rhinol Laryngol. 2008;117(12):919–924. doi:10.1177/000348940811701210
82. Nativ-Zeltzer N, Bayoumi A, Mandin VP, et al. Validation of the PILL-5: a 5-item patient reported outcome measure for Pill Dysphagia. Front Surg. 2019;6:43. doi:10.3389/fsurg.2019.00043
83. Murry T, Chan K, Carrau RL. Clinical Management of Swallowing Disorders.
84. Cavalcanti A, Amaral MF, Silva e Dutra FCM, Santos AVF, Licursi LA, Silveira ZC. Adaptive eating device: performance and satisfaction of a person with Parkinson’s disease. Can J Occup Ther. 2020;87(3):211–220. doi:10.1177/0008417420925995
85. Greenwood DI. Nutrition Management of Amyotrophic Lateral Sclerosis. Nutr Clin Pract. 2013;28(3):392–399. doi:10.1177/0884533613476554
86. Ji EK, Wang HH, Jung SJ, et al. The changes for strength of oropharyngeal muscles in patients with dementia and dysphagia. Brain NeuroRehabil. 2019;12(2). doi:10.12786/bn.2019.12.e12
87. Curtis JA, Mocchetti V, Rameau A. Concurrent validity of the IOPI and tongueometer orofacial strength measurement devices. Laryngoscope. 2023;133(11):3123–3131. doi:10.1002/lary.30782
88. Crary MA, Carnaby Mann GD, Groher ME, Helseth E. Functional benefits of dysphagia therapy using adjunctive sEMG biofeedback. Dysphagia. 2004;19(3):160–164. doi:10.1007/s00455-004-0003-8
89. Poorjavad M, Talebian S, Ansari NN, Soleymani Z. Surface electromyographic assessment of swallowing function. Iran J Med Sci. 2017;42(2):194–200. doi:10.1007/s00455-001-0095-3
90. Constantinescu G, Kuffel K, Aalto D, Hodgetts W, Rieger J. Evaluation of an automated swallow-detection algorithm using visual biofeedback in healthy adults and head and neck cancer survivors. Dysphagia. 2018;33(3):345–357. doi:10.1007/s00455-017-9859-2
91. Nakamori M, Yoshikawa K, Toko M, et al. High-density surface electromyography evaluation of the suprahyoid muscles in patients with Parkinson’s disease. J Neurol Sci. 2024;466:123266. doi:10.1016/j.jns.2024.123266
92. Manor Y, Mootanah R, Freud D, Giladi N, Cohen JT. Video-assisted swallowing therapy for patients with Parkinson’s disease. Parkinsonism Related Disord. 2013;19(2):207–211. doi:10.1016/j.parkreldis.2012.10.004
93. De Marchi F, Contaldi E, Magistrelli L, Cantello R, Comi C, Mazzini L. Telehealth in neurodegenerative diseases: opportunities and challenges for patients and physicians. Brain Sciences. 2021;11(2):237. doi:10.3390/brainsci11020237
94. Schneider F, Althaus A, Backes V, Dodel R. Psychiatric symptoms in Parkinson’s disease. Eur Archiv Psychiatry Clin Neurosci. 2008;258(Suppl 5):55–59. doi:10.1007/s00406-008-5012-4
95. Chen Y-R, Tan C-H, Su H-C, et al. Investigating the interaction between neuropsychiatry features and daily activities on social function in patients with Parkinson’s disease with mild cognitive impairment. BJPsych Open. 2022;8(6):e205–e205. doi:10.1192/bjo.2022.611
96. Jiménez Arberas E, Ordoñez Fernández FF, Rodríguez Menéndez S. Psychosocial impact of mobility assistive technology on people with neurological conditions. Disability Rehabil. 2021;16(5):465–471. doi:10.1080/17483107.2019.1648571
97. Rosinczuk J, Koltuniuk A. The influence of depression, level of functioning in everyday life, and illness acceptance on quality of life in patients with Parkinson’s disease: a preliminary study. Neuropsychiatr Dis Treat. 2017;13:881–887. doi:10.2147/NDT.S132757
98. Curnow E, Rush R, Gorska S, Forsyth K. Differences in assistive technology installed for people with dementia living at home who have wandering and safety risks. BMC Geriatr. 2021;21(1):613. doi:10.1186/s12877-021-02546-7
99. Rony RJ, Amir S, Ahmed N, et al. Understanding the sociocultural challenges and opportunities for affordable wearables to support poststroke upper-limb rehabilitation: qualitative study. JMIR Rehabil Assist Technol. 2024;11:e54699–e54699. doi:10.2196/54699
100. Hung C-H, Chen M-H, Fan S-C. Enhancing occupational therapy education: evaluating the impact of a STEAM-based assistive technology curriculum using Kirkpatrick’s four-level model. Br J Occup Ther. 2024;87(8):512–523. doi:10.1177/03080226241239563
101. Borgnis F, Desideri L, Converti RM, Salatino C. Available assistive technology outcome measures: systematic review. JMIR Rehabil Assist Technol. 2023;10(1):e51124–e51124. doi:10.2196/51124
102. Holden SK, Jones WE, Baker KA, Boersma IM, Kluger BM. Outcome measures for Parkinson’s disease dementia: a systematic review. Mov Disord Clin Pract. 2016;3(1):9–18. doi:10.1002/mdc3.12225
103. Kruse CS, Fohn J, Umunnakwe G, Patel K, Patel S. Evaluating the facilitators, barriers, and medical outcomes commensurate with the use of assistive technology to support people with dementia: a systematic review literature. Healthcare. 2020;8(3):278. doi:10.3390/healthcare8030278
104. Itoh S, Miwa H, Wu VX, et al. Acceptance of care technologies to support activities of daily living by middle-aged and older adults in Japan: a cross-sectional study. Int J Nurs Stud Adv. 2021;3:100042. doi:10.1016/j.ijnsa.2021.100042
105. Luis-Martínez R, Monje MHG, Antonini A, Sánchez-Ferro Á, Mestre TA. Technology-enabled care: integrating multidisciplinary care in Parkinson’s disease through digital technology. Front Neurol. 2020;11:575975. doi:10.3389/fneur.2020.575975
106. Russell J, Inches J, Carroll CB, Bergmann JHM. A modular, deep learning-based holistic intent sensing system tested with Parkinson’s disease patients and controls. Front Neurol. 2023;14:1260445. doi:10.3389/fneur.2023.1260445
107. Ortiz-Barrios M, Cleland I, Donnelly M, et al. Integrated approach using intuitionistic fuzzy multicriteria decision-making to support classifier selection for technology adoption in patients with Parkinson disease: algorithm development and validation. JMIR Rehabil Assist Technol. 2024;11:e57940–e57940. doi:10.2196/57940
108. Teymourian H, Tehrani F, Longardner K, et al. Closing the loop for patients with Parkinson disease: where are we? Nat Rev Neurol. 2022;18(8):497–507. doi:10.1038/s41582-022-00674-1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Preferences for Rehabilitation in Persons with a History of Stroke: A Discrete Choice Experiment
Noto S, Murata T, Saito S, Watanabe T, Kobayashi M
Patient Preference and Adherence 2023, 17:1611-1620
Published Date: 12 July 2023