Back to Journals » Journal of Hepatocellular Carcinoma » Volume 13
An Inflammation-Associated Prognostic Model for Hepatocellular Carcinoma Following Radical Resection
Authors Zhai Y, Gan B, Guan R ![]() , Lin Y, Lu Y
, Lin Y, Lu Y
Received 5 October 2025
Accepted for publication 25 December 2025
Published 8 January 2026 Volume 2026:13 567300
DOI https://doi.org/10.2147/JHC.S567300
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ahmed Kaseb
Yanyun Zhai,1,* Biling Gan,1,* Renguo Guan,1 Ye Lin,1 Yanxia Lu2
1Department of Hepatobiliary Surgery, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People’s Republic of China; 2Department of Operating Room, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ye Lin; Yanxia Lu, Email [email protected]; [email protected]
Background: Hepatocellular carcinoma (HCC) remains poor, and inflammatory markers have emerged as potential predictors. This study aimed to develop and validate a nomogram for predicting overall survival (OS) in patients with HCC after radical hepatectomy by integrating inflammatory markers with clinicopathological factors.
Methods: We retrospectively analyzed patients with HCC who underwent radical hepatectomy at the Guangdong Provincial People’s Hospital between 2014 and 2018. The patients were randomly assigned (2:1 ratio) to the training and validation cohorts. Independent prognostic factors were identified using univariate and multivariate Cox regression analyses to construct a nomogram. The performance of the model was assessed using ROC, calibration, and decision curve analysis (DCA) and compared with established staging systems (AJCC 8th edition TNM, BCLC, and CNLC).
Results: The training and validation cohorts included 242 and 121 patients, respectively. Aspartate aminotransferase-to-platelet ratio index (APRI), systemic inflammation response index (SIRI), and microvascular invasion (MVI) were identified as independent prognostic factors (P < 0.05). In the training cohort, the nomogram achieved AUCs of 0.837, 0.778, and 0.793 for the 1-, 3-, and 5-year OS, respectively. The corresponding AUCs in the validation cohort were 0.712, 0.746, and 0.746, respectively. The calibration curves and DCA confirmed the robust predictive ability of the model. The nomogram AUCs were significantly higher than those of all staging systems (P < 0.05).
Conclusion: The proposed nomogram, incorporating APRI, SIRI, and MVI, effectively predicts OS in patients with HCC following radical resection and outperforms conventional staging systems.
Keywords: hepatocellular carcinoma, inflammatory markers, microvascular invasion, nomogram, prognosis
Introduction
Liver cancer, a globally significant malignancy, is the second most frequent cause of cancer-related mortality in China, accounting for >50% of worldwide incident cases annually.1 Hepatocellular carcinoma (HCC) is the predominant histopathological subtype of primary liver malignancy, accounting for >75% of global cases.2 Currently, a wide range of treatment options is available for treating HCC. Although recent basic research has found that ferroptosis and pyroptosis can inhibit HCC cells,3,4 radical resection remains the most effective therapeutic approach for patients with early stage liver cancer.5 However, despite undergoing radical surgery, most HCC patients still have poor overall survival outcomes.6 Therefore, developing and validating a model capable of predicting the prognosis of patients with HCC is of significant clinical importance.
Currently, the Barcelona Clinical Liver Cancer (BCLC) staging system, American Joint Committee on Cancer (AJCC) staging system (TNM), and Chinese National Liver Cancer (CNLC) staging system are the primary clinical scoring systems used to assess prognosis in patients (HCC) patients.7–9 However, these systems are primarily based on anatomical and hepatic function characteristics and fail to adequately incorporate molecular or immunological markers reflecting the biological behavior of the tumor. Recent literature suggests that inflammatory markers may serve as predictors of overall postoperative survival in patients.10–12 In recent years, prognostic models based on inflammatory biomarkers have shown potential. However, most existing models exhibit significant limitations: some validate the prognostic value of a single marker, but lack clinical utility; others rely on small-sample, single-center data, raising questions about their generalizability, or failing to demonstrate significant advantages over standard staging systems in model comparisons. For example, the platelet-to-lymphocyte ratio (PLR) is an independent risk factor for extrahepatic metastasis following radical hepatocellular carcinoma resection.13 Similarly, the Xiangya Hospital team discovered that the Prognostic Nutritional Index (PNI) and Systemic Inflammatory Index (SII) can predict HCC patient outcomes.14 Although Guo et al successfully demonstrated the predictive value of inflammatory markers for early postoperative recurrence in hepatitis B-associated hepatocellular carcinoma,15 the predictive efficacy of these markers for long-term overall survival and distant recurrence (eg, 2–5 years postoperatively) remains unclear. We aimed to integrate these scattered, known indicators with key pathological features through multivariate Cox regression analysis to construct a visual, user-friendly nomogram prediction tool. This enables clinicians to input specific parameters for individual patients with HCC and directly calculate their precise survival probability, guide adjuvant therapy, and follow-up intensity.
Methods
Study Design and Patients
This retrospective study analyzed patients with HCC who underwent radical hepatectomy at the Department of Hepatobiliary Surgery at Guangdong Provincial People’s Hospital from 2014 to 2018. The inclusion criteria were as follows: (1) histopathological confirmation of hepatocellular carcinoma via preoperative biopsy or postoperative specimen based on the Asia-Pacific Clinical Practice Guidelines on the management of HCC;16 (2) surgical resection margin exceeding 1 cm from the tumor edge with no significant residual lesions at the first postoperative follow-up; (3) Child-Pugh grade A or B. Exclusion criteria: (1) cholangiocarcinoma, mixed hepatocellular carcinoma, or metastatic carcinoma originating from other organs; (2) prior neoadjuvant therapy; (3) concomitant malignant tumors; and (4) incomplete clinical information or loss to follow-up. Ultimately, 363 patients with HCC were enrolled in this study. The final cohort was randomly assigned in a 2:1 ratio to training and validation groups. The patient selection and randomization process are illustrated in Figure 1.
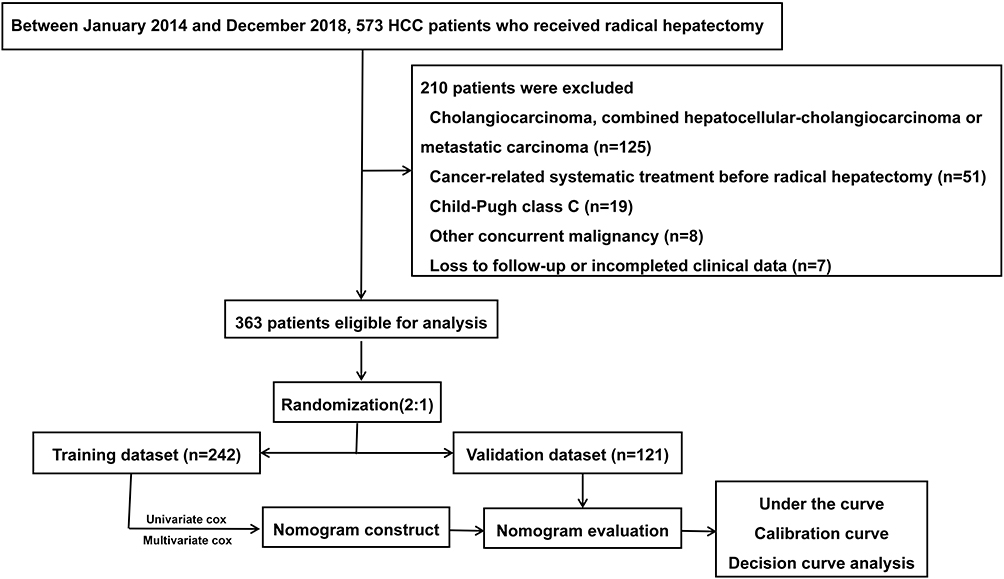 |
Figure 1 Screening and randomization process of study samples. |
Data Collection
The clinical and pathological factors potentially influencing the prognosis of patients with HCC who underwent curative surgery were collected by retrieving medical records from our hospital. Clinical parameters included age, gender, history of hepatitis B virus infection, alpha-fetoprotein (AFP), neutrophil count (×109/L), lymphocyte count (×109/L), monocyte count (×109/L), platelet count (PLT, ×109/L), prothrombin time (PT), total bilirubin (TB), alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transpeptidase (γ-GGT), albumin (g/L), and fibrinogen.
Preoperative imaging characteristics primarily included the tumor number, maximum tumor diameter, macroscopic venous or biliary tumor thrombus, distant organ invasion, and ascites. Postoperative pathological factors included Edmondson staging, microvascular invasion (MVI), and tumor capsule integrity.
Definition of Inflammatory Markers
The neutrophil-to-lymphocyte ratio (NLR),17 platelet-to-lymphocyte ratio (PLR), γ-glutamyltransferase/platelet ratio (GPR), AST-to-platelet ratio index (APRI), preoperative prognostic nutritional index (PNI) = 5 × lymphocyte count (109/L) + albumin (g/L),18 fibrinogen/lymphocyte ratio (FLR), AST-to-neutrophil ratio index (ANRI), systemic immune-inflammation index (SII) = platelet count × neutrophil count/lymphocyte count,19 and systemic inflammation response index (SIRI) = neutrophil count × monocyte count/lymphocyte count.
Follow-Up
All patients undergoing radical hepatocellular carcinoma resection received outpatient and telephone follow-up. The first postoperative review occurred within one month; subsequent reviews were conducted every three months for the first five years post-surgery; thereafter, reviews were scheduled every six months. Follow-up assessments included biochemical function, tumor markers, hepatitis B virus (HBV) DNA, complete blood count, coagulation parameters, and contrast-enhanced CT or MR imaging (MRI). The primary survival outcome was overall survival (OS). OS was defined as the time interval from the date of surgery to the last follow-up visit or the time of death.
Nomogram Construction and Validation
Univariate Cox regression analysis was performed to identify variables that could potentially affect the prognosis. These variables were then incorporated into the multivariate Cox regression analysis to determine the independent prognostic factors. The nomogram was developed based on the results of multivariate Cox proportional hazards regression analysis. The model took the form of a linear predictor (LP), calculated as follows: LP = (βAPRI × APRI value) + (βSIRI × SIRI value) + (βMVI × MVI status), where β represents the regression coefficient for each variable derived from the multivariate Cox model. This linear predictor corresponds to the log of the hazard ratio for each patient. The “rms” package in R was used to graphically represent the model as a nomogram, which translates the complex regression equation into a user-friendly scoring system. In the nomogram, each predictor is assigned a point scale; the points for all predictors are summed to obtain a total point score, which is then projected to the bottom scales to estimate the probability of 1-, 3-, and 5-year overall survival. Receiver operating characteristic (ROC) curves were plotted, and the area under the curve (AUC) was calculated to assess the predictive capability of the nomogram. Calibration curves were plotted to evaluate the consistency between the observed and predicted diagnoses.20 Decision curve analysis (DCA) was performed to further determine the clinical applicability of the nomogram by quantifying the net benefit as the threshold probability increased.21 We selected five representative machine-learning algorithms commonly used in medical prognosis prediction as comparative benchmarks: logistic regression (LR), decision tree (DT), naive Bayes (NB), support vector machine (SVM), and gradient boosting (GB).22 We compared the AUC values, sensitivity, and specificity of all models for predicting 1-year, 3-year, and 5-year overall survival.
Statistical Analysis
Continuous variables following a normal distribution were analyzed using unpaired Student’s t-test. For non-normally distributed data, the Mann–Whitney U-test was used. Categorical variables were compared using Pearson’s chi-squared test or Fisher’s exact test. Risk scores were calculated for all patients with HCC in this study based on the nomogram, categorizing patients into high-, intermediate-, and low-risk groups according to their scores. Survival analysis among different risk groups was conducted by plotting Kaplan-Meier curves, and survival differences were validated using the Log rank test. All statistical analyses were performed using R software (version 4.1.0, http://www.r-project.org/). Statistical significance was set at P < 0.05, and all tests were two-sided.
Results
Patient Characteristics
The median follow-up duration for 363 patients was 36 months, with 76 deaths recorded at the end of the follow-up. The mean age was 54.05 ± 11.33 years. The numbers of patients classified as BCLC-0, BCLC-A, BCLC-B, and BCLC-C stages were 50, 241, 32, and 40, respectively. Among the 363 patients, postoperative pathology indicated the presence of MVI in 30%. Further analysis demonstrated balanced baseline characteristics between training and validation cohorts. Table 1 summarizes the baseline characteristics of the patients in this retrospective study.
 |
Table 1 Baseline Characteristics of Patients with Included HCC |
Univariate and Multivariate Cox Analysis of Prognosis After Radical Surgery in Hepatocellular Carcinoma Patients
In the training cohort, univariate retrospective analysis of the aforementioned inflammatory markers and clinical-pathological variables indicated that AFP, NLR, APRI, SIRI, and MVI were associated with prognosis in patients with HCC undergoing radical surgery (P < 0.05), whereas BCLC classification, tumor capsule integrity, and Edmondson classification were not associated with prognosis (P > 0.05). We further incorporated these prognostic factors into multivariate regression analysis. Results identified APRI (HR: 1.60; 95% CI: 1.12–2.28; P < 0.01), SIRI (HR: 1.70; 95% CI: 1.13–2.54; P < 0.01), and MVI (HR: 2.33; 95% CI: 1.23–4.40; P < 0.01) as independent risk factors for HCC prognosis. The detailed results are presented in Table 2.
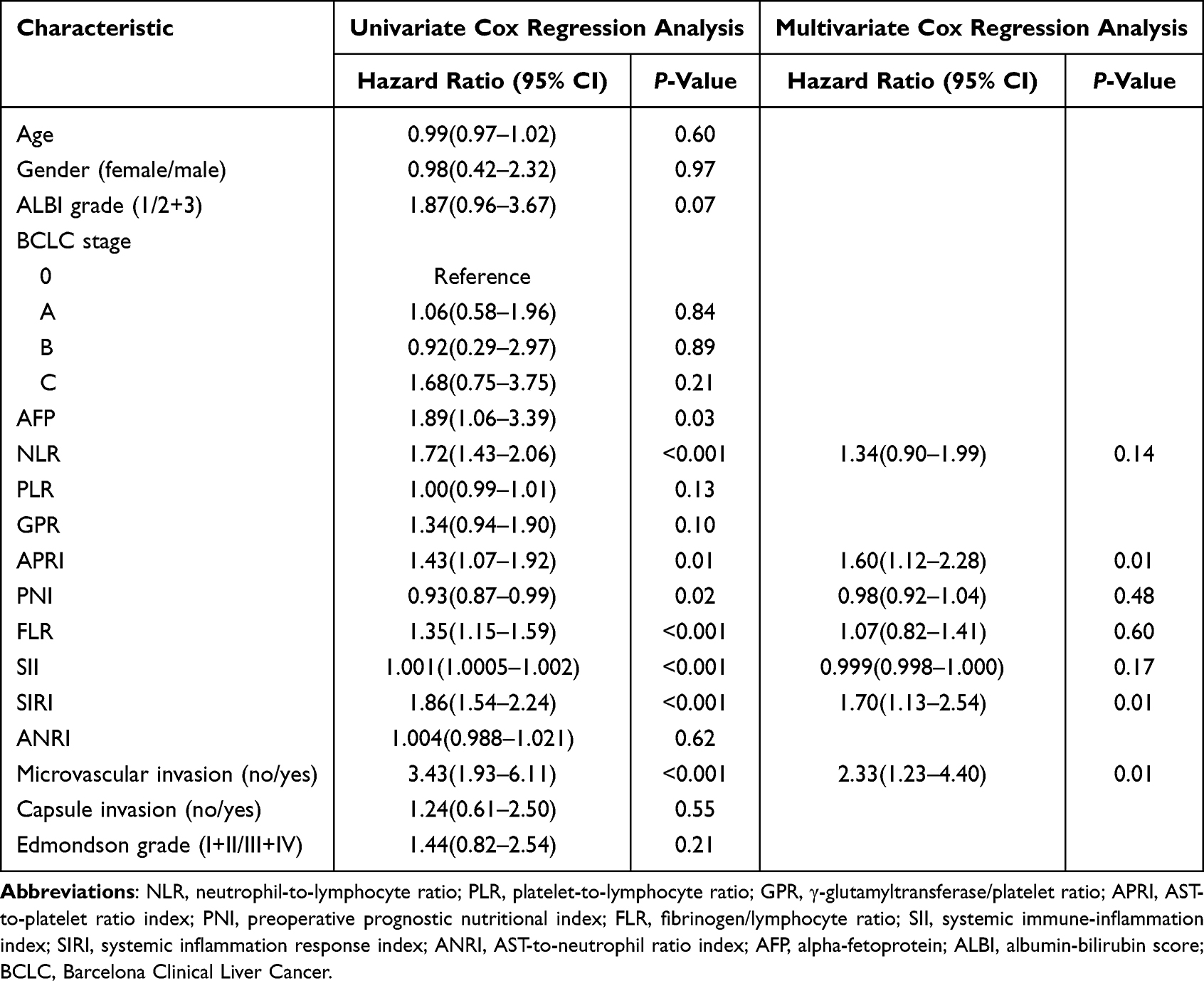 |
Table 2 Univariate and Multivariate Cox Analysis of Overall Survival of HCC Patients Following Radical Surgery |
Development and Validation of a Nomogram Model for HCC Prognosis Prediction
Three independent predictors identified by multivariate analysis were incorporated to construct a prognostic nomogram (Figure 2). The nomogram operates by assigning a score to each variable on a point scale (top axis). For a given patient, the points for their APRI, SIRI, and MVI status were summed to yield a total point value. This total score is then projected downward to the corresponding survival probability axes at the bottom, providing individualized predictions for 1-, 3-, and 5-year overall survival. For instance, a patient with elevated APRI and SIRI values combined with the presence of MVI would accumulate a high total score, indicating a low probability of survival. We further plotted ROC curves and calculated AUC to evaluate the predictive capability of the nomogram. Notably, in the training cohort, the 1-, 3-, and 5-year AUC values of this novel nomogram were 0.837, 0.778, and 0.793, respectively (Figure 3A). In the validation cohort, the AUC values for the new nomogram at 1, 3, and 5 years were 0.712, 0.746, and 0.746, respectively (Figure 3B).
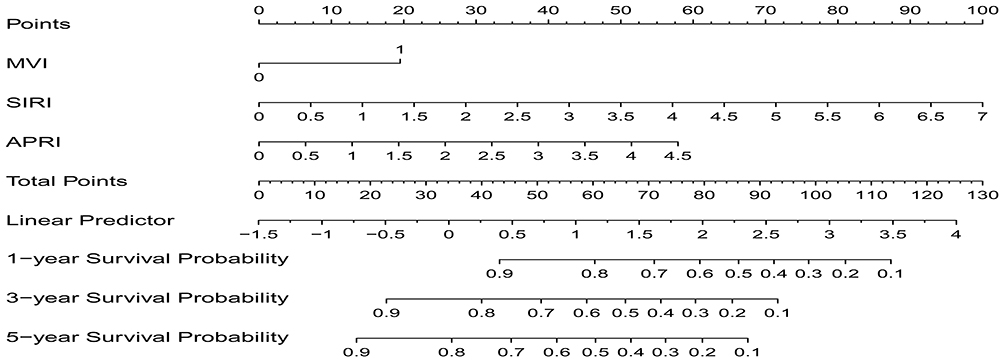 |
Figure 2 Nomogram model established in this study. |
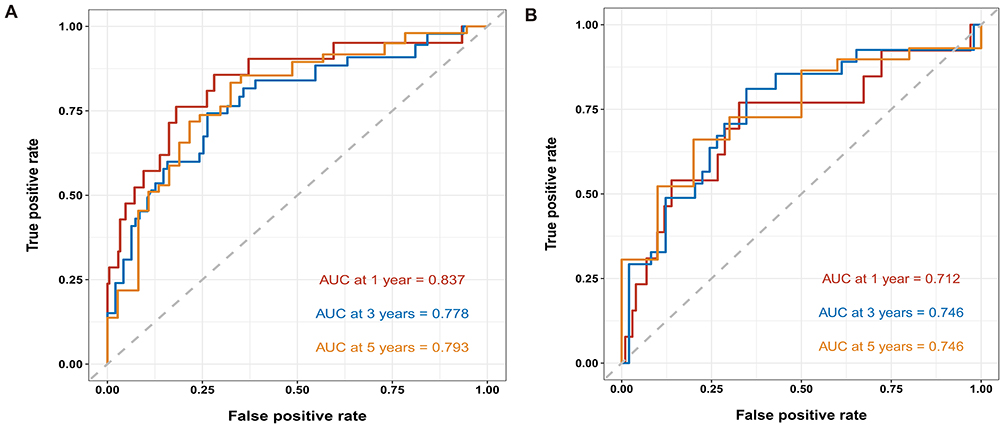 |
Figure 3 ROC curves for 1-, 3-, and 5-year predictive performance in the training set (A) and validation set (B). |
The AUC values indicate that our predictive model had good sensitivity and specificity. Calibration curves demonstrated that the predicted HCC prognosis probabilities from the nomogram were closely aligned with actual HCC outcomes in both the training group (mean absolute error = 0.023) and the validation group (mean absolute error = 0.035) (Figure 4). Furthermore, when the risk threshold exceeded 0.25 in both cohorts, our nomogram model provided a standardized net clinical benefit for patients with HCC (Figure 5A and B). Moreover, our nomogram model demonstrated predictive performance comparable to the aforementioned complex machine learning algorithms in the total cohort. Detailed comparative data are summarized in Table 3.
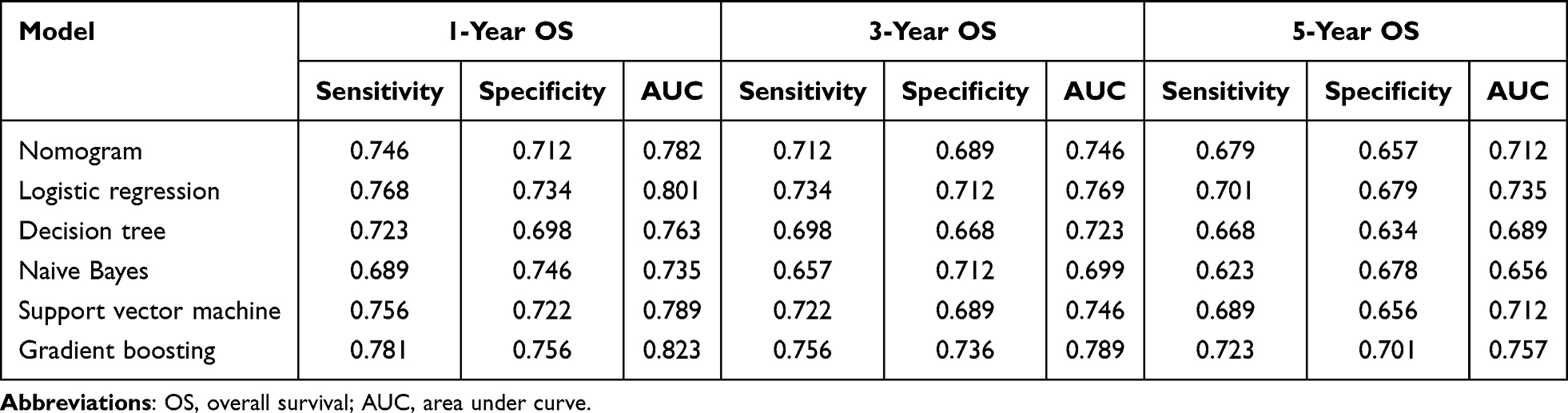 |
Table 3 Comparison of Predictive Capabilities Between the Nomogram Model and Five Other Machine Learning Algorithms |
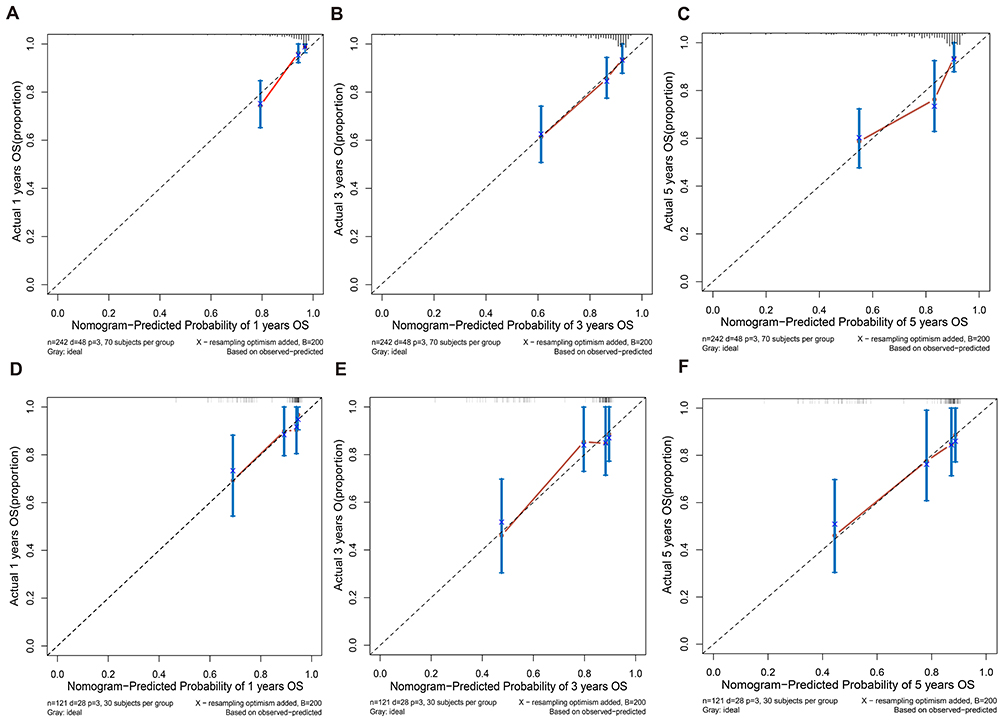 |
Figure 4 Calibration curves for the training cohort (A–C) and validation cohort (D–F). |
 |
Figure 5 Decision curve analysis (DCA) for the training cohort (A) and validation cohort (B). |
Patients with HCC were stratified into low-, intermediate-, and high-risk groups based on their nomogram scores. Survival curves demonstrated significant differences in overall survival among the three subgroups (Figure 6A, all P < 0.001). Finally, comparing our nomogram model with internationally prevalent HCC staging systems, time-ROC analysis revealed that our nomogram demonstrated significantly higher AUC values than the AJCC 8th Edition TNM, BCLC, and CNLC staging systems (all P < 0.05; Figure 6B).
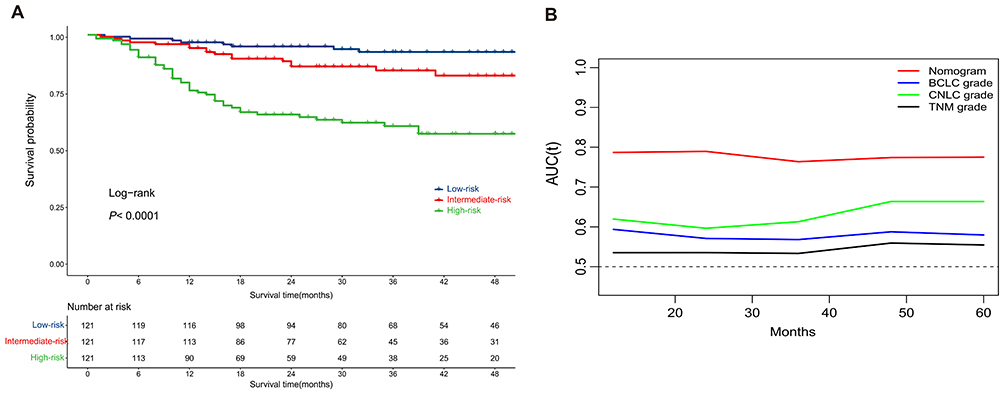 |
Figure 6 Comparison of overall survival in HCC patients across different risk subgroups (A). Comparison of time-dependent ROC values between the nomogram model and internationally recognized HCC staging systems (B). |
Discussion
Hepatocellular carcinoma accounts for 85% of primary liver cancers and remains one of the most common malignant tumors worldwide. Between 2020 and 2040, approximately 1.4 million new cases of hepatocellular carcinoma are projected globally, with approximately 1.3 million deaths attributed to the disease by 2040.23 Due to China’s large population infected with the hepatitis B virus, the country accounts for over half of the world’s new HCC diagnoses and deaths. Despite the advances in targeted immunotherapy, curative resection remains the most effective treatment modality. This study aimed to establish and validate a novel prognostic model for overall postoperative survival in patients with HCC and to evaluate the outcomes of patients undergoing curative surgery. In this study, we enrolled 363 patients who underwent radical resection and constructed a nomogram model primarily based on the APRI, SIRI, and MVI. Further analysis of the AUC, calibration curves, and decision curves demonstrated that the nomogram model possessed excellent predictive capability. Finally, compared to internationally used HCC staging systems, the nomogram model developed in this study significantly distinguished patients with different risk levels.
In this study, APRI, SIRI, and MVI were identified as independent risk factors for overall survival following radical resection for hepatocellular carcinoma. Numerous previous studies have demonstrated that MVI is a risk factor for HCC recurrence, thereby affecting the overall survival of patients with this disease.24–26 A recent prospective Phase III clinical trial found that adjuvant FOLFOX-based hepatic artery infusion chemotherapy significantly reduced the postoperative recurrence risk in patients with hepatocellular carcinoma involving microvascular invasion while demonstrating favorable safety profiles.27 Systemic inflammation is a key driver of malignant cell proliferation, invasion, and metastasis.28 SIRI, a peripheral blood marker of systemic inflammatory response, was calculated as monocytes × neutrophils/lymphocytes. Monocytes promote tissue remodeling, tumor invasion, and metastasis by secreting proinflammatory factors and differentiating into type II tumor-associated macrophages.29,30 Neutrophils also exert pro-neoplastic effects in the tumor microenvironment through mechanisms such as vascular endothelial growth factor production, to promote tumor progression.31 Conversely, low lymphocyte counts correlate with systemic inflammation, impaired cell-mediated killing, and accelerated cancer progression.32
In this study, the APRI emerged as an independent prognostic risk factor for hepatocellular carcinoma. The aspartate aminotransferase (AST)-to-platelet ratio index (APRI) serves as a noninvasive indicator for assessing liver function.33 AST level reflects the severity of liver cirrhosis and hepatic dysfunction. In patients with hepatitis B, hepatitis B virus infection damages hepatocytes, while chronic inflammation simultaneously induces hepatocyte proliferation, leading to the formation of cirrhotic nodules. The cyclical process of hepatocyte injury and proliferation may contribute to hepatocellular carcinoma development.34 Additionally, platelets (PLT) are implicated in regulating tumor angiogenesis within the tumor immune microenvironment, supplying nutrients to neoplastic tissues, and facilitating metastasis.35 Thus, the APRI, a composite measure of AST and PLT-reflects hepatocellular HCC prognosis by assessing liver functional reserve, hepatic inflammation, and microenvironmental immune status.
Systemic inflammatory markers do not exist in isolation; they likely mirror the interaction between the body’s systemic immune status and the local tumor immune microenvironment. A recent study indicated that reduced peripheral blood NLR correlated with the induction of interferon-γ responses, which in turn drives antigen presentation and the expression of pro-inflammatory gene sets, accompanied by remodeling of the intratumoral T-cell repertoire.36 A retrospective study indicated that high NLR was significantly associated with the presence of tumoral CD8+ tumor-infiltrating lymphocytes and CD33+ cells in the TIME of patients with pancreatic ductal adenocarcinoma.37 Moreover, a favorable systemic inflammatory state (eg, high LMR, low SII) may reflect robust antitumor immune surveillance, which is closely associated with effective infiltration and functional activation of cytotoxic T cells within the tumor. Based on the above observations, we propose that our nomogram model effectively predicts prognosis precisely because it indirectly captures and quantifies the unfavorable systemic and localized immune status in patients. The inflammatory markers and pathological features integrated into the model collectively provide a comprehensive picture of host-tumor interactions.
This study has several limitations. First, the primary focus of this study was the development of a clinical predictive model that did not directly analyze immune cell infiltration in tumor tissue samples. Therefore, the aforementioned discussion regarding the association between systemic inflammation and the tumor microenvironment remains a reasonable inference based on the existing literature. Future studies will directly validate the correlation between this model’s score and specific tumor microenvironment features, such as the CD8+/Treg cell ratio and macrophage polarization state, using techniques such as multiplex immunofluorescence staining, flow cytometry, or spatial transcriptomics. This provided a robust mechanistic foundation for this model. Second, the majority of patients in this cohort had a HBV background. While this inclusion criterion ensured cohort homogeneity, it also limited the direct applicability of the model to hepatocellular carcinoma patients with other etiologies, such as metabolic dysfunction-associated steatohepatitis (MASLD) or hepatitis C virus (HCV). Finally, this study was conducted at a single center; external validation in a multicenter, multifactorial cohort represents a primary step for future research.
In summary, we developed and internally validated a novel nomogram that integrates APRI, SIRI, and MVI to predict overall survival in HBV-related HCC after radical resection. The model demonstrated superior discriminative ability compared with conventional staging systems in our cohort. However, the promising performance observed necessitates further external validation in multicenter, etiologically diverse populations before clinical implementation. If prospectively validated, this accessible tool could aid clinicians in risk stratification, potentially identifying high-risk patients who may benefit from intensified adjuvant therapy, and more vigilant follow-up surveillance.
Data Sharing Statement
The datasets used and analyzed during the current study are available from Yanxia Lu upon reasonable request.
Ethics Approval
This multi-institutional retrospective study was approved by the Institutional Review Board of Guangdong Provincial People’s Hospital (KY2023-150-01). All procedures involving human participants were performed in accordance with the 1975 Declaration of Helsinki (6th Revision, 2008).
Patient Consent
Informed consent was obtained from all participants. Written informed consent was obtained from all patients for anonymized information to be published in this article.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas, took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was conducted with no funding support.
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Sun L, Yang Y, Li Y, Li Y, Zhang B, Shi R. The past, present, and future of liver cancer research in China. Cancer Lett. 2023;574:216334. doi:10.1016/j.canlet.2023.216334
2. Brown ZJ, Tsilimigras DI, Ruff SM, et al. Management of Hepatocellular Carcinoma: a Review. JAMA Surg. 2023;158(4):410–11. doi:10.1001/jamasurg.2022.7989
3. Zhang YQ, Shi CX, Zhang DM, Zhang LY, Wang LW, Gong ZJ. Sulforaphane, an NRF2 agonist, alleviates ferroptosis in acute liver failure by regulating HDAC6 activity. J Integr Med. 2023;21(5):464–473. doi:10.1016/j.joim.2023.08.002
4. Zhao C, Zheng T, Wang R, et al. Synergistically Augmenting Cancer Immunotherapy by Physical Manipulation of Pyroptosis Induction. Phenomics. 2024;4(3):298–312. doi:10.1007/s43657-023-00140-y
5. Hwang SY, Danpanichkul P, Agopian V, et al. Hepatocellular carcinoma: updates on epidemiology, surveillance, diagnosis and treatment. Clin Molecular Hepatol. 2025;31(Suppl):S228–S254. doi:10.3350/cmh.2024.0824
6. Vaclav T. Surgical treatment of hepatocellular carcinoma. Klin Onkol. 2020;33(Supplementum 3):30–33. doi:10.14735/amko20203S30
7. Xie DY, Zhu K, Ren ZG, Zhou J, Fan J, Gao Q. A review of 2022 Chinese clinical guidelines on the management of hepatocellular carcinoma: updates and insights. Hepatobiliary Surg Nutr. 2023;12(2):216–228. doi:10.21037/hbsn-22-469
8. Mauro E, Forner A. Barcelona Clinic Liver Cancer 2022 update: linking prognosis prediction and evidence-based treatment recommendation with multidisciplinary clinical decision-making. Liver Int. 2022;42(3):488–491. doi:10.1111/liv.15180
9. Gao TM, Bai DS, Qian JJ, Zhang C, Jin SJ, Jiang GQ. The growth rate of hepatocellular carcinoma is different with different TNM stages at diagnosis. Hepatobiliary Pancreat Dis Int. 2021;20(4):330–336. doi:10.1016/j.hbpd.2021.02.005
10. Giannone F, Slovic N, Pessaux P, Schuster C, Baumert TF, Lupberger J. Inflammation-related prognostic markers in resected hepatocellular carcinoma. Front Oncol. 2023;13:1267870. doi:10.3389/fonc.2023.1267870
11. Song R, Ni H, Huang J, et al. Prognostic Value of Inflammation-Immunity-Nutrition Score and Inflammatory Burden Index for Hepatocellular Carcinoma Patients After Hepatectomy. J Inflamm Res. 2022;15:6463–6479. doi:10.2147/JIR.S386407
12. Zhou T, Fang J, Huang J, et al. Prognostic Value of Inflammatory Markers in HBV-Related HCC After Hepatectomy Based on a Clinical Database. J Invest Surg. 2025;38(1):2475020. doi:10.1080/08941939.2025.2475020
13. Chen Y, Zeng J, Guo P, Zeng J, Liu J. Prognostic Significance of Platelet-to-Lymphocyte Ratio (PLR) in Extrahepatic Metastasis of Hepatocellular Carcinoma After Curative Resection. Cancer Manag Res. 2021;13:1395–1405. doi:10.2147/CMAR.S290738
14. Wang D, Hu X, Xiao L, et al. Prognostic Nutritional Index and Systemic Immune-Inflammation Index Predict the Prognosis of Patients with HCC. J Gastrointest Surg. 2021;25(2):421–427. doi:10.1007/s11605-019-04492-7
15. Wenpei G, Yuan L, Liangbo L, et al. Predictive value of preoperative inflammatory indexes for postoperative early recurrence of hepatitis B-related hepatocellular carcinoma. Front Oncol. 2023;13:1142168. doi:10.3389/fonc.2023.1142168
16. Lau G, Obi S, Zhou J, et al. APASL clinical practice guidelines on systemic therapy for hepatocellular carcinoma-2024. Hepatol Int. 2024;18(6):1661–1683. doi:10.1007/s12072-024-10732-z
17. Du J, Huang Z. NLR stability predicts response to immune checkpoint inhibitors in advanced hepatocellular carcinoma. Sci Rep. 2024;14(1):19583. doi:10.1038/s41598-024-68048-9
18. Wei SM, Zeng ZX, Pan RJ, et al. Prognostic Value of the SII-PNI Score in Unresectable HCC Treated with Transcatheter Arterial Chemoembolization Combined with Lenvatinib and PD-1 Inhibitors. J Inflamm Res. 2025;18:7545–7557. doi:10.2147/JIR.S520339
19. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
20. Austin PC, Harrell FE Jr, van Klaveren D. Graphical calibration curves and the integrated calibration index (ICI) for survival models. Stat Med. 2020;39(21):2714–2742. doi:10.1002/sim.8570
21. Vickers AJ, Holland F. Decision curve analysis to evaluate the clinical benefit of prediction models. Spine J. 2021;21(10):1643–1648. doi:10.1016/j.spinee.2021.02.024
22. Ai YT, Zhou S, Wang M, Zheng TY, Hu H, Zhou PJ. Development of a machine learning-based risk prediction model for mild cognitive impairment with spleen-kidney deficiency syndrome in the elderly. J Integr Med. 2025;23(4):390–397. doi:10.1016/j.joim.2025.06.005
23. Rumgay H, Arnold M, Ferlay J, et al. Global burden of primary liver cancer in 2020 and predictions to 2040. J Hepatol. 2022;77(6):1598–1606. doi:10.1016/j.jhep.2022.08.021
24. Hao L, Zhang ZN, Han S, Miao YD, Lin S-X, Miao Y-D. New frontiers in hepatocellular carcinoma: precision imaging for microvascular invasion prediction. World J Gastroenterol. 2025;31(8):102224. doi:10.3748/wjg.v31.i8.102224
25. Li Z, Xu L, Zhu S, Qi X, Zhang W, Tang Y. Current Advances in Classification, Prediction and Management of Microvascular Invasion in Hepatocellular Carcinoma. J Cell Mol Med. 2025;29(15):e70746. doi:10.1111/jcmm.70746
26. Zheng Z, Guan R, Jianxi W, et al. Microvascular Invasion in Hepatocellular Carcinoma. A Review of Its Definition, Clinical Significance, and Comprehensive Management. J Oncol. 2022;2022:9567041. doi:10.1155/2022/9567041
27. Li SH, Mei J, Cheng Y, et al. Postoperative Adjuvant Hepatic Arterial Infusion Chemotherapy With FOLFOX in Hepatocellular Carcinoma With Microvascular Invasion. A Multicenter, Phase III, Randomized Study. J Clin Oncol. 2023;41(10):1898–1908. doi:10.1200/JCO.22.01142
28. Elinav E, Nowarski R, Thaiss CA, Hu B, Jin C, Flavell RA. Inflammation-induced cancer: crosstalk between tumours, immune cells and microorganisms. Nat Rev Cancer. 2013;13(11):759–771. doi:10.1038/nrc3611
29. Genard G, Lucas S, Michiels C. Reprogramming of Tumor-Associated Macrophages with Anticancer Therapies: radiotherapy versus Chemo- and Immunotherapies. Front Immunol. 2017;8:828. doi:10.3389/fimmu.2017.00828
30. Lippitz BE, Harris RA. Cytokine patterns in cancer patients: a review of the correlation between interleukin 6 and prognosis. Oncoimmunology. 2016;5(5):e1093722. doi:10.1080/2162402X.2015.1093722
31. Dings RP, Nesmelova I, Griffioen AW, Mayo KH. Discovery and development of anti-angiogenic peptides: a structural link. Angiogenesis. 2003;6(2):83–91. doi:10.1023/B:AGEN.0000011730.94233.06
32. Diakos CI, Charles KA, McMillan DC, Clarke SJ. Cancer-related inflammation and treatment effectiveness. Lancet Oncol. 2014;15(11):e493–503. doi:10.1016/S1470-2045(14)70263-3
33. Santol J, Kim S, Gregory LA, et al. An APRI+ALBI-Based Multivariable Model as a Preoperative Predictor for Posthepatectomy Liver Failure. Ann Surg. 2025;281(5):861–871. doi:10.1097/SLA.0000000000006127
34. Zhu GQ, Wang K, Wang B, et al. Aspartate aminotransferase-to-platelet ratio index predicts prognosis of hepatocellular carcinoma after postoperative adjuvant transarterial chemoembolization. Cancer Manag Res. 2019;11:63–79. doi:10.2147/CMAR.S186150
35. Placke T, Örgel M, Schaller M, et al. Platelet-derived MHC class I confers a pseudonormal phenotype to cancer cells that subverts the antitumor reactivity of natural killer immune cells. Cancer Res. 2012;72(2):440–448. doi:10.1158/0008-5472.CAN-11-1872
36. Hwang M, Canzoniero JV, Rosner S, et al. Peripheral blood immune cell dynamics reflect antitumor immune responses and predict clinical response to immunotherapy. J ImmunoTher Cancer. 2022;10(6):e004688. doi:10.1136/jitc-2022-004688
37. Li J, Wang J, Li Y, et al. Peripheral blood neutrophil-to-lymphocyte ratio as a prognostic marker and its association with the tumor-immune microenvironment in pancreatic cancer: a retrospective cohort study. J Gstrointestinal Oncol. 2025;16(3):1248–1257. doi:10.21037/jgo-2025-283
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.