Back to Journals » OncoTargets and Therapy » Volume 12
An Immunoscore System Based On CD3+ And CD8+ Infiltrating Lymphocytes Densities To Predict The Outcome Of Patients With Colorectal Adenocarcinoma
Authors Trabelsi M ![]() , Farah F, Zouari B, Jaafoura MH, Kharrat M
, Farah F, Zouari B, Jaafoura MH, Kharrat M ![]()
Received 7 April 2019
Accepted for publication 18 September 2019
Published 21 October 2019 Volume 2019:12 Pages 8663—8673
DOI https://doi.org/10.2147/OTT.S211048
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Nicola Silvestris
Mouna Trabelsi,1,2 Faten Farah,1 Bechir Zouari,3 Mohamed Habib Jaafoura,4 Maher Kharrat1
1Department of Human Genetic (LR99ES10), Faculty of Medicine, University of Tunis El Manar, Tunis 1006, Tunisia; 2Faculty of Sciences, University of Tunis El Manar, Foyer Universitaire, Tunis 2092, Tunisia; 3Department of Preventive Medicine, Faculty of Medicine, University of Tunis El Manar, Tunis 1006, Tunisia; 4Department of Anatomopathology, Faculty of Medicine, University of Tunis El Manar, Tunis 1006, Tunisia
Correspondence: Mouna Trabelsi
Department of Human Genetic (LR99ES10), Faculty of Medicine, University of Tunis El Manar, 15 Rue Djebel Lakhdhar, Tunis 1006, Tunisia
Tel +216 51 008 770
Email [email protected]
Purpose: The aim of this study was to evaluate the Immunoscore (IS) methodology as a prognostic marker of colorectal adenocarcinoma in Tunisian population. Tumor blocks were retrospectively collected from 106 patients with sporadic colorectal cancer.
Methods: Immunohistochemical staining and images analysis software were used to quantify the density of CD3+ and CD8+ tumor-infiltrating lymphocytes in the center of the tumor and invasive margin.
Results: The density of CD3+ and CD8+ was significantly associated with 5-year overall survival (P=0.001 and P=0.00098, respectively) and 5-year disease-free survival (P=0.0006 and P=0.0056, respectively). The earlier stage and the absence of vascular emboli showed a significant association with IS analysis. Cox multivariate regression analysis revealed that Immunoscore (from I0 to I4) was more significantly correlated with overall survival (P=0.00011) and disease-free survival (P=0.0008) than Tumor-Node-Metastasis (TNM) staging (P=0.057 and P=0.039, respectively). Patients with low IS were associated with inferior disease-free survival and overall survival, contrary to patients with high IS.
Conclusion: This is the first study which evaluated the prognostic value of IS methodology in colorectal cancer in African and Arabic population. The IS methodology carries out in this study allows to estimate the risk of relapse in patients with colorectal cancer. Overall, our results support the implementation of the consensus Immunoscore as a new component for the classification of cancer, designated TNM-Immune.
Keywords: colorectal cancer, immunoscore, AJCC/TNM-classification, tumor-infiltrating lymphocytes, digital pathology, immunotherapy
Introduction
The classification of colorectal cancer (CRC) is based on Tumor-Node-Metastasis (TNM) staging which allows the estimation of the prognosis of the resected tumors and then the choice of the appropriate treatment.1–3 However, by this classification, prognosis assessments and treatment protocol can vary from patient to patient within the same histological tumor stage, hence its limitations.4 Approximately, 20% of stage II CRC have a relapse after tumor resection.5 Thus, many studies have tried to identify novel markers such as immunological biomarkers to expand the therapeutic arsenal and overcome TNM limits.6 In past years, the role of tumor-infiltrating lymphocytes (TIL) as an anti-tumor immune response becomes evident.7–9 Indeed, tumor microenvironment consists of many types of leukocytes such as macrophages, natural killer (NK), B lymphocytes, cytotoxic and memory T lymphocytes. Naito et al10 were the first showing that CD8+ cytotoxic T-cells represent a prognostic factor. These findings were also supported by the studies of Murphy, Nagtegaal and Chiba.11–13 Recently, many studies showed the significant correlation between the densities of T-infiltrating lymphocytes and the prognosis of CRC. Moreover, a high density of CD8+ T-lymphocytes is associated with an improved prognosis in colorectal cancer.14 This correlation was also supported by the chemotherapy treatment efficiency at the metastatic site.15 Among several immunological biomarkers, the ratio of CD8+/CD3+ T-cells density was recently proposed as being a significant prognostic marker in comparison to TNM staging.
Furthermore, the location, type and density of infiltrating cells in tumoral microenvironment could influence the evolution of CRC.16 Since 2012, a novel classification called “Immunoscore” (IS) for colorectal cancer based on the quantification of CD3+ and CD8+ T-cell densities in the center of the tumor (CT) and in invasive margin (IM) has been proposed along with TNM staging.17–19 An international consortium was initiated with the support of the Society for Immunotherapy of Cancer (SITC) to validate the consensus Immunoscore in clinical practice for CRC patients. The final report was published to demonstrate the significant and robust effect of IS to predict survival, local or distant tumor recurrence and treatment response.20 In the light of all these findings cited, the aims of this current study were: (1) first, was to confirm the prognostic value of the Immunoscore for the patients with colorectal adenocarcinoma after radical surgery (2) second, was to compare accuracy of the standard TNM staging and the IS, (3) third, was to evaluate the performance of TIL to predict the choice of adjuvant treatment and (4) finely, was to demonstrate the feasibility and reproducibility of the IS method.
Materials And Methods
Patients
This study enrolled 106 Tunisian patients retrospectively assigned with sporadic colorectal adenocarcinoma diagnosed at the Department of Pathology, Charles Nicole University Hospital (CNUH), Tunis, Tunisia between January 2007 and December 2010. All patients have undergone a primary resection of the colon cancer tumor and a mesorectum excision for rectal cancer. Demographics information of patients (sex and age), tumor features, the American Joint Committee on Cancer (AJCC)/TNM staging system (I-IV), anatomic site, histological grade, vascular-lymphatic and perineural invasions were obtained from pathologic reports. Cases having an age ≤40 years were considered as young patients. Information is about surgery, adjuvant treatment and survival outcomes were obtained from medical records archives. Adjuvant chemotherapy (Folfox 4, Xeloda and/or, Folfiri) was administrated to 51 patients. Only one patient received an adjuvant radiotherapy. The mean period of follow-up was 52 months [0–115 months].
Pathological Study
The hematoxylin and eosin (H&E) sections were analyzed by two pathologists. Each pathologist gave information following criteria of the World Health Organization (WHO)21 about tumor localization (distal, proximal and rectum), differentiation grade (well, moderate and poor), histological type (non-mucinous and mucinous cancers were those containing more than 50% of extracellular mucin), vascular emboli (VE) or lymphatic invasion (LI) or perineural invasion (PI) (VELIPI status), TNM staging system (7th edition) and macroscopic aspects. The lymph node ratio (LNR) is defined as the number of positive lymph nodes divided by the total number of lymph nodes examined.22
Immunohistochemical Staining
Different steps were taken: sections of 4 µm thickness were cut from paraffin tissue blocks and mounted on silanized slides. Antigen retrieval solution (10X concentrate, Novocastra, Leica), primary antibodies (Rabbit monoclonal recognizing human CD3 (Ventana Medical Systems Cat# 790-4341, RRID: AB_2335978) and CD8 (Ventana Medical Systems Cat# 790-4460, RRID: AB_2335985)) and secondary antibody (rabbit-anti-mouse IgG, Bond Refine Detection Kit, Leica) were performed according to the manufacturer’s recommendations in an automate Bench Mark Ventana. Finally, sections were subsequently incubated with 3,3-diamino-benzidine (DAB+ chromogen, Novolink, Leica), counterstained with Haematoxylin (Novocastra, Leica) and mounted with a special glue (Eukitt, GmbH, Medite). The internal positive control was used for quality assurance.
Quantification Of Tumor-Infiltrating Lymphocytes And Determination Of The Immunoscore
Slides were scanned with NanoZoomer scanner 2.0-HT (Hamamatsu C9600-02) and the acquired images were processed using the Architect XD software (Definiens Developer XD 2.0). Image analysis software with dedicated Immunoscore module (Plug-in, INSERM/AP-HP, Paris, France) was used to determine the mean staining intensities of each slide, allowing a better sensitivity and avoiding underestimation of the total cell count (Figure 1A and B). A total of 412 images of the center of tumors (CT) and their invasive margin (IM) were analyzed to quantify CD3+ and CD8+ T-cell densities. In fact, the CT was defined as the region containing stroma and intra-tumoral cells and the IM was defined as the region of 200–500 μm between tumor microenvironment and normal mucosa, chosen by the software after manual delimitation. The best-performing algorithm to measure the IS has been described in the large international retrospective validation cohort led by the Society for Immunotherapy of Cancer (SITC).17 For each marker (CD3+ and CD8+) and each region (CT and IM), a percentile is derived from these distributions and an average percentile is calculated based on these four values. Patients were stratified according to IS reported as I0, 1-2-3-4 based on the following average percentile classes, respectively: [0%; 10%] - [>10%; 25%] - [>25%; 70%] - [>70%; 95%] - [>95%; 100%].4,18,19 Scores I0 and I1 corresponding to low-infiltrating lymphocytes densities of CD3+ and CD8+, I2 to moderate density, while I3 and I4 to high densities. Overall, a variability of the mean density between the patients was observed in each score (CD3: min = 10.1 - max = 6291 cells/mm2; CD8: min = 3.2 - max =3017 cells/mm2).
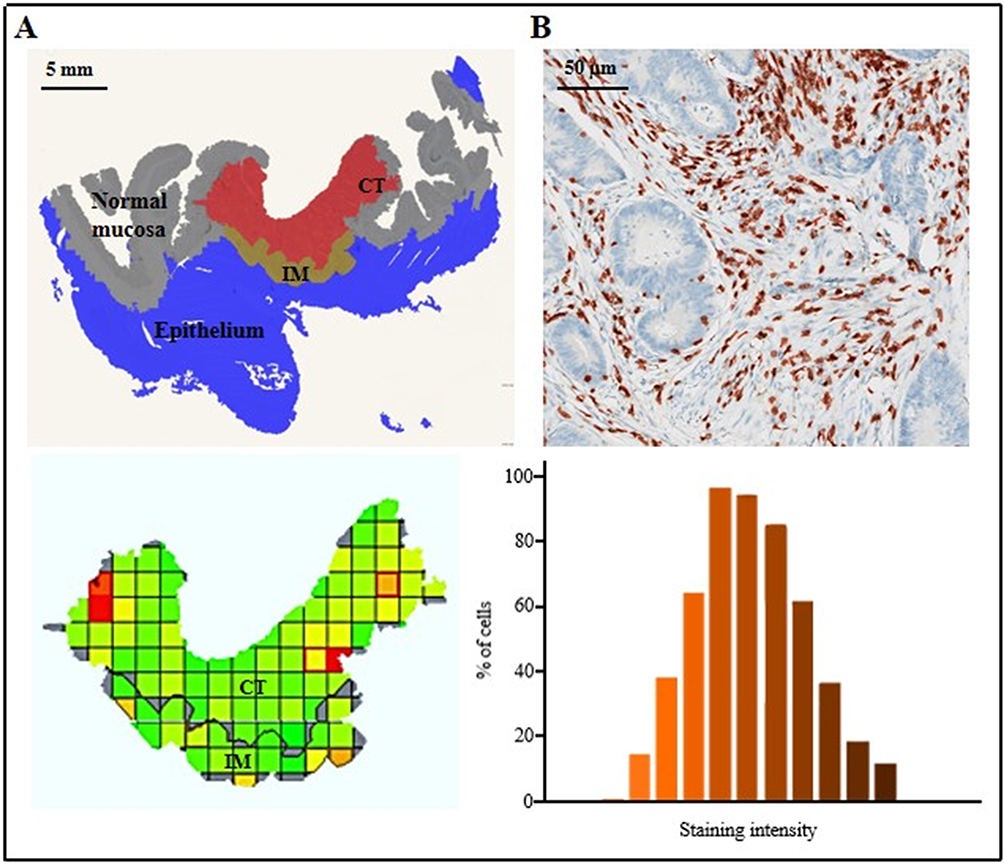 |
Figure 1 Image analysis software (with Immunoscore module) used to determine the infiltration T-cell densities. (A) The colorectal tissue is divided into tiles including center of tumor (CT) and invasive margin (IM). (B) Immunohistochemistry of colorectal tumor stained for CD3+ T-cells (Top, in brown), and histogram of the staining intensities of positive cells detected by software leading to a valid counting (Bottom: mean brown intensity ~242 arbitrary units; middle bar chart). |
Statistical Analysis
A statistical study was performed using Statistical Package for the Social Sciences (SPSS, version 19.0) and R Software (survival package, version 3.3.0). The survival data were analyzed by establishing survival curves according to the Kaplan-Meier Method (Log Rank test). Survival was divided into overall survival (OS: period between the first and last examination) and death-free survival (DFS: period between first examination and relapse). To identify the prognostic survival factors, we used an univariate analysis method (factor by factor) and a multivariate Cox regression analysis was performed for identifying the risk factors independently associated to survival (OS and DFS).
Results
Clinical And Pathological Data
Overall, 106 patients with colorectal cancer were included (Table 1). The sex ratio (Men/Women: 64/42) was equal to 1.5 and the mean age for Men was 62.07 years [33 to 84 years], whereas for Women it was 61.98 years [25 to 88 years]. 11.32% of our cases were young patients (≤40 years). We have noted the accidental discovery of the disease in 17 cases (16%). The distal colon was the predominant tumor location in 55.66% of cases and the most histological type was non-mucinous adenocarcinoma (90.6%). The majority of the tumor was well differentiated (67.96%). The features of poor prognostic, node metastasis, visceral metastasis and VELIPI were present in 44.3% of cases. Twenty-six of total metastatic patients (n=39) had metastasis in the time of diagnosis, mainly in the liver. Fifty-one patients have received an adjuvant treatment including 7 patients stage II with a high risk of relapse (presence of VELIPI criteria), 15 patients stage III and 29 patients stage IV. Different protocols were administrated for secondary localization including orally with Xeloda (300 mg/m2/day) for two weeks and intravenously with Folfox (Eloxatin, 5-Fluorouracil and Folinic acid or Oxaliplatin, 5-Fluorouracil and folinic acid) for six cycles or Folfiri (Compto, 5-Fluorouracil and Folinic acid) for three cycles. Protocols, number of cycles and doses vary according to the anatomopathological status of the patient. Univariate analysis showed that OS and DFS are influenced by T stage, N stage, TNM staging, LNR, VELIPI criteria, and CD3+CT/IM and CD8+CT/IM infiltrating lymphocytes (Table 2).
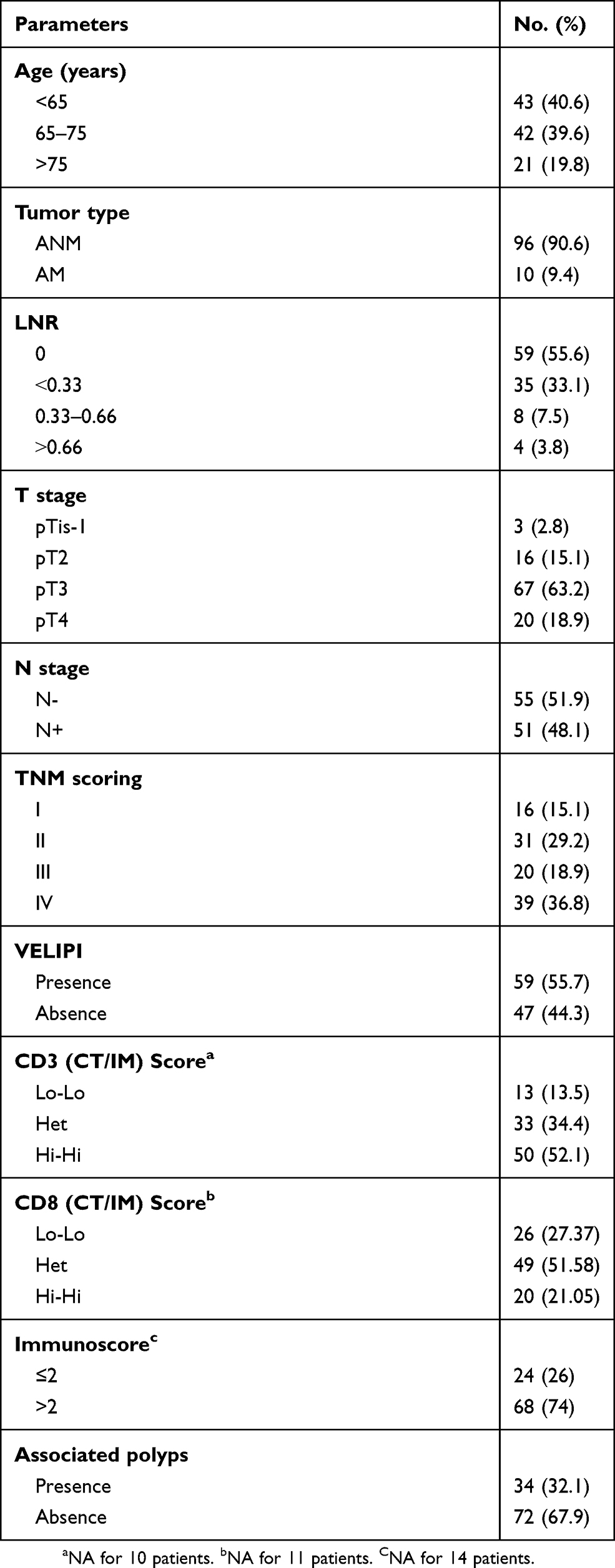 |
Table 1 Demographic And Clinicopathological Features Of 106 Primary CRCs Patients |
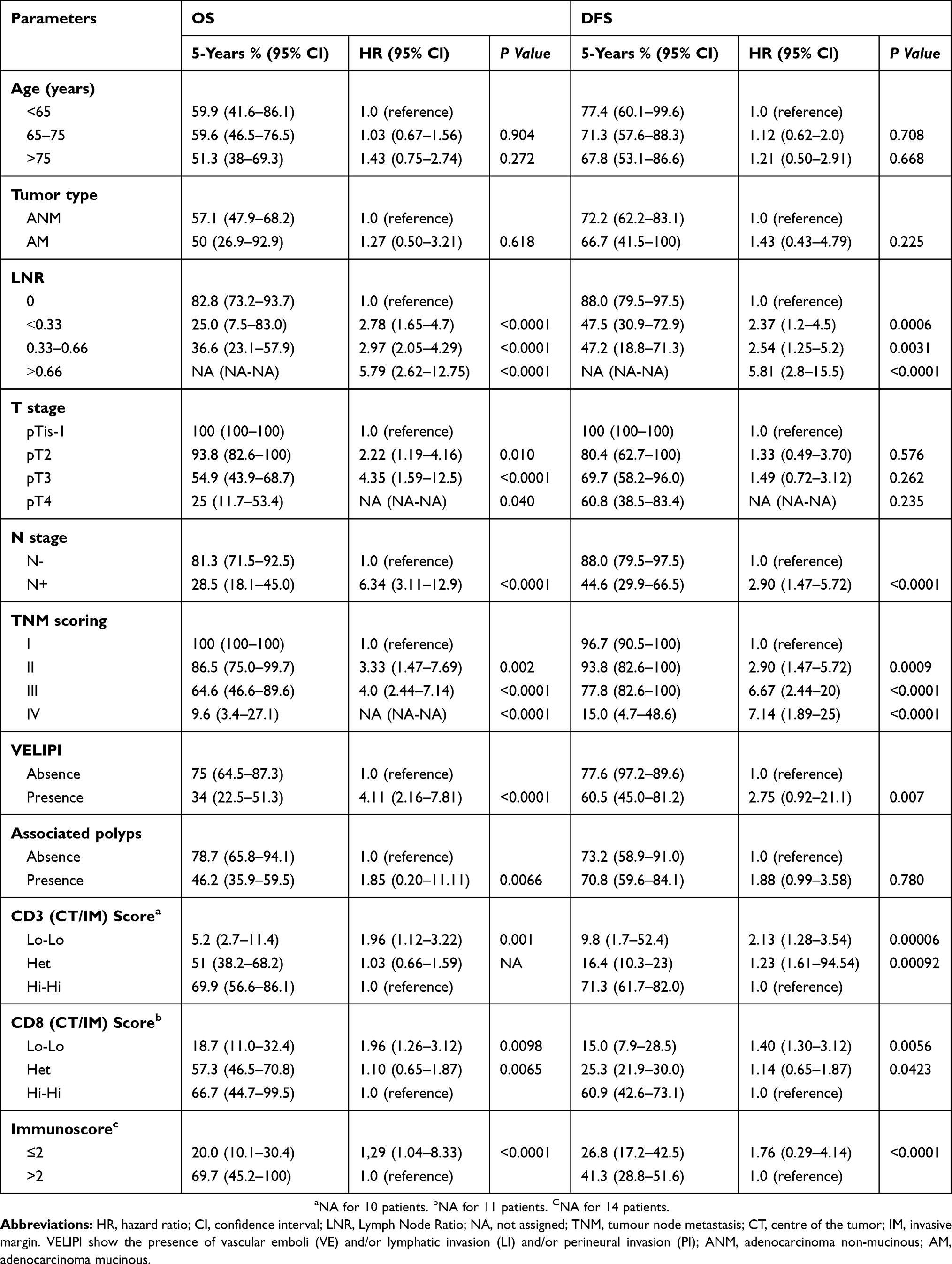 |
Table 2 Univariate Analysis For Overall Survival (OS) And Disease-Free Survival (DFS) Among Patients With Colorectal Adenocarcinoma |
Analysis Of TIL
The cases with high density in CT and IM regions were classified as High-High “Hi-Hi” (Figure 2A). Those who are with a high density in a single region (CT or IM) for one marker were considered Heterogenous “Het” (Figure 2C) and those who are with low densities in both regions were classified as Low-Low “Lo-Lo” (Figure 2B). In our study, both densities of CD3+ and CD8+ T-cells were lower in tumor tissue compared with invasive margin. A significant correlation was found between CD3+ and CD8+ T-cells density in IM (r_0.26) (Table 3). A combined analysis for both regions (CT and IM) of the same marker (CD3+ or CD8+) was performed and a significant association was found between survival (OS: Figure 3 and DFS: Figure 4) and the densities of T-infiltrating lymphocytes.
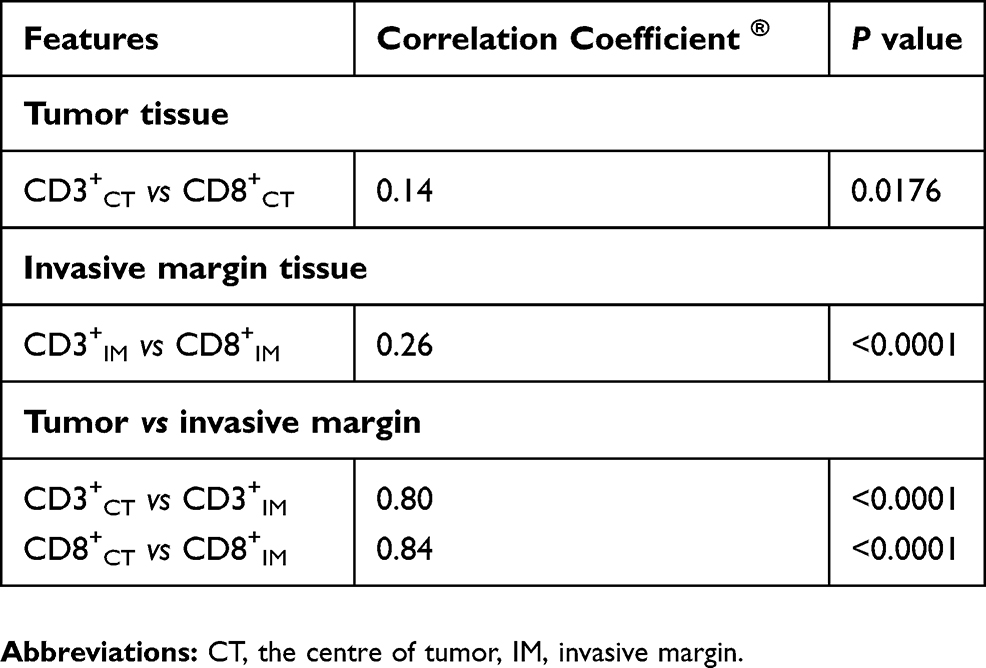 |
Table 3 Association Between T-Infiltrating Lymphocytes Densities In The Center Of The Tumor And Invasive Margin Tissues |
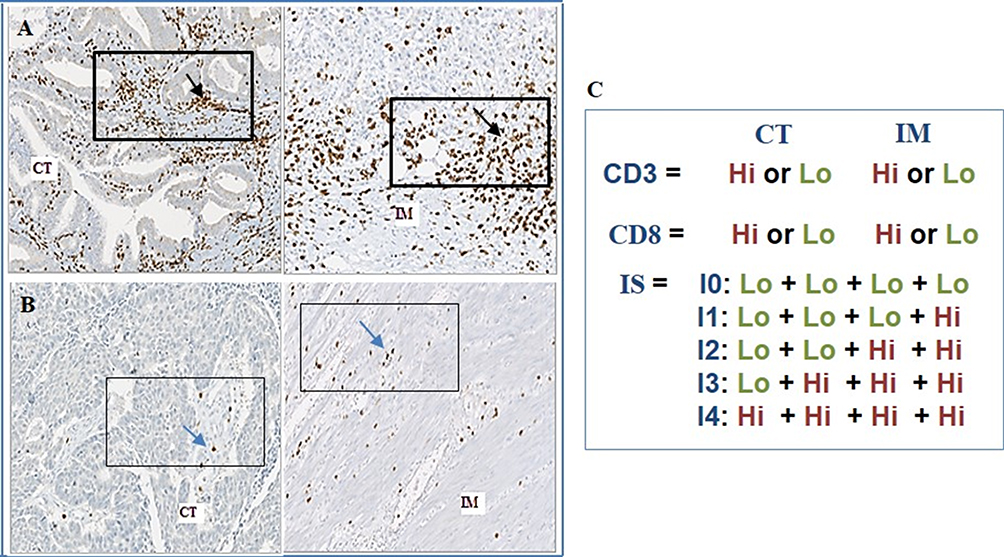 |
Figure 2 Representative figures of immunohistochemistry for tumor-infiltrating CD8+ immune cells and schematic description of the Immunoscore model. (A) Immunostaining for CD8+ illustrates a high number (black arrow) of positive T-cells in the CT (Left) and IM (right) regions. (B) Immunostaining for CD8+ illustrates a low number (Blue arrow) of positive T-cells in CT (Left) and IM (Right) regions (Magnification x200). (C) The IS model is based on the quantification of CD3+ and CD8+ in the CT and IM. All patients were grouped into high-density (Hi in dark square) and low-density (Lo in light square). Score I0 correspond to low infiltrating lymphocytes densities of CD3+/CD8+ in both regions (CT plus IM), while score I4 correspond to high densities of CD3+/CD8+ in both regions. |
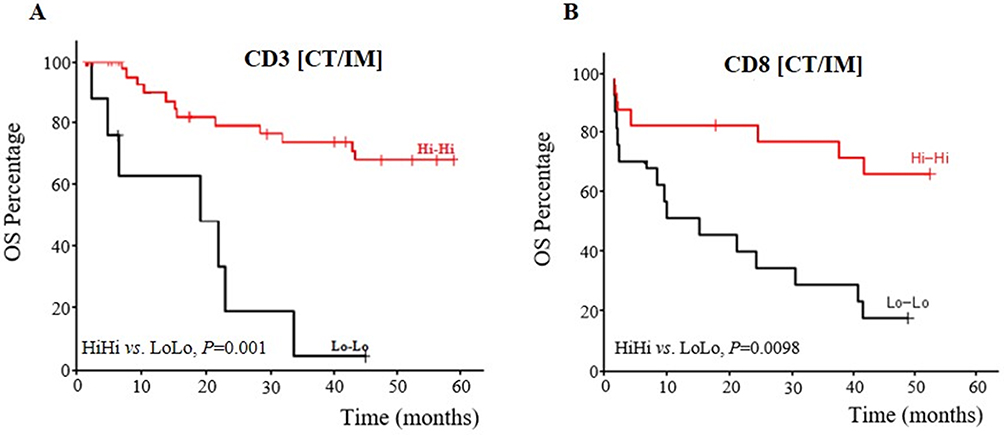 |
Figure 3 A Kaplan-Meier estimates of overall survival. (A) Kaplan-Meier curve for overall survival according to the tumor-infiltrating lymphocytes CD3+ (B) Overall survival according to the tumor-infiltrating lymphocytes CD8+. For each marker (CD3+ and CD8+), we observed a significant difference (P <0.005) between patients with low densities (Lo-Lo; black line), and high densities (Hi-Hi; red line). |
 |
Figure 4 A Kaplan-Meier estimates of disease-free survival. (A) Kaplan-Meier curve for disease-free survival according to the tumor-infiltrating lymphocytes CD3+. (B) Overall survival according to the tumor-infiltrating lymphocytes CD8+. |
Evaluation Of The IS
The scoring system depends on the total number of high densities of CD3+CT/IM and CD8+CT/IM. 4% of our cases presented an I0 score, 10% an I1 score, 12% an I2 score, 42% an I3 score and finely 32% an I4 score. The decreasing risk of relapse was inversely proportional to IS. Kaplan-Meier analysis showed a strong association between lower IS (IS≤2: I0-I2) and shorter OS and DFS, and between higher IS (>2: I3 and I4) and longer OS and DFS (P <0.0001 for DFS and OS) (Table 2). Survival curves illustrating the overall survival and disease-free survival with the IS system are shown in Figure 5. Cox multivariate regression model (IS and TNM staging) showed that IS has a highly significant correlation with OS (HR: 2.70; P=0.0001) and DFS (HR: 2.10; P=0.0008) compared to TNM staging system (HR: 1.92; P=0.057 for OS and HR: 1.95; P=0.039 for DFS) (Table 4). This result underlines that IS can be considered the highly significant prognostic factor.
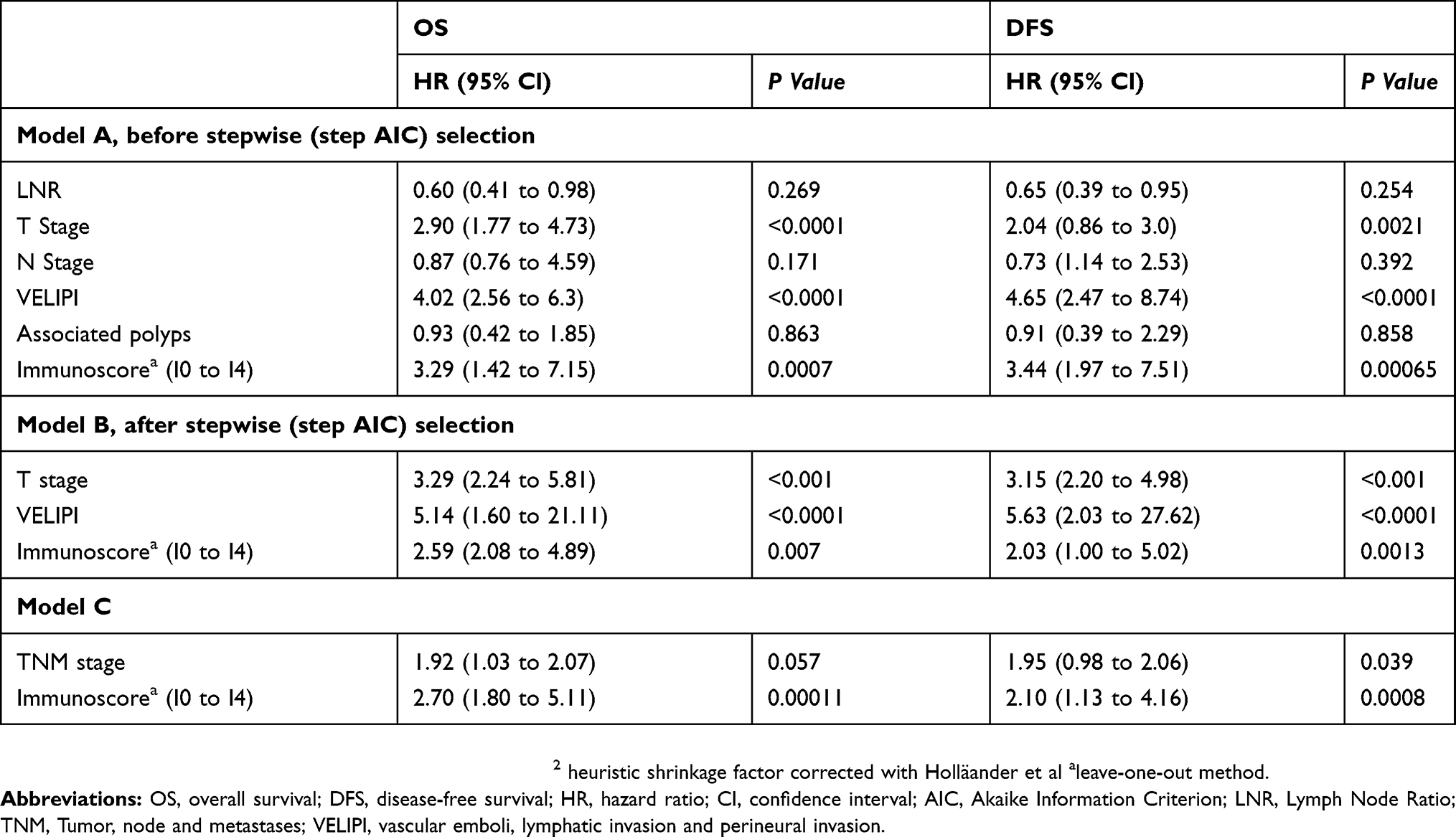 |
Table 4 Multivariate Cox Regression Analysis For IS And TNM Stage That Correlate With Overall Survival And Disease-Free Survival |
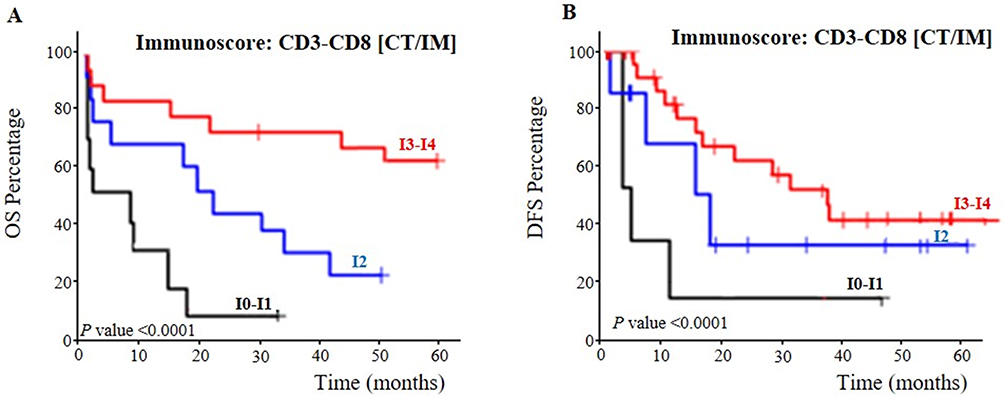 |
Figure 5 Kaplan-Meier estimates of survival. (A) Disease-free survival according to the Immunoscore of patients with colorectal adenocarcinoma. (B) Overall survival according to the Immunoscore. Patients with an Immunoscore ≤2 (I0, I1 and I2) experienced a poor postoperative outcome and thus could be grouped together. Patients with an Immunoscore >2 (I3 and I4) experienced a good postoperative outcome and thus could be grouped together. |
Discussion
For over 80 years, the most common system for classifying cancer, especially colorectal cancer, was the TNM staging, which gives incomplete information about prognostic and clinical outcome among patients with the same histological tumor stage.1–3 Indeed, TNM staging does not take into account the host immune response and focuses only on the tumor cells.23 From the beginning of the twenty-first century, growing evidence supports the important role of the immune response in the tumor. Moreover, the ability to avoid immune escape was introduced as another hallmark in the study of the tumor microenvironment.24
The determination of novel markers will allow us to choose a better-personalized treatment avoiding under/over treatment for CRC patients. Several data collected from some colorectal cancer cohort show that the presence of infiltrating lymphocytes in primitive tumors improves prognostic values for OS and DFS.25–29 Galon and Pagès showed that tumor-infiltrating lymphocytes, especially with CD3+, are directly correlated with micro-invasive status and the presence of CD8+ T-cells in the center of the tumor suggests their essential role in the immune response and disease outcome.2,30 However, the anti-tumoral immunity promotes the immunoediting, process which enables the emergence of tumor cells.31–35 Since 2012, the new classification called “IS”, based on the quantification of CD3+ and CD8+ T-cells densities in the CT and IM was proposed18,36 as a strong prognostic and predictive factor and it is now endorsed by many studies.6,37–40 CD3+ and CD8+ T-cells were chosen as markers, because of the quality of the staining and the stability of these antigens.
In this context, we aimed to evaluate the prognostic value of IS in the Tunisian population. Our result showed a statistically significant difference between CD8+IM and CD8+CT (P <0.0001), which is concordant with several studies.19,40–42 Percentages of CD3+ and CD8+ T-cell densities are inversely proportional, in both CT and IM, with tumor proliferation stage (from I to IV). These results were in line with publications showing a beneficial impact of cytotoxic T lymphocytes with various tumors: colorectal, breast, melanoma, bladder, ovarian, renal, and lung.2,29,43–45 These data suggest that tumor escape should be considered as a result of the balance between tumor infiltration mechanism and host immune response.29,46
In addition, our result confirms the importance of IS in the center of the tumor similarly as a prognostic and predictive novel marker. This is sustained with earlier literature reports.6,19,41 On the other hand, the high number of CD3+ and CD8+ infiltrating T-cells are confirmed as being better predictive factors for survival in comparison with other immune-related cells.2,18,47–49 In this study, CRC patients having lower IS (from I0 to I2) in advanced-stage tumors (III and IV-TNM staging) showed poor outcomes compared with patients with higher IS (Figure 5A and B). The univariate analysis confirmed this result (P <0.0001 for OS and DFS) and the multivariate analysis confirms that IS is more significant than the TNM scoring system. This finding is consistent with many reports.37,40,41 Cox model regression shows that DFS has a strongly significant correlation with IS (P=0.0008) compared to the TNM staging system (P= 0.039), which is also available for OS (Table 4). These results were in concordance with the study of Anitei et al.19
Pagès et al20 were found, in their study concerning the international validation of the consensus Immunoscore for colon cancer, that the ability of IS to predict overall survival was superior to that of existing tumor risk factors such as VELIPI criteria, mucinous colloid type, differentiation, and MSI status. In fact, the predictive role of immunoprofiling will become a fundamental tool for patients’ management. Typically, the tumors develop multiple mechanisms to evade the endogenous immune response, including “immune checkpoints” that can terminate immune responses after antigen activation. The immune checkpoints are necessary for developing immunotherapeutic approaches, especially for colorectal cancer.6 Thus, the use of Immunoscore, as a novel strategy in clinical routine, is necessary to assess the prognostic and predictive values accurately and to choose the best therapeutic choice for patients.
Conclusion
To summarize, the TNM staging system is widely used to evaluate CRC prognosis, but unfortunately, it cannot predict the response of treatment. The reproducibility and robustness of the IS methodology as a strong prognostic marker favor its implementation as a new component in the classification of cancer, TNM-Immune. Moreover, the IS has a strongly significant effect for predicting survival, treatment response and local or distant tumor relapse. The combined analysis of CD3 + and CD8 + IS markers was not only reliable for prognosis but was also very useful to choose the best cancer treatments. Patients presenting a low rate of infiltrating T-cells will require additional treatment to chemotherapy with antibodies which allow reactivating the anti-tumoral immune response. This first investigation will serve as a working model, to apply it to a larger number of patients and also, to other African and Arab population.
Acknowledgments
We thank Professor Pagès Franck, Dr. Kirilovsky Amos and Dr. Marliot Florence for imaging software assistance, Professor Mezlini Amel for given information about adjuvant treatment of patients, Professor Soumaya Rammeh for agreeing to give us the archived blocks of patients and Christian Boehringer of the Definiens Company for expert advice in digital pathology image quantification.
Ethics Approval And Consent To Participate
The study was approved by the Ethics Committee of Salah Azaïz Cancer Institute (ISA/2018/22) and all the samples were obtained with written informed consent and analyzed anonymously. The study was conducted in accordance with the Declaration of Helsinki.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. House AK, Watt AG. Survival and the immune response in patients with carcinoma of the colorectum. Gut. 1979;20(10):868–874. doi:10.1136/gut.20.10.868
2. Galon J, Costes A, Sanchez-Cabo F, et al. Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science. 2006;313(5795):1960–1964. doi:10.1126/science.1129139
3. Jass JR. Lymphocytic infiltration and survival in rectal cancer. J Clin Pathol. 1986;39(6):585–589. doi:10.1136/jcp.39.6.585
4. Galon J, Pages F, Marincola FM, et al. The immune score as a new possible approach for the classification of cancer. J Transl Med. 2012;10:1. doi:10.1186/1479-5876-10-1
5. Nazemalhosseini-Mojarad E, Mohammadpour S, Torshizi Esafahani A, et al. Intratumoral infiltrating lymphocytes correlate with improved survival in colorectal cancer patients: independent of oncogenetic features. J Cell Physiol. 2019;234(4):4768–4777. doi:10.1002/jcp.27273
6. Galon J, Fox BA, Bifulco CB, et al. Immunoscore and immunoprofiling in cancer: an update from the melanoma and immunotherapy bridge 2015. J Transl Med. 2016;14:273. doi:10.1186/s12967-016-1029-z
7. Diederichsen AC, Hjelmborg J, Christensen PB, et al. Prognostic value of the CD4+/CD8+ ratio of tumour infiltrating lymphocytes in colorectal cancer and HLA-DR expression on tumour cells. Cancer Immunol Immunother. 2003;52(7):423–428. doi:10.1007/s00262-003-0388-5
8. Ohtani H. Focus on TILs: prognostic significance of tumor infiltrating lymphocytes in human colorectal cancer. Cancer Immun. 2007;7:4.
9. Baglietto L, Lindor NM, Dowty JG, et al. Risks of Lynch syndrome cancers for MSH6 mutation carriers. J Natl Cancer Inst. 2010;102(3):193–201. doi:10.1093/jnci/djp473
10. Naito Y, Saito K, Shiiba K, et al. CD8+ T cells infiltrated within cancer cell nests as a prognostic factor in human colorectal cancer. Cancer Res. 1998;58(16):3491–3494.
11. Nagtegaal ID, Marijnen CA, Kranenbarg EK, et al. Local and distant recurrences in rectal cancer patients are predicted by the nonspecific immune response; specific immune response has only a systemic effect–a histopathological and immunohistochemical study. BMC Cancer. 2001;1:7. doi:10.1186/1471-2407-1-7
12. Chiba T, Ohtani H, Mizoi T, et al. Intraepithelial CD8+ T-cell-count becomes a prognostic factor after a longer follow-up period in human colorectal carcinoma: possible association with suppression of micrometastasis. Br J Cancer. 2004;91(9):1711–1717. doi:10.1038/sj.bjc.6602201
13. Murphy J, O’Sullivan GC, Lee G, et al. The inflammatory response within Dukes’ B colorectal cancers: implications for progression of micrometastases and patient survival. Am J Gastroenterol. 2000;95(12):3607–3614. doi:10.1111/j.1572-0241.2000.03377.x
14. Koch M, Beckhove P, Op Den Winkel J, et al. Tumor infiltrating T lymphocytes in colorectal cancer: tumor-selective activation and cytotoxic activity in situ. Ann Surg. 2006;244(6):
15. Halama N, Michel S, Kloor M, et al. Localization and density of immune cells in the invasive margin of human colorectal cancer liver metastases are prognostic for response to chemotherapy. Cancer Res. 2011;71(17):5670–5677. doi:10.1158/0008-5472.CAN-11-0268
16. Salama P, Phillips M, Grieu F, et al. Tumor-infiltrating FOXP3+ T regulatory cells show strong prognostic significance in colorectal cancer. J Clin Oncol. 2009;27(2):186–192. doi:10.1200/JCO.2008.18.7229
17. Galon J, Pages F, Marincola FM, et al. Cancer classification using the Immunoscore: a worldwide task force. J Transl Med. 2012;10:205. doi:10.1186/1479-5876-10-205
18. Galon J, Mlecnik B, Bindea G, et al. Towards the introduction of the ‘Immunoscore’ in the classification of malignant tumours. J Pathol. 2014;232(2):199–209. doi:10.1002/path.4287
19. Anitei MG, Zeitoun G, Mlecnik B, et al. Prognostic and predictive values of the immunoscore in patients with rectal cancer. Clin Cancer Res. 2014;20(7):1891–1899. doi:10.1158/1078-0432.CCR-13-2830
20. Pages F, Mlecnik B, Marliot F, et al. International validation of the consensus Immunoscore for the classification of colon cancer: a prognostic and accuracy study. Lancet. 2018;391(10135):2128–2139. doi:10.1016/S0140-6736(18)30789-X
21. Jass JR. The pathological classification of colorectal cancer. Ann Acad Med Singapore. 1987;16(3):469–473.
22. Petrelli F, Borgonovo K, Barni S. The emerging issue of ratio of metastatic to resected lymph nodes in gastrointestinal cancers: an overview of literature. Eur J Surg Oncol. 2011;37(10):836–847. doi:10.1016/j.ejso.2011.07.008
23. Gao P, Song YX, Wang ZN, et al. Is the prediction of prognosis not improved by the seventh edition of the TNM classification for colorectal cancer? Analysis of the surveillance, epidemiology, and end results (SEER) database. BMC Cancer. 2013;13:123. doi:10.1186/1471-2407-13-123
24. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–674. doi:10.1016/j.cell.2011.02.013
25. Bindea G, Mlecnik B, Fridman WH, et al. Natural immunity to cancer in humans. Curr Opin Immunol. 2010;22(2):215–222. doi:10.1016/j.coi.2010.02.006
26. Fridman WH, Dieu-Nosjean MC, Pages F, et al. The immune microenvironment of human tumors: general significance and clinical impact. Cancer Microenviron. 2013;6(2):117–122. doi:10.1007/s12307-012-0124-9
27. Fridman WH, Galon J, Dieu-Nosjean MC, et al. Immune infiltration in human cancer: prognostic significance and disease control. Curr Top Microbiol Immunol. 2011;344:1–24. doi:10.1007/82_2010_46
28. Fridman WH, Galon J, Pages F, et al. Prognostic and predictive impact of intra- and peritumoral immune infiltrates. Cancer Res. 2011;71(17):5601–5605. doi:10.1158/0008-5472.CAN-11-1316
29. Fridman WH, Pages F, Sautes-Fridman C, et al. The immune contexture in human tumours: impact on clinical outcome. Nat Rev Cancer. 2012;12(4):298–306. doi:10.1038/nrc3245
30. Pages F, Berger A, Camus M, et al. Effector memory T cells, early metastasis, and survival in colorectal cancer. N Engl J Med. 2005;353(25):2654–2666. doi:10.1056/NEJMoa051424
31. Clemente CG, Mihm MC
32. Dalerba P, Maccalli C, Casati C, et al. Immunology and immunotherapy of colorectal cancer. Crit Rev Oncol Hematol. 2003;46(1):33–57.
33. Zhang L, Conejo-Garcia JR, Katsaros D, et al. Intratumoral T cells, recurrence, and survival in epithelial ovarian cancer. N Engl J Med. 2003;348(3):203–213. doi:10.1056/NEJMoa020177
34. Takata Y, Nakamoto Y, Nakada A, et al. Frequency of CD45RO+ subset in CD4+CD25(high) regulatory T cells associated with progression of hepatocellular carcinoma. Cancer Lett. 2011;307(2):165–173. doi:10.1016/j.canlet.2011.03.029
35. Sun C, Sun H, Zhang C, et al. NK cell receptor imbalance and NK cell dysfunction in HBV infection and hepatocellular carcinoma. Cell Mol Immunol. 2015;12(3):292–302. doi:10.1038/cmi.2014.91
36. Ascierto PA, Capone M, Urba WJ, et al. The additional facet of immunoscore: immunoprofiling as a possible predictive tool for cancer treatment. J Transl Med. 2013;11:54. doi:10.1186/1479-5876-11-54
37. Mlecnik B, Bindea G, Kirilovsky A, et al. The tumor microenvironment and Immunoscore are critical determinants of dissemination to distant metastasis. Sci Transl Med. 2016;8(327):327ra26. doi:10.1126/scitranslmed.aad6352
38. Kirilovsky A, Marliot F, El Sissy C, et al. Rational bases for the use of the Immunoscore in routine clinical settings as a prognostic and predictive biomarker in cancer patients. Int Immunol. 2016;28(8):373–382. doi:10.1093/intimm/dxw021
39. Mlecnik B, Bindea G, Angell HK, et al. Integrative analyses of colorectal cancer show immunoscore is a stronger predictor of patient survival than microsatellite instability. Immunity. 2016;44(3):698–711. doi:10.1016/j.immuni.2016.02.025
40. Yao Q, Bao X, Xue R, et al. Prognostic value of immunoscore to identify mortality outcomes in adults with HBV-related primary hepatocellular carcinoma. Medicine. 2017;96(17):e6735. doi:10.1097/MD.0000000000006735
41. Kwak Y, Koh J, Kim DW, et al. Immunoscore encompassing CD3+ and CD8+ T cell densities in distant metastasis is a robust prognostic marker for advanced colorectal cancer. Oncotarget. 2016;7(49):81778–81790. doi:10.18632/oncotarget.13207
42. Sun C, Xu J, Song J, et al. The predictive value of centre tumour CD8(+) T cells in patients with hepatocellular carcinoma: comparison with Immunoscore. Oncotarget. 2015;6(34):35602–35615. doi:10.18632/oncotarget.5801
43. Laghi L, Bianchi P, Miranda E, et al. CD3+ cells at the invasive margin of deeply invading (pT3-T4) colorectal cancer and risk of post-surgical metastasis: a longitudinal study. Lancet Oncol. 2009;10(9):877–884. doi:10.1016/S1470-2045(09)70186-X
44. Deschoolmeester V, Baay M, Van Marck E, et al. Tumor infiltrating lymphocytes: an intriguing player in the survival of colorectal cancer patients. BMC Immunol. 2010;11:19. doi:10.1186/1471-2172-11-19
45. Lugli A, Karamitopoulou E, Panayiotides I, et al. CD8+ lymphocytes/tumour-budding index: an independent prognostic factor representing a ‘pro-/anti-tumour’ approach to tumour host interaction in colorectal cancer. Br J Cancer. 2009;101(8):1382–1392. doi:10.1038/sj.bjc.6605318
46. Hanahan D, Weinberg RA. The hallmarks of cancer. Cell. 2000;100(1):57–70. doi:10.1016/s0092-8674(00)81683-9
47. Galon J, Angell HK, Bedognetti D, et al. The continuum of cancer immunosurveillance: prognostic, predictive, and mechanistic signatures. Immunity. 2013;39(1):11–26. doi:10.1016/j.immuni.2013.07.008
48. Gao Q, Qiu SJ, Fan J, et al. Intratumoral balance of regulatory and cytotoxic T cells is associated with prognosis of hepatocellular carcinoma after resection. J Clin Oncol. 2007;25(18):2586–2593. doi:10.1200/JCO.2006.09.4565
49. Mlecnik B, Tosolini M, Kirilovsky A, et al. Histopathologic-based prognostic factors of colorectal cancers are associated with the state of the local immune reaction. J Clin Oncol. 2011;29(6):610–618. doi:10.1200/JCO.2010.30.5425
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.