")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
An Evaluation of Cabozantinib for the Treatment of Renal Cell Carcinoma: Focus on Patient Selection and Perspectives
Authors Iaxx R, Lefort F, Domblides C, Ravaud A , Bernhard JC, Gross-Goupil M
Received 5 March 2022
Accepted for publication 22 May 2022
Published 2 June 2022 Volume 2022:18 Pages 619—632
DOI https://doi.org/10.2147/TCRM.S251673
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Garry Walsh
Romain Iaxx,1 Felix Lefort,1,2 Charlotte Domblides,1– 3 Alain Ravaud,1,2 Jean-Christophe Bernhard,2,4 Marine Gross-Goupil1
1Department of Medical Oncology, Hôpital Saint-André, Bordeaux University Hospital, Bordeaux, France; 2Bordeaux University, Bordeaux, France; 3ImmunoConcEpt, CNRS UMR 5164, Bordeaux University, Bordeaux, 33076, France; 4Department of Urology, Hôpital Pellegrin, Bordeaux University Hospital, Bordeaux, France
Correspondence: Marine Gross-Goupil, Hôpital Saint-André, 1 rue Jean Burguet, Bordeaux Cedex, 33076, France, Tel +33556795808, Fax +33556795896, Email [email protected]
Abstract: Cabozantinib is an oral tyrosine kinase inhibitor (TKI) with activity against several receptors involved in the angiogenesis pathway, including vascular endothelial growth factor receptor (VEGFR), c-MET and AXL. The antiangiogenic properties of cabozantinib led to its use as a monotherapy for the treatment of metastatic renal cell cancer (RCC), and quickly resulted in this treatment becoming part of the standard of care for these tumors. Since the advent of immune checkpoint inhibitors (ICIs), new standards of care have emerged in first-line settings, involving dual ICI or ICI–VEGF-TKI (including ICI–cabozantinib) combination treatments, and leading to a more complex algorithm of care. Cabozantinib remains an option in second-line settings and is still a first-line standard of care treatment in cases where the use of ICIs is contraindicated. This review focuses on the selection of patients who may benefit most from cabozantinib therapy, including those with bone and brain metastases and those with a non-clear cell RCC histology. The need to consider disease-related symptoms, comorbidities, age, drug interactions and biomarker analyses in the choice of therapeutic strategy is also highlighted. Finally, the perspectives for the use of cabozantinib in RCC treatment are discussed.
Keywords: renal cancer, cabozantinib, patient selection, prognosis, efficacy, safety
Introduction
Renal cell cancer (RCC) accounts for 3% of adult cancers and is the 12th most common cancer worldwide.1 The most frequent histologic subtype is clear cell RCC.2 One-third of the tumors are metastatic at diagnosis. Furthermore, despite surgery, local disease will recur and become metastatic in around one-third of cases. Major therapeutic advances have radically changed the therapeutic landscape and prognosis of the disease. The first of these major advances was the development of antiangiogenic agents, such as tyrosine kinase inhibitors that target the vascular endothelial growth factor receptor (VEGFR–TKIs) and, bevacizumab, a monoclonal antibody directed against VEGF. More recently, further therapeutic advances have been made following the demonstration of efficacy of immune checkpoint inhibitors (ICIs), including anti-programmed death (PD-1), anti-programmed death ligand (PD-L1), and anti-cytotoxic T-lymphocyte-associated protein 4 (CTLA4) immunotherapies. During the antiangiogenic decade, several agents have been evaluated and integrated into the therapeutic armamentarium for RCC: first-generation TKIs sunitinib, sorafenib and pazopanib; second-generation TKIs such as axitinib, tivozanib; and, later, cabozantinib, a TKI that differs from the other agents both in terms of its activity against a range of tyrosine kinases, in addition to VEGFR, and in terms of its toxicity profile, more recently lenvatinib. This review describes the role that cabozantinib plays in the treatment of RCC.
Mechanism of Action
Cabozantinib is an oral TKI targeting several receptors involved in angiogenesis pathways, such as VEGFR2, c-MET and RET (glial cell line-derived neurotrophic factor rearranged during transfection receptor), as well as the c-Kit, AXL, TIE2 (tyrosine kinase with immunoglobulin and EGF homology domains), ROS1, TYRO3, MERTK (myeloid epithelial reproductive tyrosine kinase), TRKB (tropomyosin receptor kinase B) and FLT3 (Fms like tyrosine kinase 3) receptors. All of these targets and pathways are implicated in cancer development and progression.3,4 Inhibition of the VEGFR blocks angiogenesis, cell tubule formation, cellular migration and invasion, and cell proliferation, and induces apoptosis.5 It is this blockade that underpins the clinical efficacy of all available VEGFR–TKIs.
However, most patients being treated with anti-VEGF/VEGFR agents will experience disease progression, due to the development of definitive resistance to antiangiogenic therapies or at least transient insensitivity to VEGFR inhibition.6 This resistance to treatment led to the introduction of the notion of VEGFR-TKI rechallenge, as the need for continuous antiangiogenic pressure with subsequent lines of VEGFR-TKI therapy.7 Although the molecular and cellular mechanisms involved in resistance are still under investigation, it appears that the c-MET receptor plays a key role in this process. The binding of the ligand, the hepatocyte growth factor (HGF) to the c-MET receptor leads to the activation of multiple cellular pathways resulting in angiogenesis, cell proliferation and cell invasion. MET amplification, or more rarely activating MET mutations, have been found to be involved in the pathogenesis of multiple solid cancers, such as gastric, esophageal, and non-small cell bronchopulmonary cancer.8 Moreover, MET is a powerful angiogenesis activator and interacts with the VEGFR to induce overexpression of VEGF-A. The activation of MET contributes to an increase in angiogenic signaling, and, in addition, provides tumor cells with an alternative angiogenic pathway.9 Thus, the double inhibition of VEGF and MET is an important therapeutic strategy for preventing or overcoming primary or acquired resistance to anti-VEGFR drugs.
Of note, cMET also seems to be implicated in the development of bone metastasis. In this case the mechanism involves the stimulation of the receptor activator of NFKB ligand (RANKL) and macrophage colony stimulating factor (M-CSF) expression,10 two key factors in the physiopathology of secondary bone lesions. Cabozantinib therefore shows significant tropism for bone metastasis, regardless of the site of the primary tumor.11–13
Cabozantinib is an inhibitor of the RET receptor, which has also been implicated in tumor development via a mechanism involving the activation of the MAP kinase and PI3K-AKT pathways. In addition, the RET receptor is implicated in the inflammation process, with its activation resulting in an increase of cytokines in the tumor microenvironment, leading to the recruitment of suppressive immune cells and thus allowing tumor growth and invasion.
Pharmacokinetics
Cabozantinib is an oral medication, which can be administered either in a tablet formulation (CABOMETYX®, 60 mg free base equivalent dose, approved for RCC) or in a capsule formulation (COMETRIQ®, 140 mg free base equivalent dose, approved for the treatment of metastatic medullary thyroid cancer). These two formulations are not bioequivalent.14 Distribution of the drug is fast, with a peak between 2 and 5 hours after oral intake, and it has a long plasma half-life, estimated at around 120 hours. The steady-state concentration is reached after 15 days.15 It should be noted that absorption is modified by high-fat meals, leading to a 40.5% increase in the maximum concentration (Cmax) and a 57% increase in the area under the curve (AUC) for cabozantinib. Thus, patients receiving cabozantinib are instructed not to eat for at least 2 hours before and 1 hour after drug administration.16 Metabolism is hepatic and mediated by cytochrome P450 3A4, leading to potential drug–drug interactions, especially with CYP 3A4 inducers and inhibitors.17 Cabozantinib then undergoes elimination, mostly through the feces (54%) and urine (27%). Mild or moderate kidney failure (filtration rate >30 mL/min) does not significantly modify the pharmacokinetics of cabozantinib, allowing the drug to be used with caution in patients with renal impairment, without any dosage adjustments. In contrast, lowering of the starting dose should be considered in case of mild or moderate hepatic impairment.18,19 The pharmacokinetics of cabozantinib in case of severe kidney or hepatic impairment have not been studied. Finally, interpatient variability in the overall pharmacokinetic profile of the drug has been reported among patients with various cancer types.20
From a clinical perspective, the impact of drug exposure on clinical efficacy has been studied using exposure-response models. Predictions based on these models were mainly in favor of a correlation between exposure and response.21 Interestingly, in real-world studies, better clinical outcomes have been observed in patients who required dose reductions. This need for dose reduction may be a potential indicator of a high individual exposure, especially in the case of cabozantinib which has a narrower therapeutic index than most of the other TKIs.22,23
Clinical Efficacy
Cabozantinib Monotherapy as a First-Line Treatment for Patients with Metastatic RCC Before Immune Checkpoint Inhibitors Became Available
The first trial evaluating cabozantinib in RCC was a Phase I study involving 25 patients with metastatic RCC (MRCC) who had been heavily pretreated with a median of two prior systemic agents including, in the majority of cases (88%), at least one type of anti-VEGF therapy. The patients in this study received 140 mg of cabozantinib daily, in the capsule formulation (COMETRIQ®).24 Common adverse events were fatigue (80%), diarrhea (64%), anorexia (36%), and vomiting (36%). The most frequent grade ≥3 toxicities included fatigue (20%), diarrhea (12%), and pulmonary embolism (12%), but vomiting, anorexia and palmar-plantar erythrodysesthesia (4%) were also reported. These events led to dose reductions in 20 of the 25 patients, with the median daily dose after dose adjustment being 75.5 mg. A partial response to treatment was observed in 28% of patients, and the disease was reported as stable in 52% of the patients.
Cabozantinib was then evaluated in a Phase III trial, METEOR, in which 658 patients with MRCC who had experienced disease progression after anti-VEGFR therapy were randomized with a 1:1 ratio into groups that received either cabozantinib (60 mg daily dosage) or everolimus (10 mg daily dosage).25 The primary endpoint was progression-free survival (PFS) and secondary endpoints were the objective response rate (ORR) and overall survival (OS). The primary endpoint was reached with a significantly superior median PFS in the cabozantinib group (7.4 months; 95% confidence interval [CI]: 5.6 to 9.1) versus the everolimus group (3.8 months; 95% CI: 3.7 to 5.4), indicating that cabozantinib treatment led to a 42% reduction in the risk of progression or death (hazard ratio [HR]: 0.58; 95% CI 0.45 to 0.75; p<0.001). The ORR was also significantly higher for the cabozantinib arm than for the everolimus arm (21% versus 5%; p<0.001), and the median OS was 21.4 months for the cabozantinib group compared to 16.5 months for the everolimus group (HR: 0.66; 95% CI 0.53–0.83; p=0.00026).13 These data contributed to the approval of cabozantinib in second-line settings for patients with disease progression after previous exposure to at least one antiangiogenic agent, and to its inclusion in the National Comprehensive Cancer Network (NCCN) and European Society for Medical Oncology (ESMO) clinical practice guidelines.26 It is important to note that at this time, first-line treatments involving combinations with ICIs had not yet been approved or made available.
The role of cabozantinib as a first-line therapy for MRCC was then evaluated in MRCC patients with an intermediate or poor prognosis according to the International Metastatic Renal Cell Carcinoma Database Consortium (IMDC) classification.27 This Phase II study, the CABOSUN trial, included 157 patients naïve to systemic treatment.28 Patients were randomly assigned in a 1:1 ratio to groups that received either standard treatment with sunitinib (50 mg daily: 4 weeks on, 2 weeks off) or cabozantinib (60 mg daily, continuous dosage). Patient characteristics were well balanced: 81% of the patients included had intermediate-risk MRCC, 19% had a poor-risk MRCC, and 36.7% had bone metastasis. The primary outcome, PFS, was significantly better in the cabozantinib group than in the sunitinib group (8.2 versus 5.6 months, respectively), and the risk of disease progression or death in the cabozantinib group was reduced by 34% (adjusted HR: 0.66; 95% CI 0.46–0.95; one-sided p=0.012). A planned subgroup analysis also showed the benefit of cabozantinib over standard sunitinib treatment in both intermediate- and poor-risk MRCC patients. Among the secondary outcomes, the ORR was also higher with cabozantinib: 20% (95% CI,12.0–30.8) versus 9% (95% CI, 3.7–17.6); whereas the median between-group difference in OS did not reach statistical significance: 26.6 months (95% CI 14.6—not estimable) with cabozantinib and 21.2 months (95% CI 16.3—27.4) with sunitinib (HR: 0.80 [95% CI 0.53—1.21]).29 Subgroup analysis of patients stratified according to the presence or absence of bone metastases revealed no differences in the ORR or in PFS.30 Tolerance evaluations revealed that the incidence of grade ≥3 adverse events was similar between the two groups (67% for cabozantinib versus 68% for sunitinib), with these events including diarrhea, fatigue, hypertension, and palmar-plantar erythrodysesthesia. Dose reductions were more frequent with cabozantinib than with sunitinib (58% versus 49%), but treatment discontinuation rates due to toxicity were similar: 20% with cabozantinib and 21% with sunitinib. These data contributed to the approval of cabozantinib in a first-line setting in IMDC-classified intermediate- or poor-risk MRCC patient populations, and to its inclusion as a first-line treatment for these patient populations in the NCCN and ESMO clinical practice guidelines. As noted above, at this time first-line combination treatments with ICIs had not yet been approved and made available.31
First-Line Combination Treatments in Patients with MRCC
Finally, systemic therapies for MRCC have changed considerably over the last few years, with the treatment standards involving the use of ICIs. Both dual ICI combinations and VEGFR-TKI–ICI combinations have been found to have clinical benefits in terms of PFS, the ORR and OS compared to sunitinib32–37 in studies involving patients with an intermediate or poor prognosis, as well as in all-comer trials. These combination treatments are thus considered as the new standard of care (Tables 1 and 2). Cabozantinib has recently been evaluated in combination with nivolumab in the CHECKMATE 9ER trial. This multicentric phase III study included 651 patients with previously untreated advanced or MRCC of any IMDC prognostic risk score. The patients were randomized with a 1:1 ratio into either a group receiving treatment with cabozantinib (40 mg daily dosage) and nivolumab (240 mg every 2 weeks), or a group receiving sunitinib alone (50 mg daily, 4 weeks out of 6).35 The primary endpoint, PFS, was significantly better for the combination therapy arm than for the sunitinib arm, with a median PFS of 16.6 months for the combination group versus 8.3 months for the sunitinib group (HR: 0.51; 95% CI 0.41 to 0.64; p<0.001). The cabozantinib–nivolumab combination also led to an improvement in the ORR (55.7% versus 27.1%; p<0.001), and the complete response rate also increased over time with a median follow-up of 32.9 months (12.4 versus.5.2%).36 In addition, the combination therapy led to a significant improvement in OS, which was maintained over time (median of 37.7 months for the combination therapy arm versus 34.3 months for the sunitinib arm; HR: 0.70, 95% CI 0.55–0.90). Similar findings were observed among subgroups, most notably those stratified by PDL1 status. Grade ≥3 adverse events occurred in 75.3% of the patients in the cabozantinib–nivolumab treatment arm, compared to in 70.6% of the patients in the sunitinib treatment arm. Moreover, treatment-related adverse events were reported in 60.6% and 50.9% of the patients in these groups, respectively. Global treatment discontinuation rates were similar in both groups, occurring in 19.7% and 16.9% of cases, respectively. However, in the cabozantinib–nivolumab group, the 19.7% of patients who discontinued therapy included those who discontinued nivolumab only (6.9%), those who discontinued cabozantinib only (7.5%), and those who discontinued both treatments (5.6%). The toxicity profile of cabozantinib when used in combination with nivolumab did not differ from that observed when it is used in monotherapy. Thus, diarrhea remained one of the most frequent adverse events (grade ≥ 3: 6.9%), together with hypertension (grade ≥ 3: 12.5%). The combination appeared to have a manageable impact on liver function, with 5.3% of patients having grade ≥3 increases in aminotransferase (ALT) levels. These toxicity data indicate that the combination of cabozantinib and nivolumab has a toxicity profile that is similar to that of other combinations of TKIs and immunotherapy, and that this combination provides a feasible therapeutic option as a first-line treatment (1Tables –3).
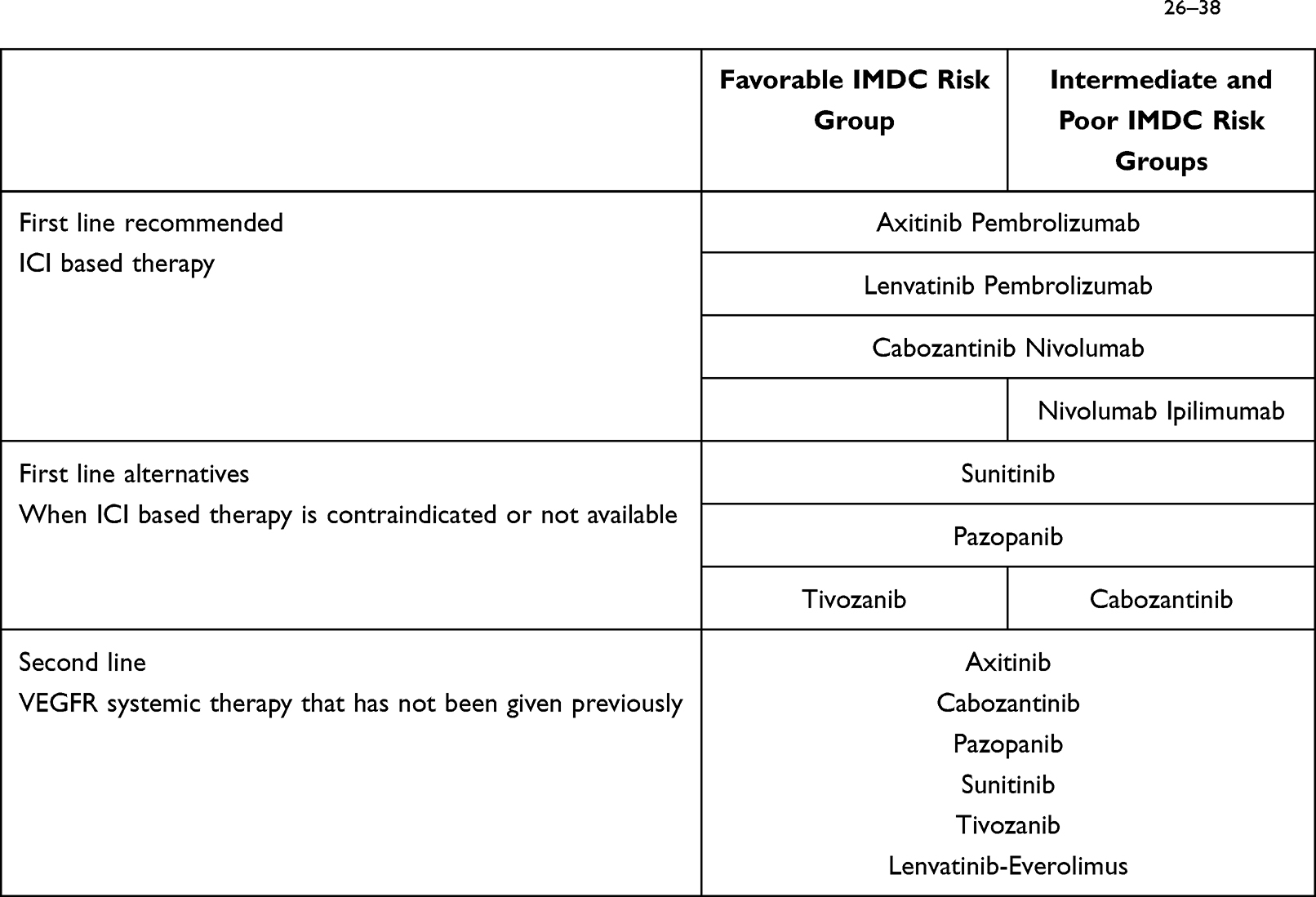 |
Table 1 European Recommendation of Systemic First and Second Line Treatment of ccRCC26–38 |
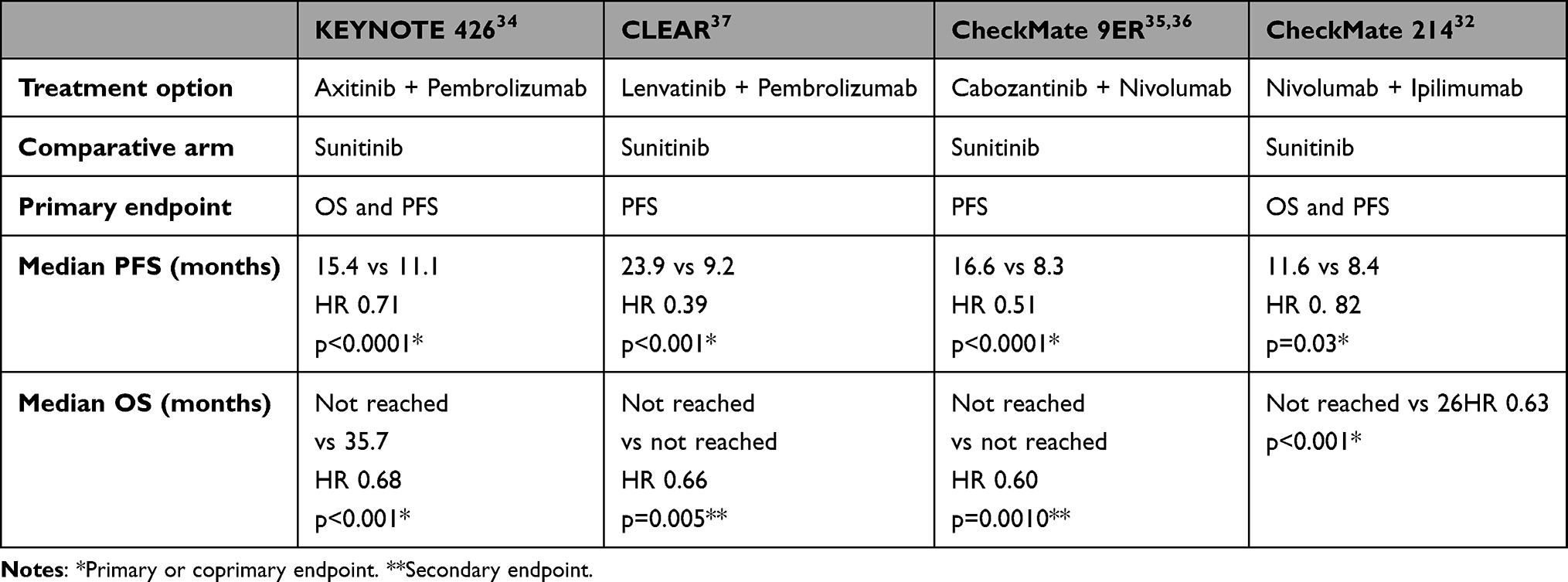 |
Table 2 Summary of Efficacy of the Combination in 1st Line |
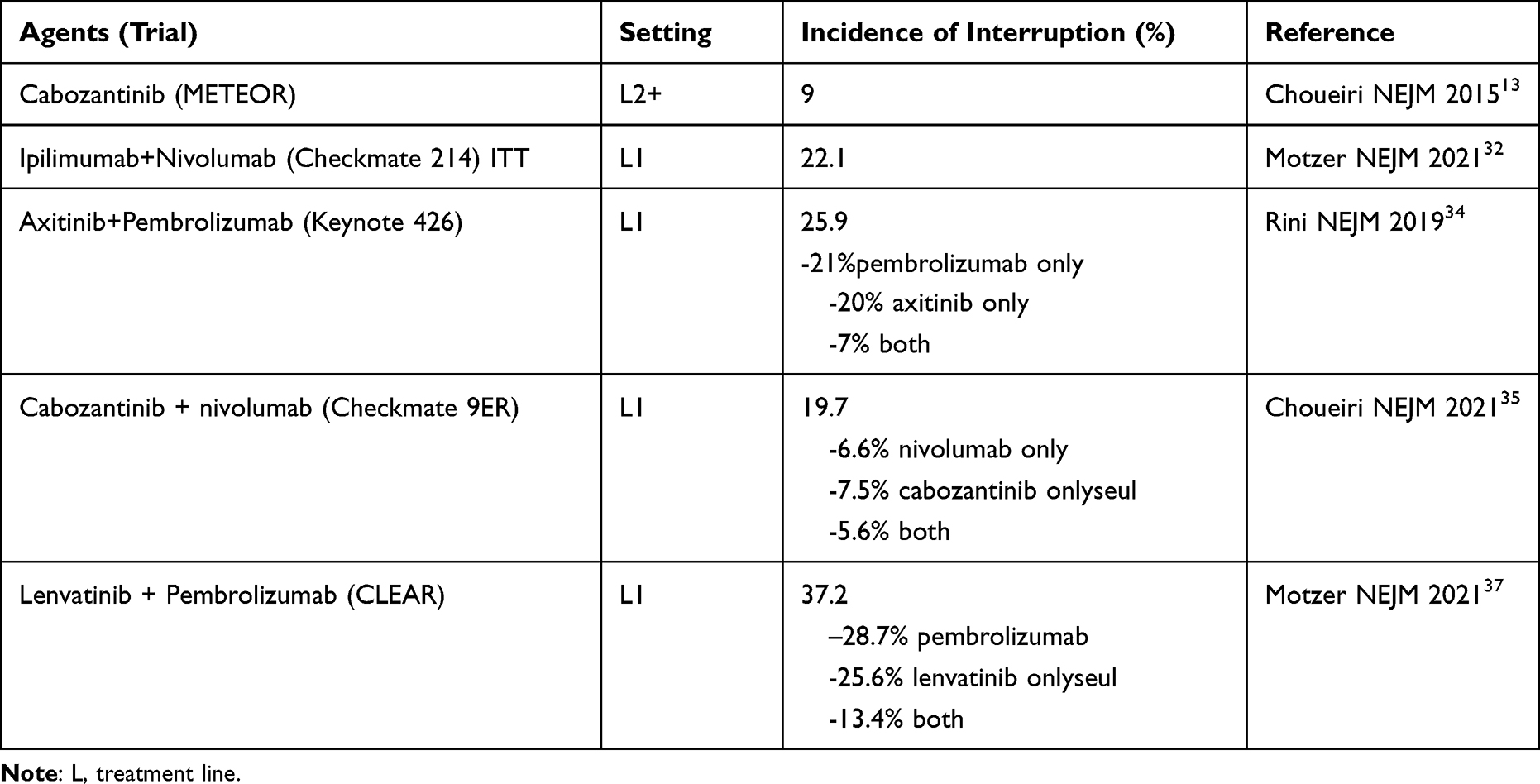 |
Table 3 Summary of the Incidence of Drug Interruption in Patients Treated with Cabozantinib, Nivolumab, or with First-Line Combination Therapies |
Finally, greater improvements in quality of life were reported by patients in the cabozantinib–nivolumab group, compared to those in the sunitinib group. These data contributed to the approval of these combination treatments in first-line settings in IMDC-classified MRCC patient populations and to their inclusion in NCCN and ESMO clinical practice guidelines.38
Cabozantinib in the Context of First-Line Combination Therapies with ICIs and VEGFR–TKIs in Patients with MRCC
The role played by cabozantinib in the treatment of MRCC has been challenged by the introduction of new standard first-line treatments for MRCC patients. Indeed, evidence from clinical trials would seem to suggest that there is no place for cabozantinib, or for other VEGFR–TKIs, in first-line settings except in cases where there is a contraindication to ICIs.32
However, it is important to consider that cabozantinib may also influence immunological responses. Cabozantinib has been shown to impact the tumor microenvironment, causing tumor cells to become more sensitive to immune-mediated cell death.39,40 This process appears to be induced through the inhibition of TK receptor signaling in the tumor microenvironment.41–43
Comparisons of the major standard primary endpoints (OS, PFS or ORR) from the pivotal clinical studies published so far do not provide clear guidance for therapeutic choices between the different combinations of ICIs and VEGFR–TKIs, particularly as the study populations and/or tumor characteristics differed slightly between studies. In addition, no comparative studies of these combinations have been conducted or initiated. So far, the only additional information available on the most appropriate combination of therapies – mostly based on complete response rates, early progression, rapid control of symptoms and the initial evolution of the PFS curve over the first 3 months of treatment – comes from position papers from experts in the field.44
Cabozantinib Monotherapy After Treatment with ICI–VEGFR-TKI or ICI–ICI Combinations
The importance of sequential treatment for patients with RCC was emphasized previously during the era when antiangiogenic agents were the only treatment option.45 New data are now needed to confirm the best forms of second-line treatment after combination therapy. The vast majority of studies conducted so far involved the use of retrospective data, and thus prospective data are limited. However, all available data suggest that the therapeutic benefits of cabozantinib are maintained when it is used in a second-line setting, even after first-line ICI–VEGFR-TKI therapy. In one retrospective study, the response rate to cabozantinib was found to be 36%, and the mean time to failure was 6.5 months.46 Of note, none of the data reported have provided any indication of the superiority of one TKI over another in terms of response rates or PFS, with the TKIs analyzed including sunitinib, axitinib, cabozantinib and pazopanib.47,48 Recently, the CABOSEQ trial has focused on assessing the efficacy of cabozantinib in second-line settings, using data from the IMDC cohort database.49 Among the 346 patients identified, 78 had been previously treated with nivolumab-ipilimumab, 46 with ICI-TKI, and 222 with another type of treatment. The IMDC risk scores were good for 12.6% of these patients, intermediate for 62.6%, and poor for 24.8%. No between-group differences were observed in the time to event endpoints and response rates, demonstrating the efficacy of cabozantinib, regardless of the treatment combination used in the first line of therapy. After first-line nivolumab-ipilimumab therapy, the median time to failure for cabozantinib was 6.90 months (range: 6.05-NR), and that after ICI-TKI therapy was 5.72 months (range: 4.41-NR). The median of OS with second-line cabozantinib therapy reached 21.44 months (range: 12.07-NR) after nivolumab-ipilimumab therapy, and 15.68 months (range: 9.27-NR) after ICI-TKI therapy. The overall response rates to second-line cabozantinib therapy after nivolumab-ipilimumab and after ICI-TKI therapy were 26.4% and 32.5%, respectively. Very few data are currently available concerning the efficacy of cabozantinib after first-line treatment with lenvatinib-pembrolizumab. Further studies are therefore essential for assessing the efficacy of second-line cabozantinib therapy in this context.
The CABOPOINT trial will, in the near future, provide much needed prospective data on the efficacy of second-line cabozantinib treatment (NCT03945773).50
Patient Selection
In comparison to the other TKIs widely used for the treatment of RCC, cabozantinib has specific properties that justify its use in particular subgroups of patients.
Bone Metastasis
As stated above, cabozantinib shows tropism for bone metastasis and specific aspects of the mechanism of action of cabozantinib may differentiate this agent from other VEGFR–TKIs. Cabozantinib has been shown to inhibit osteoclast function, reducing the RANKL/osteoprotegerin ratio in osteoblasts.51 The impact of this on bone remodeling can be rapid: 5 days in preclinical models.52 The results of the first clinical trials also seemed to show that cabozantinib displayed specific tropism for bone metastasis. In the METEOR trial (the first phase III trial using cabozantinib in RCC), cabozantinib resulted in particularly promising improvements in OS for patients with secondary bone lesions (HR: 0.54; 95% CI: 0.34–0.84), compared with patients without secondary bone lesions (HR: 0.71; 95% CI: 0.55–0.91). Similar results were observed for PFS with a HR of 0.33 (95% CI: 0.21–0.51) for patients with bone metastasis versus a HR of 0.57 (95% CI: 0.45–0.71) for patients without bone metastasis.13 Encouraging data for patients with bone lesions were also obtained in the CABOSUN trial, with a HR for median PFS of 0.54 (95% CI: 0.31–0.95) for patients with bone lesions, compared with a HR of 0.78 (95% CI: 0.48–1.21) for those without bone lesions.28 In a systematic review evaluating the impact of cabozantinib on OS – including three randomized phase III trials, METEOR, CABOSUN and EXAM (medullary thyroid cancer) – cabozantinib was found to lead to improvements in OS compared with standard care both for groups with bone metastases and for those without bone metastases, with the risk of death in these groups being reduced by 53% (HR 0.47; 95% CI 0.26–0.87; p=0.02) and 44% (HR 0.56; 95% CI: 0.40–0.79; p=0.001), respectively.53
Brain Metastasis
Among the various subgroups of RCC patients, those with brain metastasis are a matter of particular concern. Due to their poor prognosis, these patients are rarely included in clinical trials and data are lacking. In 2019, a small Italian retrospective study evaluated the safety and efficacy of cabozantinib therapy in 12 patients with RCC and brain metastasis prior to treatment and in those that had received at least one previous type of VEGFR–TKI therapy.54 The results of this study were promising, both in terms of the safety profile of cabozantinib, with no major neurological side effects being reported and grade 3/4 adverse events being rated at 36%, and in terms of clinical efficacy, with an ORR of 50%, a disease control rate of 75% and a median PFS of 5.8 months. Five of the patients included in this study received concomitant brain-directed therapy and no further progression of brain disease was documented in these patients. More recently, a larger international multicentric cohort study included 88 patients with brain metastasis from RCC.55 Of these patients, 33 were treated exclusively with cabozantinib (cohort A), whereas the 55 other patients received a local concomitant treatment (cohort B). It should be noted that almost all the patients in cohort A had received a previous locoregional treatment: 15% had undergone surgery and 70% had received whole-brain or stereotactic radiotherapy. Again, the results of this study were promising: 55% of the patients in cohort A showed an intracranial response and 48% showed an extracranial response (median OS: 15 months). In addition, 47% of the patients in cohort B showed an intracranial response and 38% showed an extracranial response (median OS: 16 months). The safety profile observed for cabozantinib in this larger study was similarly favorable, with, most notably, no unexpected side effects being documented. Although further prospective studies are needed, particularly comparative studies involving other systemic therapies, the retrospective studies that have already been conducted provide evidence supporting the use of cabozantinib in patients with RCC and brain metastasis. A prospective trial evaluating the efficacy of cabozantinib in patients with brain metastasis is ongoing (NCT03967522).
Non-Clear Cell Renal Cell Carcinoma
Studies of the therapeutic effect of first-generation of VEGFR–TKIs in patients with non-clear cell RCC have provided disappointing results. In a real-world study involving 66 papillary tumor patients identified among 112 non-clear cell RCC patients treated with cabozantinib regardless of the line of treatment,56 18 patients (27%) were reported to have achieved a partial response (95% CI: 17–40) to cabozantinib therapy. Median time to failure was 6.9 months (95% CI: 4.6–10.1) and 12-month OS was 46% (95% CI: 31–60). In addition, the results of a retrospective study, CABOREAL, showed that cabozantinib led to an OS of 16.1 months after the beginning of treatment for patients with papillary type I carcinoma and an OS 8.1 months for those with papillary type 2 carcinoma, with the study population including patients regardless of their previous line of treatment.57
More recently, in a randomized phase II trial, SWOG 1500, in which response rates of patients with papillary RCC to savolitinib, cabozantinib, and crizotinib were compared with those to the existing standard of care with sunitinib, cabozantinib was found to be superior in terms of the length of PFS in patients with papillary RCC who were naïve to VEGFR–TKI treatment.58 Overall, the median for PFS was 9.0 months (95% CI: 6–12) in the cabozantinib arm compared with 5.6 months (3–7) in the sunitinib arm (HR: 0.60; 95% CI: 0.37–0.97, one-sided p=0.019). The response rate for cabozantinib was also significantly higher than that for sunitinib, 23% versus 4%, respectively (two-sided p=0.010). These findings thus defined a new standard of care for these VEGFR–TKI naïve patients and provided a new therapeutic option for other patients with this RCC subtype.56
The results of the CABOREAL retrospective study also showed that cabozantinib was associated with efficacy in patients with primary tumors with a sarcomatoid component.58 Thirty patients had tumors with sarcomatoid features and an objective response was achieved in 20% of these patients (95% CI: 8–39). Median time to failure was 5.1 months (95% CI: 2.8–6.2) and 12-month OS was 25% (95% CI: 8–47).
Finally, a phase II trial has assessed the efficacy of combined nivolumab and cabozantinib treatment in 40 patients with papillary, unclassified or translocation-associated RCC.59 Among the 26 patients included in this study who received the combined treatment as a first-line therapy, the progression rate (PR) was 54% (14 patients), whereas in patients who received the combined as a second-line treatment the PR was 36% (5/14 patients).
Symptoms
The tumor response rate to second-generation VEGFR–TKIs appears to be higher than that to first-generation agents, which could translate for patients into a better chance of having less severe disease-related symptoms.26 The findings of the recent CHECKMATE 9ER trial, in which the safety and efficacy of combined nivolumab and cabozantinib treatment was compared to that of sunitinib and disease-related symptoms were assessed using the functional assessment of cancer therapy kidney cancer symptom index – disease-related symptom (FKSI-DRS) subscale, appear to support this hypothesis, with between-group differences significantly in favor of the combination treatment being observed at all time points.35 The results of this study also found that the combined treatment led to an ORR of 55.7% (versus 27.1% with sunitinib), and was associated with a shorter median time to response (2.8 months for the combined therapy versus 4.2 months for sunitinib), although these more favorable outcomes may also be related to the efficacy of nivolumab.
Pharmacokinetics – Drug–Drug Interactions
Like many other drugs, cabozantinib is metabolized by the liver through the activity of cytochrome P450 3A4, leading to potential drug–drug interactions. More specifically, it has been demonstrated that rifampicin, a CYP 3A4 inducer, increases the hepatic clearance of cabozantinib and results in a 77% decrease in the AUC for cabozantinib in healthy volunteers.18 Following on from the METEOR trial, exposure-response models were developed to assess the relationship between cabozantinib concentrations and efficacy. The results of this study showed that higher doses of cabozantinib (60 mg versus 40 mg or 20 mg) led to greater antitumor activity, supporting the fact that the response is correlated to exposure. However, it should be noted that this dose–response relationship may be limited by toxicity as the 60 mg dose is often poorly tolerated.21,22 Thus, concomitant cabozantinib treatment with rifampicin – as well as with several other known CYP 3A4 inducers, including antiepileptic drugs (carbamazepine, phenobarbital, and phenytoin), enzalutamide, and St. John’s Wort – should be avoided. At the same time, CYP 3A4 inhibitors – such as ketoconazole, clarithromycin and protease inhibitors – have been shown to increase the AUC of cabozantinib, with ketoconazole leading to an estimated AUC increase of 38% in healthy volunteers. In addition, cabozantinib has been shown in vitro to be a substrate of multidrug resistance-associated protein 2 (MRP2), and to be an inhibitor of P-glycoprotein (P-gp) transport activities.18
Thus, caution is warranted when simultaneously prescribing cabozantinib with other medications. Of note, even though the solubility, and thus absorption, of cabozantinib is dependent on pH, the concomitant use of proton pump inhibitors (PPIs) is tolerated. Indeed, no difference in efficacy outcomes or toxicity profile has been found, although these agents have been shown to reduce the AUC for cabozantinib by ≤20%.16,60,61
Toxicity Profile
Cabozantinib, like other VEGFR–TKIs, is associated with a large array of side effects, including fatigue, gastrointestinal toxicities (diarrhea, vomiting, and anorexia), hypertension, hand–foot syndrome, coagulation disorders and proteinuria.62 Although reporting criteria may differ between clinical trials, diarrhea often appears to be one of the most frequent and disabling adverse events. It was reported in 75% and 72% of the patients treated with cabozantinib in the METEOR and CABOSUN trials, respectively, with 13% and 10% of patients classed having diarrhea of grade ≥3.13,28 General measures such as dietary recommendations and symptomatic treatments (ie loperamide) may help to relieve symptoms, although the effectiveness of these measures has never been studied in patients being treated with cabozantinib, and dose reductions are sometimes necessary.63 Fatigue is another major side effect of cabozantinib, reported with a frequency of 59% in the METEOR trial and 86% in the CABOSUN trial (grade 3 in 11% and 6% of patients, respectively).13,28 As the origin of fatigue is often multifactorial, its management remains challenging and is dominated by nonpharmacological interventions, such as physical activity when feasible, or by the identification and treatment of differential diagnoses (for instance depression, testosterone deficiency or hypothyroidism). As with diarrhea, dose reduction may be required in patients with fatigue. Hypertension has been reported in 37% of patients treated with cabozantinib in the METEOR trial (grade 3 or 4 in 15% of patients) and in 81% of those in the CABOSUN trial (grade 3 or 4 in 28% of patients).13,28 After appropriate monitoring and diagnosis, the management of this adverse event should not differ from that recommended by standard hypertension guidelines, although the use of angiotensin receptor blockers may be of interest as they have been shown to have the potential to inhibit cancer cell growth and migration.64
Thus, even with optimal nonpharmacological and pharmacological support, dose holds and dose reductions are frequently needed: overall, they were reported in 62% of patients treated with 60mg cabozantinib in the METEOR trial and in 58% of those in the CABOSUN trial.13,28 In addition, although the starting dose of cabozantinib is reduced to 40 mg per day when it is used in combination with nivolumab, at least one dose reduction was necessary in 56.3% of the patients in the Checkmate-9ER trial.35
Due to the long half-life of cabozantinib, the median dose hold has been estimated to be between 7 and 9 days when used in monotherapy.65 Dose reductions should carried out in steps of 20 mg/day, leading to a daily dosage of 40 mg after the first reduction and 20 mg after the second reduction when cabozantinib is used in monotherapy, or to a daily dosage of 20 mg after the first reduction when cabozantinib is used in combination with nivolumab.66 Cabozantinib may sometimes be restarted at the same dosage, depending on factors, such as the nature of the adverse event, its severity, or the presence of a potentially reversible trigger.
These findings justify the need for caution with the use of cabozantinib and other VEGFR–TKIs in some patients, taking into consideration comorbidities or the disease localization. Evidence suggests that peculiar attention should be paid to weight loss as the occurrence of this adverse event was probably underestimated in clinical trials: weight loss of grade 3 or 4 was reported in 3% and 4% of patients in the METEOR and CABOSUN trials,13,27 respectively; compared to in 11% of patients in real-life conditions.67 This adverse event also appears to occur more often after prolonged exposure to cabozantinib, with the cumulative incidence of grade 2 and 3 weight loss being reported to increase to 44.1% and 13.6%, respectively, in patients who responded to cabozantinib after more than 6 months. The median time to grade 2 weight loss was 11.9 months.
Comorbidities
Some of the side effects associated with cabozantinib and other VEGFR–TKIs, can, in rare cases, be potentially life threatening. Thus, the presence of several comorbidities may necessitate extreme caution with or avoidance of the use of antiangiogenic agents. This is most notably the case for cardiovascular disorders, such as severe hypertension and coagulation disorders.
Age
Although there is no recommendation for dose adjustments in elderly patients, the tolerability of cabozantinib may differ in this population. Adverse events were reported to occur faster and more often in elderly patients (n=27) than in younger patients in the METEOR trial, with median times for grade 3 adverse events of 3.4 weeks versus 16.1 weeks, respectively.68 Moreover, dose reductions of cabozantinib were needed in 85% of elderly patients, but in only 61% of younger patients. Regarding efficacy, no differences were observed between age groups: PFS was 7.4 months for patients under 65 years of age versus 8.1 months for patients between the ages of 65 and 74, and 9.4 months for patients aged 75 years or above.67 In the CABOREAL retrospective study, the median OS reported was 16.2 months for patients between 65 and 75 years of age and 13.3 months for those over 75 years of age, with a median follow‑up of 13.3 months.69
Other Comorbidities or Previous Treatments
The use of cabozantinib has to take into account the balance between the efficacy of the drug and clinical considerationsin particular, the risk of digestive disorders such as perforation or fistula of the aerodigestive system. Thus, the use of VEGFR–TKIs, and especially that of cabozantinib, may be problematic in case of serious digestive complications, including metastasis of the digestive tract or peritoneal carcinomatosis, or a history of perforation or previous external radiation.70
Biomarker Analyses
Despite many studies, there are currently no predictive biomarkers to guide the selection of ICI or TKI combination therapies, or the type of TKI. However, the impact of tumor levels of PD-L1 expression on treatment efficacy was evaluated in the Checkmate-9ER trial through a planned subanalysis of stratified data.35 All patients, regardless of the level of expression of PD-L1, were found to benefit more from cabozantinib–nivolumab combination therapy than from sunitinib treatment. However, the PD-L1 biomarker may help to guide the choice between prescribing an ICI–ICI or an ICI–TKI combination: the results of a meta-analysis revealed that a lack of PD-L1 expression (levels below 1%), may indicate that selecting a TKI-ICI combination, rather than an ICI–ICI combination (such as nivolumab-ipilimumab) would provide optimal treatment, with no differences according to PD-L1 status being observed between the potential ICI-TKI combinations.71 Molecular signatures, such as the angiogenic signature validated in the IMmotion 150 trial, may be more useful for selecting TKIs.72 This genetic signature has already been shown to be indicative of outcomes of bevacizumab combination therapies, and is of interest for the evaluation of predicted outcomes with cabozantinib treatment. In addition, the results of the biomarker-driven BIONNIK trial indicated that evaluating angiogenic or immune response-driven signatures to randomized treatments may be interesting for guiding the selection between VEGFR–TKI combinations or VEGFR–TKI treatment alone, and ICI–ICI combinations.73 The results of this study have been validated with the first-generation VEGFR–TKI, sunitinib. Further studies, involving cabozantinib, are needed to confirm the potential usefulness of these signatures to guide the therapeutic selection of this drug.
Studies of the predictive efficacy of the range of VEGFR–TKI family members through analysis of their predominant impact of angiogenesis, has raised questions about the impact of cabozantinib on other targets. In a recent study, METEOR study tumor samples were tested for a range of protein markers of angiogenesis, including an analysis of microvascular density (MVD) by immunohistochemistry.74 As expected, a high MVD was associated with improved outcomes in MRCC, but was not predictive of the efficacy of cabozantinib. Nevertheless, the high efficacy of cabozantinib in low-grade angiogenic tumors allows speculation that antitumor activity is not exclusively mediated by VEGFR inhibition.
In this context, although the expression of tyrosine kinase receptors has been associated with worse outcomes in patients with MRCCs treated with sunitinib,75 the expression of these receptors was not confirmed to be predictive of the potential efficacy of cabozantinib treatment for MRCC during the METEOR trial. Indeed, a low plasma AXL level was only found to be predictive of a relative improvement in PFS for cabozantinib, and was not significantly predictive of the benefit of treatment with cabozantinib.76
Perspectives
Over the past few years, the therapeutic landscape of MRCC has undergone major changes. After a decade dominated by a monoantiangiogenic therapy (most notably with sunitinib), first-line systemic treatments are now being used in combination with other treatments and always involve at least one ICI. As a result of this major shift in therapeutic strategy, cabozantinib may play a major in the treatment of MRCC, with the results of the pivotal CHECKMATE-9ER trial assessing in the use of cabozantinib in combination with nivolumab supporting the need to consider cabozantinib combination therapy as one of the new standards of care in the first-line treatment of advanced RCC or MRCC. Indeed, this combination therapy has been approved by the Food and Drug Administration (FDA) and the European Medicines Agency (EMA).
The range of combination treatments may be expanded even further, depending on the results of the ongoing COSMIC-313 trial focusing on the potential benefits of a “triplet” association as a first-line therapy (NCT03937219). In this study, cabozantinib was added in the experimental arm in combination with two checkpoint inhibitors: nivolumab and ipilimumab. If the outcomes for primary endpoints are favorable, this new triplet association could become a new standard of care. Nevertheless, the long-term strategy for MRCC is likely to become a matter of concern as, to date, few data are available about the best treatment sequences to use in first- and second-line settings.
Although combination treatments are the new standard of care in first-line settings, the use of cabozantinib monotherapy should still be considered in second-line settings in well-defined subgroups of patients. Most notably, patients with bone or brain metastasis of RCC may benefit from the tropism of cabozantinib in these localizations. Similarly, patients experiencing highly symptomatic disease may also benefit from cabozantinib treatment. However, other second-line treatments for MRCC are currently being investigated, including the association of belzutifan and lenvatinib, which is currently being evaluated in comparison with cabozantinib in an ongoing two-arm phase III trial (NCT04586231).
In addition, the use of combinations of ICIs and VEGFR–TKIs in second-line settings has also been evaluated. The combination of cabozantinib with atezolizumab has shown encouraging clinical activity in a phase Ib study,77 and is now being evaluated as a second- or third-line treatment in an ongoing phase III trial.
Overall, irrespective the line of treatment, there is a need for additional data to confirm the benefits of cabozantinib in the treatment of bone and brain metastases, particularly as patients are now living longer and these forms of disease evolution over time are being encountered more frequently.
In non-clear cell RCC, additional data on the efficacy of cabozantinib are pending (NCT 03541902, NCT 03635892, NCT 04413123, NCT 04644432, and NCT 03685448) and specific clinical randomized trials according tumor subtype will be of great interest.
The landscape of adjuvant therapy in intermediate- or high-risk primary clear cell tumors is also evolving, with the approval of ICI for these indications. Ongoing trials are exploring combinations of ICIs but none of the trials initiated so far are exploring combinations including cabozantinib or other VEGFR–TKIs.
However, the use of the standard dose of cabozantinib over 12 weeks has been evaluated in a neo-adjuvant setting in 16 patients with locally advanced non-metastatic clear cell RCC. Although all patients had tumor shrinkage, only five patients (29.4%) had a tumor response.78 This is in line with previous reports investigating other VEGFR–TKIs in neo-adjuvant settings. However, it should be noted that neo-adjuvant treatment of RCC is not a standard of care, as it not considered as an option. Indeed, the ability to perform a nephrectomy is based on the urologist’s experience, and neo-adjuvant treatment is not usually considered in expert centers as treatment for decreasing tumor size.
As regards the safety concerns of cabozantinib treatment, efforts are needed to understand and minimize the risk of significant weight loss after prolonged exposure. This information could be of great interest to avoid any interruptions in administration of this effective treatment.
Conclusion
Cabozantinib is one of the leading second-generation VEGFR–TKIs for the treatment of MRCC. It targets a range of TK receptors in addition to VEGFR, such as c-MET and AXL, but the contribution of this additional activity to treatment efficacy has not been fully explored. More recently, combined cabozantinib–nivolumab therapy became one of the three standard of care treatments for MRCC in first-line settings. Further studies are essential to assess the benefits of cabozantinib compared to other treatments in patients with bone or brain metastases, and in those with non-clear cell RCC histology and/or sarcomatoid features.
Disclosure
Professor Alain Ravaud reports grants, personal fees, from Pfizer and Ipsen, personal fees from MSD, Merck GA, BMS, and Eisai, during the conduct of the study. Dr Marine Gross-Goupil reports non-financial support from Ipsen, MSD, Pfizer, and Roche, outside the submitted work; also a member of consulting board for BMS, Ipsen, MSD. The authors report no other conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394–424. doi:10.3322/caac.21492
2. Hsieh JJ, Purdue MP, Signoretti S, et al. Renal cell carcinoma. Nat Rev Dis Primer. 2017;3(1):17009. doi:10.1038/nrdp.2017.9
3. Yakes FM, Chen J, Tan J, et al. Cabozantinib (XL184), a novel MET and VEGFR2 inhibitor, simultaneously suppresses metastasis, angiogenesis, and tumor growth. Mol Cancer Ther. 2011;10(12):2298–2308. doi:10.1158/1535-7163.MCT-11-0264
4. Tímár J, Döme B. Antiangiogenic drugs and tyrosine kinases. Anticancer Agents Med Chem. 2008;8(5):462–469. doi:10.2174/187152008784533035
5. Dj H, Lm E. Role of the vascular endothelial growth factor pathway in tumor growth and angiogenesis. J Clin Oncol off J Am Soc Clin Oncol. 2005;23:5. doi:10.1200/JCO.2005.06.081
6. Ravaud A, Digue L, Trufflandier N, Smith D. VEGFR TKI “resistance” or transient clinical insensitivity to VEGFR TKI in metastatic renal cell carcinoma. Ann Oncol off J Eur Soc Med Oncol. 2010;21(2):431–432. doi:10.1093/annonc/mdp548
7. Ravaud A, Gross-Goupil M. Overcoming resistance to tyrosine kinase inhibitors in renal cell carcinoma. Cancer Treat Rev. 2012;38(8):996–1003. doi:10.1016/j.ctrv.2012.01.003
8. Awad MM, Oxnard GR, Jackman DM, et al. MET Exon 14 mutations in non-small-cell lung cancer are associated with advanced age and stage-dependent MET genomic amplification and c-met overexpression. J Clin Oncol off J Am Soc Clin Oncol. 2016;34(7):721–730. doi:10.1200/JCO.2015.63.4600
9. Shojaei F, Lee JH, Simmons BH, et al. HGF/c-Met acts as an alternative angiogenic pathway in sunitinib-resistant tumors. Cancer Res. 2010;70(24):10090–10100. doi:10.1158/0008-5472.CAN-10-0489
10. Lee C, Whang YM, Campbell P, et al. Dual targeting c-met and VEGFR2 in osteoblasts suppresses growth and osteolysis of prostate cancer bone metastasis. Cancer Lett. 2018;414:205–213. doi:10.1016/j.canlet.2017.11.016
11. Smith DC, Smith MR, Sweeney C, et al. Cabozantinib in patients with advanced prostate cancer: results of a phase II randomized discontinuation trial. J Clin Oncol off J Am Soc Clin Oncol. 2013;31(4):412–419. doi:10.1200/JCO.2012.45.0494
12. Smith MR, Sweeney CJ, Corn PG, et al. Cabozantinib in chemotherapy-pretreated metastatic castration-resistant prostate cancer: results of a phase II nonrandomized expansion study. J Clin Oncol off J Am Soc Clin Oncol. 2014;32(30):3391–3399. doi:10.1200/JCO.2013.54.5954
13. Choueiri TK, Escudier B, Powles T, et al. Cabozantinib versus everolimus in advanced renal cell carcinoma (METEOR): final results from a randomised, open-label, Phase 3 trial. Lancet Oncol. 2016;17(7):917–927. doi:10.1016/S1470-2045(16)30107-3
14. Nguyen L, Benrimoh N, Xie Y, Offman E, Lacy S. Pharmacokinetics of cabozantinib tablet and capsule formulations in healthy adults. Anticancer Drugs. 2016;27(7):669–678. doi:10.1097/CAD.0000000000000366
15. Lacy SA, Miles DR, Nguyen LT. Clinical Pharmacokinetics and Pharmacodynamics of Cabozantinib. Clin Pharmacokinet. 2017;56(5):477–491. doi:10.1007/s40262-016-0461-9
16. Nguyen L, Holland J, Mamelok R, et al. Evaluation of the effect of food and gastric pH on the single-dose pharmacokinetics of cabozantinib in healthy adult subjects. J Clin Pharmacol. 2015;55(11):1293–1302. doi:10.1002/jcph.526
17. Nguyen L, Holland J, Miles D, et al. Pharmacokinetic (PK) drug interaction studies of cabozantinib: effect of CYP3A inducer rifampin and inhibitor ketoconazole on cabozantinib plasma PK and effect of cabozantinib on CYP2C8 probe substrate rosiglitazone plasma PK. J Clin Pharmacol. 2015;55(9):1012–1023. doi:10.1002/jcph.510
18. Cabometyx-epar-product-information.pdf. Available from: https://www.ema.europa.eu/en/documents/product-information/cabometyx-epar-product-information_en.pdf.
19. Nguyen L, Holland J, Ramies D, et al. Effect of renal and hepatic impairment on the pharmacokinetics of cabozantinib. J Clin Pharmacol. 2016;56(9):1130–1140. doi:10.1002/jcph.714
20. Lacy S, Yang B, Nielsen J, Miles D, Nguyen L, Hutmacher M. A population pharmacokinetic model of cabozantinib in healthy volunteers and patients with various cancer types. Cancer Chemother Pharmacol. 2018;81(6):1071–1082. doi:10.1007/s00280-018-3581-0
21. Lacy S, Nielsen J, Yang B, Miles D, Nguyen L, Hutmacher M. Population exposure-response analysis of cabozantinib efficacy and safety endpoints in patients with renal cell carcinoma. Cancer Chemother Pharmacol. 2018;81(6):1061–1070. doi:10.1007/s00280-018-3579-7
22. Krens SD, van Erp NP, Groenland SL, et al. Exposure-response analyses of cabozantinib in patients with metastatic renal cell cancer. BMC Cancer. 2022;22(1):228. doi:10.1186/s12885-022-09338-1
23. Albiges L, Fléchon A, Chevreau C, et al. Real-world evidence of cabozantinib in patients with metastatic renal cell carcinoma: results from the CABOREAL Early Access Program. Eur J Cancer Oxf Engl. 2021;142:102–111. doi:10.1016/j.ejca.2020.09.030
24. Choueiri TK, Pal SK, McDermott DF, et al. A phase I study of cabozantinib (XL184) in patients with renal cell cancer. Ann Oncol off J Eur Soc Med Oncol. 2014;25(8):1603–1608. doi:10.1093/annonc/mdu184
25. Choueiri TK, Escudier B, Powles T, et al. Cabozantinib versus everolimus in advanced renal-cell carcinoma. N Engl J Med. 2015;373(19):1814–1823. doi:10.1056/NEJMoa1510016
26. Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol off J Eur Soc Med Oncol. 2016;27(suppl 5):v58–v68. doi:10.1093/annonc/mdw328
27. Heng DYC, Xie W, Regan MM, et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: results from a large, multicenter study. J Clin Oncol off J Am Soc Clin Oncol. 2009;27(34):5794–5799. doi:10.1200/JCO.2008.21.4809
28. Choueiri TK, Halabi S, Sanford BL, et al. Cabozantinib versus sunitinib as initial targeted therapy for patients with metastatic renal cell carcinoma of poor or intermediate risk: the alliance A031203 CABOSUN trial. J Clin Oncol off J Am Soc Clin Oncol. 2017;35(6):591–597. doi:10.1200/JCO.2016.70.7398
29. Choueiri TK, Hessel C, Halabi S, et al. Cabozantinib versus sunitinib as initial therapy for metastatic renal cell carcinoma of intermediate or poor risk (Alliance A031203 CABOSUN randomised trial): progression-free survival by independent review and overall survival update. Eur J Cancer Oxf Engl. 2018;94:115–125. doi:10.1016/j.ejca.2018.02.012
30. George DJ, Hessel C, Halabi S, et al. Cabozantinib versus sunitinib for untreated patients with advanced renal cell carcinoma of intermediate or poor risk: subgroup analysis of the Alliance A031203 CABOSUN trial. Oncologist. 2019;24(11):1497–1501. doi:10.1634/theoncologist.2019-0316
31. Escudier B, Porta C, Schmidinger M, et al. Renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up†. Ann Oncol off J Eur Soc Med Oncol. 2019;30(5):706–720. doi:10.1093/annonc/mdz056
32. Motzer RJ, Tannir NM, McDermott DF, et al. Nivolumab plus ipilimumab versus sunitinib in advanced renal-cell carcinoma. N Engl J Med. 2018;378(14):1277–1290. doi:10.1056/NEJMoa1712126
33. Motzer RJ, Penkov K, Haanen J, et al. Avelumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019;380(12):1103–1115. doi:10.1056/NEJMoa1816047
34. Rini BI, Plimack ER, Stus V, et al. Pembrolizumab plus axitinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2019;380(12):1116–1127. doi:10.1056/NEJMoa1816714
35. Choueiri TK, Powles T, Burotto M, et al. Nivolumab plus cabozantinib versus sunitinib for advanced renal-cell carcinoma. N Engl J Med. 2021;384(9):829–841. doi:10.1056/NEJMoa2026982
36. Powles T, Choueiri TK, Burotto M, et al. Final overall survival analysis and organ-specific target lesion assessments with two-year follow-up in CheckMate 9ER: nivolumab plus cabozantinib versus sunitinib for patients with advanced renal cell carcinoma. J Clin Oncol. 2022;40(6_suppl):350. doi:10.1200/JCO.2022.40.6_suppl.350
37. Motzer R, Alekseev B, Rha SY, et al. CLEAR trial investigators. lenvatinib plus pembrolizumab or everolimus for advanced renal cell carcinoma. N Engl J Med. 2021;384(14):1289–1300. PMID: 33616314. doi:10.1056/NEJMoa2035716
38. Powles T; ESMO Guidelines Committee. Electronic address: [email protected]. Recent eUpdate to the ESMO clinical practice guidelines on renal cell carcinoma on cabozantinib and nivolumab for first-line clear cell renal cancer: renal cell carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol off J Eur Soc Med Oncol. 2021;32(3):422–423. doi:10.1016/j.annonc.2020.11.016
39. Kwilas AR, Ardiani A, Donahue RN, Aftab DT, Hodge JW. Dual effects of a targeted small-molecule inhibitor (cabozantinib) on immune-mediated killing of tumor cells and immune tumor microenvironment permissiveness when combined with a cancer vaccine. J Transl Med. 2014;12(1):294. doi:10.1186/s12967-014-0294-y
40. Patnaik A, Swanson KD, Csizmadia E, et al. Cabozantinib eradicates advanced murine prostate cancer by activating antitumor innate immunity. Cancer Discov. 2017;7(7):750–765. doi:10.1158/2159-8290.CD-16-0778
41. Akalu YT, Rothlin CV, Ghosh S. TAM receptor tyrosine kinases as emerging targets of innate immune checkpoint blockade for cancer therapy. Immunol Rev. 2017;276(1):165–177. doi:10.1111/imr.12522
42. Ocaña-Guzman R, Vázquez-Bolaños L, Sada-Ovalle I. Receptors that inhibit macrophage activation: mechanisms and signals of regulation and tolerance. J Immunol Res. 2018;2018:8695157. doi:10.1155/2018/8695157
43. Yang J, Yan J, Liu B. Targeting VEGF/VEGFR to modulate antitumor immunity. Front Immunol. 2018;9:978. doi:10.3389/fimmu.2018.00978
44. Vano YA, Ladoire S, Elaidi R, et al. First-line treatment of metastatic clear cell renal cell carcinoma: what are the most appropriate combination therapies? Cancers. 2021;13(21):5548. doi:10.3390/cancers13215548
45. Iacovelli R, Cartenì G, Sternberg CN, et al. Clinical outcomes in patients receiving three lines of targeted therapy for metastatic renal cell carcinoma: results from a large patient cohort. Eur J Cancer Oxf Engl. 2013;49(9):2134–2142. doi:10.1016/j.ejca.2013.02.032
46. McGregor BA, Lalani AKA, Xie W, et al. Activity of cabozantinib after immune checkpoint blockade in metastatic clear-cell renal cell carcinoma. Eur J Cancer Oxf Engl. 2020;135:203–210. doi:10.1016/j.ejca.2020.05.009
47. Auvray M, Auclin E, Barthelemy P, et al. Second-line targeted therapies after nivolumab-ipilimumab failure in metastatic renal cell carcinoma. Eur J Cancer Oxf Engl. 2019;108:33–40. doi:10.1016/j.ejca.2018.11.031
48. Barata PC, De Liano AG, Mendiratta P, et al. The efficacy of VEGFR TKI therapy after progression on immune combination therapy in metastatic renal cell carcinoma. Br J Cancer. 2018;119(2):160–163. doi:10.1038/s41416-018-0104-z
49. Navani V, Wells C, Boyne DJ, et al. CABOSEQ: the efficacy of cabozantinib post up-front immuno-oncology combinations in patients with advanced renal cell carcinoma: results from the International Metastatic Renal Cell Carcinoma Database Consortium (IMDC). J Clin Oncol. 2022;40(6_suppl):318. doi:10.1200/JCO.2022.40.6_suppl.318
50. Albiges L, Schmidinger M, Taguieva-Pioger N, Perol D, Grünwald V, Guemas E. CaboPoint: a Phase II study of cabozantinib as second-line treatment in patients with metastatic renal cell carcinoma. Future Oncol Lond Engl. 2021. doi:10.2217/fon-2021-1006
51. Stern PH, Alvares K. Antitumor agent cabozantinib decreases RANKL expression in osteoblastic cells and inhibits osteoclastogenesis and PTHrP-stimulated bone resorption. J Cell Biochem. 2014;115(11):2033–2038. doi:10.1002/jcb.24879
52. Haider MT, Hunter KD, Robinson SP, et al. Rapid modification of the bone microenvironment following short-term treatment with Cabozantinib in vivo. Bone. 2015;81:581–592. doi:10.1016/j.bone.2015.08.003
53. Bersanelli M, Buti S, Ghidini A, Tiseo M, Petrelli F. A metanalysis on cabozantinib and bone metastases: true story or commercial gimmick? Anticancer Drugs. 2020;31(3):211–215. doi:10.1097/CAD.0000000000000883
54. Peverelli G, Raimondi A, Ratta R, et al. Cabozantinib in renal cell carcinoma with brain metastases: safety and efficacy in a real-world population. Clin Genitourin Cancer. 2019;17(4):291–298. doi:10.1016/j.clgc.2019.05.002
55. Hirsch L, Martinez Chanza N, Farah S, et al. Clinical activity and safety of cabozantinib for brain metastases in patients with renal cell carcinoma. JAMA Oncol. 2021;7(12):1815–1823. doi:10.1001/jamaoncol.2021.4544
56. Martínez Chanzá N, Xie W, Asim Bilen M, et al. Cabozantinib in advanced non-clear-cell renal cell carcinoma: a multicentre, retrospective, cohort study. Lancet Oncol. 2019;20(4):581–590. doi:10.1016/S1470-2045(18
57. Fléchon A, Chevreau CM, Topart D, et al. 732P Cabozantinib in non-clear cell metastatic renal cell carcinoma and sarcomatoid renal cell carcinoma: real-world data from the CABOREAL study. Ann Oncol. 2020;31:S572–S573. doi:10.1016/j.annonc.2020.08.804
58. Pal SK, Tangen C, Thompson IM, et al. A comparison of sunitinib with cabozantinib, crizotinib, and savolitinib for treatment of advanced papillary renal cell carcinoma: a randomised, open-label, Phase 2 trial. Lancet Lond Engl. 2021;397(10275):695–703. doi:10.1016/S0140-6736(21)00152-5
59. Lee CH, Voss MH, Carlo MI, et al. Nivolumab plus cabozantinib in patients with non-clear cell renal cell carcinoma: results of a phase 2 trial. J Clin Oncol. 2021;39(15_suppl):4509. doi:10.1200/JCO.2021.39.15_suppl.4509
60. Fogli S, Porta C, Del Re M, et al. Optimizing treatment of renal cell carcinoma with VEGFR-TKIs: a comparison of clinical pharmacology and drug-drug interactions of anti-angiogenic drugs. Cancer Treat Rev. 2020;84:101966. doi:10.1016/j.ctrv.2020.101966
61. Rassy E, Cerbone L, Auclin E, et al. The Effect of Concomitant Proton Pump Inhibitor and Cabozantinib on the Outcomes of Patients with Metastatic Renal Cell Carcinoma. Oncologist. 2021;26(5):389–396. doi:10.1002/onco.13711
62. Roodhart JM, Langenberg MH, Witteveen E, Voest EE. The molecular basis of class side effects due to treatment with inhibitors of the VEGF/VEGFR pathway. Curr Clin Pharmacol. 2008;3(2):132–143. doi:10.2174/157488408784293705
63. Schmidinger M, Danesi R. Management of adverse events associated with cabozantinib therapy in renal cell carcinoma. Oncologist. 2018;23(3):306–315. doi:10.1634/theoncologist.2017-0335
64. Wasa J, Sugiura H, Kozawa E, Kohyama K, Yamada K, Taguchi O. The tumor suppressive effect of angiotensin II type 1 receptor antagonist in a murine osteosarcoma model. Anticancer Res. 2011;31(1):123–127.
65. McGregor B, Mortazavi A, Cordes L, Salabao C, Vandlik S, Apolo AB. Management of adverse events associated with cabozantinib plus nivolumab in renal cell carcinoma: a review. Cancer Treat Rev. 2022;103:102333. doi:10.1016/j.ctrv.2021.102333
66. DosingandAdministrationGuide.pdf. Available from: https://www.cabometyxhcp.com/sites/default/files/2021-03/DosingandAdministrationGuide.pdf.
67. Colomba E, Alves Costa Silva C, Le Teuff G, et al. 965P - Weight loss is an underestimated adverse event with cabozantinib in patients with metastastic renal cell carcinoma (mRCC). Ann Oncol. 2019;30:v390–v391. doi:10.1093/annonc/mdz249.061
68. Donskov F, Motzer RJ, Voog E, et al. Outcomes based on age in the phase III METEOR trial of cabozantinib versus everolimus in patients with advanced renal cell carcinoma. Eur J Cancer Oxf Engl. 2020;126:1–10. doi:10.1016/j.ejca.2019.10.032
69. Gross-Goupil M, Fléchon A, Mourey L, et al. 722P Cabozantinib in elderly patients: results from a subanalysis of the CABOREAL study. Ann Oncol. 2020;31:S566–S567. doi:10.1016/j.annonc.2020.08.794
70. Blevins DP, Dadu R, Hu M, et al. Aerodigestive fistula formation as a rare side effect of antiangiogenic tyrosine kinase inhibitor therapy for thyroid cancer. Thyroid off J Am Thyroid Assoc. 2014;24(5):918–922. doi:10.1089/thy.2012.0598
71. Quhal F, Mori K, Bruchbacher A, et al. First-line immunotherapy-based combinations for metastatic renal cell carcinoma: a systematic review and network meta-analysis. Eur Urol Oncol. 2021;4(5):755–765. doi:10.1016/j.euo.2021.03.001
72. McDermott DF, Huseni MA, Atkins MB, et al. Clinical activity and molecular correlates of response to atezolizumab alone or in combination with bevacizumab versus sunitinib in renal cell carcinoma. Nat Med. 2018;24(6):749–757. doi:10.1038/s41591-018-0053-3
73. Vano Y, Elaidi RT, Bennamoun M, et al. LBA25 Results from the phase II biomarker driven trial with nivolumab (N) and ipilimumab or VEGFR tyrosine kinase inhibitor (TKI) in naïve metastatic kidney cancer (m-ccRCC) patients (pts): the BIONIKK trial. Ann Oncol. 2020;31:S1157. doi:10.1016/j.annonc.2020.08.2254
74. Denize T, Farah S, Cimadamore A, et al. Biomarkers of angiogenesis and clinical outcomes to cabozantinib and everolimus in patients with metastatic renal cell carcinoma from the phase III METEOR trial. Clin Cancer Res off J Am Assoc Cancer Res. 2022;28(4):748–755. doi:10.1158/1078-0432.CCR-21-3088
75. Zucca LE, Morini Matushita MA, da Silva Oliveira RJ, et al. Expression of tyrosine kinase receptor AXL is associated with worse outcome of metastatic renal cell carcinomas treated with sunitinib. Urol Oncol. 2018;36(1):
76. Powles T, Choueiri TK, Motzer RJ, et al. Outcomes based on plasma biomarkers in METEOR, a randomized phase 3 trial of cabozantinib vs everolimus in advanced renal cell carcinoma. BMC Cancer. 2021;21(1):904. doi:10.1186/s12885-021-08630-w
77. Pal SK, McGregor B, Suárez C, et al. Cabozantinib in combination with atezolizumab for advanced renal cell carcinoma: results from the COSMIC-021 study. J Clin Oncol off J Am Soc Clin Oncol. 2021;39(33):3725–3736. doi:10.1200/JCO.21.00939
78. Bilen MA, Liu Y, Nazha B, et al. Phase 2 study of neoadjuvant cabozantinib in patients with locally advanced non-metastatic clear cell renal cell carcinoma.. J Clin Oncol. 2022;40(6_suppl):340. doi:10.1200/JCO.2022.40.6_suppl.340
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.