Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
An Analysis of the Risk Factors for Adding-on Phenomena After Posterior Hemivertebral Resection and Pedicle Screw Fixation for the Treatment of Congenital Scoliosis Caused by Hemivertebral Malformation
Authors Bao BX, Yan H, Tang JG, Qiu DJ, Wu YX, Cheng XK
Received 6 December 2021
Accepted for publication 24 March 2022
Published 13 April 2022 Volume 2022:18 Pages 409—419
DOI https://doi.org/10.2147/TCRM.S352793
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor De Yun Wang
Bei-Xi Bao, Hui Yan, Jia-Guang Tang, Dao-Jing Qiu, Yu-Xuan Wu, Xiao-Kang Cheng
Department of Orthopedic Surgery, Beijing Tongren Hospital, Capital Medical University, Beijing, 100730, People’s Republic of China
Correspondence: Jia-Guang Tang, Department of Orthopedic Surgery, Beijing Tongren Hospital, Capital Medical University, No. 1 of Dongjiaominxiang Street, Dongcheng District, Beijing, 100730, People’s Republic of China, Tel/Fax +86 13911003227, Email [email protected]
Objective: To retrospectively analyze the risk factors for adding-on phenomena (AOP) after posterior hemivertebral resection (PHR) and pedicle screw fixation for the treatment of congenital scoliosis (CS) caused by hemivertebral (HV) malformation.
Methods: Patients with CS who underwent surgery and were followed up for more than five years were included in this study. The d general data, such as gender, age, HV segment, Risser sign, and triangular cartilage, postoperative complications, and imaging data at different periods, including the standard anteroposterior and lateral x-rays of the total spine were collected.
Results: In total, 58 patients were included in this study, of which 10 experienced AOP and 48 did not. The results of the single-factor analysis showed that there were statistically significant differences between the patients with AOP and those without in terms of the HV direction, lowest instrumented vertebra (LIV)–upper instrumented vertebra (UIV) (P < 0.05), and postoperative trunk shift (P < 0.05). The results of the logistic regression analysis showed that the HV direction and the postoperative trunk displacement distance were the main risk factors for postoperative AOP. The area under the receiver operating characteristic curve was 0.842 (P < 0.001). The best cut-off value of the adding-on index as an indicator of the occurrence of AOP after surgery was 0.67. When the adding-on index was > 0.67, the incidence of postoperative AOP was 90.0%, and the non-occurrence rate was 22.9%.
Conclusion: PHR and pedicle screw fixation is an effective way to treat HV malformation in CS. The HV direction, LIV–UIV, and postoperative TS are risk factors for AOP in patients with CS treated with PHR and pedicle screw fixation. The adding-on index has a high degree of accuracy for the prediction of the occurrence of AOP after PHR and pedicle screw fixation.
Keywords: congenital scoliosis, hemivertebral resection, adding-on phenomena
Introduction
The most common cause of congenital scoliosis (CS) is hemivertebral (HV) malformation, which is caused by unilateral vertebral defects. There are three main types of scoliosis: CS (most common), congenital kyphosis, and congenital lordosis (least common).1 Aside from some unsegmented or incarcerated hemivertebrae, most hemivertebrae have normal growth plates. Therefore, as a patient grows, the malformation of their spine becomes increasingly serious. As the spine grows, it is difficult to control the progression of CS. Without treatment, 85% of patients will suffer from scoliosis of >41°,2 and non-surgical treatment is not effective. Among CS cases, 75% are of the progressive type, and 5–10% can be treated using braces.3
The purpose of surgical intervention is to correct the abnormal development of the chest and abdominal cavity and control the progression of spine malformation. HV resection is a safe and effective surgical treatment for CS and has achieved good clinical results. Moreover, posterior HV resection is associated with a shorter operation time, less blood loss, and a lower incidence of complications.4 In a multicenter trial, Yaszay et al5 compared three surgical methods: hemiepiphysiodesis or in situ fusion, internal fixation fusion (the hemivertebra is not excised), and hemivertebra resection with internal fixation and fusion. For young patients, the correction effect of the posterior HV resection is better than the other two surgical methods, and it can improve the condition of the malformation, but it has an increased risk of complications over the other two surgical methods, including an increased incidence of neural injury.
The distal adding-on phenomenon (AOP) manifests as the loss of correction after scoliosis, the offset and rotation of the lumbar vertebrae, and wedging changes of the distal fixation of the vertebral discs.6 This phenomenon is most common in adolescent patients with idiopathic scoliosis, but it can also occur after surgery for CS. Chang et al first reported AOP after HV resection. During postoperative follow-up, two patients exhibited a distal AOP, with the progression of scoliosis exceeding 10°, and treatment with a brace was required.7 Avoiding the distal AOP is an important consideration in surgery for scoliosis.
There is controversy surrounding the incidence of and factors that increase the risk of AOP. Due to its high incidence and poor radiological and clinical prognosis, the risk factors and predictive indicators of AOP have been widely studied and evaluated. However, research on the incidence of the distal AOP and its risk factors is based on adolescent idiopathic scoliosis (AIS). At present, there is no research related to risk factors for the AOP after posterior hemivertebral resection (PHR) and pedicle screw fixation. The purpose of this research is to retrospectively analyze these risk factors to minimize the incidence of these complications.
Materials and Methods
This study included patients with CS who underwent PHR and pedicle screw fixation at our spine center from January 2007 to January 2015 and were followed up for more than five years. All surgeries were completed by the corresponding author. Before data collection and analysis, this study was approved by the ethics committee.
Inclusion criteria were as follows: (1) congenital spinal deformity caused by hemivertebra requiring surgical treatment (a curve magnitude >25° and/or with fast progression, including documented progression of a curve of >5° at the six-month follow-up and/or failure of conservative treatment); (2) more than five years of radiographic follow-up after initial surgery; (3) no arthropathy or discrepancy of the lower limbs.
Exclusion criteria were as follows: (1) anterior approach; (2) operated by using hooks as anchors; (3) more than one hemivertebra or combination with other congenital spinal deformity; (4) previous spinal surgery.
Diagnostic criteria for AOP were as follows: the postoperative deterioration of the curve below spinal fusion instrumentation associating; (1) increase in the Cobb angle of the lumbar curve; (2) and/or an increase in the number of vertebrae included in this curve; (3) a deviation of more than 5 mm in the lowest instrumented vertebra (LIV) from the central sacral vertical line; (4) an increase in the narrowing of the first vertebra below instrumentation of more than 5°.6
Data Collection and Statistical Analysis
General data, including gender, age, HV segment, Risser sign (≤3 or >3), and triangular cartilage (open or closed), were collected. Postoperative complications, including the AOP, proximal junctional kyphosis, formation of pseudoarticulation, crankshaft phenomenon, postoperative progression of scoliosis, offset of the internal fixation, wound infection, and injury to the great vessel, were recorded. Doctors analyzed the standard anteroposterior and lateral X-rays of the full-length spine before surgery, after surgery, two years after surgery, and during the last follow-up (≥5 years after surgery).
The orthographic X-ray of the patient’s full-length spine was measured (see Figure 1). The measurement indicators included segmental scoliosis (SeS), total main scoliosis (TmS), trunk shift (TS), and apical vertebral translocation (AVT). Full-length lateral X-rays of the patient’s spine were measured (Figure 2), including segmental kyphosis (SK) and sagittal balance (SB). SeS is the angle formed by the upper endplate of the vertebral body above the hemivertebra and the lower endplate of the vertebral body below the hemivertebra. TmS is the maximum scoliosis angle between the two most inclined vertebrae in the main bend. TS is the vertical distance from the center of the sacrum to the vertical line from the midpoint of the C7 vertebral body. AVT is the vertical distance from the center of the sacrum to the midpoint of the hemivertebra. SK is the angle from the upper endplate of the upper hemivertebra to the lower endplate of the lower hemivertebra. SB is the distance drawn from the perpendicular of C7 to the posterior upper angle of the sacrum. When the C7 plumb line is in front of the posterior upper angle of the sacrum, it is specified as positive (+); upper instrumented vertebra (UIV) and LIV are specified as negative values (−) when the C7 plumb line is located behind the posterior upper corner of the sacrum. LIV–UIV is the number of segments between the upper and lower fixed vertebrae. The upper end vertebra (UEV) and lower end vertebra (LEV) are the vertebral bodies with the largest tilt at the end and end of the structural elbow, respectively. LEV–UEV is the number of vertebral bodies involved in lateral bending. Figure 3 shows a typical case of a nine-year-old girl with congenital scoliosis. The hemivertebra is located in L2. The patient showed AOP at the two-year follow-up. According to the measurements of preoperative and postoperative scoliosis and kyphosis, the correction rate of the main curve and kyphosis were calculated. The correction rate of the main curve is calculated as (preoperative TmS − postoperative TmS) ÷ preoperative TmS × 100 (%). The correction rate of kyphosis is calculated as (preoperative segmental kyphosis [SK] − postoperative SK) ÷ preoperative SK × 100 (%). The apical vertebral translocation before and after the surgery was expressed using ΔAVT.
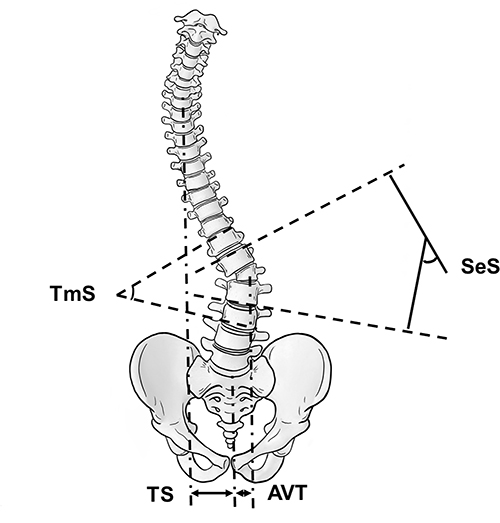 |
Figure 1 Measurement of the coronal index: segmental scoliosis, total main scoliosis, trunk shift, and apical vertebral translocation. |
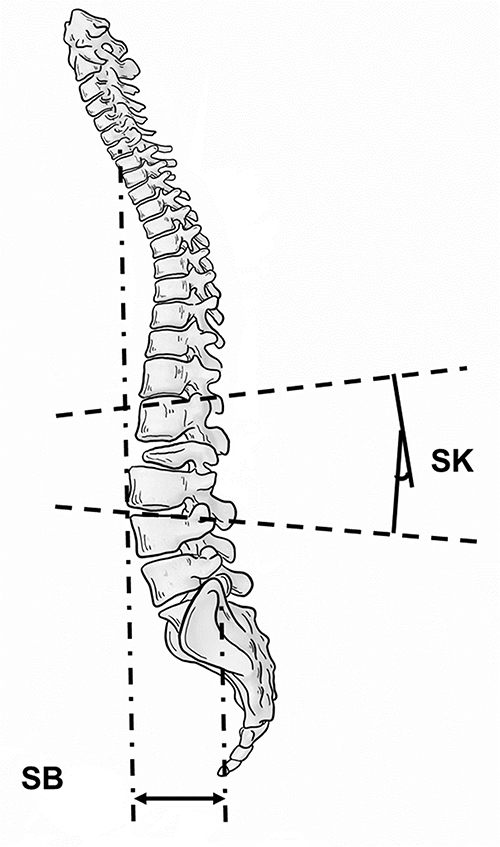 |
Figure 2 Sagittal measurement index: segmental kyphosis and sagittal balance. |
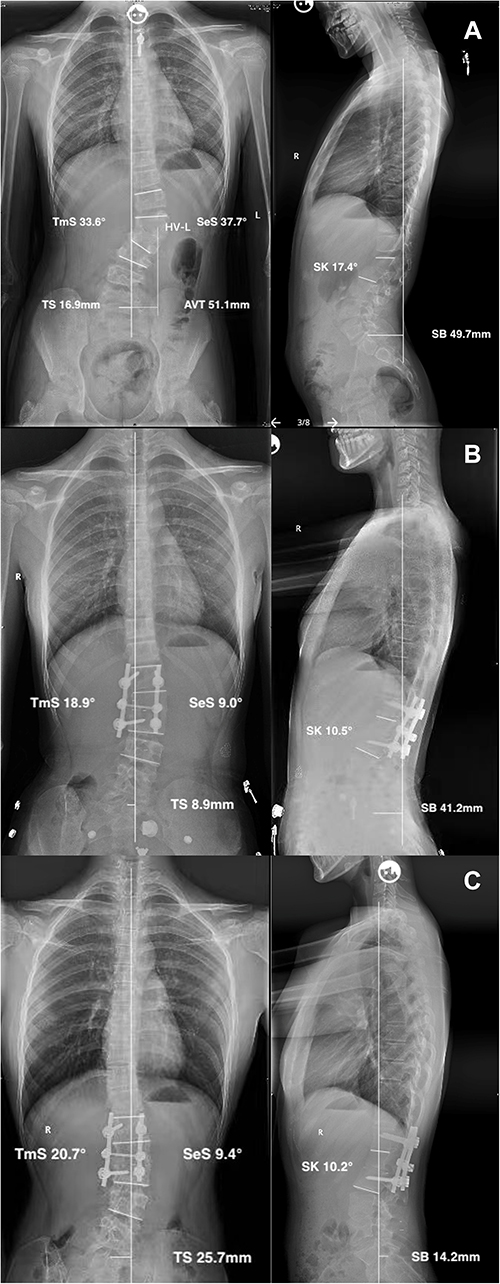 |
Figure 3 A nine-year-old girl with congenital scoliosis is shown. The hemivertebra is located in L2. The standard standing long cassette anterior–posterior (AP) and lateral (L) radiographs were performed preoperatively (A), at the two-year follow-up (B), and at the 10-year follow-up visit (C). The patient showed adding-on phenomena at the two-year follow-up. |
All parameters were obtained twice by two independent surgeons, and the average of the four measurements was calculated. Data analysis was performed using the SPSS 25 software (IBM, USA). Univariate analysis was performed using the χ2, Student’s t-test, or nonparametric test. Multivariate linear analysis was used to determine independent risk factors for AOP. From this, the regression equation was obtained, and the adding-on index was determined. A P value of <0.05 was considered statistically significant.
Results
General Data
A total of 58 patients were included in this study (23 males and 35 females). The mean age of the study cohort was 12.2 years old (range from 3 to 39 years), with a mean follow-up of 68 months (range from 60 to 122 months). The general data and imaging parameters of all patients are shown in Table 1.
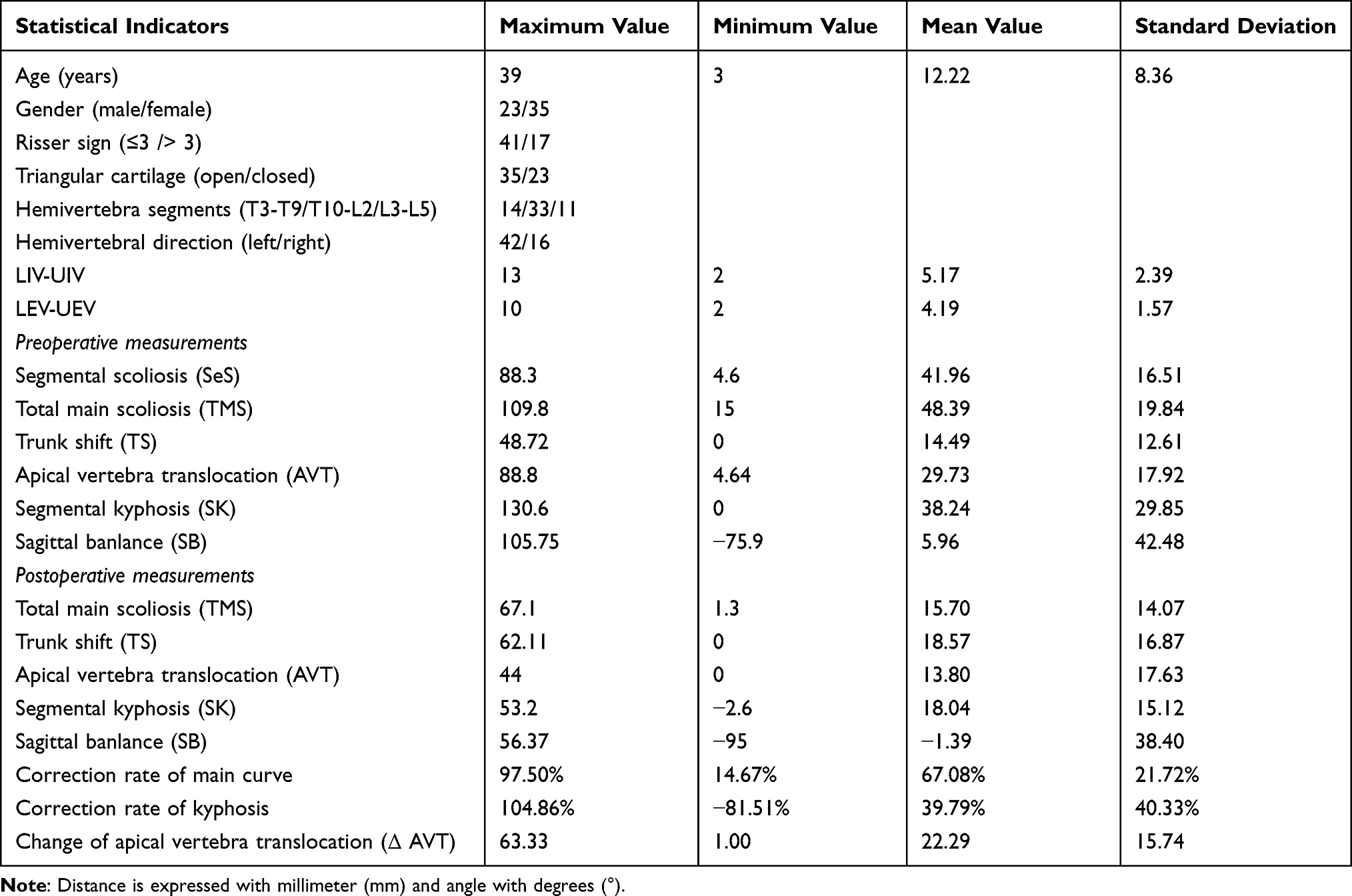 |
Table 1 General Data of Included Patients |
Postoperative Complications
Of the 58 patients, 10 experienced postoperative AOP and six suffered from proximal junctional kyphosis. The intraoperative and postoperative complications are shown in Table 2.
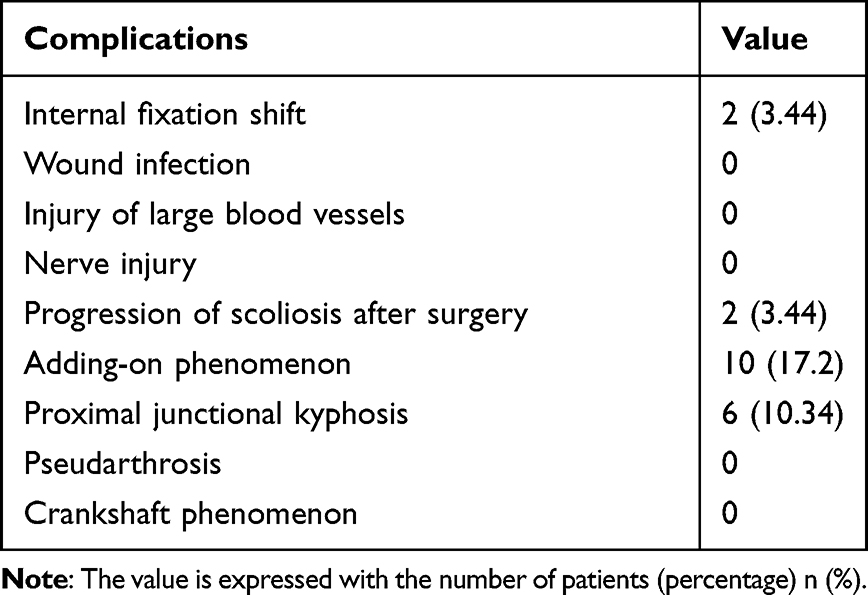 |
Table 2 Intraoperative and Postoperative Complications for Patients |
Univariate Analysis
Of the 58 patients, 10 patients experienced AOP after surgery (add-on group) and 48 had no AOP at the last follow-up (non-add-on group). The results of the univariate analysis showed that the HV direction influenced the incidence of AOP after surgery. The incidence of AOP after surgery for the left hemivertebrae was 9.5% and for the right hemivertebrae was 37.5% (P < 0.05). After surgery, the LIV–UIV was 3.90 ± 1.20 in the add-on group and 5.44 ± 2.28 in the non-add-on group (P < 0.05). The postoperative TS was 28.10 ± 14.53 in the add-on group and 16.59 ± 16.07 in the non-add-on group (P < 0.05).
No statistically significant differences were observed between the add-on and non-add-on groups in terms of age, gender, HV segment, Risser’s sign, triangular cartilage (open or closed), preoperative TS, preoperative and postoperative TmS, AVT, SK, sagittal balance distance, correction rate of the postoperative main curve, correction rate of kyphosis, LEV–UEV, and ΔAVT (P > 0.05; see Table 3).
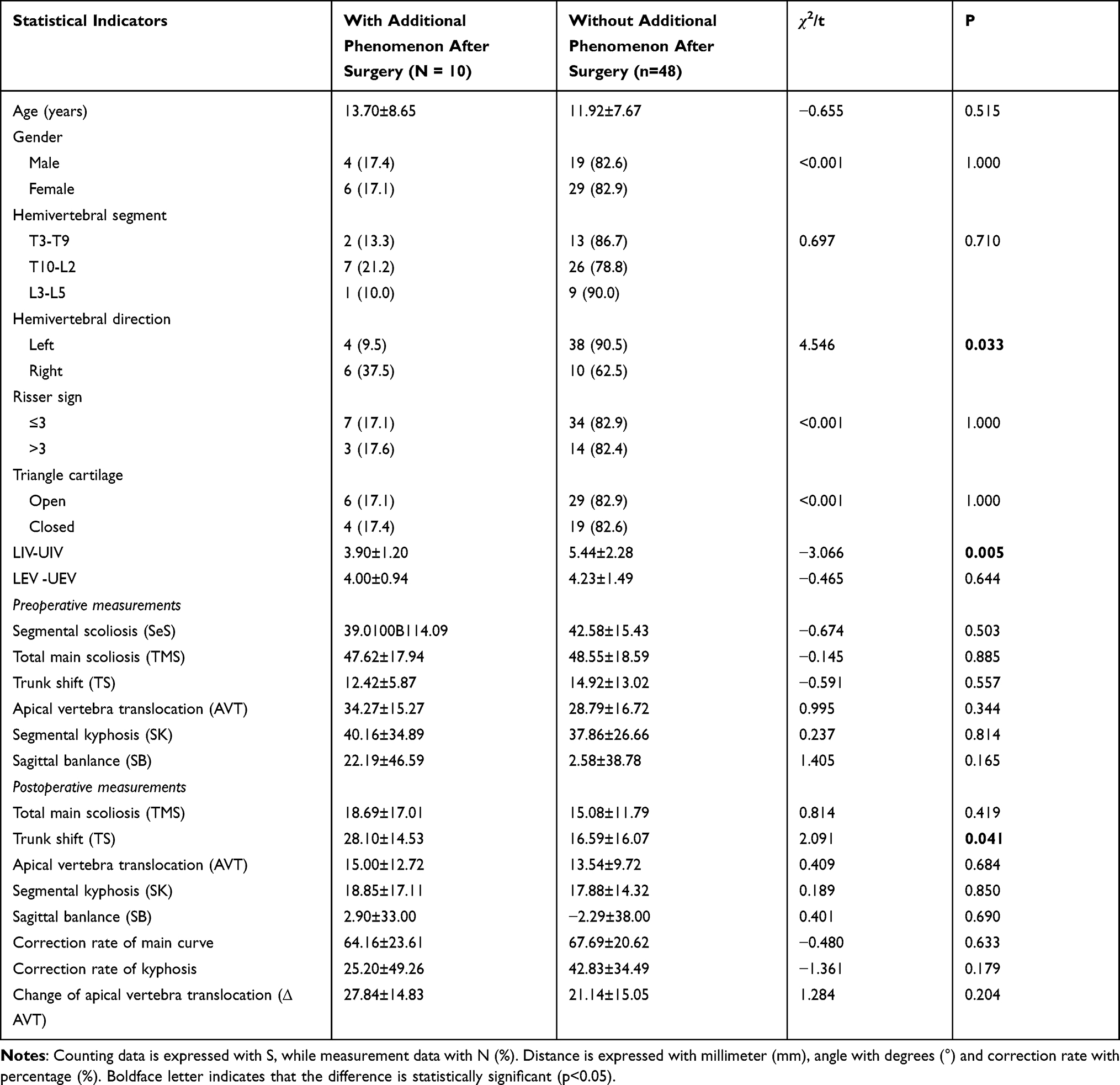 |
Table 3 Comparison of General Data and Imaging Indicators of Patients with and without Additional Phenomena After Surgery |
Logistic Regression Analysis of Risk Factors for Adding-on Phenomena After Surgery
Logistic regression analysis of the above three factors showed that the HV direction (OR: 95% confidence interval (CI): 1.29–40.13; P = 0.025), LIV–UIV (OR: 95% CI: 0.27–0.99; P = 0.045), and the postoperative TS (95% CI: 1.00–1.11; P = 0.039) were the main risk factors for postoperative AOP (see Table 4). According to the regression equation, the adding-on index was defined as −0.61 − 1.97 × the HV direction (R = 1, L = 0) − 0.66 × (LIV–UIV) + 0.05 × postoperative TS.
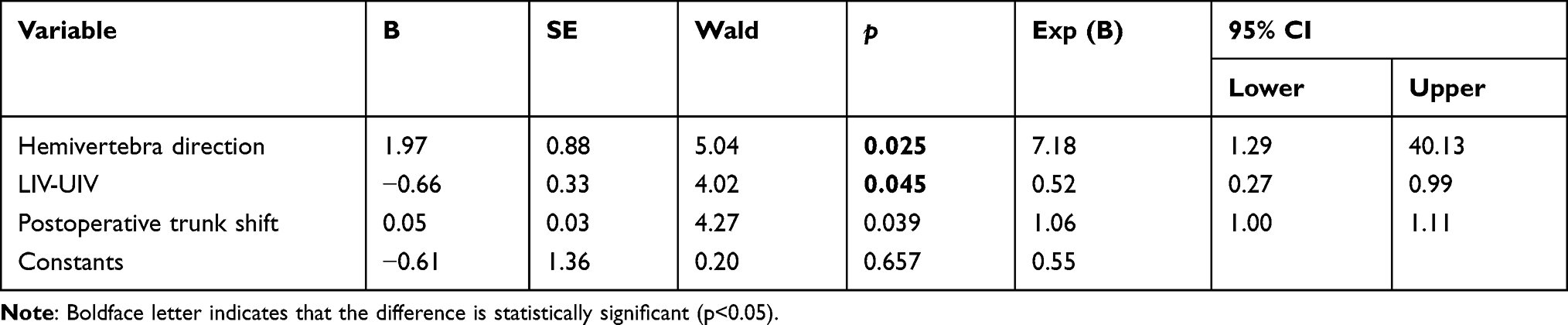 |
Table 4 Logistic Regression Analysis of Risk Factors for Patients with Additional Phenomena After Surgery |
Receiver Operating Characteristic Curve
The receiver operating characteristic (ROC) curve is shown in Figure 4. The results show that the area under the curve is 0.842 (95% CI: 0.708–0.975; P < 0.001), indicating that the ROC curve effectively predicts the occurrence of postoperative AOP. According to the ROC curve, the best cut-off value for the adding-on index as an indicator of the occurrence of AOP after surgery is 0.67. When the adding-on index is >0.67, the incidence of postoperative AOP is 90.0%, and the non-occurrence rate is 22.9%.
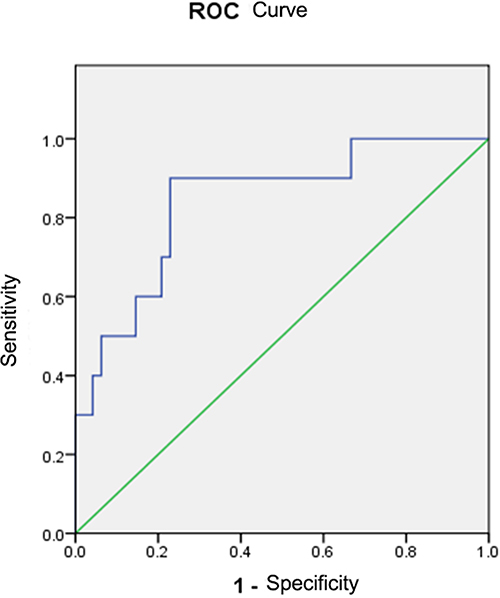 |
Figure 4 The receiver operating characteristic curve obtained after using the adding-on index to predict the occurrence of postoperative AOP is shown. The area under the curve is 0.842. |
Discussion
PHR and pedicle screw fixation is a safe and effective surgery. The surgical indications for HV resection for children older than 18 months are half-segmented and fully segmented hemivertebrae; thoracic, lumbar, or lumbosacral hemivertebrae; isolated defects; and unbalanced trunks.8
In recent years, research has shown that an increasing number of surgeons are using simple posterior HV resection to treat HV deformities. In 2017, Erturer et al4 evaluated the radiological and clinical effects of PHR and pedicle screw fixation in treating congenital spinal deformities. The correction rate of the malformation of the spinal coronal plane was 31%, and the average kyphotic angle was 45.7° preoperatively and 2.7° during follow-up. Huang et al9 evaluated the effectiveness and safety of the one-stage posterior HV resection for the treatment of multiple hemivertebrae. The correction rate of scoliosis was 73.3%, with correction rates of the proximal and distal compensatory curves of 70.0% and 79.1%, respectively, and a correction rate of segmental kyphosis/lordosis of 65.5%. Subsequently, Huang et al10 studied the effect of posterior HV resection of the upper thoracic segment. The average correction rate of segmental scoliosis was 80.2%, and the overall correction rate of scoliosis was 73.9%. The correction rates of the distal compensatory curve and segmental kyphosis were 64.9% and 65.5%, respectively. During the last follow-up, the Scoliosis Research Society (SRS)-22 scores of all patients had improved significantly over their preoperative scores.
Postoperative AOP are a common idiopathic complication for adolescents after scoliosis surgery, with an incidence reported in the literature of 2–51% (Lehman: 2%,11 Cao: 13.8%,12 Matsumoto: 18.8%,13 Kwan: 25%,14 Suk: 33.3%,15 Wang: 51.1%)5 AOP can also occur after surgery for CS. The incidence of postoperative AOP in this study was 17.2%, and it was the most common postoperative complication in this group of patients. This article first studied the risk factors for AOP after HV resection treated with PHR and pedicle screw fixation. Through univariate and logistic regression analysis, it was concluded that the HV direction, LIV–UIV, and postoperative TS were risk factors for AOP after treating CS with PHR and pedicle screw fixation.
The occurrence of AOP is closely related to the selection of fixed segments. Scholars such as Ilharreborde16 analyzed the influence of the length of posterior fusion on the clinical and imaging results of AIS. Although short-segment fusion can ensure a higher functional score, the incidence of AOP using this method is higher than selective fusion because the fused segment is shorter. Nohara et al17 compared the surgical effects between patients treated with anterior selective fusion (ASF) and posterior spinal fusion (PSF). During the 10-year follow-up, the incidence of distal AOP in the PSF group was lower than in the ASF group. They believed that the shorter length of the fused segments in the ASF group led to the higher incidence of AOP. The results of this study showed that LIV–UIV was a risk factor for postoperative AOP, indicating that short-segment fusion causes AOP after surgery in patients with CS.
The present study also shows that HV direction is a risk factor for postoperative AOP in patients with CS. The incidence of postoperative AOP in patients with malformation in the right hemivertebrae was 37.5%, which was significantly higher than 9.5% in patients with malformation in the left hemivertebrae. In this study, all patients with malformation in the right hemivertebrae had their main curves on the right side, which caused the L4 vertebra to tilt to the right; this may be the reason for the higher incidence of postoperative AOP in these patients. Miyanji et al18 suggested that, for adolescent patients with idiopathic scoliosis whose L4 tilted to the right, selecting NV-1 or NV as LIV can avoid AOP after surgery. Erdemir et al19 and Suk et al20 also suggested choosing NV-1 or NV as LIV to avoid postoperative AOP. Therefore, we suggest that for patients with a malformation in the right hemivertebrae, the fusion segment can be extended correspondingly to prevent the occurrence of postoperative AOP.
Postoperative coronal balance is a risk factor for AOP. The results of this study show that postoperative total main scoliosis is not a risk factor for postoperative AOP in patients with CS but postoperative TS is an important indicator of postoperative coronal balance. The average postoperative TS of patients in the add-on group was 28.10 mm and in the non-add-on group was 16.59 mm. For patients with postoperative coronal balance, the incidence of AOP was 10.3%. If HV resection and PHR and pedicle screw fixation are to be adopted, it is advisable to, as far as possible, reduce the TS and restore the coronal balance postoperatively to avoid AOP.
Previous studies on adolescent patients with idiopathic scoliosis have shown that the occurrence of AOP is related to their age and the maturity of their bones. Luk et al21 analyzed the risk factors of distal AOP in Lenke type 1A AIS, and the age of patients with postoperative AOP was significantly lower than patients without AOP. However, it is not only age but also bone maturity that is a factor in the incidence of distal AOP. Clinically, Risser’s sign and triangular cartilage (open or closed) are used to evaluate bone maturity. Wang,22 Bai,23 and Schlechter24 studied the causes of the distal AOP in AIS. The results of these studies showed that, as bone maturity increases, the incidence of postoperative AOP decreases. However, the results also showed that age, Risser’s sign, and triangular cartilage are not indicators of the risk of AOP in patients with CS. When compared with patients with AIS, in patients with CS caused by HV malformation, the segments are more localized and primarily located in some part of the hemivertebra, resulting in the risk of further progression of the deformity after HV resection being relatively small.
The regression equation for the adding-on index is −0.61 − 1.97 × the HV direction (R = 1, L = 0) − 0.66 × (LIV–UIV) + 0.05 × postoperative TS. The results of the ROC curve analysis show that the best cut-off value for the adding-on index to predict the occurrence of AOP after surgery is 0.67. When the adding-on index is >0.67, the incidence of postoperative AOP is 90%. These findings indicate that the occurrence of postoperative AOP is predictable, and the adding-on index is suitable for this prediction.
Based on the results of this study, we recommend the following: (1) When selecting the fused segment, in addition to considering the size of the scoliosis angle, the influence of the HV direction on the selection of the fixation or fusion segment should also be considered. (2) The fixation or fusion segment should be selected in a proper manner to reduce the occurrence of postoperative AOP. (3) For patients with a malformation in the right hemivertebrae, the fused segment can be appropriately extended. (4) When correcting a malformation with surgery, reduce the TS and try to restore the coronal balance as much as possible to decrease the likelihood of postoperative AOP.
In this study, during the follow-up, none of the patients with postoperative AOP needed to undergo repeat surgery, which we believe is attributable to the compensation of the unfused segments, shoulders, pelvis, and lower limbs. However, postoperative AOP should be avoided if possible.
This study had some limitations. First, it was a retrospective study, and due to the limitations in the study design, the incidence of complications may be underestimated. The accuracy of the data in a forward-looking study is higher than in a retrospective one. Second, this study does not include the clinical results relating to patients’ quality of life during follow-up. Future research is needed to further analyze the relationship between clinical results (including the SRS-24 and Oswestry Disability Index) and postoperative AOP. Finally, the sample size of this study was relatively small, and a large-scale study is needed.
Conclusion
PHR and pedicle screw fixation is an effective method for treating CS caused by HV malformation. The direction of the hemivertebrae, LIV–UIV, and TS are risk factors for AOP after PHR and pedicle screw fixation. According to the regression equation, the adding-on index is defined as −0.61 − 1.97 × the HV direction (R = 1, L = 0) − 0.66 × (LIV–UIV) + 0.05 × postoperative TS. The adding-on index has a high predictive accuracy for the occurrence of AOP after PHR and pedicle screw fixation. In patients with problems in the right hemivertebrae, when using PHR and pedicle screw fixation to treat CS caused by hemivertebrae, the fused segment should be appropriately extended, postoperative TS should be minimized, and the balance of the coronal position should be restored. With these measures, the occurrence of postoperative AOP can be avoided.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki. This study was conducted with approval from the Ethics Committee of Beijing Tongren Hospital. A written informed consent was obtained from legal guardians of all participants.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Winter RB, Lonstein JE, Boachie-Adjei O. Congenital spinal deformity. Instr course lect. 1996;45:117–127.
2. McMaster MJ, Ohtsuka K. The natural history of congenital scoliosis. A study of two hundred and fifty-one patients. J Bone Joint Surg Am. 1982;64(8):1128–1147. doi:10.2106/00004623-198264080-00003
3. Winter RB, Moe JH, Lonstein JE. Posterior spinal arthrodesis for congenital scoliosis. An analysis of the cases of two hundred and ninety patients, five to nineteen years old. J Bone Joint Surg Am. 1984;66(8):1188–1197. doi:10.2106/00004623-198466080-00006
4. Erturer RE, Kilinc BE, Gokcen B, Erdogan S, Kara K, Ozturk C. The results of hemivertebra resection by the posterior approach in children with a mean follow-up of five years. Adv Orthop. 2017;2017:4213413. doi:10.1155/2017/4213413
5. Yaszay B, O’Brien M, Shufflebarger HL, et al. Efficacy of hemivertebra resection for congenital scoliosis: a multicenter retrospective comparison of three surgical techniques. Spine. 2011;36(24):2052–2060. doi:10.1097/BRS.0b013e318233f4bb
6. Wang Y, Hansen ES, Høy K, Wu C, Bünger CE. Distal adding-on phenomenon in Lenke 1A scoliosis: risk factor identification and treatment strategy comparison. Spine. 2011;36(14):1113–1122. doi:10.1097/BRS.0b013e3181f51e95
7. Chang DG, Kim JH, Ha KY, Lee JS, Jang JS, Suk SI. Posterior hemivertebra resection and short segment fusion with pedicle screw fixation for congenital scoliosis in children younger than 10 years: greater than 7-year follow-up. Spine. 2015;40(8):E484–E491. doi:10.1097/BRS.0000000000000809
8. Bollini G, Docquier PL, Viehweger E, Launay F, Jouve JL. Lumbar hemivertebra resection. J Bone Joint Surg Am. 2006;88(5):1043–1052. doi:10.2106/JBJS.E.00530
9. Huang Y, Feng G, Song Y, et al. Efficacy and safety of one-stage posterior hemivertebral resection for unbalanced multiple hemivertebrae: a more than 2-year follow-up. Clin Neurol Neurosurg. 2017;160:130–136. doi:10.1016/j.clineuro.2017.07.009
10. Huang Y, Feng G, Liu L, et al. Posterior hemivertebral resection for upper thoracic congenital scoliosis: be aware of high risk of complications. J Pediatr Orthop B. 2019;28(1):1–9. doi:10.1097/BPB.0000000000000538
11. Lehman RA Jr, Lenke LG, Keeler KA, et al. Operative treatment of adolescent idiopathic scoliosis with posterior pedicle screw-only constructs: minimum three-year follow-up of one hundred fourteen cases. Spine. 2008;33(14):1598–1604. doi:10.1097/BRS.0b013e318178872a
12. Cao K, Watanabe K, Kawakami N, et al. Selection of lower instrumented vertebra in treating Lenke type 2A adolescent idiopathic scoliosis. Spine. 2014;39(4):E253–E261. doi:10.1097/BRS.0000000000000126
13. Matsumoto M, Watanabe K, Hosogane N, et al. Postoperative distal adding-on and related factors in Lenke type 1A curve. Spine. 2013;38(9):737–744. doi:10.1097/BRS.0b013e318279b666
14. Kwan MK, Chiu CK, Tan PH, et al. Radiological and clinical outcome of selective thoracic fusion for patients with Lenke 1C and 2C adolescent idiopathic scoliosis with a minimum follow-up of 2 years. Spine J. 2018;18(12):2239–2246. doi:10.1016/j.spinee.2018.05.007
15. Suk SI, Lee SM, Chung ER, Kim JH, Kim SS. Selective thoracic fusion with segmental pedicle screw fixation in the treatment of thoracic idiopathic scoliosis: more than 5-year follow-up. Spine. 2005;30(14):1602–1609. doi:10.1097/01.brs.0000169452.50705.61
16. Ilharreborde B, Ferrero E, Angelliaume A, et al. Selective versus hyperselective posterior fusions in Lenke 5 adolescent idiopathic scoliosis: comparison of radiological and clinical outcomes. Eur Spine J. 2017;26(6):1739–1747. doi:10.1007/s00586-017-5070-2
17. Nohara A, Kawakami N, Saito T, et al. Comparison of surgical outcomes between anterior fusion and posterior fusion in patients with AIS Lenke type 1 or 2 that underwent selective thoracic fusion -long-term follow-up study longer than 10 postoperative years. Spine. 2015;40(21):1681–1689. doi:10.1097/BRS.0000000000001121
18. Miyanji F, Pawelek JB, Van Valin SE, Upasani VV, Newton PO. Is the lumbar modifier useful in surgical decision making?: Defining two distinct Lenke 1A curve patterns. Spine. 2008;33(23):2545–2551. doi:10.1097/BRS.0b013e3181891822
19. Erdemir C, Musaoğlu R, Selek Ö, Ü G, Şarlak AY. Distal fusion level selection in Lenke 1A curves according to axial plane analyses. Spine J. 2015;15(11):2378–2384. doi:10.1016/j.spinee.2015.07.004
20. Suk SI, Lee SM, Chung ER, Kim JH, Kim WJ, Sohn HM. Determination of distal fusion level with segmental pedicle screw fixation in single thoracic idiopathic scoliosis. Spine. 2003;28(5):484–491. doi:10.1097/01.BRS.0000048653.75549.40
21. Luk KD, Don AS, Chong CS, Wong YW, Cheung KM. Selection of fusion levels in adolescent idiopathic scoliosis using fulcrum bending prediction: a prospective study. Spine. 2008;33(20):2192–2198. doi:10.1097/BRS.0b013e31817bd86a
22. Wang Y, Bünger CE, Zhang Y, Wu C, Li H, Hansen ES. Distal adding on in Lenke 1A scoliosis: what causes it? How can it be prevented? Spine Deform. 2014;2(4):301–307. doi:10.1016/j.jspd.2014.04.003
23. Bai J, Chen K, Wei Q, et al. Selecting the LSTV as the lower instrumented vertebra in the treatment of Lenke types 1A and 2A adolescent idiopathic scoliosis: a minimal 3-year follow-up. Spine. 2018;43(7):E390–E398. doi:10.1097/BRS.0000000000002375
24. Schlechter J, Newton P, Upasani V, et al. Risk factors for distal adding-on identified: what to watch out for. Spine J. 2008;8(5–supp–S):164. doi:10.1016/j.spinee.2008.06.772
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.