Back to Journals » Patient Preference and Adherence » Volume 17
An Age-Stratified Cross-Sectional Study of Physical Activity and Exercise Adherence of Stroke Survivors in Rural Regions
Authors Lin B ![]() , Xue L, An B, Zhang Z, Zhang W
, Xue L, An B, Zhang Z, Zhang W ![]()
Received 14 April 2023
Accepted for publication 4 August 2023
Published 15 August 2023 Volume 2023:17 Pages 2013—2023
DOI https://doi.org/10.2147/PPA.S417220
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Beilei Lin,1,2 Lihong Xue,1 Baoxia An,1 Zhenxiang Zhang,2 Weihong Zhang2
1Nursing Department, Henan Huaxian People Hospital, Anyang City, Henan Province, People’s Republic of China; 2Nursing and Health School, Zhengzhou University, Zhengzhou City, Henan Province, People’s Republic of China
Correspondence: Zhenxiang Zhang; Weihong Zhang, Nursing and Health school, Zhengzhou University, No 100 Science Avenue, Zhengzhou City, People’s Republic of China, Email [email protected]; [email protected]
Objective: To describe the Physical Activity and Exercise (PAE) adherence of stroke survivors in rural regions, additionally, to analyze the influential factors through age stratification.
Methods: This is a cross-sectional study. Totally, 596 stroke patients (65.70± 10.76 years) from three rural regions were selected, PAE scale was used for measuring compliance. The influential factors among different age groups were explored separately. This study adheres to the EQUATOR checklist, SROBE.
Results: Only 17.8% (106) of participants regularly participated in PAE. Altogether, 42.45% were classified as a young-middle age group, and the rest 57.55% were in the old age group. Positive attitudes and better PAE-relevant knowledge were protective factors for adherence in the young and middle-aged group (OR=0.683; 95% CI 0.173~0.588 and OR=0.939; 95% CI 0.013~0.114), as well as in the old group (OR=0.704; 95% CI 0.193~0.534 and OR=0.929; 95% CI 0.035~0.118); having no home rehabilitation equipment was a strong risk factor for younger patients (OR=16.078; 95% CI 1.235~4.320); however, without hemiplegia can positively affect their adherence (OR=0.891; 95% CI 0.045~0.229). In addition, the presence of a spouse can lead to a better compliance among old patients (OR=0.436; 95% CI − 0.496~-0.165).
Conclusion: It is necessary to improve the knowledge of physical activity in rural stroke patients of all ages. It is of great significance to install home rehabilitation equipment to promote exercise for young and middle-aged stroke patients. While for the old stroke patients, we strongly suggest focusing on the role of spouses, which would be more useful in low-income regions.
Keywords: stroke, physical activity, exercise, adherence, rural area, influential factors
Introduction
Stroke is the third-leading cause of death in many western countries,1 while it has been the leading cause of death and disability in China for recent years.2,3 Moreover, the recurrence rate of stroke and the disease burden are continuously increasing,1,3 and many rural areas remain underserved worldwide for a lack of stroke specialists. In 2013, a national survey of 155 urban and rural centers in China showed that the stroke caused burden has increased greatly, especially in rural areas where the prevalence rate of stroke increased by 155%.2 What is more, a study from Canada found that rural hospitals has higher 30-day in-hospital mortality rates than that of the urban academic hospitals.4 Additionally, many European rural areas are facing similar difficult problems as well.5 The stroke caused burden in rural areas is particularly heavy; which may be attributed to a lack of knowledge and poor awareness of disease prevention,6 irrational dietary habits and exercise beliefs,7 higher burden of stroke risk factors,8 and the uneven availability of specialist stroke care.3 For instance, a study conducted in Peru showed that people in rural areas who experience stroke received very little poststroke care and rehabilitation.9 Therefore, the high incidence, prevalence, disability, mortality, and burden have made the stroke in rural areas a serious public health problem worldwide.10 Not only do rural patients find it difficult to obtain rehabilitation sources, but the development and distribution of stroke follow-up guidelines are insufficiently implemented.11
The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) comprehensively explored the risk factors for cardiovascular diseases (CVD) and revealed that metabolic risks and body mass index significantly increased.12 The importance of regular physical activity and exercise (PAE) for cardiovascular health has been well documented, numerous systematic reviews have confirmed the benefits of physical activity in maintaining motor function across all stages of life after stroke.13–16 Regular exercise has positive effects on stroke survivors’ physical improvement, which could also benefit cognitive function17 and life quality.18 According to reports from Physical Activity and Exercise Recommendations for Stroke Survivors from the American Heart Association, physical activity is defined as “any bodily movement produced by skeletal muscles that results in energy expenditure” whereas exercise is “a subset of physical activity that is planned, structured, and repetitive and has a final or an intermediate objective for the improvement or maintenance of physical fitness.” The recommended frequency and duration of continuous training exercise range from 20 to 60 minutes per day and 3–7 days per week, depending on the patient’s fitness level.15,19
Although stroke survivors can counsel and benefit from increased participation in physical activity, as well as the appropriate prescription for exercise training, they may cease physical activity or reduce the frequency and duration, as reported by many studies conducted in urban areas,20–22 even without disability, only 32.4% of stroke patients adhered to aerobic activity guidelines, and 56.6% were presented with long sedentary time.23 Meanwhile, an important progress has been made in promoting stroke treatment and long-term management in metropolitan areas,6,24 however, the management of stroke patients in rural and remote areas has not generated sufficient concern, and reports about adherence conducted in these regions are also sparse. Given the high stroke burden, poor control of risk factors, and unhealthy lifestyle in rural areas, etc., it is particularly urgent to focus on patients’ PAE adherence in these rural regions. In addition, the epidemiological evidence suggest that the stroke incidence in young and middle-aged adults have been rising for the past two decades,25,26 due to the different varied underlying mechanisms and prognosis in old stroke patients,27 the optimal management of different stroke patients is still unknown, their behavioral characteristics need to be investigated separately. And, as age increases, adults may be more likely to adhere to self-paced versus prescribed moderate-intensity exercise.28 Thus, the impact of aging on exercise adherence in rural regions is worthy to be explored. In the current study, the cross-sectional survey is intended to investigate the PAE compliance among rural stroke patients, analyze the potential risk factors stratified by age, and propose corresponding counter measures for stroke prevention in rural regions.
Materials and Methods
Study Design and Participants
This is a cross-sectional study, a convenience sampling method was administered. Firstly, according to the economic level and research feasibility, three rural areas (northern, central and southern region of Henan Province) which could represent different economic levels were conveniently selected, among which northern region includes Anyang and Puyang; the central region includes Zhengzhou and Xuchang; while the southern region includes Nanyang and Zhumadian. Then, we recruited stroke patients from these three rural regions with the help of local hospitals and village committees. At the same time, we recruited six local college students who had returned to their hometowns during the holidays, trained them and asked them conduct the survey as summer social practice work during the summer vacation. All investigators participated voluntarily and underwent training and testing. The target population was adults aged above 18 years of age with a diagnosis of stroke, including ischemic stroke and hemorrhage stroke. Individuals were excluded if they had severe physical or mental disorders that prevented them from completing the questionnaire or if they had any other severe medical condition that prevented them from cooperating with the investigator. The data were collected at the patients’ homes or a centralized room in the village by trained investigators. After the survey, all participants were invited to carefully review and immediately confirm their responses to the questionnaire. Manuals of Life after Stroke Guide designed by the research team was given to each participant as a gift whether they completed the questionnaires or not. The guideline for reporting this study is the STROBE checklist (Supplementary File 1).
Measures
The Demographic Information Questionnaire
The demographic and disease-specific data questionnaire29 was designed and used to collect information on age, gender, education level, marital status, time since stroke, number of complications, the experience of community rehabilitation, etc.
Physical Activity and Exercise Adherence Scale (PAEAS)
The PAEAS was developed based on a literature review, qualitative review, expert consultation, and cognitive interviews (Supplementary File 2). Seven experts were consulted, and twenty patients were reviewed to improve clarity and rigor.30 The PAEAS has been previously tested30 and used31,32 among Chinese stroke patients in urban areas to determine their adherence to the recommended physical activity and exercise regimen. It contains 14 items organized into the following three sections: adherence to PAE participation (PAEP) with 8 items; adherence to PAE monitoring (PAEM) with 3 items; and adherence to PAE advice-seeking (PAEA) with 3 items. The scores of each question range from 1 (“never”) to 4 (“always”), and higher scores indicate better adherence. The adherence rate M can be calculated using the formula “M=actual score/max”, where max is obtained by multiplying the number of entries by 4. The adherence rate is defined as high at ≥75%, moderate at 50%–75%, and low at ≤50%.33,34 The Cronbach’s alpha value of the PAEAS is 0.900, and for each domain, the value ranges from 0.705 to 0.897. The scale content validity index (S-CVI) is computed as 0.950.35
Stroke Attitudes and Knowledge Questionnaire (SAKQ)
The SAKQ was developed based on the literature and was used in previous studies,32 we modified the questionnaire according to the characteristics of rural stroke patients. The formal version used in this study contains 23 yes-or-no items for knowledge and 14 Likert three-point items for attitude. The knowledge section can be divided into three sections, stroke accident (6 items), risk factors (11 items), and physical activity (6 items). All the answers were given a score of 1 or 0 (right or wrong, respectively), higher scores indicated a better understanding of stroke. The attitude section was used to measure patients’ attitudes toward physical activity and exercise. The responses of each item are divided into three levels, that is “important”, “not sure” and “not important”, which are scored as 3 points, 2 points, and 1 point. For this section, higher scores indicated a better attitude toward physical activity and exercise. The Cronbach’s α of the two sections are 0.832 and 0.873, respectively, and the split-half reliability is 0.749 and 0.765; the Content Validity Index (S-CVI) of the knowledge and attitude section is computed as 0.843 and 0.760.
Statistical Analysis
All statistical analyses were conducted in SPSS 21.0 software (https://spss.software.informer.com/21.0/). The data were divided into two groups by age, participants under 65 years old were classified as a young-middle group, while patients 65 or over were recognized as the old group. The differences in demographic characteristics between the two groups were analyzed using the chi-square test. The normal distribution test was confirmed before analysis. The data were statistically described (counting data using mean ± standard deviation, measurement data using frequency and percentage). Two unrelated groups’ mean scores were compared using a two-independent-sample t-test, while differences between three or more groups’ scores were tested through one-way analysis of variance (ANOVA). Pearson correlation methods were used to analyze the relations between knowledge, attitude, and PAE adherence. The multivariate logistic regression was used to explore the influencing factors of rural stroke patients’ PAE adherence both in the young-middle and old groups. Two-tailed p-values <0.05 were considered significant.
Results
Characteristics of the Study Sample in Two Groups
A total of 700 rural stroke patients were recruited, 596 of them were investigated with the remaining 104 patients refused to participate or failed to complete the questionnaires. The average response rate was 85.14%. Data were analyzed for the 596 subjects, their ages ranged from 33 to 90 years, with an average age of 65.70±10.76 years, 42.45% of them were classified as the young-middle group, 57.55% were classified as the old group. Patients with ischemic stroke accounted for 70.64%, and hemorrhagic stroke accounted for 29.36%. For the participants in young-middle group, their educational level was significantly higher than patients in the old group (proportion of patients with nine years or higher school study experience 42.29% VS 21.58%, X2=46.106, df=3, P<0.001), self-reported labor ability was better (62.06% VS 50.15%, X2=8.351, df=1, P=0.004), and care-giving tasks are more often undertaken by the spouse (74.31% VS 53.06%, X2=27.922, df=1, P<0.001). The PAD adherence scores of each sub-group were analyzed and compared (Table 1).
 |
Table 1 Characteristics of the Participants and PAE Adherence Differences (N = 596) |
Status of PAE Adherence in Two Groups
The average score of PAE adherence of rural young-middle and old stroke patients was 34.77±8.19 and 33.64±8.11 respectively, with a range from 14 to 56. Then, we classified the stroke patients into high, medium, and low adherence levels,30 the proportion of each level is shown in Figure 1. It showed that 82.2% of participants were at low or mid-level, 25.7% of the young-middle age stroke patients showed low adherence while 27.1% of the older patients’ adherence was at low-level.
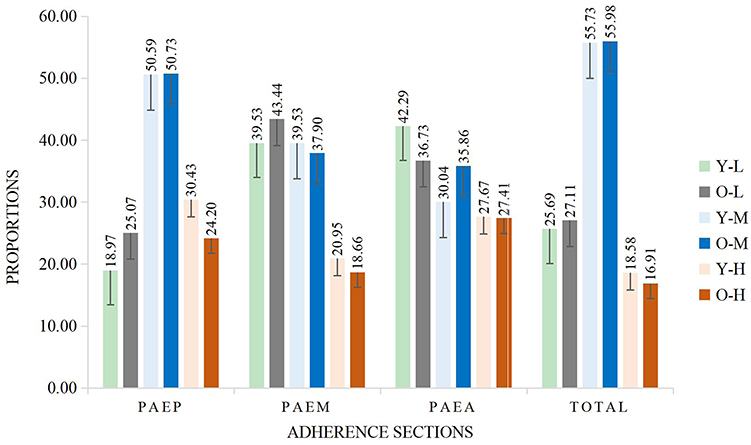 |
Figure 1 The proportions of PAE adherence levels among stroke patients in Young-middle and Old group. Notes: Y, O, L, M, H represent young-middle, old, low, medium and high, respectively; for example, Y-L means young-middle aged group with low-level PAE adherence account for 18.97%. The adherence rate M is ranked as high at M ≥0.75, mid-level at 0.50 < M < 0.75 and low at M ≤ 0.50. |
The Correlations Between Knowledge, Attitude, and PAE Adherence in Two Groups
The results showed that the stroke-related beliefs of stroke patients in rural areas were poor, and the accuracy rate of disease-related knowledge was only 48.69%. The score of stroke accident knowledge was 2.74±1.668 (6 points), risk factors 5.65±3.008 (11 points), and physical activity knowledge was 2.94±1.551 (6 points). Furthermore, the average score of attitudes was only 18.29±6.179, while the maximum score was 56 points. No significant difference in attitude or knowledge between the two groups was found (P>0.05). Further analysis showed that low or moderate correlations existed among attitude, knowledge, and PAE adherence in both young-middle and old groups (Table 2).
 |
Table 2 The Correlations Between Knowledge, Attitude and PAE Adherence (r, N = 596) |
Influencing Factors of PAE Adherence in Two Groups
The variables that had been previously shown to be significantly correlated with adherence in young-middle and old groups (referred to Table 1 and 2) were analyzed using multivariate logistic regression. Results showed that knowledge relevant to physical activity and attitude were protective influential factors for PAE adherence, indicating that more information about PAE and better attitude could promote physical activity or exercise among both young-middle and old stroke patients, while hemiplegia was a barrier in the young-middle group and home rehabilitation equipment was facilitator; spouses could play a positive role on maintaining adherence of the elderly (Table 3).
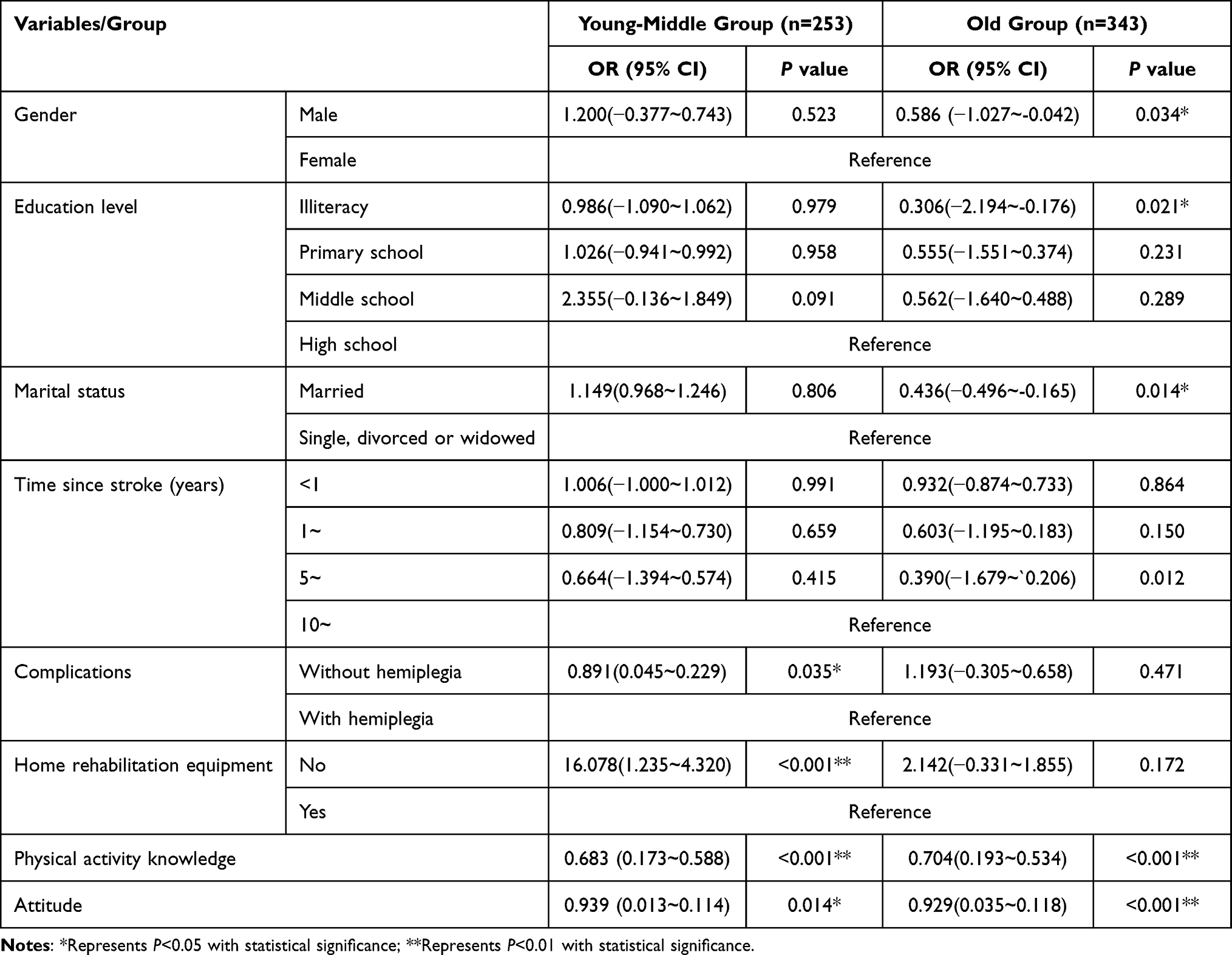 |
Table 3 Influential Factors of PAE Adherence in Two Groups (N = 596) |
Discussion
Stroke prevention in rural areas is more challenging,8,36 and health resources also need to be more equitably distributed, health inequities are still an objective fact that most developing countries are facing.8,37 Theoretical and empirical evidence regarding the benefits of regular physical activity or exercise is accumulating.15,19 However, to our knowledge, this study is the first to explore the PAE adherence of stroke survivors in rural areas. And with the progressive rejuvenation of stroke incidence, young patients have more heterogenous needs than old patients.38 Thus, it is of great value to explore the compliance of patients in different age groups and its influencing factors.
Consistent with a similar study conducted in urban areas,32 this study found that most of the stroke patients in rural areas showed low or moderate levels of adherence, not only the younger patients but also the elderly stroke patients. More than half of the young-middle aged (55.73%) and older patients (55.98%) showed a moderate level of adherence, what is more, only 17.80% of the participants’ adherence in this survey were at a high level (18.58% of the younger patients and 16.91% of the old patients), it was slightly lower than the adherence of urban stroke patients (20.19% at a high level).32 This result may be explained by the fact that when compared with that of urban residents, the participation of rural residents in sports activities was decreased, a survey39 conducted by the Center for Nutrition and Health of the Chinese Centers for Disease Control and Prevention showed that the proportion of adult farmers in rural areas participating in exercise was significantly lower than that of individuals in cities. Additionally, health-related resources disparity between metropolitan regions and rural areas could be also a reason for this minor difference.3,36 New areas of determinants research have identified environmental and genetic factors contributing to physical inactivity.40 Furthermore, a low level of literacy among rural stroke residents may have also contributed to the discrepant results, 32.55% of the respondents are illiterate in this study, while the number was only 14.90% among participants in urban areas.32 However, no matter in urban or rural areas, PAE compliance is not very good, which may be related to the cognitive and physical frailty caused by stroke, and studies have indeed confirmed that frailty affects the compliance behavior of individuals with stroke.41,42
Regarding the influential factors of PAE adherence in this study, knowledge about physical activity was a positive factor, as well as attitudes toward stroke. However, the results showed that after discharge, stroke patients in rural areas had very limited knowledge about stroke, the total accuracy rate of the knowledge section was less than 50% (48.69%). Most of the participants could not give correct answers to questions about stroke accidents (45.67%), risk factors (51.36%), and physical activity (49.09%). In addition, they showed a rather negative attitude toward disease prevention and risk factors, the average score of the attitudes dimension was only 18.29, while the theoretical maximum was 56 points. This finding is consistent with other studies conducted in rural areas.43 Therefore, we can conclude that stroke patients in rural areas not only have poor knowledge of the disease but also have a serious misunderstanding of the importance of controlling stroke-related risk factors. This finding may have a certain relationship with the generally low level of health literacy of residents in Chinese rural areas, several surveys have shown that the health literacy regarding chronic disease prevention among rural residents was only 8.4%.7,44 After all, inequitable distribution of health resources between urban and rural areas is common.45 And this is why studies always suggest that all interventions should be based on the provision of patient education, it could effectively improve stroke patients’ knowledge and behavioral outcomes in rural areas.46
This study also found that the patients’ PAE adherence within 1 year after onset was slightly higher than their adherence after 1~10 years, even if no significant difference was found. Similarly, a longitudinal follow-up study in China showed that after discharge, stroke patients showed higher adherence at the early stage after discharge.31 This may be associated with the limited supervision from local general practitioners or nurses in long term, while nearly 70% of the stroke patients in rural areas have no access to follow-up service after discharge in this study, 69.98% for the old group and 71.94% for the young-middle group, respectively. Another longitudinal study conducted in Australia also revealed that stroke patients’ physical activity levels were reduced immediately post-stroke.47 There is evidence that stroke patients with advanced age, long-term illness, and activity of daily life (ADL) disability are more susceptible to frailty,48 and frailty is reported to be a contributing factor to lower adherence to treatment or rehabilitation.42 Those evidences can also help to understand why in this study no hemiplegia was a protective factor. In addition, stroke patients who lived with spouses showed a higher adherence, which indicated the importance of spousal roles in rural families, especially for elderly stroke patients, the protective effect of spouses was stronger than the younger group (OR=0.436; P<0.05). Therefore, it could be an alternative in rural communities to consider spouses’ important contribution on promoting patients’ participation in physical activity.49
Emerging evidence confirms that physical and social environmental factors are also key determinants of PAE adherence.12,40 In this study, the self-reported PAE compliance score of young and middle-aged stroke patients with home rehabilitation equipment was significantly higher than that of patients without home rehabilitation environment (42.74±8.920 vs 34.44+8.010, OR=16.078), however, few patients mentioned that they have rehabilitation aid at home. The results further suggest a possible effect of lack of resources in rural households on adherence.23,50 Considering the social needs of younger patients,38 public or shared rehabilitation room could be useful and economical for this population. Furthermore, we found that only 28.06% of young-middle age and 30.32% of old stroke patients had received professional help from their village doctors, this phenomenon may indicate that the home rehabilitation environment is an important facilitator for physical activity after stroke in rural and remote areas as well. However, even if the building environment in person-centered stroke rehabilitation at home51 or conducting family-based stroke intervention could be useful for long-term recovery, it is really difficult to take steps to improve the home rehabilitation environment in rural China with inadequate medical resources and rehabilitation services.52 To effectively address this problem, virtual rehabilitation may be a more cost-effective alternative for stroke patients in rural areas.53
Study Limitations
First, with limited resources, we chose a convenience sampling method to recruit stroke patients, which would affect the representativeness of the results. Therefore, to fully understand the adherence status of stroke patients in rural areas, a systematic randomized sampling method is essential. For the second limitation, we only analyzed the effect of knowledge and attitude on stroke patients’ physical adherence; we did not address social support, family functioning, self-efficacy, disease-related frailty and other potential factors, which will affect the main conclusion, especially for rural areas. Finally, this study could be only representing the status in China, for Henan is the largest agricultural province in China, however, considering the economic levels or health policies are various among different countries, more evidences are needed for further comparison and analysis in the futures.
Conclusions
In summary, stroke patients in rural areas have poor knowledge about stroke, and their attitudes or perceptions of the importance of physical activity after stroke were less positive, similar problems were found among both young-middle age and old participants. Additionally, most of the rural stroke patients do not adhere to the physical activity and exercise recommended by relevant guidelines, their physical activity adherence needs to be improved to facilitate their physical and psychological rehabilitation. Our study also highlighted the importance of health education, especially the benefits of physical activity and exercise. Furthermore, installing home exercise equipment and enhancing the role of the spouse may have a positive effect on promoting physical activity and exercise. Further studies should establish a scientific and standardized system to educate stroke patients and their caregivers, develop virtual or real home environments, trigger their intrinsic motivation, and improve their adherence to secondary strategies for stroke prevention.
Abbreviations
ADL, Activity of Daily Life; PAE, Physical activity and exercise; PAEAS, Physical Activity and Exercise Adherence Scale; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; OR, odd risk; CVD, cardiovascular diseases; PAEP, PAE participation; PAEM, PAE monitoring; PAEA, PAE advice-seeking; S-CVI, scale content validity index; SAKQ, Stroke Attitudes and Knowledge Questionnaire; ANOVA, Analysis of variance.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available due to the fact that they do not provide the more necessary information, but are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of Zhengzhou University (ZZURIB2016-003). All participants received and agreed with the informed consent.
Consent for Publication
Consent to publish has been approved by all authors.
Acknowledgments
The authors would like to thank all the investigators and participants of this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The author disclosed receipt of the following financial support for the research of this article: Youth Project of National Natural Science Foundation of China (Grant number 72104221); Science and Technology Department of Henan Province (Grant number 232102310170/22IRTSTHN027).
Disclosure
The authors declare that they have no conflict of interest.
References
1. Krishnamurthi RV, Ikeda T, Feigin VL. Global, regional and country-specific burden of ischaemic stroke, intracerebral haemorrhage and subarachnoid haemorrhage: a systematic analysis of the global burden of disease study 2017. Neuroepidemiology. 2020;2020:1–9.
2. Wang W, Jiang B, Sun H, et al. Prevalence, incidence, and mortality of stroke in China: results from a nationwide population-based survey of 480 687 adults. Circulation. 2017;135(8):759–771. doi:10.1161/CIRCULATIONAHA.116.025250
3. Wu S, Wu B, Liu M, et al. Stroke in China: advances and challenges in epidemiology, prevention, and management. Lancet Neurol. 2019;18(4):394–405. doi:10.1016/S1474-4422(18)30500-3
4. Fleet R, Bussières S, Tounkara FK, et al. Rural versus urban academic hospital mortality following stroke in Canada. PLoS One. 2018;13(1):e0191151. doi:10.1371/journal.pone.0191151
5. Hubert GJ, Santo G, Vanhooren G, et al. Recommendations on telestroke in Europe. Eur Stroke J. 2019;4(2):101–109. doi:10.1177/2396987318806718
6. Chen X, Orom H, Hay JL, et al. Differences in rural and urban health information access and use. J Rural Health. 2019;35(3):405–417. doi:10.1111/jrh.12335
7. Meihua W, Cuiping Z, Xiaofang X. Investigation and analysis of the status of family rehabilitation in rural stroke patients. Nurs Res. 2016;30(5c):1912–1914.
8. Kamin Mukaz D, Dawson E, Howard VJ, et al. Rural/urban differences in the prevalence of stroke risk factors: a cross-sectional analysis from the REGARDS study. J Rural Health. 2022;38(3):668–673. doi:10.1111/jrh.12608
9. Miranda JJ, Moscoso MG, Yan LL, et al. Addressing post-stroke care in rural areas with Peru as a case study. Placing emphasis on evidence-based pragmatism. J Neurol Sci. 2017;375:309–315. doi:10.1016/j.jns.2017.02.027
10. Dong K, Yang Q, Duan F, et al. Stroke and (or) myocardial infarction attributable to modifiable risk factors in Henan, China. J Am Soc Hypertens. 2018;12(7):524–533. doi:10.1016/j.jash.2018.03.013
11. Pedersen RA, Petursson H, Hetlevik I. Stroke follow-up in primary care: a prospective cohort study on guideline adherence. BMC Fam Pract. 2018;19(1):179. doi:10.1186/s12875-018-0872-9
12. Collaborators GRF. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1923–1994.
13. Garcia-Rudolph A, Sanchez-Pinsach D, Salleras EO, Tormos JM. Subacute stroke physical rehabilitation evidence in activities of daily living outcomes: a systematic review of meta-analyses of randomized controlled trials. Medicine. 2019;98(8):e14501. doi:10.1097/MD.0000000000014501
14. Plummer P, Iyigun G. Effects of physical exercise interventions on dual-task gait speed following stroke: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2018;99(12):2548–2560. doi:10.1016/j.apmr.2018.04.009
15. Billinger SA, Arena R, Bernhardt J, et al. Physical activity and exercise recommendations for stroke survivors: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2014;45(8):2532–2553. doi:10.1161/STR.0000000000000022
16. Diep L, Kwagyan J, Kurantsin-Mills J, Weir R, Jayam-Trouth A. Association of physical activity level and stroke outcomes in men and women: a meta-analysis. J Womens Health. 2010;19(10):1815–1822. doi:10.1089/jwh.2009.1708
17. Brunt A, Albines D, Hopkins-Rosseel D. The effectiveness of exercise on cognitive performance in individuals with known vascular disease: a systematic review. J Clin Med. 2019;8(3):294. doi:10.3390/jcm8030294
18. Hou L, Du X, Chen L, et al. Exercise and quality of life after first-ever ischaemic stroke: a two-year follow-up study. Int J Neurosci. 2018;128(6):540–548. doi:10.1080/00207454.2017.1400971
19. Gordon NF, Gulanick M, Costa F, et al. Physical activity and exercise recommendations for stroke survivors: an American Heart Association Scientific statement from the Council on Clinical Cardiology, Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention; the Council on Cardiovascular Nursing; the Council on Nutrition, Physical Activity, and Metabolism; and the Stroke Council. Circulation. 2004;109:2031–2041. doi:10.1161/01.CIR.0000126280.65777.A4
20. Levy T, Laver K, Killington M, Lannin N, Crotty M. A systematic review of measures of adherence to physical exercise recommendations in people with stroke. Clin Rehabil. 2019;33(3):535–545. doi:10.1177/0269215518811903
21. Miller KK, Porter RE, DeBaun-Sprague E, Van Puymbroeck M, Schmid AA. Exercise after stroke: patient adherence and beliefs after discharge from rehabilitation. Top Stroke Rehabil. 2017;24(2):142–148. doi:10.1080/10749357.2016.1200292
22. Tiedemann A, Sherrington C, Dean CM, et al. Predictors of adherence to a structured exercise program and physical activity participation in community dwellers after stroke. Stroke Res Treat. 2012;2012:136525. doi:10.1155/2012/136525
23. Choi YA, Lee JS, Park JH, Kim YH. Patterns of physical activity and sedentary behavior and their associated factors among nondisabled stroke survivors. Maturitas. 2022;158:10–15. doi:10.1016/j.maturitas.2021.11.009
24. Li Y, Zhang X, Sang H, et al. Urban-rural differences in risk factors for ischemic stroke in northern China. Medicine. 2019;98(21):e15782. doi:10.1097/MD.0000000000015782
25. Ekker MS, Boot EM, Singhal AB, et al. Epidemiology, aetiology, and management of ischaemic stroke in young adults. Lancet Neurol. 2018;17(9):790–801. doi:10.1016/S1474-4422(18)30233-3
26. Singhal AB, Biller J, Elkind MS, et al. Recognition and management of stroke in young adults and adolescents. Neurology. 2013;81(12):1089–1097. doi:10.1212/WNL.0b013e3182a4a451
27. Van Alebeek ME, Arntz RM, Ekker MS, et al. Risk factors and mechanisms of stroke in young adults: the FUTURE study. J Cereb Blood Flow Metab. 2018;38(9):1631–1641. doi:10.1177/0271678X17707138
28. Lee HH, Dunsiger S, Connell Bohlen L, Boyle HK, Emerson JA, Williams DM. Age moderates the effect of self-paced exercise on exercise adherence among overweight adults. J Aging Health. 2020;32(3–4):154–161. doi:10.1177/0898264318812139
29. Beilei L. Status and Influencing Factors of Physical Activity Adherence for Community-Dwelling Stroke Survivors. Zhengzhou: Nursing and Health School, Zhengzhou University; 2012.
30. Beilei L, Zhenxiang Z, Yumei S, Yongxia M, Junfang X, Yaqi Z. Compilation of physical activity compliance scale and reliability and validity test in community stroke patients. Chin J Rehabil Med. 2013;28(6):574–578.
31. Hai S, Shengwen S, Huiqin W, et al. Study on the dynamic changes of rehabilitation exercise compliance in stroke patients. Chin J Nurs. 2016;51(6):712–715.
32. Lin B, Zhang Z, Mei Y, Liu L, Ping Z. The influential factors of adherence to physical activity and exercise among community-dwelling stroke survivors: a path analysis. J Clin Nurs. 2022;31(17–18):2632–2643. doi:10.1111/jocn.16091
33. Duncan PW, Horner RD, Reker DM, et al. Adherence to postacute rehabilitation guidelines is associated with functional recovery in stroke. Stroke. 2002;33(1):167–177. doi:10.1161/hs0102.101014
34. Fengjuan L. Study on the Compliance of Patients with Breast Cancer After Operation and its Influencing Factors [Master’s thesis]. Guangzhou: Scool of Nursing, Sun Yat-sen University; 2008.
35. Denise F, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;2006(26):489–497.
36. Javor A, Ferrari J, Posekany A, Asenbaum-Nan S. Stroke risk factors and treatment variables in rural and urban Austria: an analysis of the Austrian Stroke Unit Registry. BMJ open. 2019;14(4):e0214980.
37. Smits C, Toelsie JR, Eersel M, Krishnadath I. Equity in health care: an urban and rural, and gender perspective; the Suriname health study. AIMS Public Health. 2018;5(1):1–12. doi:10.3934/publichealth.2018.1.1
38. Perin C, Bolis M, Limonta M, et al. Differences in rehabilitation needs after stroke: a similarity analysis on the ICF core set for stroke. Int J Environ Res Public Health. 2020;17(12):4291. doi:10.3390/ijerph17124291
39. Caicui D, Fan Y, Weiyan G. Analysis of Chinese farmers’ leisure time exercise in 2010~2012. J Nutri. 2017;39(6):712–715.
40. Bauman AE, Reis RS, Sallis JF, Wells JC, Loos RJ, Martin BW. Correlates of physical activity: why are some people physically active and others not? Lancet. 2012;380(9838):258–271. doi:10.1016/S0140-6736(12)60735-1
41. Huang YN, Yan FH, Wang XY, et al. Prevalence and risk factors of frailty in stroke patients: a meta-analysis and systematic review. J Nutr Health Aging. 2023;27(2):96–102.
42. Levine DA, Langa KM, Fagerlin A, et al. Physician decision-making and recommendations for stroke and myocardial infarction treatments in older adults with mild cognitive impairment. PLoS One. 2020;15(3):e0230446. doi:10.1371/journal.pone.0230446
43. Oguoma VM, Nwose EU, Bwititi PT. Cardiovascular disease risk prevention: preliminary survey of baseline knowledge, attitude and practices of a Nigerian rural community. N Am J Med Sci. 2014;6(9):466–471. doi:10.4103/1947-2714.141644
44. Xianggang H, Longpeng Y, Walter S. Investigation on the health literacy level of rural residents and the influencing factors of disease. Chin J Clin. 2014;42(1):43–45.
45. Jiang S, Seslar SP, Sloan LA, Hansen RN. Health care resource utilization and costs associated with atrial fibrillation and rural-urban disparities. J Manag Care Spec Pharm. 2022;28(11):1321–1330. doi:10.18553/jmcp.2022.28.11.1321
46. Ruiz-Perez I, Bastos A, Serrano-Ripoll MJ, Ricci-Cabello I. Effectiveness of interventions to improve cardiovascular healthcare in rural areas: a systematic literature review of clinical trials. Prev Med. 2019;119:132–144. doi:10.1016/j.ypmed.2018.12.012
47. Moore SA, Hallsworth K, Plötz T, Ford GA, Rochester L, Trenell MI. Physical activity, sedentary behaviour and metabolic control following stroke: a cross-sectional and longitudinal study. Disabil Rehabil. 2013;8(1):e55263.
48. Xu R, Li Q, Guo F, Zhao M, Zhang L. Prevalence and risk factors of frailty among people in rural areas: a systematic review and meta-analysis. BMJ open. 2021;11(4):e043494. doi:10.1136/bmjopen-2020-043494
49. Zhou B, Zhang J, Zhao Y, et al. Caregiver-delivered stroke rehabilitation in rural China the RECOVER randomized controlled trial. Stroke. 2019;50(7):1825–1830. doi:10.1161/STROKEAHA.118.021558
50. Nicholson S, Sniehotta FF, van Wijck F, et al. A systematic review of perceived barriers and motivators to physical activity after stroke. Int J Stroke. 2013;8(5):357–364. doi:10.1111/j.1747-4949.2012.00880.x
51. Kylen M, von Koch L, Pessah-Rasmussen H, Ytterberg C, Heylighen A, Elf M. The importance of the built environment in person-centred stroke rehabilitation at home. Int J Stroke. 2019;14(4_SUPPL):50.
52. Han J, Mao WJ, Ni JX, et al. Rate and determinants of recurrence at 1 year and 5 years after stroke in a low-income population in rural China. Front Neurol. 2020;11:11. doi:10.3389/fneur.2020.00011
53. Funao H, Tsujikawa M, Momosaki R, Shimaoka M. Virtual reality applied to home-visit rehabilitation for hemiplegic shoulder pain in a stroke patient: a case report. J Rural Med. 2021;16(3):174–178. doi:10.2185/jrm.2021-003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.