Back to Journals » Infection and Drug Resistance » Volume 15
Amphotericin B May Decrease the Serum Level of Voriconazole: A Case Report and Brief Review of Literature
Received 16 May 2022
Accepted for publication 5 September 2022
Published 12 September 2022 Volume 2022:15 Pages 5397—5400
DOI https://doi.org/10.2147/IDR.S374853
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Zhen Hu, Huaying Zhou
Department of Infectious Diseases, The Second Xiangya Hospital, Central South University, Changsha, Hunan, 410011, People’s Republic of China
Correspondence: Huaying Zhou, Department of Infectious Diseases, The Second Xiangya Hospital, Central South University, Changsha, Hunan, 410011, People’s Republic of China, Email [email protected]
Background: Combination therapy with amphotericin B (AmB) and Voriconazole are sometimes used due to reducing AmB-related adverse reactions and improving outcomes. However, there was no report whether AmB would affect the serum level of Voriconazole.
Case Presentation: A patient was in presumption of invasive fungal infection. Voriconazole and amphotericin B was combined for administration. The results showed that serum levels of Voriconazole were dramatically reduced when combined AmB, whereas went up when receiving Voriconazole alone.
Conclusion: AmB might decrease the level of Voriconazole. Such a combination of AmB and Voriconazole cannot be considered appropriate until more data are available.
Keywords: amphotericin B, voriconazole, fungal infection, drug interaction
Background
Amphotericin B (AmB) is a broad-spectrum antifungal agent produced by the bacterium Streptomyces nodosus. It is indicated for the treatment of life-threatening invasive fungal infection. However, adverse events, particularly nephrotoxicity, are limiting factors in achieving an effective dose. In order to reduce adverse reactions and improve outcomes, combination antifungal therapy is sometimes administrated. This will inevitably enhance the risk of clinically significant drug–drug interactions. In review of the literature, about 8 cases reported the therapeutic efficacy of AmB in combination with Voriconazole in invasion fungal infection.1–8 However, there is no literature on the two drug interaction. Here, we present a case of drug interaction between AmB and Voriconazole, which has not been described in the literature.
Case Presentation
A 57-year-old man was admitted to our hospital in August 2020 on account of significant loss of weight and appetite over the past 4 months and fever for 1 month. Few positive findings were noted on the physical examination except the patient was poor development with a body weight of 45 kg (body mass index: 14.2 kg/m2), and had anemic appearance and hepato-splenomegaly. No palpable lymph nodes were found. The patient was HIV-seronegative and was considered immunocompetent. He was a builder. On admission, the serum 1.3- beta-D-glucan level increased significantly. The Histoplasma capsulatum was presumed by microscopic examination of the bone marrow smear (Figure 1). However, no measurement was made for Histoplasma capsulatum antigen. Drug susceptibility testing for Histoplasma capsulatum should have been performed, but unfortunately, we did not conduct it since the blood and bone marrow culture were all negative. The Metagenomic Next Generation Sequencing Test in bone marrow was also negative. Antifungal therapy with Voriconazole (Pfizer Inc, New York, NY, USA, 6 mg/kg intravenously every 12 hours for the first 24 hours, then 4 mg/kg oral every 12 hours) instead of amphotericin B was first introduced due to lack of experience with AmB. Trough serum levels of Voriconazole were monitored weekly after 5 days of therapy to ensure adequate absorption, with a goal of achieving a concentration of 2 to 5μg/mL. 7.40μg/mL,5.29μg/mL, 3.79μg/mL of serum level of Voriconazole were obtained. But the patient did not make improvement. Voriconazole was stopped. Intravenous liposome AmB (New Asia pharmaceutical, Shanghai, China) was gradually added at the dose of 3 mg/kg daily. Two weeks later, the patient’s clinical symptoms, such as his fever and loss of appetite, began to improve. But the patient did not tolerate chemotherapy very well with markedly elevated sera creatinine levels. Intravenous AmB liposomal (reduced to 1 mg/kg daily) plus Voriconazole (4 mg/kg oral every 12 hours 4 mg/kg twice daily after initiation of a loading dose) was administered. Monitoring Voriconazole serum levels continued regularly. 0.52μg /mL, 1.71μg/mL, 0.86μg/mL of serum level of Voriconazole were obtained. Glutathione was co-administrated to protecting hepatic and renal function during hospital. The patient with good adherence did not take any agent or food supplements (ie, phenytoin, St.John’t wort, etc.) that influenced the blood drug level of Voriconazole. Liposomal AmB (L-AmB) was stopped due to presumption of drug interactions between Voriconazole and AmB. Voriconazole (4 mg/kg oral every 12 hours) alone was administrated for subsequent therapy. 3.20μg /mL, 5.29μg /mL, 4.46μg /mL of serum trough concentration of Voriconazole were obtained, which were significantly higher than previous result. This suggested that AmB may decrease the serum levels of Voriconazole. Unfortunately, due to be unable to test the serum concentration of AmB, we could not observe the influence of Voriconazole on AmB levels.
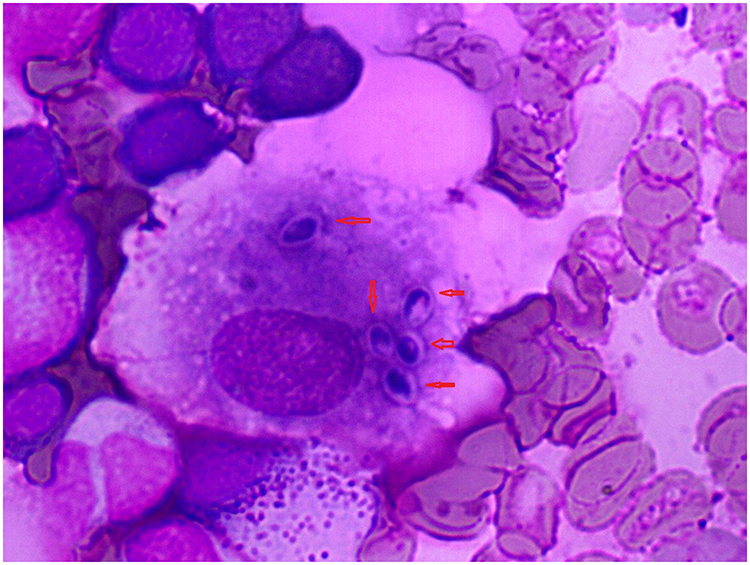 |
Figure 1 Wright stain finding of bone marrow smear demonstrated intracellular oval budding yeast (red arrows) of Histoplasma capsulatum. (1000 × magnification oil lens). |
Sample Collection, Storage and Bio-Analysis
Venous blood samples (2 mL) were collected into anticoagulant tubes. The samples were collected at least 3 days after initiation of a loading dose or maintenance and an adjusted dose of 4 days as well as within 2 h before any maintenance doses.9 All Voriconazole plasma concentration was measured by an automatic two-dimensional liquid chromatography (2D-HPLC, Demeter Instrument Co., Ltd., Changsha, Hunan, China).10 The two-dimensional separation conditions consisted of the following: the first dimensional chromatographic column was FRO C18 (100mm × 3.0 mm, 5μm, ANAX); and the flow rate: 1.0 mL/min. The second dimensional chromatographic column was ASTON HD C18 (150 mm × 4.6 mm, 5μm, ANAX). The stability of blood sample at room temperature for 8 h and at-20°C of three repeated freeze-thaw cycles was within ±8.00% and ±10.0%, respectively. Besides, the laboratory performed annual external quality assessment (EQA) to ensure the accuracy of the measurement results.
Discussion
Combination therapy with AmB and Voriconazole is sometimes used due to reducing AmB-related adverse reactions and improving outcomes, especially in refractory invasive fungal infection. However, no study reported whether AmB affected the serum level of Voriconazole. In review of the literature, about eight literature evaluated the therapeutic efficacy of AmB combined with Voriconazole in invasive fungal infection.1–8 Two reports are in vitro observations,1,2 three reports are in the animal study,3–5 and three reports are in patient observation.6–8 The vitro observations showed combinations antifungal therapy exhibited promising results and no apparent antagonistic interaction was detected. One animal observation indicated that the efficacy of monotherapy and the two-drug combinations therapy was similar; activity was neither enhanced nor reduced with combination therapy. Another two animal studies observed that the AmB + Voriconazole combination was most effective at reducing tissue burden, sterilizing tissues, and reducing mortality than AmB alone or Voriconazole alone. One human observational data showed the triple combination of AmB, caspofungin and Voriconazole may be an option worth exploring in patients with refractory fungal infections who do not appear to be improving on more standard therapy.6 Another two patients observation demonstrated AmB combined with Voriconazole may rapidly improve clinical manifestation, substantially shorten the hospitalization time.7,8 The interaction between the two drugs was not mentioned in vivo studies.1–8 None of them tested the serum level of Voriconazole. Here, we discovered AmB might lower the level of Voriconazole. We observed the serum levels of Voriconazole were in normal levels (7.40μg/mL, 5.29μg/mL, 3.79μg/mL; 3.20μg /mL, 5.29μg /mL, 4.46μg/mL) when Voriconazole was administrated alone. The Voriconazole concentration would be reduced (0.52μg /mL, 1.71μg/mL, 0.86μg/mL) when combined AmB, which indicated AmB might decrease the level of Voriconazole. However, the mechanism underlying is not clear. Voriconazole, an extended spectrum azole, its metabolisation takes place in the liver, at the level of P450 CYP2C19, CYP2C9, and CYP3A4, and its products of metabolism are excreted by the kidneys.11 Only 2% of the dose excreted in urine is unchanged. There may be a variety of drug–drug interactions that must be considered. AmB is another important drug widely used to treat serious systemic fungal infections. It has a terminal half-life of 127 h in healthy subjects and its distribution differs widely between organs, and the highest AmB concentrations are reached in the liver12 with the potential to alter hepatic cellular integrity.13,14 In perfused rat livers, it has been demonstrated that AmB reduces bile flow, decreases bile acid secretion and alter hepatic P-450 activity. Thus, it is possible that AmB affects the level of Voriconazole by altering hepatic p450 activity. But the mechanism needs further research.
Conclusion
In summary, our results showed AmB may decrease the serum concentration of Voriconazole, such a combination of AmB and Voriconazole cannot be considered appropriate until more data are available.
Ethics and Consent
The Ethics Committees of The Second Xiangya Hospital of Central South University (LYF-20221 26) approved this study, the institutional agreed to publish the case details.
Consent for Publication
The patient provided written informed consent for publication of clinical details and images in this study.
Acknowledgments
We are grateful to the patients for giving consent for the case report.
Funding
This work was supported by Natural Science Foundation of Hunan Province (2019JJ50886).
Disclosure
The authors report no conflicts of interest in this work.
References
1. O’Shaughnessy EM, Meletiadis J, Stergiopoulou T, et al. Antifungal interactions within the triple combination of amphotericin B, caspofungin and Voriconazole against Aspergillus species. J Antimicrob Chemother. 2006;58(6):1168–1176. doi:10.1093/jac/dkl392
2. Oz Y, Kiremitci A, Dag I, et al. Postantifungal effect of the combination of caspofungin with Voriconazole and amphotericin B against clinical Candida krusei isolates. Med Mycol. 2013;51(1):60–65. doi:10.3109/13693786.2012.697198
3. Chandrasekar PH, Cutright JL, Manavathu EK. Efficacy of Voriconazole plus amphotericin B or micafungin in a Guinea-pig model of invasive pulmonary aspergillosis. Clin Microbiol Infect. 2004;10(10):925–928. doi:10.1111/j.1469-0691.2004.00958.x
4. Silva EG, Paula CR, Dias AL, et al. Combination efficacy of Voriconazole and amphotericin B in the experimental disease in immunodeficient mice caused by fluconazole-resistant Cryptococcus neoformans. Mycopathologia. 2011;171(4):261–266. doi:10.1007/s11046-010-9375-5
5. Kirkpatrick WR, Coco BJ, Patterson TF. Sequential or combination antifungal therapy with Voriconazole and liposomal amphotericin B in a guinea pig model of invasive aspergillosis. Antimicrob Agents Chemother. 2006;50(4):1567–1569. doi:10.1128/AAC.50.4.1567-1569.2006
6. Verma A, Williams S, Trifilio S, et al. Successful treatment of concomitant pulmonary zygomycosis and aspergillosis with a combination of amphotericin B lipid complex, caspofungin, and Voriconazole in a patient on immunosuppression for chronic graft-versus-host disease. Bone Marrow Transplant. 2004;33(10):1065–1066. doi:10.1038/sj.bmt.1704485
7. Liu JY, Liu J, Su XH, et al. Amphotericin B plus fluorocytosine combined with Voriconazole for the treatment of non-HIV and non-transplant-associated cryptococcal meningitis: a retrospective study. BMC Neurol. 2022;22(1):274. doi:10.1186/s12883-022-02803-1
8. Fujioka K, Nagai T, Kinoshita Y, et al. Successful treatment with Voriconazole combined with amphotericin B-liposome for fluconazole-resistant pulmonary cryptococcosis after renal transplantation. CEN Case Rep. 2019;8(4):261–265. doi:10.1007/s13730-019-00403-6
9. Chen K, Zhang X, Ke X, et al. Individualized medication of voriconazole: a practice guideline of the division of therapeutic drug monitoring, Chinese pharmacological society. Ther Drug Monit. 2018;40:663–674. doi:10.1097/FTD.0000000000000561
10. Tang D, Song BL, Yan M, et al. Identifying factors affecting the pharmacokinetics of Voriconazole in patients with liver dysfunction: a population pharmacokinetic approach. Basic Clin Pharmacol Toxicol. 2019;125(1):34–43. doi:10.1111/bcpt.13208
11. Hulin A, Dailly E, Le Guellec C. Level of evidence for therapeutic drug monitoring of Voriconazole. Therapie. 2011;66:109–114. doi:10.2515/therapie/2011009
12. Christiansen KJ, Bernard EM, Gold JWM, et al. Distribution and activity of amphotericin B in humans. J Infect Dis. 1985;152(5):1037–1043. doi:10.1093/infdis/152.5.1037
13. Massa T, Sinha DP, Frantz JD, et al. Subcronic toxicity studies of N-D-ornithyl amphotericin B methyl ester in dogs and rats. Fundam Appl Toxicol. 1985;5(4):737–753. doi:10.1016/0272-0590(85)90198-8
14. Inselmann G, Schimanski A, Jahns R, et al. Liposomal amphotericin B (AmBisome) application and hepatic microsomal enzyme function in the rat. Mycoses. 1999;42(7–8):459–463. doi:10.1046/j.1439-0507.1999.00506.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.