Back to Journals » The Application of Clinical Genetics » Volume 13
Alternating Hemiplegia of Childhood: Understanding the Genotype–Phenotype Relationship of ATP1A3 Variations
Authors Capuano A, Garone G ![]() , Tiralongo G
, Tiralongo G ![]() , Graziola F
, Graziola F ![]()
Received 16 December 2019
Accepted for publication 27 February 2020
Published 30 March 2020 Volume 2020:13 Pages 71—81
DOI https://doi.org/10.2147/TACG.S210325
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Martin Maurer
Alessandro Capuano,1 Giacomo Garone,1,2 Giuseppe Tiralongo,1 Federica Graziola1
1Movement Disorders Clinic, Department of Neuroscience and Neurorehabilitation, IRCCS Bambino Gesù Children’s Hospital, Rome, Italy; 2University Hospital Pediatric Department, IRCCS Bambino Gesù Children’s Hospital, University of Rome Tor Vergata, Rome, Italy
Correspondence: Alessandro Capuano
Movement Disorders Clinic, Department of Neuroscience and Neurorehabilitation, IRCCS Bambino Gesù Children’s Hospital, Viale Di San Paolo, Rome 15 – 00153, Italy
Tel +39 066 859 4092
Email [email protected]
Abstract: Alternating hemiplegia of childhood (AHC) is a rare neurological disorder affecting children with an onset before 18 months. Diagnostic clues include transient episodes of hemiplegia alternating in the laterality or quadriparesis, nystagmus and other paroxysmal attacks as tonic and dystonic spells. Epilepsy is also a common feature. In the past, a great effort has been done to understand the genetic basis of the disease leading to the discovery of mutations in the ATP1A3 gene encoding for the alpha3 subunit of Na+/K+ATPase, a protein already related to another disease named Rapid Onset Dystonia Parkinsonism (RDP). ATP1A3 mutations account for more than 70% of cases of AHC. In particular, three hotspot mutations account for about 60% of all cases, and these data have been confirmed in large population studies. Specifically, the p.Asp801Asn variant has been found to cause 30– 43% of all cases, p.Glu815Lys is responsible for 16– 35% of cases and p.Gly947Arg accounts for 8– 15%. These three mutations are associated with different clinical phenotype in terms of symptoms, severity and prognosis. In vitro and in vivo models reveal that a crucial role of Na+/K+ATPase pump activity emerges in maintaining a correct membrane potential, survival and homeostasis of neurons. Herein, we attempt to summarize all clinical, genetic and molecular aspects of AHC considering ATP1A3 as its primary disease-causing determinant.
Keywords: ATP1A3, Na+/K+ATPase, AHC, genetics, animal models
Introduction
First described in 1971 by Verret and Steele in 8 children,1 the syndrome of alternating hemiplegia of childhood (AHC, OMIM #614820) was defined only 9 years later by Krägeloh and Aicardi,2 who described five novel cases and reviewed the previous reports discussing the nosology of this entity. Specific diagnostic criteria for AHC, named “Aicardi criteria,” were first proposed in 1993.3 Since then, the original criteria were periodically updated, in order to support clinical recognition of this peculiar neurodevelopmental disorder.4–7
In 2012, two independent research groups – an international consortium8 and a German group9 – identified de novo heterozygous mutations in the ATP1A3 as the cause of AHC. Soon after, a Japanese study replicated this finding,10 providing further evidence that ATP1A3 mutations causing AHC.
Heterozygous ATP1A3 mutations had been already reported to cause another entity previously described on a clinical basis: rapid-onset dystonia-parkinsonism (RDP, DYT12, OMIM #128235), a rare and peculiar movement disorder inherited in an autosomal dominant manner.11 In 2014, ATP1A3 have been reported to cause another neurological entity: cerebellar ataxia, areflexia, pes cavus, optic atrophy and sensorineural hearing loss (CAPOS) syndrome (OMIM #601338).12,13 In addition, over the recent years, two other phenotypes related to ATP1A3 mutations have emerged: the early infantile epilepsy with encephalopathy (EIEE)14,15 and the recurrent encephalopathy with cerebellar ataxia (RECA) phenotype.16,17
Most of the patients with ATP1A3 pathogenic variants fall into one of these phenotypes,18 which underlie a nearly non-overlapping subset of causative mutations.19,20 Nevertheless, some individuals show atypical features or combine features of two or more of these major phenotypes.20–24 On the other hand, some pathogenic variants have been reported to cause different phenotypes, even in the same family.4,25–27 As a result, it has been proposed to consider ATP1A3-related disorders as a clinical continuum rather than distinct entities, with an age-dependent pattern of emergence and progression of different signs and symptoms.16,18,19
Despite the growing number of reports describing intermediate and overlapping forms between the major ATP1A3-related phenotypes, AHC remains a well-defined and recognizable syndrome, whose clinical identification is essential to orientate molecular investigations.
In this review, we summarize knowledge on AHC, focusing on clinical diagnostic clues, genotype–phenotype correlations and functional effect of ATP1A3 variants of this condition.
Clinical Features
Classic AHC
AHC is a peculiar neurodevelopmental disorder characterized by a constellation of paroxysmal neurological manifestations, among which recurrent episodes of hemiplegia involving either side of the body and alternating in laterality are the hallmark of this disease.18 Quadriplegic attacks can occur in isolation or as a generalization of a hemiplegic attack. In addition, paroxysmal manifestations include tonic or dystonic spells (either of one limb, one hemibody or generalized), oculomotor abnormalities and dysautonomic phenomena (uni- or bilateral mydriasis, flushing, pallor) may occur alone or in association with hemiplegic attacks.19 Paroxysmal episodes usually occur before 18 months of age, with a median age of onset of 3–5 months. Nevertheless, onset may range from the neonatal period to 4 years of age.
Paroxysmal abnormal ocular movements (including monocular and binocular nystagmus, strabismus, disconjugate gaze, ocular bobbing, ocular flutter) are often the first neurological manifestations, occurring in isolation before the onset of other paroxysmal spells.28
Paroxysmal events typically recognize emotional or environmental trigger factors (exercise, exposure to light, sounds or hot water, specific foods), while symptoms are relieved by sleep and post-awakening periods.7 A high variability in duration and frequency of paroxysms has been reported, even in the same patient, lasting from minutes to entire days and occurring up to several times per day.28
Beyond paroxysmal manifestations, AHC is also characterized by persistent, interictal neurological abnormalities, whose prevalence increases with age. Developmental issues (speech and language delay, cognitive deficits, behavioral problems) with various degrees of severity are the most common finding, followed by dysarthria, ataxia, chorea, dystonia, and, less frequently, pyramidal tract signs.7,27,29 Neurological deterioration may show a stepwise progression, with discrete motor or cognitive decline following a prolonged paroxysmal episode. Fixed neurological deficits often show a rostrocaudal gradient of severity, with severity of oro-mandibular dystonia and dysarthria overcoming upper and lower limbs dystonia severity.7
Up to 50% of AHC patients develop epileptic seizures.4,5,30,31 Epilepsy can be focal or generalized, with multiple seizure types and localizations, and it is often drug-resistant. Moreover, a high frequency and recurrence rate of refractory status epilepticus has been reported.32
The last version of the clinical criteria for AHC recognizes major (diagnostic) and minor (supporting) criteria, and include a set of standardized definitions for a simplified description of paroxysmal episodes, in order to provide to caregivers a more accessible language to document events.7 Particularly the criteria included 1) the onset of the symptoms before 18 months, 2) repeated episodes of hemiplegia alternating laterally or 3) repeated episodes of quadriplegia or plegia, 4) other paroxysmal episodes including dystonic attacks, 5) oculomotor abnormalities or automatic symptoms, 6) vanishing of the symptoms with sleep and 7) evidence of developmental delay and/or other neurological abnormalities as dystonia, ataxia or chorea.7 From a pharmacological point of view, the most frequent drugs used in AHC are flunarizine, benzodiazepines, carbamazepine, barbiturates and valproic acid. It has been wildly demonstrated that flunarizine and benzodiazepines show a greater improvement in dystonic or plegic episodes.5 Mikati et al particularly demonstrated that flunarizine, a calcium antagonist, reduces the duration, severity, and frequency of the hemiplegic attacks in up to 80% of AHC patients.33
On the other hand, antipsychotics, selective serotonin reuptake inhibitors, gabapentin, and acetazolamide were invariably ineffective.5
Atypical AHC
Besides the classic AHC phenotype, several atypical features have been described. With regard to age at onset, a delayed occurrence of hemiplegic attacks up to 4 years of age has been described.25 Regarding cognitive impairment, mild cases with normal development have been reported.33 Other uncommon features include a predominantly dystonic phenotype, the absence of quadriplegic attacks,33 or the occurrence of alternating upper limb monoplegia.34
In addition, some patients combine typical AHC paroxysms with the features of either early-onset encephalopathy14,35,36 or RDP.23,37–39
Aside from AHC, a distinct nosological entity with milder course, characterized by episodes of unilateral or bilateral weakness arising exclusively out of sleep has been described.40–46 Although the first report of this condition dates back to the original description of AHC by Verret and Steele,1 its distinct nosology was recognized only in 1994, when the term benign nocturnal alternating hemiplegia of childhood (BNAHC) was proposed to differentiate this entity from AHC.40 In BNAHC, (hemi)plegic attacks only onset from sleep, and there is no progression to neurological or intellectual impairment. In addition, other paroxysmal events such as tonic or dystonic spells and oculomotor abnormalities are lacking.40,41 To date, 14 cases of BNAHC have been reported, all but one affecting boys.42 Albeit rarely tested, no association between BNAHC and ATP1A3 mutations has been described.42 Among the 14 patients, only 2 performed a Whole Exome Sequencing (WES) analysis and in only 1 case it was disclosed a heterozygous 16p11.2 microdeletion involving, among others PRRT2 gene. PRRT2 encodes for a transmembrane protein containing a proline-rich domain and is associated with episodic kinesigenic dyskinesia-1 (OMIM #128200).42 Although several familial cases have been reported,40,41,45 the genetic basis (if any) of this condition is still elusive. A proper WES analysis should be performed to better investigate this condition and the role of regulatory additional genetic factors should be considered.
Role of ATP1A3 Gene Disruption
Na+/K+-ATPase Structure and Function
ATP1A1-4 genes encode for four α subunit – respectively α1-4 – of Na+/K+ ATPase. Pump is ubiquitously expressed in the central nervous system (CNS) and it is constituted by almost two subunits: one alpha (α – containing the catalytic site for ATP hydrolysis and binding the ions) and one beta (β, responsible for the structural and functional asset of the α-subunit).47 Although α1 isoform is present in whole CNS and α2 in the astrocytes, the α3 is expressed only in the neurons – GABAergic neurons in all nuclei of the basal ganglia (striatum, globus pallidus, subthalamic nucleus, and substantia nigra), several thalamic nuclei, cortex, cerebellum, red nucleus, and several areas of the midbrain (reticulotegmental nucleus of pons) and hippocampus;48 while expression was not significant in the dopaminergic cells of substantia nigra.49,50 This ion pump is essential for the maintenance of the electrogenic homeostasis of neural cells, exchanging Na+ and K+ ions across the plasma membrane coupled to ATP hydrolysis, setting the membrane potential both in resting potential (α1) and after an action potential (α2, α3).
The α3 isoform is encoded by the ATP1A3 gene (OMIM #182350) on chromosome 19q13 encodes for the α3 subunit of the Na+/K+-ATPase, an ubiquitous, electrogenic transmembrane ATPase first described in 195751 and located on the cytosolic side of the outer plasma membrane.52 Exporting 3 Na+ and importing 2 K+ ions for every single ATP molecule hydrolyzed, the Na+/K+-ATPase maintains the gradient of a higher extracellular Na+ concentration and a higher K+ intracellular level.53,54
Although α3 is the subunit predominantly expressed in neurons, some neurons express α1 – that is predominantly expressed in glial cells. Compared to α1, the α3 subunit shows a lower affinity for Na+ and K+, and lower voltage dependence, enabling a rapid normalization of transmembrane gradient after a series of action potentials.55
The α subunit of the Na+/K+-ATPase contains 3 cytoplasmic and one transmembrane regions. The cytoplasmic domains include the phosphorylation (“P”) domain, the nucleotide-binding (“N”) domain and the actuator (“A”) domain.53 As in the other members of the P-type ATPase superfamily, the Na+/K+-ATPase forms a phosphorylated intermediate during the reaction cycle. The P domain harbors a highly conserved Asp-Lys-Thr-Gly-Lys sequence, whose aspartate residue (falling in the 366 position) is phosphorylated by transfer of the γ-phosphate group of an ATP molecule.56 The A domain contains a Thr-Gly-Glu-Ser motif that bonds, through the glutamate residue, the water molecule needed for aspartyl-phosphate hydrolysis in the catalytic site.57 The transmembrane region is composed of 10 transmembrane helices (TM1-10), of which helices TM4-6 contain the cation binding sites and TM8 contributes to the biding of the third Na+ ion.57,58
To allow ions exchange, during the reaction cycle the protein undergoes critical conformational changes, reversing the accessibility and specificity of the cation binding sites.59 In the so-called E1 state, the α subunit is accessible from the cytoplasmic side and is Na+-selective. The binding of 3 Na+ triggers the phosphorylation of the Asp366 residue from ATP, leading to the E1P state. As a result, Na+ ions are transported across the membrane and released on the extracellular side. By Na+ release, the protein turns into the E2P state, which is an extracellular accessible, K+-selective conformation. The binding of 2 K+ ions on the cytoplasmic side triggers the dephosphorylation by hydrolysis of the Asp366 residue, with transition to the E2 state. The low-affinity binding of an ATP molecule to the E2 state stimulates the transition to the E1 state, whose low affinity for K+ ions determines their release in the cytosol. The higher affinity for ATP and Na+ ions of the E1 state causes the binding of the Na+ and the following phosphorylation of the P-domain. Rotation of the A domain and rearrangements of TM1-6 mediate these conformational transitions.59–64
The β-subunit – of which three differentially expressed isoforms (β1-3) exist – acts as a molecular chaperon that facilitates the transport from the endoplasmic reticulum to the plasma membrane of the α subunit and permits its correct folding and membrane integration.65,66
In addition to ion transport across the cellular membrane, the Na+/K+-ATPase has been shown to have different functions, including modulation of signal transduction via PI3K, PLC-γ and MAPK cascades, protein interactions with other transmembrane enzymes and scaffolding proteins and regulation of other transporter activity.20,67,68
ATP1A3 Pathogenic Variants Location and Effect
As shown in Figure 1, ATP1A3 mutations affect the whole coding sequence. Differently from RDP causing mutations – that are distributed throughout the gene – AHC causing variants are more frequently found in exons 17 and 18.20 With regard to the affected functional domain, most AHC-causing variants affect the ions binding sites or the transmembrane segments that harbor the binding residues (Figure 2).57 A smaller group of mutations is found in transmembrane helices other than the ion binding segments. Furthermore, several mutations affect the cytoplasmic extensions of the transmembrane helices TM3-5, that connect these helices with the cytoplasmic A-, N- and P-domains (the so-called “stalk” mutations).57 This latter cytoplasmic domain has been found to harbor several AHC-causing variants, while a small group of pathogenic variants have been found to affect the extracellular loop between TM7 and TM8.
|
Figure 1 Distribution of AHC-causing variants along the ATP1A3 gene and mRNA. Note: Columns show the number of AHC-causing variants (light grey bars) and the total number of pathogenic ATP1A3 variants (dark grey bars) reported in each exon. Abbreviations: AHC, alternating hemiplegia of childhood; Nt, Nucleotides; bp, basepairs. |
|
Figure 2 Location of AHC-causing variants in the ATP1A3 protein. Notes: White dots show AHC-causing variants, black dots indicate variants causing EIEE with the presence of hemiplegic attacks, blue-and-white dots show variants causing both RDP and AHC. According to functional domains localization, variants are divided into ion binding site variants (black), membrane variants (blue), stalk variants (green), P domain variants (purple) and extracellular variants (red). The three-different cytosolic domains of the ATP1A3 protein are indicated in red (A domain), green (N domain) and blue (P domain). Abbreviations: AHC, alternating hemiplegia of childhood; EIEE, early infantile epileptic encephalopathy; RDP, rapid-onset dystonia-parkinsonism. |
As a result, a vast proportion of AHC-causing variants are expected to affect the ion binding and transport, while another consistent group of mutations is expected to affect enzyme phosphorylation.57
For some of the ion-binding sites mutations (Asp801Asn, Asp923Asn, Ser137Tyr, Phe780Leu, Ile810Asn), experimental evidence of defective Na+ binding has been provided,69–71 while for other variants impaired Na+ binding has been shown with mutations affecting the corresponding residue in the α1 paralog.57 Of note, few mutations have been reported in the transmembrane helices far from the ion-binding sites (such as TM1-2 and TM9-10). Interestingly, variants affecting the N-cytoplasmic domain or the C-terminus domain have been described only in RDP.
Genotype–Phenotype Correlation
Emergence and Frequency of Different AHC-Causing Variants
Although AHC is a sporadic disorder due to de novo variants, few autosomal dominant inherited cases have been reported.4,25,26,72 Germline mosaicism has been reported in familial cases of other ATP1A3-related disorders,73 but it has not been described in AHC so far.
Despite the growing number of pathogenic variants reported, the largest cohort studies conducted in different populations (European, North American and Chinese cohorts) demonstrated that three variants account for about 60% of all cases.4,30,74 Specifically, the p.Asp801Asn variant has been found to cause 30–43% of all cases, p.Glu815Lys is responsible for 16–35% of cases and p.Gly947Arg accounts for 8–15% (Figure 3).
|
Figure 3 Frequency of AHC-causing variants in different cohorts. Notes: The graph shows the relative frequency of variants affecting each specific ATP1A3 residue in a North American (blue line, N= 151), European (red line, N= 130) and a Chinese (black line, N= 45) cohort. The peaks are expressed as the percentage of the total number of AHC patients in each cohort. The three hotspots for AHC-causing variants (Asp801, Glu915 and Gly947) are indicated above the corresponding peak. Abbreviation: AHC, alternating hemiplegia of childhood. |
As previously stated, the location of ATP1A3 mutations along the coding sequence shows a genotype–phenotype correlation of the ATP1A3 clinical spectrum. Only specific mutation – particularly near the transmembrane domains – and consequently protein alterations result in AHC (Rosewich H. Neurology 2014).27
Three recurrent missense mutations count for 60% of all AHC cases. Fifteen percent of AHC have no mutation identified but meet the clinical criteria. In a recent report by Panagiotakaki al. clinical data of a large cohort of 155 patients from the international Consortium of AHC were deeply reviewed and an attempt to discretely genotype–phenotype correlation was done.30 First, interestingly, ATP1A3 mutations were detected in 85% of patients, confirming that a small group of patients met the criteria for AHC without any molecular genetic diagnosis. The study also confirmed the relative incidence of the three most common mutations: p.Asp801Asn, p.Glu815Lys and p.Gly947Arg. Of these, Glu815Lys was associated with a more severe phenotype, with drug-resistant epilepsy, profound intellectual disability and severe dystonia as neurological main findings. p.Asp801Asn appears to be associated with a milder phenotype with later onset of the paroxysmal events and less frequent plegic attacks; the majority of patients present moderate intellectual disability with a higher rate of behavioral problems. p.Gly947Arg seems to correlate with a positive prognosis; the onset of the paroxysmal event is the latest when compared with other two mutations, moreover no severe intellectual disability has been reported. In conclusion, the three mutations show a gradient of severity of the symptoms: p.Glu815Lys > p.Asp801Asn > p.Gly947Arg. Table 1 summarizes the clinical spectrum associated with the three most common mutations.
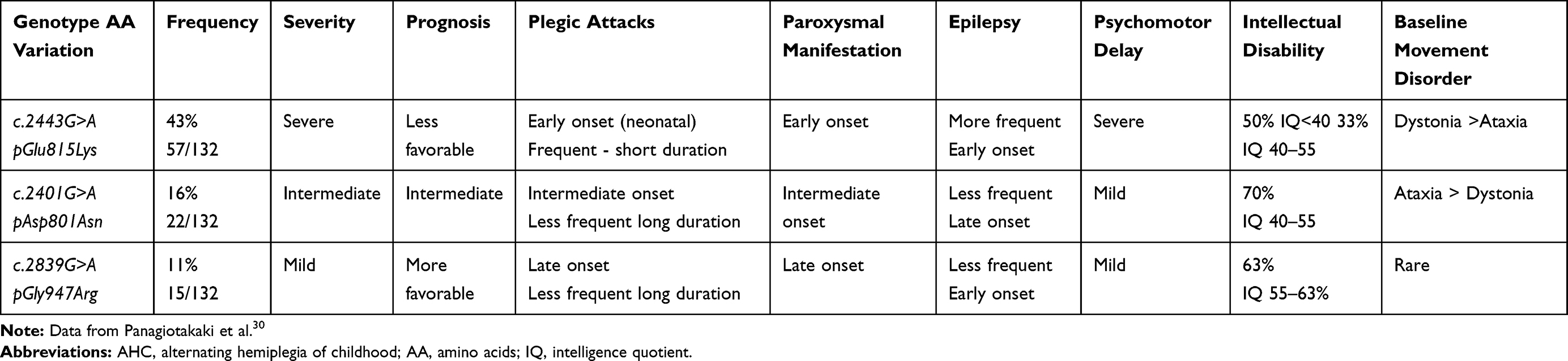 |
Table 1 Clinical Features of Most Common ATP1A3 Variants Causing AHC |
Evidence from in vitro and in vivo Studies
A great contribution to explaining the clinical heterogeneity associated with ATP1A3 mutations as well as to improve our knowledge and develop new therapeutic strategies, arises from cellular and animal models.
Cellular Studies
In the neuron presenting the α3 allele mutation, Na+/K+ ATPase shows reduced sodium affinity, leading to an elevated intracellular Na+ concentration with many possible dramatic events such as increased influx Ca++ ions into the cell with toxic effects and liberation of excitatory aminoacids.50 Moreover, it has been supposed that an altered uptake of dopamine secondary to the abnormal Na+ gradient is partially responsible for the ATPase related syndrome.4,75 This alteration leads to dystonia and/or parkinsonism without degeneration of the nigrostriatal pathway,54,75 but it has not been demonstrated by PET and DAT-SCAN study in RDP patient, which explains lack of response to levodopa in these patients.76
Heterogeneity in the phenotypic spectrum shown by AHC patients and by patients with RDP suggests different underlying cellular consequences relevant to the pathological mechanisms. In general, from the first description and characterization of ATP1A3 mutations associated with AHC,8 the activity of Na+/K+ pump seems to be responsible of pathogenicity in AHC. Thus, it was reasonable that in RDP, most mutations affected protein expression and cell surface expressions, and in the AHC, an altered activity of the pump could explain the phenotype.8 Several studies have been conducted to clarify that issue71,77 and one useful approach was by using induced Pluripotent Stem (iPS) cells. Recently, in a model of iPS cells derived neurons from AHC patients carrying the missense mutation p.Gly947Arg, lower levels of ouabain-sensitive outward current (a net outward transport of a Na+ ions) have been demonstrated compared to controls.77 Furthermore, as it may be predicted by a lower intracellular K+ ion concentration, neurons exhibit a resting membrane potential similar to resting cell with altered excitability, dealing with the hypothesis of a loss of function mechanism.77
Moreover, in a very recent study (2019), Arystarkhova et al point out that severity of phenotype cannot be explained solely by reduction of pump activity and other cellular mechanisms are hypothesized from experimental data, including misfolding protein at Golgi apparatus level and consequent ratio between good and bad alleles, by competition.78
Animal in vivo Studies
Several mouse models have been developed to study in vivo consequences of α3 isoform variants. There are five main models which have been exhaustively studied, summarized in Table 2. The first model was characterized by Moseley et al (2007).79 Introducing a single base pair mutation in intron 4 (α3+/KOI4), with aberrant splicing knocking out the allele (Atp1a3tm1/Ling/+), replicated by other authors,80,81 these mice displayed both maniacal-like phenotype, increased by methamphetamine response, and seizures with an increased motor activity. In 2013, Ikeda et al49 proposed another mouse model with the large deletion from 2 to 6 exons (α3+/ E2−6): for the first time, affected mice disclosed dystonia induced by intracerebellar kainite injections. Because of the large deletion and the sequential aberrant product, the clinical pattern of the above two models was very severe and far from the human ATP1A3 phenotype. Clapcote et al71 were the first to develop a mouse model with single nucleotide substitution causing a single aminoacid substitution (I810N, Myshkin α3+/I810N). In his work, he described mice with severe seizures both spontaneous and evoked by vestibular stress (running, leaping), behavioural arrest (freezing-like) and death after partial complex seizures with secondary generalization. Another similar mutant model has been described by Hunayan et al in 2015, modelling the pAsp801Asn variant, called Mashl +/- (α3+/D801N). The model recalls many features of AHC such as dystonia and hemiplegia, with cerebellar involvement (ataxia and tremor). Recently another mouse model of AHC has been reported. This novel knock-in mouse model (Atp1a3E815K+/-, Matoub, Matb+/-) expresses the E815K mutation of the Atp1a3 gene (the most severe common phenotype of AHC).83 In their elegant study, authors clearly demonstrated that mutated mice expressed behavioural and neurophysiological features, resembling the most severe form of AHC. In particular, the motor initiative was poor, the motor performance was deeply impaired (e.g. coordination, balance, abnormal gait), and interestingly, other than epilepsy, many mice were observed to pass during spontaneous seizure or provoked seizures for sudden unexpected death in epilepsy (SUDEP).83 Of note, the hemiplegia and dystonia episodes were both spontaneous and induced by high level of stress (e.g. water contact or cage change), likely in the human phenotype. It’s noteworthy to underlie that although differences among the proposed models exist, some features are common including the brain hyperexcitability, motor abnormalities (spontaneous or provoked) and behaviour alterations, according to a pivotal role of ATP1A3 in brain functioning.
E2−6): for the first time, affected mice disclosed dystonia induced by intracerebellar kainite injections. Because of the large deletion and the sequential aberrant product, the clinical pattern of the above two models was very severe and far from the human ATP1A3 phenotype. Clapcote et al71 were the first to develop a mouse model with single nucleotide substitution causing a single aminoacid substitution (I810N, Myshkin α3+/I810N). In his work, he described mice with severe seizures both spontaneous and evoked by vestibular stress (running, leaping), behavioural arrest (freezing-like) and death after partial complex seizures with secondary generalization. Another similar mutant model has been described by Hunayan et al in 2015, modelling the pAsp801Asn variant, called Mashl +/- (α3+/D801N). The model recalls many features of AHC such as dystonia and hemiplegia, with cerebellar involvement (ataxia and tremor). Recently another mouse model of AHC has been reported. This novel knock-in mouse model (Atp1a3E815K+/-, Matoub, Matb+/-) expresses the E815K mutation of the Atp1a3 gene (the most severe common phenotype of AHC).83 In their elegant study, authors clearly demonstrated that mutated mice expressed behavioural and neurophysiological features, resembling the most severe form of AHC. In particular, the motor initiative was poor, the motor performance was deeply impaired (e.g. coordination, balance, abnormal gait), and interestingly, other than epilepsy, many mice were observed to pass during spontaneous seizure or provoked seizures for sudden unexpected death in epilepsy (SUDEP).83 Of note, the hemiplegia and dystonia episodes were both spontaneous and induced by high level of stress (e.g. water contact or cage change), likely in the human phenotype. It’s noteworthy to underlie that although differences among the proposed models exist, some features are common including the brain hyperexcitability, motor abnormalities (spontaneous or provoked) and behaviour alterations, according to a pivotal role of ATP1A3 in brain functioning.
 |
Table 2 Summary of Pre-Clinical Mouse Models of ATP1A3 Mutations Related to AHC |
Conclusion
With the growing emergence of new phenotypes related to ATP1A3 along together with the high accessibility to genetic tests in this new era, clinicians and scientists have renewed their interest in ATP1A3-related disorders. In particular, since the discovery that ATP1A3 mutations are causative of AHC, great efforts have been made to understand how disruption of normal functions of ATPase activity may lead to different phenotypes of the disease. Although many pathogenic mechanisms contributing to AHC and RDP are still unknown, AHC phenotypes have been better understood and delineated, thus, in the last years, a genotype–phenotype correlation has been attempted in order to classify main discrete phenotypes. AHC is a complex condition where clinical picture includes paroxysmal events fluctuating over time, dystonia, epilepsy, ataxia as well as intellectual disability and behavioral disorders; consequently, understanding the natural course, prognosis and expectance is very crucial for patients’ care, clinicians, and care-givers. For the three most frequent and recurrent mutations in the population (as shown in Figure 3), we are reasonably able to know what clinical course will be, what conditions we have to treat, and maybe, predict the prognosis. Unfortunately, a relatively small percentage of patients remains without diagnosis or does not fall in one of these three discrete phenotypic categories; most of them present neurological signs and symptoms variably associated revealing the nature of continuum spectrum of ATP1A3 disease. Nevertheless, for all patients, understanding the ultimate molecular mechanisms underlying the disruptions of ATP1A3 protein function is the goal to achieve new therapeutic approaches. In vitro modelling as well as animal models of disease increasingly phenotyping the human clinical condition are the promising framework where new effective treatment can be developed.
Acknowledgments
We wish to thank all families of our patients and AISEA onlus (Italian Association of Alternating Hemiplegia of Childhood) for their unconditional support.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Verret S, Steele JC. Alternating hemiplegia in childhood: a report of eight patients with complicated migraine beginning in infancy. Pediatrics. 1971;47(4):675–680.
2. Krägeloh I, Aicardi J. Alternating hemiplegia in infants: report of five cases. Dev Med Child Neurol. 1980;22(6):784–791. doi:10.1111/j.1469-8749.1980.tb03746.x
3. Bourgeois M, Aicardi J, Goutières F. Alternating hemiplegia of childhood. J Pediatr. 1993;122(5 Pt 1):673–679. doi:10.1016/S0022-3476(06)80003-X
4. Viollet L, Glusman G, Murphy KJ, et al. Alternating hemiplegia of childhood: retrospective genetic study and genotype-phenotype correlations in 187 subjects from the US AHCF registry. PLoS One. 2015;10(5):e0127045. doi:10.1371/journal.pone.0127045
5. Panagiotakaki E, Gobbi G, Neville B, et al. Evidence of a non-progressive course of alternating hemiplegia of childhood: study of a large cohort of children and adults. Brain. 2010;133(Pt 12):3598–3610. doi:10.1093/brain/awq295
6. Sweney MT, Silver K, Gerard-Blanluet M, et al. Alternating hemiplegia of childhood: early characteristics and evolution of a neurodevelopmental syndrome. Pediatrics. 2009;123(3):e534–e541. doi:10.1542/peds.2008-2027
7. Rosewich H, Sweney MT, DeBrosse S, et al. Research conference summary from the 2014 international task force on ATP1A3-related disorders. Neurol Genet. 2017;3(2):e139. doi:10.1212/NXG.0000000000000139
8. Heinzen EL, Swoboda KJ, Hitomi Y, et al. De novo mutations in ATP1A3 cause alternating hemiplegia of childhood. Nat Genet. 2012;44(9):1030–1034. doi:10.1038/ng.2358
9. Rosewich H, Thiele H, Ohlenbusch A, et al. Heterozygous de-novo mutations in ATP1A3 in patients with alternating hemiplegia of childhood: a whole-exome sequencing gene-identification study. Lancet Neurol. 2012;11(9):764–773. doi:10.1016/S1474-4422(12)70182-5
10. Ishii A, Saito Y, Mitsui J, et al. Identification of ATP1A3 mutations by exome sequencing as the cause of alternating hemiplegia of childhood in Japanese patients. PLoS One. 2013;8(2):e56120. doi:10.1371/journal.pone.0056120
11. de Carvalho Aguiar P, Sweadner KJ, Penniston JT, et al. Mutations in the Na+/K+ -ATPase alpha3 gene ATP1A3 are associated with rapid-onset dystonia parkinsonism. Neuron. 2004;43(2):169–175. doi:10.1016/j.neuron.2004.06.028
12. Heimer G, Sadaka Y, Israelian L, et al. CAOS-episodic cerebellar ataxia, areflexia, optic atrophy, and sensorineural hearing loss: a third allelic disorder of the ATP1A3 gene. J Child Neurol. 2015;30(13):1749–1756. doi:10.1177/0883073815579708
13. Demos MK, van Karnebeek CD, Ross CJ, et al. A novel recurrent mutation in ATP1A3 causes CAPOS syndrome. Orphanet J Rare Dis. 2014;9:15. doi:10.1186/1750-1172-9-15
14. Paciorkowski AR, McDaniel SS, Jansen LA, et al. Novel mutations in ATP1A3 associated with catastrophic early life epilepsy, episodic prolonged apnea, and postnatal microcephaly. Epilepsia. 2015;56(3):422–430. doi:10.1111/epi.12914
15. Marzin P, Mignot C, Dorison N, et al. Early-onset encephalopathy with paroxysmal movement disorders and epileptic seizures without hemiplegic attacks: about three children with novel ATP1A3 mutations. Brain Dev. 2018;40(9):768–774. doi:10.1016/j.braindev.2018.05.008
16. Dard R, Mignot C, Durr A, et al. Relapsing encephalopathy with cerebellar ataxia related to an ATP1A3 mutation. Dev Med Child Neurol. 2015;57(12):1183–1186. doi:10.1111/dmcn.12927
17. Sabouraud P, Riquet A, Spitz M-A, et al. Relapsing encephalopathy with cerebellar ataxia are caused by variants involving p.Arg756 in ATP1A3. Eur J Paediatr Neurol. 2019;23(3):448–455. doi:10.1016/j.ejpn.2019.02.004
18. Brashear A, Sweadner KJ, Cook JF, et al. ATP1A3-Related Neurologic Disorders. 2008 Feb 7 [Updated 2018 Feb 22]. In: Adam MP, Ardinger HH, Pagon RA, et al, editors. GeneReview® [Internet]. Seattle, WA: University of Washington, Seattle; 1993–2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK1115/.
19. Carecchio M, Zorzi G, Ragona F, Zibordi F, Nardocci N. ATP1A3-related disorders: an update. Eur J Paediatr Neurol. 2018;22(2):257–263. doi:10.1016/j.ejpn.2017.12.009
20. Heinzen EL, Arzimanoglou A, Brashear A, et al. Distinct neurological disorders with ATP1A3 mutations. Lancet Neurol. 2014;13(5):503–514. doi:10.1016/S1474-4422(14)70011-0
21. Anselm IA, Sweadner KJ, Gollamudi S, Ozelius LJ, Darras BT. Rapid-onset dystonia-parkinsonism in a child with a novel atp1a3 gene mutation. Neurology. 2009;73(5):400–401. doi:10.1212/WNL.0b013e3181b04acd
22. Kanemasa H, Fukai R, Sakai Y, et al. De novo p.Arg756Cys mutation of ATP1A3 causes an atypical form of alternating hemiplegia of childhood with prolonged paralysis and choreoathetosis. BMC Neurol. 2016;16:174. doi:10.1186/s12883-016-0680-6
23. Pittock SJ, Joyce C, O’Keane V, et al. Rapid-onset dystonia-parkinsonism: a clinical and genetic analysis of a new kindred. Neurology. 2000;55(7):991–995. doi:10.1212/WNL.55.7.991
24. Jaffer F, Fawcett K, Sims D, et al. Familial childhood-onset progressive cerebellar syndrome associated with the ATP1A3 mutation. Neurol Genet. 2017;3(2):e145. doi:10.1212/NXG.0000000000000145
25. Roubergue A, Roze E, Vuillaumier-Barrot S, et al. The multiple faces of the ATP1A3-related dystonic movement disorder. Mov Disord. 2013;28(10):1457–1459. doi:10.1002/mds.25396
26. Boelman C, Lagman-Bartolome AM, MacGregor DL, McCabe J, Logan WJ, Minassian BA. Identical ATP1A3 mutation causes alternating hemiplegia of childhood and rapid-onset dystonia parkinsonism phenotypes. Pediatr Neurol. 2014;51(6):850–853. doi:10.1016/j.pediatrneurol.2014.08.015
27. Rosewich H, Ohlenbusch A, Huppke P, et al. The expanding clinical and genetic spectrum of ATP1A3-related disorders. Neurology. 2014;82(11):945–955. doi:10.1212/WNL.0000000000000212
28. Sweney MT, Newcomb TM, Swoboda KJ. The expanding spectrum of neurological phenotypes in children with ATP1A3 mutations, alternating hemiplegia of childhood, rapid-onset dystonia-parkinsonism, CAPOS and beyond. Pediatr Neurol. 2015;52(1):56–64. doi:10.1016/j.pediatrneurol.2014.09.015
29. Jasien JM, Bonner M, D’alli R, et al. Cognitive, adaptive, and behavioral profiles and management of alternating hemiplegia of childhood. Develop Med Child Neurol. 2019;61(5):547–554. doi:10.1111/dmcn.2019.61.issue-5
30. Panagiotakaki E, De Grandis E, Stagnaro M, et al. Clinical profile of patients with ATP1A3 mutations in alternating hemiplegia of childhood-a study of 155 patients. Orphanet J Rare Dis. 2015;10:123. doi:10.1186/s13023-015-0335-5
31. Saito Y, Inui T, Sakakibara T, Sugai K, Sakuma H, Sasaki M. Evolution of hemiplegic attacks and epileptic seizures in alternating hemiplegia of childhood. Epilepsy Res. 2010;90:248–258. doi:10.1016/j.eplepsyres.2010.05.013
32. Uchitel J, Helseth A, Prange L, et al. The epileptology of alternating hemiplegia of childhood. Neurology. 2019;93(13):e1248–e1259. doi:10.1212/WNL.0000000000008159
33. Mikati MA, Kramer U, Zupanc ML, Shanahan RJ. Alternating hemiplegia of childhood: clinical manifestations and long-term outcome. Pediatr Neurol. 2000;23(2):134–141. doi:10.1016/S0887-8994(00)00157-0
34. Delorme C, Hainque E, Roze E. Alternating upper limb monoplegia due to ATP1A3 mutation. Pediatr Neurol. 2017;68:79–80. doi:10.1016/j.pediatrneurol.2016.12.001
35. Stagnaro M, Pisciotta L, Gherzi M, et al. ATP1A3 spectrum disorders: A video-documented history of 7 genetically confirmed early onset cases. Eur J Paediatr Neurol. 2018;22(2):264–271. doi:10.1016/j.ejpn.2018.01.010
36. Schirinzi T, Graziola F, Cusmai R, et al. ATP1A3-related epileptic encephalopathy responding to ketogenic diet. Brain Dev. 2018;40(5):433–438. doi:10.1016/j.braindev.2018.01.002
37. Sasaki M, Ishii A, Saito Y, et al. Genotype-phenotype correlations in alternating hemiplegia of childhood. Neurology. 2014;82(6):482–490. doi:10.1212/WNL.0000000000000102
38. Pereira P, Guerreiro A, Fonseca M, Halpern C, Pinto-Basto J, Monteiro JP. A distinct phenotype in a novel ATP1A3 mutation: connecting the two ends of a spectrum. Mov Disord Clin Pract. 2016;3(4):398–401. doi:10.1002/mdc3.12263
39. Termsarasab P, Yang AC, Frucht SJ. Intermediate phenotypes of ATP1A3 mutations: phenotype-genotype correlations. Tremor Other Hyperkinet Mov (N Y). 2015;5:336.
40. Andermann E, Andermann F, Silver K, Levin S, Arnold D. Benign familial nocturnal alternating hemiplegia of childhood. Neurology. 1994;44(10):1812–1814. doi:10.1212/WNL.44.10.1812
41. Chaves-Vischer V, Picard F, Andermann E, Dalla Bernardina B, Andermann F. Benign nocturnal alternating hemiplegia of childhood: six patients and long-term follow-up. Neurology. 2001;57(8):1491–1493. doi:10.1212/WNL.57.8.1491
42. Maas RPPWM, Kamsteeg E-J, Mangano S, et al. Benign nocturnal alternating hemiplegia of childhood: a clinical and nomenclatural reappraisal. Eur J Paediatr Neurol. 2018;22(6):1110–1117. doi:10.1016/j.ejpn.2018.07.012
43. Mangano S, Fontana A, Spitaleri C, Mangano GR. Benign nocturnal alternating hemiplegia of childhood: a new case with unusual findings. Brain Dev. 2014;36(5):408–410. doi:10.1016/j.braindev.2013.06.004
44. Sartori S, Vecchi M, Toldo I, Boniver C, Dalla Bernardina B, Maria Laverda A. Benign nocturnal alternating hemiplegia of childhood: the first clinical report with paroxysmal events home-video recordings. Mov Disord. 2008;23(11):1605–1608. doi:10.1002/mds.v23:11
45. Villéga F, Picard F, Espil-Taris C, Husson M, Michel V, Pedespan J-M. Benign nocturnal alternating hemiplegia of childhood: two cases with positive evolution. Brain Dev. 2011;33(6):525–529. doi:10.1016/j.braindev.2010.08.008
46. Wagener-Schimmel LJJC, Nicolai J. Child neurology: benign nocturnal alternating hemiplegia of childhood. Neurology. 2012;79(18):e161–e163. doi:10.1212/WNL.0b013e318271f7a6
47. Mercer RW, Biemesderfer D, Bliss DP
48. Bøttger P, Tracz Z, Heuck A, Nissen P, Romero-Ramos M, Lykke-Hartmann K. Distribution of Na/K-ATPase alpha 3 isoform, a sodium-potassium P-type pump associated with rapid-onset of dystonia parkinsonism (RDP) in the adult mouse brain. J Comp Neurol. 2011;519(2):376–404. doi:10.1002/cne.v519.2
49. Ikeda K, Satake S, Onaka T, et al. Enhanced inhibitory neurotransmission in the cerebellar cortex of Atp1a3-deficient heterozygous mice. J Physiol. 2013;591(13):3433–3449. doi:10.1113/jphysiol.2012.247817
50. Holm TH, Lykke-Hartmann K. Insights into the pathology of the α3 Na(+)/K(+)-ATPase ion pump in neurological disorders; lessons from animal models. Front Physiol. 2016;7:209. doi:10.3389/fphys.2016.00209
51. Skou JC. The influence of some cations on an adenosine triphosphatase from peripheral nerves. Biochim Biophys Acta. 1957;23(2):394–401. doi:10.1016/0006-3002(57)90343-8
52. Pivovarov AS, Calahorro F, Walker RJ. Na+/K+-pump and neurotransmitter membrane receptors. Invert Neurosci. 2018;19(1):1. doi:10.1007/s10158-018-0221-7
53. Pirahanchi Y, Aeddula NR. Physiology, Sodium Potassium Pump (Na+ K+ Pump) [Updated 2019 Jan 21]. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537088/.
54. Blanco-Arias P, Einholm AP, Mamsa H, et al. A C-terminal mutation of ATP1A3 underscores the crucial role of sodium affinity in the pathophysiology of rapid-onset dystonia-parkinsonism. Hum Mol Genet. 2009;18(13):2370–2377. doi:10.1093/hmg/ddp170
55. McGrail KM, Phillips JM, Sweadner KJ. Immunofluorescent localization of three Na,K-ATPase isozymes in the rat central nervous system: both neurons and glia can express more than one Na,K-ATPase. J Neurosci. 1991;11(2):381–391. doi:10.1523/JNEUROSCI.11-02-00381.1991
56. Crambert G, Hasler U, Beggah AT, et al. Transport and pharmacological properties of nine different human Na, K-ATPase isozymes. J Biol Chem. 2000;275(3):1976–1986. doi:10.1074/jbc.275.3.1976
57. Holm R, Toustrup-Jensen MS, Einholm AP, Schack VR, Andersen JP, Vilsen B. Neurological disease mutations of α3 Na+,K+-ATPase: structural and functional perspectives and rescue of compromised function. Biochim Biophys Acta. 2016;1857(11):1807–1828. doi:10.1016/j.bbabio.2016.08.009
58. Clausen MV, Hilbers F, Poulsen H. The structure and function of the Na,K-ATPase isoforms in health and disease. Front Physiol. 2017;8:371.
59. Kanai R, Ogawa H, Vilsen B, Cornelius F, Toyoshima C. Crystal structure of a Na+-bound Na+,K+-ATPase preceding the E1P state. Nature. 2013;502(7470):201–206. doi:10.1038/nature12578
60. Post RL, Hegyvary C, Kume S. Activation by adenosine triphosphate in the phosphorylation kinetics of sodium and potassium ion transport adenosine triphosphatase. J Biol Chem. 1972;247(20):6530–6540.
61. Morth JP, Pedersen BP, Toustrup-Jensen MS, et al. Crystal structure of the sodium-potassium pump. Nature. 2007;450(7172):1043–1049. doi:10.1038/nature06419
62. Ogawa H, Shinoda T, Cornelius F, Toyoshima C. Crystal structure of the sodium-potassium pump (Na+,K+-ATPase) with bound potassium and ouabain. Proc Natl Acad Sci USA. 2009;106(33):13742–13747. doi:10.1073/pnas.0907054106
63. Shinoda T, Ogawa H, Cornelius F, Toyoshima C. Crystal structure of the sodium-potassium pump at 2.4 A resolution. Nature. 2009;459(7245):446–450. doi:10.1038/nature07939
64. Laursen M, Yatime L, Nissen P, Fedosova NU. Crystal structure of the high-affinity Na+K+-ATPase-ouabain complex with Mg2+ bound in the cation binding site. Proc Natl Acad Sci USA. 2013;110(27):10958–10963. doi:10.1073/pnas.1222308110
65. Geering K. The functional role of beta subunits in oligomeric P-type ATPases. J Bioenerg Biomembr. 2001;33(5):425–438. doi:10.1023/A:1010623724749
66. Geering K. Functional roles of Na,K-ATPase subunits. Curr Opin Nephrol Hypertens. 2008;17(5):526–532. doi:10.1097/MNH.0b013e3283036cbf
67. Reinhard L, Tidow H, Clausen MJ, Nissen P. Na(+),K(+)-ATPase as a docking station: protein-protein complexes of the Na(+),K(+)-ATPase. Cell Mol Life Sci. 2013;70(2):205–222. doi:10.1007/s00018-012-1039-9
68. Blom H, Rönnlund D, Scott L, et al. Spatial distribution of Na+-K+-ATPase in dendritic spines dissected by nanoscale superresolution STED microscopy. BMC Neurosci. 2011;12:16. doi:10.1186/1471-2202-12-16
69. Weigand KM, Messchaert M, Swarts HGP, Russel FGM, Koenderink JB. Alternating Hemiplegia of Childhood mutations have a differential effect on Na(+),K(+)-ATPase activity and ouabain binding. Biochim Biophys Acta. 2014;1842(7):1010–1016. doi:10.1016/j.bbadis.2014.03.002
70. Einholm AP, Toustrup-Jensen MS, Holm R, Andersen JP, Vilsen B. The rapid-onset dystonia parkinsonism mutation D923N of the Na+, K+-ATPase alpha3 isoform disrupts Na+ interaction at the third Na+ site. J Biol Chem. 2010;285(34):26245–26254. doi:10.1074/jbc.M110.123976
71. Clapcote SJ, Duffy S, Xie G, et al. Mutation I810N in the alpha3 isoform of Na+,K+-ATPase causes impairments in the sodium pump and hyperexcitability in the CNS. Proc Natl Acad Sci USA. 2009;106(33):14085–14090. doi:10.1073/pnas.0904817106
72. Kanavakis E, Xaidara A, Papathanasiou-Klontza D, Papadimitriou A, Velentza S, Youroukos S. Alternating hemiplegia of childhood: a syndrome inherited with an autosomal dominant trait. Dev Med Child Neurol. 2003;45:833–836. doi:10.1111/j.1469-8749.2003.tb00899.x
73. Hully M, Ropars J, Hubert L, et al. Mosaicism in ATP1A3-related disorders: not just a theoretical risk. Neurogenetics. 2017;18:23–28. doi:10.1007/s10048-016-0498-9
74. Yang X, Gao H, Zhang J, et al. ATP1A3 mutations and genotype-phenotype correlation of alternating hemiplegia of childhood in Chinese patients. PLoS One. 2014;9(5):e97274. doi:10.1371/journal.pone.0097274
75. Rodacker V, Toustrup-Jensen M, Vilsen B. Mutations Phe785Leu and Thr618Met in Na+,K+-ATPase, associated with familial rapid-onset dystonia parkinsonism, interfere with Na+ interaction by distinct mechanisms. J Biol Chem. 2006;281(27):18539–18548. doi:10.1074/jbc.M601780200
76. Brashear A, Mulholland GK, Zheng QH, Farlow MR, Siemers ER, Hutchins GD. PET imaging of the pre-synaptic dopamine uptake sites in rapid-onset dystonia-parkinsonism (RDP). Mov Disord. 1999;14(1):132–137. doi:10.1002/1531-8257(199901)14:1<132::AID-MDS1022>3.0.CO;2-J
77. Simmons CQ, Thompson CH, Cawthon BE, et al. Direct evidence of impaired neuronal Na/K-ATPase pump function in alternating hemiplegia of childhood. Neurobiol Dis. 2018;115:29–38. doi:10.1016/j.nbd.2018.03.009
78. Arystarkhova E, Haq IU, Luebbert T, et al. Factors in the disease severity of ATP1A3 mutations: impairment, misfolding, and allele competition. Neurobiol Dis. 2019;132:104577. doi:10.1016/j.nbd.2019.104577
79. Moseley AE, Williams MT, Schaefer TL, et al. Deficiency in Na,K-ATPase α isoform genes alters spatial learning, motor activity, and anxiety in mice. J Neurosci. 2007;27(3):616–626. doi:10.1523/JNEUROSCI.4464-06.2007
80. DeAndrade MP, Yokoi F, vanGroen T, Lingrel JB, Li Y. Characterization of Atp1a3 mutant mice as a model of rapid- onset dystonia with parkinsonism. Behav Brain Res. 2011;216(2):659–665.
81. Kirshenbaum GS, Clapcote SJ, Duffy S, et al. Mania-like behavior induced by genetic dysfunction of the neuron-specific Na+,K+-ATPase alpha3 sodium pump. Proc Natl Acad Sci U S A. 2012;109(6):2174.
82. Hunanyan AS, Fainberg NA, Linabarger M, et al. Knock-in mouse model of alternating hemiplegia of childhood: behavioral and electrophysiologic characterization. Epilepsia. 2015;56(1):82–93. doi:10.1111/epi.12878
83. Helseth AR, Hunanyan AS, Adil S, et al. Novel E815K knock-in mouse model of alternating hemiplegia of childhood. Neurobiol Dis. 2018;119:100–112. doi:10.1016/j.nbd.2018.07.028
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.