Back to Journals » Cancer Management and Research » Volume 14
Allogeneic Stem Cell Transplantation with Sequential Melphalan-Based Conditioning in AML: Residual Morphological Blast Count Determines the Risk of Relapse
Authors Sockel K, Stölzel F ![]() , Hönl F, Baldauf H, Röllig C
, Hönl F, Baldauf H, Röllig C ![]() , Wermke M, von Bonin M, Teipel R, Link-Rachner C, Brandt K, Kroschinsky F
, Wermke M, von Bonin M, Teipel R, Link-Rachner C, Brandt K, Kroschinsky F ![]() , Hänel M, Morgner A, Klesse C, Ehninger G, Platzbecker U, Bornhäuser M
, Hänel M, Morgner A, Klesse C, Ehninger G, Platzbecker U, Bornhäuser M ![]() , Schetelig J, Middeke JM
, Schetelig J, Middeke JM
Received 19 September 2021
Accepted for publication 23 December 2021
Published 15 February 2022 Volume 2022:14 Pages 547—559
DOI https://doi.org/10.2147/CMAR.S339846
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Ahmet Emre Eşkazan
Katja Sockel,1 Friedrich Stölzel,1 Franziska Hönl,1 Henning Baldauf,2 Christoph Röllig,1 Martin Wermke,1 Malte von Bonin,1 Raphael Teipel,1 Cornelia Link-Rachner,1 Kalina Brandt,1 Frank Kroschinsky,1 Mathias Hänel,3 Anke Morgner,3 Christian Klesse,2 Gerhard Ehninger,1 Uwe Platzbecker,4 Martin Bornhäuser,1 Johannes Schetelig,1,2,* Jan Moritz Middeke1,*
1Medical Clinic and Policlinic I, University Hospital Carl Gustav Carus and Medical Faculty of the TU Dresden, Dresden, Germany; 2Clinical Trials Unit, DKMS, Dresden, Germany; 3Department of Medicine III, Chemnitz Hospital, Chemnitz, Germany; 4Department of Hematology, Cellular Therapy and Hemostaseology, Leipzig University Hospital, Leipzig, Germany
*These authors contributed equally to this work
Correspondence: Jan Moritz Middeke, Medical Clinic and Policlinic I, University Hospital Carl Gustav Carus and Medical Faculty of the TU Dresden, Fetscherstr. 74, Dresden, 01307, Germany, Tel +49-0351-458-15603, Fax +49-0351-458-4373, Email [email protected]
Introduction: Allogeneic hematopoietic cell transplantation (HCT) during chemotherapy-induced aplasia may offer long-term survival in acute myeloid leukemia (AML) with otherwise poor prognosis including ELN adverse risk, relapsed or refractory disease. However, the value of residual morphologic disease prior HCT in this context has not been conclusively settled until yet. Therefore, we aimed to investigate variables predicting outcome in this unique setting of sequential conditioning therapy, with a focus on pretreatment morphologic blast count. In contrast to the most popular FLAMSA-RIC protocol, we used a melphalan-based conditioning regimen during aplasia.
Methods: We retrospectively analyzed data from 173 AML patients who underwent a sequential melphalan-based conditioning therapy between 2003 and 2015 at our centre. All patients participated either in the prospective Phase 2 BRIDGE trial (NCT01295307), the Phase 3 AML2003 study (NCT00180102) or were treated according to this protocol and underwent allogeneic HCT after melphalan-based conditioning in treatment-induced aplasia.
Results: Median bone marrow blast count prior to conditioning was 10% (range, 0– 96%). Four year probabilities of EFS and OS were 34% (95% CI, 28– 43%) and 43% (95% CI, 36– 52%), respectively. In multivariate analysis, blast count > 20% was associated with worse EFS (HR = 1.93; p = 0.009) and OS (HR = 1.80; p = 0.026). This effect was not significant anymore for HCT during 1st line therapy.
Conclusion: Allogeneic HCT in aplasia with a melphalan-based conditioning regimen has the potential to cure a subset of adverse risk AML patients, even with persistent morphological disease prior HCT. However, a high pre-transplant blast count still indicates patients with a dismal prognosis, especially in the relapsed patient group, for whom post-transplant strategies should be considered to further optimize post HCT outcome.
Keywords: acute myeloid leukemia, ELN high risk, AML relapse/refractory, early allogeneic transplantation in aplasia, blast count, melphalan-based conditioning, sequential conditioning
Introduction
Despite recent progress in the molecular characterization of AML and the resulting clinical development for individualized therapeutic approaches, the prognosis of ELN adverse risk AML remains poor with frequent primary induction failures and relapse rates of 70–90%.1 The chance for long-term survival in relapsed patients is only around 10%.2–4 Allogeneic hematopoietic cell transplantation (HCT) represents the most potent anti-leukemic treatment for this unfavorable patient group. However, less than half of the relapsed/refractory patients will proceed to allogeneic HCT5,6 due to treatment-related morbidity, absence of a suitable donor or inability to achieve any kind of remission before HCT.
The value of allogeneic HCT for AML patients who are not in complete remission (CR) before transplantation is still a matter of debate, as long-term survival rates in patients undergoing classical allogeneic HCT without CR are poor at approximately 10–30%.7,8 Therefore, salvage chemotherapy prior to HCT is generally recommended to achieve blast reduction or ideally blast clearance. But what about patients who will unlikely respond to salvage chemotherapy attempts due to their unfavorable genetic characteristics? In general, only 50% of patients will achieve complete remission after intensive chemotherapy,9,10 with increased risk of treatment-related morbidity and mortality, leaving a part of them ineligible for a curative allogeneic HSCT procedure. In addition, repeated application of salvage courses could select chemo-resistant leukemia clones.
Several studies indicate that allogeneic HCT from chemotherapy-induced aplasia (so-called “sequential transplantation”) could be a promising approach to offer this curative treatment strategy to patients who have not yet achieved a complete remission and would therefore not be considered for a standard curative transplant concept.11–14 However, the impact of residual bone marrow blasts prior to early HCT in aplasia has not been clearly defined yet.
Therefore, we aimed to investigate the impact of pretransplant variables predicting outcome in this specific setup of allogeneic HCT in aplasia for patients with ELN high-risk or refractory/relapsed AML, with a focus on residual morphologic blast count prior HCT.
Materials and Methods
Study Design and Patient Eligibility
This retrospective study included all AML patients with either high ELN 2010 risk at initial diagnosis (irrespective of a documented CR) or poor early response after first induction therapy (IT), as well as primary induction failure or even relapse after standard therapy, who participated either in the prospective phase 2 BRIDGE trial (NCT01295307),15 in the phase 3 AML2003 study (NCT00180102)16 or were treated according to the AML 2003 protocol. All patients underwent allogeneic HCT after melphalan-based conditioning in treatment-induced aplasia between January, 1, 2003 and May, 1, 2015 at the University Hospital Dresden, a tertiary care center with a large transplant program.
The AML2003 study was a randomized 1st line therapy study with a genetic-based risk stratification. All patients received at least one induction chemotherapy with daunorubicin (60 mg/m2 days 3–5) and cytarabine (100 mg/m2 days 1–7). Patients with adverse risk AML were randomized to the control arm (HCT in 1st CR) or the experimental arm (early HCT in aplasia after the 1st or 2nd IT cycle without previously documented CR), while the melphalan-based conditioning regimen was only applied to patients in the experimental arm (details see “transplant procedure”). The BRIDGE trial, on the other hand, investigated a salvage therapy approach for relapsed/refractory AML patients. Refractory disease was defined as ⩾5% blasts in the bone marrow (BM) after the 2 induction cycles or no reduction in BM blasts at day +15 after 1st induction therapy. All patients received at least one cycle of salvage therapy according to the CLARA protocol (clofarabine 30 mg/m2 day1-5 and cytarabine 1 g/m2 day 1–5). All patients within the BRIDGE trial received a melphalan-based conditioning regimen.
A bone marrow assessment within 30 days prior to transplantation was required for inclusion into the analysis. Patients with second allogeneic HCT or missing written informed consent for analyses of clinical data were excluded. Out of 228 poor risk AML patients 173 met the eligibility criteria and could be analyzed.
Morphological Evaluation
The most recent bone marrow assessment prior to the start of conditioning therapy was evaluated. In general, the blast count was assessed from bone marrow aspirates. The average blast count was evaluated under the microscope by two experienced medical technical assistants as well as two haematologists with long experience in cytomorphological AML diagnostics. At least 200 cells were counted. If no spicules were present, the blast count was evaluated via bone marrow biopsy by two experienced hematopathologists.
Transplant Procedures
All patients received a dose-reduced melphalan-based conditioning regimen with either fludarabine (30 mg/m2, day - 6 to day - 2) and melphalan (150 mg/m2 on day - 2) according to the AML2003 trial protocol16 or clofarabine (30 mg/m2, day −6 to day - 3) and melphalan (140 mg/m2 on day - 2) according to the BRIDGE trial protocol.15 Anti-thymocyte globulin (ATG) was given to all patients with an unrelated donor within the AML 2003 study, while patients participating in the BRIDGE trial only received ATG in case of a partially mismatched donor. HLA compatibility of patient and donor was assessed at the maximum level of available HLA typing (4-digit PCR or sequence-based typing results). Graft versus Host Disease (GVHD) prophylaxis consisted of a calcineurin inhibitor in combination with short-course methotrexate or mycophenolate mofetil, while posttransplant-cyclophosphamide was used in haploidentical transplantations.
Definitions
The remission status prior to HCT and cytogenetic risk group was defined according to the ELN 2010 recommendations.17 Grading of acute and chronic graft versus host disease (GVHD) was performed according to consensus criteria.18,19
Statistical Analysis
Data from 173 patients meeting eligibility criteria were included in the analyses. Primary objective of the study was to investigate variables, including residual bone marrow blast count, predicting event-free survival (EFS) – with relapse/progression or death as events, overall survival (OS), cumulative incidence of relapse (CIR) and non-relapse-mortality (NRM). All time-dependent events were calculated from time of allogeneic transplantation. Relapse and NRM were considered as competing events. The cumulative incidences of acute GVHD and chronic GVHD were also assessed, with death considered as competing event.
Survival rates and cumulative incidences at different time intervals were calculated using Kaplan Meier estimators and cumulative incidence estimators. Univariate analyses were performed by means of Log rank test for EFS and OS and score test of univariate cause-specific Cox models for the competing risk outcomes. The bone marrow blast count was modeled a priori in 3 categories in analogue to common classification systems (<5%, 5–20% and ≥20%). To analyze the continuous effect of blast count on EFS and CIR, splines-based hazard ratio (HR) curves were applied. Multivariate analyses were performed by Cox regression models, adjusted for bone marrow blast count, age, Karnofsky performance status, AML type, genetic risk according to ELN 2010, treatment line, conditioning regimen and donor type. Competing events were analyzed by cause-specific Cox models. A p-value <0.05 was considered to indicate statistical significance without correction for multiple testing.
Results
Patient Characteristics and Transplant Characteristic
Data from 173 patients were evaluable. Median patient age was 56 years (range, 17 to 75 years). Half of the patients had a pre-HCT Karnofsky score less than 90%. Sixty-one percent of the patients suffered from de novo AML, 30% had secondary AML and 9% treatment related acute leukemia (tAML). Detailed patient characteristics are listed in Table 1.
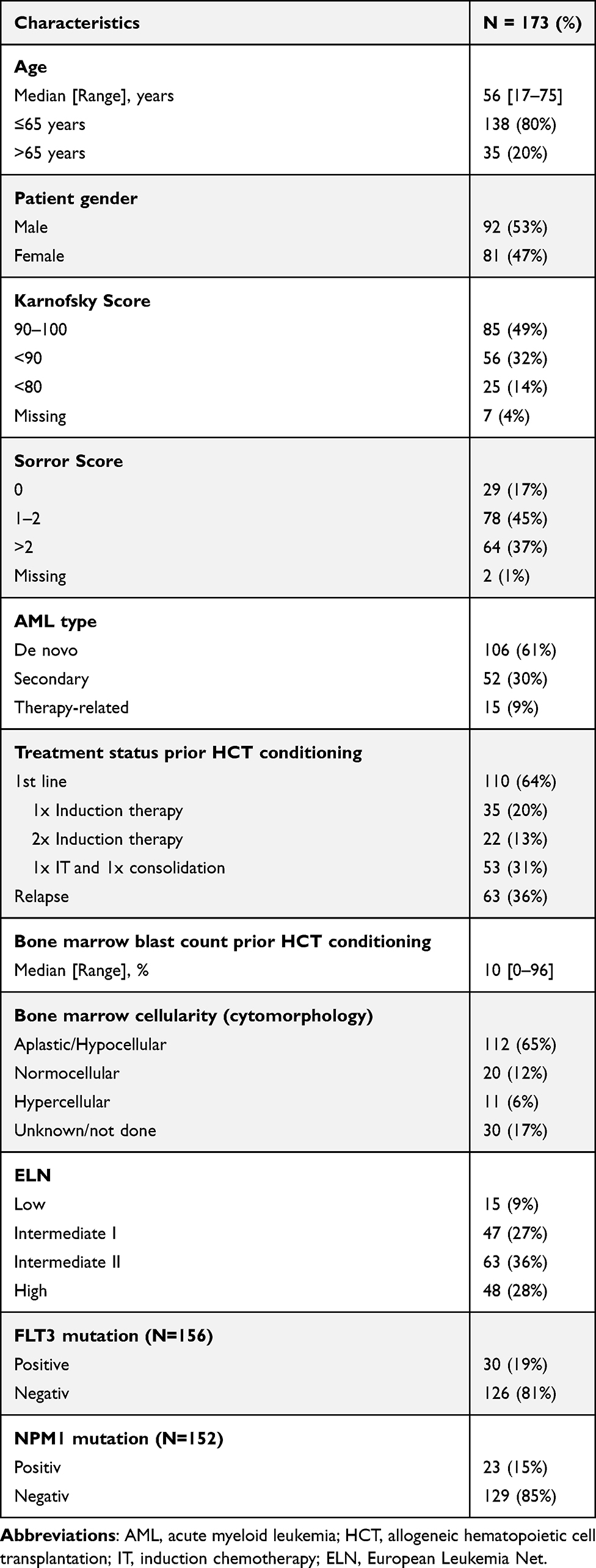 |
Table 1 Patient Characteristics |
The conditioning regimen consisted of Fludarabine/Melphalan (Flu/Mel) in 140 (81%) patients and Clofarabine/Melphalan (Clo/Mel) in 33 (19%) patients. Anti-thymocyte globulin was given to 70 patients (41%). Most patients received peripheral blood stem cells, while 15 patients (9%) received bone marrow stem cells. GVHD prophylaxis was cyclosporin A-based in the majority of patients (88%), in 8% tacrolimus-based and only 4% received alternative prophylaxis regimen. Donor types included 40 matched siblings (23%), 82 matched unrelated (47%), 34 (20%) partially matched unrelated and 17 haploidentical donors (10%).
Treatment status and blast count at HCT
Allogeneic HCT was part of the first-line treatment in 64% of the patients, while 36% suffered from relapsed disease. In the latter group, 27 patients (43%) had experienced relapse within the first six months after first CR. First-line treatment consisted of either one or two cycles of classic 7+3 induction with cytarabine and daunorubicin (DA) or one cycle of DA followed by a high-dose cytarabine containing regimen.
The median bone marrow blast count prior to allogeneic HCT was 10% (range, 0–96%) with 33% of patients having a blast count <5%, 33% of patients with a blast count of 5–20% and 27% of patients with a blast count greater than 20%. Bone marrow evaluation was done median 10 days before allogeneic HCT (range 4–30 days before HCT). Bone marrow cellularity was either aplastic or hypocellular in the majority of patients (n = 112; 64%) and only 31 patients (18%) had a normo- or hypercellular marrow.
GVHD
The cumulative incidences of acute GVHD of grade II–IV and grade III–IV at day +100 were 42% (95% CI, 35–50%) and 22% (95% CI, 15–28%), respectively. The cumulative incidences of chronic GVHD (limited or extensive) or extensive chronic GVHD at 4 years post-transplantation were 31% (95% CI, 24–39%) and 21% (95% CI, 14–28%), respectively.
Survival, Relapse and TRM
The median follow-up time from transplantation was 4.3 years (range, 0.1–11 years). At four years, the probabilities of OS and EFS were 43% (95% CI, 36–52%) and 34% (95% CI, 28–43%), respectively (Figure 1).
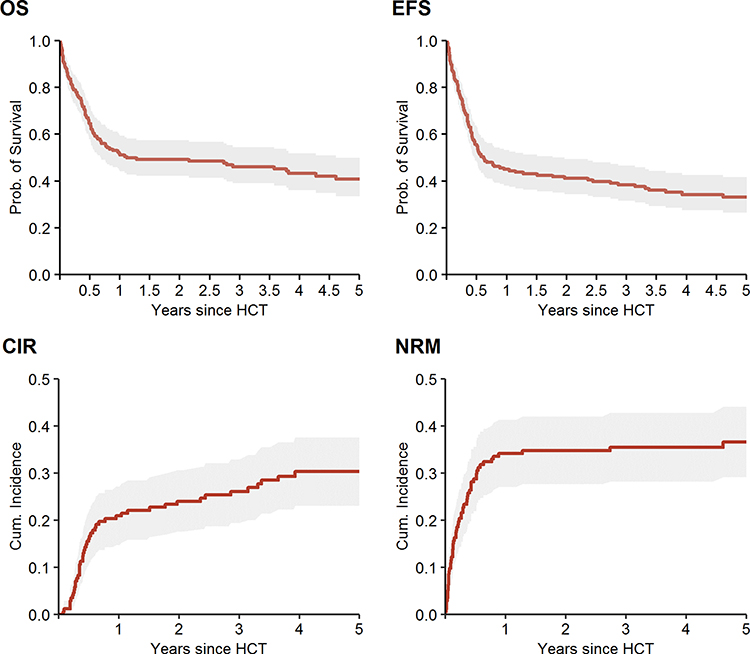 |
Figure 1 OS, EFS, CIR and NRM for the entire cohort. Abbreviations: OS, overall survival; EFS, event-free survival; CIR, cumulative incidence of relapse; NRM, non-relapse mortality; Prob., probability; HCT, allogeneic hematopoietic cell transplantation. |
The 4 year CIR was 30% (95% CI, 23–38%) and the 4 year NRM 36% (95% CI, 28–43%). Main causes of NRM were infectious complications (n = 33; 19%), GVHD (n = 14; 8%) and bleeding (n = 3; 3%). The median time to relapse following HCT was 5 months (range, 1–47).
Multivariate Analysis
In multivariate analysis for EFS, a high blast count >20% vs <5% (HR = 1.93; p = 0.009) and increasing age (HR 1.19; p = 0.040) were significant adverse risk factors. Overall survival (OS) was negatively impacted by a high blast count >20% vs blast count <5% (HR 1.8; p = 0.026), increasing age (HR 1.26; p = 0.012) and tAML vs de novo AML (HR 2.1; p = 0.039). Complete results of multivariate analyses are summarized in Table 2.
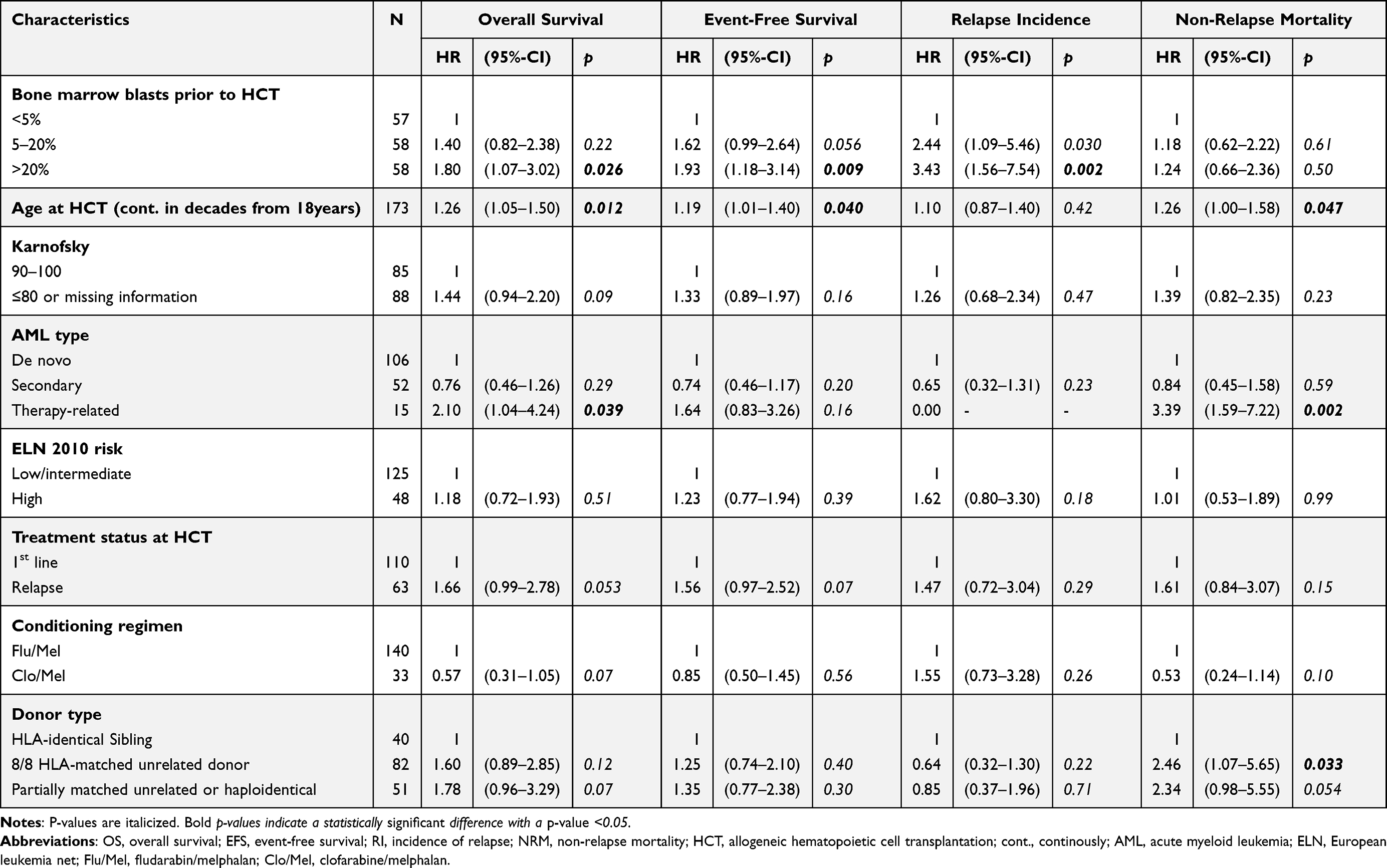 |
Table 2 Multivariate Analysis for Overall Survival, Event-Free Survival, Relapse Incidence and Non-Relapse Mortality |
Impact of Blast Count Prior to HCT
The pretransplant bone marrow blast count impacted patient outcome significantly (Figure 2). The 4 year EFS and OS was 46% (95% CI, 34–62%) and 54% (95% CI, 42–69%) in patients with less than 5% blasts, 30% (95% CI, 20–45%) and 40% (95% CI, 28–57%) in patients with 5–20% blasts and only 27% (95% CI, 17–42%) and 36% (95% CI, 25–52%) in patients with more than 20% blasts, respectively.
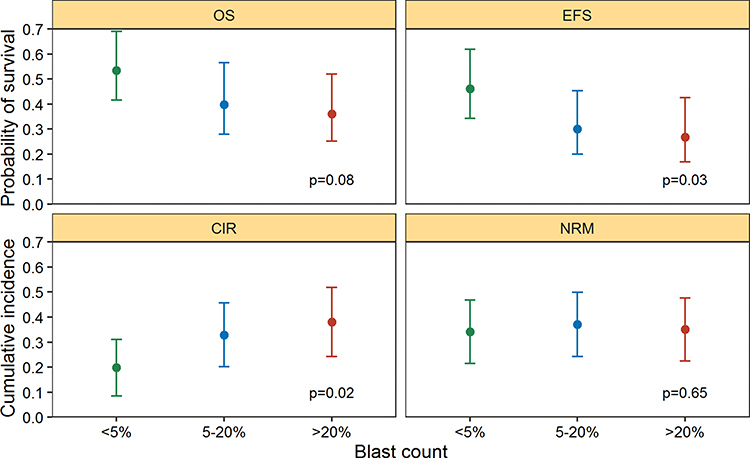 |
Figure 2 Four year point estimator of treatment outcome by pretransplant bone marrow blast count. The dots display the point estimates, whereas the bars display the corresponding 95% confidence intervals. The p values represent the Log rank test for OS and EFS and the score test of univariate cause-specific Cox models for CIR and NRM. Abbreviations: OS, overall Survival; EFS, event-free survival; CIR, cumulative incidence of relapse; NRM, non-relapse mortality. |
To investigate the impact of the residual blasts count on EFS and CIR the hazard ratio was analyzed as a continuous variable, adjusted for relevant covariates (Figure 3). While the HR of EFS rises almost linearly with increasing blast counts up to 20%, the curve starts to flatten from 20%, indicating that a blast count greater than 20% has no additional detrimental impact on EFS. In contrast, the continuous HR for CIR increased almost linearly.
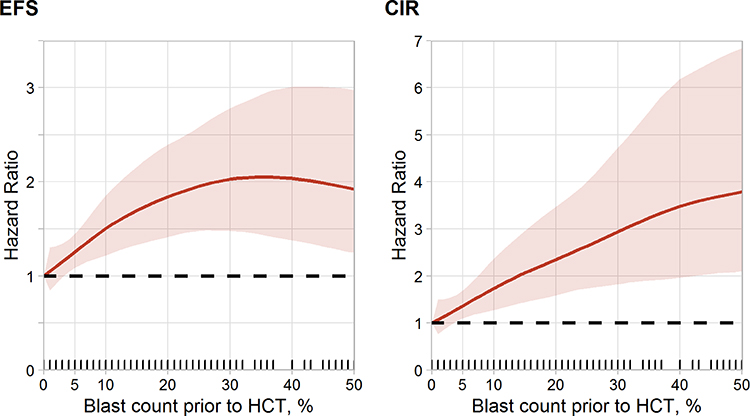 |
Figure 3 Effect of bone marrow blast count prior to HCT on event-free survival and on incidence of relapse. The red curve displays the smoothed spline-based hazard ratio of the dependence of the bone marrow blast count prior to HCT on the all-time risk of relapse or death (left panel) and the all-time risk of relapse (right panel). The hazard ratio is adjusted for age, Karnofsky performance status, AML type, ELN risk, treatment status at HCT, conditioning and donor type. The ribbon represent the pointwise 90% confidence intervals of the hazard ratios. The small lines on x-axis display the individual blast counts of patients having blast counts of 50% at most. Abbreviation: EFS, event-free survival; CIR, cumulative incidence of relapse; HCT, allogeneic hematopoietic cell transplantation. |
Notably, the impact of residual blast counts on the risk of relapse, EFS and OS was more pronounced (see Figure 4) for relapsed patients than for patients who underwent allogeneic HCT during 1st line therapy (ELN adverse risk, poor early response after 1st IT or primary refractoriness). This was indicated by interaction tests for a blast count greater than 20% and treatment status (p = 0.045 for EFS, p = 0.09 for OS, p = 0.07 for the risk of relapse, and p = 0.3 for NRM).
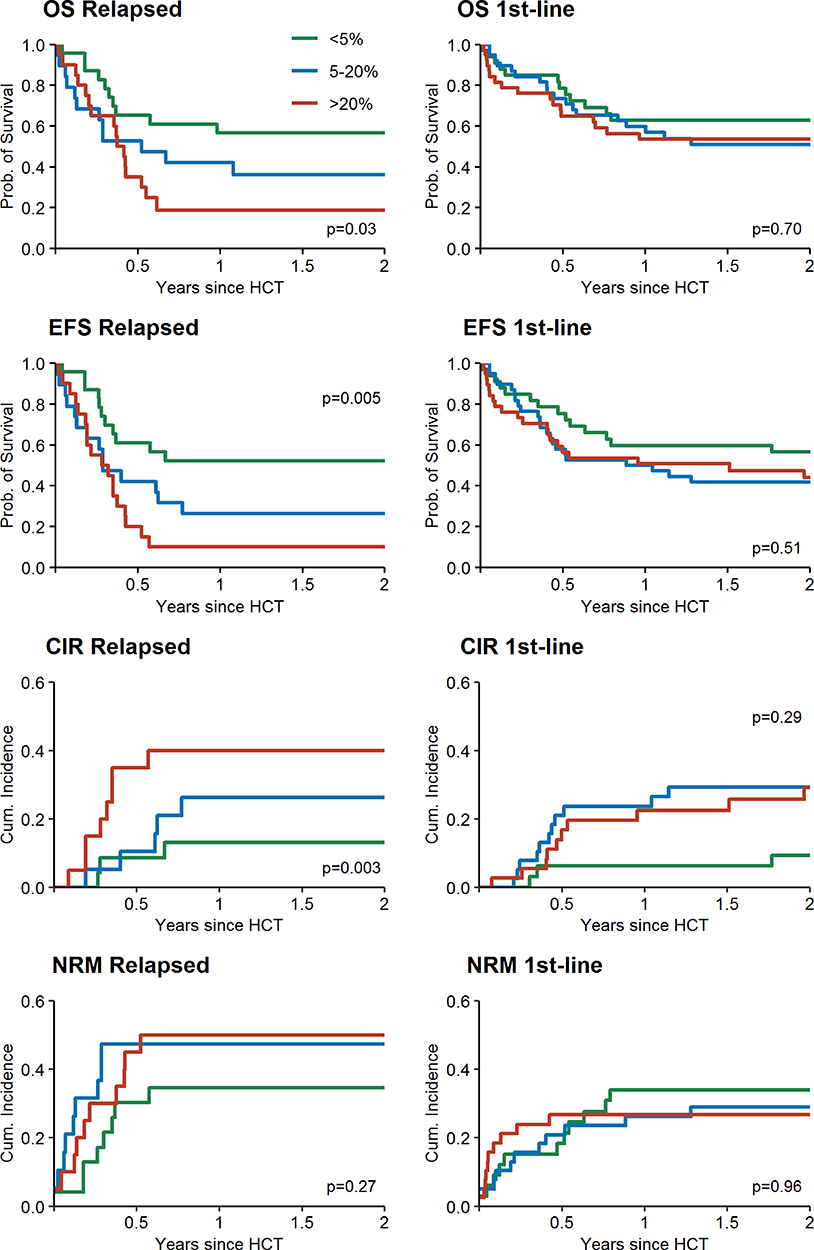 |
Figure 4 OS, EFS, CIR and NRM for relapsed patients (left side) and first-line patients (right side). Abbreviations: OS, overall survival; EFS, event-free survival; CIR, cumulative incidence of relapse; NRM, non-relapse mortality; Prob., probability; HCT, allogeneic hematopoietic cell transplantation. |
Discussion
Allogeneic stem cell transplantation represents the only curative treatment strategy for poor risk AML including ELN high-risk disease, poor early response, induction failure or relapse.9,20 Whether the induction of complete remission prior HCT by induction- or salvage chemotherapy is superior to a sequential conditioning approach from aplasia (without documented CR) is a matter of debate. While patients who survived salvage treatment and achieved a complete remission may benefit from remission induction chemotherapy, patients who do not achieve at least a morphological blast-free marrow may simply accumulate toxicity by multiple salvage approaches.
We and others have previously published promising results for early HCT during chemotherapy-induced aplasia, offering this curative treatment approach to patients who might otherwise not proceed to allogeneic HCT due to lack of remission prior HCT.11–14,21 The most popular regimen in this context is the classical FLAMSA-RIC regimen - a sequential treatment approach consisting of a cytoreductive chemotherapy with fludarabine, cytarabine and amsacrine (FLAMSA) followed by a reduced intensity conditioning (RIC), containing 4 Gy TBI and high dose cyclophosphamide. Reported 4-year OS rates range from 32% in the subgroup of relapsed/refractory AML patients13 up to 72.7% for high-risk AML in first CR.22 Few variations of the classical FLAMSA-RIC regimen were established, using busulfan or treosulfan instead of TBI,23,24 since retrospective studies suggested that the addition of low-dose TBI in the RIC context did not improve outcomes.25
In contrast to the above-mentioned protocols, we used a melphalan-based RIC-conditioning regimen, given the fact that melphalan-based regimens are well known for their good disease control and manageable toxicities26. These properties represent a promising prerequisite in the context of sequential allogeneic HCT, where some of the patients are still dealing with toxic effects of the preceding intensive chemotherapy and many of them are characterized by an aplastic bone marrow. Another group27 has currently published data using melphalan in the context of sequential HCT. In their approach, however, a single melphalan infusion was administered in median 5 days (1–18) before start of the remaining conditioning regimen.
We could demonstrate a good long-term survival in this unfavorable risk group after transplantation in aplasia with an OS rate of 44% at 4 years (95% CI, 35% to 51%). These results are within the upper level of previously published data in a conventional allogeneic HCT setting with myeloablative (MAC) conditioning, where 5-year OS rates of 19–42% have been reported for ELN high-risk patients in CR, primary refractory or relapsed patients.28–30
Considering the median age of 56 years in our patient cohort (representing the standard patient group for whom MAC conditioning is usually considered), our results raise the question whether MAC regimen is really necessary in the younger poor risk AML group or whether early allogeneic HCT in aplasia with a dose reduced conditioning might be more appropriate. A similar assumption was stated recently by Rodríguez-Arbolí et al,31 who analyzed a total of 1018 active relapsed/refractory AML patients between 18 and 50 years within a large EBMT registry data analysis, concluding that FLAMSA-RIC may be more beneficial than MAC conditioning in terms of similar 2-year RFS but lower NRM in patients with active relapsed/refractory AML.
Of note, Rodriguez-Arboli et al reported a very low 2-year NRM of 7% in the FLAMSA-RIC group – however, the young median age of 39 years must be taken into account.31 Higher NRM rates were described by Schmid et al13 with a 1-year NRM of 27%. Similar NRM rates were published by Craddock et al,32 who used a modified FLAMSA-Bu regimen and by Sheth et al23 who reported a 2-year NRM of 25% (median age 52 years). In our cohort, we observed a 4-year NRM of 36% among patients with a median age of 56 years. This was mainly due to infectious complications, especially in the early course after transplantation, highlighting a potential risk of the long neutropenic period between aplasia-inducing chemotherapy and transplantation. Further improvements especially in the selection and timing of the preceding aplasia-inducing chemotherapy are warranted. Nevertheless, the high NRM highlights the fragility of this patient population, indicating that additional chemotherapy attempts to achieve remission prior HCT will unlikely contribute to improved survival.
Multivariate analysis for overall survival and event free survival revealed an increased blast count as a strong predictor for poor outcome. The association between lower blast counts before HCT and higher survival rates has been described by other investigators.30,33,34 Notably, some retrospective studies indicate that the blast count in the HCT setting during aplasia may not be as significant as in the conventional transplantation scheme. In the publication of Stoelzel et al,12 who retrospectively evaluated 65 high-risk and 30 relapsed AML patients, no significant impact of a marrow blast count less or higher than 20% was found. In contrast, Pfrepper et al34 reported a significant adverse effect of blast counts >20% on OS in a small group of 44 refractory AML patients and Schmid et al13 reported at least a predictive trend of bone marrow blast count <50% or >50% on treatment outcome. A slightly different patient population may have been causal for these differences and we have to point out that in comparison to the other cited publications one-third of our study cohort underwent HCT in complete remission.
Notably, while increased blast count strongly predicted outcome for the entire cohort, subgroup and interaction analyses suggest that this effect was less pronounced in patients who underwent HCT during 1st line therapy (ELN high-risk, poor early response or primary refractoriness after standard induction) compared to relapsed AML. Similarly, Schmid et al made the observation that outcome after HCT in aplasia was superior for patients proceeding to HCT early in their disease course after no more than 2 IT courses.13 Prospective trials are necessary to answer which patients with residual disease will benefit from proceeding to allo HCT with sequential conditioning and which patients need additional attempts to induce remission prior to allo HCT. In an ongoing multicenter randomized controlled trial, we are currently challenging the value of salvage chemotherapy versus immediate allo HCT after sequential conditioning for patients with residual AML (NCT02461537). Interestingly, ELN 2010 criteria showed no significant impact on EFS and OS. The impact of the current active ELN 2017 criteria could not be assessed since comprehensive molecular data were not available for the entire patient cohort transplanted between 2003 and 2015. It is worth noting that supportive therapy has further evolved in recent years. Better outcomes might thus be expected in contemporary patients.
Conclusion
In conclusion, although this study has limitations, regarding the retrospective design and the lack of comprehensive molecular data, allogeneic HCT in aplasia after melphalan-based conditioning provided good long-term relapse-free survival in a large patient cohort of 178 poor risk AML patients. Consequently, this transplant concept allows for a curative treatment approach even in AML patients with residual morphological disease prior HCT, who might otherwise not proceed to HCT. Nevertheless, relapse risk, particularly within the first six months, remains considerably high. Indeed, the pretransplant blast count has a relevant impact on survival rates, especially in the relapsed patient group. Since high residual blast counts after an attempt to induce remission or at relapse might rather indicate aggressive AML biology and chemotherapy resistance, further salvage chemotherapy to induce a remission prior HCT appears less attractive compared to early alloHCT after sequential conditioning. Post-transplant pre-emptive or prophylactic therapy (eg, hypomethylating agents or tyrosine kinase inhibitors with or without donor lymphocyte infusions)35–42 will be necessary to maintain remission after alloHCT in more of these poor risk AML patients. Finally, a prospective study concept combining sequential conditioning HCT in aplasia with a posttransplant maintenance strategy might be a promising approach to offer a curative treatment strategy to patients who might otherwise not be considered for a standard curative transplant concept at all.
Acknowledgments
This study was presented in part at the 42nd Annual Meeting of the European Society for Blood and Marrow Transplantation (EBMT), 3.April–0.6. April 2016, Valencia, Spain
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Ethics Approval and Informed Consent
The study was conducted in accordance to the Declaration of Helsinki and approved by the responsible ethics committees (IRB of the Technical university Dresden, IORG0001076). Only data from patients who had signed informed consent on retrospective analyses of clinical data at the time of transplantation were included.
Disclosure
Dr Martin Wermke reports personal fees, grants, and/or non-financial support from Novartis, Pfizer, Roche, Lilly, Bristol Myers Squibb, Cellex, Boehringer Ingelheim, ISA Pharmaceuticals, Gemoab, AstraZeneca, Immatics, and Amgen, outside the submitted work. The authors declare no other potential conflicts of interest for this work.
References
1. Cornelissen JJ, Gratwohl A, Schlenk RF, et al. The European LeukemiaNet AML Working Party consensus statement on allogeneic HSCT for patients with AML in remission: an integrated-risk adapted approach. Nat Rev Clin Oncol. 2012;9(10):579–590.
2. Breems DA, Van Putten WL, Huijgens PC, et al. Prognostic index for adult patients with acute myeloid leukemia in first relapse. J Clin Oncol. 2005;23(9):1969–1978.
3. Burnett AK, Goldstone A, Hills RK, et al. Curability of patients with acute myeloid leukemia who did not undergo transplantation in first remission. J Clin Oncol. 2013;31(10):1293–1301.
4. Ganzel C, Sun Z, Cripe LD, et al. Very poor long‐term survival in past and more recent studies for relapsed AML patients: the ECOG‐ACRIN experience. Am J Hematol. 2018;93:1074–1081.
5. Ofran Y, Rowe JM. Treatment for relapsed acute myeloid leukemia: what is new? Curr Opin Hematol. 2012;19:89–94.
6. Forman SJ, Rowe JM. The myth of the second remission of acute leukemia in the adult. Blood. 2013;121(7):1077–1082.
7. Duval M, Klein JP, He W, et al. Hematopoietic stem-cell transplantation for acute leukemia in relapse or primary induction failure. J Clin Oncol. 2010;28:3730–3738.
8. Oyekunle AA, Kröger N, Zabelina T, et al. Allogeneic stem-cell transplantation in patients with refractory acute leukemia: a long-term follow-up. Bone Marrow Transplant. 2006;37:45–50.
9. Thol F, Schlenk RF, Heuser M, Ganser A. How I treat refractory and early relapsed acute myeloid leukemia. Blood.2015;126(3):319–327.
10. Liu Yin JA, Wheatley K, Rees JKH, et al. Comparison of ‘sequential’ versus ‘standard’ chemotherapy as re‐induction treatment, with or without cyclosporine, in refractory/relapsed acute myeloid leukaemia (AML): results of the UK Medical Research Council AML‐R trial. Br J Haematol. 2001;113:713–726.
11. Platzbecker U, Thiede C, Füssel M, et al. Reduced intensity conditioning allows for up-front allogeneic hematopoietic stem cell transplantation after cytoreductive induction therapy in newly-diagnosed high-risk acute myeloid leukemia. Leukemia. 2006;20:707–714.
12. Stolzel F, Platzbecker U, Mohr B, et al. Early intervention with allogeneic hematopoietic cell transplantation during chemotherapy-induced aplasia in patients with high-risk acute myeloid leukemia. Leukemia. 2013;27:2068–2072.
13. Schmid C, Schleuning M, Schwerdtfeger R, et al. Long-term survival in refractory acute myeloid leukemia after sequential treatment with chemotherapy and reduced-intensity conditioning for allogeneic stem cell transplantation. Blood. 2006;108:1092–1099.
14. Schmid C, Schleuning M, Tischer J, et al. Early allo-SCT for AML with a complex aberrant karyotype—results from a prospective pilot study. Bone Marrow Transplant. 2012;47:46–53.
15. Middeke JM, Herbst R, Parmentier S, et al. Clofarabine salvage therapy before allogeneic hematopoietic stem cell transplantation in patients with relapsed or refractory AML: results of the BRIDGE trial. Leukemia. 2016;30(2):261–267.
16. Schetelig J, Schaich M, Schäfer-Eckart K, et al. Hematopoietic cell transplantation in patients with intermediate and high-risk AML: results from the randomized Study Alliance Leukemia (SAL) AML 2003 trial. Leukemia. 2015;29(5):1060–1068.
17. Döhner H, Estey EH, Amadori S, et al. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood. 2010;115(3):453–474.
18. Przepiorka D, Weisdorf D, Martin P, et al. 1994 consensus conference on acute GVHD grading. Bone Marrow Transplant. 1995;15(6):825–828.
19. Atkinson K, Horowitz MM, Gale RP, Lee MB, Rimm AA, Bortin MM. Consensus among bone marrow transplanters for diagnosis, grading and treatment of chronic graft-versus-host disease. Committee of the International Bone Marrow Transplant Registry. Bone Marrow Transplant. 1989;4(3):247–254.
20. Schlenk RF, Döhner H. Genomic applications in the clinic: use in treatment paradigm of acute myeloid leukemia. Hematology Am Soc Hematol Educ Program. 2013;1:324–330.
21. Schneidawind D, Federmann B, Faul C, Vogel W, Kanz L, Bethge WA. Allogeneic hematopoietic cell transplantation with reduced-intensity conditioning following FLAMSA for primary refractory or relapsed acute myeloid leukemia. Ann Hematol. 2013;92(10):1389–1395.
22. Schmid C, Schleuning M, Hentrich M, et al. High antileukemic efficacy of an intermediate intensity conditioning regimen for allogeneic stem cell transplantation in patients with high-risk acute myeloid leukemia in first complete remission. Bone Marrow Transplant. 2008;41(8):721–727.
23. Sheth V, Labopin M, Canaani J, et al. Comparison of FLAMSA-based reduced intensity conditioning with treosulfan/fludarabine conditioning for patients with acute myeloid leukemia: an ALWP/EBMT analysis. Bone Marrow Transplant. 2019;54:531–539.
24. Saraceni F, Labopin M, Brecht A, et al. Fludarabine-treosulfan compared to thiotepa-busulfan-fludarabine or FLAMSA as conditioning regimen for patients with primary refractory or relapsed acute myeloid leukemia: a study from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation (EBMT). J. Hematol. Oncol. 2019;12:44.
25. Aoki J, Seo S, Kanamori H, et al. Impact of low-dose TBI on outcomes of reduced intensity conditioning allogeneic hematopoietic stem cell transplantation for AML. Bone Marrow Transplant. 2016;51:604–606.
26. Al Malki MM, Nathwani N, Yang D, et al. Melphalan-based reduced-intensity conditioning is associated with favorable disease control and acceptable toxicities in patients older than 70 with hematologic malignancies undergoing allogeneic hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2018;24(9):1828–1835.
27. Steckel NK, Groth C, Mikesch JH, et al. High-dose melphalan-based sequential conditioning chemotherapy followed by allogeneic haematopoietic stem cell transplantation in adult patients with relapsed or refractory acute myeloid leukaemia. Br J Haematol. 2018;180(6):840–853.
28. Tallman MS, Dewald GW, Gandham S, et al. Impact of cytogenetics on outcome of matched unrelated donor hematopoietic stem cell transplantation for acute myeloid leukemia in first or second complete remission. Blood. 2007;110:409–417.
29. Koreth J, Schlenk R, Kopecky KJ, et al. Allogeneic stem cell transplantation for acute myeloid leukemia in first complete remission: systematic review and meta-analysis of prospective clinical trials. JAMA. 2009;301(22):2349–2361.
30. Craddock C, Labopin M, Pillai S, et al. Factors predicting outcome after unrelated donor stem cell transplantation in primary refractory acute myeloid leukaemia. Leukemia. 2011;25(5):808–813.
31. Rodríguez-Arbolí E, Labopin M, Tischer J, et al. FLAMSA-Based Reduced-Intensity Conditioning versus Myeloablative Conditioning in Younger Patients with Relapsed/Refractory Acute Myeloid Leukemia with Active Disease at the Time of Allogeneic Stem Cell Transplantation: an Analysis from the Acute Leukemia Working Party of the European Society for Blood and Marrow Transplantation. Biol Blood Marrow Transplant. 2020;26(11):2165–2173.
32. Craddock C, Jackson A, Loke J, et al. Augmented reduced-intensity regimen does not improve postallogeneic transplant outcomes in acute myeloid leukemia. J Clin Oncol. 2021;39(7):768–778.
33. Todisco E, Ciceri F, Boschini C, et al. Factors predicting outcome after allogeneic transplant in refractory acute myeloid leukemia: a retrospective analysis of Gruppo Italiano Trapianto di Midollo Osseo (GITMO). Bone Marrow Transplant. 2017;52:955–961.
34. Pfrepper C, Klink A, Behre G, et al. Risk factors for outcome in refractory acute myeloid leukemia patients treated with a combination of fludarabine, cytarabine, and amsacrine followed by a reduced-intensity conditioning and allogeneic stem cell transplantation. J Cancer Res Clin Oncol. 2016;142:317–324.
35. Schmid C. Labopin M., Schaap N., et al. Prophylactic donor lymphocyte infusion after allogeneic stem cell transplantation in acute leukaemia – a matched pair analysis by the Acute Leukaemia Working Party of EBMT. Br J Haematol. 2019;184:782–787.
36. Jedlickova Z, Schmid C, Koenecke C, et al. Long-term results of adjuvant donor lymphocyte transfusion in AML after allogeneic stem cell transplantation. Bone Marrow Transplant. 2016;51:663–667.
37. Platzbecker U, Middeke JM, Sockel Ket al. Measurable residual disease-guided treatment with azacitidine to prevent haematological relapse in patients with myelodysplastic syndrome and acute myeloid leukaemia (RELAZA2): an open-label, multicentre, phase 2 trial. Lancet Oncol. 2018;12:1668–1679.
38. Gao L, Zhang Y, Wang S, et al. Effect of rhG-CSF combined with decitabine prophylaxis on relapse of patients with high-risk MRD-Negative AML after HSCT: an open-label, multicenter, randomized controlled trial. J Clin Oncol. 2020;38(36):4249–4259.
39. Bug G, Burchert A, Wagner E-M, et al. Phase I/II study of the deacetylase inhibitor panobinostat after allogeneic stem cell transplantation in patients with high-risk MDS or AML (PANOBEST trial). Leukemia. 2017;31:2523–2525.
40. Levis MJ, Chen YB, Hamadani M, Horowitz MM, Jones RJ. Blood and marrow transplant clinical trials network. FLT3 Inhibitor maintenance after allogeneic transplantation: is a placebo-controlled, randomized trial ethical? J Clin Oncol. 2019;37(19):1604–1607.
41. Jetani H, Garcia-Cadenas I, Nerreter T, et al. CAR T-cells targeting FLT3 have potent activity against FLT3-ITD+ AML and act synergistically with the FLT3-inhibitor crenolanib. Leukemia. 2018;32:1168–1179.
42. Fan M, Li M., Gao L.et al. Chimeric antigen receptors for adoptive T cell therapy in acute myeloid leukemia. J. Hematol Oncol. 2017;10:151.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.