Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
All-Cause and Cause-Specific Mortality in Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Authors Zhao G ![]() , Wang L, Lei S, Li Y, Li J
, Wang L, Lei S, Li Y, Li J ![]() , Feng Z
, Feng Z
Received 26 August 2025
Accepted for publication 22 December 2025
Published 30 December 2025 Volume 2025:20 Pages 4173—4190
DOI https://doi.org/10.2147/COPD.S563250
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Guixiang Zhao,1,2 Lu Wang,1– 3 Siyuan Lei,1– 3 Ya Li,1,2 Jiansheng Li,1– 3 Zhenzhen Feng1– 3
1Department of Respiratory Diseases, the First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, Henan, People’s Republic of China; 2The First Clinical Medical College, Henan University of Chinese Medicine, Zhengzhou, Henan, People’s Republic of China; 3Collaborative Innovation Center for Chinese Medicine and Respiratory Diseases Co-Constructed by Henan Province & Education Ministry of P.R. China/Henan Key Laboratory of Chinese Medicine for Respiratory Diseases, Henan University of Chinese Medicine, Zhengzhou, Henan, People’s Republic of China
Correspondence: Zhenzhen Feng, Department of Respiratory Diseases, the First Affiliated Hospital of Henan University of Chinese Medicine, Zhengzhou, 450003, People’s Republic of China, Tel +86-861-14981659, Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is a major global cause of death, imposing substantial socioeconomic and healthcare burdens. This meta-analysis synthesizes evidence on all-cause and cause-specific mortality risks in COPD populations to identify high-risk subgroups and guide precision management strategies.
Methods: We searched PubMed, Embase, Web of Science, and Cochrane Library for cohort studies reporting death risks in COPD from database inception to April 10, 2025. Study screening, data extraction, and quality assessment were independently performed by two investigators. Meta-analyses pooled risks for all-cause and cause-specific mortality. Sensitivity analyses tested robustness; publication bias was assessed via funnel plots and Egger’s test.
Results: Twenty-seven studies covering 286,314 showed COPD patients had significantly higher all-cause mortality versus non-COPD individuals (HR, 1.80; 95% CI: 1.40– 2.30). Mortality risk exhibited a graded increase with COPD severity compared to non-COPD individuals: mild (HR, 1.32; 95% CI: 1.19– 1.47), moderate (HR, 1.62; 95% CI: 1.45– 1.81), severe (HR, 2.18; 95% CI: 1.59– 2.99), and very severe (HR, 2.94; 95% CI: 1.78– 4.85). When stratified by smoking status, COPD patients had consistently higher mortality than their non-COPD counterparts within each subgroup: never-smokers (HR, 1.41; 95% CI: 1.27– 1.56), former smokers (HR, 1.37; 95% CI: 1.30– 1.45), and current smokers (HR, 1.48; 95% CI: 1.25– 1.76). The presence of comorbidities further amplified mortality risks in COPD patients versus non-COPD individuals, particularly in those with respiratory diseases (HR, 3.64; 95% CI: 3.10– 4.27), cardiovascular diseases (HR, 1.29; 95% CI: 1.10– 1.50), and all-cancers (HR, 1.69; 95% CI: 1.37– 2.10), especially lung cancer (HR, 2.57; 95% CI: 2.04– 3.24).
Conclusion: COPD patients have significantly higher death risks than non-COPD individuals, worsening with disease severity. Independent determinants of COPD-attributable mortality risk comprise smoking, coexisting respiratory diseases, cardiovascular diseases, and cancer (particularly lung cancer). These findings provide an evidence-based foundation for developing targeted intervention strategies to mitigate COPD-related mortality.
Keywords: chronic obstructive pulmonary disease, mortality risk, systematic review, meta-analysis
Introduction
Chronic obstructive pulmonary disease (COPD) is a major contributor to global mortality, with death tolls rising from 2.2 million (6th leading cause) in 1990 to 3.5 million (4th) in 2021.1–3 Global Burden of Disease projections indicate COPD will become the third leading cause of death by 2050,4 annual COPD deaths may exceed 7 million by 2060—surpassing combined diabetes and asthma mortality.5 This trajectory impedes progress toward United Nations Sustainable Development Goal (SDG) 3.4, which targets a one-third reduction in premature non-communicable disease mortality by 2030.6 Economically, COPD mortality accounts for 68.3% of the disease’s total burden, costing $49.1 billion annually in lost productivity.7
As an unambiguous endpoint reflecting disease severity and healthcare system efficacy, mortality data provide a critical benchmark for assessing health system performance and optimizing resource allocation to high-risk populations. Reinforcing this, the World Health Organization (WHO) designates COPD mortality surveillance as Essential Indicator E119 for SDG 3.4—explicitly aligning with its mandate for a 30% reduction in non-communicable disease mortality by 2030.8 Given COPD’s established preventability and treatability, identifying modifiable risk factors underlying COPD-attributable mortality is an urgent public health priority. Indeed, a complex interplay of factors significantly influences the risk of death in individuals with COPD. Major determinants include: disease severity;9 history of acute exacerbations;10 comorbidities (such as cardiovascular disease, lung cancer, and metabolic syndrome);11 and demographic/lifestyle factors (including smoking, low body mass index, older age, and low socioeconomic status).12 Understanding how these factors modulate not just overall survival, but also specific causes of death, is crucial for risk stratification and targeted interventions. Therefore, synthesizing evidence on both all-cause and cause-specific mortality by these variables is essential.
Epidemiological research into mortality associated with COPD has been increasing; however, existing studies have predominantly examined the impact of single factors on all-cause mortality exclusively.13–15 Although a meta-analysis has examined all-cause mortality in patients with mild COPD,16 a critical gap persists: to our knowledge, no study has concurrently synthesized evidence on both all-cause and major cause-specific mortalities within a unified analytical framework. This limitation precludes a holistic understanding of COPD mortality patterns. To address this gap, our meta-analysis provides an integrated synthesis of existing evidence on all-cause and cause-specific mortality in COPD patients, with specific focus on quantifying differential effects of key factors across these outcomes via subgroup and meta-regression analyses.
Methods
The protocol for this systematic review has been prospectively registered in the international Prospective Register of Systematic Reviews (CRD420251103371) (https://www.crd.york.ac.uk/PROSPERO/view/CRD420251103371), and the entire study was conducted in strict accordance with the PRISMA 2020 statement17 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses).
Search Strategy
A systematic literature search was conducted in PubMed, Embase, the Cochrane Library, and Web of Science for studies on COPD mortality, with language restricted in English. The search encompassed records from database inception to 10 April 2025. To ensure comprehensive identification of relevant literature, we manually screened the reference lists of included articles. The search strategy utilized a combination of Medical Subject Headings terms and free-text keywords, including “COPD” “mortality” and related synonyms. The detailed search strategy is provided in Supplementary Table 1.
Eligibility Criteria
Studies were included based on the following predefined criteria: (1) study populations comprised individuals with clinically confirmed COPD; (2) control groups consisted of non-COPD individuals; (3) study design was restricted to cohort studies; (4) primary outcomes included mortality, with studies required to report multivariable-adjusted hazard ratios (HRs) or relative risks (RRs) and corresponding 95% confidence intervals (CIs) relative to reference groups.
Exclusion Criteria
Studies were excluded according to the following criteria: (1) conference abstracts, comments, and reviews; (2) studies with incomplete data reporting or lacking outcomes of interest; (3) duplicate publications; (4) For studies utilizing the same dataset by identical authors, only the publication with the longest follow-up duration or the largest sample size was retained.
Study Selection and Data Extraction
Two independent reviewers (GX Z and L W) conducted initial screening by evaluating titles and abstracts of identified records. Following independent cross-checking of screening decisions, potentially eligible studies were provisionally selected. Any disagreements unresolved after discussion were adjudicated by a third reviewer (ZZ F). The full-text articles of provisionally included studies were subsequently obtained and independently assessed by both reviewers against predefined eligibility criteria. Final inclusion was restricted to studies meeting all inclusion requirements.
Data extraction was performed using a customized Microsoft Excel spreadsheet. The extracted information encompassed: (1) basic study characteristics: title, first author, publication year, and country of conduct; (2) participant characteristics: source population, sample size, diagnostic criteria, and mortality verification methods; (3) outcome indicators of interest: effect estimates with corresponding 95% CI for all relevant endpoints; (4) adjusted covariates in statistical models; (5) follow-up duration.
Quality Assessment
Two reviewers independently assessed risk of bias in the included cohort studies using the Newcastle-Ottawa Scale (NOS)18 – an 8-item tool evaluating three domains: (1) participant selection, (2) group comparability, and (3) outcome assessment. Studies were scored on a 9-star system and categorized as low quality (0–3 stars), moderate quality (4–6 stars), or high quality (7–9 stars).
Statistical Analysis
Statistical analyses were performed using Stata 15.0 (Stata Corp, College Station, TX). Pooled HRs with 95% CI were calculated. In all analyses, the hazard ratio represents the mortality risk in a specific group of COPD patients compared to the corresponding group of non-COPD individuals who share the same characteristics (eg, same sex, smoking status, or comorbidity status). Heterogeneity was assessed using χ2-tests and quantified by I2 statistics, with thresholds of 25%, 50%, and 75% indicating low, moderate, and high heterogeneity, respectively. A fixed-effects model was applied when heterogeneity was nonsignificant (I2 < 50%, P ≥ 0.1). Otherwise, a random-effects model was employed. Subgroup analyses were conducted to explore sources of substantial heterogeneity or assess covariate effects. Sensitivity analyses examined robustness through sequential exclusion of individual studies. Publication bias was evaluated by funnel plot symmetry and Egger’s linear regression test for outcomes with ≥10 studies. If detected, the trim-and-fill method was employed for bias correction. Statistical significance was defined as P < 0.05.
Results
Identification of Studies
The initial search identified 45,766 records from four databases: PubMed (n = 20,128), Cochrane Library (n = 3,931), Embase (n = 8,918), and Web of Science (n = 12,789). After removal of 16,119 duplicates, 29,647 records underwent title/abstract screening, excluding 29,599 irrelevant studies. Full-text assessment of 48 articles led to the exclusion of 21 studies, yielding 27 eligible cohort studies.19–45 The literature selection process is detailed in Figure 1.
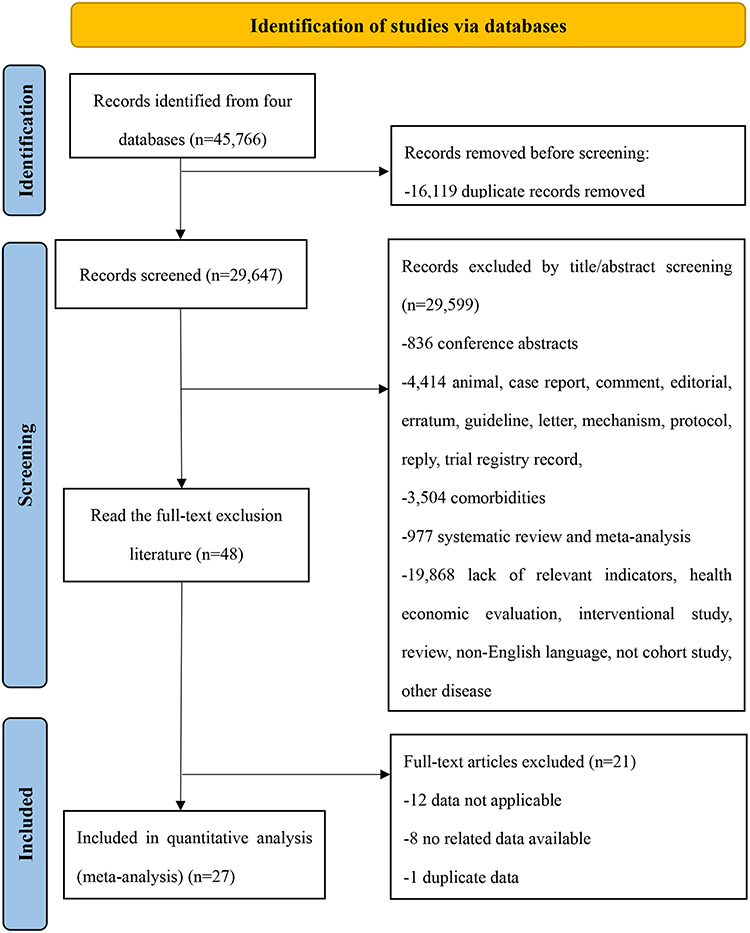 |
Figure 1 Flowchart of literature screening. |
Study Characteristics
This systematic review incorporated 27 cohort studies covering 286,314 participants. Eleven studies enrolled fewer than 1,000 participants, while 16 studies included ≥ 1,000 individuals. COPD diagnosis was primarily based on spirometry (22 studies), supplemented by International Classification of Diseases codes (4 studies) and registry records (1 study). The studies originated from 13 countries, with the United States, United Kingdom, and Denmark contributing the largest proportion. Geographically, 13 studies were from Europe, 9 from the Americas, and 5 from the Western Pacific. Two studies were from upper-middle-income countries (UMICs) and 25 from high-income countries (HICs). Follow-up duration ranged from 4 to 29 years, with 14 studies reporting <10 years and 13 studies reporting ≥10 years. Notably, only one study had a minimum follow-up of 4 years; all others follow-up durations of ≥ 5 years. Overall, the basic characteristics of included studies are summarized in Table 1. Adjusted confounding factors in the included literature in Supplementary Table 2.
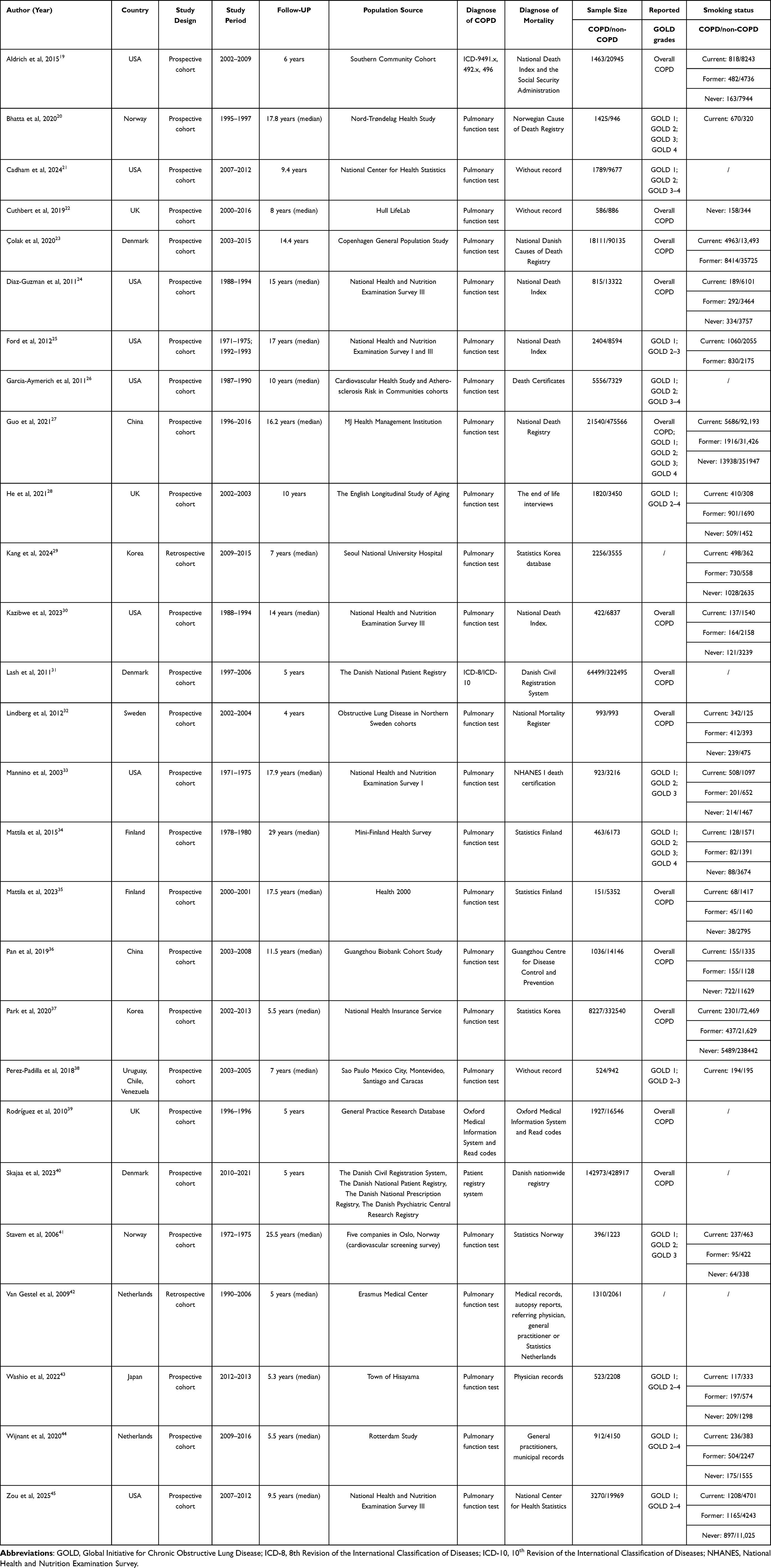 |
Table 1 Basic Characteristics of the Included Studies |
Of the 27 included studies reporting mortality risk in COPD, 13 provided data on overall COPD mortality without distinction by GOLD grade.19,22–24,27,30–32,35–37,39,40 Other studies reported risk data for specific GOLD grades, as follows: GOLD 1 (13 studies),20,21,25–28,33,34,38,41,43–45 GOLD 2 (7 studies),20,21,26,27,33,34,41 GOLD 3 (5 studies),20,27,33,34,41 and GOLD 4 (3 studies).20,27,34 In addition, several studies presented combined risk estimates for adjacent GOLD grades, including GOLD 2–3 (2 studies),25,38 GOLD 2–4 (4 studies),28,43–45 and GOLD 3–4 (2 studies).21,26 Regarding smoking status, the numbers of current, former, and never-smokers among COPD and non-COPD individuals were reported in 20,19,20,23–25,27–30,32–38,41,43–45 18,19,23–25,27–30,32–37,41,43–45 and 1719,22,24,27–30,32–37,41,43–45 studies, respectively. Pooled analysis indicated that in the COPD group, there were 19,925 current smokers, 17,022 former smokers, and 24,386 never-smokers. In the non-COPD group, the corresponding numbers were 208,704, 115,751, and 644,016, respectively.
Quality Assessment
Methodological quality appraisal was conducted using the NOS. All 27 cohort studies satisfied criteria for comparability of cohorts and explicitly defined follow-up duration, thereby achieving total NOS scores ≥ 7. These results demonstrate high methodological quality across included studies (Supplementary Table 3).
Meta-Analysis of All-Cause Mortality Risk
All-Cause Mortality Risk in Overall COPD
Thirteen studies19,22–24,27,30–32,35–37,39,40 involving overall COPD cohorts (n = 255,923) reported all-cause mortality data. The pooled analysis revealed a significantly elevated all-cause mortality risk in COPD patients compared with non-COPD (HR, 1.80; 95% CI: 1.40–2.30) (Figure 2). Subgroup analyses stratified by geographic region, country, follow-up duration, income level, and sample size indicated statistically significant differences across all subgroups (P < 0.05) (Figure 3). Leave-one-out sensitivity analysis confirmed the robustness of pooled estimates (Supplementary Figure 1).
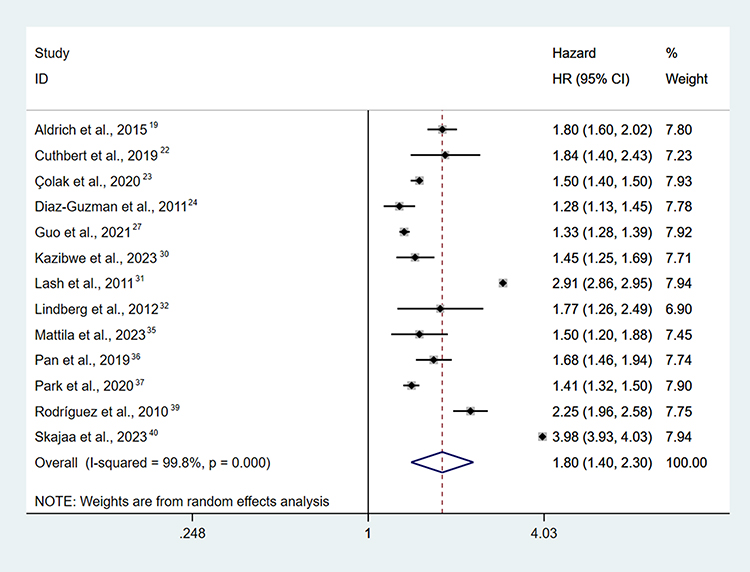 |
Figure 2 Forest plot of mortality risk of overall COPD compared with non-COPD individuals. |
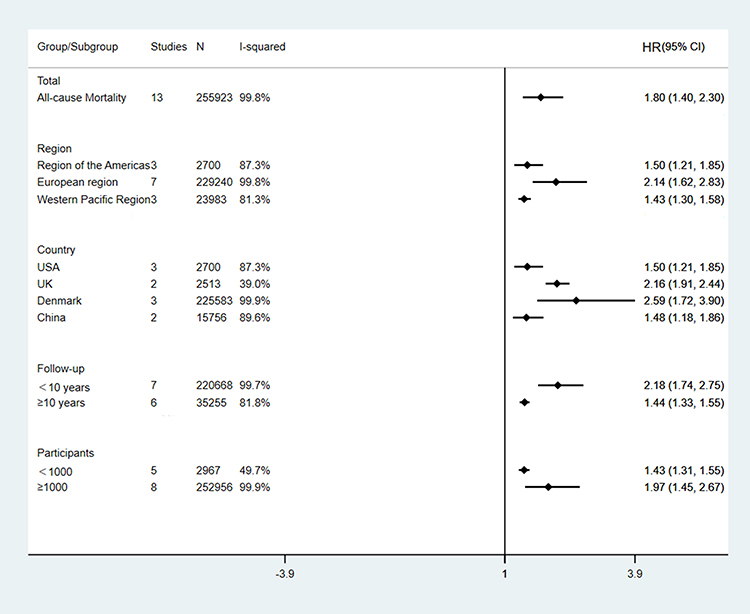 |
Figure 3 Pooled forest plot of mortality risk of overall COPD by subgroup analysis. |
All-Cause Mortality Risk of COPD in Different Severity Grades
Quantitative analysis demonstrated that patients with COPD had significantly higher all-cause mortality across all GOLD stages compared to non-COPD individuals (all P < 0.001), with a progressively increasing risk corresponding to disease severity. The HRs were as follows: GOLD 1 (HR, 1.32; 95% CI:1.19–1.47),20,21,25–28,33,34,38,41,43–45 GOLD 2 (HR, 1.62; 1.45–1.81),20,21,26,27,33,34,41 GOLD 3 (HR, 2.18; 1.59–2.99),20,27,33,34,41 and GOLD 4 (HR, 2.94; 1.78–4.85).20,27,34 Furthermore, analyses of combined severity groups also showed consistently elevated risks: GOLD 2–3 (HR, 2.79; 1.86–4.18),25,38 GOLD 2–4 (HR, 1.73; 1.61–1.85),28,43–45 and GOLD 3–4 (HR, 3.23; 2.11–4.93)21,26 (Table 2). Forest plots are provided in Supplementary Figures 2–8.
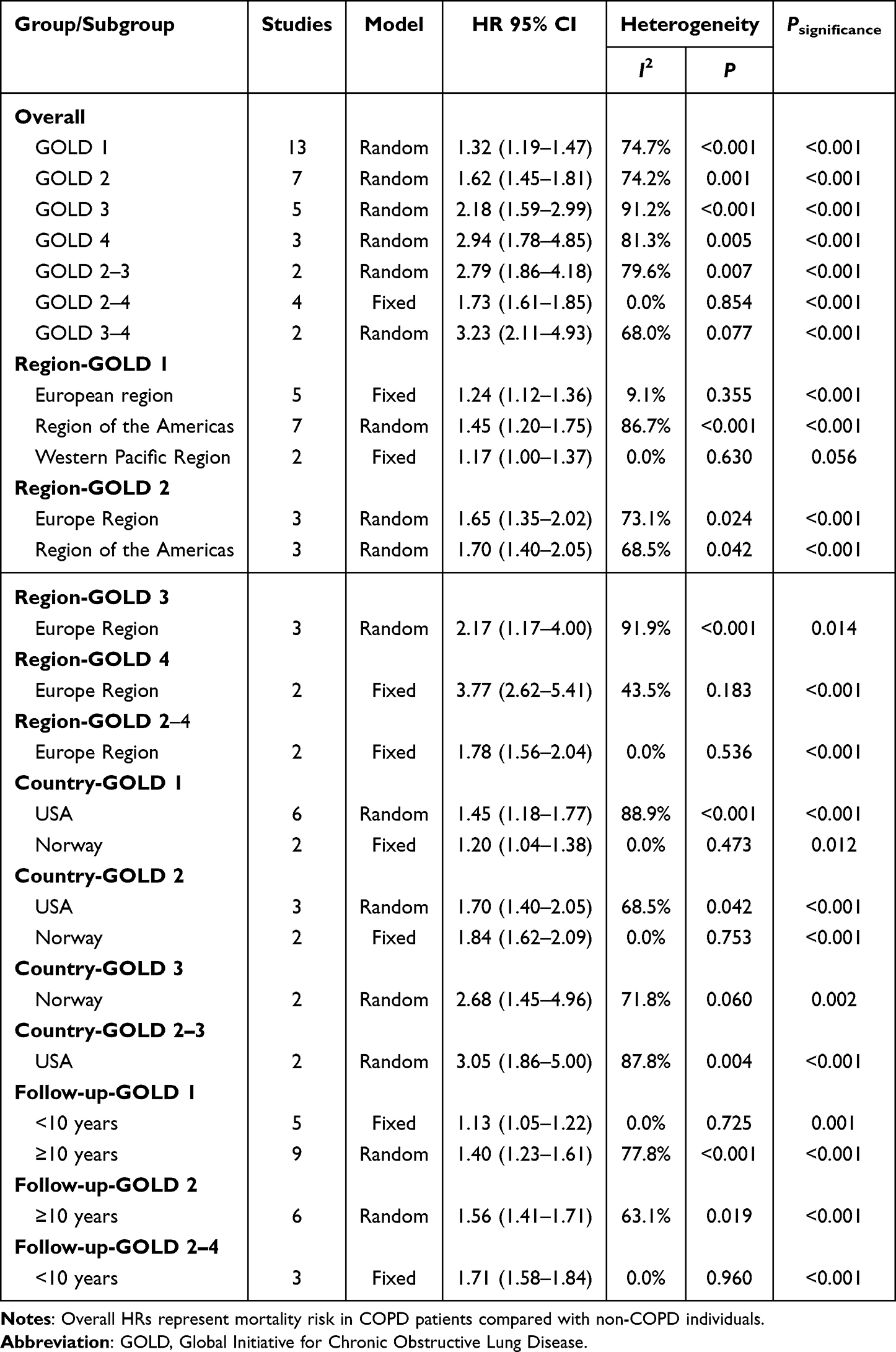 |
Table 2 All-Cause Mortality Risk of COPD in Different Severity Grades |
Stratified analysis by geographic region and GOLD stage further indicated a consistent severity-risk gradient across all regions and countries, except for GOLD 1 patients in the Western Pacific region, where the association was not statistically significant (P > 0.05) (Table 2). Sensitivity analysis restricted to GOLD 1 cohorts with ≥10 included studies confirmed the robustness of these findings (Supplementary Figure 9).
All-Cause Mortality Risk of COPD in Different Smoking Status
Pooled analyses of all-cause mortality risk stratified by smoking status and GOLD classification demonstrated a consistent graded elevation in mortality risk with increasing COPD severity across all smoking strata: among never-smokers, individuals with COPD exhibited higher mortality compared to never-smokers without COPD in the overall COPD group (HR, 1.41; 95% CI: 1.27–1.56),27,29,37 GOLD 1 (HR, 1.14; 95% CI: 1.02–1.28),27,33,45 GOLD 2 (HR, 1.36; 95% CI: 1.25–1.47),27,33 and GOLD 3 (HR, 1.82; 95% CI: 1.66–2.00);27,33 among former smokers, COPD individuals had higher mortality than former smokers without COPD, with corresponding HRs of 1.37 (95% CI: 1.30–1.45) for overall COPD,27,37 1.10 (95% CI: 0.98–1.22) for GOLD 1,27,33,45 1.56 (95% CI: 1.43–1.69) for GOLD 2,27,33 and 2.41 (95% CI: 1.26–4.60) for GOLD 3;27,33 among current smokers, COPD individuals showed higher mortality compared to current smokers without COPD, with HRs of 1.48 (95% CI: 1.25–1.76) for overall COPD,27,29,37 1.26 (95% CI: 1.10–1.43) for GOLD 1,27,33,45 1.61 (95% CI: 1.41–1.84) for GOLD 2,27,33 and 2.39 (95% CI: 1.52–3.78).27,33 (Figure 4).
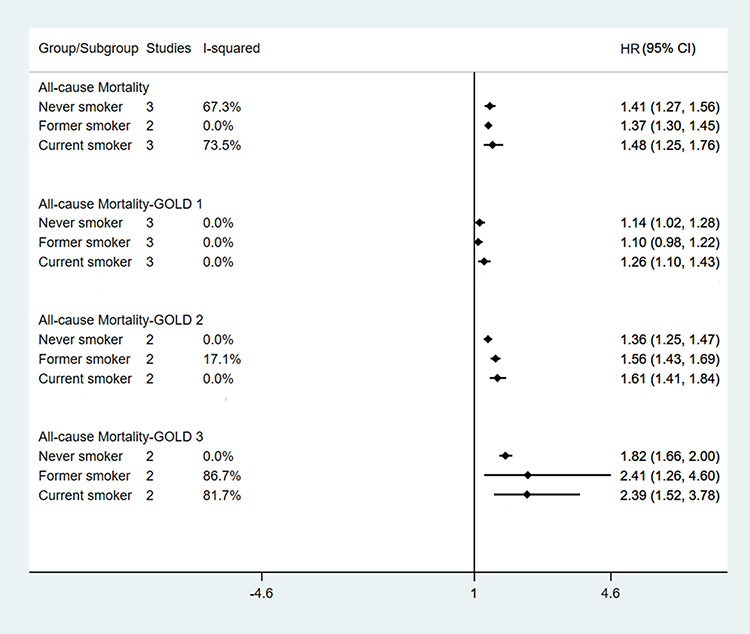 |
Figure 4 Pooled forest plot of mortality risk in COPD compared with non-COPD stratified by smoking status. |
All-Cause Mortality Risk of COPD in Different Diseases
Two studies conducted a quantitative analysis of all-cause mortality risk by subgroup in patients with COPD comorbid with respiratory disease (overall COPD,23,35 GOLD,28,34 and GOLD 2–428,43). The pooled results showed that among individuals with respiratory diseases, COPD patients had the following all-cause mortality risks compared to non-COPD patients: an overall HR of 3.64 (95% CI: 3.10–4.27) for COPD, 1.71 (95% CI: 1.03–2.82) for GOLD 1, and 2.70 (95% CI: 0.37–19.81) for GOLD 2–4. A significant association between respiratory diseases and all-cause mortality was observed in the overall COPD and GOLD 1 groups (both P < 0.05), but not in the GOLD 2–4 group (P = 0.329) (Table 3).
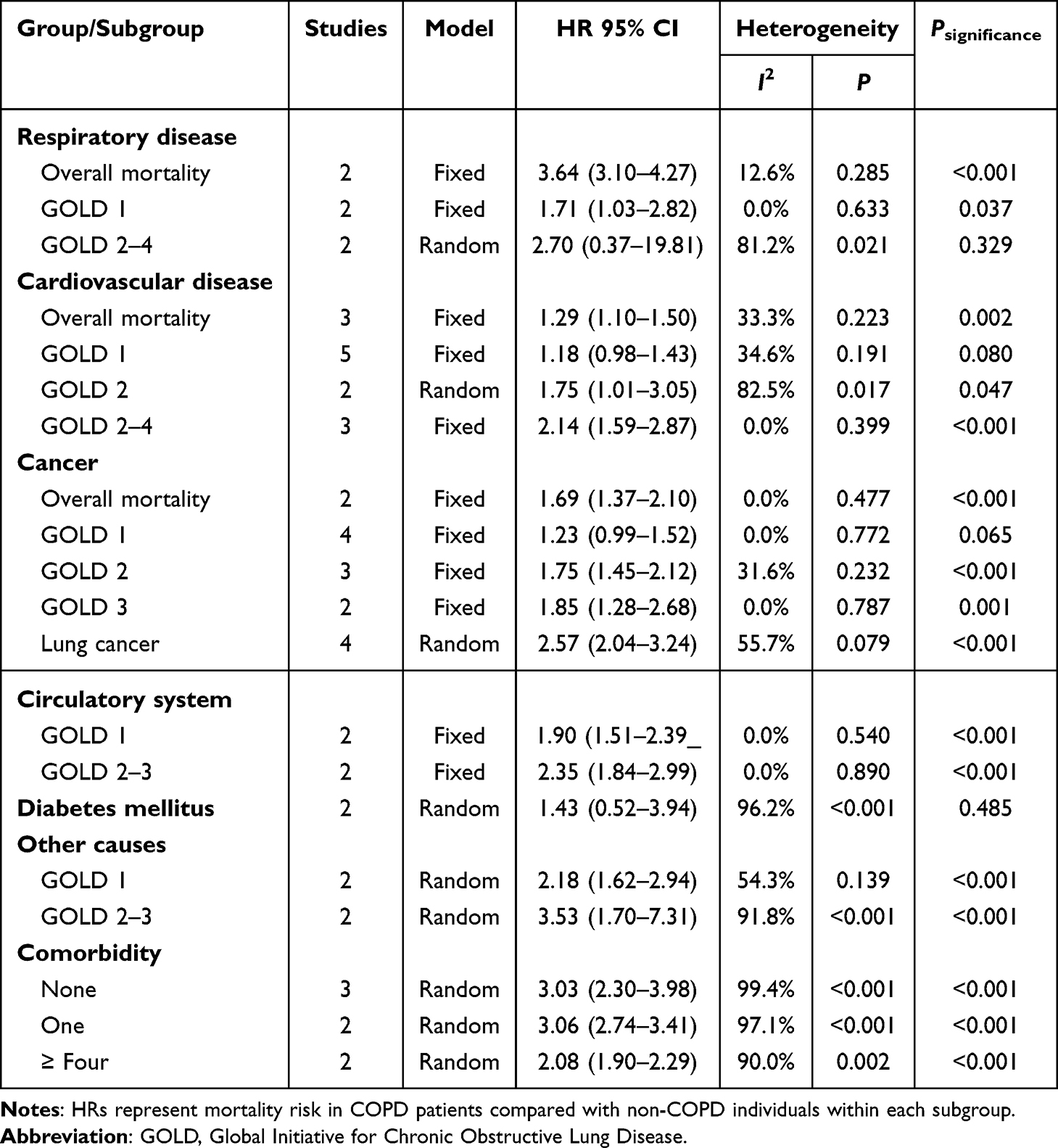 |
Table 3 All-Cause Mortality Risk of COPD in Different Diseases |
Aggregated quantitative synthesis from three studies on overall COPD,35–37 five on GOLD 1,21,28,34,43,44 two on GOLD 2,21,34 and three on GOLD 2–428,43,44 demonstrated that COPD patients with comorbid cardiovascular disease had a higher mortality risk compared with non-COPD individuals with cardiovascular disease: overall COPD (HR, 1.29; 95% CI: 1.10–1.50), GOLD 1 (HR, 1.18; 95% CI: 0.98–1.43), GOLD 2 (HR, 1.75; 95% CI: 1.01–3.05) and GOLD 2–4 (HR, 2.14; 95% CI: 1.59–2.87), with statistical significance (P < 0.05) observed in all groups except GOLD stage 1 (Table 3).
The risk of cancer-attributable all-cause mortality was evaluated in several studies comparing COPD patients to non-COPD individuals with cancer. The analysis involved: two studies for the overall COPD population,35,42 four for GOLD 1,21,34,42,43 three for GOLD 2,21,34,42 and two for GOLD 3 studies.34,42 Fixed-effect meta-analyses revealed a statistically significant increase in risk for overall COPD (HR, 1.69; 95% CI: 1.37–2.10), GOLD 2 (HR, 1.75; 95% CI: 1.45–2.12), and GOLD 3 (HR, 1.85; 95% CI: 1.28–2.68). The risk increase for GOLD 1 was not statistically significant (HR, 1.23; 95% CI: 0.99–1.52). Additionally, a separate analysis of four studies on lung cancer-specific mortality also showed a significantly elevated risk (HR, 2.57; 95% CI: 2.04–3.24), as presented in Table 3.
Two studies37,40 evaluated the association of all-cause mortality between patients with COPD and non-COPD individuals among populations with diabetes. The pooled analysis revealed on statistically significant difference in risk (HR, 1.43; 95% CI: 0.52–3.94). Additionally, a study25 comprising two prospective cohorts further analyzed cause-specific mortality stratified by GOLD severity in COPD patients compared to non-COPD individuals. The results demonstrated significantly elevated mortality risks due to both circulatory diseases and other causes across all COPD severity groups (P < 0.05) (Table 3). Specifically, the HRs for circulatory disease mortality were 1.90 (95% CI: 1.51–2.39) in the GOLD 1 group and 2.35 (95% CI: 1.84–2.99) in the GOLD 2–3 group. Meanwhile, the corresponding HRs for mortality from other causes were 2.18 (95% CI: 1.62–2.94) in the GOLD 1 group and 3.53 (95% CI: 1.70–7.31) in the GOLD 2–3 group.
Three studies31,37,40 evaluated the risk of mortality between COPD patients and non-COPD individuals in the absence of comorbidities. The results demonstrated a significantly elevated risk of death among COPD patients, with a pooled HR of 3.03 (95% CI: 2.30–3.98). Furthermore, two studies31,40 assessed the difference in mortality risk between COPD and non-COPD subjects when both groups had pre-existing comorbidities. The results showed that HR was 3.06 (95% CI: 2.74–3.41) in individuals with one comorbidity, and 2.08 (95% CI: 1.90–2.29) in those with four or more comorbidities (Table 3).
All-Cause Mortality Risk of COPD in Different Sex
A sex-stratified meta-analysis of all-cause mortality in patients with COPD revealed divergent risk profiles: male patients with COPD exhibited a significantly elevated mortality risk compared with non-COPD males for overall COPD (HR, 1.38; 95% CI: 1.33–1.44)27,32,37 and GOLD 1 (HR, 1.17; 95% CI: 1.06–1.29).27,45 In contrast, female patients with COPD showed a significantly higher mortality risk than non-COPD females in unstratified cohorts (HR, 1.32; 95% CI: 1.25–1.40),27,37 but no statistically significant increase was observed for GOLD 1 stage (HR, 1.09; 95% CI: 0.97–1.22; P = 0.172)27,45 (Table 4).
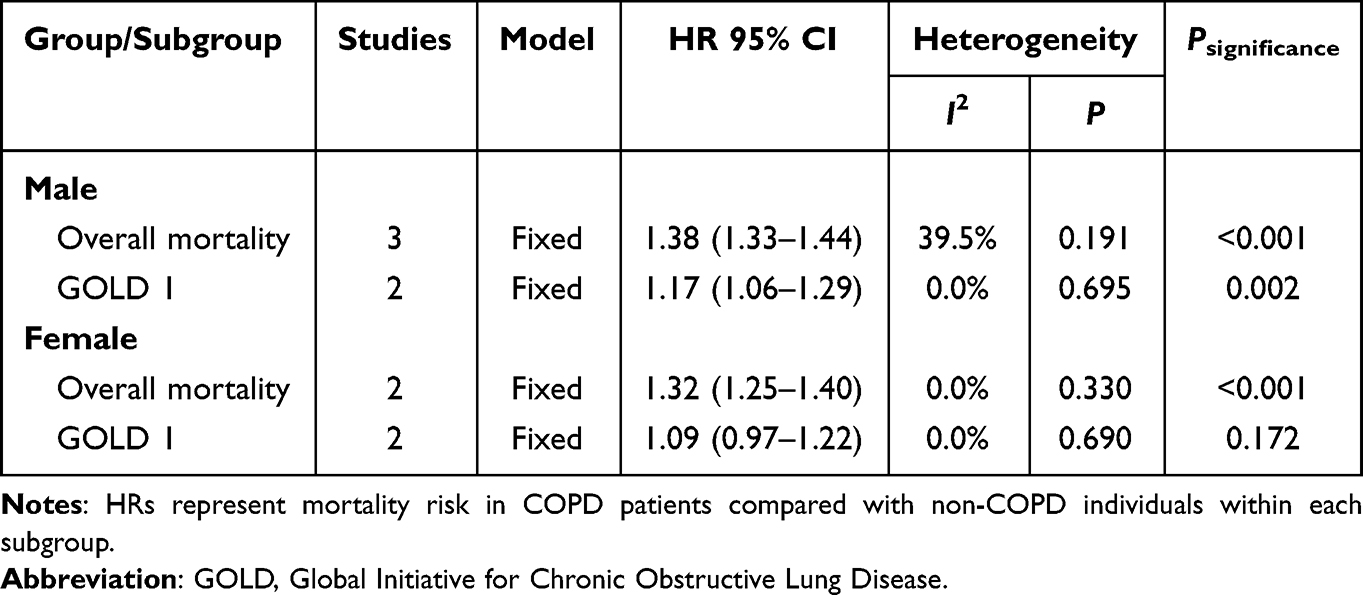 |
Table 4 All-Cause Mortality Risk of COPD in Different Sex |
Publication Bias
Egger’s regression test detected significant publication bias in overall COPD mortality studies (t = −2.45, P = 0.032). Trim-and-fill adjustment yielded a recalibrated pooled HR of 1.80 (95% CI: 1.41–2.30), which demonstrated striking concordance with the pre–adjustment estimate (HR, 1.80; 95% CI: 1.40–2.30), confirming analytical robustness. For GOLD 1 cohorts, Egger’s test indicated no significant bias (P = 0.219). Publication bias analyses were omitted for others due to insufficient studies (n < 10), with detailed results provided in Supplementary Figures 10 and 11.
Discussion
This systematic meta-analysis, integrating data from 27 cohort studies encompassing 286,314 COPD patients, provides the first comprehensive assessment of all-cause mortality risk in this population. Results demonstrated a significantly increased all-cause mortality risk among COPD patients versus non-COPD individuals (HR,1.80; 95% CI: 1.40–2.30). Crucially, this risk association persisted consistently across all COPD severity strata, comorbidities (respiratory, cardiovascular, and cancers), smoking behavior categories (never-smokers, former smokers, current smokers), and both genders. Risk-stratified analyses further revealed a progressive mortality risk escalation with advancing disease severity. Collectively, these findings robustly confirm COPD’s pervasive adverse impact on all-cause mortality, providing critical evidence for prognostic assessment and clinical management optimization.
COPD presents a critical global public health challenge, necessitating precise mortality risk assessment to optimize clinical management and improve prognosis.46–48 This study confirms significantly elevated all-cause mortality in COPD patients versus non-COPD controls, a pattern persisting across diverse geographical regions, income levels, and countries, due to core pathophysiological mechanisms of COPD-progressive airflow limitation and systemic inflammation.49 Notably, higher COPD-attributed mortality estimates in HICs compared to UMICs likely reflect systemic limitations in many UMICs, such as constrained healthcare infrastructure and inadequate disease awareness, which elevate underdiagnosis rates and cause significant under-ascertainment of COPD as an underlying cause of death.50 Furthermore, Europe demonstrates higher COPD-attributed mortality risk than the Americas and Western Pacific regions, attributable to its older population structure, prolonged history of widespread smoking prevalence, and crucially, more advanced healthcare systems with robust mortality surveillance mechanisms that enhance detection and accurate certification of COPD as a contributing or underlying cause of death.
Precise stratification of mortality risk across distinct COPD severity levels is critical for accurate prognostic assessment, optimized healthcare resource allocation, and individualized management strategies. Our analysis demonstrates a graded increase in mortality risk with progressive disease severity, consistent with established evidence.51–53 Crucially, supporting histopathological evidence54 reveals detectable microscopic alterations in lung tissue even at early stages (GOLD 1–2), prior to overt emphysematous destruction. These include early elastin fibers loss within alveolar attachments and progressive luminal narrowing in terminal bronchioles–pathological changes that correlate with advancing disease severity. This dual pathology, characterized by small airway remodeling and diminished parenchymal elastic recoil, underlies the heightened incidence of complications such as hypoxemia and chronic respiratory failure in severe airflow limitation. Consequently, this pathophysiological progression translates into a significantly elevated mortality risk.
Tobacco smoking constitutes the principal modifiable risk factor for COPD,55,56 with cohort evidence consistently demonstrating elevated all-cause mortality risk in smokers versus never-smokers across all disease severity strata–reflecting a positive correlation between smoking intensity and both COPD incidence and mortality.57,58. Notably, the mortality risk in never-smokers with COPD was also significantly higher compared to non-COPD individuals. Although potential inconsistencies in the diagnosis of COPD among never-smokers cannot be fully excluded, the fact that most included studies adopted pulmonary function testing as the core diagnostic criterion ensures the overall reliability of this subgroup analysis. Pathogenetically, smoking mediates damage through interrelated mechanisms:59–61 at the airway level, smoke constituents stimulate mucus hypersecretion and impair ciliary function, compromising mucociliary clearance; at the functional level, smoke exposure induces bronchospasm and persistent airflow limitation; and at the molecular level, smoke triggers immune cell infiltration and disrupts the protease-antiprotease balance, accelerating parenchymal destruction. Smoking cessation represents the single most potent primary preventive and secondary interventional measure. Robust evidence confirms that quitting smoking not only reduces disease incidence but also significantly attenuates mortality risk among individuals with established COPD.62,63
COPD disproportionately affects older adults, with its hallmark persistent pulmonary and systemic inflammation significantly elevating comorbidity risk.64,65 Meta-analysis66 evidence corroborated that cardiovascular and cancer comorbidities substantially increase long-term mortality risk in COPD patients, aligning with the present findings. Pathogenetically, COPD is characterized as a systemic inflammatory condition; pulmonary inflammation triggers systemic responses via inflammatory mediator release, subsequently impairing cardiovascular, metabolic, and other physiological systems.67,68 This multisystem dysfunction drives diverse comorbidities, ultimately accelerating functional decline, quality of life deterioration, and worsened prognosis.69,70 Notably, COPD-associated mortality risk is elevated in both genders. While females typically exhibit lower cumulative tobacco exposure than males, inhalation of poorly ventilated cooking fumes represents a significant gender-specific risk factor for COPD-related mortality among women.
To our knowledge, as the first comprehensive meta-analysis quantifying COPD-attributable mortality, this study demonstrates these core strengths: First, by restricting inclusion to cohort studies, it capitalizes on prospective designs to enhance causal inference validity while mitigating selection bias. Second, incorporated studies further exhibit rigorous methodology with extended follow-up durations (96% ≥ 5 years), ensuring robust survival estimates through sufficient endpoint accrual. Third, all extracted HRs were consistently multivariable-adjusted, substantially reducing confounding effects on pooled estimates. Fourth, beyond providing all-cause mortality risk stratified by COPD severity, we systematically evaluated the effects of smoking status and comorbidity burden, thereby establishing a multidimensional evidence base to inform personalized prognosis and targeted interventions.
Notwithstanding the above strengths, this study has several limitations. First, the geographic representation of included studies is suboptimal: 93% originated from HICs, with merely two from UMICs and none from low-income nations; this imbalance may substantially underestimate the global COPD mortality burden due to unaccounted epidemiological heterogeneity. Second, insufficient cohort numbers restricted multidimensional risk exploration, preventing rigorous assessment of determinants such as e-cigarette exposure, body mass index, and age. Furthermore, the assessment of comorbidities was limited to broad categories. Due to this constraint in the available data, a pooled analysis of the impact of specific individual diseases on COPD mortality was not feasible. Third, Due to the limited number of available studies, we were unable to conduct further investigations to explore the sources of substantial heterogeneity for some outcomes with high heterogeneity. Fourth, heterogeneity in adjusted confounders across studies impedes sensitivity analyses of critical variables, potentially compromising the precision of effect size estimates. Last but not least, heterogeneity may exist in the definition of “never-smokers,” particularly regarding the consideration and extent of secondhand smoke exposure. The lack of such standardization could lead to inconsistencies in case identification and may compromise the accuracy of risk estimates associated with COPD in never-smokers. Consequently, future research should develop prospective cohorts spanning multilingual and diverse socioeconomic contexts, standardizing covariate collection to enhance global generalizability and precision of COPD mortality risk prediction.
Conclusion
This study provides the first systematic evidence demonstrating significantly elevated all-cause mortality risk in COPD patients compared with non-COPD cohorts. Tobacco exposure, coexisting cardiovascular disorders, other respiratory diseases, and malignancies (notably lung cancer) were identified as major modifiable risk factors. A progressive mortality risk gradient was strongly associated with advancing disease severity, necessitating intensified comprehensive management across all stages. Crucially, the excessive mortality risk exhibited a sex-independent pattern. Given this risk profile, public health strategies should prioritize COPD risk reduction through early identification and coordinated management of high-risk cohorts to alleviate disease burden. Collectively, these findings provide an evidence-based foundation for optimizing clinical interventions and informing health policy development.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China’s Young Scientists Fund (Grant No. 82205313, 82505808), National Key R&D Program of China (Grant No. 2023YFC3502600), Henan Province Key R&D and Promotion Program (Grant No. 252102310457, 252102310459), Henan Province Medical Science and Technology Key Project Joint Construction Program (Grant No. LHGJ20240673, LHGJ20240671), Joint Construction Research Project of the National Traditional Chinese Medicine Inheritance and Innovation Center (Grant No. 2024ZXZX1177), Special Research Project on Traditional Chinese Medicine of Henan Province (Grant No. 2025ZY2001), and Key Scientific Research Project of Higher Education Institutions in Henan Province (Grant No. 26A360003).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Vestbo J, Hurd SS, Agustí AG. et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary. Am J Respir Crit Care Med. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
2. Lopez AD, Shibuya K, Rao C, et al. Chronic obstructive pulmonary disease: current burden and future projections. Eur Respir J. 2006;27(2):397–412. doi:10.1183/09031936.06.00025805
3. World Health Organization. Chronic obstructive pulmonary disease (COPD). Available from: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-copd.
4. GBD 2021 Forecasting Collaborators. Burden of disease scenarios for 204 countries and territories, 2022-2050: a forecasting analysis for the Global Burden of Disease Study 2021. Lancet. 2024;403(10440):2204–2256. doi:10.1016/S0140-6736(24)00685-8
5. World Health Organization. Projections of mortality and causes of death, 2016 and 2060. Available from: https://colinmathers.com/2022/05/10/.
6. United Nations. Transforming our world: the 2030 Agenda for Sustainable Development. Available from: https://docs.un.org/zh/A/RES/70/1.
7. Soriano JB, Kendrick PJ, Paulson KR, GBD Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
8. World Health Organization. SDG Target 3.4 Non-communicable diseases and mental health. Available from: https://www.who.int/data/gho/data/themes/topics/sdg-target-3_4.
9. Flynn RWV, MacDonald TM, Chalmers JD, Schembri S. The effect of changes to GOLD severity stage on long term morbidity and mortality in COPD. Respir Res. 2018;19(1):249. doi:10.1186/s12931-018-0960-3
10. Lindenauer PK, Dharmarajan K, Qin L, Lin Z, Gershon AS, Krumholz HM. Risk Trajectories of Readmission and Death in the First Year after Hospitalization for Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2018;197(8):1009–1017. doi:10.1164/rccm.201709-1852OC
11. Divo M, Cote C, de Torres JP, et al. Comorbidities and risk of mortality in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2012;186(2):155–161. doi:10.1164/rccm.201201-0034OC
12. Ferrera MC, Labaki WW, Han MK. Advances in Chronic Obstructive Pulmonary Disease. Annu Rev Med. 2021;72:119–134. doi:10.1146/annurev-med-080919-112707
13. Soler-Cataluña JJ, Martínez-García MA, Román Sánchez P, Salcedo E, Navarro M, Ochando R. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax. 2005;60(11):925–931. doi:10.1136/thx.2005.040527
14. Suissa S, Dell’Aniello S, Ernst P. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67(11):957–963. doi:10.1136/thoraxjnl-2011-201518
15. Wade RC, Martinez FJ, Criner GJ, et al. ECG-based risk factors for adverse cardiopulmonary events and treatment outcomes in COPD. Eur Respir J. 2025;65(2):2400171. doi:10.1183/13993003.00171-2024
16. Zou W, Ou J, Wu F, et al. Association of mild chronic obstructive pulmonary disease with all-cause mortality: a systematic review and meta-analysis. Pulmonology. 2025;31(1):2416813. doi:10.1016/j.pulmoe.2023.09.002
17. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
18. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol. 2010;25(9):603–605. doi:10.1007/s10654-010-9491-z
19. Aldrich MC, Munro HM, Mumma M, et al. Chronic obstructive pulmonary disease and subsequent overall and lung cancer mortality in low-income adults. PLoS One. 2015;10(3):e0121805. doi:10.1371/journal.pone.0121805
20. Bhatta L, Leivseth L, Carslake D, et al. Comparison of pre- and post-bronchodilator lung function as predictors of mortality: the HUNT Study. Respirology. 2020;25(4):401–409. doi:10.1111/resp.13648
21. Cadham CJ, Oh H, Han MK, et al. The prevalence and mortality risks of PRISm and COPD in the United States from NHANES 2007-2012. Respir Res. 2024;25(1):208. doi:10.1186/s12931-024-02841-y
22. Cuthbert JJ, Kearsley JW, Kazmi S, et al. The impact of heart failure and chronic obstructive pulmonary disease on mortality in patients presenting with breathlessness. Clin Res Cardiol. 2019;108(2):185–193. doi:10.1007/s00392-018-1342-z
23. Çolak Y, Nordestgaard BG, Vestbo J, Lange P, Afzal S. Comparison of five major airflow limitation criteria to identify high-risk individuals with COPD: a contemporary population-based cohort. Thorax. 2020;75(11):944–954. doi:10.1136/thoraxjnl-2020-214559
24. Diaz-Guzman E, Khosravi M, Mannino DM. Asthma, chronic obstructive pulmonary disease, and mortality in the U.S. population. COPD. 2011;8(6):400–407. doi:10.3109/15412555.2011.611200
25. Ford ES, Mannino DM, Zhao G, Li C, Croft JB. Changes in mortality among US adults with COPD in two national cohorts recruited from 1971-1975 and 1988-1994. Chest. 2012;141(1):101–110. doi:10.1378/chest.11-0472
26. Garcia-Aymerich J, Serra Pons I, Mannino DM, Maas AK, Miller DP, Davis KJ. Lung function impairment, COPD hospitalisations and subsequent mortality. Thorax. 2011;66(7):585–590. doi:10.1136/thx.2010.152876
27. Guo C, Yu T, Chang LY, et al. Mortality risk attributable to classification of chronic obstructive pulmonary disease and reduced lung function: a 21-year longitudinal cohort study. Respir Med. 2021;184:106471. doi:10.1016/j.rmed.2021.106471
28. He D, Sun Y, Gao M, et al. Different Risks of Mortality and Longitudinal Transition Trajectories in New Potential Subtypes of the Preserved Ratio Impaired Spirometry: evidence From the English Longitudinal Study of Aging. Front Med Lausanne. 2021;8:755855. doi:10.3389/fmed.2021.755855
29. Kang HR, Kim SJ, Nam JG, Park YS, Lee CH. Impact of Smoking and Chronic Obstructive Pulmonary Disease on All-Cause, Respiratory, and Cardio-Cerebrovascular Mortality. Int J Chron Obstruct Pulmon Dis. 2024;19:1261–1272. doi:10.2147/COPD.S458356
30. Kazibwe R, Ahmad MI, Luqman-Arafat TK, Chen H, Yeboah J, Soliman EZ. Relationship between abnormal P-wave axis, chronic obstructive pulmonary disease and mortality in the general population. J Electrocardiol. 2023;79:100–107. doi:10.1016/j.jelectrocard.2023.03.085
31. Lash TL, Johansen MB, Christensen S, et al. Hospitalization rates and survival associated with COPD: a nationwide Danish cohort study. Lung. 2011;189(1):27–35. doi:10.1007/s00408-010-9274-z
32. Lindberg A, Larsson LG, Muellerova H, Rönmark E, Lundbäck B. Up-to-date on mortality in COPD - report from the OLIN COPD study. BMC Pulm Med. 2012;12:1. doi:10.1186/1471-2466-12-1
33. Mannino DM, Buist AS, Petty TL, Enright PL, Redd SC. Lung function and mortality in the United States: data from the First National Health and Nutrition Examination Survey follow up study. Thorax. 2003;58(5):388–393. doi:10.1136/thorax.58.5.388
34. Mattila T, Vasankari T, Kanervisto M, et al. Association between all-cause and cause-specific mortality and the GOLD stages 1-4: a 30-year follow-up among Finnish adults. Respir Med. 2015;109(8):1012–1018. doi:10.1016/j.rmed.2015.06.002
35. Mattila T, Vasankari T, Kauppi P, Mazur W, Härkänen T, Heliövaara M. Mortality of asthma, COPD, and asthma-COPD overlap during an 18-year follow up. Respir Med. 2023;207:107112. doi:10.1016/j.rmed.2022.107112
36. Pan J, Adab P, Jiang CQ, et al. All-cause and cause-specific mortality from restrictive and obstructive spirometric patterns in Chinese adults with and without dyspnea: guangzhou Biobank Cohort Study. Respir Med. 2019;151:66–80. doi:10.1016/j.rmed.2019.04.002
37. Park HY, Kang D, Lee H, et al. Impact of chronic obstructive pulmonary disease on mortality: a large national cohort study. Respirology. 2020;25(7):726–734. doi:10.1111/resp.13678
38. Perez-Padilla R, Wehrmeister FC, de Oca MM, et al. Outcomes for symptomatic non-obstructed individuals and individuals with mild (GOLD stage 1) COPD in a population based cohort. Int J Chron Obstruct Pulmon Dis. 2018;13:3549–3561. doi:10.2147/COPD.S175527
39. Rodríguez LA, Wallander MA, Martín-Merino E, Johansson S. Heart failure, myocardial infarction, lung cancer and death in COPD patients: a UK primary care study. Respir Med. 2010;104(11):1691–1699. doi:10.1016/j.rmed.2010.04.018
40. Skajaa N, Laugesen K, Horváth-Puhó E, Sørensen HT. Comorbidities and mortality among patients with chronic obstructive pulmonary disease. BMJ Open Respir Res. 2023;10(1):e001798. doi:10.1136/bmjresp-2023-001798
41. Stavem K, Sandvik L, Erikssen J. Can global initiative for Chronic Obstructive Lung Disease stage 0 provide prognostic information on long-term mortality in men? Chest. 2006;130(2):318–325. doi:10.1378/chest.130.2.318
42. van Gestel YR, Hoeks SE, Sin DD, et al. COPD and cancer mortality: the influence of statins. Thorax. 2009;64(11):963–967. doi:10.1136/thx.2009.116731
43. Washio Y, Sakata S, Fukuyama S, et al. Risks of Mortality and Airflow Limitation in Japanese Individuals with Preserved Ratio Impaired Spirometry. Am J Respir Crit Care Med. 2022;206(5):563–572. doi:10.1164/rccm.202110-2302OC
44. Wijnant SRA, De Roos E, Kavousi M, et al. Trajectory and mortality of preserved ratio impaired spirometry: the Rotterdam Study. Eur Respir J. 2020;55(1):1901217. doi:10.1183/13993003.01217-2019
45. Zou W, Ou J, Wu F, et al. Risk of All-Cause Mortality in Mild Chronic Obstructive Pulmonary Disease: evidence From the NHANES III and 2007-2012. Int J Chron Obstruct Pulmon Dis. 2025;20:217–229. doi:10.2147/COPD.S497634
46. Boers E, Barrett M, Su JG, et al. Global Burden of Chronic Obstructive Pulmonary Disease Through 2050. JAMA Network Open. 2023;6(12):e2346598. doi:10.1001/jamanetworkopen.2023.46598
47. Halpin DMG. Mortality of patients with COPD. Expert Rev Respir Med. 2024;18(6):381–395. doi:10.1080/17476348.2024.2375416
48. GBD 2019 Chronic Respiratory Diseases Collaborators. Global burden of chronic respiratory diseases and risk factors, 1990-2019: an update from the Global Burden of Disease Study 2019. EClinicalMedicine. 2023;59:101936. doi:10.1016/j.eclinm.2023.101936
49. Goldcopd. Global Strategy For Prevention, Diagnosis And Management Of Copd: 2025 Report. Available from: https://goldcopd.org/2025-gold-report/.
50. Siddharthan T, Pollard SL, Quaderi SA, et al. Discriminative Accuracy of Chronic Obstructive Pulmonary Disease Screening Instruments in 3 Low- and Middle-Income Country Settings. JAMA. 2022;327(2):151–160. doi:10.1001/jama.2021.23065
51. Karloh M, Fleig Mayer A, Maurici R, Pizzichini MMM, Jones PW, Pizzichini E. The COPD Assessment Test: what Do We Know So Far?: a Systematic Review and Meta-Analysis About Clinical Outcomes Prediction and Classification of Patients Into GOLD Stages. Chest. 2016;149(2):413–425. doi:10.1378/chest.15-1752
52. Crisafulli E, Sartori G, Huerta A, et al. Association Between Rome Classification Among Hospitalized Patients With COPD Exacerbations and Short‑Term and Intermediate‑Term Outcomes. Chest. 2023;164(6):
53. Celli BR. Predictors of mortality in COPD. Respir Med. 2010;104(6):773–779. doi:10.1016/j.rmed.2009.12.017
54. Booth S, Hsieh A, Mostaco-Guidolin L, et al. A Single-Cell Atlas of Small Airway Disease in Chronic Obstructive Pulmonary Disease: a Cross-Sectional Study. Am J Respir Crit Care Med. 2023;208(4):472–486. doi:10.1164/rccm.202303-0534OC
55. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report GOLD Executive Summary. Am J Respir Crit Care Med. 2017. 195(5):557–582. doi:10.1164/rccm.201701-0218PP
56. Kamal R, Srivastava AK, Kesavachandran CN. Meta-analysis approach to study the prevalence of chronic obstructive pulmonary disease among current, former and non-smokers. Toxicol Rep. 2015;2:1064–1074. doi:10.1016/j.toxrep.2015.07.013
57. Cook SF, Hirschtick JL, Fleischer NL, et al. Cigarettes, ENDS Use, and Chronic Obstructive Pulmonary Disease Incidence: a Prospective Longitudinal Study. Am J Prev Med. 2023;65(2):173–181. doi:10.1016/j.amepre.2023.01.038
58. Josephs L, Culliford D, Johnson M, Thomas M. Improved outcomes in ex-smokers with COPD: a UK primary care observational cohort study. Eur Respir J. 2017;49(5):1602114. doi:10.1183/13993003.02114-2016
59. Upadhyay P, Wu CW, Pham A, et al. Animal models and mechanisms of tobacco smoke-induced chronic obstructive pulmonary disease (COPD). J Toxicol Environ Health B Crit Rev. 2023;26(5):275–305. doi:10.1080/10937404.2023.2208886
60. Hikichi M, Mizumura K, Maruoka S, Gon Y. Pathogenesis of chronic obstructive pulmonary disease (COPD) induced by cigarette smoke. J Thorac Dis. 2019;11(Suppl 17):S2129–S2140. doi:10.21037/jtd.2019.10.43
61. Lu Z, Van Eeckhoutte HP, Liu G, et al. Necroptosis Signaling Promotes Inflammation, Airway Remodeling, and Emphysema in Chronic Obstructive Pulmonary Disease. Am J Respir Crit Care Med. 2021;204(6):667–681. doi:10.1164/rccm.202009-3442OC
62. GBD 2021 Tobacco Forecasting Collaborators. Forecasting the effects of smoking prevalence scenarios on years of life lost and life expectancy from 2022 to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet Public Health. 2024;9(10):e729–e744. doi:10.1016/S2468-2667(24)00166-X
63. Shin SH, Kim T, Kim H, Cho J, Kang D, Park HY. Impact of smoking reduction on lung cancer risk in patients with COPD who smoked fewer than 30 pack-years: a nationwide population-based cohort study. Respir Res. 2024;25(1):133. doi:10.1186/s12931-024-02741-1
64. Barnes PJ, Celli BR. Systemic manifestations and comorbidities of COPD. Eur Respir J. 2009;33(5):
65. Chen W, Thomas J, Sadatsafavi M, FitzGerald JM. Risk of cardiovascular comorbidity in patients with chronic obstructive pulmonary disease: a systematic review and meta-analysis. Lancet Respir Med. 2015;3(8):631–639. doi:10.1016/S2213-2600(15)00241-6
66. Caprino R, Sartori G, Sartori F, Fantin A, Crisafulli E. Factors associated with risk of death in hospitalized patients for exacerbation of chronic obstructive pulmonary disease: an updated scoping review. Expert Rev Respir Med. 2024;18(6):435–445. doi:10.1080/17476348.2024.2375426
67. Mannino DM, Thorn D, Swensen A, Holguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 2008;32(4):962–969. doi:10.1183/09031936.00012408
68. Sin DD, Anthonisen NR, Soriano JB, Agusti AG. Mortality in COPD: role of comorbidities. Eur Respir J. 2006;28(6):
69. Fabbri LM, Celli BR, Agustí A, et al. COPD and multimorbidity: recognising and addressing a syndemic occurrence. Lancet Respir Med. 2023;11(11):1020–1034. doi:10.1016/S2213-2600(23)00261-8
70. Wang M, Lin EP, Huang LC, Li CY, Shyr Y, Lai CH. Mortality of Cardiovascular Events in Patients With COPD and Preceding Hospitalization for Acute Exacerbation. Chest. 2020;158(3):973–985. doi:10.1016/j.chest.2020.02.046
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.