Back to Journals » Drug Design, Development and Therapy » Volume 20
Alfentanil May Reduce Early Postoperative Nausea and Vomiting in Moderate-to-High Risk Patients Undergoing Gastrointestinal Endoscopy: A Prospective Double-Blind Randomized Study
Authors Gu XY ![]() , Cao JF, Zhang XY, Cheng Y, Jiang LQ, Ma L
, Cao JF, Zhang XY, Cheng Y, Jiang LQ, Ma L ![]()
Received 30 January 2026
Accepted for publication 13 May 2026
Published 20 May 2026 Volume 2026:20 598415
DOI https://doi.org/10.2147/DDDT.S598415
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leonidas Panos
Xiao-Yu Gu,1,2 Jin-Feng Cao,2 Xin-Yang Zhang,2 Yao Cheng,2 Liu-Qin Jiang,2 Lei Ma1
1Department of Anesthesiology, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China; 2Department of Anesthesiology, NO.215 Hospital of Shaanxi Nuclear Industry, Xianyang, People’s Republic of China
Correspondence: Lei Ma, Department of Anesthesiology, The Second Affiliated Hospital of Xi’an Jiaotong University, No. 157, Xi Wu Road, Xi’an, 710004, People’s Republic of China, Email [email protected] Liu-Qin Jiang, Department of Anesthesiology, NO.215 Hospital of Shaanxi Nuclear Industry, No. 35 Wei-Yang West Road, Xianyang, 712000, People’s Republic of China, Email [email protected]
Objective: This trial aimed to compare the effects of alfentanil and sufentanil on postoperative nausea and vomiting (PONV) in patients at moderate-to-high risk undergoing sedated gastrointestinal endoscopy.
Methods: Two hundred and eighteen patients were randomized to receive either alfentanil (6.7 μg/kg) or sufentanil (0.1 μg/kg) combined with propofol. The primary outcome was the incidence of PONV within 24 hours postoperatively. Other outcomes included PONV in the post-anesthesia care unit (PACU) and at 48 hours, hemodynamic profiles, induction and recovery times, propofol consumption, and other adverse events.
Results: The 24-hour PONV incidence did not differ significantly between groups (0.95% vs. 3.85%, p=0.21). However, during the PACU stay, the alfentanil group had a significantly lower incidence of PONV (0.95% vs. 7.69%, p=0.02) and lower PONV scores (p=0.02). Alfentanil also resulted in a significantly shorter induction time (p< 0.01) and more stable intraoperative hemodynamics. The total propofol dose, examination duration, PACU discharge time, and incidence of other adverse events were comparable between groups.
Conclusion: For patients at moderate-to-high risk of PONV undergoing sedated endoscopy, alfentanil may associate with a significant reduction in early PONV and faster induction compared to sufentanil, without increasing propofol requirements or other clinical risks. Although the 24-hour PONV risk appeared similar, the improvement in early recovery quality suggests that alfentanil may be a favorable option for efficient sedation. These findings are preliminary and warrant confirmation in larger trials.
Keywords: PONV, alfentanil, sufentanil, painless gastroenteroscopy, Apfel score
Background
Postoperative nausea and vomiting (PONV) is one of the most undesirable adverse events following surgery.1 It can significantly prolong a patient’s stay in the post-anesthesia care unit (PACU). Studies have shown that each episode of vomiting delays discharge by approximately 20 minutes on average, which not only increases additional nursing time and medication use but also severely impacts the patient’s recovery experience. The incidence of PONV is approximately 30% in the general surgical population and can be as high as 80% in high-risk groups.2 The increased risk of PONV is associated with multiple factors, including pediatric patients, female sex, a history of PONV or motion sickness, non-smoking status, and the use of volatile anesthetics and postoperative opioids. Among these, young, non-smoking women undergoing brief outpatient procedures (eg, gastrointestinal endoscopy or hysteroscopy) represent a group that concentrates multiple high-risk features. Consequently, this population exhibits a persistently high incidence of PONV and is widely recognized as a high-risk cohort.3 For outpatient patients undergoing painless gastrointestinal endoscopy, persistent vomiting after discharge may lead to serious consequences such as dehydration, electrolyte imbalances, and an increased risk of bleeding (eg., after polypectomy). Even in mild cases, it may delay the resumption of oral intake, physical activity, and normal function, thereby affecting the overall recovery process. Severe PONV can cause anxiety, fear, and psychological distress regarding future surgeries. The simplified risk score developed by Apfel et al is a clinical tool that integrates key risk factors to estimate the probability of PONV, with a diagnostic performance of approximately 65–70% in both sensitivity and specificity.4 This scoring system incorporates four risk factors:5 (1) female gender, (2) history of motion sickness or previous PONV, (3) non-smoker status, and (4) planned postoperative opioid use. Each present factor contributes one point, yielding a total score ranging from 0 to 4, which correlates with the following estimated PONV risks: 0 points (~10%), 1 point (~20%), 2 points (~40%), 3 points (~60%), and 4 points (~80%). Patients with a score of ≥2 are classified as being at moderate to high risk for PONV.2 While propofol is indeed the cornerstone agent for procedural sedation due to its favorable recovery profile and intrinsic antiemetic properties, its use as a monotherapy has limitations.6 Propofol provides minimal analgesia, and the intense noxious stimulation during endoscope insertion and maneuvering can lead to inadequate sedation, patient movement, coughing, or hemodynamic instability, potentially compromising procedure safety and success. Therefore, common practice supports the combination of propofol with a short-acting opioid analgesic to provide balanced sedation-analgesia, reducing propofol requirements and improving procedural conditions.
Currently, there is a lack of multicenter, large-scale studies on the incidence of nausea and vomiting following painless gastroenteroscopy. However, some scholars suggest that the rate of postoperative nausea and vomiting (PONV) associated with sufentanil combined with propofol ranges from 10% to 25%.7–9 This reported incidence remains clinically significant, especially in the high-risk populations defined above. The adverse reaction may tend to affect recovery quality and cause significant discomfort after painless gastroenteroscopy. Thus, the central clinical dilemma is not whether to use an opioid, but how to select an opioid that minimizes its contribution to PONV while effectively facilitating the procedure.
Alfentanil is a short-acting opioid analgesic. As a fentanyl analog, it possesses one-tenth the potency of fentanyl but exhibits a significantly faster onset of action, achieving a peak effect within 1.4 minutes after intravenous administration.10 These properties make it a particularly appealing agent for procedural sedation during gastrointestinal endoscopy. Its rapid onset (as quick as 45 seconds) and a duration of analgesia of approximately 15 minutes are well-suited to the timeframe of bidirectional endoscopy.11 Furthermore, its rapid recovery profile, due to a high metabolic clearance rate, is ideal for outpatient settings.12 Clinically, alfentanil has also been associated with a favorable safety profile, including hemodynamic stability and a lower incidence of respiratory depression, nausea, and vomiting compared to equipotent doses of fentanyl.13,14
Based on its favorable pharmacokinetic and safety profile, we hypothesized that alfentanil would be associated with a lower incidence of PONV compared to sufentanil in patients at moderate-to-high risk undergoing gastrointestinal endoscopy. To test this hypothesis, we conducted a randomized controlled trial to determine whether alfentanil represents a more suitable opioid choice for this patient population.
Methods
Study Design and Ethics
This study was designed as a single-center, double-blind, randomized controlled trial. Patients were randomly allocated to either the sufentanil or alfentanil group in a 1:1 ratio using a computer-generated randomization sequence. Allocation concealment was ensured by storing the sequence in sealed envelopes accessible only to nursing staff not involved in the study. A double-blind design was implemented. Both participants and investigators were blinded to group assignments. The study medications were prepared in identical transparent solutions labeled only with study identification numbers. Investigators administered the designated “analgesic agent” without knowledge of its identity and recorded intraoperative data accordingly.
It was approved by the Ethics Committee of NO.215 Hospital of Shaanxi Nuclear Industry [approval number:2024(045)] and registered with the Chinese Clinical Trial Registry (Registration Number: ChiCTR2400093509). Written informed consent was obtained from all individual participants included in the study. All procedures adhered to the Declaration of Helsinki.
Patients
This study enrolled outpatients who underwent painless gastroenteroscopy between December 2024 and September 2025. The inclusion criteria were as follows: (1) outpatients scheduled for a combined gastroenteroscopy procedure, which included both gastroscopy and colonoscopyduring the same session; (2) an Apfel score of 2 to 4; (3) age between 18 and 64 years. The exclusion criteria included: (1) patients undergoing special therapeutic procedures, such as polypectomy; (2) long-term use of opioid medications; (3) long-term use of antiemetic drugs; (4) history of allergy to general anesthetics; (5) severe hepatic or renal dysfunction; (6) American Society of Anesthesiologists (ASA) physical status classification greater than III.
Interventions
All enrolled patients were randomly allocated into two groups: a sufentanil group and an alfentanil group. Patients in both groups underwent a standardized fasting protocol, abstaining from clear fluids for 3 hours and solid foods for 8 hours prior to the procedure. Upon arrival in the procedure room, all patients received supplemental oxygen via a nasal cannula at a flow rate of 5 L/min. Standard monitoring was established, including electrocardiography (ECG), oxygen saturation (SpO2), non-invasive blood pressure (NIBP) and respiratory rate (RR). Patients in the sufentanil group received an intravenous bolus of sufentanil (Yichang Renfu Pharmaceutical Co., Ltd., China) at 0.1 μg/kg, while those in the alfentanil group received alfentanil (Yichang Renfu Pharmaceutical Co., Ltd., China) at 6.7 μg/kg (sufentanil and alfentanil doses were converted to equivalent morphine equivalents). Following this, propofol (Xi’an Libang Pharmaceutical Co., Ltd., China) was administered intravenously at a slow injection rate of 1–1.5 mg/kg to both groups. The gastroscopy procedure was initiated once a Modified Observer’s Assessment of Alertness/Sedation (MOAA/S) score of less than 1 (no response to painful stimulus) was achieved.
All patients were transferred to the PACU for observation following the completion of gastroenteroscopy. Patients were eligible for discharge from the hospital upon achieving an Aldrete score of ≥9. Telephone follow-ups were conducted for all patients at 24 and 48 hours after the procedure to assess the occurrence of any adverse effects, including PONV (assessed using a standardized PONV scoring tool)15 and other specific discomforts.
Hypotension was defined as either a systolic blood pressure (SBP) below 90 mmHg or a reduction of more than 20% from the baseline value. In cases of hypotension, dopamine was administered intravenously at a dose of 1–2 mg. Bradycardia was defined as a heart rate (HR) less than 55 beats per minute or a decrease exceeding 20% from baseline accompanied by hypotension. Atropine (0.3–0.5 mg) was administered if the heart rate fell below 50 beats per minute. Hypoxemia was defined as SpO2 below 90% for more than 10 seconds,16 while respiratory depression was defined as a RR below 6 breaths per minute.17 For episodes of hypoxemia or respiratory depression, initial management included increasing the oxygen flow rate to 8–10 L·min−1 and performing airway maneuvers such as head tilt–chin lift or jaw thrust. In severe cases, mask-assisted positive-pressure ventilation was implemented.
Sample Size Calculation
Based on the results of the preliminary trial and previously published literature citing a PONV incidence of up to 22% with sufentanil-propofol sedation, we estimated a sample size of 198 patients in this study using G*Power 3.1, which had a statistical power (1-β) of 0.8, a two-sided test with α = 0.05, an expected incidence rate of 0.08 in the experimental group (p1), and 0.22 in the control group (p2). With zα/2 = 1.95996, zβ = 0.84162, and an allocation ratio (k) of 1. Accounting for an anticipated dropout rate of 10%, the final required total sample size was increased to 218 subjects.
It should be noted that the actual observed incidence in the control group was considerably lower than the estimate used for this calculation. This discrepancy and its implications for the study’s statistical power are discussed in the Limitations section.
Statistical Analysis
Statistical analyses were performed using SPSS version 27.0 (SPSS Inc., Chicago, IL, USA). Normality of continuous data was tested using the Shapiro–Wilk test. For those meeting the normality assumption, homogeneity of variances was further examined using Levene’s test prior to parametric comparisons. Data are presented as mean ± standard deviation (SD) for normally distributed continuous variables, which were compared using the independent samples t-test, while non-normally distributed continuous variables are expressed as median with interquartile range (IQR) and were compared with the Mann–Whitney U-test. Categorical variables, presented as number (percentage), were analyzed using the Chi-squared test or Fisher’s exact test when expected frequencies were <5. For all low-incidence binary outcomes, Fisher’s exact test was used; details are given in the table footnotes. A two-sided p-value < 0.05 was considered statistically significant.
Patient Characteristics
Baseline characteristics, including age, BMI, Apfel score, ASA physical status, personal habits (smoking and alcohol consumption), and medical history (hypertension, diabetes, coronary heart disease, hypothyroidism, and surgical history) were compared between the two groups. The groups were well-balanced at baseline, with no statistically significant differences in these demographics and clinical characteristics (all p > 0.05) (Table 1).
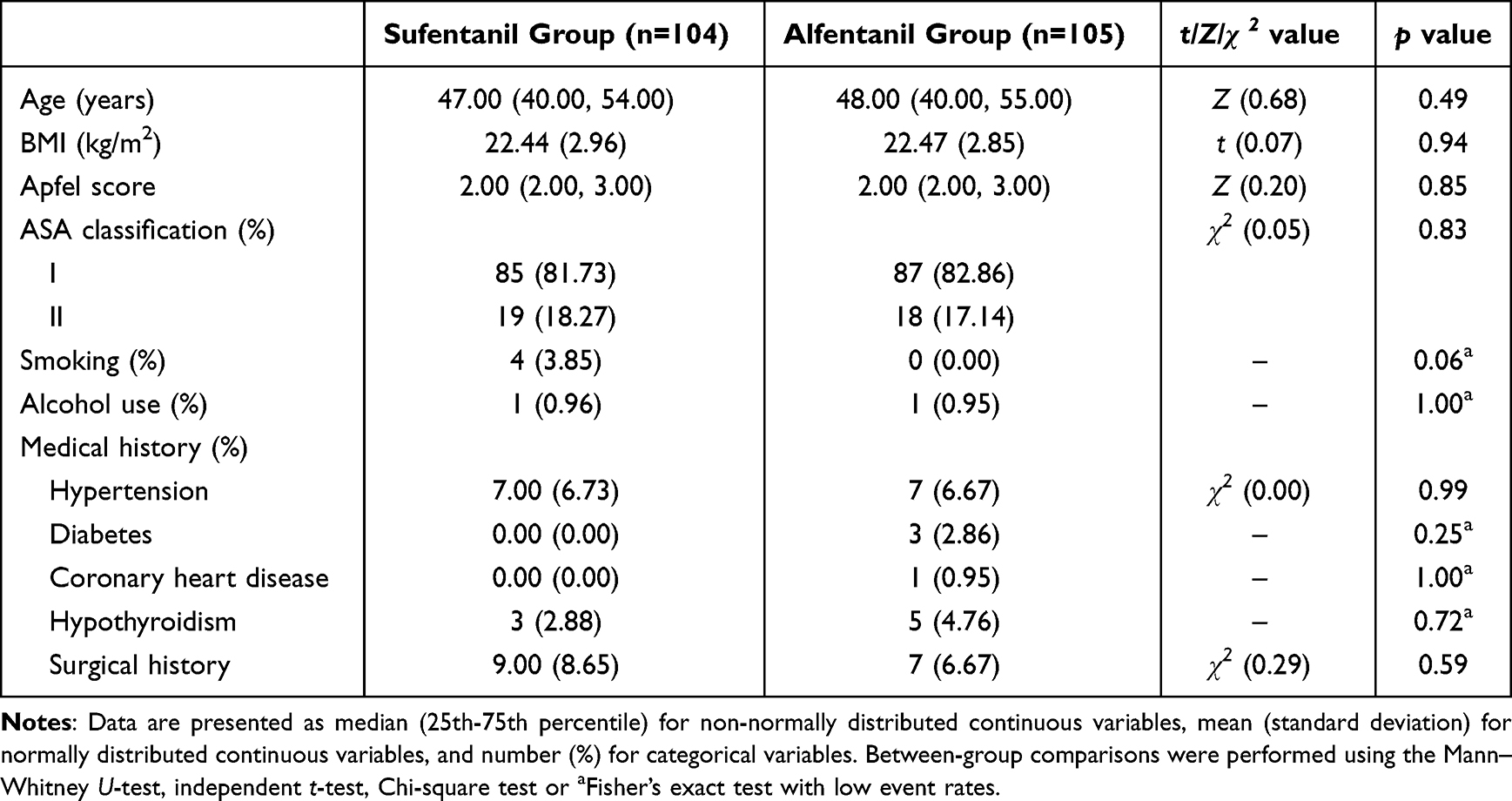 |
Table 1 Characteristics of Patients |
Outcomes
Primary outcomes
The incidence of postoperative nausea and vomiting (PONV) within 24 hours, defined as a PONV score15 ≥ 1.
Other Outcomes
- PONV scores at PACU, 24 and 48 hours postoperatively; the incidence of PONV at PACU and 48 hours.
- Hemodynamic and respiratory parameters during the procedure, including HR, SpO2, non-invasively measured mean arterial pressure (MAP), and RR at different time points (T0 is the time upon entering the operation room; T1 is the time of post-induction; T2 is the time upon endoscopic insertion into the esophagus; T3 is the time at the end of the; T4 is the time of upon recovery).
- Perioperative procedural data, including induction time, examination duration, and the induction and total doses of propofol, were recorded and compared. Additionally, recovery parameters such as the time to discharge from the post-anesthesia care unit (from the end of examination to departure) was also analyzed.
- Procedure-related Adverse Events: The incidence of intraoperative adverse events, including hiccups, coughing, body movement, hypotension, hypoxemia, respiratory depression, and bradycardia. The rescue dose of granisetron was also analyzed.
Results
Of the 218 patients enrolled, 108 were allocated to receive sufentanil and 110 to alfentanil. In the sufentanil group, five patients were excluded from analysis (one lost to follow-up, two requiring hospitalizations for polypectomy, and two with protocol deviations). In the alfentanil group, four patients were lost to follow-up. Consequently, the final analysis comprised 104 patients in the sufentanil group and 105 in the alfentanil group (Figure 1).
 |
Figure 1 The flowchart of the study. |
Primary Result
Contrary to our primary hypothesis, there was no statistically significant difference in the 24-hour incidence of PONV between the alfentanil group (0.95%) and the sufentanil group (3.85%) (p = 0.21, Fisher’s exact test) (Table 2).
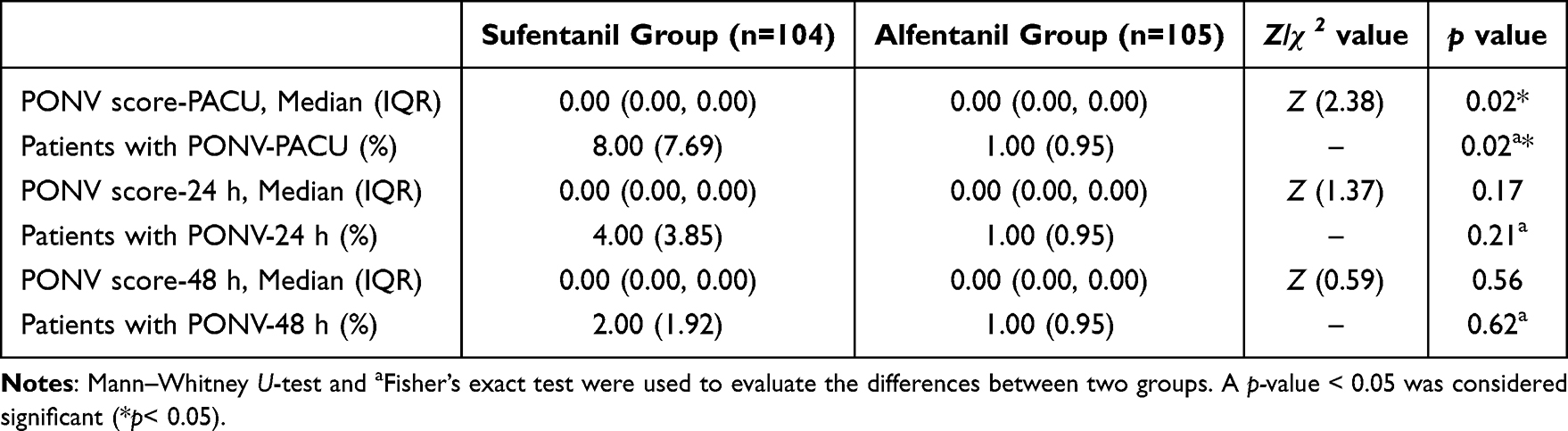 |
Table 2 Postoperative Adverse Events Data |
A post hoc power analysis was performed based on the actual observed incidence rates (0.95% vs. 3.85%) and sample sizes. Using a two-sided Fisher’s exact test with α=0.05, the achieved statistical power to detect this difference was 26.5%.
Other Results
- PONV scores (Z = 2.38, p = 0.02) and the incidence of PONV (p = 0.02, Fisher’s exact test) were significantly lower in the alfentanil group (0.95%) compared with sufentanil group (7.69%) during the PACU stay. However, no statistically significant differences were observed between the groups at 24 and 48 hours postoperatively (p > 0.05) (Table 2).
- The values of HR, SpO2, MAP and RR exhibited dynamic changes from baseline T0 in both groups. In both sufentanil and alfentanil group, HR, MAP, SpO2 and RR showed significant fluctuations, different from their T0 baseline at multiple time points (p < 0.05). The sufentanil group demonstrated a more pronounced reduction in SpO2 compared to the alfentanil group (Figure 2).
- The induction time was significantly shorter in the alfentanil group than in the sufentanil group (Figure 3A, Z = 3.03, p < 0.01). In contrast, there were no significant differences between the groups in examination duration, emergence time, or time to discharge from the PACU (Figure 3B–D, p > 0.05). Similarly, the induction and total doses of propofol were comparable between the two groups (Figure 3E and F, p > 0.05).
- A comparison of intraoperative adverse events revealed no statistically significant differences between the sufentanil and alfentanil groups for any specific event, including hiccups, coughing, body movement, hypotension, hypoxemia and respiratory depression (p > 0.05, Table 3). Notably, a non-significant trend was observed in the consumption of the rescue antiemetic granisetron (p > 0.05, Table 3). Additionally, no episodes of severe bradycardia were observed in either group.
- Post Hoc Subgroup Analysis by Apfel Score.
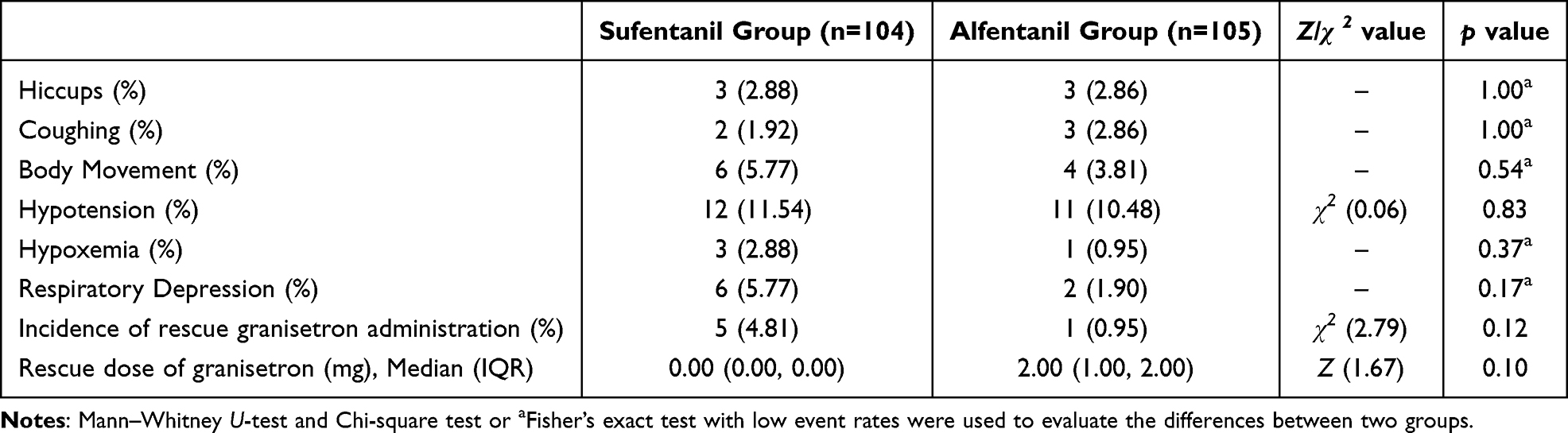 |
Table 3 Intraoperative Adverse Events Data and Rescue Dose of Granisetron |
 |
Figure 2 Hemodynamic parameters, including HR (A), SpO2 (B), MAP (C) and RR (D), at different time points in two groups. Data are presented as median (IQR). Friedman test was applied to assess overall differences across time points. When significant effects were detected (p < 0.05), post hoc pairwise comparisons were conducted using Wilcoxon signed-rank tests with Bonferroni correction for multiple comparisons (adjusted α=0.01). * means statistically significant differences versus T0 in sufentanil group: p<0.05 (corrected). # means statistically significant differences versus T0 in alfentanil group: p<0.05 (corrected). T0 is the time upon entering the operation room (baseline); T1 is the time of post-induction; T2 is the time upon endoscopic insertion into the esophagus; T3 is the time at the end of the examination; T4 is the time of upon recovery. Abbreviations: HR, heart rates; SpO2, oxygen saturation; MAP, mean arterial pressure; RR, respiratory rate. |
 |
Figure 3 Comparison of procedural timings and propofol consumption, including introduction time (A), examination duration (B), emergence time (C), PACU discharge time (D), induction propofol dosage (E), and total propofol dosage (F) between the sufentanil and alfentanil groups. Group comparisons were performed using Mann‑Whitney U tests. p < 0.05 was considered statistically significant. Abbreviation: PACU, post‑anesthesia care unit. |
To examine the potential effect modification by baseline risk, a post hoc analysis stratifying patients in PACU by Apfel score was conducted, consistent with the principle of risk-stratified PONV management.18
Among patients with an Apfel score of 2 (moderate risk), the incidence of PONV was 0% in the alfentanil group, compared to 7.69% in the sufentanil group (p = 0.03, Fisher’s exact test; RR = 0.92, 95% CI: 0.86 to 0.99) (Figure 4). In the subgroup of patients with an Apfel score of 3 (high risk), the incidence of PONV was 5.26% in the alfentanil group, compared to 15.38% in the sufentanil group (p = 0.26, Fisher’s exact test) (Figure 4). With the sufentanil group as the reference, the relative risk for “PONV not occurring” in the alfentanil group was 0.89 (95% CI: 0.77 to 1.04). Since the confidence interval includes 1, this risk reduction was not statistically significant.
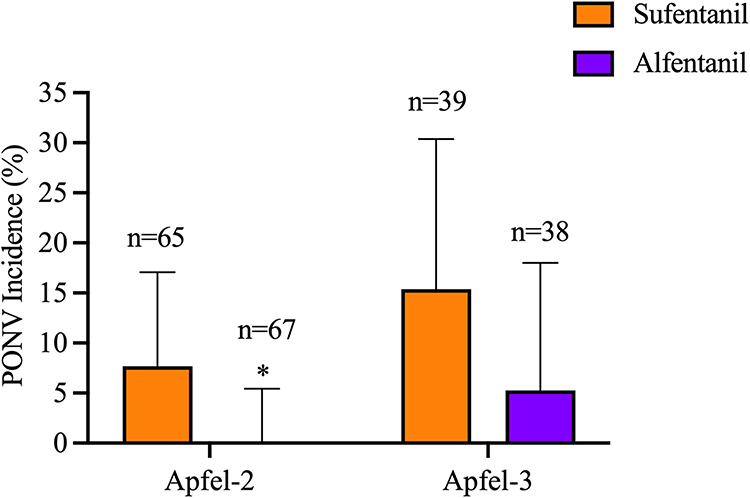 |
Figure 4 PONV incidence in the PACU Stratified by Apfel Score (Post Hoc Analysis). Data are presented as percentage incidence with 95% confidence intervals (error bars). The number of patients (n) in each subgroup is indicated above the corresponding bar. Between-group comparisons within each Apfel score stratum were performed using Fisher’s exact test. *p < 0.05 was considered statistically significant. |
Discussion
Given the acknowledged role of opioids as a key risk factor for PONV and the challenge of isolating their independent effects in clinical research, this study was framed within the concept of opioid-associated PONV (O-PONV).19 To address this, a standardized protocol was designed to directly compare two opioid regimens—alfentanil versus sufentanil—on the risk of PONV when administered atop a uniform propofol-based sedation in patients at moderate-to-high risk undergoing gastrointestinal endoscopy. It demonstrated that alfentanil significantly reduced early PONV in the PACU compared to sufentanil. However, this advantage did not extend to the postoperative 24 and 48-hour periods, during which the incidence of PONV was comparable between the two groups. As the study to focus specifically on this at-risk population, our findings provide valuable insights for rational opioid selection in this clinical context.
Contrary to our initial hypothesis that alfentanil would reduce the 24-hour incidence of PONV in patients at moderate-to-high risk, our findings revealed a more nuanced temporal effect. Specifically, alfentanil significantly reduced early PONV in the PACU compared to sufentanil. However, this advantage did not extend to the 24-hour period following discharge. This time-limited effect can be attributed to the distinct pharmacokinetic profile of alfentanil. With its rapid onset and ultra-short duration of action, the emetogenic effect of alfentanil dissipates more quickly after discontinuation. Consequently, patients in the alfentanil group experienced significantly less PONV during the critical early recovery phase in the PACU, thereby enhancing immediate post-procedure comfort. In line with the findings of Lei et al20 in daytime hysteroscopy, where the alfentanil group demonstrated a lower incidence and severity of PONV at 2 hours postoperatively compared to the sufentanil group, our study also observed a consistent early PONV reduction with alfentanil.
Interestingly, despite the reduction in early PONV, the time to discharge from the PACU did not differ significantly between the two groups. A plausible explanation is that although the incidence of PONV was higher in the sufentanil group, the severity of episodes was comparable. More importantly, a standardized rescue protocol was implemented wherein any patient with a PONV score ≥2 promptly received granisetron. This approach aligns with the key recommendation from the Fifth PONV Consensus Guidelines21 to “provide antiemetic treatment to patients with PONV who did not receive prophylaxis or when prophylaxis failed”. The timely administration of rescue treatment from a different pharmacological class likely mitigated subsequent symptoms, which is the most probable reason why the early reduction in PONV with alfentanil did not translate into a difference in long-term outcomes at 24 hours.22 With the exception of two patients in the sufentanil group who experienced prolonged stays (35 and 79 minutes, respectively), all other patients in both groups were discharged within 30 minutes, indicating that isolated severe episodes, rather than the overall rate of PONV, were the primary determinant of delayed discharge in this group.
The pathophysiology of PONV is time-dependent. Early PONV in the PACU is primarily driven by residual anesthetic effects and the direct stimulation of gastrointestinal endoscopy, whereas late PONV within 24 hours post-discharge is influenced by a different set of factors, including the initiation of oral intake, restoration of bowel function, postoperative pain, ambulation, and the use of oral opioid analgesics.2 The absence of a long-term benefit with alfentanil can be understood through a confluence of clinical and methodological insights. First, the implementation of a standardized rescue protocol, wherein any patient with a PONV score ≥2 received prompt granisetron, effectively mitigated subsequent symptoms in the sufentanil group after PACU discharge. This proactive management neutralized the theoretical late PONV risk associated with sufentanil, thereby equilibrating the 24-hour outcomes between the groups. Second, and critically, a post hoc power analysis based on the actually observed, much lower incidence rates (sufentanil: 3.85% vs. alfentanil: 0.95%) yielded a statistical power of only 26.5% for the primary 24-hour PONV comparison. This underscores a key methodological insight: historical PONV incidence rates (around 20–25%) cited in earlier literature for similar sedation protocols6–8 may no longer reflect current clinical reality, likely due to advancements in standardized perioperative management. Consequently, our study was underpowered. The observed statistical equivalence at 24 hours therefore cannot be interpreted as definitive evidence of clinical equipoise but rather as an inconclusive finding that warrants verification in a study designed with a more contemporary estimate of baseline risk.
Notably, our observation of PONV at the 48-hour revealed an intriguing phenomenon. Although the overall incidence was very low and did not differ between the sufentanil (n=2) and alfentanil (n=1) groups, the three affected patients all developed mild symptoms (PONV score=1) exclusively in the 24–48-hour window, reporting no nausea in the first 24 hours. This clinical picture is characteristic of late-onset PONV, which is driven by pathophysiological mechanisms distinct from those of early PONV. While early PONV primarily stems from residual anesthetic effects and acute procedural stimulation, late-onset PONV is typically associated with factors emerging during the resumption of daily activities.2 These include: (1) the postoperative use of oral opioid analgesics, a well-established trigger; (2) the restoration of gastrointestinal function and dietary intake; and (3) increased ambulation, which may affect the vestibular system or induce orthostatic hypotension. This pattern further corroborates our central conclusion: the ultra-short duration of action of alfentanil precludes any protective effect against PONV triggered by these novel, late-phase factors. Consequently, both groups reverted to an identical, very low baseline risk level at 48 hours. From a clinical perspective, the minimal PONV burden observed at this late time point, with all cases being mild and self-limiting without rescue medication, suggests that the overall long-term PONV burden in this at-risk population is low within an optimized enhanced recovery pathway. Nevertheless, the low frequency of these events precludes robust statistical comparison in our cohort, warranting attention in future larger-scale studies.
The subgroup analysis of this study suggests that the protective effect of alfentanil against PONV may be risk-stratification-dependent. In patients with an Apfel score of 2, alfentanil significantly reduced the risk of PONV, corresponding to a relative risk reduction of 7.7%. It has been noted in reviews that alfentanil is associated with a lower incidence of nausea and vomiting compared to opioids like fentanyl.23 However, in high-risk patients with an Apfel score of 3, this effect did not reach statistical significance. The wide confidence interval indicates that the current sample size may be insufficient to detect a true difference in this subgroup, or it may imply that in a very high-risk context, inter-drug differences are obscured by other dominant factors.24 In summary, alfentanil shows a clear protective trend in moderate-risk patients, but its benefit in high-risk patients requires further validation in larger studies. This highlights the need to tailor clinical choices based on individual patient risk assessment.
Furthermore, this study revealed a significantly shorter induction time in the alfentanil group compared to the sufentanil group, directly reflecting alfentanil’s pharmacological advantage of rapid onset and establishing an efficient start to the procedure.25 Notably, the total examination duration and total propofol consumption were comparable between the two groups. This observation indicates that comparable depths of sedation were achieved and that the procedural stimulation and complexity were similar, thereby excluding these factors as potential confounders for recovery outcomes such as PONV. Throughout the procedure, the alfentanil group demonstrated a more stable hemodynamic profile, a finding that is robustly supported by a recent direct comparative randomized trial.20,26 Regarding safety, the incidence of specific adverse events, including hypotension, respiratory depression, body movement, and coughing, did not differ significantly between the groups. This finding confirms that the superior early recovery quality provided by alfentanil was not achieved at the expense of additional clinical risks, indicating an overall comparable safety profile to sufentanil.
Several limitations should be considered. First and foremost, the statistical power was substantially lower than planned. The sample size calculation was based on an estimated control group PONV incidence of 22%, derived from historical data. The actual observed incidence was 3.85%, leading to a post hoc power of only 26.5% for the primary outcome. This severely limits the ability to draw definitive conclusions regarding the equivalence of the two regimens for 24-hour PONV, as the study was underpowered to detect a clinically meaningful difference if one existed. Therefore, the non-significant finding for the primary endpoint should be interpreted as inconclusive rather than evidence of no difference. Second, the single-center nature of this trial may affect the external validity of our conclusions, necessitating confirmation from multi-center studies. Finally, the sample size provides limited power to statistically compare the incidence of uncommon adverse events. Therefore, larger, multi-center trials are required to robustly assess potential differences in the safety profiles of alfentanil and sufentanil.
Conclusion
In conclusion, this randomized trial demonstrates that in patients at moderate-to-high risk of PONV undergoing sedated gastrointestinal endoscopy, alfentanil was associated with a statistically significant reduction in early PONV during the PACU stay and a more rapid anesthesia induction compared to sufentanil, without increasing propofol requirements or other immediate clinical risks. However, the study was underpowered to detect a difference in the primary endpoint of 24-hour PONV due to a substantially lower-than-anticipated baseline event rate. Therefore, the finding of no significant difference at 24 hours should be interpreted with caution. The observed profile—early benefits with a favorable safety balance—suggests that alfentanil may be a valuable option within enhanced recovery pathways for ambulatory endoscopy, particularly when optimizing early recovery quality is a priority. These findings require validation in larger, adequately powered studies designed with contemporary estimates of PONV incidence.
Data Sharing Statement
The data are available from the corresponding author Ma Lei ([email protected]) on reasonable request.
Funding
This trial was funded by the NO.215 Hospital of Shaanxi Nuclear Industry Scientific Research Project (Grant No. 215KYJJ-202411).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gan TJ, Diemunsch P, Habib AS, et al. Consensus guidelines for the management of postoperative nausea and vomiting. Anesthesia Analg. 2014;118(1):85–12. doi:10.1213/ANE.0000000000000002
2. Gan TJ, Belani KG, Bergese S, et al. Fourth consensus guidelines for the management of postoperative nausea and vomiting. Anesthesia Analg. 2020;131(2):411–448. doi:10.1213/ANE.0000000000004833
3. Zhang H, Zhang M, Hao L, et al. Comparison of the effects of ciprofol and propofol on postoperative nausea and vomiting in patients undergoing outpatient hysteroscopy. DDDT. 2024;18:5701–5707. doi:10.2147/DDDT.S489223
4. Knoth S, Weber B, Lotz H, Vojnar B, Eberhart LHJ. Update PO(N)V – was gibt es Neues zu Prophylaxe und Therapie von Übelkeit und Erbrechen nach Operationen? Anaesthesiologie. 2025;74(3):171–186. doi:10.1007/s00101-025-01510-z
5. Apfel CC, Roewer N, Korttila K. How to study postoperative nausea and vomiting. Acta Anaesthesiol Scand. 2002;46(8):921–928. doi:10.1034/j.1399-6576.2002.460801.x
6. Gotoda T, Akamatsu T, Abe S, et al. Guidelines for sedation in gastroenterological endoscopy (second edition). Digestive Endoscopy. 2021;33(1):21–53. doi:10.1111/den.13882
7. Wang GQ. Comparison of the effect of Alfentanil and Sufentanil combined with Propofol intravenous continuous pumping in gastroscopy treatment. China Mod Med. 2021;28(25):132–135. Chinese.
8. Wang GQ. Comparison of anesthetic effects between alfentanil and sufentanil assisted by continuous intravenous infusion of propofol in painless colonoscopy. Lab Med Clinic. 2022;19(03):405–408. Chinese. doi:10.3969/ji.ssn.1672-9455.2022.03.033
9. Shuai SC, Yang YC, Han J, et al. Efficacy of opioid-free anesthesia for gastrointestinal endoscopy in patients with high risk of nausea and vomiting. China J Endosc. 2023;29(9):23–30. Chinese. doi:10.12235/E20220604
10. Zhang J, Liu R, Bi R, et al. Comparison of ciprofol–alfentanil and propofol–alfentanil sedation during bidirectional endoscopy: a prospective, double-blind, randomised, controlled trial. Digestive Liver Dis. 2024;56(4):663–671. doi:10.1016/j.dld.2023.09.016
11. Ziesenitz VC, Vaughns JD, Koch G, Mikus G, Van Den Anker JN. Correction to: pharmacokinetics of fentanyl and its derivatives in children: a comprehensive review. Clin Pharmacokinet. 2018;57(3):393–417. doi:10.1007/s40262-017-0609-2
12. Xin Y, Chu T, Wang J, Xu A. Sedative effect of remimazolam combined with alfentanil in colonoscopic polypectomy: a prospective, randomized, controlled clinical trial. BMC Anesthesiol. 2022;22(1):262. doi:10.1186/s12871-022-01805-3
13. Bilgin H, Başağan Moğol E, Bekar A, Işçimen R, Korfali G. A comparison of effects of alfentanil, fentanyl, and remifentanil on hemodynamic and respiratory parameters during stereotactic brain biopsy. J Neurosurg Anesthesiol. 2006;18(3):179–184. doi:10.1097/01.ana.0000210998.10410.2e
14. Langevin S, Lessard MR, Trépanier CA, Baribault JP. Alfentanil causes less postoperative nausea and vomiting than equipotent doses of fentanyl or sufentanil in outpatients. Anesthesiology. 1999;91(6):1666. doi:10.1097/00000542-199912000-00019
15. Myles PS, Wengritzky R. Simplified postoperative nausea and vomiting impact scale for audit and post-discharge review. Br J Anaesth. 2012;108(3):423–429. doi:10.1093/bja/aer505
16. Goyal R, Hasnain S, Mittal S, Shreevastava S. A randomized, controlled trial to compare the efficacy and safety profile of a dexmedetomidine-ketamine combination with a propofol-fentanyl combination for ERCP. Gastrointest Endosc. 2016;83(5):928–933. doi:10.1016/j.gie.2015.08.077
17. Miner JR, Heegaard W, Plummer D. End-tidal carbon dioxide monitoring during procedural sedation. Acad Emerg Med. 2002;9(4):275–280. doi:10.1111/j.1553-2712.2002.tb01318.x
18. Kovac AL. Postoperative nausea and vomiting in pediatric patients. Pediatr Drugs. 2021;23(1):11–37. doi:10.1007/s40272-020-00424-0
19. Cho S, Bang H, Shin S, et al. Opioid-associated postoperative nausea and vomiting in women undergoing laparoscopic hysterectomy: a network meta-analysis. Medicina. 2025;61(10):1728. doi:10.3390/medicina61101728
20. Lei X, Zhang T, Huang X. Comparison of a single intravenous infusion of alfentanil or sufentanil combined with target-controlled infusion of propofol for daytime hysteroscopy: a randomized clinical trial. Therap Adv Drug Safety. 2024;15:20420986241292231. doi:10.1177/20420986241292231
21. Gan TJ, Jin Z, Ayad S, et al. Fifth consensus guidelines for the management of postoperative nausea and vomiting: executive summary. Anesthesia Analg. 2025. doi:10.1213/ANE.0000000000007816
22. Darvall JN, De Silva AP, Von Ungern-Sternberg B, et al. Chewing gum to treat postoperative nausea and vomiting in female patients: a multicenter randomized trial. Anesthesiology. 2025;142(3):454–464. doi:10.1097/ALN.0000000000005283
23. Kovac AL. Management of postoperative nausea and vomiting in children. Pediatr Drugs. 2007;9(1):47–69. doi:10.2165/00148581-200709010-00005
24. Sun X, Briel M, Walter SD, Guyatt GH. Is a subgroup effect believable? Updating criteria to evaluate the credibility of subgroup analyses. BMJ. 2010;340(3):c117. doi:10.1136/bmj.c117
25. Mandel JE. Considerations for the use of short-acting opioids in general anesthesia. J Clin Anesth. 2014;26(1):S1–S7. doi:10.1016/j.jclinane.2013.11.003
26. Zhu H, Sun Y, Wang T, Wu Z. Alfentanil and propofol induced anesthesia for patients with huge endotracheal tumor undergoing fiberoptic bronchoscopic interventional therapy: case report. Transl Cancer Res. 2022;11(8):2946–2952. doi:10.21037/tcr-22-199
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.