")
Back to Journals » Clinical Interventions in Aging » Volume 18
Aging Stigma and the Health of US Adults Over 65: What Do We Know?
Received 19 August 2023
Accepted for publication 1 December 2023
Published 15 December 2023 Volume 2023:18 Pages 2093—2116
DOI https://doi.org/10.2147/CIA.S396833
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Julie Ober Allen,1,2 Nadine Sikora1
1Department of Health and Exercise Science, University of Oklahoma, Norman, OK, USA; 2Research Center for Group Dynamics, Institute for Social Research, University of Michigan, Ann Arbor, MI, USA
Correspondence: Julie Ober Allen, University of Oklahoma, 1401 Asp Ave, Norman, OK, 73019, USA, Tel +1 405 325 4984, Email [email protected]
Abstract: This narrative review assessed the current state of research on aging stigma and health relevant to US adults ages 65 and older. We adopted a stigma framework to highlight aging stigma as a meaningful social construct and the complex ways in which it may be harmful for health. We identified 29 studies of various types (experimental, intervention, cross-sectional quantitative, longitudinal quantitative, and qualitative) published between 2010 and 2023 that investigated relationships between concepts related to aging stigma and health. Aging stigma was associated with poor short- and long-term health outcomes spanning cognition, psychological wellbeing, physical health, and hospitalizations. The premise that aging stigma is harmful to health was moderately well supported, while evidence that health influenced aging stigma was weak. Collectively, studies provided insight into several mechanisms through which aging stigma may affect the health of older US adults, while also highlighting areas for future research. Potential strategies for addressing aging stigma as a public health hazard were discussed.
Keywords: ageism, perceptions of aging, discrimination, prejudice, stereotypes, stereotype threat
Introduction
Stigma is increasingly recognized as a social and structural phenomenon relevant to health and health disparities. In a landmark article on the conceptualization of stigma, Link and Phelan1 documented the growth of research on stigma, which was mentioned in the title or abstract of 19 Medline indexed articles in 1980 and increased to 114 articles in 1999. In a recent update to their search using PubMed, we found that stigma was mentioned in over 5000 articles in 2022. For the purposes of this article, we defined stigma as negative beliefs and stereotypes linked to socially constructed categories that serve as the basis for prejudice, discrimination, and the social marginalization of individuals and groups labeled with those categories.1–3 Stigmatized people are often considered to be fundamentally different, which is used to justify social distancing and differential treatment. These limit access to opportunities and resources, result in loss of status, restrict self-determination and rights, and are associated with a range of negative outcomes including poor health. The concept of stigma has been applied to diverse sociodemographic characteristics, behaviors, lifestyle circumstances, and health outcomes. One category laden with negative stereotypes that has received limited attention in the stigma literature is old age. While research on the social construction of aging and old age has grown in the past 15 years, this work typically adopts the vocabulary and framework of ageism rather than aging stigma. While closely related, the theoretical conceptualization of stigma prompts consideration of some aspects of how our society thinks about and treats aging, older adults, and old age that are insightful in a review of what we know about aging stigma and how it may affect the health of US adults ages 65 and older.
An important point highlighted within the stigma framework is that while socially meaningful categories of human differences are widely believed to be biological attributes of individuals and groups, they are, in fact, socially constructed labels. Age is one of the most commonly cited demographic categories in the contemporary US. Yet beliefs and attitudes associated with age, particularly old age, are not limited to impartial discussions of chronological age. Rather, research shows that societal beliefs and attitudes about aging and older adults in the US are dominated by narrow, overwhelmingly negative stereotypes of how older adults should behave, what they should look like, and what are reasonable and appropriate expectations of aging.4 Once categories of differences are established, they are generally taken for granted and become ingrained, normative, and widespread.1 Old age has been described as the most deeply rooted, unquestioned, and socially acceptable stigmatized category affecting a sizable percentage of the US population.5–7 Preschool aged children have been shown to recognize old age as an important social category and espouse ageist prejudices.8 Variations in the aging stigma that children absorb early in life persist into adulthood and become increasingly self-relevant as people transition into the category of older adults, particularly as they receive reinforcement that they fit into the category of older adults.9 Survey studies have reported that between 60% and 81% of older adults endorse internalized ageist beliefs.10,11
Another key characteristic of socially meaningful categories is that they are used to create social, and sometimes physical, distance from stigmatized groups.7 This creates an “us versus them” dynamic. Older adults in the US are often physically segregated into age-specific housing and with specialized services and contexts designed for their age group. Many exit the workforce, voluntarily or not, which is a context characterized by intergenerational relations. Segregation of this type tends to minimize interactions and the development of interpersonal relationships across age categories, thereby reducing opportunities for aging stereotypes to be broken down.12 Social distancing generally serves to disempower stigmatized groups, restricting access to economic, social, and political power.1 Consistent with this, older adults are discriminated against in employment, housing, and healthcare.13–15 In a nationally representative sample, over 93% of US adults ages 50–80 reported that they were affected by different examples of aging stigma on a regular basis.10 Extent of age segregation and affected life domains vary within the older US adult population but become more common with increasing age (eg, on average, 80-year olds are more age segregated than 60-year olds).7
One dissimilarity between aging stigma and many other stigmatized categories is that aging stigma is only experienced during a portion of the life course once members of the dominant age group transition into the category of older adults. Consistent with many other stigmatized categories, however, the defining characteristics of old age are vague. There is a lack of consensus on when old age begins, whether at a specific chronological age or based on other indicators such as life stage, level of independence, or health status. The transition into the older adult category and accompanying ambiguity regarding its timing are believed to generate anxiety about being considered old.16 Efforts to avoid or delay membership in this category may account for the $13 billion spent annually in the US on products and procedures in the anti-aging industry.17 Further, there may be discrepancies in how people self-categorize their age group membership versus how others categorize them. Both are important, as they represent different mechanisms through which aging stigma is believed to affect health and wellbeing. Worthy of note, is that while stigmatized groups are, typically, socially marginalized across multiple domains, older adults collectively appear to retain some advantages associated with their former privilege, such as voting power and relatively low poverty rates.18,19
Negative outcomes experienced by stigmatized individuals and groups are generally assumed to be a consequence of the labels they have been assigned. Beliefs that poor health is inevitable in old age are pervasive and entrenched despite evidence to the contrary.10 Strategies to improve health outcomes among older adults tend to be individually focused, such as providing access to affordable medical care, reducing isolation, and encouraging healthy behaviors. Yet, there is a growing body of evidence in support of the premise that many adverse health outcomes commonly found within the older US adult population are caused or exacerbated by internalized aging stigma and external sources of age-based discrimination.5,9,10,20 Several recent reviews of quantitative research have documented that age-related beliefs, prejudices, and discrimination, measured in different ways and across diverse samples, were consistently associated with a broad array of adverse health outcomes.21–23 This suggests an alternative strategy for improving health outcomes among the older US adult population characterized by reducing negative aging stigma within broader society, reframing narrative about aging and old age to be more diverse and positive, and developing practices and policies to prevent aging stigma from negatively affecting the health and wellbeing of older adults.5,24
Aging stigma is believed to affect health through multiple pathways.1,25,26 Older adults who internalize aging stigma may have negative self-perceptions, poor psychological health,27 and begin to embody negative stereotypes related to old age.9 Feeling threatened by aging stereotype may generate psychological distress, cognitive load, and coping responses with ramifications for health.12 External cues of aging stigma are ubiquitous, repeatedly reminding and reinforcing ageist prejudices and preventing older adults from disregarding the social importance of this stigmatized category.28 Anticipated or actual incidents of age-based discrimination can activate cognitive, emotional, and physiological stress responses, which, if frequent, are believed to accelerate aging processes and increase risk for chronic disease.5,29,30 Older adults may delay or avoid healthcare seeking or receive suboptimal care, when aging stigma has negatively affected the quality of their interactions with healthcare providers and institutions. Even when older adults do seek healthcare services, they have been documented as not receiving medically appropriate procedures or treatments.31 Finally, people categorized as older adults by others may experience negative prejudice and discrimination in social interactions and in their treatment by institutions and policies. Given the pervasiveness of aging stereotypes combined with the numerous ways in which they can affect health, it is likely that the health of most older adults is affected in some way, even if they are unaware of it. The magnitude of aging stigma for health, however, may vary based on self- and external categorization as old, how much individuals believe and are concerned about negative aging stereotypes, the frequency and severity of ageist cues, prejudice, and discrimination people encounter, and other factors.
The objective of this review article was to generate a narrative summary and synthesis of recent research providing insight on what we know about aging stigma and its relationships to the health of US adults ages 65 and older. This review complements and is distinct from recently published reviews on ageism and health21–23 in several ways. First, we adopted a stigma framework to emphasize aspects of aging stigma as a social construct and potential mechanisms through which stigma may affect health warranting further recognition and consideration. Second, we focused narrowly on adults ages 65 and older residing in the US to minimize heterogeneity of the sample. Inconsistent definitions of old age and broad age groups included in aging stigma and health research have the potential to weaken, if not confound, findings on associations and mechanisms of aging stigma and health. Age 65 has become a commonly identified lower threshold for the older adult category in the US with the mid-60s marking average retirement age,32 eligibility for older adult benefits and federal entitlement programs (eg, senior housing, Medicare, Social Security), and the age identified most often in social media, policy discussions, and research on older adults in the US. Adults ages 65 and older are more likely than those in their 50s and early 60s to self-identify and/or be categorized by others as older adults,10,33 making aging stigma more salient to their lived experiences and health. As these represent two commonly identified mechanisms through which aging stigma is posited to affect health, associations between these concepts are expected to be more consistent and stronger among older age groups. We focused on studies within the US because, while old age has been identified as a meaningful social category and construct associated with poor health outcome across the world,34 the prevalence of aging stigma, the magnitude of its effects on health, and its manifestations are believed to vary across countries and cultures.21,34 Cross-national comparisons have reported differences in the prevalence of severe aging stigma, with the US demonstrating less aging stigma than many other countries in most, but not all, studies.35–37 A US-specific focus allowed us to confirm that associations between ageism and health documented globally were applicable to the US and assess whether aging stigma in the US was associated with a wide range of health outcomes, as suggested in scoping reviews of the global literature. Potential mechanisms linking aging stigma and health may also be culture- and context-specific due to a nation’s unique history, demographic profile and shifts over time, sociocultural values, institutions, and policies.22 For example, aging stigma surrounding being unable to live independently and nursing home care are common in the US, perhaps stemming from traditional American cultural values of self-reliance; in countries where aging adults are expected to remain living in intergenerational households, aging stigma may revolve around other topics. The findings from the current review may inform future research and interventions on aging stigma and health tailored to address the specific needs, risk factors, and contexts experienced by US adults ages 65 and older. Finally, this review considered findings from diverse types of research studies, which, facilitated by the growth of recent research on aging stigma, allowed us to group articles and critically analyze research findings according to study type: experimental, intervention, quantitative, and qualitative. This approach facilitated consideration of the differing study type strengths, weaknesses, and contributions to our understanding of potential mechanisms linking aging stigma and health in the US. Further, grouping studies by type facilitates rapid identification of the most relevant studies for readers with different interests, while simultaneously providing a more comprehensive and multi-faceted review of relevant research than has been incorporated into previous reviews.
Materials and Methods
We conducted a comprehensive review of published empirical research examining relationships between concepts related to aging stigma and health among US adults over 65. Aging stigma variables were conceptualized as reflecting negative stereotypes, prejudices, and associated discrimination related to aging and older adults that were either invoked (eg, exposure to ageist primes or materials) or captured (self-reported survey data). Aging stigma could plausibly be measured at different levels of influence (eg, communitywide, in interpersonal relationships, or experienced or internalized by individual older adults, themselves) or among varied groups with influence on the lives of adults ages ≥65 (eg, healthcare providers, family members, or work colleagues). Health was conceived of as measures of cognitive health (memory, cognitive functioning), psychological wellbeing (mental health conditions, depressive symptoms, psychological distress, self-rated mental health, affect, and quality of life), physical health (types or number of diseases or chronic health conditions, functional health, physiologic health measures/biomarkers, self-rated physical health, and pain), hospitalizations, and health behaviors (eg, physical activity, smoking, and healthcare use). For this review, health measures had to focus on outcomes among adults ages ≥65. Relationships between aging stigma and health in any hypothesized direction (eg, aging stigma contributing to poor health or vice versa) were considered.
Between May and July 2023, we conducted a systematic literature search to identify relevant articles for inclusion composed of three phases (Figure 1). In phase one, we used PubMed to identify articles assigned the “ageism” Medical Subject Heading (MESH) term or containing related keywords such as age stigma, age prejudice, perceptions of aging, or age stereotypes in the title or abstract (see Figure 1 note for complete keywords list). The search was limited to articles published in English between 2010 (coinciding with the growth of research on ageism and health in PubMed) and 2023. We further restricted the search to articles MESH indexed for adults ages ≥65 (“aged”) and the US or devoid of indexing by age group and/or geographic region. Finally, we omitted articles indexed as reviews and editorials. All components of this search strategy were combined using Boolean operators and executed as a single advanced search; therefore, there were no duplicate articles to eliminate.
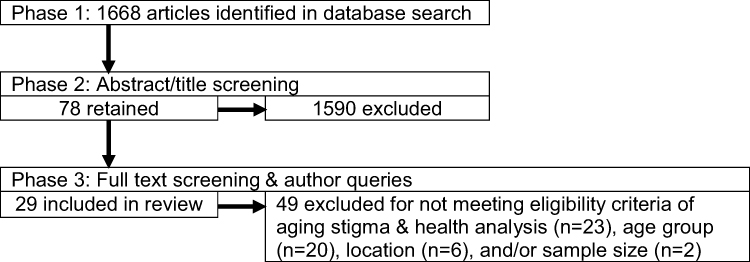 |
Figure 1 Flowchart of literature search and screening. Notes: Search criteria were empirical studies published in English between 2010 and 2023 investigating relationship between aging stigma and health among US adults ages 65+. Phase 1 PubMed database search used the ageism MESH term and keywords of age stigma, ageism, age discrimination, age prejudice, stereotype threat, perceptions of aging, aging expectations, views of aging, age beliefs, age stereotyp*, aging self stereotyp*, aging stereotyp*, age-based stereotyp*, unequal ageing, aging anxiety, ageist, and age inequality. Keyword terms ending with * will capture all uses of the truncated term with any endings. |
In phase two, we screened all article abstracts and titles. We retained those meeting the inclusion criteria or indeterminant and excluded those not meeting the inclusion criteria. In phase three, we obtained the full-text versions of all remaining articles and triaged articles as eligible for inclusion, ineligible and therefore excluded, or indeterminant due to insufficient information. For this last group, we contacted article authors by email to obtain the information required to determine eligibility. Inclusion criteria for the literature review were as follows: (1) published in English; (2) published between 2010 and 2023 and available on PubMed as of June 29, 2023; (3) empirical studies with quantitative or qualitative data; (4) sample predominantly (>50%) adults ages 65 years and older or with discrete analyses for a ≥65 subsample; (5) sample predominantly (>50%) US residents; (6) minimum sample sizes of 30 for survey/experimental research and 10 for qualitative/intervention research; and (7) containing data analyses investigating linkages between concepts related to aging stigma and health.
For each article, we extracted information on the study type (experimental, intervention, quantitative, qualitative), data source and study design, sampling methods, sample characteristics with an emphasis on descriptive statistics related to age, the ways in which aging stigma was operationalized, the health variable(s) assessed, and a summary of findings relevant to aging stigma and health. We relied on data analyses conducted by the article authors and their assessments of significant associations; when a threshold for determining significance was not indicated, p<0.05 was used. Given that the objective of this review was to provide a narrative summary and synthesis of recent research on aging stigma and health spanning diverse study types and disciplines with differing standards of rigor, we did not formally grade study quality, evaluate reporting biases, or conduct a meta-analysis. Instead, we provided detailed information related to many characteristics used to assess study quality and generalizability in the article table and narrative. Additionally, we considered the strengths and weaknesses of different types of studies and some individual studies in the discussion.
Results
Characteristics of Included Studies
We identified 29 articles meeting the inclusion criteria for this review (Table 1) including 10 experimental studies, 5 intervention studies, 12 quantitative studies, and 4 qualitative studies. Two studies bridged more than one study type (eg, experimental studies with an intervention and mixed methods studies).
 |
Table 1 Articles |
Experimental Studies
Experimental studies were heavily represented in this review. In fact, three out of the ten experimental study articles summarized findings from two related experiments, resulting in a total of 13 distinct experiments and samples. Experimental studies employed comparisons to investigate relationships between aging stigma and health, including multiple (2–6) study arms with variations in the experimental and comparison/control conditions, older and younger adult subsamples (four studies), and data collected from participants before and after exposure to aging stigma. One experimental study also tested an intervention (discussed below) to reduce the negative consequences of aging stigma.60 All experimental studies utilized regionally focused convenience samples composed of US adults in their target age range. Older adult sample sizes (or subsample sizes in studies comparing older and younger adults) ranged from 31 to 166, with an average of 81.6 participants. The approximate pooled average age for older adults across experimental studies was 71.5 years old, which closely mirrored the average ages reported in individual studies (±3.6 years).
All the experimental studies focused on how aging stigma may influence health, and not the reverse or potential reciprocal relationships. Most adopted a theoretical framework of stereotype threat12 and explored different ways in which negative aging stereotypes can be communicated, including exposure to explicit stereotyped messages, implicit and subliminal stereotype activation, and contexts with high potential to generate stereotype threat among older adults. One study tested both experimental exposure to aging stigma and participant self-reported survey data gauging perceived aging stigma.43 The primary health outcomes of interest in the experimental studies were short-term memory and/or cognitive functioning, which were assessed using standardized tasks completed in-person assessing recall and recognition (Figure 2). Other health outcomes examined in experimental studies included psychological wellbeing and stress-sensitive physiological indicators (eg, blood pressure and heart rate) (Figure 2).
 |
Figure 2 Health categories investigated by study type. Notes: Sum of studies investigating a specific health category in the figure may be higher than the actual number, as studies representing more than one study type (2) are depicted more than once. |
Intervention Studies
Five intervention studies were identified, many of which shared characteristics with and built on the findings reported in experimental studies on aging stereotype threat. On average, intervention studies were published more recently than the other types of studies examined in this review. One intervention study reported on two related experiments. Another compared older and younger adult subsamples. All included between two and seven experimental and comparison/control arms. Four intervention studies had regional convenience samples, while the fifth used online platforms to recruit a convenience sample from across the US. Older adult sample sizes ranged from 56 to 763 with an average of 272.8 participants. The approximate pooled average age for older adults in intervention studies was 71.6.
Intervention studies also assumed a theoretical framework positing that aging stigma could negatively affect health, while testing a variety of approaches to disrupt this relationship. Reviewed interventions involved task success,53 a memory training course,56 exposure to positive age stereotypes and aging messaging,55,58 and reinforcement of cultural values inconsistent with dominant US attitudes and treatment of older adults.60 All interventions focused on change at the intrapersonal level and sought to alter individual beliefs, perceptions, and skills theorized to affect health outcomes directly (eg, via internalized aging stigma) or indirectly (eg, promoting self-efficacy, self-esteem, or skills, which were theorized to buffer against or reduce aging stigma). Four of the reviewed interventions were brief (completed within ≤1 hr), low cost, relatively simple to implement, and well suited for translation to different delivery modes and target populations. The memory training program56 was longer (2 months), more time and resource intensive, and complex, while providing more contact hours, likelihood of long-term effects, and potential for benefits outside those prioritized in the intervention (eg, social relationships and changes to aging expectations in the community). Intervention studies operationalized aging stigma as stereotype threat (both explicit and implicit) and negative aging stereotypes, which were either experimentally manipulated or assessed using a wide range of survey instruments (Stereotype Threat scale,54 Metamemory in Adulthood questionnaire,57 and Views of Aging scale59). As with the experimental studies, health outcomes were predominantly short term in nature and included memory, psychological wellbeing, functional health, and motivation to be active (Figure 2). Outcome health data for the four brief interventions were collected immediately. The memory training examined outcomes over 24 months of follow-up.
Quantitative Studies
Quantitative studies were described in the largest portion of articles relevant to this review. There were three cross-sectional studies (one of which employed mixed methods75), eight longitudinal studies with data collection spanning between 2 and 12 years (average 7.1), and one study that applied meta-analysis findings to predict national health and healthcare costs attributable to ageism.11 Nearly all of these studies utilized self-reported survey data, many in combination with other forms of linked data from task performance, interviews, cognitive assessments, genetic material, home-based assessments, and Medicare and mortality records. Half the studies analyzed data collected as part of large, nationally representative survey studies collecting longitudinal health data—five studies used the Health and Retirement Survey (HRS82) and one study used the National Health and Resilience in Veterans Study (NHRVS83). Two studies used longitudinal data from the Precipitating Events Project,84 which followed a regional cohort of 754 community-residing adults ages ≥70 years for 10 years, and three used data collected from smaller regional61,75 and national77 convenience samples. Sample sizes were larger than those documented among other study types, ranging from 73 to 4765 participants and averaging nearly 2000. Quantitative study findings were based on approximately 7500–12,000 unique participants across studies. The pooled average age at baseline, not accounting for duplicates, was slightly younger than in other study types, at 69.3 years old.
Nine quantitative studies assumed the theoretical orientation that aging stigma may affect health. Two cross-sectional studies76,77 hypothesized that health may influence aging stigma, while one longitudinal study70 considered causality in both directions by investigating the temporality of aging stigma and health variables. Aging stigma was largely indicated by self-reported responses to survey measures designed to assess perceptions of aging and age-based discrimination: all five HRS studies used the Attitudes Toward Own Aging scale;63 two studies used the Expectations Regarding Aging scale;45 two used Palmore’s Ageism Survey;68 and one used the Awareness of Age-Related Change scale.78 The study estimating the impact of ageism on national health outcomes and healthcare costs11 relied on three measures related to aging stigma: Attitudes Towards Own Aging,63 Expectations Regarding Aging,45 and the Everyday Discrimination scale attributed to age.71 Three studies integrated activities to gauge aging stigma (rating of free response descriptors of older adults, evaluation of messages). Quantitative studies examined a broad array of health conditions including those investigated in experimental studies and others: memory and cognitive functioning, psychological wellbeing, functional health, pain, chronic health conditions, healthcare costs, hospitalizations, adherence to health recommendations, and physical activity (Figure 2). Longitudinal studies, in particular, were able to investigate long-term health outcomes, temporality of aging stigma relative to health outcomes, and associations between aging stigma and health changes over time (eg, incidence rates and recovery/decline).
Qualitative Studies
Four qualitative studies met the criteria for inclusion in the review, one of which employed mixed methods. Three studies were cross-sectional, and one was longitudinal with data collected over 12 months.81 Data were derived from semi-structured, individual interviews (two studies) and focus groups (two studies). All four used regional convenience samples, some representing cohorts with specific health issues or from different generations. One study was part of the Precipitating Events Project.84 Older adult samples for these studies had between 27 and 93 participants and a mean of 71. The average age for participants across qualitative studies could not be estimated, due to variations in descriptive statistics provided, but was generally older than the average age in other study types.
Assessment of aging stigma across qualitative studies varied widely but generally included expressions of internalized aging stigma, often linked to specific health conditions, perceptions of ageist prejudice and cues, and experiences of age-based discrimination. Health variables investigated in qualitative studies included aspects of psychological wellbeing, physical health outcomes, and various health behaviors (Figure 2).
Summary of Findings on Aging Stigma and Health
Overall, experimental and intervention study findings provided evidence that aging stigma, most often investigated in the form of stereotype threat, was associated with poor short-term health outcomes that fluctuate within a relatively short timeframe (ie, memory, cognitive functioning, psychological wellbeing, and motivation) among US adults ages 65 and up. This held true for aging stereotype threat activated in explicit, subtle, and contextual ways. Findings were complex, in that aging stereotype threat was associated with poorer memory and cognitive performance of some kinds, but not others, and differences were context dependent (eg, level of challenge, presence of penalties or rewards). Tests of theorized intervention models of change were often not substantiated, even if many were successful in achieving the desired end-results. For example, scores on aging stigma survey scales did not mediate the relationship between an intervention seeking to reduce aging stigma and health.53 In another study, the intervention was associated with anticipated outcomes for some groups but had no effect or was associated with undesirable outcomes in other groups.58
In cross-sectional and longitudinal quantitative studies, negative aging stigma was consistently associated with poor health outcomes. This held true for studies using variables representing many dimensions of aging stigma including stereotype threat, internalized aging stigma, perceptions of ageist cues and prejudices, and experiences of age-based discrimination. This was also true for studies investigating diverse health outcomes ranging from cognition and mental health, which were well represented in experimental and intervention studies, to chronic pain, functional health, and specific chronic illnesses. Aging stigma was estimated to account for 17 million excess health conditions and $63 billion in excess healthcare costs annually in the US.11 Qualitative studies reported similar findings, with participants generally indicating that aging stigma negatively affected their psychosocial wellbeing, chronic pain levels, and hearing.
Regarding aging stigma and the health behaviors of older adults, study findings were mixed. Quantitative studies generally did not find that aging stigma predicted health behaviors over time, specifically, physical activity levels. Qualitative studies, in contrast, made a strong case that aging stigma caused people to avoid and/or delay healthcare seeking and use of medical treatments and assistive devices. These circumstances were described as resulting in or putting individuals at risk for poor health outcomes.
Collectively, research reflecting all study types provided evidence in support of the premise that negative aging stigma may be harmful to health. The converse, which was only investigated in three quantitative studies,70,76,77 was not consistently supported and not at all supported in the single longitudinal study examined.70
Discussion
This narrative review complements and adds to the existing literature investigating linkages between the social construct of aging and health by marshalling the rich conceptualization and literature on stigma, while also focusing on research conducted with US adults ages 65 and older, as this age group is believed to be at risk for both experiencing aging stigma and its ramifications for health. Findings from 29 articles reflecting a range of study types provided moderate support for the premise that negative aging stigma is associated with a variety of poor short- and long-term health outcomes spanning cognition, psychological wellbeing, physical health, and hospitalizations among US adults ages ≥65. This was generally consistent with the findings of other review articles assessing associations between concepts related to aging stigma and health among more age and geographically diverse samples.21–23
Research investigating aging stigma and cognitive health represented the largest proportion of studies meeting the eligibility criteria for the current review (a health category investigated in 52% of articles) and was more heavily represented than in other reviews on ageism and health (eg, 15%22). This may have been a result of our inclusion of a broader range of study types. Experimental study designs, which were included in our review but often have not been included in others, are well suited to tests assessing cognitive functioning. Additionally, both cognition and stereotype threat are major areas of interest in the field of psychology, which frequently employs experimental study designs. Experimental and some intervention studies demonstrated the immediate effects of stimulating stereotype threat in explicit, subtle, and contextual ways on older adults’ cognitive status, as well as on their short-term psychological health and stress-sensitive physiological indicators. These studies provided additional evidence that aging stereotype threat may be a mechanism affecting older adult health. However, the short follow-up periods, small convenience samples, and controlled laboratory environments characteristic of these studies limit our capacity to draw conclusions about potential long-term health effects of aging stereotype threat among diverse community samples. Further, findings from studies investigating associations between aging stereotype threat and cognition were the most nuanced and challenging to synthesize. Collectively, they suggested that while aging stigma may affect short-term memory and cognitive functioning, effects were irregular—applying to some forms of cognition but not others and only under some conditions. These nuances may account for why the theorized mechanisms of change for intervention studies focused on aging stigma and cognition were not well substantiated. This review also considered three quantitative studies on cognition, all longitudinal, based on the HRS dataset and conducted by the same research team. While a strength of the experimental studies was providing insight into specific mechanisms through which aging stigma may affect health, these quantitative studies provided evidence that aging stigma may be a risk factor for adverse cognitive outcomes over time in large, national samples of older adults. These results strengthen the case that aging stigma may have severe cognitive consequences that are generalizable across the US.
Slightly less than a third (28%) of reviewed studies investigated associations between aging stigma and psychological wellbeing. Affect or mood, measured in two experimental studies using the Positive and Negative Affect Scale,85 was not associated with aging stigma. In contrast, more specific indicators of psychological wellbeing such as anxiety and depressive symptoms were associated with higher levels of aging stigma in studies of all types, cross-sectionally and longitudinally. Participants in qualitative studies specifically noted ways in which their psychological wellbeing was affected by aging stigma, predominantly, but not exclusively, in negative ways. Collectively, findings from studies on psychological wellbeing suggest that aging stigma may produce fairly specific psychological responses rather than a broad range of negative emotions. Additionally, findings suggest that aging stigma may contribute to poor psychological outcomes via multiple pathways— short term, via stereotype threat, and long term, due to internalized negative beliefs about aging and age-based discrimination.
Physical health was investigated in 24% of included articles. Quantitative studies were particularly well represented, which was fitting given that many physical health outcomes do not demonstrate variations or change over the short timeframes characteristic of experimental studies and many of the reviewed intervention studies. Across quantitative and qualitative studies, aging stigma was associated with adverse physical health without exception, with investigated outcomes ranging from functional health and chronic pain to chronic health conditions and diseases. Findings from most of these studies were based on high-quality data collected as part of large-scale, longitudinal studies (eg, HRS, NHRVS, and Precipitating Events Project). Major contributions of the quantitative studies were that their findings documented temporal relationships between aging stigma and physical health outcomes arguably generalizable to the overall US older adult population and strengthened the argument that aging stigma contributes to or perhaps even causes poor health outcomes. These studies assessed varied forms of aging stigma (negative internalized beliefs about aging, aging stereotypes, perceptions of others’ prejudices surrounding aging, and experiences of age-based discrimination), which alluded to multiple pathways through which aging stigma may influence health, but without the specificity that could be investigated using other study types. One experimental study that assessed physical health examined physiologic indicators that fluctuate over short time periods—blood pressure and heart rate—and particularly in response to acute stressors.43 Findings, however, were mixed, making it unclear whether fight or flight stress responses represent another potential mechanism linking aging stigma and health. One intervention study examined functional health as a secondary outcome;56 null findings for this outcome may have reflected a mismatch between the intervention and this outcome. Two quantitative studies concluded that aging stigma was implicated in greater hospitalization risk and costs.11,70
In the current review, evidence related to aging stigma and health behaviors was mixed, though whether relationships between these concepts were detected appeared to be patterned by behavior and study type. In three intervention and quantitative studies examining aging stigma and physical activity, associations were inconsistent. Three qualitative studies reported that concepts related to aging stigma were identified by participants as negatively affecting healthcare seeking and the use of medical treatments. In a mixed methods study, participants were described as distancing themselves from ageist stereotypes during the COVID-19 pandemic by persevering with life, which included disregarding public health recommendations.75 The mixed findings regarding aging stigma and health behaviors in the current review deviate from other reviews on ageism and health,21–23 which reported consistent relationships (largely from quantitative studies) between aging stigma and a more diverse range of health behaviors.
Collectively, the diverse types of research studies included in the current review provided fairly consistent and robust evidence that aging stigma may be harmful for a variety of health outcomes, with mixed findings for health behaviors, among US adults ages 65 and older. Experimental and intervention studies built the case that aging stigma may be associated with short-term health outcomes, while cross-sectional and longitudinal quantitative and qualitative studies documented relationships between aging stigma and long-term health outcomes. Examined studies operationalized aging stigma in a wide variety of ways—priming with ageist cues; invoking stereotype threat; and survey scales capturing attitudes, expectations, stereotypes, and discrimination related to old age and aging—that did not demonstrate any identifiable patterning in their associations with health (eg, no specific forms were more consistently associated with health or certain health categories than others). Experimental and longitudinal quantitative studies provided evidence suggestive of causality and direction of effect, especially the few studies with the objective of investigating causality in both directions.70 Overall, included studies provided evidence in support of the dominant viewpoint—that aging stigma affects health, while support for health as a potential determinant of aging stigma (examined in only three studies) was weak. These findings are consistent with both theoretical and empirical research, which posit that while relationships between aging stigma and health are likely bidirectional, the effect of aging stigma on health is greater than the opposite.9,59,86,87 Finally, a limited number of intervention studies have demonstrated the potential for mitigating the harms of aging stigma on health. The brevity and low resource requirements of several of these interventions demonstrate the potential cost-effectiveness of initiatives to combat aging stigma and potential for even larger impact of initiatives with greater dose or multilevel strategies.
Implications for Future Research and Interventions
One recommendation for future aging stigma and health research is the inclusion of more descriptive data on participant ages, as well as sub-analyses conducted with narrower age ranges of older adults (eg, 10-year spans). Both exposure to aging stigma and health status vary widely among older US adults, which is a vague category applied to people with ages spanning multiple decades. Disparities in aging stigma are generally patterned by chronological age, with adults at the older end of the old age category reporting more frequent and different kinds of aging stigma compared to those at the younger end.33 More research is needed to determine whether aging stigma differentially impacts the health of age subgroups within the older population. Further, the typical descriptive data on age included in research articles (ie, mean age, standard deviation, range) may be insufficient for clinicians, service providers, and policy-makers seeking to develop evidence-informed interventions tailored to enhance the health of specific age subgroups of older US adults. For example, it seems ill-advised to assume that study findings on aging stigma and cognition conducted among 50 years olds would be applicable to centenarians.
Exposure to aging stigma is determined by whether individuals are categorized as older adults. Aspects of visible appearance associated with aging (eg, hair color, skin characteristics, movement, and use of assistive devices) are commonly relied upon in broader society to estimate age. How old they look may also affect how older adults categorize themselves. More insight is needed on how aspects of visual appearance relate to aging stigma and, therefore, indirectly to health. Further, efforts to alter one’s appearance through the use of anti-aging products and procedures are widespread in the US. Future research is warranted to determine whether these efforts are effective at reducing experiences of aging stigma in greater society and how they affect internalized stereotypes and beliefs about aging.
Stigma is believed to negatively affect health and other outcomes in large part because it is reproduced and maintained within society.1 While not represented in this review, measures and study designs that capture the effects of aging stigma within broader society, the media, communities, and institutions are needed to provide a more comprehensive understanding of how aging stigma may affect health outcomes within the older US adult population. Combining this with current assessments of aging stigma at the individual level would facilitate investigation of the potentially synergistic effects of aging stigma across multiple levels of influence, life domains, and mechanisms.
The current study demonstrated the benefit of synthesizing findings from diverse study types for elucidating mechanisms linking aging stigma and health. Future research employing cross-disciplinary collaborations integrating multiple study types has significant potential to further advance our understanding of mechanisms linking aging stigma and health. This strategy would marshal the strengths and insights provided by different study types. This may facilitate narrowing the current theoretical and empirical gaps surrounding how acute exposures to aging stigma and associated short-term responses have a cumulative effect on the body and increase risk for long-term health outcomes such as chronic disease.5,29,30
While the current review only identified a small number of predominantly brief, individually focused interventions to reduce the potential harms of aging stigma on health, initiatives to raise awareness about aging stigma and its harms, reframe narrative about aging and older adults, and reduce age-based discrimination have grown in recent years. These initiatives may benefit from implementation science and systematic evaluations. Taking advantage of these areas of expertise would help identify and test theorized mechanisms of change, some of which were not well articulated, justified, or supported in the reviewed articles. This work could be marshalled for ongoing quality improvement, identification of best practices, and sharing of key elements with others interested in launching their own initiatives. Finally, systemic and rigorous efforts to develop and evaluate initiatives seeking to address aging stigma are essential to make the case that while aging stigma may be harmful to health, this relationship can be disrupted.
One final topic warranting consideration is the language we use. Currently, phrases such as “older adults” and “older people” are recommended for referring to this age category of people, as this terminology is perceived as being less likely to evoke negative stereotypes related to aging than other options.88 The stigma literature also advocates for careful selection of word choices. However, they recommend a more nuanced approach. This consists of dispensing with language suggesting that a stigmatized category defines a person (eg, schizophrenic) and instead prioritizing the person while also communicating a label if relevant (eg, person with schizophrenia). Perhaps, a future development in combating aging stigma and its harms will be to refer to “people of advanced age” or “adults with more years”.
Limitations
First, although this review employed systematic methods, we may have missed some research providing insight on aging stigma and the health of US adults ≥65 years old, especially studies disseminated in languages other than English, books, and the grey literature. Second, while we were purposeful in limiting our review to studies conducted with samples comprised predominantly of US adults ages ≥65 to identify nationally- and culturally-specific patterns of aging stigma and health, we recognize that research conducted with a broader age range and geographic footprint provides important information on the phenomena of aging stigma and health more generally. The current study is intended to complement other systematic reviews on this topic conducted with more heterogeneous samples (eg, ages ≥4022, ≥5021, and ≥6023, all of which included studies from across the globe). Third, consistent with a stigma framework, we only included articles if they had aging stigma variables that tapped into negative aging stereotypes. While aging stereotypes are predominantly negative and have become more negative in recent years,4,89 some aging stereotypes may be considered positive or complimentary (eg, benevolent ageism). Yet, stereotypes of all kinds disregard older adults’ individuality, reinforce narrow ideas of what older adults are supposed to be like, may be burdensome or patronizing, and are believed to be harmful to the health and wellbeing of the older adult population.90–92 Finally, we did not formally evaluate the quality of studies included in the review due to the diversity of study types included. Instead, we elected to mine this body of literature for its collective insight with some attention to indicators of quality that readers may consider. For these same reasons, a meta-analysis was not appropriate.
Conclusion
Findings across the 29 included studies provided moderate evidence that aging stigma was associated with a wide variety of adverse health outcomes among US adults over 65. The inclusion of varied study types (ie, experimental, intervention, cross-sectional quantitative, longitudinal quantitative, and qualitative) facilitated synthesis of what empirical studies have revealed about mechanisms through which aging stigma may affect health, directionality of these relationships, and unanswered questions for future research. The review compiled evidence that can be used to make the case that aging stigma is a public health hazard. It can also inform the development of tailored intervention strategies in the US to promote health and wellbeing among those categorized, whether by themselves or others, as older adults.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Link BG, Phelan JC. Conceptualizing stigma. Annu Rev Sociol. 2001;27:363–385. doi:10.1146/annurev.soc.27.1.363
2. Crocker J, Major B, Steele C. Social stigma. In: Gilbert DT, Fiske ST, editors. The Handbook of Social Psychology. Boston, MA: McGraw-Hill; 1998:504–553.
3. Goffman E. Stigma: Notes on the Management of Spoiled Identity. Englewood Cliffs, NJ: Prentice Hall; 1963.
4. Levy BR, Chung PH, Bedford T, Navrazhina K. Facebook as a site for negative age stereotypes. Gerontologist. 2014;54:172–176. doi:10.1093/geront/gns194
5. Allen JO. Ageism as a risk factor for chronic disease. Gerontologist. 2016;56:610–614. doi:10.1093/geront/gnu158
6. Angus J, Reeve P. Ageism: a threat to “aging well” in the 21st century. J Appl Gerontol. 2006;25:137–152. doi:10.1177/0733464805285745
7. Hagestad GO, Uhlenberg P. The social separation of old and young: a root of ageism. J Soc Issues. 2005;61:343–360. doi:10.1111/j.1540-4560.2005.00409.x
8. Flamion A, Missotten P, Jennotte L, Hody N, Adam S. Old age-related stereotypes of preschool children. Front Psychol. 2020;11:807. doi:10.3389/fpsyg.2020.00807
9. Levy B. Stereotype embodiment. Curr Dir Psychol Sci. 2009;6:332–336. doi:10.1111/j.1467-8721.2009.01662.x
10. Allen JO, Solway E, Kirch M, et al. Experiences of everyday ageism and the health of older US adults. JAMA Netw Open. 2022;5. doi:10.1001/jamanetworkopen.2022.17240
11. Levy BR, Slade MD, Chang ES, Kannoth S, Wang SY. Ageism amplifies cost and prevalence of health conditions. Gerontologist. 2020;60:174–181. doi:10.1093/geront/gny131
12. Steele CM. Whistling Vivaldi: And Other Stories of How Stereotypes Affect Us. New York: W.W. Norton & Company; 2010.
13. Abecassis M, Bridges ND, Clancy CJ, et al. Solid‐organ transplantation in older adults: current status and future research. Am J Transplant. 2012. doi:10.1111/j.1600-6143.2012.04245.x
14. Bender KA. An analysis of well-being in retirement: the role of pensions, health, and ‘voluntariness of retirement. J Socio Econ. 2012;41:424–433. doi:10.1016/jsocec.2011.05.010
15. Kydd A, Fleming A. Ageism and age discrimination in health care: fact or fiction? A narrative review of the literature. Maturitas. 2015;81:432–438. doi:10.1016/j.maturitas.2015.05.002
16. Weiss D, Lang FR. “They” are old but “I” feel younger: Age-group dissociation as a self-protective strategy in old age. Psychol Aging. 2012;27:153–163. doi:10.1037/a0024887
17. Research and Markets. Anti-aging products: global strategic business report; 2023. Available from: https://www.researchandmarkets.com/reports/2832312/anti-aging-products-global-strategic-business?utm_source=GNOM&utm_medium=PressRelease&utm_code=f2tbzm&utm_campaign=1416735+-+Anti-Aging+Products+Industry+Projected+to+be+Worth+%2483.2+Billion+by+2027+-+Key+Trends%2c+Opportunities+and+Players&utm_exec=joca220prd.
18. Creamer J, Shider EA, Burns K, Chen F. Poverty in the United States: 2021. US Census Bureau report P60-277; 2022. Available from: https://www.census.gov/library/publications/2022/demo/p60-277.html.
19. US Census Bureau. Voting and registration in the Election of November 2020. Press release number p20 tables; 2021. Available from: https://www.census.gov/data/tables/time-series/demo/voting-and-registration/p20-585.html.
20. Calasanti T, King N. Beyond successful aging 2.0: inequalities, ageism, and the case for normalizing old ages. J Gerontol B Psychol Sci Soc Sci. 2021;76:1817–1827. doi:10.1093/geronb/gbaa037
21. Chang ES, Kannoth S, Levy S, Wang SY, Lee JE, Levy BR. Global reach of ageism on older persons’ health: a systematic review. PLoS One. 2020;15. doi:10.1371/journal.pone.0220857
22. Hu RX, Luo M, Zhang A, Li LW. Associations of ageism and health: a systematic review of quantitative observational study studies. Res Aging. 2021;43:311–322. doi:10.1177/0164027520980130
23. Warmoth K, Tarrant M, Abraham C, Lang IA. Older adults’ perceptions of ageing and their health and functioning: a systematic review of observational study studies. Psychol Health Med. 2016;21:531–550. doi:10.1080/13548506.2015.1096946
24. Allen JO, White CJ, Moïse V, et al. Experiences of Aging in Society Project, July 2023 Report. : University of Oklahoma Stress and Health Disparities Lab; 2023. Available from: https://hdl.handle.net/11244/338894.
25. Iversen TN, Larsen L, Solem PE. A conceptual analysis of ageism. Nordic Psychol. 2009;61:4–22. doi:10.1027/1901-2276.61.3.4
26. Swift HJ, Abrams D, Lamont RA, Drury L. The risks of ageism model: how ageism and negative attitudes toward age can be a barrier to active aging. Soc Issues Policy Rev. 2017;11:195–231. doi:10.1111/sipr.12031
27. Kang H, Kim H. Ageism and psychological well-being among older adults: a systematic review. Gerontol Geriatr Med. 2022;8. doi:10.1177/23337214221087023
28. Allen JO, Solway E, Kirch M, Singer D, Kullgren JT, Malani PN. The everyday ageism scale: development and evaluation. J Aging Health. 2022. doi:10.1177/08982643211036131
29. Geronimus AT, Hicken M, Keene D, Bound J. “Weathering” and age patterns of allostatic load scores among blacks and whites in the United States. Am J Public Health. 2006;96:826–833. doi:10.2105/AJPH.2004.060749
30. Juster R-P, McEwen BS, Lupien SJ. Allostatic load biomarkers of chronic stress and impact on health and cognition. Neurosci Biobehav Rev. 2010;35:2–16. doi:10.1016/j.neubiorev.2009.10.002
31. Robb C, Chen H, Haley WE. Ageism in mental health and health care: a critical review. J Clin Geropsychology. 2002;8:1–12. doi:10.1023/A:1013013322947
32. Rutledge MS. What explains the widening gap in retirement ages by education. Report #18-10 center for retirement research at Boston college; 2018. Available from: https://crr.bc.edu/wp-content/uploads/2018/05/IB_18-10.pdf.
33. Allen JO, Elias LK, Greenwood JC. Differences and disparities in ageism affecting older adults: a review. Curr Epidemiol Rep. 2023;10:17–32. doi:10.1007/s40471-022-00316-6
34. World Health Organization. Global report on ageism; 2021.Available from: https://www.who.int/publications/i/item/9789240016866.
35. Ackerman LS, Chopik WJ. Cross-cultural comparisons in implicit and explicit age bias. Pers Soc Psychol Bull. 2021;47(6):953–968. doi:10.1177/0146167220950070
36. Lockenhoff CE, De Fruyt F, Terracciano A, et al. Perceptions of aging across 26 cultures and their culture-level associates. Psychol Aging. 2009;24(4):941–954. doi:10.1037/a0016901
37. North MS, Fiske ST. Modern attitudes toward older adults in the aging world: a cross-cultural meta-analysis. Psychol Bull. 2015;141(5):993–1021. doi:10.1037/a0039469
38. Barber SJ, Mather M. Stereotype threat can reduce older adults’ memory errors. Q J Exp Psychol. 2013;66:1888–1895. doi:10.1080/17470218.2013.840656
39. Hess TM, Auman C, Colcombe SJ, Rahhal TA. The impact of stereotype threat on age differences in memory performance. J Gerontol B Psychol Sci Soc Sci. 2003;58:3–11. doi:10.1093/geronb/58.1.P3
40. Barber SJ, Mather M, Gatz M. How stereotype threat affects healthy older adults’ performance on clinical assessments of cognitive decline: the key role of regulatory fit. J Gerontol B Psychol Sci Soc Sci. 2015;70:891–900. doi:10.1093/geronb/gbv009
41. Brubaker MS, Naveh-Benjamin M. The effects of stereotype threat on the associative memory deficit of older adults. Psychol Aging. 2018;33:17–29. doi:10.1037/pag0000194
42. Hess TM, Emery L, Queen TL. Task demands moderate stereotype threat effects on memory performance. J Gerontol B Psychol Sci Soc Sci. 2009;64B:482–486. doi:10.1093/geronb/gbp044
43. Hess TM, Growney CM, Lothary AF. Motivation moderates the impact of aging stereotypes on effort expenditure. Psychol Aging. 2019;34:56–67. doi:10.1037/pag0000291
44. Kotter-Grühn D, Hess TM. The impact of age stereotypes on self-perceptions of aging across the adult lifespan. J Gerontol B Psychol Sci Soc Sci. 2012;67:563–571. doi:10.1093/geronb/gbr153
45. Sarkisian CA, Steers WN, Hays RD, Mangione CM. Development of the 12-item expectations regarding aging survey. Gerontologist. 2005;45:240–248. doi:10.1093/geront/45.2.240
46. Krendl AC, Ambady N, Kensinger EA. The dissociable effects of stereotype threat on older adults’ memory encoding and retrieval. J Appl Res Mem Cogn. 2015;4:103–109. doi:10.1016/j.jarmac.2015.02.001
47. Molden J, Maxfield M. The impact of aging stereotypes on dementia worry. Eur J Ageing. 2017;14:29–37. doi:10.1007/s10433-016-0378-z
48. Levy BR. Improving memory in old age through implicit self-stereotyping. J Pers Soc Psychol. 1996;71:1092–1107. doi:10.1037/0022-3514.71.6.1092
49. Popham LE, Hess TM. Age differences in the underlying mechanisms of stereotype threat effects. J Gerontol B Psychol Sci Soc Sci. 2015;70:223–232. doi:10.1093/geronb/gbt093
50. Smith AM, Gallo DA, Barber SJ, Maddox KB, Thomas AK. Stereotypes, warnings, and identity-related variables influence older adults’ susceptibility to associative false memory errors. Gerontologist. 2017;57:S206–S215. doi:10.1093/geront/gnx057
51. Thomas AK, Dubois SJ. Reducing the burden of stereotype threat eliminates age differences in memory distortion. Psychol Sci. 2011;22:1515–1517. doi:10.1177/0956797611425932
52. Tan SC, Barber SJ. Confucian values as a buffer against age-based stereotype threat for Chinese older adults. J Gerontol B Psychol Sci Soc Sci. 2020;75:504–512. doi:10.1093/geronb/gby049
53. Thomas AK, Smith AM, Mazerolle M. The unexpected relationship between retrieval demands and memory performance when older adults are faced with age-related stereotypes. J Gerontol B Psychol Sci Soc Sci. 2018. doi:10.1093/geronb/gby031
54. Geraci L, Hughes ML, Miller TM, De Forrest RL. The effect of prior task success on older adults’ memory performance: examining the influence of different types of task success. Exp Aging Res. 2016;42:365–381. doi:10.1080/0361073X.2016.1191860
55. Chasteen AL, Bhattacharyya S, Horhota M, Tam R, Hasher L. How feelings of stereotype threat influence older adults’ memory performance. Exp Aging Res. 2005;31:235–260. doi:10.1080/03610730590948177
56. Levy BR, Chang ES, Lowe SR, Provolo N, Slade MD. Impact of media-based negative and positive age stereotypes on older individuals’ mental health. J Gerontol B Psychol Sci Soc Sci. 2022;77:e70–e75. doi:10.1093/geronb/gbab085
57. McDougall GJ, Monroe TB, Pituch KA, Carter MA, Abbott L. The impact of stereotype threat on memory and cognition in older adults. West J Nurs Res. 2022;44:1016–1026. doi:10.1177/01939459211029718
58. Dixon RA, Hultsch DF, Hertzog C. The metamemory in adulthood (MIA) questionnaire. Psychopharmacol Bull. 1988;24:671–688.
59. Menkin JA, Smith JL, Bihary JG. Brief Anti-ageism messaging effects on physical activity motivation among older adults. J Appl Gerontol. 2022;41:478–485. doi:10.1177/0733464820960925
60. Wurm S, Tesch-Römer C, Tomasik MJ. Longitudinal findings on aging-related cognitions, control beliefs, and health in later life. J Gerontol B Psychol Sci Soc Sci. 2007;62:P156–P164. doi:10.1093/geronb/62.3.p156
61. Andrews RM, Tan EJ, Varma VR, et al. Positive aging expectations are associated with physical activity among urban-dwelling older adults. Gerontologist. 2017;57:S178–S186. doi:10.1093/geront/gnx060
62. Han J. Chronic illnesses and depressive symptoms among older people: functional limitations as a mediator and self-perceptions of aging as a moderator. J Aging Health. 2018;30:1188–1204. doi:10.1177/0898264317711609
63. Lawton MP. The Philadelphia geriatric center morale scale: a revision. J Gerontol. 1975;30:85–89. doi:10.1093/geronj/30.1.85
64. Levy BR, Slade MD, Murphy TE, Gill TM. Association between positive age stereotypes and recovery from disability in older persons. JAMA. 2012;308:1972. doi:10.1001/jama.2012.14541
65. Levy B, Langer E. Aging free from negative stereotypes: successful memory in China and among the American deaf. J Pers Soc Psychol. 1994;66:989–997. doi:10.1037/0022-3514.66.6.989
66. Levy BR, Pietrzak RH, Slade MD. Societal impact on older persons’ chronic pain: roles of age stereotypes, age attribution, and age discrimination. Soc Sci Med. 2023;323:115772. doi:10.1016/j.socscimed.2023.115772
67. Levy BR, Chung PH, Slade MD, Van Ness PH, Pietrzak RH. Active coping shields against negative aging self-stereotypes contributing to psychiatric conditions. Soc Sci Med. 2019;228:25–29. doi:10.1016/j.socscimed.2019.02.035
68. Palmore E. The ageism survey: first findings. Gerontologist. 2001;41:572–575. doi:10.1093/geront/41.5.572
69. Levy BR, Ashman O, Slade MD. Age attributions and aging health: contrast between the United States and Japan. J Gerontol B Psychol Sci Soc Sci. 2009;64:335–338. doi:10.1093/geronb/gbp002
70. Levy BR, Slade MD, Chung PH, Gill TM. Resiliency over time of elders’ age stereotypes after encountering stressful events. J Gerontol B Psychol Sci Soc Sci. 2015;70:886–890. doi:10.1093/geronb/gbu082
71. Williams DR, Yan Y, Jackson JS, Anderson NB. Racial differences in physical and mental health: socio-economic status, stress and discrimination. J Health Psychol. 1997;2:335–351. doi:10.1177/135910539700200305
72. Levy BR, Slade MD, Pietrzak RH, Ferrucci L. Positive age beliefs protect against dementia even among elders with high-risk gene. PLoS One. 2018;13:e0191004. doi:10.1371/journal.pone.0191004
73. Levy BR, Slade MD, Pietrzak RH, Ferrucci L. When culture influences genes: positive age beliefs amplify the cognitive-aging benefit of APOE ε2. J Gerontol B Psychol Sci Soc Sci. 2020;75:e198–e203. doi:10.1093/geronb/gbaa126
74. Levy BR, Slade MD. Role of positive age beliefs in recovery from mild cognitive impairment among older persons. JAMA Netw Open. 2023;6:e237707. doi:10.1001/jamanetworkopen.2023.7707
75. McDarby M, Ju CH, Picchiello MC, Carpenter BD. Older adults’ perceptions and experiences of ageism during the COVID‐19 pandemic. J Soc Issues. 2022;78:939–964. doi:10.1111/josi.12557
76. Steward A, Hasche L. Exploring lifestyle activities to reduce internalized ageism: self-efficacy as a mediator between exercise, volunteering, computer use, and self-perceptions of aging. Int J Aging Hum Dev. 2022;94:255–272. doi:10.1177/00914150211024175
77. Voelkner AR, Caskie GIL. Awareness of age-related change and its relationship with cognitive functioning and ageism. Neuropsychol Dev Cogn B Aging Neuropsychol Cogn. 2022;1–20. doi:10.1080/13825585.2022.2088682
78. Diehl M, Brothers AF, Wahl H-W, Gabrian M. Awareness of Age-Related Change 50-Item Questionnaire (AARC-50): Measurement Guide. Colorado State University; 2018.
79. Makris UE, Higashi RT, Marks EG, et al. Ageism, negative attitudes, and competing co-morbidities – why older adults may not seek care for restricting back pain: a qualitative study. BMC Geriatr. 2015;15:39. doi:10.1186/s12877-015-0042-z
80. Mayo DM, Meuser TM, Robnett RH, Webster ME, Woolard CE. Cross-generational understandings of ageism and its perceived impacts on personal-public health. J Gerontol Soc Work. 2022;65:711–727. doi:10.1080/01634372.2021.2019865
81. Wallhagen MI. The stigma of hearing loss. Gerontologist. 2010;50:66–75. doi:10.1093/geront/gnp107
82. Sonnega A, Weir DR. The health and retirement study: a public data resource for research on aging. Open Health Data. 2014;2. doi:10.5334/ohd.am
83. Fogle BM, Tsai J, Mota N, et al. The national health and resilience in veterans study: a narrative review and future directions. Front Psychiatry. 2020;11:538218. doi:10.3389/fpsyt.2020.538218
84. Gill TM, Han L, Gahbauer EA, Leo-Summers L, Murphy TE. Cohort profile: The precipitating events project (pep study). J Nutr Health Aging. 2020;24:438–444. doi:10.1007/s12603-020-1341-4
85. Watson D, Clark LA. Negative affectivity: the disposition to experience aversive emotional states. Psychol Bull. 1984;96:465–490. doi:10.1037/0033-2909.96.3.465
86. Levy BR, Banaji MR. Implicit ageism. In: Nelson T, editor. Ageism: Stereotyping and Prejudice Against Older Persons. Cambridge, MA: MIT Press; 2002:49–75.
87. Sargent-Cox KA, Anstey KJ, Luszcz MA. The relationship between change in self-perceptions of aging and physical functioning in older adults. Psychol Aging. 2012;27:750–760. doi:10.1037/a0027578
88. Van Vleck M. Age-inclusive language: are you using it in your writing and everyday speech?. Washington: Institute for Public Health; University in St. Louis; 2022; Available from: https://publichealth.wustl.edu/age-inclusive-language-are-you-using-it-in-your-writing-and-everyday-speech/.
89. Ng R, Allore HG, Trentalange M, Monin JK, Levy BR. Increasing negativity of age stereotypes across 200 years: evidence from a database of 400 million words. PLoS One. 2015;10:e0117086. doi:10.1371/journal.pone.0117086
90. Chonody JM. Positive and negative ageism: the role of benevolent and hostile sexism. Affilia. 2016;31:207–218. doi:10.1177/0886109915595839
91. Minichiello V, Browne J, Kendig H. Perceptions and consequences of ageism: views of older people. Ageing Soc. 2000;20:253–278. doi:10.1017/S0144686X99007710
92. Vale MT, Bisconti TL, Sublett JF. Benevolent ageism: attitudes of overaccommodative behavior toward older women. J Soc Psychol. 2020;160:548–558. doi:10.1080/00224545.2019.1695567
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.