Back to Journals » Clinical Ophthalmology » Volume 19
Age-Related Variations in Anterior, Posterior, and Total Corneal Astigmatism
Authors Pothikamjorn T, Surawatsatien N, Ueathaweephol S, Somkijrungroj T
Received 17 April 2025
Accepted for publication 16 July 2025
Published 8 August 2025 Volume 2025:19 Pages 2595—2605
DOI https://doi.org/10.2147/OPTH.S531740
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Thananop Pothikamjorn,1 Nuntachai Surawatsatien,2,3 Somtaporn Ueathaweephol,3 Thanapong Somkijrungroj2,3
1Faculty of Medicine, Chulalongkorn University and King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand; 2Center of Excellence in Retina, Faculty of Medicine, Chulalongkorn University and King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand; 3Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University and King Chulalongkorn Memorial Hospital, Thai Red Cross Society, Bangkok, Thailand
Correspondence: Thanapong Somkijrungroj, Department of Ophthalmology, Faculty of Medicine, Chulalongkorn University and King Chulalongkorn Memorial Hospital, 1873 Rama IV Road, Pathumwan, Bangkok, 10330, Thailand, Tel +66 86 366 4020, Email [email protected]
Introduction: Toric intraocular lens (IOL) calculation has traditionally relied on anterior corneal astigmatism (KA), but recent trends emphasize incorporating posterior corneal astigmatism (PCA) and total corneal astigmatism (TCA). However, age-related changes and sex-based differences in PCA and TCA remain inconclusive due to limited sample sizes in previous studies.
Methods: We conducted a cross-sectional observational study using biometric measurements obtained with the IOLMaster 700. Patients with warning and failed history of corneal transplant or keratoconus were excluded. The objective was to evaluate age-related changes and sex-based differences in KA, PCA, and TCA among patients undergoing cataract surgery at a tertiary care center in Thailand.
Results: A total of 23,932 eyes were analyzed for KA, and 9,546 eyes for PCA and TCA. Data were visualized using double-angle plots. PCA demonstrated a distinctive three-point star distribution, predominantly oriented along the with-the-rule (WTR) axis, with against-the-rule (ATR) astigmatism being rare in younger patients as illustrated in graphical abstract. Across KA, PCA, and TCA, the prevalence of ATR astigmatism increased in older age group, while WTR orientation decreased. A marked shift from WTR to ATR orientation was observed at different age thresholds: 60– 65 years for KA, 75– 80 years for PCA, and 55– 65 years for TCA. KA and TCA also exhibited a preferential shift toward superonasal oblique orientation with advancing age—a pattern not observed in PCA. No significant sex-based differences were observed in mean astigmatism vector distributions across age groups.
Conclusion: Clinicians should account for age-related shifts in KA, PCA, and TCA when selecting toric IOLs, particularly in patients younger than 55 years. Preoperative counseling should address potential long-term shifts toward ATR orientation, which may influence visual outcomes in patients receiving toric IOLs aligned along other axes. Incorporating these changes into toric IOL formulae may improve patient outcomes.
Plain Language Summary: In this study, we examined how the curvature and orientation of the cornea, specifically the anterior (front), posterior (back), and total corneal astigmatism, change with age and whether there are any differences between males and females. Astigmatism is when the cornea is not perfectly round, which can cause blurred vision. For patients undergoing cataract surgery, toric intraocular lenses (IOLs) are often used to correct this condition. Traditionally, surgeons have focused only on the front part of the cornea when planning for toric IOLs, but recent advances highlight the importance of also considering the back surface and total astigmatism of the cornea. By analyzing data from nearly 24,000 eyes, we discovered that astigmatism tends to shift in orientation as people age, from a with-the-rule (WTR) pattern commonly seen in younger patients to an against-the-rule (ATR) pattern in older adults. This shift happens at different ages for different layers of the cornea with changes showing as early as age 55. We also found that this shift often moves toward a nasal side in the front and total corneal surfaces, but not in the posterior surface. Importantly, we did not observe any meaningful differences between males and females. These findings suggest that age plays a significant role in determining astigmatism patterns and should be considered when selecting and aligning toric IOLs, especially for younger patients who may continue to experience changes in corneal shape over time. Discussing these potential future shifts with patients before surgery may help improve satisfaction and long-term visual outcomes.
Keywords: anterior corneal astigmatism, posterior corneal astigmatism, total corneal astigmatism, corneal orientation, toric-IOL, cataract surgery
Introduction
In ophthalmology, personalized medicine is gaining prominence, with cataract surgery being a key example of its application. Phacoemulsification, involving the removal of the cataractous lens and precise implantation of an intraocular lens (IOL) into the capsular bag, has become a standard procedure worldwide.1 Standard nontoric lenses often result in residual astigmatism and reduced uncorrected visual acuity.2 Although this residual astigmatism can be corrected postoperatively with glasses, refractive surgery,3 or intraoperatively with techniques such as limbal relaxing incisions or extended-on-axis incision,4 these options can be unpredictable and less effective than toric IOLs, particularly in patients with high corneal astigmatism.2,5 As patient expectations for optimal refractive outcomes and reduced dependence on eyeglasses increase, toric IOLs are becoming more widely used than standard nontoric lenses.6
Accurate calculation of the appropriate toric IOL for each eye is essential to ensure satisfactory postoperative visual acuity. Corneal orientations are crucial because toric IOLs must be aligned along a specific axis.7 Various formulas take into account patient-specific factors, including anterior corneal astigmatism (keratometric astigmatism, KA), posterior corneal astigmatism (PCA), and importantly, total corneal astigmatism (TCA), which encompasses both KA and PCA.8 Previous studies reported KA tends to rotate nasally with age, shifting from with-the-rule (WTR) astigmatism to against-the-rule (ATR) astigmatism after age 70, with differences observed between the sexes.9–11 However, the changes of PCA and TCA had not been clearly described, in part because of the restricted sample sizes used in previous studies.9,12
The precision required for toric IOL implantation also demands careful surgical planning, as surgically induced astigmatism can affect the KA, PCA, and TCA in all orientations.6 Understanding the incidence and orientation of KA, PCA, and especially TCA across age groups is critical for optimizing surgical outcomes.13 Our primary outcome was to assess age-related changes and sex-based differences in KA, PCA, and TCA among patients undergoing cataract surgery. We aimed to provide comprehensive data on these corneal astigmatism parameters in larger population, particularly in younger patients requiring cataract surgery, to support more informed preoperative counseling and enhance toric IOL selection for improved surgical outcomes.
Methods
Study Design
This is a cross-sectional observational study conducted in the Department of Ophthalmology, King Chulalongkorn Memorial Hospital. We report the data regarding the STROBE and RECORD statement guidelines for reporting observational studies.14,15
Participants
We included data from patients who had undergone measurements before cataract surgery with a Zeiss IOLMaster 700 (Carl Zeiss Meditec) swept-source optical coherence tomography biometer from the first use of the machine in June 2016 to November 2022. We excluded data from patients younger than 18 years old because of ethical considerations. Other exclusion criteria included data from patients with pseudophakia or aphakia, or those who had undergone laser vision correction (LVC), such as laser in situ keratomileusis (LASIK), photorefractive keratectomy (PRK), or radial keratotomy (RK). We excluded data from patients with instrument warnings and failed keratometry acquisitions, keratoconus, and corneal transplants. No data exclusions were applied based on vitreous status.
Data Collection
Data were collected from biometric measurements made using IOLMaster 700 biometers. Acquisition dates and times were noted in addition to demographic data, which included sex, date of birth, and eye laterality. The measurements included anterior, posterior, and measured total corneal radii in millimeters, and measurements of flat corneal radii and steep corneal radii along with their respective axes.
Data Analysis
All biometric data were tabulated using Microsoft Excel 2021. Statistical analyses were conducted using StataSE18 (StataCorp). The steep axis orientation was categorized as follows: 0°–22.5° and 157.5°–180° were classified as ATR astigmatism, 67.5°–112.5° as WTR astigmatism, and 22.5°–67.5° and 112.5°–157.5° as oblique astigmatism (OBL). For the right eye, the superonasal region was defined as 22.5°–67.5° and the superotemporal region was defined as 112.5°–157.5°. For the left eye, the superonasal and superotemporal regions were mirrored using the formula (180°–α), where α represents the angle of the steep axis. For statistical analysis, all corneal radii (mm) were calculated to keratometry in diopters (D) using the formula  , with a keratometry refractive index (Ki) of 1.3375. ΔK (D) was subsequently used to analyze the incidence of astigmatic power. A data point is considered an outlier if it is more than 1.5 interquartile range above the third quartile or below the first quartile.
, with a keratometry refractive index (Ki) of 1.3375. ΔK (D) was subsequently used to analyze the incidence of astigmatic power. A data point is considered an outlier if it is more than 1.5 interquartile range above the third quartile or below the first quartile.
A double-angle plot generated using Python 3 (Python Software Foundation) via Google Colab (Alphabet Inc) was employed to visually assess age-related changes in the distribution of corneal astigmatism orientations.
Results
We collected 45,622 measurements from two swept-source optical coherence tomography biometers. After the exclusion criteria were applied, data from 3,928 eyes with aphakic lens status, phakic IOL, piggyback IOL, or pseudophakia were excluded, along with that from 628 patients who had undergone LVC. Data from 872 failed measurements and 3,655 eyes with quality warning indices were excluded. Further exclusions included data from 21 eyes with keratoconus, 208 with pre- or postcorneal transplants, and 91 from patients younger than 18 years. Ultimately, data from 23,932 eyes remained for KA analysis, and data from 9,546 eyes were available for posterior and total corneal astigmatism analysis, as shown in a flow diagram of the inclusion and exclusion process in Figure 1.
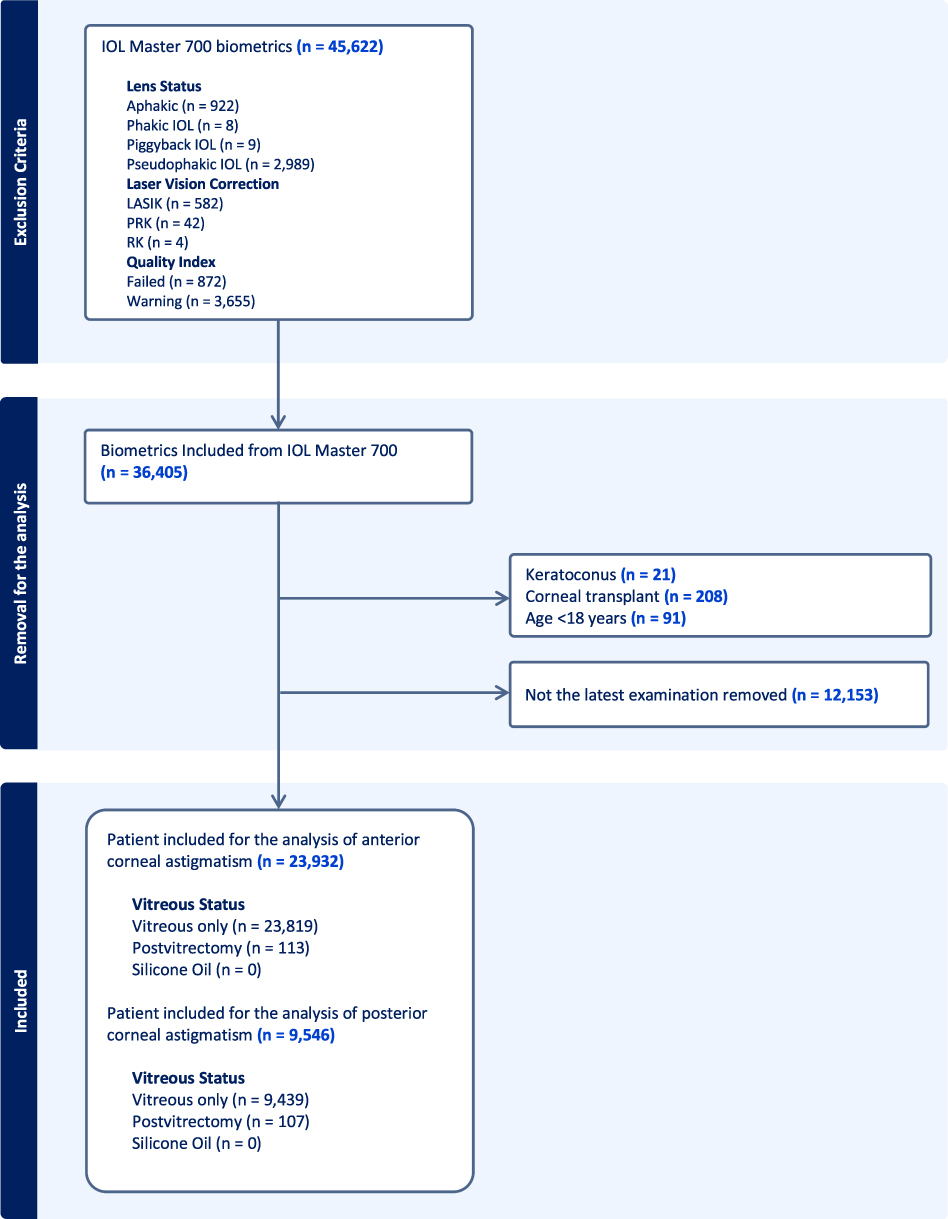 |
Figure 1 Flowchart of the inclusion and exclusion processes. Abbreviations: IOL, intraocular lens; LASIK, laser in situ keratomileusis; PRK, photorefractive keratectomy; RK, radial keratotomy. |
Age Related Changes of Corneal Astigmatism
The demographic data and the orientations of KA, PCA, and TCA are presented in Table 1. The distribution of astigmatism orientations is visualized using double-angle plots in the graphical abstract, with subgroup analyses by age group presented in Figure 2. Both KA and TCA showed a predominantly WTR orientation in younger individuals, gradually shifting toward an ATR orientation with increasing age. PCA demonstrated a distinctive three-point star distribution, predominantly aligned along the WTR axis. True vertical (90°) orientations were notably rare among WTR cases, while ATR orientations were minimal, particularly in the true horizontal direction (0° and 180°). PCA also demonstrated a trend within the center in the double-angle plot, indicating a low PCA power in every age group. A general shift from WTR to ATR orientation was observed, occurring at different age ranges: 60–65 years for KA, 75–80 years for PCA, and 55–60 years for TCA. KA and TCA powers also increased by approximately 1 D after the orientation stabilized, occurring between ages 65–80 years for KA and between 60–80 years for TCA; this trend was not observed in PCA. The mean astigmatism vectors across age groups were illustrated in the double-angle plot in Figure 3.
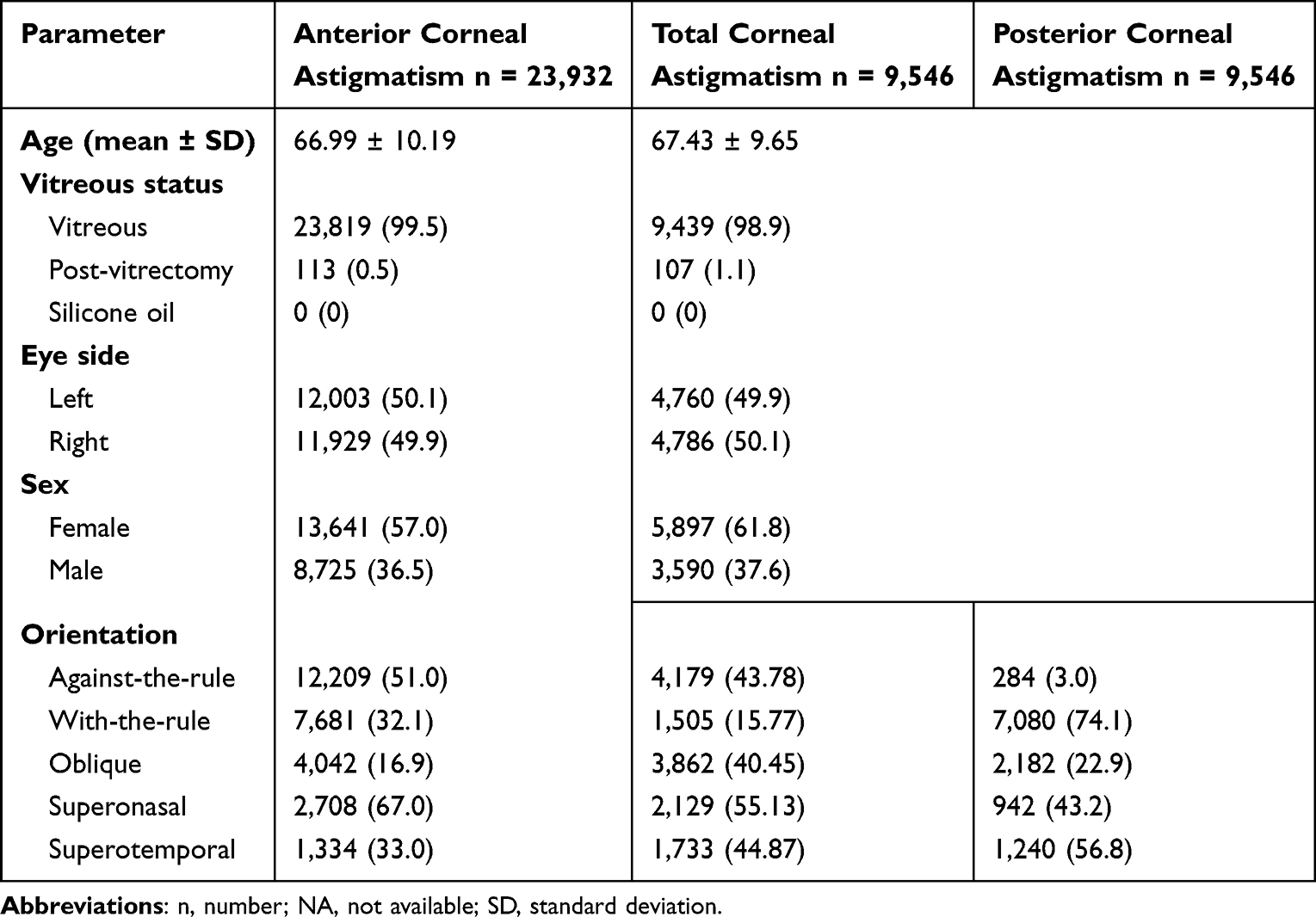 |
Table 1 Demographic Data of Patients Included in This Study |
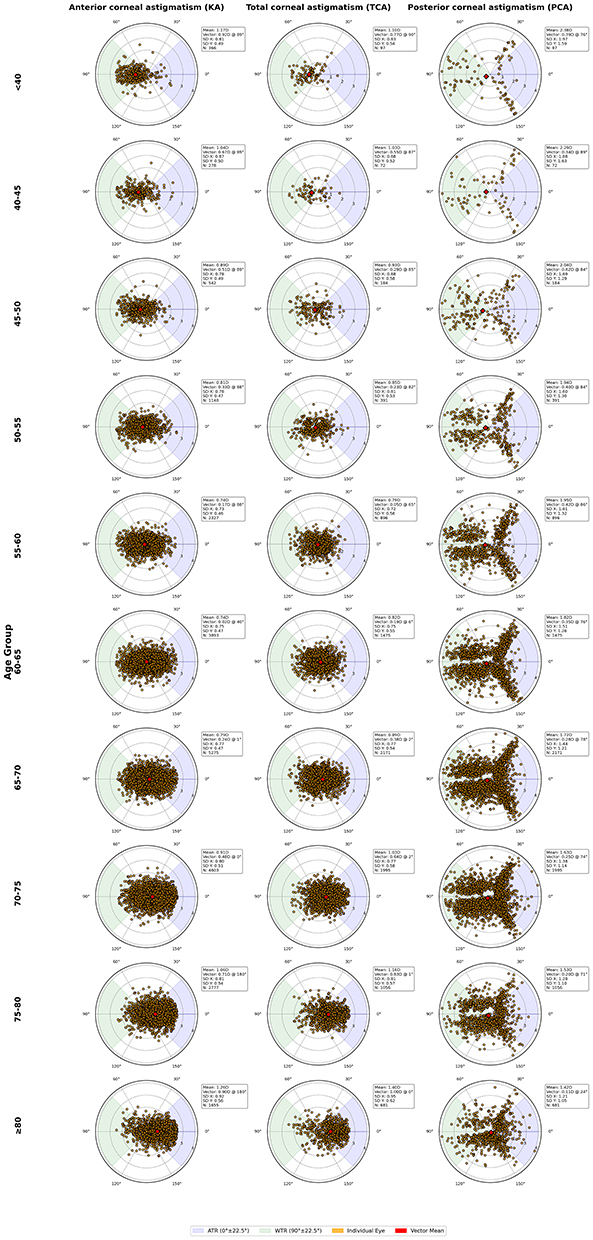 |
Figure 2 Double-angle plot of anterior, total and posterior corneal astigmatism across age groups. Abbreviations: n, number; SD, standard deviation. |
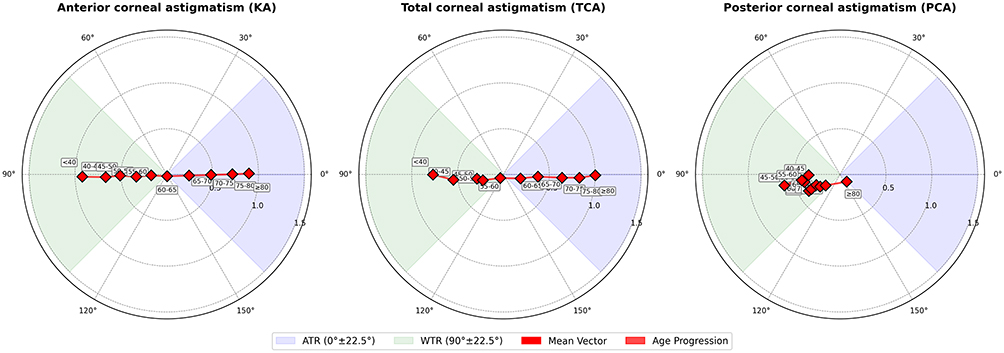 |
Figure 3 Double-angle plot of mean vectors of each age group of anterior, total and posterior corneal astigmatism. |
Corneal Astigmatism Changes in Each Eye Side and Sex
In both eyes, the KA and TCA mean vectors tended to shift from a WTR orientation toward an ATR orientation towards superonasal region between 55 and 70 years, although this change was not observed in PCA. The mean astigmatism vectors across age groups, compared between the right and left eyes, were illustrated in the double-angle plot in Figure 4. Visual inspection of the plots revealed no clinical significance in mean astigmatism vector distributions between male and female patients across age groups. The mean astigmatism vectors across age groups, compared between the male and females, were illustrated in the double-angle plot in Figure 5. Astigmatic powers increment did not have clinically significant difference to the right and left eyes and male and female patients.
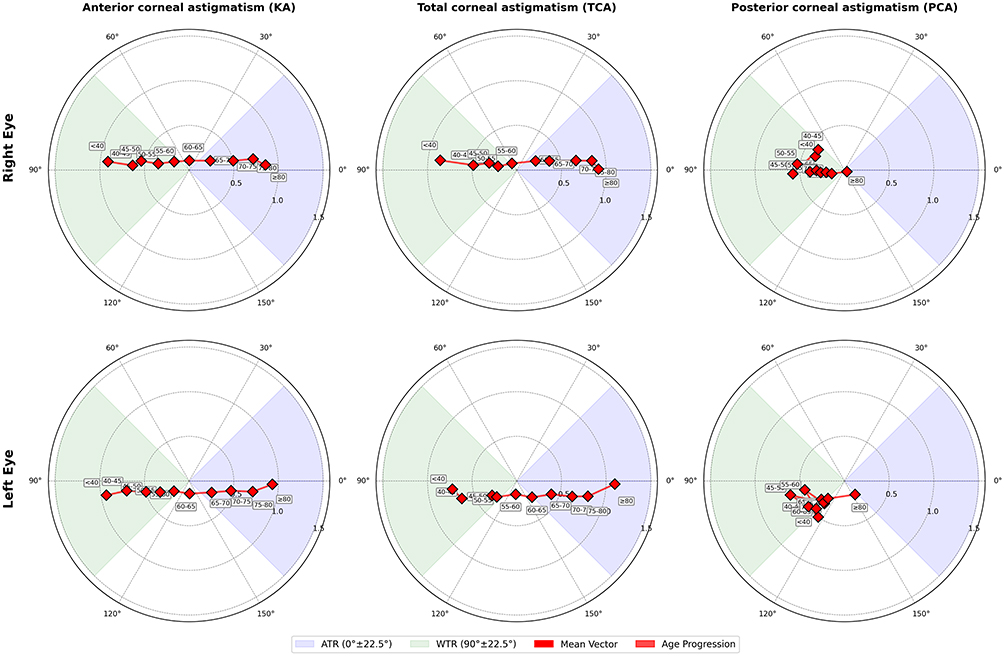 |
Figure 4 Double-angle plot of mean vectors of each age group of anterior, total and posterior corneal astigmatism compared between right and left eye. Abbreviations: OD, right eye; OS, left eye. |
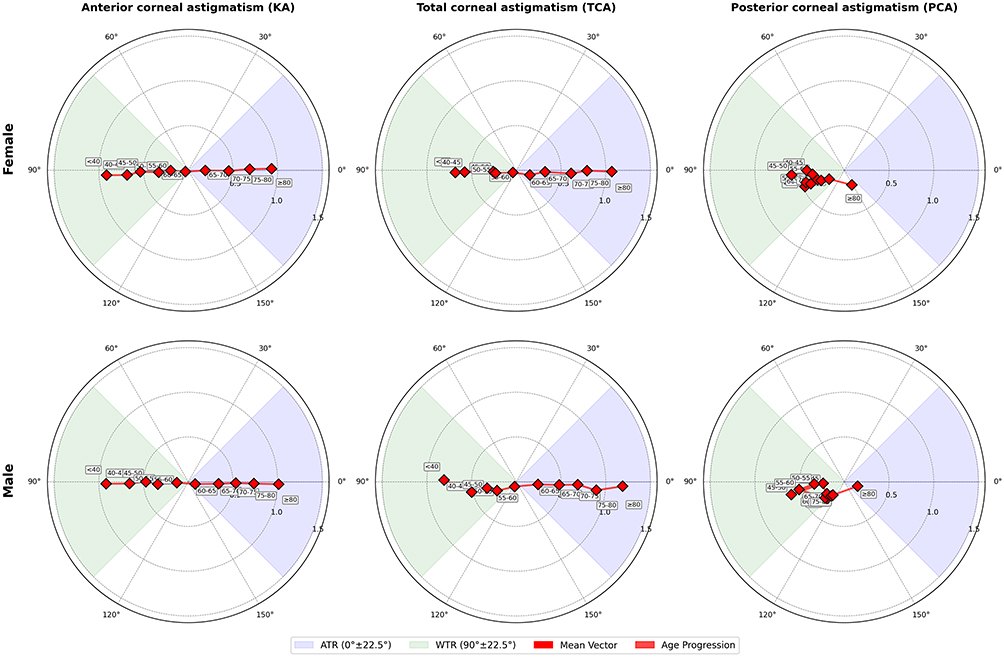 |
Figure 5 Double-angle plot of mean vectors of each age group of anterior, total and posterior corneal astigmatism compared between male and female. Abbreviations: OD, right eye; OS, left eye. |
Discussion
We observed a decrease in WTR incidence and an increase in the ATR orientation of KA in older age group which is consistent with previous findings of an age-related transition from WTR to ATR.9,11,16–19 We also observed an increase in the OBL orientation of the KA and TCA, particularly in the superonasal regions. Our findings were consistent with a previous report that clinical considerations are crucial when evaluating KA changes in older age group, particularly in the context of cataract surgery involving toric IOL implantation.20 For patients younger than 55 years, clinicians should exercise caution when implanting toric IOLs, as corneal astigmatic orientation may continue to shift with age. Such changes could result in visual deterioration due to cylindrical refractive error and higher-order aberrations arising from misalignment between the corneal steep axis and the IOL. Furthermore, postoperative monitoring of IOL alignment can help ensure optimal visual outcomes. We recommend individualized surgical planning for patients undergoing cataract surgery, especially in patients age under 55, rather than a one-size-fits-all approach to toric IOLs implantation. Nonetheless, we do not recommend delaying cataract surgery in younger patients when it is clinically indicated.
We also identified a distinct three-point star pattern in the double-angle plot for PCA, with very few ATR and true vertical (90°) cases observed in younger patients. This distribution may reflect congenital characteristics of the posterior cornea. These findings have important implications for toric IOL formulas, which often assume PCA to be oriented along the vertical axis.21 Our results suggest that such assumptions may not hold true across all age groups and should be reconsidered in younger patients. The prevalence of ATR-oriented PCA increased with age, indicating a gradual shift toward ATR alignment, which mirrors the pattern observed in the anterior cornea, albeit occurring more slowly. This finding contrasts with previous studies that reported no significant age-related rotation in PCA orientation.9,18 The similar rotational trends observed in both KA and TCA but not in PCA, suggesting that KA has a greater influence on TCA than PCA. While external factors such as eyelid closure primarily affect the anterior cornea, they may still exert some influence on PCA as well. Additionally, we observed a decrease in PCA power with advancing age. We hypothesize that this may result from age-related structural changes in the globe and anterior chamber, leading to a more circular, rather than cylindrical, posterior corneal shape. In cases where PCA and TCA are measured with appropriated cautions; we recommended IOL calculation formulae such as the Barrett True-K TK and the Emmetropia Verifying Optical (EVO) formula may be particularly useful.
When comparing laterality, the mean vectors of KA and TCA were predominantly located in the superonasal quadrant, suggesting a nasal shift tendency that aligns with findings from previously reported studies.9 However, the relatively high incidence of OBL in our dataset may be influenced by referral bias, as our tertiary teaching hospital often manages more complex cases with multiple ocular or systemic comorbidities. We did not observe any notable sex-based differences in KA, PCA, or TCA, suggesting that corneal astigmatism patterns may be individually determined and not influenced by sex, in contrast to findings reported in some previous studies.10
One of the strengths of our study is the inclusion of all patients who underwent biometric measurements using a Zeiss IOLMaster 700, minimizing selection bias. Our relatively large sample size and the inclusion of both eyes provide a robust representation of the general population in Thailand. Moreover, the biometric data were collected using strict exclusion criteria, such as the omission of cases with poor quality indices, corneal transplants, or keratoconus, which improved the precision of our measurements. However, excluding patients with poor quality indices may have slightly skewed the true incidence of corneal astigmatism, as surgeons often proceed with surgery despite these limitations, potentially leading to minor discrepancies.
Nevertheless, several limitations are acknowledged. Incomplete eye histories might have hindered our ability to assess each eye’s condition fully, and medical records may not have documented all relevant corneal pathologies. We did not include patients younger than 18 years, which limits the generalizability of our findings to pediatric populations. Other factors beyond KA, PCA, and TCA, such as retinal disease and patient preferences, also influence decisions regarding toric IOL implantation. Excluding patients with previous LVC or silicone oil implantation may have skewed our data because these conditions can alter the KA, PCA, and TCA parameters. Moreover, the double-angle plot may not depict the corneal shape as fully as in previous studies that utilized Scheimpflug tomography or videokeratography.10 Cross-sectional studies cannot determine the age-related shifts for individual patients but instead indicate trends across the population. Ethnic or geographic factors may influence the findings, as the study population was exclusively from Thailand, potentially limiting the generalizability of the results to other populations. Surgeons should carefully consider altered parameters and select the most appropriate IOL calculation formula for individual cases, considering age related changes of astigmatism. Future multicenter prospective longitudinal studies are warranted to address these limitations. Further studies should investigate the associations of KA, PCA, and TCA with surgical techniques and visual outcomes, ultimately improving cataract surgery counseling and approach in younger patients. Additionally, evaluating visual outcomes and patient satisfaction in PCA–based IOLs selection may help clarify the clinical impact of incorporating PCA into IOL calculations.
Conclusions
This study provides new insights into the age-related changes in the orientation of KA, PCA, and TCA, with no significant sex-based differences observed. We identified a clear shift from WTR to ATR astigmatism strongly associated within older age group. Additionally, the mean astigmatism vectors in KA and TCA showed a trend toward superonasal OBL orientations, suggesting a medial shift in KA and TCA with age. These findings may serve as a foundation for developing age-specific toric IOL calculation formulas and offer valuable guidance for toric IOL selection and long-term visual outcome counseling, particularly in younger patients. Surgeons should exercise caution and provide appropriate counseling when considering toric IOL implantation in younger patients due to ongoing age-related astigmatic shifts.
Data Sharing Statement
The data for our study are publicly available. Study protocol and dataset can be requested from the corresponding author by [email protected] upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Institutional Review Board of the Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand (COA No. 1333/2022), and conducted in compliance with the principles of the Declaration of Helsinki and its later amendments (2013), the Belmont Report, CIOMS Guidelines, and the International Conference on Harmonization in Good Clinical Practice (ICH-GCP). Due to the retrospective nature of the study, informed consent was not obtained. However, access to the patient database and electronic medical records was granted with a formal permission letter from the director of King Chulalongkorn Memorial Hospital. This hospital, a public general and tertiary referral center in Bangkok with approximately 1,500 beds, is operated by the Thai Red Cross Society and serves as the teaching hospital for the Faculty of Medicine, Chulalongkorn University. To ensure confidentiality, all data were de-identified and cannot be traced back to individual patients.
Acknowledgments
We extend our gratitude to Dr Tun Kuan Yeo of the National Healthcare Group Eye Institute, Tan Tock Seng Hospital, Singapore, for his invaluable recommendations for this study. We also thank Chitipat Trachu, BE of the Faculty of Engineering, Chulalongkorn University for his guidance for coding in this study. We thank Robin James Storer, PhD, from the English Language Editing Service at the Faculty of Medicine, Chulalongkorn University for editing a draft of this manuscript. We carefully reviewed and edited the results to ensure that the content is accurate and valid; that there are no concerns about potential plagiarism; that all relevant sources are cited; and that all statements in the article reporting hypotheses, interpretations, results, conclusions, limitations, and implications of the study represent the authors’ own ideas.
Funding
We did not receive any specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
None of the authors declare any potential conflicts of interest for this work.
References
1. Asbell PA, Dualan I, Mindel J, Brocks D, Ahmad M, Epstein S. Age-related cataract. Lancet. 2005;365(9459):599–609. doi:10.1016/s0140-6736(05)17911-2
2. Singh A, Pesala V, Garg P, Bharadwaj SR. Relation between uncorrected astigmatism and visual acuity in pseudophakia. Optom Vis Sci. 2013;90(4):378–384. doi:10.1097/OPX.0b013e318288afb5
3. Blehm C, Potvin R. Pseudophakic astigmatism reduction with femtosecond laser-assisted corneal arcuate incisions: a pilot study. Clin Ophthalmol. 2017;11:201–207. doi:10.2147/opth.S127279
4. Mohammad-Rabei H, Mohammad-Rabei E, Espandar G, et al. Three methods for correction of astigmatism during phacoemulsification. J Ophthalmic Vis Res. 2016;11(2):162–167. doi:10.4103/2008-322x.183924
5. Oshika T, Sugita G, Tanabe T, Tomidokoro A, Amano S. Regular and irregular astigmatism after superior versus temporal scleral incision cataract surgery. Ophthalmology. 2000;107(11):2049–2053. doi:10.1016/s0161-6420(00)00379-1
6. Singh VM, Ramappa M, Murthy SI, Rostov AT. Toric intraocular lenses: expanding indications and preoperative and surgical considerations to improve outcomes. Indian J Ophthalmol. 2022;70(1):10–23. doi:10.4103/ijo.IJO_1785_21
7. Koch DD, Ali SF, Weikert MP, Shirayama M, Jenkins R, Wang L. Contribution of posterior corneal astigmatism to total corneal astigmatism. J Cataract Refract Surg. 2012;38(12):2080–2087. doi:10.1016/j.jcrs.2012.08.036
8. Ferreira TB, Ribeiro F. How can we improve toric intraocular lens calculation methods? Current insights. Clin Ophthalmol. 2020;14:1899–1908. doi:10.2147/opth.S238686
9. Naeser K, Savini G, Bregnhøj JF. Age-related changes in with-the-rule and oblique corneal astigmatism. Acta Ophthalmol. 2018;96(6):600–606. doi:10.1111/aos.13683
10. Hayashi K, Sato T, Sasaki H, Hirata A, Yoshimura K. Sex-related differences in corneal astigmatism and shape with age. J Cataract Refract Surg. 2018;44(9):1130–1139. doi:10.1016/j.jcrs.2018.06.020
11. Kim H, An Y, Joo CK. Gender-differences in age-related changes of corneal astigmatism in Korean cataract patients. BMC Ophthalmol. 2019;19(1):31. doi:10.1186/s12886-018-1001-1
12. Hayashi K, Uno K, Manabe SI, Hirata A. Prevalence and characteristics of oblique astigmatism. Eye. 2023;37(15):3174–3179. doi:10.1038/s41433-023-02470-7
13. Holladay JT, Pettit G. Improving toric intraocular lens calculations using total surgically induced astigmatism for a 2.5 mm temporal incision. J Cataract Refract Surg. 2019;45(3):272–283. doi:10.1016/j.jcrs.2018.09.028
14. Benchimol EI, Smeeth L, Guttmann A, et al. The REporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement. PLoS Med. 2015;12(10):e1001885. doi:10.1371/journal.pmed.1001885
15. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/s0140-6736(07)61602-x
16. Ho JD, Liou SW, Tsai RJ, Tsai CY. Effects of aging on anterior and posterior corneal astigmatism. Cornea. 2010;29(6):632–637. doi:10.1097/ICO.0b013e3181c2965f
17. Wu Z, Liu C, Chen Z. Prevalence and age-related changes of corneal astigmatism in patients undergoing cataract surgery in Northern China. J Ophthalmol. 2020;2020:6385098. doi:10.1155/2020/6385098
18. Ueno Y, Hiraoka T, Beheregaray S, Miyazaki M, Ito M, Oshika T. Age-related changes in anterior, posterior, and total corneal astigmatism. J Refract Surg. 2014;30(3):192–197. doi:10.3928/1081597x-20140218-01
19. Namba H, Sugano A, Nishi K, et al. Age-related variations in corneal geometry and their association with astigmatism: the Yamagata Study (Funagata). Medicine. 2018;97(43):e12894. doi:10.1097/md.0000000000012894
20. Shao X, Zhou KJ, Pan AP, et al. Age-related changes in corneal astigmatism. J Refract Surg. 2017;33(10):696–703. doi:10.3928/1081597x-20170718-04
21. Stewart S, Yeo TK, Moutari S, McNeely R, Moore JE. Accuracy of toric intraocular lens formulas with measured posterior corneal astigmatism of different orientations. Am J Ophthalmol. 2024;266:26–36. doi:10.1016/j.ajo.2024.04.029
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of Ocular Residual Astigmatism in Eyes with Myopia and Myopic Astigmatism and Its Interaction with Other Forms of Astigmatism
Elshahat A, Hamed AM, El Habbak AH, Tabl MA
Clinical Ophthalmology 2022, 16:4179-4190
Published Date: 15 December 2022