Back to Journals » Open Access Journal of Clinical Trials » Volume 18
Africa’s Regulatory Revolution: How Harmonized Regulation Can Transform Global Clinical Trials
Authors Balinda HU ![]() , Tchafa A, Tchafa F
, Tchafa A, Tchafa F
Received 28 January 2026
Accepted for publication 18 April 2026
Published 20 May 2026 Volume 2026:18 599551
DOI https://doi.org/10.2147/OAJCT.S599551
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Henriette U Balinda, Alima Tchafa, Franck Tchafa
Publication Department, Feat Healthcare, Dallas, TX, USA
Correspondence: Henriette U Balinda, Publication Department, Feat Healthcare, 539 W. Commerce St. Suite 204, Dallas, TX, 75208, USA, Email [email protected]
Abstract: Africa bears a disproportionate share of the global disease burden yet remains underrepresented in global clinical research. Fragmented regulatory systems, variable approval timelines, and limited cross-border coordination have historically constrained multinational trials across the continent. Over the past decade, however, regional medicines regulatory harmonization initiatives and the establishment of the African Medicines Agency (AMA) have begun to transform Africa’s regulatory environment. This Commentary reviews progress achieved through regional collaboration, assesses the early role of the AMA, and examines persistent structural and capacity-related barriers. We argue that regulatory harmonization represents a pivotal opportunity to reposition Africa as a central hub for global clinical research. Realizing this potential will require sustained political commitment, investment in regulatory capacity and digital infrastructure, and deeper engagement by global sponsors and funders. Nevertheless, substantial implementation gaps remain, particularly regarding uneven state adoption, sustainable financing, and post-market surveillance capacity. Strengthening Africa’s regulatory ecosystem is not only a matter of efficiency, but also an ethical and scientific imperative for producing globally relevant and equitable clinical evidence.
Keywords: African Medicines Agency, National Medicines Regulatory Authority, regulatory convergence, clinical trial harmonization, health systems strengthening, health equity
Introduction
In 2020, as the world raced to develop COVID-19 vaccines, Africa, home to 17% of the global population, hosted less than 2% of registered clinical trials.1 This stark disparity reflects a persistent paradox: while Africa bears roughly a quarter of the global disease burden, the continent remains largely excluded from the clinical research activity that shapes prevention and treatment strategies.2,3 This underrepresentation is not simply a logistical challenge, it is also a legacy of historical exploitative and unethical research practices conducted in Africa, which have fostered institutional distrust and continue to shape how regulatory reform and sponsor engagement are perceived by African governments and communities.4
The drivers of this imbalance are well documented. Fragmented regulatory systems, variable approval timelines ranging from 60 days to over a year, and limited coordination across 54 countries have created structural barriers for researchers and pharmaceutical sponsors.5,6 These challenges are compounded by Africa’s linguistic diversity, encompassing Anglophone, Francophone, Lusophone, and Arabic-speaking regulatory environments, which creates additional complexity for harmonized documentation and cross-border trial protocols.7 These challenges increase costs, delay trial initiation, and deter inclusion of African sites in multinational studies. Yet this narrative is beginning to shift, driven by regional harmonization initiatives and the establishment of the African Medicines Agency (AMA).6,8
This Commentary was prepared with the assistance of AI-based language tools. AI assistance was used for language editing and structural refinement; all analytical content, synthesis, and conclusions were developed and validated by the authors. The application of AI tools to evidence synthesis in medical writing carries both opportunities, including efficiency and accessibility, and limitations, including risks of bias propagation and reduced critical scrutiny, considerations that warrant transparency in academic reporting.9,10
Our Commentary examines Africa’s evolving regulatory landscape, evaluates progress toward harmonization, and outlines policy actions needed to position the continent as a competitive and essential hub for global clinical research. To situate Africa’s regulatory evolution, it is useful to note that other regions, including the European Union, whose European Medicines Agency facilitates centralized authorization across member states, and ASEAN, whose ACCSQ Pharmaceutical Product Working Group supports harmonized product registration, have demonstrated that regional harmonization can substantially accelerate approval timelines while maintaining regulatory rigor.11 Africa’s approach, driven by the AMA and regional bodies, is both informed by and distinct from these models, reflecting the continent’s unique institutional landscape and capacity constraints.
Progress Through Regional Harmonization
Over the past decade, several African regions have demonstrated that collaborative regulatory approaches can substantially improve efficiency (Table 1). The East African Community Medicines Regulatory Harmonization (EAC-MRH) program has reduced median review times by 53%, from 553 days to 259 days.5 The Southern African Development Community’s ZaZiBoNa initiative enables joint assessments that participating countries can finalize in about 90 days, compared with 6–12 months for individual national reviews.12
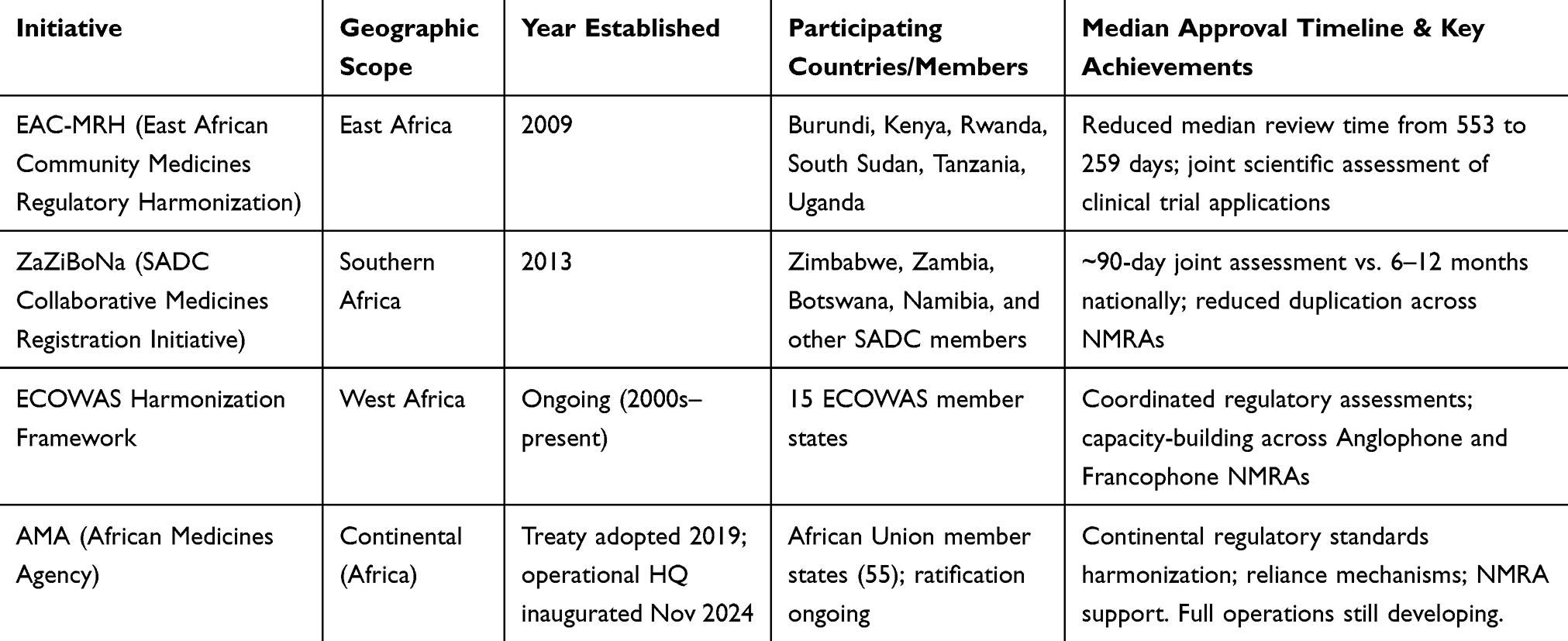 |
Table 1 Major African Regional Regulatory Harmonization Initiatives |
These initiatives operate through joint scientific assessments in which participating National Medicines Regulatory Authorities (NMRAs) review clinical trial applications collaboratively. This model reduces duplicative reviews while maintaining regulatory rigor.5,6 In West Africa, harmonization efforts under the Economic Community of West African States (ECOWAS) have similarly aimed to facilitate coordinated assessments and strengthen regulatory capacity across member states.5,6
The COVID-19 pandemic accelerated this momentum. The African Vaccine Regulatory Forum (AVAREF) coordinated parallel ethics and regulatory reviews across multiple countries to expedite clinical trial review.13 These experiences demonstrated that African regulators can move rapidly without compromising safety or scientific integrity.13
The African Medicines Agency: A Continental Vision
Building on these regional successes, the African Medicines Agency represents a transformative continental initiative. The AMA was established in 2021, and its headquarters were inaugurated in Kigali, Rwanda in November 2024.8,14 The agency’s mandate includes harmonizing regulatory standards, supporting NMRAs, and enabling reliance mechanisms that draw on assessments from trusted authorities like the US Food and Drug Administration (FDA), the European Medicines Agency (EMA), and the World Health Organization (WHO).8,15
Despite its formal establishment, the AMA remains in an early operational phase. Core elements, including technical committees, staffing, regulatory workstreams, and sustainable financing mechanisms, are still developing, and the agency has not yet initiated full-scale continent-wide assessments.8,14 Its near-term impact will depend on the speed with which member states operationalize commitments and integrate AMA processes into national regulatory pathways.8
Regulatory reliance pathways are already playing an important role in accelerating access to medicines and supporting regulatory efficiency.15 Rather than conducting fully independent reviews, many African NMRAs increasingly leverage assessments from established regulators while focusing local review on context-specific considerations such as disease epidemiology and pharmacovigilance requirements.15
Several national regulators are also setting benchmarks for performance. South Africa’s SAHPRA has documented clinical trial review processes and timelines and can move efficiently when submissions are complete.16 Rwanda has likewise built a reputation for streamlined processes, reflected in its selection to host the AMA headquarters.14
Why Africa Matters for Global Clinical Research
Beyond regulatory reform, Africa offers compelling scientific, economic, and ethical rationales for expanded participation in global clinical trials.
Scientifically, Africa’s genetic diversity is the greatest globally and offers unique value for pharmacogenomics and for understanding how genetic variation influences drug response and safety.17 The continent’s epidemiological profile, characterized by a dual burden of infectious diseases and rapidly rising non-communicable diseases, also makes African populations relevant to global therapeutic development.3
Economically, Africa’s healthcare market is projected to expand substantially by 2030, and sponsors that build regulatory expertise and research infrastructure now may benefit as markets, health systems, and regulatory frameworks mature.18
Ethically, populations that bear a disproportionate share of disease burden should be represented in the studies that shape prevention and treatment strategies. Greater inclusion promotes equity and strengthens the generalizability of clinical evidence.19 Therapies tested predominantly in high-income settings may not adequately reflect the genetic diversity, comorbidity patterns, and environmental exposures common in many African contexts.17,19 Critically, expanding trial activity must be accompanied by clear frameworks governing data ownership, intellectual property, and benefit-sharing, to ensure that African populations and institutions equitably benefit from the research conducted on the continent.
Risks and Structural Challenges
Despite its promise, the AMA and broader harmonization efforts face substantial risks. Uneven political commitment across member states may result in fragmented adoption of AMA guidance, undermining continent-wide convergence.8 Financial sustainability remains uncertain, with continued reliance on external partners for technical and operational support.8 Capacity disparities between NMRAs could also create bottlenecks, particularly in countries with limited regulatory workforce, training programs, and digital infrastructure.5,6,20
At the national level, persistent structural challenges remain. Many regulators still lack electronic submission systems, relying on paper-based processes that slow reviews and limit transparency.20 Resource constraints restrict capacity in specialized areas such as advanced biologics and complex trial designs.20 In some jurisdictions, sequential rather than parallel review by ethics committees and regulators further extends timelines.13,20
Approval time variability continues to complicate multinational trial coordination. While leading countries can complete reviews within 60–90 days, other jurisdictions may require many months or longer, increasing operational complexity and deterring sponsors from including a broader range of African sites.5,6,20
A further structural gap concerns post-approval regulatory functions. The current harmonization discourse focuses primarily on trial initiation and approval timelines; however, harmonized post-market surveillance systems have received comparatively little attention. This is a critical regulatory function where most African NMRAs face significant capacity gaps and addressing it will be essential for the long-term sustainability and credibility of expanded clinical research activity on the continent.
Digital infrastructure and technological capacity also warrant closer examination. Beyond the general need for electronic submission systems, there is growing potential for artificial intelligence and machine learning tools to support regulatory review, adverse event detection, and trial monitoring in resource-limited settings. Integrating such tools into regulatory capacity-building strategies could accelerate review timelines while reducing the human resource burden on understaffed NMRAs.
The Path Forward
Realizing Africa’s potential as a global clinical research hub will require coordinated action across stakeholders.
African research institutions must continue aligning with international standards, including ICH-GCP principles, and actively leverage regional harmonization mechanisms.5,6 Investments in institutional digital infrastructure, including professional websites, trial registries, and research databases, can improve visibility and facilitate partnerships.19 The Africa Centers for Disease Control and Prevention (Africa CDC) has emerged as a central actor in clinical research coordination and epidemic preparedness; its institutional mandate and continental reach make it a critical partner for regulatory harmonization initiatives and should be explicitly integrated into national and regional research strategies.
Pharmaceutical sponsors and contract research organizations should engage early with the AMA and regional bodies, adopt pan-African regulatory strategies, and invest in local capacity building.8,19 Engagement must be accompanied by equitable partnership models that address data ownership, intellectual property arrangements, and benefit-sharing with African institutions and governments. These investments can yield long-term returns through faster trial initiation, stronger partnerships, and improved data quality.19
Policy makers and funders should prioritize regulatory strengthening through sustained technical assistance, workforce training, and digital infrastructure support, including investment in AI-enabled regulatory tools.5–7,20 The AMA, in particular, will require predictable and durable financing to transition from a symbolic continental institution to a fully functional regulator capable of driving convergence at scale.8
Conclusion
Africa stands at a pivotal moment in its integration into global clinical research. Regional harmonization initiatives, including the EAC-MRH, ZaZiBoNa, and ECOWAS frameworks, and the establishment of the AMA have laid the foundations for meaningful participation. While progress has been substantial, the conditions for Africa’s full emergence as a global clinical research hub are not yet fully in place. Uneven state adoption, financing uncertainties, and persistent capacity gaps must be addressed concurrently with the opportunities that harmonization creates.
Every clinical trial conducted in Africa strengthens regulatory systems, builds workforce capacity, and advances health equity. Achieving this vision will require regulators to sustain harmonization momentum and expand pharmacovigilance capacity; sponsors to commit to equitable, benefit-sharing partnerships; funders to provide predictable financing for the AMA and national regulatory authorities; and policymakers to prioritize digital infrastructure and workforce development. As regulatory pathways continue to converge, those engaging now, with transparency, equity, and long-term commitment, will be positioned as leaders in one of the world’s most consequential research and healthcare markets.
Declaration of Generative AI and AI-Assisted Technologies in the Manuscript Preparation Process
During the preparation of this manuscript, the authors used an AI-assisted language tool (ChatGPT, OpenAI) to support language editing, structural refinement, and clarity of expression. All content was reviewed, edited, and validated by the authors, who take full responsibility for the accuracy, originality, and integrity of the work.
Disclosure
All authors are affiliated with Feat Healthcare, a private US‑based healthcare organization. Although Alima Tchafa is employed by Regeneron Pharmaceuticals, her association with Feat Healthcare, her authorship of this article, and all related funding and activities are fully independent of her work at Regeneron. The authors declare no direct financial relationships with pharmaceutical sponsors, contract research organizations (CROs), or entities currently operating clinical trials in Africa that would constitute a disqualifying conflict of interest. The views expressed in this commentary reflect the authors’ independent academic and professional perspectives. The authors report no other conflicts of interest in this work.
References
1. Kasprowicz VO, Chopera D, Waddilove KD. et al. African-led health research and capacity building—Is it working? BMC Public Health. 2020;20:1104. doi:10.1186/s12889-020-08875-3
2. World Health Organization. World Health Statistics 2022: Monitoring Health for the SDGs. Geneva: WHO; 2022.
3. Gouda HN, Charlson F, Sorsdahl K, et al. Burden of non-communicable diseases in sub-Saharan Africa, 1990–2017: results from the Global Burden of Disease Study 2017. Lancet Glob Health. 2019;7:e1375–5. doi:10.1016/S2214-109X(19)30374-2
4. Kass N, Ndebele P, Hyder AA. The role of corruption and unethical behaviour in precluding the placement of industry sponsored clinical trials in sub-Saharan Africa: stakeholder views. Dev World Bioethics. 2014;15(3):191–197. doi:10.1111/dewb.12059
5. Ndomondo-Sigonda M, Miot J, Naidoo S, Dodoo A, Kaale E. Medicines regulation in Africa: current state and opportunities. Pharm Med. 2017;31:383–397. doi:10.1007/s40290-017-0210-x
6. Ndomondo-Sigonda M, Miot J, Naidoo S, et al. Harmonisation of medical products regulation: a key factor for improving regulatory capacity in the African region. BMC Public Health. 2021;21:187. doi:10.1186/s12889-021-10169-1
7. Tirvassen R. The issue of languages in African continental and regional integration of higher education. In: The Issue of Languages in African Continental and Regional Integration of Higher Education Institutions. 2025.
8. Hwenda L, Ndomondo-Sigonda M, Ambali A, et al. The African Medicines Agency: the key to unlocking clinical research in Africa. Lancet. 2022;399(10340):e1088–e1089.
9. Dergaa I, Saad HB, Glenn JM, et al. From human writing to artificial intelligence generated text: examining the prospects and potential threats of ChatGPT in academic writing. Biol Sport. 2023;40(2):615–622. doi:10.5114/biolsport.2023.125623
10. Dergaa I, Saad HB, Glenn JM, et al. A thorough examination of ChatGPT-3.5 potential applications in medical writing: a preliminary study. Medicine. 2024;103(40):e39757. doi:10.1097/MD.0000000000039757
11. European Medicines Agency. Centralised Procedure at the European Medicines Agency. EMA; 2019.
12. Sithole T, Mahlangu G, Salek S, Walker S. Evaluating the success of ZaZiBoNa, the Southern African Development Community collaborative medicines registration initiative. Ther Innov Regul Sci. 2020;54:1319–1329. doi:10.1007/s43441-020-00154-y
13. World Health Organization Regional Office for Africa. African Regulatory Agencies, Ethics Committees to Expedite COVID-19 Clinical Trial Reviews. Brazzaville: WHO AFRO; 2020.
14. Xinhua. Rwanda, African Union inaugurate continental medical agency headquarters in Kigali.
15. World Health Organization. Regulatory reliance principles: general considerations and advice. WHO Technical Report Series No. 1033. Geneva: WHO; 2021.
16. South African Health Products Regulatory Authority (SAHPRA). Clinical Trial Guidelines and Standard Operating Procedures. Pretoria: SAHPRA; 2023.
17. Tishkoff SA, Reed FA, Friedlaender FR, et al. The genetic structure and history of Africans and African Americans. Science. 2009;324:1035–1044. doi:10.1126/science.1172257
18. Songwe V. Strategies for financing Africa’s health sector. Washington, DC: Brookings Institution; 2022.
19. Kok MO, Gyapong JO, Wolffers I, Ofori-Adjei D, Ruitenberg J. Towards fair and effective North–South collaboration: realising a programme for demand-driven and locally led research. Health Res Policy Syst. 2017;15:96. doi:10.1186/s12961-017-0251-3
20. Alemayehu C, Mitchell G, Nikles J. Barriers for conducting clinical trials in developing countries: a systematic review. Int J Equity Health. 2018;17:37. doi:10.1186/s12939-018-0748-6
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.