Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 14
Affective Temperament and Glycemic Control – The Psychological Aspect of Obesity and Diabetes Mellitus
Authors Lesiewska N ![]() , Kamińska A, Junik R, Michalewicz M, Myszkowski B
, Kamińska A, Junik R, Michalewicz M, Myszkowski B ![]() , Borkowska A
, Borkowska A ![]() , Bieliński M
, Bieliński M ![]()
Received 1 October 2021
Accepted for publication 9 December 2021
Published 30 December 2021 Volume 2021:14 Pages 4981—4991
DOI https://doi.org/10.2147/DMSO.S342185
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Natalia Lesiewska,1 Anna Kamińska,2 Roman Junik,2 Magdalena Michalewicz,3 Bartłomiej Myszkowski,4 Alina Borkowska,1 Maciej Bieliński1
1Chair and Department of Clinical Neuropsychology, Nicolaus Copernicus University in Toruń, Collegium Medicum in Bydgoszcz, Bydgoszcz, Poland; 2Department of Endocrinology and Diabetology, Nicolaus Copernicus University in Toruń, Collegium Medicum in Bydgoszcz, Bydgoszcz, Poland; 3Department of Pulmonology, Allergology and Pulmonological Oncology, Military Clinical Hospital No. 10 with Policlinic in Bydgoszcz, Bydgoszcz, Poland; 4Department of Obstetrics, Women’s Diseases and Oncological Gynecology, Nicolaus Copernicus University in Toruń, Collegium Medicum in Bydgoszcz, Bydgoszcz, Poland
Correspondence: Natalia Lesiewska Tel/Fax +48 52 585 37 03
Email [email protected]
Purpose: Affective temperament shows innate predisposition to affective disorders and has been studied in patients with type 2 diabetes mellitus (T2DM) and obesity. Studies describing connections between depressive disorders, obesity and T2DM, show a bidirectional way in which these disorders affect each other. Given that obesity, depression, and T2DM are still growing health problems of our times, the improvement of therapeutic strategies is required. The aim of our study was to evaluate affective temperament in obese individuals with T2DM and pre-diabetes and to investigate the correlations between affective temperaments and glycemic control.
Materials and Methods: The study enrolled 185 obese individuals (146 females; 39 males) who were diagnosed with pre-diabetes, diabetes or without any carbohydrate disorder. For affective temperament evaluation, Temperament Evaluation of Memphis, Pisa, Paris and San Diego Autoquestionnaire (TEMPS-A) was utilized; for glycemic control, the assessment of hemoglobin A1c (HbA1c) was performed.
Results: We did not observe any significant differences of affective temperament between studied groups. In the group of patients with diabetes, depressive, cyclothymic and anxious temperaments positively correlated with HbA1c values indicating worse glycemic control. Inversly, hyperthymic dimension showed negative correlation with HbA1c values.
Conclusion: Affective temperaments may affect glycemic control in obese individuals with carbohydrate disorders. Individuals with stronger expression of cyclothymic, depressive and anxious temperaments may need more medical aid for better self-management. Hence, TEMPS-A is an easy and useful tool which may significantly improve the compliance in obese patients with carbohydrate disorders.
Keywords: affective temperament, TEMPS-A, obesity, diabetes mellitus, glycemic control
Introduction
Currently, obesity is perceived as a world crisis. The prevalence of obesity increases every year, hence it creates more challenges for healthcare and economic systems. In 2013, the American Medical Association decided to perceive obesity as a chronic and complex disease to encourage physicians to tackle problems associated with obesity in different ways.1 It is believed that such aproach will diminish the stigma linked to the development of obesity.
Even though perceiving obesity as a disease still incurs many controversies, this condition is associated with severe complications. Obesity increases risk of disease of almost every system in the body, ie hypertension, dyslipidemia, cardiovascular, arthritis, breast cancer, colon cancer or endometrial cancer. In such manner obesity affects mortality and morbidity rates, worsens quality of life, and hinders daily functioning.2,3
Type 2 diabetes mellitus (T2DM) is strongly connected with obesity. Its high prevalence in obese people (and the fact that obesity is one of the most important risk factors of T2DM) has led to the term “diabesity”. T2DM is a multifactorial disease and is described as a state of hyperglycemia, hyperinsulinemia, and insulin resistance.4 T2DM contributes to greater rate of cardiovascular disease in adults which is one of the leading causes of death in diabetic patients.5 In addition, patients with prediabetes, ie, impaired glucose tolerance (IGT) or impaired fasting glucose (IFG) show increased risk of cardiovascular disease, hence greater risk of mortality due to stroke or myocardial infarction.6
Literature has shown that both obesity and T2DM exert negative effects on brain functions.7–9 Those alterations may lead to another fatal disease of our times – depression. Yet, medical databases contain abundant studies proving the link between both T2DM and obesity, and depression. Individuals with T2DM have a greater risk of developing depression compared to healthy controls.10 There are some researchers who propose a bidirectional relationship between both diseases and common pathways of their pathogenesis.11,12
Published meta-analyses yield information about the greater risk of T2DM and metabolic syndrome in patients suffering from mental diseases (bipolar disorder, major depression disorder), hence this group of patients require closer monitoring and screening tests for diabetes.10,13 Common factors which are involved in the pathogenesis of both mental diseases and metabolic syndrome (which predispose to obesity and T2DM) are: genetic links, endocrine system function, neuroinflammation and epigenetic influence.14,15 Another meta-analysis confirmed the interplay between obesity and depression; namely depression is a risk factor for obesity, and obesity is a risk factor for depression.16,17
Taken together, the interplay between T2DM, obesity, and mental diseases is evident. Therefore, patients with those conditions require a multidisciplinary approach in order to achieve better treatment results, better patient compliance or to diminish the risk of complications related to those disorders.18 For example, treatment for obesity may improve the course of depression.19 Cognitive-behavioral therapy implemented in mood disorders may contribute to better patient self-care and ameliorate treatment of diabetes.20,21
Building on the connection between the three disorders, it is crucial to develop proper screening tests evaluating predisposition of mental disorders in individuals with obesity or T2DM. In this manner, those patients who are more prone to develop mood disorders might undergo tailored preventive programs or be referred for proper treatment.
Fortunately, there are tests which may be useful in screening for mood diseases. In this study we utilized Temperament Evaluation of Memphis, Pisa, Paris and San Diego Autoquestionnaire (TEMPS-A) - this tool enables assessment of affective temperament which will be described subsequently.
The term affective temperament was proposed by Hagop Akiskal et al. Affective temperament refers to inherited personal traits and may be determined by genetic transmission or biological factors. Throughout life it is a rather stable construct, however its dysregulation can putatively predispose to greater risk of mood disorders.22–26 Affective temperament consists of five dimensions: cyclothymic, depressive, hyperthymic, anxious and irritable. So far, research results show that utilization of TEMPS-A may provide interesting data regarding the evaluation of patients’ predisposition to depression and anxiety or in determining the diagnosis of bipolar disorders.27,28
Recent literature shows that TEMPS-A as a tool has been found useful in determining affective disorders and in other conditions like insomnia or pain syndrome.29–31 The evaluation of affective temperament seems to determine which of the infertile women are more prone to the development of depression and anxiety.32 Moreover, recent research in a group of gestational diabetes patients showed promising data regarding the association between affective temperament and the development of gestational diabetes, as well as disturbances in glycemic metabolism in this group of patients.33 Hence, TEMPS-A might be of great utility in determining patients with greater susceptibility of pregnancy complications. Also in our previous work, we found associations between affective temperament dimensions and dopaminergic genes which may be involved in the development of depression in obese patients.34–36
Owing to our interesting results concerning affective temperament in obese patients, we decided to take another step in our research. The aim of this study was to scrutinize the relationship between affective temperament and the control of carbohydrate metabolism in obese patients with diabetes and pre-diabetes. Another main point of our study was to evaluate the differences between the intensity of depressive disorders in those groups of patients, and analyze whether depression is a significant factor associated with glycemic control and affective temperament.
Materials and Methods
Participants
The study enrolled 185 Caucasian people (146 females; 39 males), who were diagnosed with primary obesity. On the basis of a medical history and an oral glucose tolerance test (OGTT) patients were classified into three groups.
The first one - control group - included 87 patients without any carbohydrate disorders (65 women and 22 men), second group of 42 subjects with impaired glucose tolerance (IGT) or impaired fasting glucose (IFG) (33 women and 9 men), and third group of 56 patients (48 women and 8 men) with diabetes. The mean age of participants was 35.8±10.9 (range, 18–68 years) for no carbohydrate disorders group, 43.1±12.5 (range, 18–69 years) for IFG/IGT group, and 51.1±7.1 (range, 31–61 years) for diabetes group. Demographic characteristics are shown in Table 1. Patients were treated at the outpatient clinic at the Endocrinology and Diabetology Clinic and, with the consent of the bioethics committee, were recruited on the basis of a proposal from the attending diabetologist who carried out the therapeutic and diagnostic process. The study was conducted in accordance with the Declaration of Helsinki.
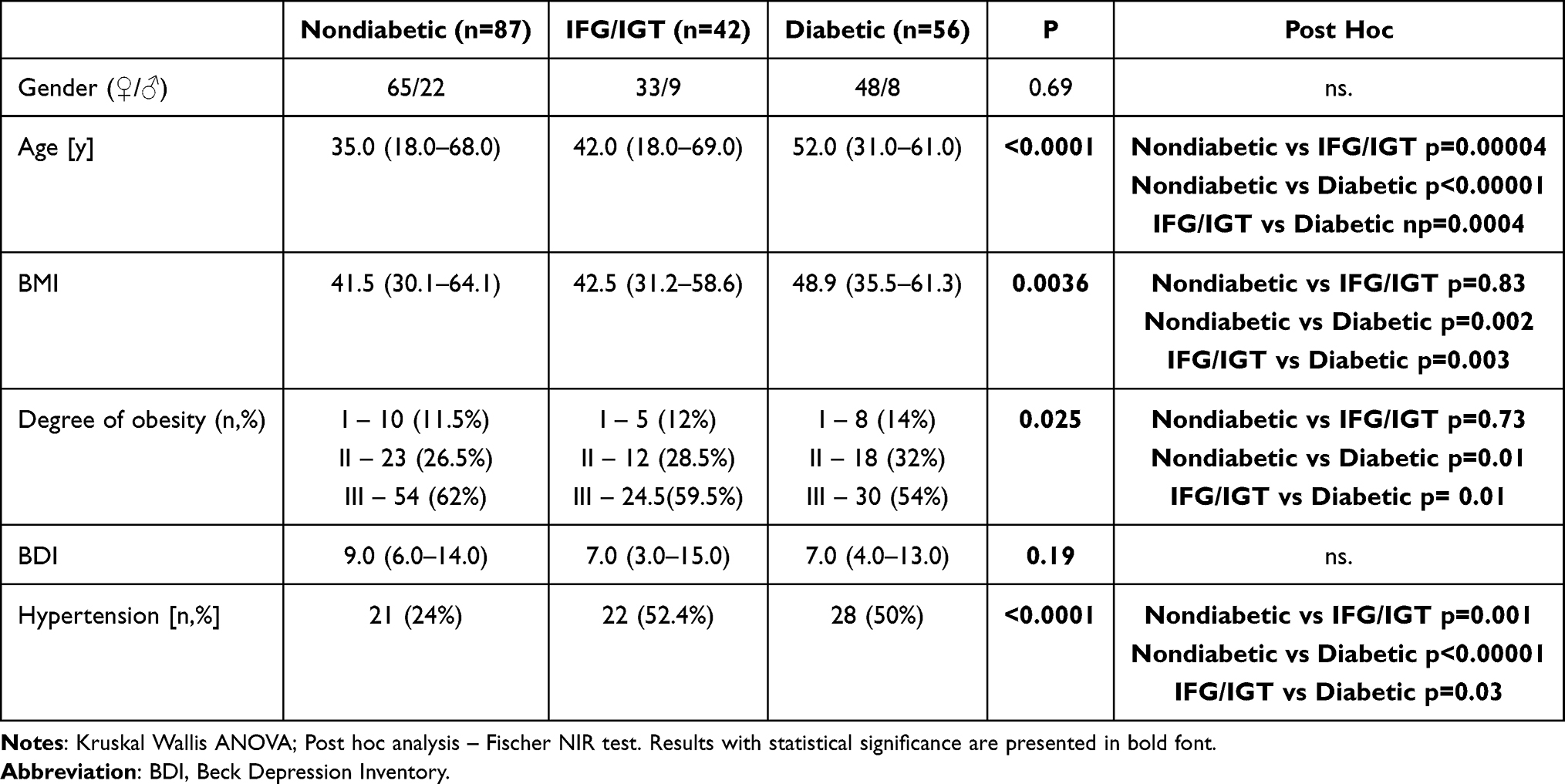 |
Table 1 Demographic and Clinical Parameters in Study Subgroups |
Participants were included in the study according to subsequent criteria: adulthood (age between 16 and 69 y.o.), consent to study participation, and primary obesity. Secondary causes of obesity were excluded due to performed medical assessment and the results of metabolic and hormonal tests. Exclusion criteria included: serious psychiatric or neurological illnesses, addictions to any illicit drugs or alcohol, or any significant somatic diseases.
We provided detailed information about the aims and the nature of the study to participants. We received written informed consent for participation from every patient. In order to conduct the study, we obtained consent of the bioethical commission at the Nicolaus Copernicus University (No 533/ 2008).
Clinical Assessments and Measures
Obesity was diagnosed according to anthropometric measures and the calculation of body mass index (BMI). BMI is a proxy for body fat concentration and is calculated as the ratio of weight (kg) to square of height (m).
Disorders associated with impaired glucose metabolism were diagnosed based on the oral glucose tolerance test performed with 75g of anhydrous glucose in solution. If the patient had a history of diabetes and received adequate treatment, he was included in the diabetic group. Glucose level was obtained at baseline, prior to glucose load, and two hours after glucose intake. Patients fasted for at least 8 hours prior to the OGTT. Depending on the result, the patients were assigned to the study subgroup:
- if the fasting glucose level was below 99 mg% (5.5 mmol/l) and the level after two hours was below 140 mg% (7.8 mmol/l), the patient had no diagnosis of carbohydrate disorders.
- If the patient had an elevated fasting glucose level above 100 mg%, and the result after two hours was normal, the patient was diagnosed with abnormal fasting glucose and was included in IFG/IGT group.
- If the patient had a glucose level after 2 hours in the range of 140 to 199 mg% (7.8–11.1 mmol/l) he was diagnosed with impaired glucose tolerance and was included in the IFG/IGT group.
- In the case of obtaining a glucose level above 200 mg% (11.1 mmol/l) in the determination after 2 hours, the patient was diagnosed with diabetes.
Metabolic status was analyzed from the blood sample and comprised C-peptide, and for glycemic control hemoglobin A1c (HbA1c).
Psychological Assessment
For psychological assessment, we utilized Temperament Evaluation of Memphis, Pisa, Paris and San Diego Autoquestionnaire (TEMPS-A) to perform an analysis of five affective temperaments.
TEMPS-A measures affective temperaments: depressive, cyclothymic, anxious, irritable and hyperthymic. TEMPS-A questionnaire consists of 110 items for females and 109 for males. Questions regarding each temperament require “yes” (score 1) or “no” (score 0) answers, and are grouped together in the following manner:
1. questions 1 to 21 (21 points) relate to depressive temperament;
2. questions 22 to 42 (21 points) relate to cyclothymic temperament;
3. questions 43 to 63 (21 points) relate to hyperthymic temperament;
4. questions 64 to 84 (21 points, 20 points in the version for men) relate to irritable temperament;
5. questions 85 to 110 (26 points) relate to anxious temperament.
Points scored for each temperament are summed up and then divided by the number of questions pertaining to each dimension. Based on that, the severity of each temperament is measured.37,38 In our study, the Polish version of TEMPS-A was utilized – TEMPS-A has been validated in a Polish population and showed satisfactory internal consistency.22,37,38
To assess the severity of depressive symptoms we used Beck Depression Inventory (BDI). The Beck Depression Inventory was developed by Aaron Beck in 1961.39 It includes the 21 (A to U) most frequently observed symptoms of depression in the following order: depressed basic mood (sadness), pessimism, feeling inadequate, loss of satisfaction, guilt, expectation of punishment, lack of self-acceptance, self-accusation, wish to die, cry for help, irritability, withdrawal from social contact, lack of decision, distorted body image, difficulties at work, sleep disturbances, fatigue, loss of appetite, weight loss, somatic complaints, low energy levels. The patient is asked to select the severity of the individual symptoms on a scale from 0 to 3. After completing the scale, all points are added up. BDI has been translated into Polish language and validated in a Polish population.40,41
Statistical Analysis
Using the Shapiro–Wilk test, it was determined that the test group did not meet the normal distribution criteria. Statistical significance of differences among 3 groups was examined by the Kruskal–Wallis analysis of variance (ANOVA). The NIR Fisher test was used for post hoc analyses. The significance of differences between the two groups was tested using the Mann Whitney U test. Correlation analysis was performed using the R-Spearman correlation test. Analysis of covariance (ANCOVA) was performed to examine interaction among anthropometric (gender, age, BMI), psychological (affective temperaments) effects on fasting glucose and HbA1c. Effect size was determined using Cohen’s d. Statistica 13.0 was used for statistical analyses.
Results
Table 1 shows demographic and clinical parameters of the studied groups. The group of patients with diabetes mellitus showed the highest BMI values. Both pre-diabetes and diabetic groups demonstrated significant percentage of comorbid hypertension. However, BDI results were insignificant in all groups.
Typical differences in biochemical parameters related to carbohydrate metabolism were observed in the studied group of patients (Table 2). The group of diabetic patients had the highest levels of not only fasting glucose and HbA1c, but also C-peptide as a marker of insulin resistance.
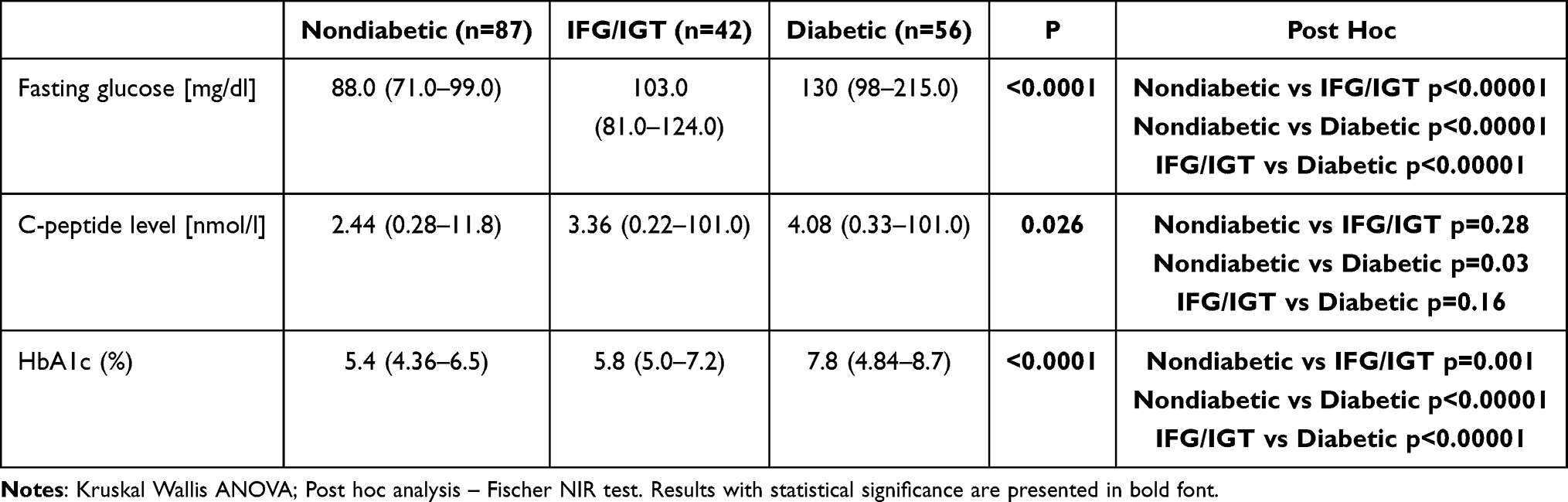 |
Table 2 Metabolic Results in Study Subgroups (Median and Range) |
Psychometric properties for TEMPS-A, BDI, and biochemicals in study group with a breakdown into women and men are included in Table 3. Men were characterized by a higher level of C-peptide, HbA1c and an irritable temperament.
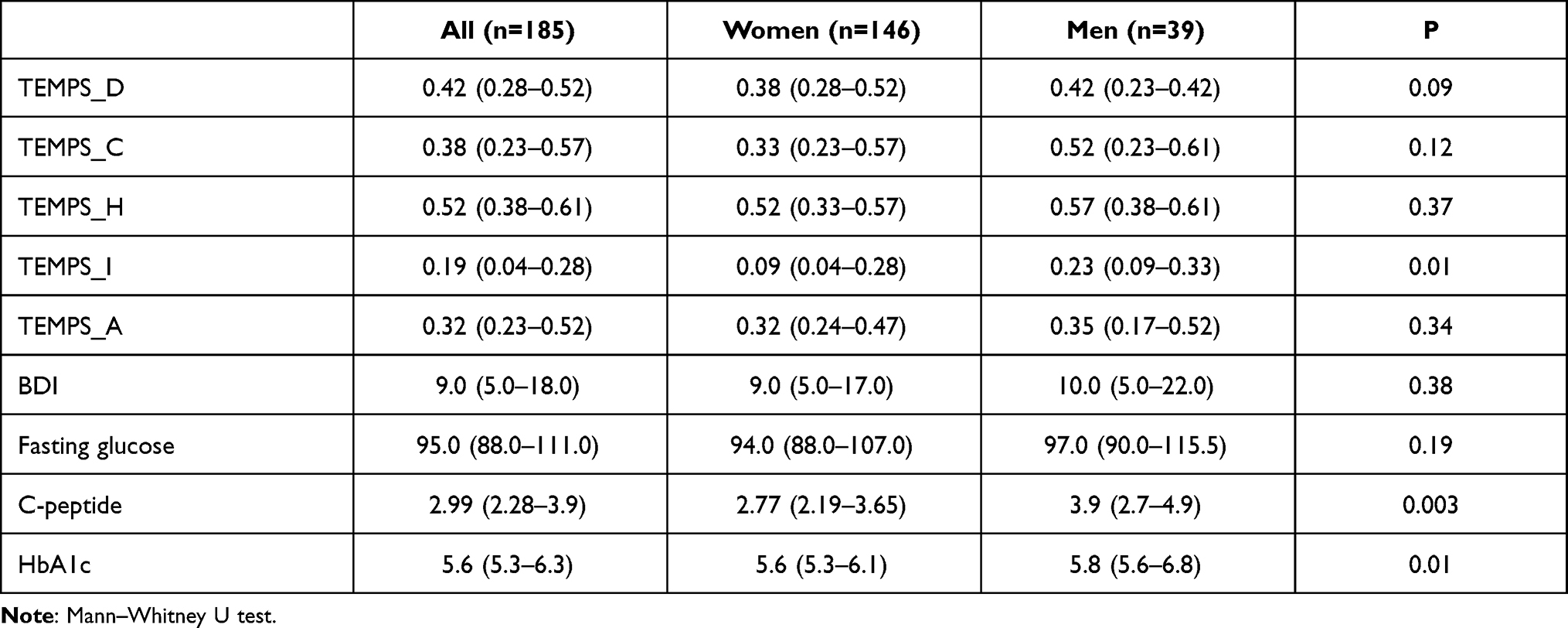 |
Table 3 Psychometric Properties for TEMPS-A and BDI in Study Group |
Further analyses concerned the comparison of the intensity of affective temperaments in the studied subgroups. They did not reveal any significant differences (Table 4).
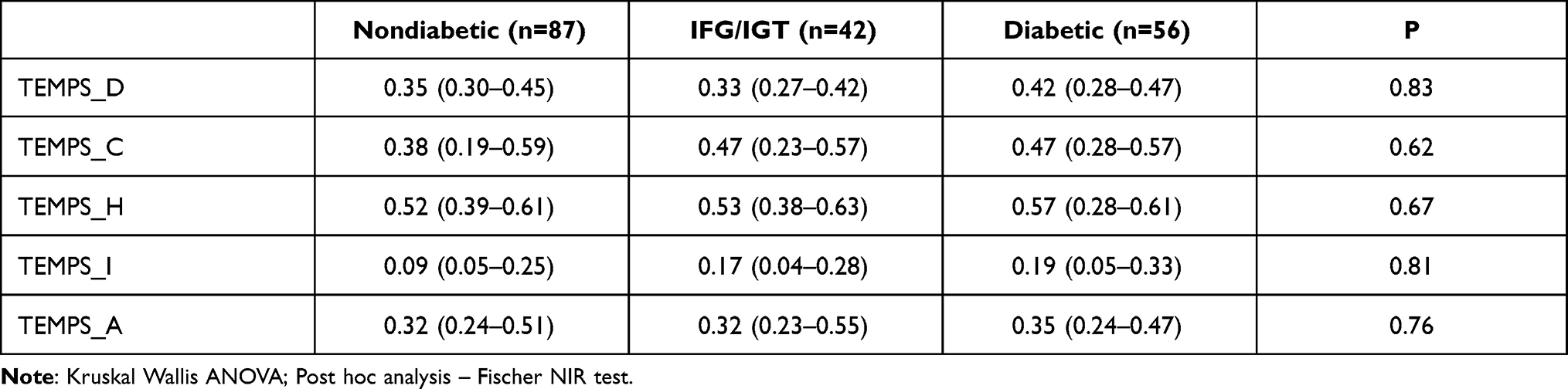 |
Table 4 TEMPS-A Affective Temperament Results in Study Subgroups (Median and Q25-Q75) |
In subgroups with carbohydrate metabolism disorders - prediabetes and diabetes - the correlations of affective temperaments with the level of fasting glucose and the level of HbA1c were analyzed. In IGT/IFG group, only hyperthymic temperament was significantly associated with higher fasting glucose levels. In the subgroup of diabetic patients, depressive, cyclothymic and anxious temperaments correlated with significantly higher glycemic levels. Inversely, hyperthymic temperament correlated with lower glycemic values. A significantly higher level of HbA1c was associated with a higher intensity of anxious temperament (Table 5).
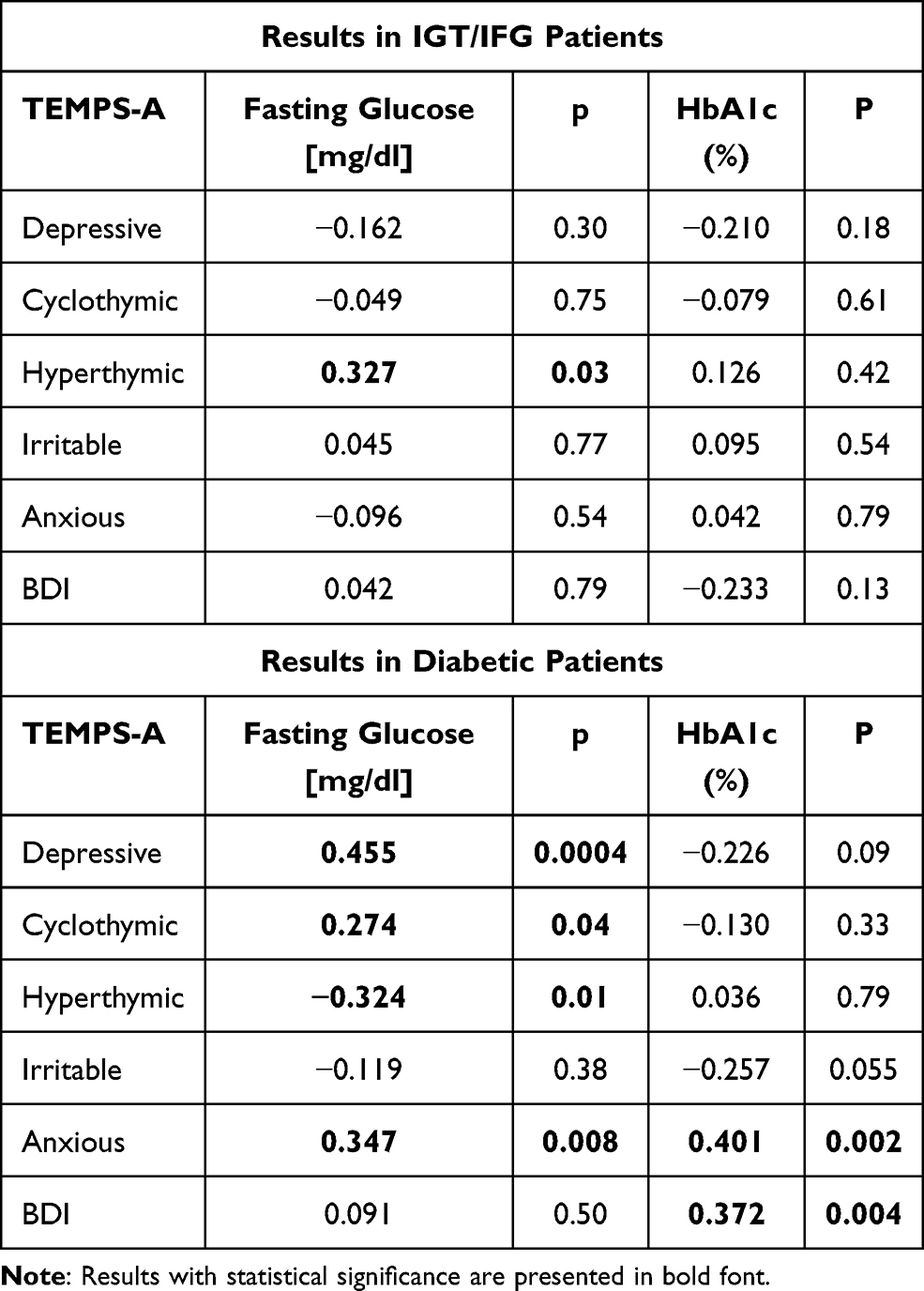 |
Table 5 R-Spearman Correlations of TEMPS-A and BDI Scores with Metabolic Parameters |
In the studied group of patients, the ANCOVA analysis of covariance confirmed the significance of the relationship between the cyclothymic temperament and fasting glucose; and anxious temperament and level of HbA1c (Table 6).
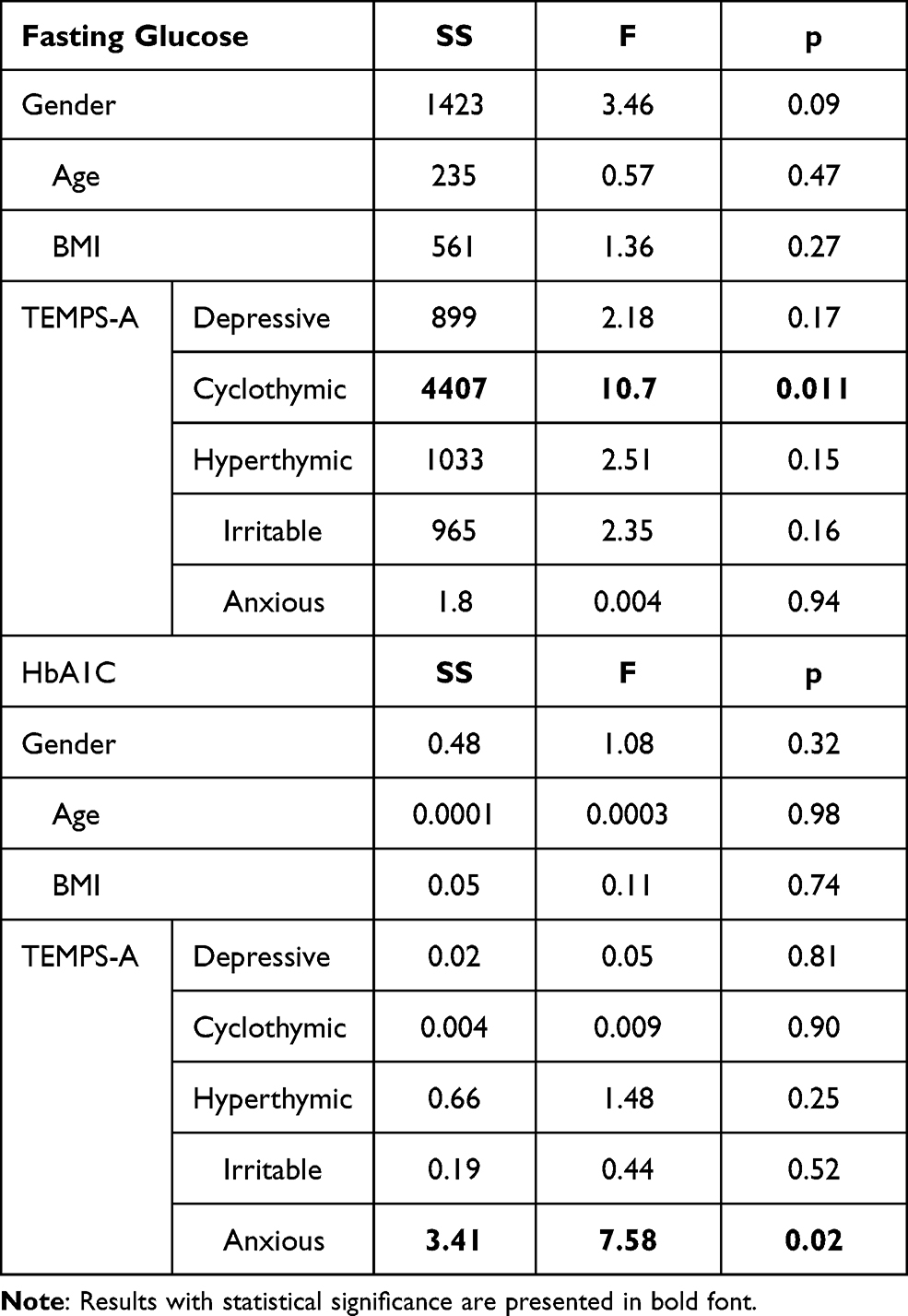 |
Table 6 ANCOVA Mulitocovariance Test in Diabetes Group |
Discussion
The aim of this study was to analyze affective temperament in context of biochemical factors in obese patients suffering from diabetes mellitus and pre-diabetes.
Results presented in Table 1 indicate that individuals with diabetes mellitus were older and showed greater intensity of obesity in comparison to the other two groups. Those results are consistent with findings of epidemiological studies and publications regarding risk factors of T2DM.42–44 Also, diabetic patients presented significant results regarding the percentage of hypertension; it is well known that both diseases often appear concomitantly.45 Comorbidity between hypertension and pre-diabetes was significant as well, which is consistent with findings in the literature.46
Obtained scores of BDI in all groups were insignificant. Depression is an important risk factor for both obesity and diabetes. Researchers also established evidence that obesity and diabetes might contribute to greater susceptibility to depression, however there are still many uncertainties regarding the exact mechanism responsible for this pathomechanism.11,12,16,17 We reckon, that the possible explanation of our results might result from this bidirectional effect between depression, obesity and diabetes and therefore none of the groups obtained significant results regarding the intensity of depressive symptoms.
Table 2 reflects metabolic results in all three groups of patients. We obtained statistically significant results regarding fasting plasma glucose (FPG) levels, as well as HbA1c values in all groups. Those results are consistent with the definition and diagnostic criteria of IFG and T2DM.47 Building on these results, the T2DM group showed the worst glycemic control due to elevated HbA1c levels and fasting plasma glucose (FPG).47–49
Previously mentioned results also point to the association between obesity and T2DM. The term “diabesity” reflects the close relationship between both obesity and diabetes. Those chronic disorders stem from disturbances involving environmental, genetic, behavioral or physiological factors. Greater calorie intake and lower physical activity, which is characteristic of obesity, may lead to hyperglycemia and insulin-resistance which favor the development of T2DM.4,50
Temperament consists of constitutional or genetic aspects of a human’s personality. Hagop Akiskal proposed that affective temperament might point to the innate predispositions to affective disorders, if one’s exposed to biological or environmental stressors.23,26
Obtained results, as shown in Table 4, showed no significant differences of affective temperament dimensions in obese prediabetic and diabetic group. These outcomes point to the environmental relations between diabesity and susceptibility to mood disorders. Genetic factors do not seem to be a common factor connecting vulnerability to affective disorders and obese individuals with T2DM. In their study, Mezuk et al showed strong evidence, that environmental factors rather than genetic ones are involved in the pathomechanisms of T2DM and depressive disorders. One of the most important is stress exposure, which may affect eating habits, leading to overeating foods rich in sugar or fat.51,52
Table 5 reflects results of correlations between both: glycemic control (measured with HbA1c) and fasting glucose values; and TEMPS-A dimensions. Obtained data point to the significant relationship between affective temperament and glycemic status in both pre-diabetic and diabetic obese patients.
Diabetes requires proper self-management and, in order to achieve treatment goals, patients need adequate education provided by health professionals.53 Data show that psychological factors are crucial in glycemic control.12,54–57 For instance, depression, anxiety or stress may influence daily life choices, the willingness to self-care and adherence to physician’s recommendations. It has been shown that psychological support may contribute to better compliance and in this manner enhance therapeutic effects of applied treatment.53
The concept that temperament is linked to weight gain has been studied using various questionnaires designed to evaluate temperament, including TEMPS-A.36,58,59 Evidence has shown that temperament is linked to the progression of metabolic syndrome and central obesity.60 The study of Altinbas et al even pointed to the relationship between seasons of the year and the greater risk of metabolic syndrome in subjects with depressive temperament.61 Metabolic syndrome is closely related to obesity and T2DM. Obtained results of obese patients with T2DM point to the positive correlations between FPG levels and temperaments – depressive, anxious and cyclothymic – and HbA1c and anxious temperament. Other researchers have also studied the relation between temperament and glycemic control in diabetic patients and shared similar results regarding the relation between HbA1c and anxious temperament. In their work, Hall et al obtained results showing negative relationship between anxious temperament and HbA1c at the beginning of the diagnosis.62 Anxious temperament was also a good predictor for pre-diabetes. Taken together, those results display beneficial role of anxious temperament in earlier detection of pre-diabetes and diabetes. Patients with high scores of anxious temperament presented greater motivation for seeking proper medical help, due to their increased concerns regarding their new diagnosis. However, in the group of patients who were already diagnosed with diabetes, anxious temperament was associated with lower physical activity even though this group of patients was already educated about managing their disease. Individuals with anxious temperament, by showing greater concerns and arousal, may hinder proper educational processes which are essential for adequate self-management of diabetes.
Another work of Gois et al obtained results linking depressive and anxious temperament to worse metabolic control expressed with HbA1c values.63 Both affective temperaments may be viewed as factors predisposing to greater distress which may link the vulnerability to depressive disorders in diabetic patients.64 The distress may act bidirectionally, ie, emotional distress related to the disease may affect self-care and medication adherence - which may impact HbA1c values; however worse compliance to physician’s recommendations and worse glycemic control may bring about greater distress and in this manner influence proper disease management.65,66 Similar findings have been obtained in a study which scrutinized the moderating model of affective temperament on the role of depression and diabetes management. Both anxious and depressive temperaments led to greater distress and severity of depressive symptoms which aggravated compliance and glycemic control.67
Our results also indicate the positive correlation between cyclothymic and only FPG values. Unfortunately we did not show significant results between cyclothymic temperament and HbA1c. In the work of Yamamoto et al, cyclothymic temperament was significantly associated with worse glycemic control in diabetic patients.68 The possible explanation is that individuals with cyclothymic temperament seem to be prone to addictive behaviors like overeating and in this manner they try to cope with distress and changes of mood.69,70 Such behavior may also be responsible for worse compliance in managing T2DM and reflect worse HbA1c values. Published results also indicate that cyclothymic temperament is linked to morbid obesity or eating disorders like binge eating.59,71,72
In our study, hyperthymic temperament was associated with higher FPG levels in pre-diabetic patients, but in diabetic ones showed negative correlation with HbA1c values. Established data indicate protective role of hyperthymic temperament in mood disorders, which may be a potential explanation of better coping with distress and better glycemic control.73 Later in their work, the same authors proposed the dual role of hyperthymic temperament. Within TEMPS-A questionnaire, hyperthymic temperament consists of both protective items like the item concerning self-confidence, as well as risk items which may point to the vulnerability traits similar to irritable temperament – “the irritable components of hyperthymic temperament”.74 Given that irritable temperament has been associated with poor glycemic control in diabetic patients, this may be a possible explanation of ambiguous results of hyperthymic temperament in our study.75
To sum up, our results indicate that the evaluation of affective temperament may be useful in the assessment of the course of pre-diabetes and T2DM in obese individuals. Moreover, patients with anxious, depressive and cyclothymic temperament might need even more attention from various specialists (dietitians, psychologists, diabetologists) to adjust proper management of their disease. More research on this issue would provide more interesting and helpful data.
Limitations
The main limitation of this study is the relatively small sample of research groups. Moreover the study lacked a control group of healthy, lean persons.
Conclusion
To our knowledge this is the first study assessing affective temperament glycemic control in obese persons with pre-diabetes and T2DM. Obtained results indicate that cyclothymic, anxious and depressive temperament correlate with worse glycemic control in T2DM, however hyperthymic dimension seems to have a protective effect on glycemia. The evaluation of affective temperament may be useful in order to create more tailored educational programs for obese patients with carbohydrate disorders.
Abbreviations
T2DM, type 2 diabetes mellitus; TEMPS-A, Temperament Evaluation of Memphis, Pisa, Paris and San Diego Autoquestionnaire; TEMPS-A, anxious temperament; TEMPS-D, depressive temperament; TEMPS-I, irritable temperament; TEMPS-C, cyclothymic temperament; TEMPS-H, hyperthymic temperament; HbA1c, hemoglobin A1c; IGT, impaired glucose tolerance; IFG, impaired fasting glucose; FGP, fasting glucose plasma; BDI, Beck Depression Inventory.
Acknowledgments
This research was not supported by any external foundation.
Disclosure
The authors declare no conflicts of interest in association with this manuscript.
References
1. Pollack A AMA recognizes obesity as a disease. NYTimescom; 2013. Available from: http://nyti.ms/1Guko03.
2. McDonald ME, Bender DP. Endometrial cancer: obesity, genetics, and targeted agents. Obstet Gynecol Clin North Am. 2009;46(1):89–105. doi:10.1016/j.ogc.2018.09.006
3. Wills JCK. The evolution of human adiposity and obesity: where did it all go wrong? Dis Models Mech. 2012;5:595–607. doi:10.1242/dmm.009613
4. Zimmet P, Alberti KG, Shaw J. Global and societal implications of the diabetes epidemic. Nature. 2001;414(6865):782–787. doi:10.1038/414782a
5. Sarwar N, Gao P, Seshasai SR, et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet. 2010;375(9733):2215–2222. doi:10.1016/S0140-6736(10)60484-9
6. Huang Y, Cai X, Mai W, et al. Association between prediabetes and risk of cardiovascular disease and all cause mortality: systematic review and meta-analysis. BMJ. 2016;355:i5953. doi:10.1136/bmj.i5953
7. Zilliox LA, Chadrasekaran K, Kwan JY, et al. Diabetes and Cognitive Impairment. Curr Diab Rep. 2016;16(9):87. doi:10.1007/s11892-016-0775-x
8. Bischof GN, Park DC. Obesity and aging: consequences for cognition, brain structure, and brain function. Psychosom Med. 2015;77(6):697–709. doi:10.1097/PSY.0000000000000212
9. Bieliński M, Lesiewska N, Junik R, et al. Dopaminergic Genes polymorphisms and prefrontal cortex efficiency among obese people - whether gender is a differentiating factor? Curr Mol Med. 2019;19(6):405–418. doi:10.2174/1566524019666190424143653
10. Nouwen A, Winkley K, Twisk J, et al. European Depression in Diabetes (EDID) Research Consortium. Type 2 diabetes mellitus as a risk factor for the onset of depression: a systematic review and meta-analysis. Diabetologia. 2010;53(12):2480–2486. doi:10.1007/s00125-010-1874-x
11. Mansur RB, Brietzke E, McIntyre RS. Review: is there a “metabolic- mood syndrome”? A review of the relationship between obesity and mood disorders. Neurosci Biobehav Rev. 2015;52:89–104. doi:10.1016/j.neubiorev.2014.12.017
12. Lustman PJ, Clouse RE. Depression in diabetic patients: the relationship between mood and glycemic control. J Diabetes Complicat. 2005;19(2):113–122.
13. Vancampfort D, Correll CU, Galling B, et al. Diabetes mellitus in people with schizophrenia, bipolar disorder and major depressive disorder: a systematic review and large scale meta-analysis. World Psychiatry. 2016;15(2):166–174. doi:10.1002/wps.20309
14. Vancampfort D, Stubbs B, Mitchell AJ, et al. Risk of metabolic syndrome and its components in people with schizophrenia and related psychotic disorders, bipolar disorder and major depressive disorder: a systematic review and meta-analysis. World Psychiatry. 2015;14(3):339–347. doi:10.1002/wps.20252
15. Ellingrod VL, Taylor SF, Dalack G, et al. Risk factors associated with metabolic syndrome in bipolar and schizophrenia subjects treated with antipsychotics: the role of folate pharmacogenetics. J Clin Psychopharmacol. 2012;32(2):261–265. doi:10.1097/JCP.0b013e3182485888
16. Luppino FS, de Wit LM, Bouvy PF, et al. Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch Gen Psychiatry. 2010;67(3):220–229. doi:10.1001/archgenpsychiatry.2010.2
17. Mannan M, Mamun A, Doi S, et al. Prospective associations between depression and obesity for adolescent males and females- a systematic review and meta-analysis of longitudinal studies. PLoS One. 2016;11(6):e0157240. doi:10.1371/journal.pone.0157240
18. Jung I, Kwon H, Park SE, et al. Increased risk of cardiovascular disease and mortality in patients with diabetes and coexisting depression: a nationwide population-based cohort study. Diabetes Metab J. 2021;45(3):379–389. doi:10.4093/dmj.2020.0008
19. Linde JA, Simon GE, Ludman EJ, et al. A randomized controlled trial of behavioral weight loss treatment versus combined weight loss/depression treatment among women with comorbid obesity and depression. Ann Behav Med. 2011;41(1):119–130. doi:10.1007/s12160-010-9232-2
20. Semenkovich K, Brown ME, Svrakic DM, et al. Depression in type 2 diabetes mellitus: prevalence, impact, and treatment. Drugs. 2015;75(6):577–587. doi:10.1007/s40265-015-0347-4
21. Mukherjee N, Chaturvedi SK. Depressive symptoms and disorders in type 2 diabetes mellitus. Curr Opin Psychiatry. 2019;32(5):416–421. doi:10.1097/YCO.0000000000000528
22. Akiskal HS, Akiskal KK. Special issue: TEMPS: temperament evaluation of Memphis, Pisa, Paris and San Diego. J Affect Disord. 2005;85:1–242. doi:10.1016/j.jad.2004.12.003
23. Akiskal HS, Akiskal K. Cyclothymic, hyperthymic and depressive temperaments as subaffective variants of mood disorders. In: Tasman A, Riba MB, editors. Annual Review. Vol. II. Washington, D.C.: American Psychiatry Press; 1992:43–62.
24. Von Zerssen D, Akiskal HS. Personality factors in affective disorders: historical developments and current issues with special reference to the concepts of temperament and character. J Affect Disord. 1998;51:1–5. doi:10.1016/s0165-0327(98)00151-7
25. Goodwin FK, Redfield Jamison K. Manic-Depressive Illness: Bipolar Disorders and Recurrent Depression.
26. Akiskal HS, Akiskal KK, Haykal RF, et al. TEMPS-A: progress towards validation of a self-rated clinical version of the temperament evaluation of the Memphis, Pisa, Paris, and San Diego Autoquestionnaire. J Affect Disord. 2005;85:3–16. doi:10.1016/j.jad.2004.12.001
27. Mendlowicz MV, Jean-Louis G, Kelsoe JR, et al. A comparison of recovered bipolar patients, healthy relatives of bipolar probands, and normal controls using the short TEMPS-A. J Affect Disord. 2005;85(1–2):147–151. doi:10.1016/j.jad.2004.01.012
28. Shahini M, Shala M, Xhylani P, et al. Challenging predictions between affective temperaments, depression and anxiety in a Kosovo student community sample. Int J Psychiatry Clin Pract. 2018;22(4):282–288. doi:10.1080/13651501.2018.1426771
29. Morishita C, Kameyama R, Toda H, et al. Utility of TEMPS-A in differentiation between major depressive disorder, bipolar I disorder, and bipolar II disorder. PLoS One. 2020;15(5):e0232459. doi:10.1371/journal.pone.0232459
30. Oniszczenko W, Rzeszutek M, Stanisławiak E. Affective Temperaments, Mood, and Insomnia Symptoms in a Nonclinical Sample. Behav Sleep Med. 2019;17(3):355–363. doi:10.1080/15402002.2017.1357121
31. Badil Güloğlu S, Tunç S. The assessment of affective temperament and life quality in myofascial pain syndrome patients. Int J Psychiatry Clin Pract. 2020;21:1–6. doi:10.1080/13651501.2020.1833039
32. Işik Ulusoy S, Colak E. Effects of temperamental characteristics on depression-anxiety levels and the quality of life in infertile women. Medeni Med J. 2020;35(3):226–235. doi:10.5222/MMJ.2020.96646
33. Rezaei Ardani A, Tara F, Hatami SB, Naghizadeh Kashani S, Emadzadeh M, Nahidi M. Affective temperaments and the risk of gestational diabetes mellitus. Int J Psychiatry Clin Pract. 2021;22:1–6. doi:10.1080/13651501.2021.1872648
34. Perugi G, Toni C, Maremmani I, et al. The influence of affective temperaments and psychopathological traits on the definition of bipolar disorder subtypes: a study on bipolar I Italian national sample. J Affect Disord. 2012;136(1–2):e41–e49. doi:10.1016/j.jad.2009.12.027
35. Morishita C, Kameyama R, Toda H, et al. Utility of TEMPS-A in differentiation between major depressive disorder, bipolar I disorder, and bipolar II disorder. PLoS One. 2020;15(5):e0232459.
36. Lesiewska N, Borkowska A, Junik R, et al. The association between affective temperament traits and dopamine genes in obese population. Int J Mol Sci. 2019;20(8):1847. doi:10.3390/ijms20081847
37. Dembińska-Krajewski D, Rybakowski J. The Temperament Evaluation of Memphis, Pisa, and San Diego Auto-questionnaire (TEMPS-A) an important tool to study affective temperament. J Psychiatr Pol. 2014;48:261–276.
38. Borkowska A, Rybakowski JK, Dróżdż W, et al. Polish validation of the TEMPS-A: the profile of affective temperaments in a college student population. J Affect Disord. 2010;123:36–41. doi:10.1016/j.jad.2009.09.024
39. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561–571. doi:10.1001/archpsyc.1961.01710120031004
40. Wiglusz MS, Landowski J, Michalak L, Cubała WJ. Validation of the Polish version of the Beck Depression Inventory in patients with epilepsy. Epilepsy Behav. 2017;77:58–61. doi:10.1016/j.yebeh.2017.09.023
41. Parnowski T, Jernajczyk W. Beck’s depression inventory in the rating of mood in normal subjects and in patients with affective disturbances. Psychiatr Pol. 1977;11:417–425.
42. Zheng Y, Ley S, Hu F. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat Rev Endocrinol. 2018;14:88–98. doi:10.1038/nrendo.2017.151
43. World Health Organisation (WHO). Global Reports on Diabetes. Working Papers. 2016. id:10553, eSocialSciences.
44. Fletcher B, Gulanick M, Lamendola C. Risk factors for type 2 diabetes mellitus. J Cardiovasc Nurs. 2002;16(2):17–23. doi:10.1097/00005082-200201000-00003
45. Strain WD, Paldánius PM. Diabetes, cardiovascular disease and the microcirculation. Cardiovasc Diabetol. 2018;17(1):57. doi:10.1186/s12933-018-0703-2
46. Kleinherenbrink W, Osei E, den Hertog HM, et al. Prediabetes and macrovascular disease: review of the association, influence on outcome and effect of treatment. Eur J Intern Med. 2018;55:6–11. doi:10.1016/j.ejim.2018.07.001
47. Association American Diabetes. Updates to the standards of medical care in diabetes-2018. Diabetes Care. 2018;41(9):2045–2047. doi:10.2337/dc18-su09
48. Roohk H, Zaidi A. A review of glycated albumin as an intermediate glycation index for controlling diabetes. J Diabetes Sci Technol. 2008;2:1114–1121. doi:10.1177/193229680800200620
49. Guerin-Dubourg A, Catan A, Bourdon E, et al. Structural modifications of human albumin in diabetes. Diabetes Metab. 2012;38:171–178. doi:10.1016/j.diabet.2011.11.002
50. Astrup A, Finer N. Redefining type 2 diabetes: ‘diabesity’ or ‘obesity dependent diabetes mellitus’? Obes Rev. 2000;1(2):57–59. doi:10.1046/j.1467-789x.2000.00013.x
51. Mezuk B, Heh V, Prom-Wormley E, et al. Association between major depression and type 2 diabetes in midlife: findings from the Screening Across the Lifespan Twin Study. Psychosom Med. 2015;77(5):559–566. doi:10.1097/PSY.0000000000000182
52. Nicolucci A, Kovas Burns K, Holt RI, et al. Diabetes attitudes, wishes and needs second study (DAWN2): cross-national benchmarking of diabetes-related psychosocial outcomes for people with diabetes. Diabetic Med. 2013;30(7):767–777. doi:10.1111/dme.12245
53. Anderson RM. Is the problem of compliance all in our heads? Diabetes Educ. 1985;11(1):31–34. doi:10.1177/014572178501100106
54. Lustman PJ, Frank BL, McGill JB. Relationship of personality characteristics to glucose regulation in adults with diabetes. Psychosom Med. 1991;53:305–312. doi:10.1097/00006842-199105000-00004
55. Toobert DJ, Glasgow RE. Problem solving and diabetes self-care. J Behav Med. 1991;14:71–86. doi:10.1007/BF00844769
56. van Dooren FE, Denollet J, Verhey FR, et al. Psychological and personality factors in type 2 diabetes mellitus, presenting the rationale and exploratory results from The Maastricht Study, a population-based cohort study. BMC Psychiatry. 2016;16:17. doi:10.1186/s12888-016-0722-z
57. McKellar JD, Humphreys K, Piette JD. Depression increases diabetes symptoms by complicating patients’ self-care adherence. Diabetes Educ. 2004;30:485–492. doi:10.1177/014572170403000320
58. Carey WB. Temperament and increased weight gain in infants. J Dev Behav Pediatr. 1985;6:128–131. doi:10.1097/00004703-198506000-00006
59. Amann B, Mergl R, Torrent C, et al. Abnormal temperament in patients with morbid obesity seeking surgical treatment. J Affect Disord. 2009;118:155–160. doi:10.1016/j.jad.2009.01.020
60. Sovio U, King V, Miettunen J, et al. Cloninger’s temperament dimensions, socio-economic and lifestyle factors and metabolic syndrome markers at age 31 years in Northern Finland Birth Cohort 1966. J Health Psychol. 2007;12:371–382. doi:10.1177/1359105307074301
61. Altinbas K, Guloksuz S, Oral ET. Metabolic syndrome prevalence in different affective temperament profiles in bipolar-I disorder. Braz J Psychiatry. 2013;35(2):131–135. doi:10.1590/1516-4446-2011-0746
62. Hall PA, Rodin GM, Vallis TM, et al. The consequences of anxious temperament for disease detection, self-management behavior, and quality of life in Type 2 diabetes mellitus. J Psychosom Res. 2009;67(4):297–305. doi:10.1016/j.jpsychores.2009.05.015
63. Gois C, Barbosa A, Ferro A, et al. The role of affective temperaments in metabolic control in patients with type 2 diabetes. J Affect Disord. 2011;134(1–3):52–58. doi:10.1016/j.jad.2011.05.021
64. Collins MM, Corcorant P, Perry IJ. Anxiety and depression symptoms in patients with diabetes. Diabet Med. 2009;26:153–161. doi:10.1111/j.1464-5491.2008.02648.x
65. Gonzalez JS, Peyrot M, McCarl LA, et al. Depression and diabetes treatment nonadherence: a meta-analysis. Diabetes Care. 2008;31:2398–2403. doi:10.2337/dc08-1341
66. Fisher L, Mullan JT, Arean P, et al. Diabetes distress but not clinical depression or depressive symptoms is associated with glycemic control in both cross-sectional and longitudinal analyses. Diabetes Care. 2010;33(1):23–28. doi:10.2337/dc09-1238
67. Belvederi Murri M, Mamberto S, Briatore L, et al. The interplay between diabetes, depression and affective temperaments: a structural equation model. J Affect Disord. 2017;219:64–71. doi:10.1016/j.jad.2017.05.018
68. Yamamoto T, Sakurai K, Watanabe M, et al. Cyclothymic temperament is associated with poor medication adherence and disordered eating in type 2 diabetes patients: a case-control study. Diabetes Ther. 2021;12(9):2611–2624. doi:10.1007/s13300-021-01121-y
69. Maremmani I, Perugi G, Pacini M, et al. Toward a unitary perspective on the bipolar spectrum and substance abuse: opiate addiction as a paradigm. J Affect Disord. 2006;93:1–12. doi:10.1016/j.jad.2006.02.022
70. Cooper Z, Fairburn CG. The evolution of “enhanced” cognitive behavior therapy for eating disorders: learning from treatment nonresponse. Cogn Behav Pract. 2011;18:394–402. doi:10.1016/j.cbpra.2010.07.007
71. Ramacciotti CE, Paoli RA, Ciapparelli A, et al. Affective temperament in the eating disorders. Weight Disord. 2004;9(2):114–119. doi:10.1007/BF03325054
72. D’Ambrosio V, Albert U, Bogetto F, et al. Obsessive-compulsive disorder and cyclothymic temperament: an exploration of clinical features. J Affect Disord. 2010;127(1–3):295–299. doi:10.1016/j.jad.2010.06.007
73. Karam EG, Salamoun MM, Yeretzian JS, et al. The role of anxious and hyperthymic temperaments in mental disorders: a national epidemiologic study. World Psychiatry. 2010;9(2):103–110. doi:10.1002/j.2051-5545.2010.tb00287.x
74. Karam EG, Itani L, Fayyad J, et al. Temperament and suicide: a national study. J Affect Disord. 2015;184:123–128. doi:10.1016/j.jad.2015.05.047
75. Shamsi A, Khodaifar F, Arzaghi SM, et al. Is there any relationship between medication compliance and affective temperaments in patients with type 2 diabetes? J Diabetes Metab Disord. 2014;13(1):96. doi:10.1186/s40200-014-0096-z
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.