Back to Journals » Infection and Drug Resistance » Volume 19
Aerobic Microbiological Profile and Antimicrobial Resistance Trends in Sterile Body Fluid Infections Over Nine Years: A Retrospective Analysis from a Tertiary-Care Center
Authors Alharbi NA ![]() , Alshafie HA, Haddad M, Muhajir AA, Alqahtani AJ, Shabi Y, Altalhi MO
, Alshafie HA, Haddad M, Muhajir AA, Alqahtani AJ, Shabi Y, Altalhi MO ![]() , Bahkali MH
, Bahkali MH ![]() , Alsaeed TS, Alshehri AA, Alqahtani MA, Elgujja A
, Alsaeed TS, Alshehri AA, Alqahtani MA, Elgujja A ![]() , Alshahrani FS
, Alshahrani FS ![]()
Received 31 December 2025
Accepted for publication 6 May 2026
Published 18 May 2026 Volume 2026:19 590059
DOI https://doi.org/10.2147/IDR.S590059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Alberto Ospina Stella
Nada Abdullah Alharbi,1 Hanan Ali Alshafie,2 Moayad Haddad,3 Abdulrahman Abdullah Muhajir,4 Abdulah J Alqahtani,5 Yahya Shabi,5 Mansour O Altalhi,6 Mohammed H Bahkali,7 Thamir Saad Alsaeed,8 Abdullah A Alshehri,9 Mohammed A Alqahtani,10 Abba Elgujja,11 Fatimah Saad Alshahrani11,12
1Department of Basic Medical Sciences, College of Medicine, Princess Nourah bint Abdulrahman University, Riyadh, 11671, Saudi Arabia; 2Department of Medical Microbiology Laboratory, Prince Mohammed bin Nasser Hospital, Jazan Health Cluster, Jazan, Saudi Arabia; 3Microbiology laboratory, King Fahad Central Hospital, Jazan, Saudi Arabia; 4Medical Microbiology Unit, Jazan Regional Laboratory, Jazan, Saudi Arabia; 5Department of Microbiology and Clinical Parasitology, College of Medicine, King Khalid University, Abha, Saudi Arabia; 6Department of Basic Medical Science, College of Medicine, Majmaah University, Majmaah, 11952, Saudi Arabia; 7Clinical Microbiology Department, Pathology and Clinical Laboratory Medicine Administration, King Fahad Medical City, Riyadh, 11525, Saudi Arabia; 8Department of Biology and Immunology, College of Medicine, Qassim University, Qassim, Saudi Arabia; 9Microbiology laboratory, Prince Mohammed bin Abdulaziz Hospital, Riyadh, Saudi Arabia; 10Microbiology Section, Pathology and Medical Laboratories Department and Blood Banks, Security Forces Hospital, Riyadh, Kingdom of Saudi Arabia; 11Infection Prevention and Control Department, King Saud University Medical City, Riyadh, Saudi Arabia; 12Infectious Diseases Division, Internal Medicine Department, College of Medicine, King Saud University, Riyadh, Saudi Arabia
Correspondence: Abba Elgujja, Email [email protected]
Background: Sterile body fluid infections represent life-threatening conditions requiring prompt, targeted therapy, yet long-term regional surveillance data on pathogen distribution and antimicrobial resistance (AMR) in these infections remain scarce. This study assessed nine-year trends in aerobic microbiological patterns and AMR in sterile body fluid isolates in a tertiary care hospital.
Methods: We conducted a retrospective observational study of all peritoneal, pleural, and pericardial fluid samples processed between 2016 and 2024. Only the first unique isolate per patient was included. Organisms were identified and antimicrobial susceptibility testing performed according to CLSI standards using automated and manual methods. Demographic and microbiological characteristics were summarized descriptively, while group comparisons used Chi-square, Fisher’s exact test, ANOVA, or t-tests. Logistic regression evaluated year-on-year changes in non-susceptibility. Intermediate categories were included within non-susceptible interpretations. Institutional ethical approval was obtained.
Results: A total of 764 unique isolates were analyzed, predominantly from peritoneal (84%) and pleural (16%) fluids. Gram-negative organisms accounted for 74.8% of isolates, with Escherichia coli, Klebsiella pneumoniae subspecies, and Pseudomonas aeruginosa being most frequent. ESBL-producing Enterobacterales constituted 24.1% of isolates, while 5.5% were CRE. MRSA represented 23.5% of Staphylococcus isolates. Non-fermenters demonstrated substantially higher resistance to carbapenems and aminoglycosides. Logistic regression showed significant annual declines in non-susceptibility to gentamicin, cefepime, ceftazidime, and meropenem (p < 0.05), while colistin exhibited a non-significant upward trend. Yeast isolates remained highly susceptible to azoles and echinocandins. Because anaerobic culture was performed selectively, findings primarily reflect aerobic and facultative organisms rather than the full pathogen spectrum.
Conclusion: In this aerobic dataset, Gram-negative pathogens predominate in sterile body fluid infections, with notable ESBL burden and emerging CRE. Despite encouraging improvements in susceptibility to several agents, AMR remains dynamic and clinically consequential. Findings highlight the need for ongoing surveillance, strengthened antimicrobial stewardship, and integration of molecular resistance testing to optimize empiric therapy. Although limited by its single-center retrospective design, these findings provide long-term aerobic surveillance data but must be interpreted within the context of limited anaerobic culture.
Keywords: sterile body fluid infections, antimicrobial resistance, AMR, gram-negative bacteria, extended-spectrum β-lactamase, ESBL, carbapenem-resistant Enterobacterales, CRE, methicillin-resistant Staphylococcus aureus, MRSA, antimicrobial susceptibility testing, infection epidemiology
Introduction
Sterile body fluid infections, including peritonitis, pleural empyema, and pericardial infections, are medical emergencies associated with high morbidity and mortality.1–3 Accurate pathogen identification is essential for source control and appropriate antimicrobial therapy.1–4 Mortality rates for secondary peritonitis may exceed 30% in some cohorts, and empyema carries a reported mortality of 10–20%, particularly when source control or effective antimicrobial therapy is delayed.1–3
The epidemiology of sterile fluid infections differs substantially between community-acquired and hospital-acquired syndromes. Community-acquired empyema and SBP often involve Streptococcus spp. and Enterobacterales, whereas hospital-acquired infections more frequently involve Enterococcus, Pseudomonas, and other multidrug-resistant organisms.1–4 This distinction is clinically important but could not be consistently determined from laboratory records.
Because peritoneal, pleural, and pericardial spaces are physiologically sterile, any microbial growth is clinically meaningful and requires rapid diagnostic evaluation and targeted treatment. These infections arise from diverse etiologies—such as gastrointestinal perforation, complicated pneumonia, hematogenous spread, postoperative complications, or invasive procedures—and frequently affect critically ill patients who are at increased risk for antimicrobial resistance (AMR).4,5
The microbial landscape of sterile body fluid infections is dominated globally by Gram-negative organisms.1–4 Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa are consistently among the most commonly identified pathogens in intra-abdominal and pleural infections.5,6 Their clinical significance is amplified by the increasing prevalence of extended-spectrum β-lactamase (ESBL)-producing Enterobacterales and carbapenem-resistant Enterobacterales (CRE), both of which are associated with delays in effective therapy, increased need for advanced antimicrobials, longer hospital stays, and higher mortality.7–10
Gram-positive organisms—including methicillin-resistant Staphylococcus aureus (MRSA), Enterococcus faecium, coagulase-negative staphylococci (CoNS), and Enterococcus faecalis—also contribute substantially to sterile site infections, particularly in healthcare-associated settings, where multidrug resistance is increasingly common.11,12 CoNS represent both contamination and true infection in vulnerable populations.12
Fungal pathogens, especially Candida species, are emerging as important causes of sterile body fluid infections in immunocompromised and critically ill patients. Recent global surveillance data show rising resistance to azoles and echinocandins, particularly among Candida glabrata, complicating empiric and definitive antifungal therapy.13,14 Although anaerobes—such as Bacteroides fragilis—play a recognized role in secondary peritonitis, most hospital microbiology laboratories primarily report aerobic and facultative anaerobic organisms in routine culture workflows; thus, long-term sterile body fluid datasets often disproportionately reflect aerobes and clinically significant yeasts.15
Despite the global escalation of AMR, there is a notable scarcity of long-term surveillance data focused specifically on sterile body fluid infections, especially in the Middle East. Existing studies in Saudi Arabia and the Gulf Cooperation Council (GCC) region have documented increasing ESBL and carbapenem resistance in bloodstream and urinary isolates, but sterile body fluid–specific epidemiological data remain extremely limited.16–18 Given the distinct pathogen distribution, severe clinical implications, and therapeutic urgency associated with these infections, institution-specific surveillance is essential to guide empiric therapy, support antimicrobial stewardship programs, and detect emerging resistance threats.
The microbiology of sterile body fluid infections differs markedly between community-acquired and hospital-acquired syndromes, with the former often dominated by Streptococcus species and Entero-bacterales, and the latter more commonly involving Enterococcus, Staphylococcus aureus, Pseudomonas, and other multidrug-resistant organisms. This epidemiological distinction is central to interpreting resistance patterns but could not be fully delineated in our dataset.
Regional studies consistently report high ESBL prevalence and increasing carbapenem resistance among major pathogens in Saudi Arabia and the GCC.7–10 Despite regional AMR concerns, long-term sterile body fluid surveillance remains scarce. This study addresses this gap using nine-year microbiological and AMR data from a Saudi tertiary-care center. The objectives were to (1) characterize the distribution of bacterial and fungal pathogens; (2) assess the prevalence of key resistance phenotypes such as ESBL, CRE, and MRSA; and (3) evaluate temporal trends in antimicrobial non-susceptibility. These findings aim to strengthen evidence-based clinical decision-making and contribute to regional AMR surveillance efforts.
This study is designed as a longitudinal microbiological surveillance analysis aimed at characterizing pathogen distribution and antimicrobial resistance trends in aerobic isolates from sterile body fluids, rather than identifying causal determinants of resistance.
Methods
Study Design and Setting
This retrospective observational study was conducted at a tertiary-care academic medical center in Riyadh, Saudi Arabia (2016–2024), which serves a large adult and pediatric population and provides advanced surgical, critical care, and interventional services. The microbiology laboratory is accredited and participates in internal and external quality assurance programs. All sterile body fluid samples processed between January 1, 2016, and December 31, 2024, were eligible for inclusion. The study adhered to STROBE guidelines for reporting observational studies.1 The demographic and clinical characteristics of patients across organism categories are summarized in Table 1. Demographic characteristics according to inpatient and outpatient settings are presented in Table 2.
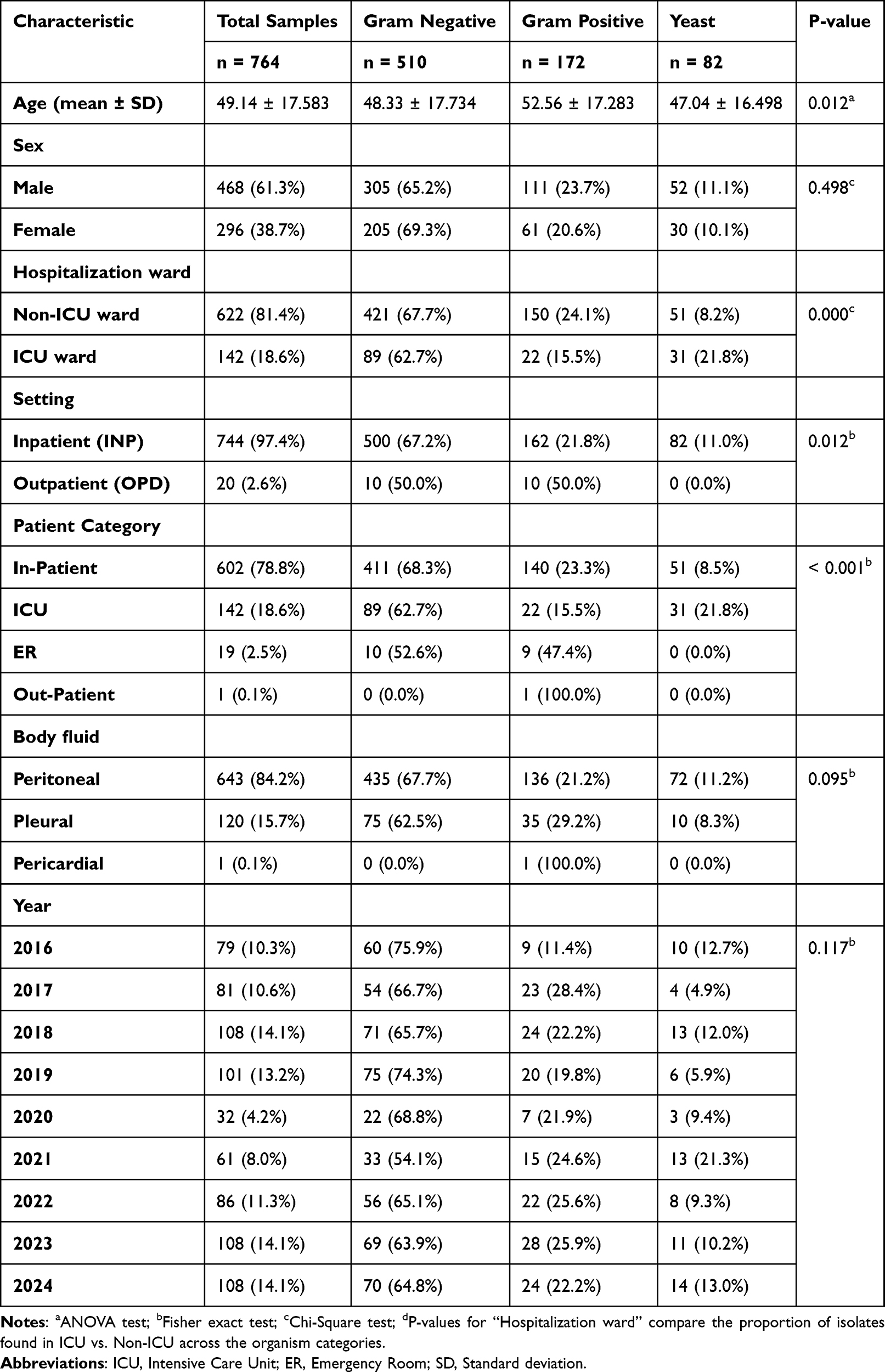 |
Table 1 Distribution of Demographic and Clinical Characteristics According to Isolated Organism Categories |
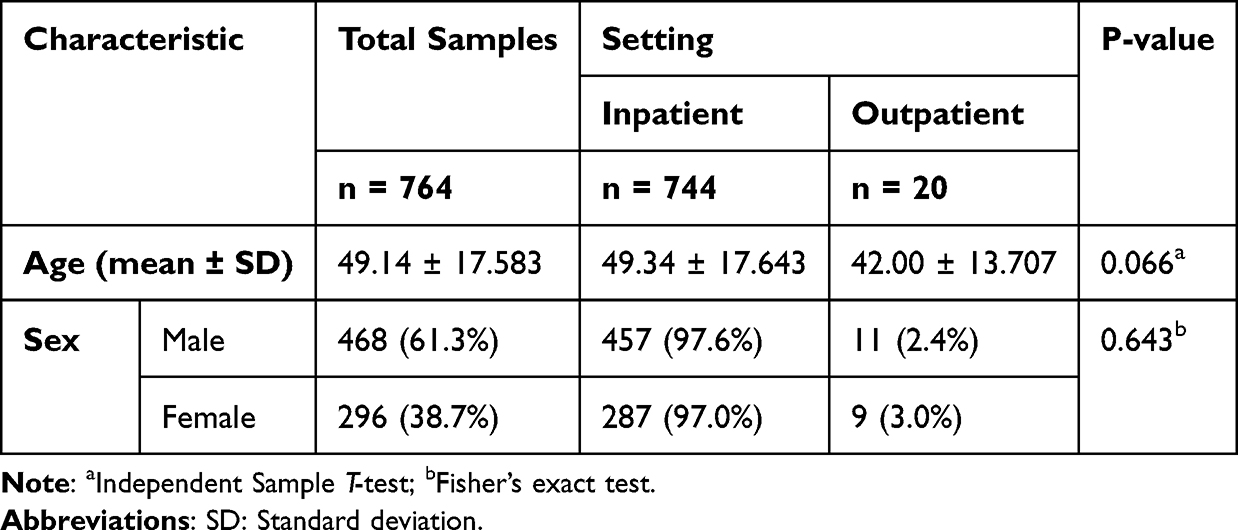 |
Table 2 Demographic Characteristics of Patients Across Inpatient and Outpatient Settings |
Specimen Types, Collection, and Processing
Sterile body fluids included peritoneal, pleural, and pericardial fluids. Cerebrospinal, synovial, and vitreous/ocular fluids were excluded a priori due to differing microbiological profiles and clinical pathways. Peritoneal fluid samples were analyzed in aggregate; distinction between spontaneous bacterial peritonitis (SBP), secondary peritonitis, and peritoneal dialysis (PD) effluent was not possible due to retrospective coding limitations.
Because specimen labels did not reliably differentiate spontaneous bacterial peritonitis, secondary peritonitis, and PD-associated peritonitis, source stratification was incomplete and may influence interpretation of organism distribution.
Samples were collected aseptically by treating clinicians and transported promptly at room temperature to the microbiology laboratory. Specimens with insufficient volume (<1 mL), improper labeling, or prolonged transportation (>2 hours) were rejected according to laboratory policy. Also, duplicate samples, contaminants, and isolates lacking full susceptibility results were excluded. CoNS were assessed against clinical/laboratory criteria to determine significance.12
Upon receipt, each specimen underwent direct Gram stain and cytological assessment. Specimens were inoculated onto standard aerobic culture media (blood agar, MacConkey agar, chocolate agar) and Sabouraud dextrose agar for yeast. Anaerobic culture was performed selectively when clinically indicated (eg, suspected secondary peritonitis), consistent with institutional workflow, as anaerobic organisms require specialized transport and processing not routinely applied to all sterile fluids.2 Cultures were incubated for up to 72 hours aerobically or under CO2 as needed.
Because anaerobic culture was performed selectively rather than routinely, the dataset incompletely reflects the true burden of anaerobic pathogens—particularly in secondary peritonitis and late-stage empyema, where anaerobes such as Bacteroides fragilis, Prevotella, and anaerobic streptococci play major roles.19 The resulting pathogen distribution therefore primarily reflects aerobic and facultative organisms.
Microbiological Processing and Identification
Samples were collected in sterile containers and processed according to standard microbiological procedures. Where required, specimens were centrifuged prior to inoculation. Organism identification was performed using [VITEK/MALDI-TOF], and in cases of discordant results, confirmatory testing was performed using standard laboratory protocols.
Matrix-assisted laser desorption ionization–time of flight mass spectrometry (MALDI-TOF MS; Bruker Biotyper) was introduced in 2021 and used for confirmatory identification thereafter. These platforms are validated and widely used for rapid, accurate microbial identification in clinical laboratories.3,4 Identification databases were updated periodically per manufacturer recommendations.
Polymicrobial cultures were reported when ≥2 clinically significant organisms grew from the same specimen, and each organism was counted separately. Organisms judged to be contaminants based on laboratory and clinical parameters (eg, coagulase-negative staphylococci without supporting clinical evidence) were excluded. Aeromonas species were excluded during data curation due to known environmental contamination concerns.
Antimicrobial Susceptibility Testing (AST)
AST was performed using the VITEK® 2 automated system supplemented by manual disk diffusion or gradient diffusion (Etest) where required. Interpretations followed Clinical and Laboratory Standards Institute (CLSI) guidelines applicable to the year in which the isolate was processed.15 Selective antimicrobial susceptibility testing was applied based on organism type and clinical relevance. For colistin, susceptibility testing was performed using broth microdilution in accordance with CLSI recommendations. Due to the retrospective design, detailed clinical variables (eg, underlying conditions, infection source classification, and outcomes) were not consistently available.
We acknowledge that using contemporaneous breakpoints introduces a potential confounder, as breakpoint definitions (eg, for carbapenems and cephalosporins) evolved during the study period. This may influence temporal trend analysis, as changing interpretive thresholds can artificially elevate or reduce resistance rates independent of true MIC drift. Historical MIC data were not available to retrospectively harmonize all isolates to 2024 standards, representing a significant methodological limitation. However, this approach preserves the clinical categorization reported to treating teams at the time of infection.
Because CLSI breakpoints for cephalosporins, carbapenems, and other key agents changed over the study period, classification of susceptibility is influenced not only by biological shifts but also by evolving interpretive standards. Historical MIC values were unavailable for retrospective harmonization to 2024 criteria. This constitutes a major threat to validity for resistance trend analysis, and some observed changes may partially reflect breakpoint evolution rather than true microbiological improvement.
Intermediate results were classified as non-susceptible for analytic purposes, in line with established AMR reporting conventions. ESBL production was confirmed using CLSI-recommended phenotypic methods (cefotaxime/ceftazidime with and without clavulanate).5 Carbapenem-resistant Enterobacterales (CRE) were defined as Enterobacterales exhibiting non-susceptibility to imipenem, meropenem, and/or ertapenem. Methicillin-resistant Staphylococcus aureus (MRSA) was identified using cefoxitin screening and/or mecA detection where available.
Susceptible-Dose-Dependent (SDD) and Intermediate categories were grouped with Resistant isolates as “non-susceptible” for epidemiologic analysis. While analytically appropriate for surveillance, these categories differ clinically in dosing and therapeutic implications, and the aggregation may slightly alter resistance proportions for agents such as cefepime and piperacillin-tazobactam.
Colistin susceptibility testing was performed using broth microdilution, the only CLSI-endorsed method for determining colistin MICs.7 Disk diffusion and automated system colistin results were not used for interpretation.
Fungal Susceptibility Testing
Yeast isolates underwent antifungal susceptibility testing using CLSI M27 broth microdilution methodology.8 Antifungals tested included fluconazole, voriconazole, micafungin, caspofungin, and flucytosine. Clinical breakpoints and epidemiologic cut-off values (ECVs) were applied based on CLSI M59/M60 guidelines.9
Data Management and Exclusion Criteria
Data were extracted from the laboratory information system and cross-verified manually. To avoid over-representation, only the first unique isolate per organism per patient per clinical episode was included. Repeat isolates with identical organism identification and resistance profiles were excluded as duplicates; however, isolates with new species or new susceptibility patterns were included. Polymicrobial cultures were counted as separate isolates.
Recurrent episodes in the same patient (eg, repeated PD-associated peritonitis) were counted as new events only when the organism or resistance phenotype differed. This approach minimizes overrepresentation of persistent colonization while allowing inclusion of clinically distinct infections.
Exclusions included contaminants, duplicate isolates, environmental organisms (eg, Aeromonas), and samples lacking complete AST profiles. Missing data were handled by listwise deletion.
All data reprocessing and coding were performed using Microsoft Excel 2021.
Statistical Analysis
Statistical analyses were conducted using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics summarized demographic and microbiological characteristics. Continuous variables were presented as means ± standard deviation (SD) and compared using independent t-tests or analysis of variance (ANOVA). Categorical variables were compared using Chi-square or Fisher’s exact tests.
Temporal trends in antimicrobial non-susceptibility were evaluated using binary logistic regression, with year as a continuous predictor. Regression outputs included coefficients (B), standard errors (SE), Wald χ2 values, p-values, odds ratios (OR), and 95% confidence intervals (CI). No multivariable adjustment was applied, consistent with ecological AMR trend analyses.10 Multiple-comparison corrections were not applied, as the objective was exploratory AMR surveillance rather than hypothesis testing.
Logistic regression analyses were unadjusted due to the absence of complete covariate data. Therefore, findings should be interpreted as descriptive trends rather than causal associations.
Some regression coefficients (eg, cefepime OR 0.003, meropenem OR 0.039) likely reflect sparse yearly resistance counts or outlier years rather than dramatic biological shifts. These values should therefore be interpreted cautiously.
A significance threshold of p < 0.05 (two-tailed) was used for all analyses.
Quality Assurance
The laboratory adhered to internal quality control procedures and participated in external proficiency testing programs, including College of American Pathologists (CAP) and other regional schemes, ensuring reliability and accuracy of identification and AST results.11 Instruments underwent routine calibration and maintenance per manufacturer protocols.
Ethical Approval
The study was approved by the Research Ethics Committee at King Khalid University (IRB KKU-153-2025-31). As a retrospective analysis of anonymized laboratory data, the requirement for informed consent was waived by the institutional ethics committee, not by the authors, and in accordance with the principles of the Declaration of Helsinki.
Results
Specimen Overview and Flow
Across the study period, a total of 764 clinically significant isolates were recovered from sterile body fluid specimens. After removing duplicates, contaminants, and samples lacking complete antimicrobial susceptibility data, these 764 unique isolates formed the dataset for analysis. Of these, 682 (89.3%) were bacterial isolates and 82 (10.7%) were yeasts. The bacterial isolates were distributed across peritoneal, pleural, and pericardial fluids, with peritoneal fluid representing the vast majority of samples.
Distribution of Organisms by Gram Reaction
Gram-negative bacteria predominated, accounting for nearly three-quarters (74.8%) of all bacterial isolates. Among these Gram-negative organisms, fermenters were the dominant group, representing 74.7% of Gram-negatives (55.9% of all bacteria), while non-fermenters accounted for 25.3% (18.9% of all bacteria).
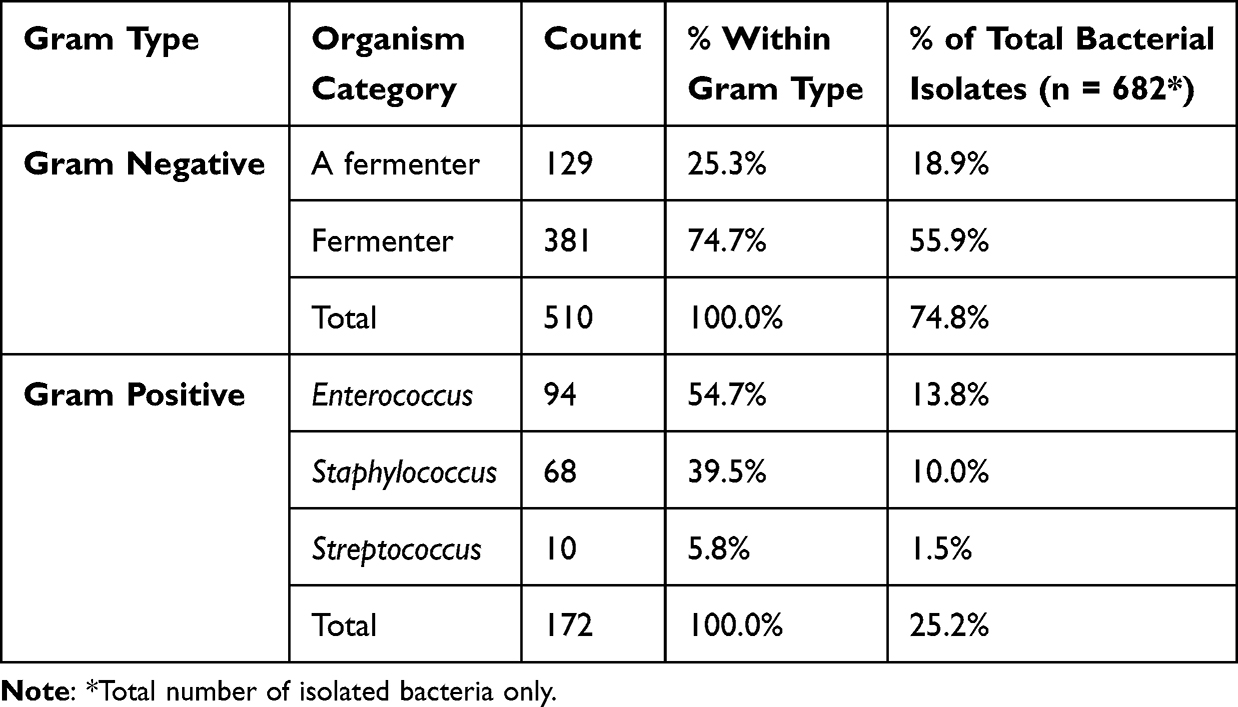 |
Table 3 Distribution of Organism Categories Within Gram-Positive and Gram-Negative Isolates |
Gram-positive organisms constituted 25.2% of bacterial isolates. Within this group, Enterococcus species were the most common, representing over half of Gram-positive isolates, followed by Staphylococcus species (including MRSA and MSSA) and a much smaller proportion of Streptococcus species. Subgroup counts for Streptococcus spp., pericardial isolates, and CRAB were small and should be interpreted descriptively. The detailed distribution of organisms by species and subgroup is presented in Table 3. The distribution of isolates by specimen type is summarized in Table 4.
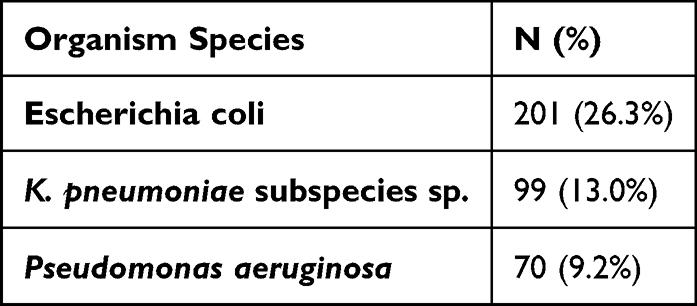 |
Table 4 Most Common Organism Species in Study Population |
Most Common Species Isolated (Table 4)
At the species level, Escherichia coli was the single most frequently isolated pathogen, comprising 26.3% of all isolates. It was followed by:
- Klebsiella pneumoniae subspecies (13.0%)
- Pseudomonas aeruginosa (9.2%)
Together, these organisms formed a substantial portion of the microbiological burden in sterile body fluids. Other relevant pathogens included Staphylococcus aureus, E. faecalis, E. faecium, and various Candida species.
Prevalence of Major Resistance Phenotypes (Table 5).
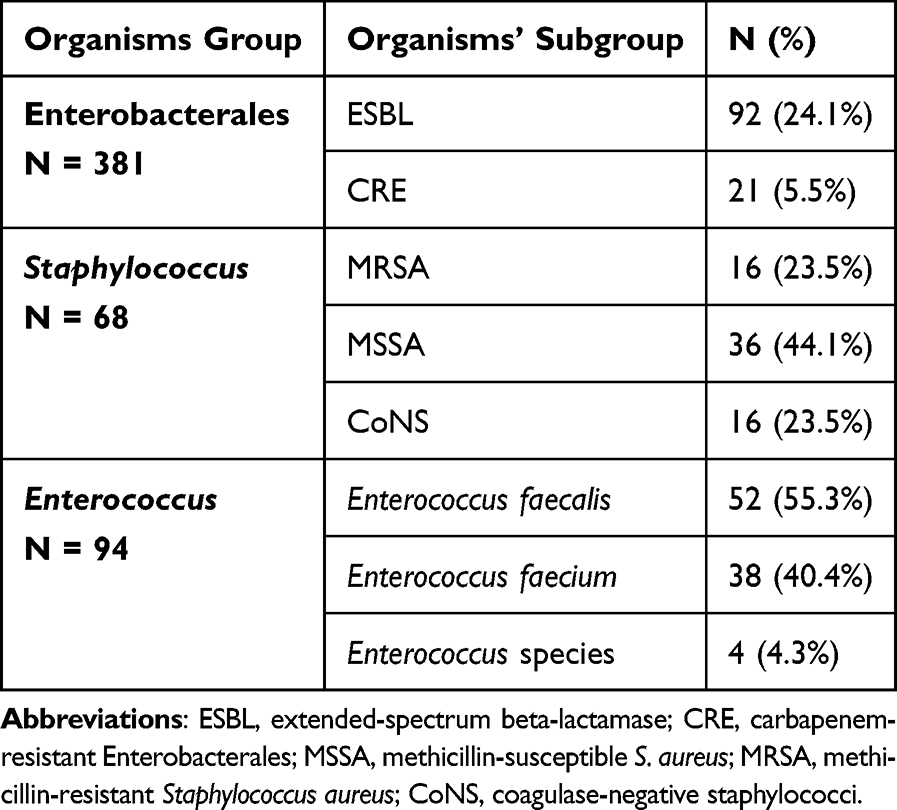 |
Table 5 Prevalence of Species Subgroups Among Enterobacterales, Staphylococcus, and Enterococcus Isolates |
Enterobacterales
Among the 381 Enterobacterales isolates:
- 24.1% were ESBL producers
- 5.5% were carbapenem-resistant Enterobacterales (CRE)
These findings reflect significant β-lactam resistance within this group. Annual CRE rates are illustrated in Figure 1. ESBL trends over time are shown in Figure 2.
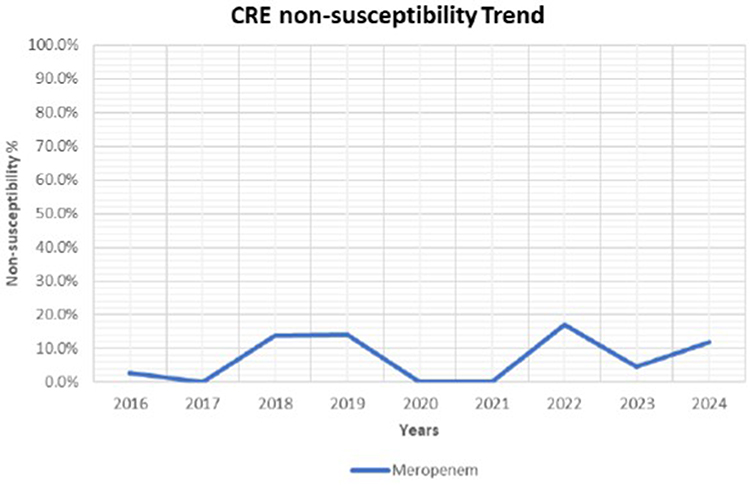 |
Figure 1 CRE non-susceptibility Trend. |
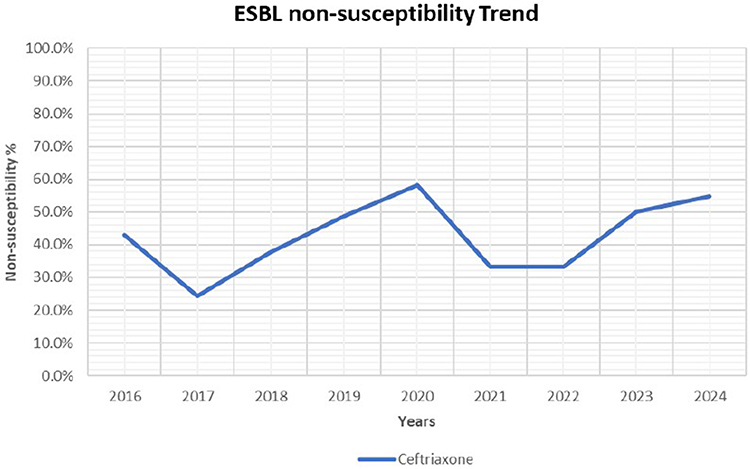 |
Figure 2 ESBL non-susceptibility Trend. |
Staphylococcus Species
Among 68 Staphylococcus isolates:
- 23.5% were MRSA
- 44.1% MSSA
- 23.5% coagulase-negative staphylococci
Enterococcus Species
Among 94 Enterococcus isolates:
- E. faecalis accounted for 55.3%
- E. faecium for 40.4%
- Other species were uncommon
Non-fermenters
Seven isolates of carbapenem-resistant Acinetobacter baumannii (CRAB) were identified, representing a clinically important multidrug-resistant subgroup.
Distribution Across Body Fluid Types (Table 6)
Because only one pericardial fluid isolate was recovered, this category was excluded from all statistical comparisons and is presented descriptively only. Peritoneal fluid accounted for the majority of isolates (83.7%), reflecting the high clinical frequency of intra-abdominal infections. Pleural fluid contributed 16.1% of isolates, while only one organism was recovered from pericardial fluid.
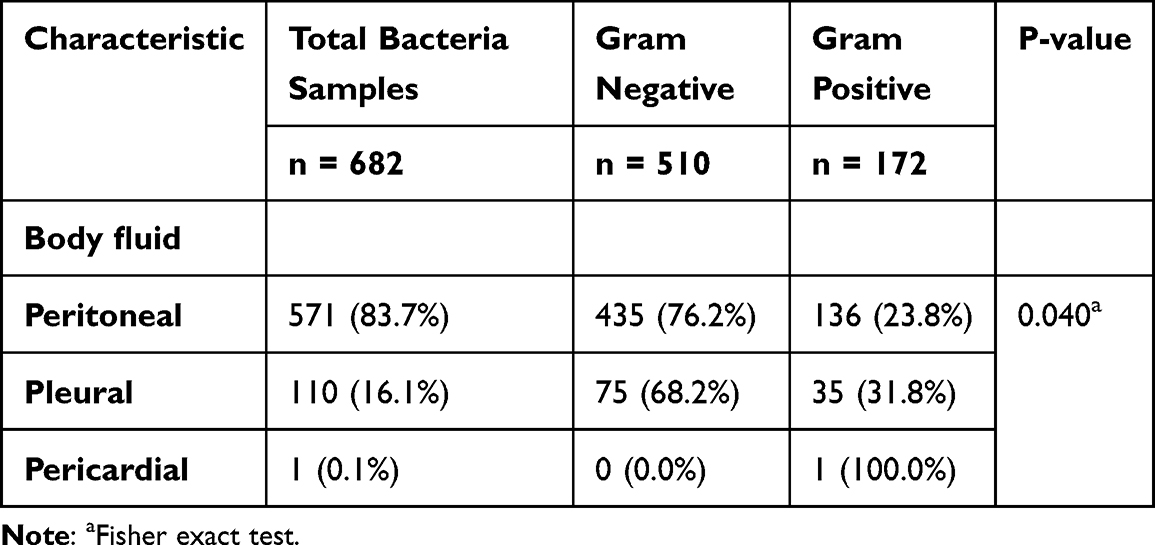 |
Table 6 Distribution of Gram-Negative and Gram-Positive Bacteria by Sterile Body Fluid Type (n = 682) |
The proportion of Gram-negative bacteria varied significantly by body fluid type:
- Peritoneal fluid: 76.2% Gram-negative
- Pleural fluid: 68.2% Gram-negative
- Pericardial fluid: One Gram-positive isolate
The difference in Gram distribution between fluid types was statistically significant (p=0.040). However, due to the singular isolate in the pericardial group (n=1), this significance is driven primarily by the comparison between peritoneal and pleural fluids.
Antimicrobial Susceptibility Patterns
Gram-Negative Bacteria
Fermenting Gram-negative organisms demonstrated high resistance to amoxicillin–clavulanate and third-generation cephalosporins. Non-fermenters—particularly P. aeruginosa and A. baumannii—exhibited markedly higher non-susceptibility rates to carbapenems, aminoglycosides, and fluoroquinolones compared with fermenters. Non-susceptibility patterns among fermenters and non-fermenters are detailed in Table 7.
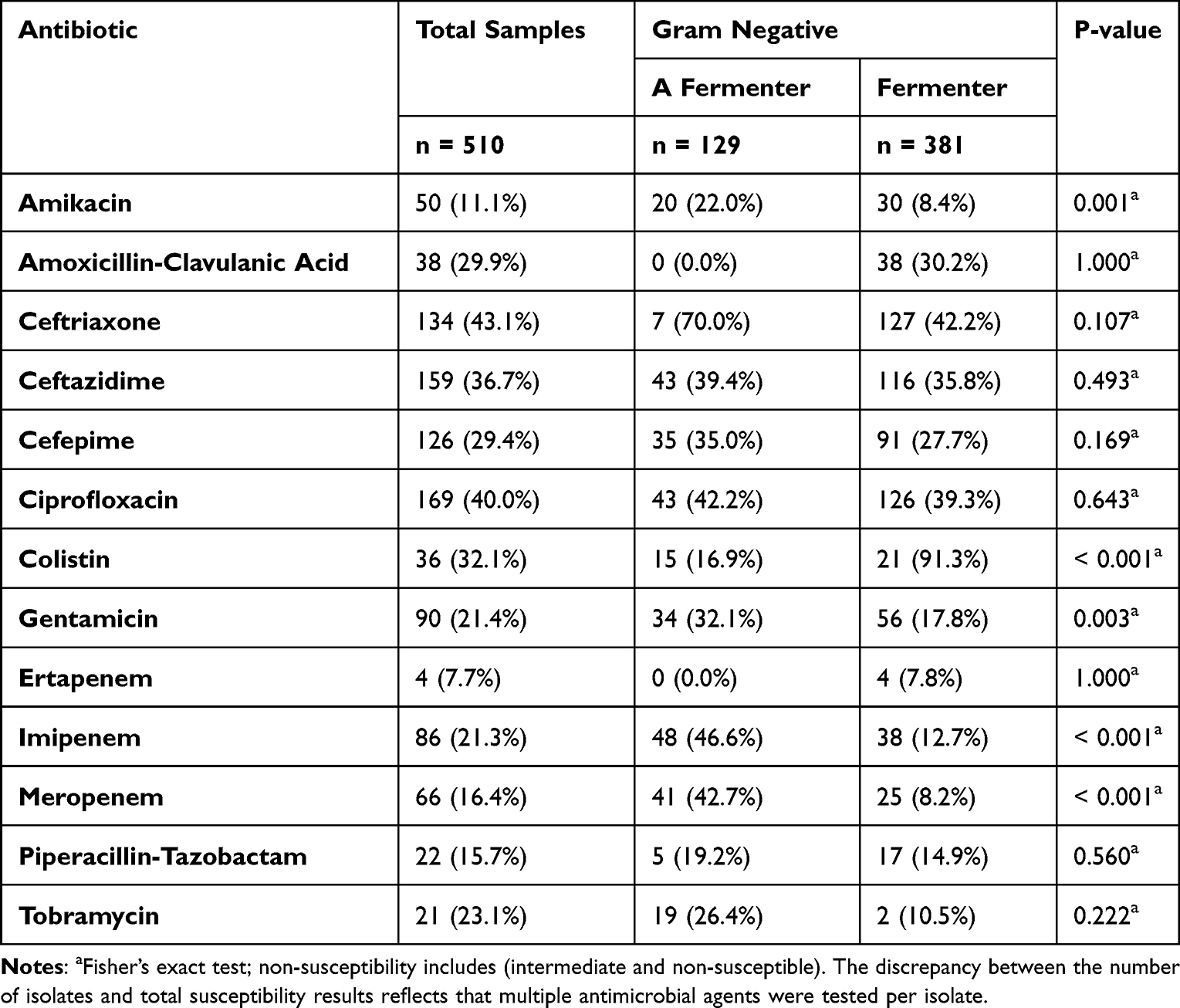 |
Table 7 Non-Susceptibility Rates Between Gram Negative Species for Antibiotics Specific for Gram Negatives |
Gram-Positive Bacteria
MRSA isolates remained fully susceptible to vancomycin, linezolid, and daptomycin. Enterococcus species showed predictable patterns:
- Variable susceptibility to ampicillin
- High susceptibility to vancomycin and linezolid
- No vancomycin-resistant Enterococcus (VRE) detected
Susceptibility profiles for Gram-positive organisms are shown in Table 8. This Gram distribution remained broadly consistent across the study period. Differences between Gram-negative and Gram-positive organisms were consistent across fluid types and clinical settings, with Gram-negative isolates predominating overall, as presented in Table 9.
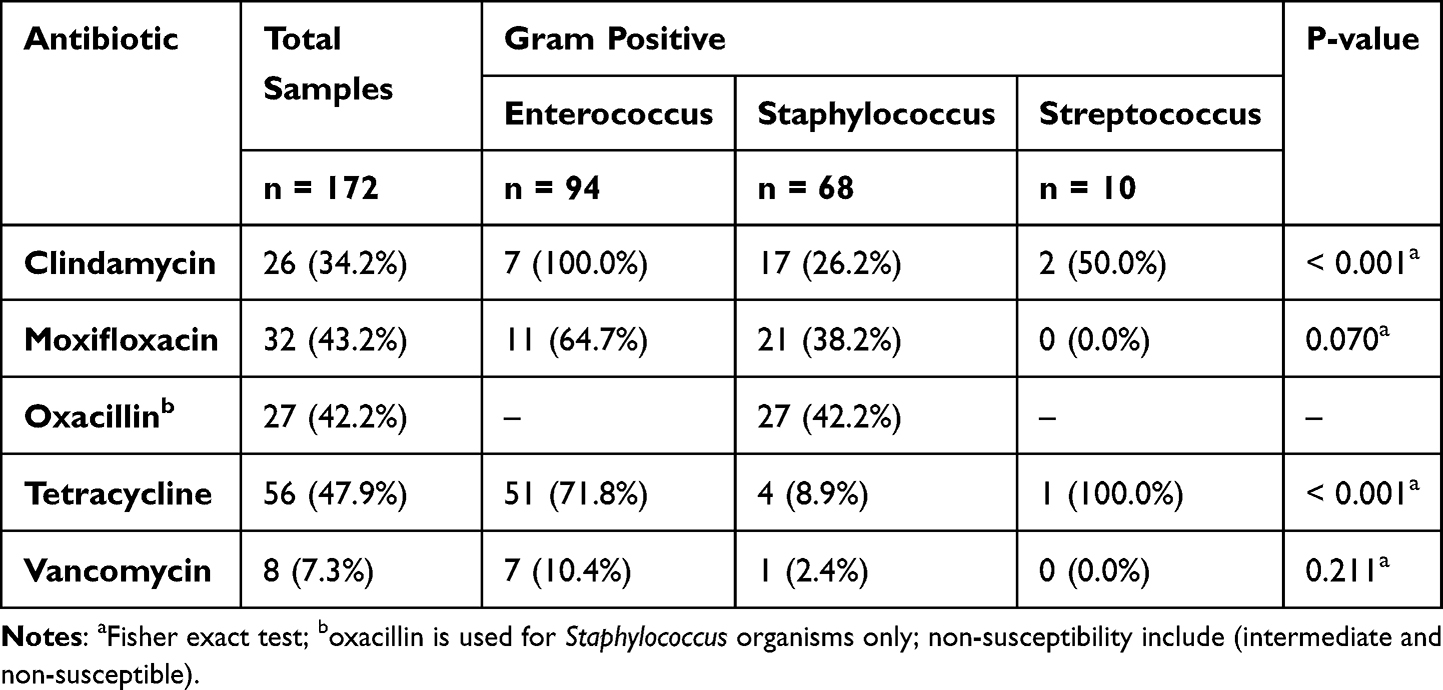 |
Table 8 Non-Susceptibility Rates Between Gram Positive Species to Antibiotics Specific for Gram Positives |
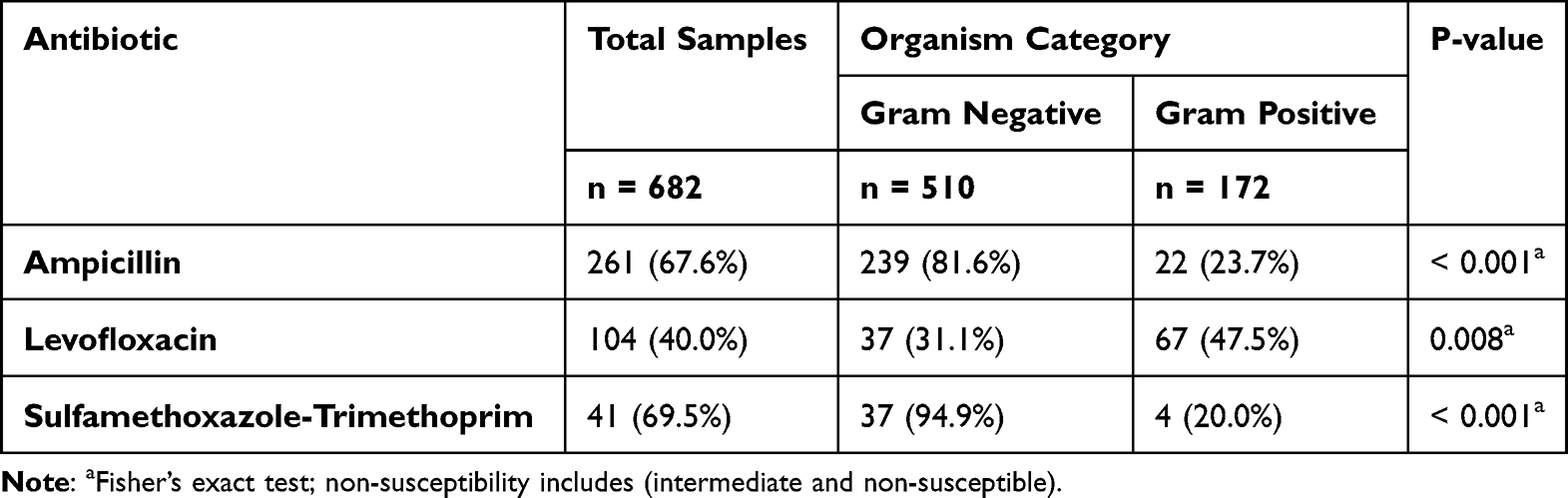 |
Table 9 Non-Susceptibility Rates Between Gram Negative and Gram Positive for Shared Antibiotics |
Yeasts
Yeast isolates retained high susceptibility to azoles and echinocandins, with >95% susceptibility to micafungin and caspofungin. No multidrug-resistant yeast phenotypes were identified. Antifungal susceptibility results for yeasts are summarized in Table 10. The proportion of intermediate results within non-susceptible isolates is detailed in Table 11.
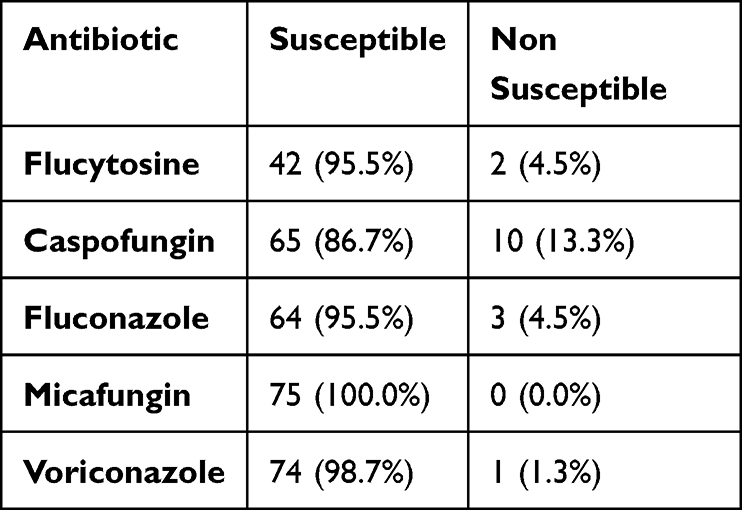 |
Table 10 Prevalence of Susceptibility and Non-Susceptibility Rates in Yeast to Antifungal Specific for Yeast |
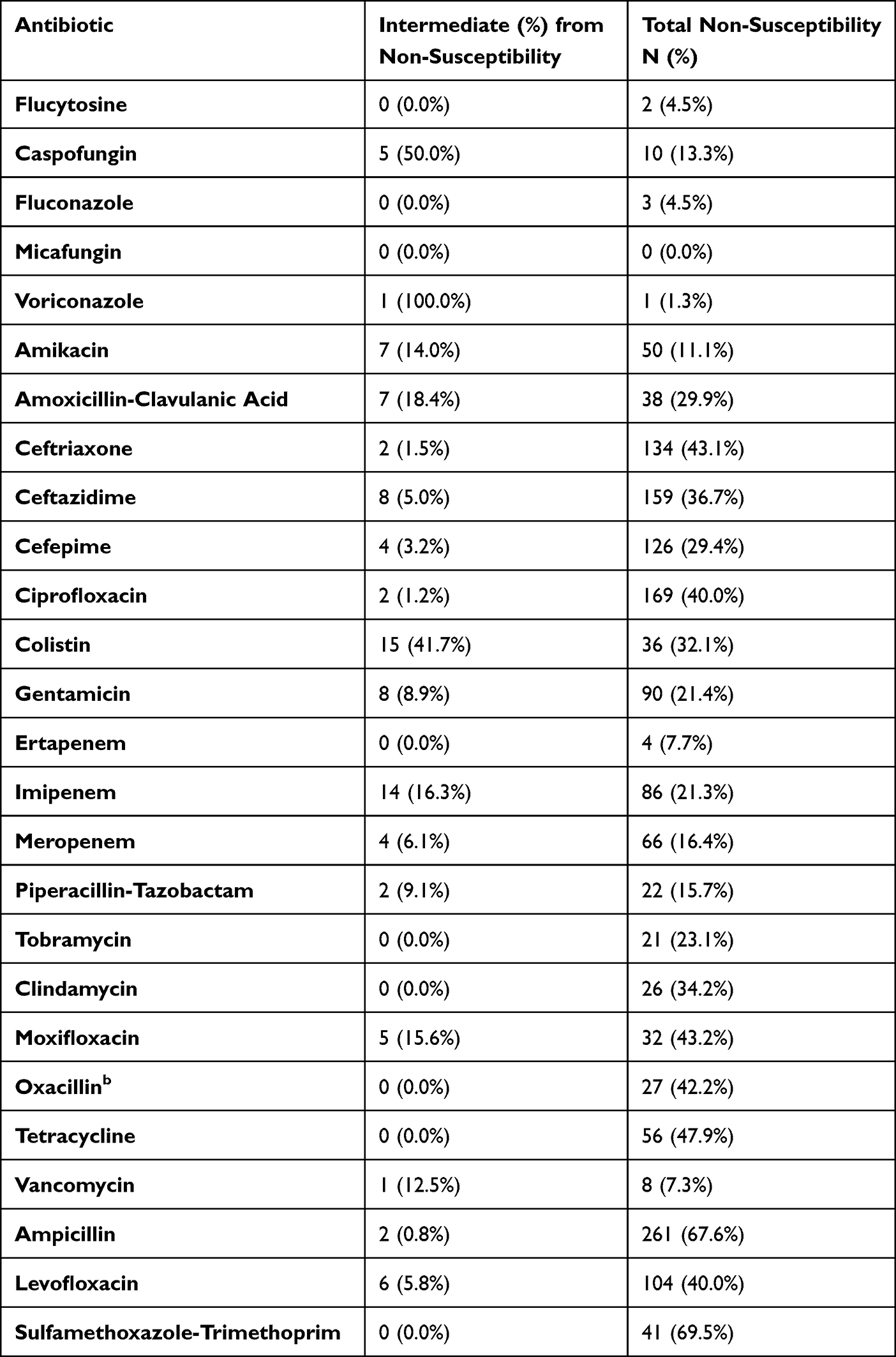 |
Table 11 Frequencies of Intermediate Cases Inside Non-Susceptibility |
Temporal Trends in Antimicrobial Non-Susceptibility (Table 12)
Regression analysis revealed significant year-over-year reductions in non-susceptibility for several key antibiotics:
- Gentamicin: significant annual decline
- Ceftazidime: significant annual decline
- Cefepime: significant annual decline
- Meropenem: significant annual decline
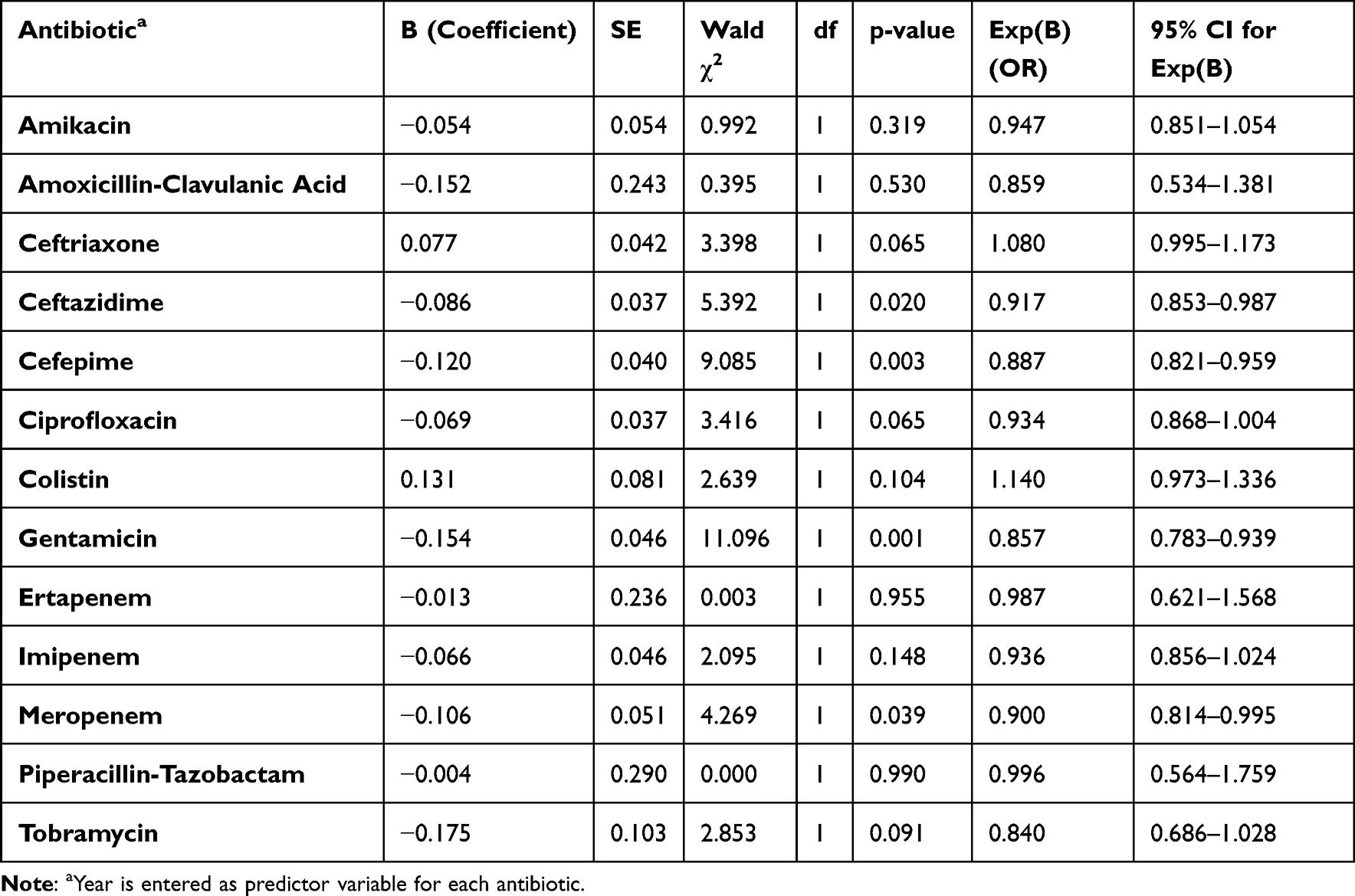 |
Table 12 Logistic Regression Models for Antibiotics Non-Susceptibility Trends for Gram Negative Species |
These findings indicate progressive improvement in susceptibility patterns across the study period, particularly among Gram-negative organisms. These findings should be interpreted as descriptive temporal trends, as regression analyses were unadjusted for potential confounders.
Non-significant trends were observed for ciprofloxacin, imipenem, tobramycin, ertapenem, and colistin.
Some regression coefficients (eg, cefepime OR 0.003, meropenem OR 0.039) likely reflect sparse yearly resistance counts or outlier years rather than dramatic biological shifts. These values should therefore be interpreted cautiously. Table 13 illustrates the logistic regression models for antibiotics non-susceptibility trends for gram positive species. Table 14 illustrates the logistic regression models for antibiotics non-susceptibility trends for gram negative and positive species together.
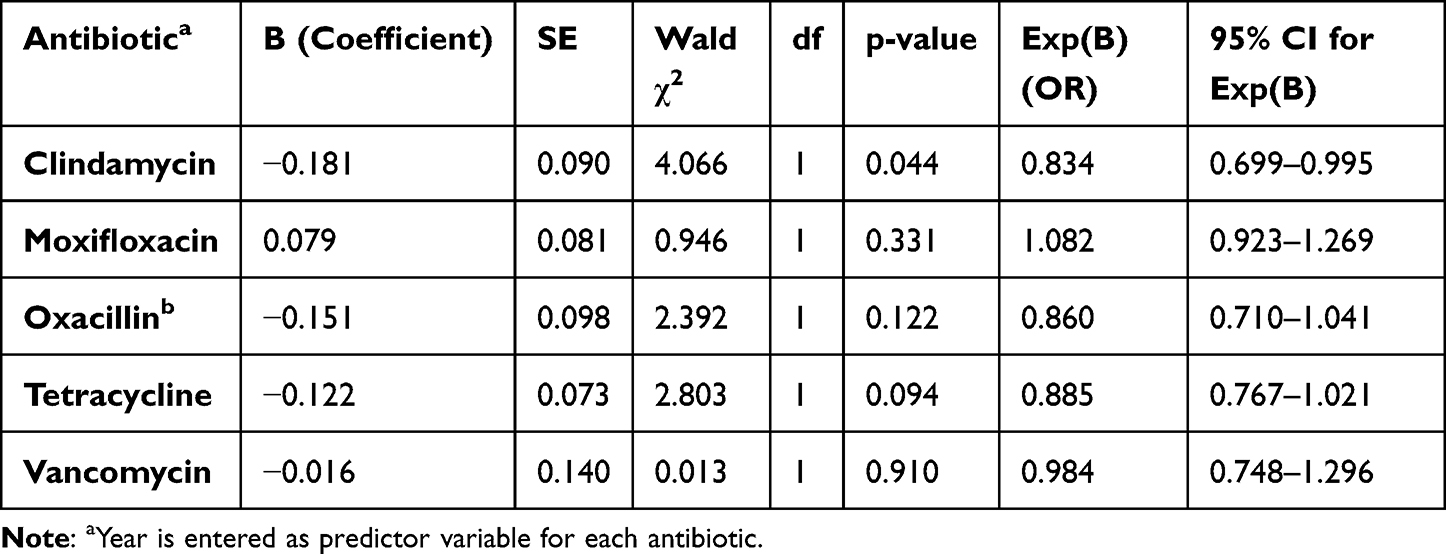 |
Table 13 Logistic Regression Models for Antibiotics Non-Susceptibility Trends for Gram Positive Species |
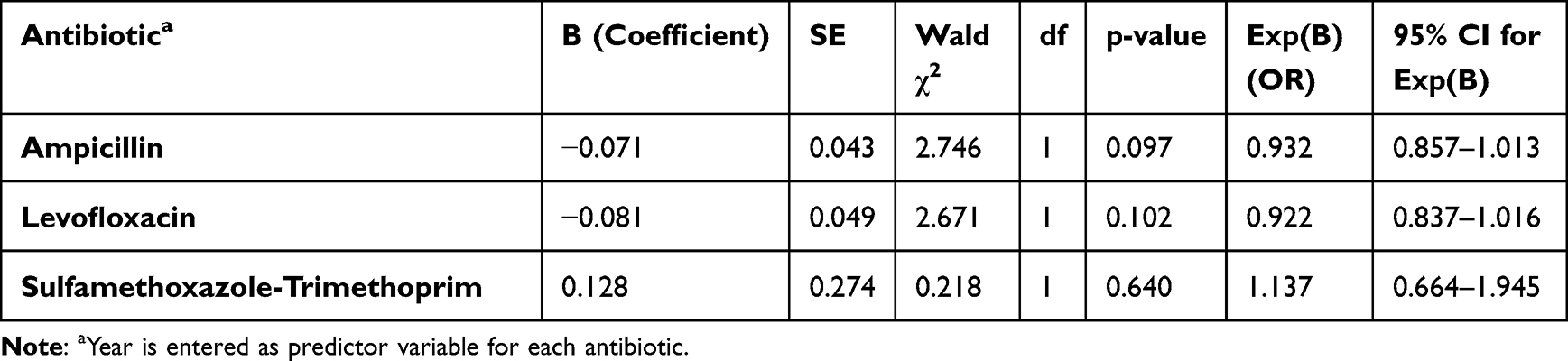 |
Table 14 Logistic Regression Models for Antibiotics Non-Susceptibility Trends for Gram Negative and Positive Species Together |
Summary of Principal Findings
- Gram-negative bacteria dominated sterile body fluid cultures (74.8%).
- E. coli, K. pneumoniae, and P. aeruginosa were the most common pathogens.
- High ESBL prevalence (24.1%) and moderate CRE prevalence (5.5%) were observed among Enterobacterales.
- MRSA accounted for nearly one-quarter of Staphylococcus isolates.
- Significant reductions in non-susceptibility were detected for gentamicin, ceftazidime, cefepime, and meropenem.
Yeasts remained highly susceptible to available antifungal agents.
Interpretation of resistance patterns among low-frequency groups—including Streptococcus spp. (n=10), CRAB, and pericardial isolates—should be considered descriptive due to limited statistical power. We propose replacing line graphs with annual proportion bar charts with 95% confidence intervals to facilitate interpretation of variability and precision in yearly resistance estimates.
Comprehensive antimicrobial susceptibility profiles are detailed in Tables 7–11. Additional stratified analyses and extended antimicrobial resistance comparisons are presented in Tables 13 and 14.
Discussion
This nine-year analysis provides one of the most detailed evaluations of pathogens isolated from sterile body fluids in a tertiary-care setting in Saudi Arabia. The dominance of Gram-negative organisms—particularly Escherichia coli, Klebsiella pneumoniae, and Pseudomonas aeruginosa—aligns with established epidemiological patterns for intra-abdominal and pleural infections.1–4 These organisms are well-recognized as the leading causes of secondary peritonitis, abdominal sepsis, and hospital-associated pleural infections due to gastrointestinal translocation, postoperative contamination, and severe pneumonia.1–4
The stronger dominance of Gram-negatives in peritoneal fluid is consistent with classical secondary peritonitis, whereas pleural infections more frequently involve Gram-positive organisms due to their association with post-pneumonic empyema.4,5 It is critical to interpret the Gram-negative dominance (74.8%) within the context of study methodology. As anaerobic culture was not routine, strict anaerobes (eg, Bacteroides spp., Fusobacterium spp).—which are key pathogens in secondary peritonitis and mature empyema—are under-represented. Consequently, our data likely overestimates the relative proportion of aerobic Gram-negative bacilli compared to true polymicrobial burden.
Furthermore, the relatively high proportion of Gram-negative isolates in pleural fluid differs from many Western CA-empyema cohorts, where Streptococcus species predominate. This pattern is more consistent with hospital-acquired or postoperative empyema, suggesting our pleural dataset may include a higher proportion of HA infections.4,20,21
Importantly, peritoneal fluid in our dataset encompassed a heterogeneous case-mix, including spontaneous bacterial peritonitis (SBP), secondary peritonitis, and peritoneal dialysis (PD)-associated peritonitis. These clinical entities differ substantially in microbial etiology—SBP is typically monomicrobial and Enterobacterales-predominant, secondary peritonitis is frequently polymicrobial and anaerobe-rich,22 and PD peritonitis more commonly involves skin flora such as coagulase-negative Staphylococci and Enterococcus. Because specimen referral pathways did not systematically distinguish these categories, the resulting pathogen distribution likely over-represents SBP and under-represents polymicrobial postoperative infections. Consequently, the Gram-negative predominance observed in the study reflects aerobic isolates and may not represent the full spectrum of secondary peritonitis.
However, because SBP, secondary peritonitis, and PD-associated peritonitis could not be reliably separated, the observed organism distribution likely over-represents monomicrobial SBP and under-represents polymicrobial surgical peritonitis. Consequently, the Gram-negative predominance observed in the study reflects aerobic isolates and may not represent the full spectrum of secondary peritonitis, in which anaerobes comprise a major component.
The high proportion of ESBL-producing Enterobacterales (24%) and notable CRE prevalence (5.5%) reflect patterns reported in Saudi Arabia and the Gulf Cooperation Council (GCC), where ESBL prevalence commonly exceeds 20–30% and CRE incidence continues to rise.5,6 These phenotypes pose major therapeutic challenges, often requiring carbapenems, ceftazidime–avibactam, or colistin, and are associated with increased mortality and longer hospital stays.9,10 The predominance of E. coli and K. pneumoniae among resistant Enterobacterales reflects global resistance trends.9
Non-fermenting Gram-negative organisms demonstrated markedly higher resistance than fermenters, with A. baumannii showing carbapenem resistance. CRAB is recognized internationally as a critical priority pathogen due to its limited treatment options, high attributable mortality, and persistence in hospital environments.16,17 Its recovery from sterile body fluids underscores the severity of illness in affected patients and highlights the importance of infection prevention and control (IPC) measures.
Enterococcus species accounted for a substantial proportion of Gram-positive isolates. This is consistent with their frequent involvement in postoperative and healthcare-associated intra-abdominal infections, particularly among immunocompromised or surgical patients.11 The absence of vancomycin-resistant Enterococcus (VRE) aligns with several regional studies reporting low VRE prevalence in Saudi Arabia despite increasing global rates.12 MRSA represented nearly a quarter of Staphylococcus aureus isolates, a pattern similar to regional pleural and soft-tissue infection studies.14 Importantly, all MRSA isolates remained susceptible to vancomycin, linezolid, and daptomycin.
Yeast isolates, although fewer than bacterial isolates, displayed high susceptibility to azoles and echinocandins. This is consistent with global surveillance programs such as SENTRY and ARTEMIS, which report high susceptibility among Candida albicans and variable susceptibility among non-albicans species.13,14 No multidrug-resistant yeast phenotypes such as Candida auris were identified, though this organism has emerged in the Middle East and warrants continued surveillance.17
A key finding of this study was the significant decline in non-susceptibility to gentamicin, ceftazidime, cefepime, and meropenem. Although caution is warranted—given the possibility of confounding from case mix variation, diagnostic evolution, or shifting test platforms—several published studies have shown improved susceptibility patterns following antimicrobial stewardship (AMS) and IPC interventions.22–24 While our dataset cannot attribute causation, these trends are encouraging and may reflect broader institutional AMS efforts. However, non-stewardship drivers must also be considered; these include shifts in patient case-mix (eg, post-COVID-19 admission patterns) and potential fluctuations in the ratio of community-acquired versus hospital-acquired infections presenting to the emergency department.
Additionally, because antibiotic consumption data, stewardship implementation dates, and infection prevention interventions were not available for correlation, attributing resistance declines to AMS or IPC measures remains speculative. Alternative explanations—such as shifts in patient demographics, post-COVID changes in case mix, or a higher proportion of community-acquired infections—may also contribute.
The low recovery of Streptococcus species, particularly S. pneumoniae, from pleural fluid may reflect vaccination impact, improved pneumonia management, or under-representation of early-stage parapneumonic effusions; later-stage empyema typically yields mixed flora including anaerobes, which were not uniformly cultured.25 The high prevalence of Enterococcus species in peritoneal isolates may relate to underlying surgical, oncologic, or immunosuppressed populations. The near absence of pericardial isolates is expected given the rarity of purulent pericarditis.
Collectively, this study provides a comprehensive long-term overview of sterile body fluid microbiology and resistance patterns, filling an important gap in regional infectious disease surveillance and offering actionable insights to guide empiric therapy and stewardship strategies.
The primary contribution of this study lies in its long-term surveillance perspective, providing institution-specific resistance trends to support empiric therapy decisions.
Limitations
This study has several limitations. The absence of routine anaerobic culture represents a key limitation, particularly for intra-abdominal and pleural infections where anaerobic organisms are clinically significant. Consequently, the observed predominance of Gram-negative organisms reflects aerobic isolates only and may underestimate the true polymicrobial burden. Others are:
- As a retrospective isolate-based study, it lacked detailed clinical data such as patient demographics, comorbidities, hospitalization status, prior antimicrobial exposure, and clinical outcomes, all of which may influence organism distribution and resistance patterns.
- The inability to stratify peritoneal fluid by infection source is a significant limitation. The aggregation of Spontaneous Bacterial Peritonitis (typically monomicrobial, Enterobacterales-dominant) with Secondary Peritonitis (polymicrobial) and Peritoneal Dialysis peritonitis (often Staphylococcus or skin-flora associated) obscures specific risk profiles. Future prospective surveillance must distinguish these clinical entities to improve granular utility.
- CLSI breakpoint modifications over the nine-year period represent a substantial limitation for resistance trend interpretation. Without harmonized retrospective MIC re-analysis, observed temporal shifts may reflect interpretive changes rather than true microbiological evolution.15
- Certain organism groups—such as Streptococcus spp., CRAB, and pericardial isolates—had small sample sizes, limiting precision. Subgroup analyses involving organisms with low counts (eg, Streptococcus spp., CRAB, pericardial isolates) lack statistical power, limiting reliability of associated p-values.
- This is a single-center study, which may limit generalizability to other hospitals with different patient populations or AMR epidemiology.
- Fungal species identification beyond Candida spp. was limited, preventing deeper characterization of non-albicans epidemiology.
- Anaerobic cultures were not routinely performed, limiting this analysis to aerobic and facultative organisms and preventing full characterization of the pathogen spectrum in secondary peritonitis or advanced empyema.
- Because peritoneal dialysis–associated peritonitis could not be reliably distinguished from other peritoneal infections, organism distribution and resistance patterns among peritoneal isolates may partially reflect PD-associated pathogens.
- Finally, clinical outcomes (eg, mortality, length of stay, need for drainage procedures) were not available, preventing correlation between AMR patterns and clinical impact.
Future Directions
Future studies should incorporate multi-center datasets to strengthen representativeness, integrate clinical variables to correlate AMR with outcomes, and include routine anaerobic culture and fungal speciation for greater microbiological accuracy. Routine molecular AMR surveillance (eg, ESBL and Carbapenemase gene typing) would clarify resistance evolution over time.
Molecular characterization of resistance mechanisms—particularly ESBL and carbapenemase genes—would clarify the drivers of resistance phenotypes. Linking microbiological trends to antibiotic consumption data, surgical practices, and stewardship interventions would enhance causal inference.
These findings should be interpreted within the context of the study’s aerobic scope, peritoneal source heterogeneity, selective anaerobic culture, and breakpoint evolution across the study period.
Finally, development of sterile-body-fluid–specific institutional and regional antibiograms would support more accurate empiric therapy.
Conclusion
This nine-year review provides one of the most comprehensive aerobic microbiological profiles of sterile body fluid infections from a tertiary-care center in Saudi Arabia. Gram-negative organisms predominated across peritoneal and pleural samples, with substantial ESBL and carbapenem resistance burdens that reflect regional and global AMR trends. Although encouraging reductions in non-susceptibility were observed for several key antibiotics—including gentamicin, ceftazidime, cefepime, and meropenem—these trends should be interpreted cautiously given breakpoint evolution, source heterogeneity among peritoneal fluids, and the limited inclusion of anaerobic organisms.
Despite these limitations, the dataset offers important insights into local pathogen distribution and resistance evolution. It demonstrates the necessity of sterile-fluid–specific antibiograms and highlights institutional progress toward improved antimicrobial governance. Sustained and standardized surveillance, improved specimen stratification, and broadened anaerobic diagnostics are essential to refining empirical therapy and reducing diagnostic uncertainty. Ultimately, these findings underscore the need for coordinated stewardship, infection prevention, and laboratory capacity-building efforts to mitigate the evolving threat of AMR in high-risk clinical settings.
Recommendations
- Develop sterile body fluid–specific antibiograms: Empiric therapy for peritonitis and empyema should be guided by compartment-specific resistance patterns rather than general hospital antibiograms.
- Routinely distinguish peritoneal infection subtypes: Laboratory and clinical workflows should ensure clear labelling of SBP, secondary peritonitis, and PD-associated peritonitis to enable meaningful AMR interpretation.
- Implement routine anaerobic cultures: Secondary peritonitis and late-stage empyema cannot be accurately characterized without systematic anaerobic culture, which should be integrated into standard protocols.
- Future AMR trend analyses should store MIC values to allow retrospective reinterpretation and reduce bias from evolving breakpoints.
- Expand surveillance to multi-center networks: A regional sterile body fluid AMR surveillance platform would provide more robust epidemiology and support national antimicrobial guidelines.
- Integrate molecular diagnostics: Carbapenemase and ESBL gene detection would enable more precise tracking of resistance mechanisms and outbreak detection.
- Strengthen antimicrobial stewardship and IPC synergy: Targeted interventions should address high-risk areas such as surgical units, ICUs, and PD programs, where AMR burden is greatest.
- Upgrade data reporting and visualization: Adoption of annual bar charts with confidence intervals will improve transparency and interpretability of AMR trends.
These findings should be interpreted within the context of the study’s aerobic scope, peritoneal source heterogeneity, selective anaerobic culture, and breakpoint evolution across the study period.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sartelli M, Viale P, Catena F, et al. WSES guidelines for management of intra-abdominal infections. World J Emerg Surg. 2013;8:3. doi:10.1186/1749-7922-8-3
2. Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of complicated intra-abdominal infection in adults and children. Clin Infect Dis. 2010;50(2):133–18. doi:10.1086/649110
3. Montravers P, Lepape A, Misset B, et al. Clinical and microbiological profiles of secondary peritonitis (CIAO Study). Clin Microbiol Infect. 2015;21 Suppl 1:S7–15. doi:10.1016/j.cmi.2014.12.015
4. Gupta A, Agrawal A, Wright C, et al. Empyema thoracis: epidemiology, microbiology, and management. Clin Microbiol Rev. 2022;35(1):e00106–21. doi:10.1128/CMR.00106-21
5. Pitout JDD, Nordmann P, Poirel L. Carbapenemase-producing Klebsiella pneumoniae: a key pathogen. Antimicrob Agents Chemother. 2015;59(10):5873–5884. doi:10.1128/AAC.01019-15
6. Logan LK, Weinstein RA. Epidemiology of carbapenem-resistant Enterobacteriaceae. J Infect Dis. 2017;215 Suppl 1:S28–36. doi:10.1093/infdis/jiw282
7. Aly M, Balkhy HH. AMR among Enterobacteriaceae in Saudi Arabia. J Infect Public Health. 2012;5(3):209–219. doi:10.1016/j.jiph.2012.02.002
8. Zowawi HM, Balkhy HH, Walsh TR, Paterson DL. β-lactamase–producing Gram-negatives in GCC states. Clin Microbiol Infect. 2013;19(10):894–903. doi:10.1111/1469-0691.12222
9. Zowawi HM, Harris PN, Roberts MJ, et al. MDR Gram-negative bacteria in urology. Nat Rev Urol. 2015;12(10):570–584. doi:10.1038/nrurol.2015.199
10. Balkhy HH, El-Saed A, Maghraby R, et al. AMR surveillance in Saudi Arabia. Saudi Med J. 2019;40(11):1201–1215. doi:10.15537/smj.2019.11.24543
11. Miller WR, Munita JM, Arias CA. Mechanisms of antibiotic resistance in enterococci. Infect Dis Clin North Am. 2020;34(4):751–771. doi:10.1016/j.idc.2020.08.004
12. Becker K, Heilmann C, Peters G. Coagulase-negative staphylococci. Clin Microbiol Rev. 2014;27(4):870–926. doi:10.1128/CMR.00109-13
13. Arendrup MC. Candida and candidemia. Clin Microbiol Infect. 2013;19(1):1–7. doi:10.1111/1469-0691.12040
14. Perlin DS, Rautemaa-Richardson R, Alastruey-Izquierdo A. Global antifungal resistance. Lancet Infect Dis. 2017;17(12):e383–92. doi:10.1016/S1473-3099(17)30316-X
15. Humphries RM, Abbott AN, Hindler JA. Understanding revised CLSI breakpoints. Clin Infect Dis. 2019;69(12):2145–2150. doi:10.1093/cid/ciz633
16. Gales AC, Seifert H, Gur D, Castanheira M, Jones RN, Sader HS. SENTRY surveillance of A. baumannii and S. maltophilia. Open Forum Infect Dis. 2019;6(Suppl 1):S34–46. doi:10.1093/ofid/ofz031
17. Zhang S, Li Y, Wang X, et al. Risk factors for carbapenem-resistant A. baumannii colonization. Front Microbiol. 2025;15:1519906. doi:10.3389/fmicb.2024.1519906
18. Van Duin D, Paterson DL. Multidrug-resistant bacteria in the community. Infect Dis Clin North Am. 2016;30(2):377–390. doi:10.1016/j.idc.2016.02.004
19. De Bus L, Gadeyne B, De Waele J, et al. Antimicrobial de-escalation in the critically ill. Int J Antimicrob Agents. 2019;54(2):89–97. doi:10.1016/j.ijantimicag.2019.04.011
20. Rahman NM, Chapman SJ, Davies RJO. Management of pleural infection. Clin Chest Med. 2013;34(1):117–132. doi:10.1016/j.ccm.2012.11.001
21. Baur D, Gladstone BP, Burkert F, et al. Effect of antimicrobial stewardship: systematic review. Lancet Infect Dis. 2017;17(9):990–1001. doi:10.1016/S1473-3099(17)30325-0
22. Brook I. Microbiology and management of peritonitis. Clin Microbiol Rev. 1994;7(2):175–189. doi:10.1128/CMR.7.2.175
23. Kaki R, Elligsen M, Walker S, Simor A, Palmay L, Daneman N. Impact of AMS programs. Clin Infect Dis. 2011;52(7):870–876. doi:10.1093/cid/cir068
24. Kollef MH, Micek ST. AMS programs: mandatory for ICUs. Crit Care. 2012;16(6):179. doi:10.1186/cc11694
25. Kourtis AP, Hatfield K, Baggs J, et al. Trends in MRSA/MSSA bloodstream infections. MMWR. 2019;68(9):214–219. doi:10.15585/mmwr.mm6809e1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.