Back to Journals » Journal of Asthma and Allergy » Volume 15
Aero-Allergen Sensitization in the General Population: Longitudinal Analyses of the LEAD (Lung Heart Social Body) Study
Authors Kölli F, Breyer MK, Hartl S, Burghuber O, Wouters EFM, Sigsgaard T ![]() , Pohl W, Kohlböck G, Breyer-Kohansal R
, Pohl W, Kohlböck G, Breyer-Kohansal R
Received 16 December 2021
Accepted for publication 4 March 2022
Published 11 April 2022 Volume 2022:15 Pages 461—473
DOI https://doi.org/10.2147/JAA.S349614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Luis Garcia-Marcos
Franziska Kölli,1,2 Marie-Kathrin Breyer,2,3 Sylvia Hartl,1– 3 Otto Burghuber,1,2 Emiel FM Wouters,2,4 Torben Sigsgaard,5 Wolfgang Pohl,6 Gabriele Kohlböck,2 Robab Breyer-Kohansal2,3
1Sigmund Freud University, Faculty of Medicine, Vienna, Austria; 2Ludwig Boltzmann Institute for Lung Health, Vienna, Austria; 3Department of Respiratory and Critical Care Medicine, Clinic Penzing, Vienna, Austria; 4NUTRIM School of Nutrition and Translational Research in Metabolism, University Medical Center, Maastricht, The Netherlands; 5Department of Public Health, Section of Environment, Occupation & Health, Aarhus University, Aarhus, Denmark; 6Karl Landsteiner Institute for Clinical and Experimental Pneumology, Clinic Hietzing, Vienna, Austria
Correspondence: Franziska Kölli, Ludwig Boltzmann Institute for Lung Health, Sanatroium Street 2, Vienna, 1140, Austria, Tel +436645127500, Email [email protected]
Background: Monitoring of sensitization may become a non-invasive marker of impaired epithelial barrier function related to changing environmental conditions.
Objective: To longitudinally evaluate the prevalence and associated factors for positive skin prick tests (SPT) in a general population cohort.
Methods: Baseline and 4-year follow-up data from the longitudinal LEAD study are used for the current analyses. Risk factors for SPT were analyzed by multivariate binary logistic regression analyses, including residence (urban/rural), sex, socioeconomic status (SES), allergic and/or respiratory diseases, lung function testing, blood eosinophils, body composition, lifestyle habits, family history, pets in household, and exposure to tobacco smoke in childhood/adolescence (6– 18 years) and adulthood (≥ 19 years).
Results: In total, 1439 children/adolescents and 9844 adults with valid SPTs were included in these analyses. The prevalence of sensitization at baseline was 37.6% and was higher in males in every age group, except 10–< 15 years. Individuals with doctor´s diagnosed allergy, asthma or parental allergy were more likely to have a positive SPT; in adulthood, sensitization was more common in those with a high SES. A lower occurrence of sensitization was associated with the presence of a dog in the household in childhood/adolescence and with smoking in adulthood. The prevalence and intensity (number of positive SPT reactions) increased after a 4-year follow-up, especially in children/adolescents.
Conclusion: Sensitization is common in the general Austrian population and more likely in males than females. Longitudinal monitoring of sensitization in children/adolescents may identify environmental triggers related to changes in urbanization, industrialization and domestic lifestyle. ClinicalTrials.gov NCT01727518.
Keywords: allergy, sensitization, aero-allergens, childhood/adolescence, adults
Introduction
Over the last half century, allergy to environmental antigens has become more common, with prevalence varying from 17–69%,1,2 and house dust mite3 and grass pollen4 being the most common aero-allergens.5 Epidemiological studies suggest a higher prevalence of sensitization in males,2,6–8 younger individuals,4,5,9 and in those with higher educational status,5 and lower prevalence in the elderly,4,10 with mixed data on the correlation with smoking.11,12
Sensitization is a well-known risk factor for the development of respiratory symptoms and disease manifestations such as allergic rhinitis, allergic conjunctivitis, wheezing, impaired lung function, and asthma.4,13–15 Early-life sensitization is related to decreased lung function by school age,14 and in adolescence,16 and to wheezing,17 eczema,17 and a higher risk of developing asthma by 7 years of age.14 Family history of allergy is not only known to be a risk factor for sensitization and allergy in offspring18 but also associated with allergic symptoms in offspring, especially eczema.13
It is also known that there are differences in dog dander sensitization and it is possible to be sensitized only to male or female dogs.19
The skin prick test (SPT) is a minimally invasive, inexpensive and reliable diagnostic method of detecting an immediate (Type I) sensitization and is therefore suitable to assess the presence of allergy. Longitudinal data on the progression of SPT reactivity from childhood to adulthood are scarce. One such study followed a cohort of 200 Healthy newborns in Finland from birth to 20 years of age; SPT positivity at a young age forecasted SPT positivity in adulthood, with an increase in sensitization over 6- and 15-year follow-up periods.20 In contrast, in a Swedish population study in adults the prevalence of positive SPTs decreased with increasing age.10 However, longitudinal data from childhood up to the elderly population are still missing and analyzed in this work. The Austrian LEAD (Lung, hEart, sociAl, boDy) study, a population-based longitudinal cohort offers the opportunity to assess allergy prevalence in different age groups, as well as to evaluate SPT positivity longitudinally over the whole life span.21
The current analyses aim to investigate the prevalence and age- and sex distribution of positive SPT in the general population both at baseline and after a 4-year follow-up. Furthermore, determining factors associated with positive SPT at baseline are studied.
Methods
Ethics
The Austrian LEAD study is approved by the local Ethics committee of Vienna (protocol number: EK-11-117-0711). All participants signed written informed consent; those for children under the age of 18 had to be signed by their parents or legal representative.21 The manuscript was conducted in accordance with the Declaration of Helsinki. Data is accessible from one of the co-authors Priv.-Doz. Dr. Breyer-Kohansal.
Study Design
The Austrian LEAD study (ClinicalTrials.gov; NCT01727518) has been described in detail elsewhere.21 It is a longitudinal, observational, population-based cohort study that has recruited 11,423 participants (47.6% male) aged 6–82 years. The cohort was randomly recruited in Vienna and Lower Austria, stratified by age, sex and residential area. Comparison with data published by the Governmental Statistic Department and the Austrian Governmental Microcensus showed almost identical distribution of age, gender, ethnicity, educational level and smoking status supporting the representativeness of the LEAD cohort for the Austrian population.21 The baseline visit took place between 2012 and 2016, with the 4-year-follow up taking place between 2017 and 2021. Exclusion criteria were limited to current pregnancy, current breastfeeding, or poor language skills.
Skin Prick Test
Antihistamines or glucocorticoids were withdrawn for at least 48 h before testing. At the baseline and follow-up visits, SPT was performed on the forearms of all participants by trained technicians.22 The SPT was positive if there was a reaction ≥3 mm diameter for at least one of the allergens. The following aero-allergens were tested: ash tree, tree pollen mix (hazel, alder, birch), grass mix (Anthoxantum, Dactylis, Lolium, Phleum and Poa), mugwort, ragweed, ribwort, mites mix (Dermatophagoides Farinae and Dermatophagoides Pteronyssinus), mildew, and dog and cat dander.21 In both phases, all allergens were obtained from the company “Alk-Abello” and were the identical allergens in both, in baseline and follow-up analyzes. Thus, a batch-to-batch consistency over 4 years was given. Positive (0.1% histamine) and negative (0.9% sodium chloride) controls were included in the test panel.
Individual Factors
The presence of allergy and/or asthma was based on doctor diagnosis, with self-reporting of respiratory and allergic symptoms (wheezing, cough, dyspnea, breathlessness, rhinoconjunctivitis and eczema). Information about diagnosed asthma in siblings or allergy in parents, smoking status and pack-years, second-hand smoking, parental smoking and pets in the household was collected by an interview-based questionnaire. A list of all factors is in the online supplement (Table S1).
Lung function testing was performed according to international recommendations,23 after an adequate wash-out for any inhalation therapy. Low lung function was defined as forced expiratory volume in 1 second (FEV1) below the lower limit of normal (LLN) according to Global Lung Initiative (GLI) values.24 Airflow limitation was defined as FEV1/forced vital capacity (FVC) below the GLI LLN.25 Body composition was assessed by calculation of the body mass index (BMI), and measurement of the fat mass index (FMI) and fat-free mass index (FFMI) using whole-body dual energy X‐ray absorptiometry (DEXA; Lunar ProdigyTM, GE Healthcare©, Chicago, IL, USA). Socioeconomic status (SES) categories were based on occupational status, educational status, income status, and a combined score (for children the SES of their parents or parent with the major child custody was used).
Statistical Analysis
Statistical analyses were performed with IBM SPSS version 26.0, with level of significance set at <5%. All reported p-values are based on two-sided tests. Univariate inferential statistics for distribution comparisons include Χ2-tests for general crosstabs and Fisher’s exact tests for 2×2 tables. Statistically significant overall comparisons via Χ2-test in terms of body composition or smoking status were examined more closely using post-hoc tests for pairs of categories (Fisher´s exact tests). Indicators of risk were analyzed by binary logistic regression for childhood/adolescence and adulthood separately. Both forced entry model and backward regression model was calculated. Omnibus and Hosmer and Lemeshow goodness of fit tests were calculated for all regression models. All models were stratified by sex to consider the potential confounder. All analyses were performed separately for baseline childhood/adolescence (6–18 years) and adulthood (≥19 years) age categories. To compare SPT status between baseline and after 4-year follow-up, an alluvial plot in R was made for childhood/adolescence and adulthood categories.
Results
In total, 1439 children/adolescents aged 6–18 years and 9844 adults aged from 19–82 years with valid SPTs are included in these analyses (Table 1).
 |
Table 1 Baseline Characteristics |
Prevalence of Positive Skin Prick Test at Baseline
At baseline, the overall prevalence of a positive SPT for at least one allergen was 37.6% (N=4246), with 37.2% (N=535) in childhood/adolescence and 37.7% (N=3711) in adulthood. The prevalence was higher in males than females, both in childhood/adolescence (42.9% vs 30.5%; p<0.001) and adulthood (42.2% vs 33.7%; p<0.001) and was also higher in males in all age groups, with the exception of 10–<15 years (Figure 1). Peak prevalence was at 10–<15 years in females and 19–<29 years in males, then subsequently decreased steadily in both sexes (Figure 1).
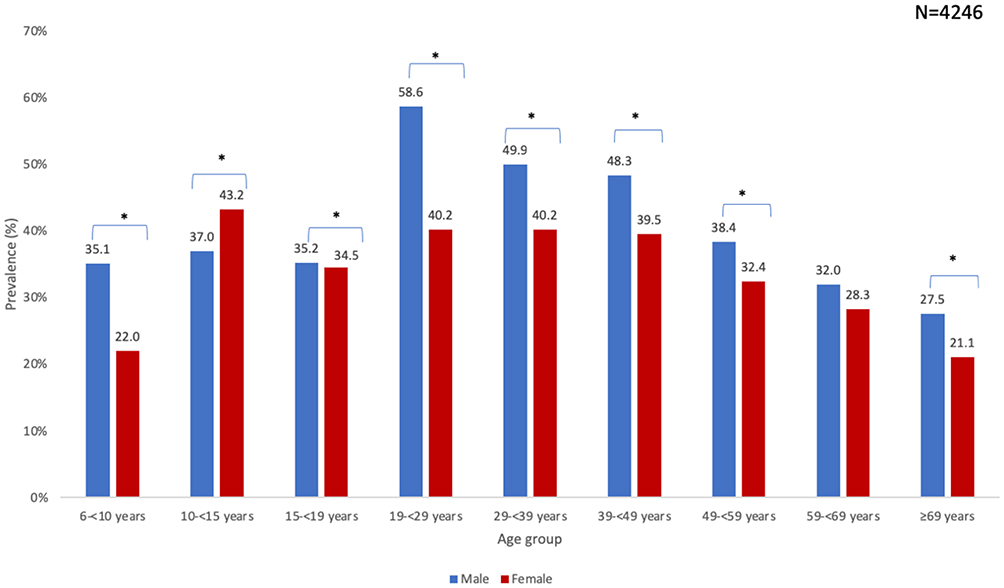 |
Figure 1 Prevalence of positive skin prick test by age and gender at baseline. *p<0.05 male vs female. |
The overall mean number of positive SPT reactions per individual was 3.02 in childhood/adolescence and 3.37 in adulthood. Among the children/adolescents who were SPT positive, 11.3% had a reaction to ≥4 allergens compared to 14.9% in adults. We did not observe any association between the numbers of positive SPT reactions and family history of atopy. However, a higher number of positive SPT reactions was significantly associated with the presence of doctor´s diagnosed asthma, neuro-dermatitis or asthma, and allergic (rhinoconjunctivitis, eczema and breathlessness) and non-allergic symptoms (wheezing and sputum production), in both age groups (Tables S2 and S3). In the subgroup with at least one SPT, adults were more likely than children/adolescents to have rhino-conjunctivitis, eczema, doctor’s diagnosed asthma, high income or SES status, COPD/chronic bronchitis/emphysema, coughing or sputum production, airflow limitation, or a second-hand or paternal smoking history (Table S4). Furthermore, compared with adults with a positive SPT, children/adolescents were significantly more likely to be male, have an urban residence, to be diagnosed with neuro-dermatitis, to have a parent with an allergy, to demonstrate lung function reversibility, to have a history of maternal smoking (both ever and during pregnancy), and to currently have a pet in their household (Table S4). At baseline 45.6% of children and 61% of adults with a positive SPT also had a doctor’s diagnosis of allergy.
Patterns of SPT Positivity at Baseline
The most prevalent allergens were grass mix and mites mix (20.8% and 22.1%, respectively, in children/adolescents; 20.7% and 19.2% in adults, Figure 2). The prevalence of sensitization was significantly higher in adulthood than childhood/adolescence for mugwort, ash tree, early tree mix, dog dander, cat dander and ribwort, while mite mix and mildew positivity were significantly more common in childhood. The prevalence of SPT positivity for every allergen was significantly higher in males than females, with the exception of mugwort and ragweed for childhood/adolescence (Figure 3). In adulthood, the prevalence of every allergen was higher in males than in females (Figure 4)
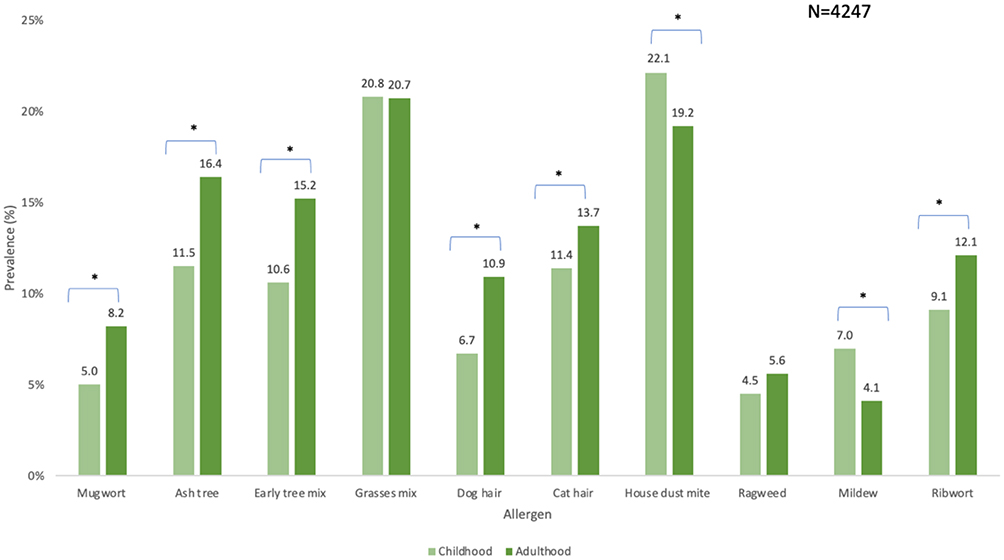 |
Figure 2 Prevalence of specific SPT at baseline in childhood /adolescence vs adulthood. *p<0.05 childhood/adolescence vs adulthood. |
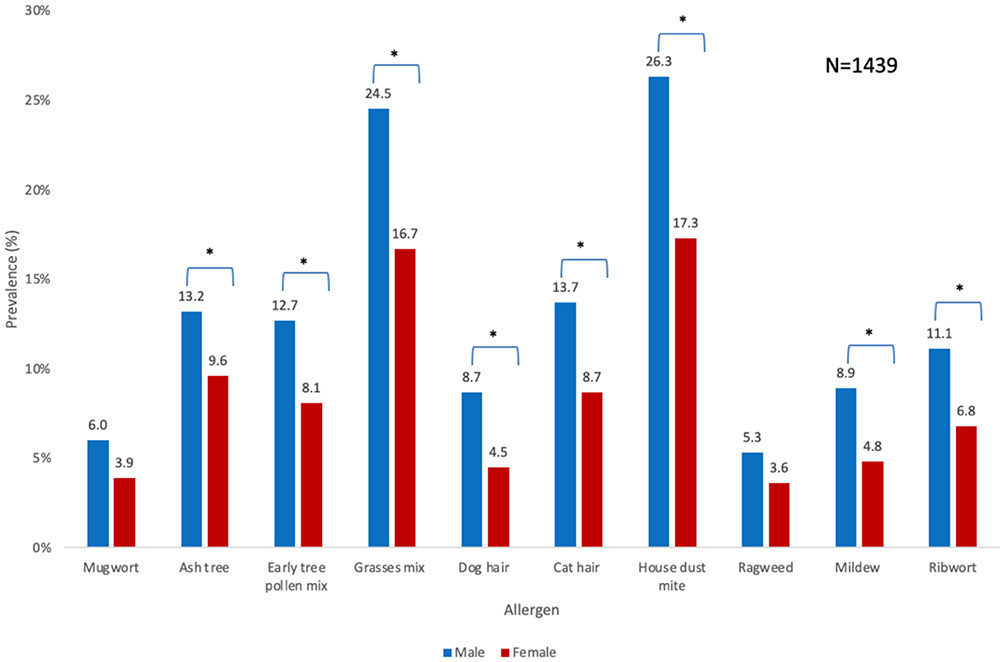 |
Figure 3 Prevalence of each allergen in childhood/adolescence by gender. *p<0.05 male vs female. |
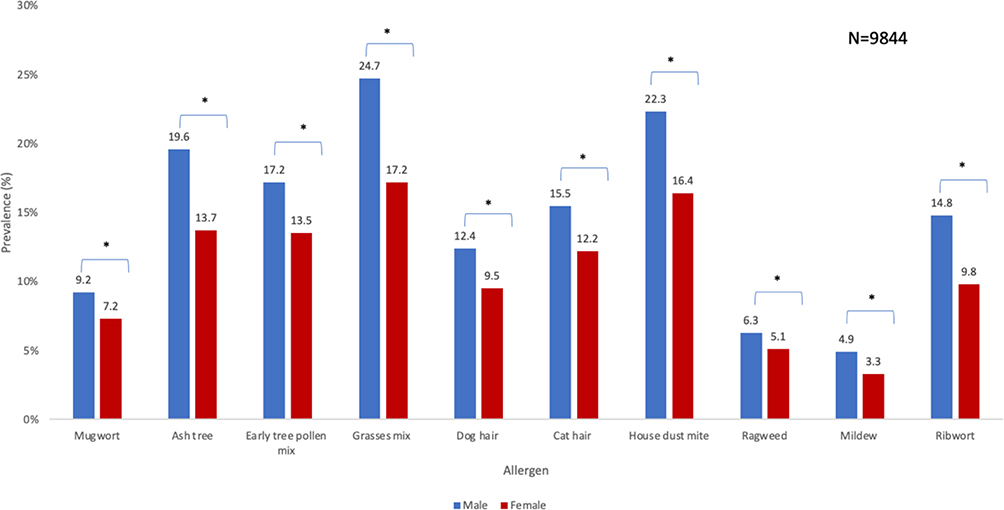 |
Figure 4 Prevalence of each allergen in adulthood by gender. *p<0.05 male vs female. |
Determining Factors of Sensitization in Childhood/Adolescence and Adulthood at Baseline
In univariate analyses, in both age groups a positive SPT was more likely in males, and those with high income status, doctor´s diagnosis of allergy or asthma, parental allergy, and symptoms of wheezing and rhinitis (Table S5). In the multivariate regression analyses in children/adolescents, males were 1.68 times (68%) more likely to have a positive SPT than females (p<0.001) (Table 2). Adjusted for sex, other factors associated with an increased likelihood of a positive SPT were age category 10–<15 or 15-<19 years vs 6–<10 years (ORs 1.94 and 2.30, p<0.001; respectively), and higher eosinophil count (OR 9.87; p<0.001). A dog in the household was associated with a decreased likelihood of a positive SPT (ORs 0.65, p=0.024; respectively).
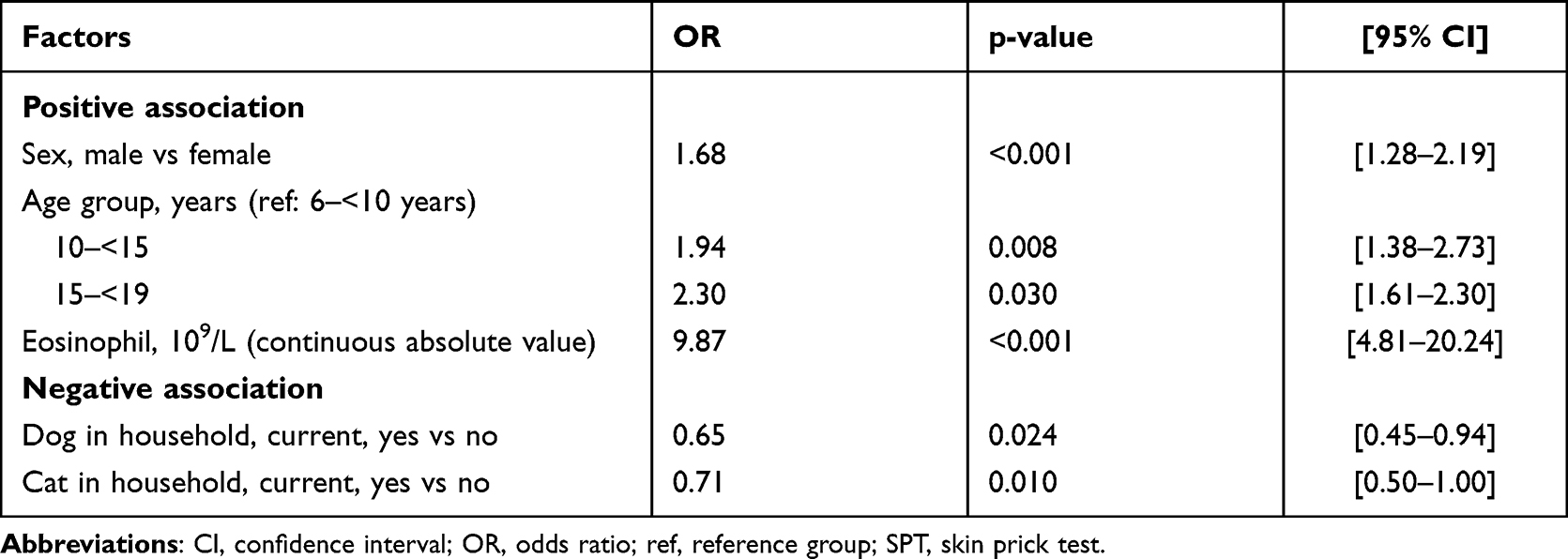 |
Table 2 Associated Factors for a Positive SPT in Childhood/Adolescence at Baseline, Mutually Adjusted (N=1439) |
In the multivariate regression analyses in adults, males were 1.86 times (86%) more likely to have a positive SPT than females (p<0.001) (Table 3). Adjusted for sex, other factors associated with an increased likelihood of a positive SPT were high SES (OR 1.27, p<0.001), parental allergy (OR 1.26, p<0.001), and higher eosinophil count (OR 3.54; p<0.001). Former (OR 0.83; p=0.002), current (OR 0.76; p<0.001), and second-hand smoking (OR 0.87; p=0.008) were associated with a decreased likelihood of a positive SPT.
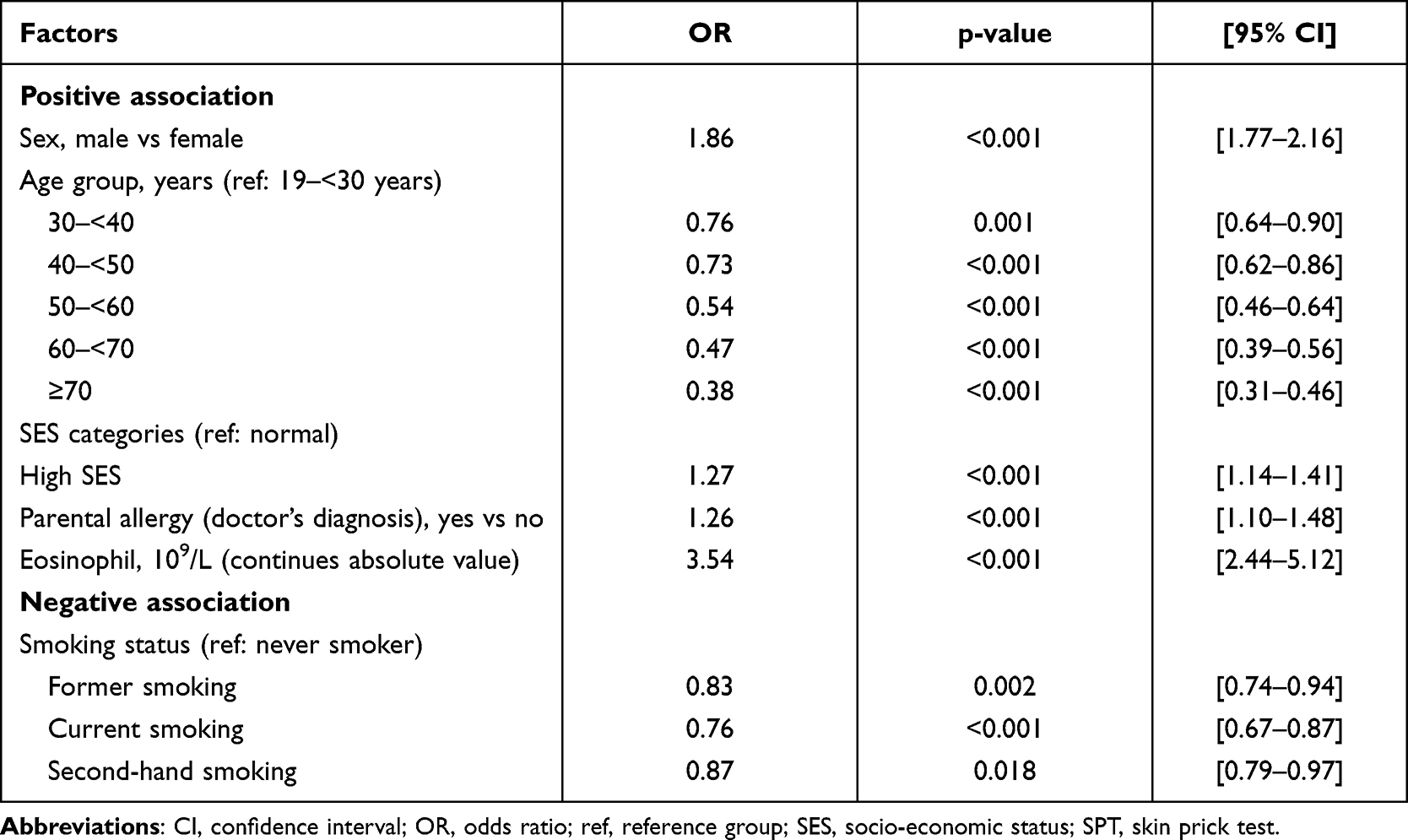 |
Table 3 Associated Factors for a Positive SPT in Adulthood at Baseline, Mutually Adjusted (N=9844) |
Follow-Up Data of SPT Positivity
The overall prevalence of sensitization at the 4-year follow-up visit was 38.6%. In childhood/adolescence, 94.0% (N=268) of the participants with a positive SPT at baseline remained positive at follow-up; 15.6% (N=77) of those who tested negative at baseline tested positive at follow-up. 6% (N=17) of initially positive tested children lost their SPT positivity. Of the 2468 adults with a positive baseline SPT, 87.7% (N=2164) were also positive at follow-up, with 8.8% (N= 370) newly testing positive at 4 years. In adulthood 12.3% (N=304) were tested positive at baseline and then negative after 4-year follow-up.
Between baseline and the 4-year follow-up, there was an overall increase in the number of positive SPT reactions, especially in childhood/adolescence, with more than half of those who had one positive SPT at baseline having an increase in the number of positive SPTs at follow-up in both age categories (Figures 5 and 6).
 |
Figure 5 Flow graph of positive skin prick test at baseline and after a 4-year follow-up period in childhood/adolescence. Abbreviation: SPT, skin prick test. |
 |
Figure 6 Flow graph of positive skin prick test at baseline and after a 4-year follow-up period in adulthood. Abbreviation: SPT, skin prick test. |
Discussion
In this population-based study, we found that: (1) a positive SPT to aero-allergens is common throughout the population; (2) a positive SPT is more likely in males than in females, except for those aged 10–<15 years; (3) the most prevalent reactions are to grass and mite mixes; (4) there are some differences in factors associated with a positive SPT between children/adolescents and adults; (5) there is an attenuation of SPT positivity with older age; (6) and finally there is an increase in positive SPT reactions over the 4-year follow up period, especially in childhood/adolescence.
The overall prevalence of sensitization at baseline to at least one of the allergens tested was 37.6%. Prior reported prevalence rates vary, ranging from 17–69%.10,26 Our results are broadly consistent with those of the Global Allergy and Asthma European Network (GA2LEN), in which the prevalence in participants from Vienna of positive reactions to the allergens tested was higher than in other countries; for example, 46% of the Viennese participants had a sensitization to grass pollen, compared to 26% from the Netherlands and 33% from Germany.27 In our study, peak sensitization occurred at the ages of 10–<15 years in females and 19–<29 years in males. These data are consistent with the National Health and Nutrition Examination Survey, in which peak prevalence was at the age of 12–24 years,5 and with prevalence data from children in Belgium, which peaked at the ages of 10–12 years.6 Increased rates of birth by cesarean delivery, increased use of antibiotics, westernized diet and association with obesity, changes in indoor and outdoor life style and activity patterns owing to modernization are considered to have an important role.28,29
The increase in prevalence and intensity of SPT positivity over the follow-up period is especially interesting. Positive SPT reactions increase by 94 children/adolescents and 66 adults, with overall increase observed in the number of positive SPTs. Although ideally these data should be confirmed by specific immunoglobulin E (IgE) measurements, they potentially indicate the impact of continuous exposure to environmental triggers. The level of serum IgE appears to be associated with the severity of symptoms in participants with allergic rhinitis.30 In a longitudinal study in children studied from birth to 20 years of age, none with a positive SPT at the age of 5 years had a subsequent negative SPT, whereas 23% of those with a negative SPT at the age of 5 years had a positive SPT at 11 years and 19% with a negative SPT at the age of 11 years had a positive SPT at 20 years.20 One explanation for the increase over time not only in allergy but in auto-immunity and other chronic conditions is the epithelial barrier hypothesis.29 The regular follow-up of SPT could potentially be an inexpensive, non-invasive marker of epithelial barrier dysfunction, and to monitor other affected tissues.29 To summarize in our study: we observed an increase of prevalence of sensitization over the 4-year follow-up period and an increase of polysensitization after 4 years in both age groups but especially in children/adolescents.
There was a male predominance of SPT positivity over almost the whole studied age range, except from 10–<15 years. Male sex as a risk factor for sensitization is well described and recognized in the literature,31 but the underlying mechanisms are poorly understood. Sex distributions could be related to an increase in female hormones, especially estrogen, which is known to play an important role in the mechanism of sensitization.32,33 Previous studies reported higher IgE values and eosinophil counts in males than females.34,35 Future research is needed to explore this sex difference and the possible role of hormone homeostasis on Type I sensitization.31,32,36
There is less information on the prevalence of atopy in the older population. The prevalence of any positive SPT at baseline was 55.3% in those aged of 20–29 years and 35.6% in those aged 40–49 years; after a 10-year follow-up period, these values decreased to 40.0% and 23.7%, respectively.10
In both childhood/adolescence and adulthood, house dust mite (22.1% and 19.2%) and grass mix (20.8% and 20.7%) were the most prevalent allergens, confirming previous data.37 The presence of a dog in household showed a negative association with a positive skin prick test in children and adolescents. The role of domiciliary dog and cat exposure at home in terms of sensitization remains controversial. Some studies have reported a decreased risk of sensitization in those who lived with a cat or a dog during their first 5 years of life,4 whereas others did not find any effect of cats or dogs on sensitization levels.16,38 Considering the concept of inflammatory resilience, living conditions linked to environmental micro-organisms early in life seem very important.15,28
Neither smoking habits nor exposure to tobacco smoke were associated with SPT sensitization in children/adolescents, although they were associated with a 10–20% decreased likelihood of a positive SPT in adults. Similarly, there were negative effects of former and current smoking on the likelihood of sensitization only in adults. We tried to avoid confounding factors by differentiating between maternal and parental smoking, and by asking specifically about second-hand smoking. However, the role of smoking and sensitization remains controversial. Paternal smoking during childhood is associated with an increased risk of sensitization in offspring, while maternal smoking is associated with a (non-significant) decreased risk.39,40 Sustained smoking itself is reported to reduce the likelihood of sensitization.11,41 Cross-sectional studies have shown a negative association of current smoking and sensitization,42,43 while others report an increasing risk of sensitization to aero- and/or food allergens,44–46 while yet others did not find any association.47
Blood eosinophil correlated with the likelihood of a positive SPT, especially in childhood/adolescence. A recent study showed a clear association between specific IgE sensitization and an increase eosinophil concentration in an adult Danish population.48 However, more studies are needed to understand the exact mechanism on the impact of blood eosinophilia and SPT positivity.
We found a 27% higher likelihood of a positive SPT in adults with higher SES, but not in children/adolescents. Previous studies reported that the higher the educational status the higher was the likelihood of sensitization.39,49,50 Future studies need to explore whether SES is an indicator of differences in domestic living conditions or exposure to other environmental triggers, particularly in adulthood.
A strength of our study is the population-based recruitment of the participants, representative of the general Austrian population in terms of age, sex, and smoking status over ages ranging from 6 to 82 years. Other strengths are that all tests were conducted in a single center by trained technicians following standardized operating procedures.
One of the limitations is that we tested only for aero-allergens. In addition, no information is available about participants’ housing conditions, domestic living conditions, or exposure to other triggers such as detergents used in laundry,51 dishwashing or other household cleaning agents.29 Due to the high number of measurements and examination within this population based study we had to do the average diameter method, however the scanned area method is theoretically more accurate in determining the SPT wheal area.52 Finally, no information is available on early life sensitization risk factors, such as cesarean delivery, antibiotic use during pregnancy, or early in life, or duration of breastfeeding.
In conclusion, this study confirms that sensitization is highly prevalent in all age groups in this Austrian population cohort, peaking in adolescence but persisting during adulthood, and with determining factors of sensitization differing between childhood/adolescence and adulthood. Importantly, we observed an increase in both the prevalence of sensitization and in the number of positive reactions over the 4-year follow-up period. Longitudinal monitoring of sensitization in children/adolescents particularly will become important to identify environmental triggers related to changes in urbanization, industrialization and lifestyle and contributing to increased allergy related burden of disease.
Highlights
Previous studies stated that prevalence of SPT positivity varies between countries and is more often in males than in females across the life span. Determinants of positive SPT are being investigated, however only in specific subgroups. We found out that the prevalence of sensitization is higher in males than in female in every age group except in 10-<15 years, there is a difference in associated factors between children and adults and that there is an increase in the prevalence of sensitization after 4 years, especially in children and adolescents. The minimal invasive skin prick test may identify a population susceptible to develop asthma and allergy – in particular in childhood and adolescence.
Abbreviations
BMI, body mass index; DEXA, dual energy X‐ray absorptiometry; FFMI, fat-free mass index; FMI, fat mass index; FEV1, forced expiratory volume in 1 second; GLI, Global Lung Initiative; IgE, Immunoglobulin E; LLN, lower limit of normal; LEAD, Lung, hEart, sociAl, body; mm, millimeter; OR, odds ratio; SPT, skin prick test; SES, socioeconomic status.
Acknowledgments
The Authors thank all participants for their willingness to contribute to advanced medical science in the field of epidemiology, lung function development and decline. Special thanks to the whole LEAD study team, who worked every day for the high quality of the data obtained.
Funding
The Austrian LEAD Study is supported by the Ludwig Boltzmann Society, the Municipal Department of Health and Environment of Vienna, the Federal State Governmental Department of Health of Lower Austria, and unrestricted scientific grants from AstraZeneca, Böhringer Ingelheim, Chiesi Pharma, Glaxo Smith Kline, Menarini Pharma, MSD, Novartis Pharma, Vivisol Health Care and Air liquide Company. None of the supporting parties had any participation in the data, nor did they contribute to the design or the content of the present manuscript.
Disclosure
Prof. Dr. Sylvia Hartl reports grants from GSK, Roche, Menarini, Böhringer, Astra Zeneca, MSD, Sanofi, and Novartis for advisory board members and speakers honorarium. Prof. Dr. Wolfgang Pohl reports grants and/or personal fees from Meda, Novartis, Roche, Sanova, Astra Zeneca, Boehringer Ingelheim, Chiesi, GSK, and MedImmune, outside the submitted work. The authors declare that they have no other conflicts of interest in this work.
References
1. Janson C, Anto J, Burney P, et al. The European community respiratory health survey: what are the main results so far? Eur Respir J. 2001;18(3):598–611. doi:10.1183/09031936.01.00205801
2. Dor-Wojnarowska A, Liebhart J, Miecielica J, et al. The Impact of Sex and Age on the Prevalence of Clinically Relevant Sensitization and Asymptomatic Sensitization in the General Population. Arch Immunol Ther Exp (Warsz). 2017;65(3):253–261. doi:10.1007/s00005-016-0425-7
3. Kupryś-Liphińka I, Elgalal A, Kuna P. Skin prick test with inhaled allergens in the general population of Lodz province. Pneumonol Alergol Pol. 2009;1:634.
4. Bjerg A, Ekerljung L, Eriksson J, et al. Increase in pollen sensitization in Swedish adults and protective effect of keeping animals in childhood. Clin Exp Allergy. 2016;46(10):1328–1336. doi:10.1111/cea.12757
5. Gergen PJ, Turkeltaub PC, Kovar MG. The prevalence of allergic skin test reactivity to eight common aeroallergens in the U.S. population: results from the second National Health and Nutrition Examination Survey. J Allergy Clin Immunol. 1987;80(5):669–679. doi:10.1016/0091-6749(87)90286-7
6. Govaere E, Gysel D, Massa G, Verhamme KMC, Doli E, De BF. The influence of age and gender on sensitization to aero-allergens. Pediatr Allergy Immunol. 2007;18(8):671–678. doi:10.1111/j.1399-3038.2007.00570.x
7. Sears MR, Burrows B, Flannery EM, Herbison GP, Holdaway MD. Atopy in childhood. I. Gender and allergen related risks for development of hay fever and asthma. Clin Exp Allergy. 1993;1:6537. doi:10.1111/j.1365-2222.1993.tb00279.x
8. Blomme K, Tomassen P, Lapeere H, et al. Prevalence of allergic sensitization versus allergic rhinitis symptoms in an unselected population. Int Arch Allergy Immunol. 2013;160(2):200–207. doi:10.1159/000339853
9. Boulet LP, Turcotte H, Laprise C, et al. Comparative degree and type of sensitization to common indoor and outdoor allergens in subjects with allergic rhinitis and/or asthma. Clin Exp Allergy. 1997;27(1):52–59. doi:10.1111/j.1365-2222.1997.tb00672.x
10. Warm K, Backman H, Lindberg A, Lundbäck B, Rönmark E. Low incidence and high remission of allergic sensitization among adults. J Allergy Clin Immunol. 2012;129(1):1. doi:10.1016/j.jaci.2011.08.033
11. Dirksen A, Nielsen NH, Madsen F, Frølund L, Dirksen A, Jørgensen T. Smoking and the development of allergic sensitization to aeroallergens in adults: a prospective population-based study. The Copenhagen Allergy Study. Allergy Eur J Allergy Clin Immunol. 2001;107(6):977–984. doi:10.1034/j.1398-9995.2000.00509.x-i1
12. Goel N, Singh BP, Arora N, Kumar R. Effect of smoking on atopic predisposition and sensitisation to allergens. Indian J Chest Dis Allied Sci. 2008;50(4):329–333.
13. Govaere E, Van Gysel D, Verhamme KMC, Doli E, De Baets F. The association of allergic symptoms with sensitization to inhalant allergens in childhood. Pediatr Allergy Immunol. 2009;20(5):448–457. doi:10.1111/j.1399-3038.2008.00805.x
14. Nickel R, Lau S, Niggemann B, et al. Messages from the German Multicentre Allergy Study. Pediatr Allergy Immunol Suppl. 2002;13:7–10. doi:10.1034/j.1399-3038.13.s.15.4.x
15. Mikkelsen S, Dinh KM, Boldsen JK, et al. Combinations of self‐reported rhinitis, conjunctivitis, and asthma predicts IgE sensitization in more than 25,000 Danes. Clin Transl Allergy. 2021;11:1. doi:10.1002/clt2.12013
16. Arshad SH, Tariq SM, Matthews S, Hakim E. Sensitization to common allergens and its association with allergic disorders at age 4 years: a whole population birth cohort study. Pediatrics. 2001;108(2):e33–e33. doi:10.1542/peds.108.2.e33
17. Owens L, Laing I, Zhang G, Le Souef P. Early sensitization is associated with reduced lung function from birth into adulthood. J Allergy Clin Immunol. 2016;137(5):1605–1607.e2. doi:10.1016/j.jaci.2015.10.030
18. Alford SH, Zoratti E, Peterson EL, Maliarik M, Ownby DR, Johnson CC. Parental history of atopic disease: disease pattern and risk of pediatric atopy in offspring. J Allergy Clin Immunol. 2004;114:5. doi:10.1016/j.jaci.2004.08.036
19. Schoos AMM, Bønnelykke K, Chawes BL, Stokholm J, Bisgaard H, Kristensen B. Precision allergy: separate allergies to male and female dogs. J Allergy Clin Immunol Pract. 2017;5:6. doi:10.1016/j.jaip.2017.03.028
20. Pesonen M, Kallio MJT, Siimes MA, Ranki A. Allergen skin prick testing in early childhood: reproducibility and prediction of allergic symptoms into early adulthood. J Pediatr. 2015;166(2):401–406.e1. doi:10.1016/j.jpeds.2014.10.009
21. Breyer-Kohansal R, Hartl S, Burghuber OC, et al. The LEAD (Lung, Heart, Social, Body) Study: objectives, Methodology, and External Validity of the Population-Based Cohort Study. J Epidemiol. 2019;29(8):315–324. doi:10.2188/jea.je20180039
22. Ruëff F, Bergmann K-C, Brockow K, et al. Hauttests zur Diagnostik von allergischen Soforttypreaktionen. Allergologie. 2011;34(04):212–228. doi:10.5414/alp34212
23. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
24. Guillien A, Soumagne T, Regnard J, Degano B. The new reference equations of the Global Lung function Initiative (GLI) for pulmonary function tests. Rev Mal Respir. 2018;35:10. doi:10.1016/j.rmr.2018.08.021
25. Quanjer PH, Stanojevic S, Cole TJ, et al. Multi-ethnic reference values for spirometry for the 3-95-yr age range: the global lung function 2012 equations. Eur Respir J. 2012;40(6):1324–1343. doi:10.1183/09031936.00080312
26. Bousquet PJ, Chinn S, Janson C, Kogevinas M, Burney P, Jarvis D. Geographical variation in the prevalence of positive skin tests to environmental aeroallergens in the European Community Respiratory Health Survey I. Allergy Eur J Allergy Clin Immunol. 2007;62(3):301–309. doi:10.1111/j.1398-9995.2006.01293.x
27. Heinzerling L, Frew AJ, Bindslev-Jensen C, et al. Standard skin prick testing and sensitization to inhalant allergens across Europe - A survey from the GA2LEN network. Allergy Eur J Allergy Clin Immunol. 2005;60(10):1287–1300. doi:10.1111/j.1398-9995.2005.00895.x
28. Renz H, Skevaki C. Early life microbial exposures and allergy risks: opportunities for prevention. Nat Rev Immunol. 2021;21:3. doi:10.1038/s41577-020-00420-y
29. Akdis CA. Does the epithelial barrier hypothesis explain the increase in allergy, autoimmunity and other chronic conditions? Nat Rev Immunol. 2021;21(11):739–751. doi:10.1038/s41577-021-00538-7
30. Corsico AG, De Amici M, Ronzoni V, et al. Allergen-Specific Immunoglobulin E and Allergic Rhinitis Severity. Allergy Rhinol. 2017;8:1. doi:10.2500/ar.2017.8.0187
31. Arruda LK, Solé D, Baena-Cagnani CE, Naspitz CK. Risk factors for asthma and atopy. Curr Opin Allergy Clin Immunol. 2005;5(2):153–159. doi:10.1097/01.all.0000162308.89857.6c
32. Cutolo M, Sulli A, Capellino S, et al. Sex hormones influence on the immune system: basic and clinical aspects in autoimmunity. Lupus. 2004;13(9):635–638. doi:10.1191/0961203304lu1094oa
33. Narita SI, Goldblum RM, Watson CS, et al. Environmental estrogens induce mast cell degranulation and enhance IgE-mediated release of allergic mediators. Environ Health Perspect. 2007;115(1):48–52. doi:10.1289/ehp.9378
34. Omenaas E, Bakke P, Elsayed S, Hanoa R, Gulsvik A. Total and specific serum IgE levels in adults: relationship to sex, age and environmental factors. Clin Exp Allergy. 1994;24(6):530–539. doi:10.1111/j.1365-2222.1994.tb00950.x
35. Hartl S, Breyer MK, Burghuber OC, et al. Blood eosinophil count in the general population: typical values and potential confounders. Eur Respir J. 2020;55(5):1901874. doi:10.1183/13993003.01874-2019
36. Malkin CJ, Pugh PJ, Jones RD, Jones TH, Channer KS. Testosterone as a protective factor against atherosclerosis - Immunomodulation and influence upon plaque development and stability. J Endocrinol. 2003;178(3):373–380. doi:10.1677/joe.0.1780373
37. Heinzerling LM, Burbach GJ, Edenharter G, et al. GA 2 LEN skin test study I: GA²LEN harmonization of skin prick testing: novel sensitization patterns for inhalant allergens in Europe. Allergy Eur J Allergy Clin Immunol. 2009;64(10):1498–1506. doi:10.1111/j.1398-9995.2009.02093.x
38. Lowe LA, Woodcock A, Murray CS, Morris J, Simpson A, Custovic A. Lung function at age 3 years: effect of pet ownership and exposure to indoor allergens. Arch Pediatr Adolesc Med. 2004;158(10):996. doi:10.1001/archpedi.158.10.996
39. Forastiere F, Agabiti N, Corbo GM, et al. Socioeconomic status, number of siblings, and respiratory infections in early life as determinants of atopy in children. Epidemiology. 1997;8(5):566. doi:10.1097/00001648-199709000-00015
40. Larsson ML, Magnuson A, Montgomery SM. Parental smoking and allergic sensitization in offspring defined by skin prick testing. Pediatr Allergy Immunol. 2005;16(5):449–452. doi:10.1111/j.1399-3038.2005.00247.x
41. Barbee RA, Kaltenborn W, Lebowitz MD, Burrows B. Longitudinal changes in allergen skin test reactivity in a community population sample. J Allergy Clin Immunol. 1987;79:1. doi:10.1016/S0091-6749(87
42. Baldacci S, Modena P, Carrozzi L, et al. Skin prick test reactivity to common aeroallergens in relation to total IgE, respiratory symptoms, and smoking in a general population sample of northern Italy. Allergy Eur J Allergy Clin Immunol. 1996;51(3):149–156. doi:10.1111/j.1398-9995.1996.tb04579.x
43. Mensinga TT, Schouten JP, Rijcken B, Weiss ST, Speizer FE. The relationship of eosinophilia and positive skin test reactivity to respiratory symptom prevalence in a community-based population study. J Allergy Clin Immunol. 1990;86(1):99–107. doi:10.1016/S0091-6749(05)80129-0
44. Havstad SL, Johnson CC, Zoratti EM, et al. Tobacco smoke exposure and allergic sensitization in children: a propensity score analysis. Respirology. 2012;17(7):1068–1072. doi:10.1111/j.1440-1843.2012.02201.x
45. Keil T, Lau S, Roll S, et al. Maternal smoking increases risk of allergic sensitization and wheezing only in children with allergic predisposition: longitudinal analysis from birth to 10 years. Allergy Eur J Allergy Clin Immunol. 2009;64(3):445–451. doi:10.1111/j.1398-9995.2008.01867.x
46. Lannerö E, Wickman M, Van Hage M, Bergström A, Pershagen G, Nordvall L. Exposure to environmental tobacco smoke and sensitisation in children. Thorax. 2008;63(2):172–176. doi:10.1136/thx.2007.079053
47. Ciaccio CE, Gentile D. Effects of tobacco smoke exposure in childhood on atopic diseases. Curr Allergy Asthma Rep. 2013;13(6):687–692. doi:10.1007/s11882-013-0389-1
48. Mikkelsen S, Boldsen JK, Møller BK, et al. Atopic respiratory diseases and IgE sensitization are associated with leukocyte subset concentrations in 14,440 blood donors. Clin Chim Acta. 2021;520:139–146. doi:10.1016/j.cca.2021.06.015
49. Kuyucu S, Saraçlar Y, Tuncer A, et al. Determinants of atopic sensitization in Turkish school children: effects of pre- and post-natal events and maternal atopy. Pediatr Allergy Immunol. 2004;15(1):62–71. doi:10.1046/j.0905-6157.2003.00115.x
50. Schäfer T, Ruhdorfer S, Weigl L, et al. School education and allergic sensitization in adults. Allergy Eur J Allergy Clin Immunol. 2001;56(12):1206–1210. doi:10.1034/j.1398-9995.2001.00208.x
51. Wang M, Tan G, Eljaszewicz A, et al. Laundry detergents and detergent residue after rinsing directly disrupt tight junction barrier integrity in human bronchial epithelial cells. J Allergy Clin Immunol. 2019;143:5. doi:10.1016/j.jaci.2018.11.016
52. Van Der Valk JPM, Gerth Van Wijk R, Hoorn E. Measurement and interpretation of skin prick test results. Clin Transl Allergy. 2016;6(1). doi:10.1186/s13601-016-0092-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.