Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Adverse Event Management in Patients with Platinum-Resistant Ovarian Cancer Treated with Niraparib and Anlotinib: Updates from the Phase II, Multi-Center ANNIE Study
Authors Deng T, Yan L, Li J ![]() , Liu G
, Liu G ![]() , Yin A, Feng Y, Zheng M, Zhang C, Huang H, Huang Q, Lin A, Jiang J
, Yin A, Feng Y, Zheng M, Zhang C, Huang H, Huang Q, Lin A, Jiang J ![]() , Kong B, Liu J
, Kong B, Liu J
Received 31 March 2025
Accepted for publication 23 June 2025
Published 21 July 2025 Volume 2025:21 Pages 1135—1147
DOI https://doi.org/10.2147/TCRM.S526755
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Ting Deng,1,* Lei Yan,2,* Jing Li,1 Guochen Liu,1 Aijun Yin,3 Yanling Feng,1 Min Zheng,1 Chuyao Zhang,1 He Huang,1 Qidan Huang,1 An Lin,4 Jie Jiang,3 Beihua Kong,3 Jihong Liu1,*
1Department of Gynecological Oncology, Sun Yat-Sen University Cancer Center, State Key Laboratory of Oncology in South China, Guangzhou, People’s Republic of China; 2Department of Health Management Center, The First Affiliated Hospital of Jinan University, The First Clinical Medical College of Jinan University, Guangzhou, People’s Republic of China; 3Department of Obstetrics and Gynecology, Qilu Hospital of Shandong University, Jinan, People’s Republic of China; 4Department of Gynecology, Fujian Provincial Cancer Hospital, Fuzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jihong Liu, Department of Gynecological Oncology, Sun Yat-Sen University Cancer Center, 651 Dong Feng Road East, Guangzhou, 510060, People’s Republic of China, Tel +86-020-87341615, Email [email protected]
Background: The primary analysis of the ANNIE study demonstrated promising anti-tumor activity of the niraparib–anlotinib combination in platinum-resistant recurrent ovarian cancer (PROC). We report updated overall survival (OS) and safety data and the management of key treatment-emergent adverse event (TEAE) from the ANNIE study.
Methods: In the multi-center, single-arm, Phase 2 ANNIE study, enrolled patients received oral niraparib 200 mg or 300 mg (baseline bodyweight-directed) once daily and anlotinib 10 mg (12 mg before protocol amendment) once daily on days 1– 14 of each 21-day cycle. Safety management involved a multidisciplinary team comprising specialist physicians, who performed monitoring and intervention for key comorbidities and TEAEs.
Results: Forty patients were enrolled. After a median follow-up of 19.0 months, the updated median OS was 18.2 months (95% confidence interval: 12.1–not evaluable). The most common TEAEs were hypertension (n=22, 55%), leukopenia (n=18, 45%), hand-foot syndrome (n=17, 43%), thrombocytopenia (n=15, 38%), neutropenia (n=14, 35%), and hypertriglyceridemia (n=12, 30%). Hypertension and cardiovascular events were mostly managed by early interventions using beta-blockers. Hypertriglyceridemia was mostly managed using atorvastatin and simvastatin. Hematological toxicities were consistent with prior studies and no severe hematologic events occurred. Protocol amendment was implemented to reduce the incidence of hand-foot syndrome, while topical glucocorticoids and non-steroidal anti-inflammatory drugs were used in patients with apparent symptoms.
Conclusion: The updated OS analysis showed sustained long-term efficacy of niraparib-anlotinib in PROC patients. The safety data reflected satisfactory tolerability and adverse event management, supporting the involvement of a multidisciplinary disease management team in ovarian cancer care.
Clinical Trial Registration: NCT04376073.
Plain Language Summary: Platinum-resistant recurrent ovarian cancer patients face limited treatment options. This study evaluated the efficacy and safety of combining niraparib (a PARP inhibitor) and anlotinib (an anti-angiogenic drug). Results showed the combination significantly prolonged overall survival, offering new hope to patients. A multidisciplinary approach controlled key side effects: beta-blockers stabilized blood pressure/heart rate, while lipid-lowering therapy-maintained cholesterol/triglyceride levels. Hematological adverse events matched those from prior single-drug studies, with no new safety concerns. This therapy is effective and safely manageable via multidisciplinary collaboration, providing clinicians a model to improve patient outcomes and quality of life.
Keywords: ovarian cancer, niraparib, anlotinib, long-term safety, multidisciplinary management
Introduction
Ovarian cancer patients face a high burden of chronic and metabolic diseases, such as hypertension and dyslipidemia, the prevalence of which can be as high as 50%–70%.1 Over 75% of ovarian cancer patients are of middle or older age, intrinsically susceptible to various chronic conditions.2–5 It is important to note that 90% of ovarian cancers are epithelial in origin, encompassing diverse histologic types (eg, high-grade serous, endometrioid) with distinct molecular alterations, clinical manifestations, and treatment responses. The remaining 10% are non-epithelial tumors, primarily including germ cell tumors (the most common ovarian neoplasms in women under 30 years, with 60–70% diagnosed at early stages), sex cord-stromal tumors, and rare entities such as small cell carcinomas.6 High levels of distress due to fear of disease recurrence can increase ovarian cancer patients’ psychological burden and cardiovascular risks.7–9 Ovarian cancer treatment can also cause cardiovascular and metabolic adverse events. The standard treatment of surgical debulking induces abrupt hormonal imbalance and leads to elevated cardiovascular risks.10 Common cancer therapies, including alkylating agents (chemotherapy) and antiangiogenic agents (biological therapy), are often accompanied by vascular toxicities.2,11,12 For ovarian cancer, most patients receive adjuvant chemotherapy, while selected individuals may undergo three or more cycles of neoadjuvant chemotherapy (NACT) before debulking surgery. Notably, NACT allows for upfront assessment of chemosensitivity and identification of patients at heightened relapse risk.13 Unfortunately, gynecologic oncologists often do not have sufficient knowledge or resources to attend to non-oncologic comorbid conditions and/or adverse events, leaving patients to seek care independently from other specialist departments. Such a fragmented approach would adversely affect patients’ quality of life and treatment adherence. In response, we endeavored to incorporate a comprehensive treatment-emergent adverse events (TEAE) management model into a recent clinical trial we conducted, where an elevated safety management need was anticipated during the study design.
The multi-center, single-arm, phase 2 ANNIE trial (NCT04376073) evaluated the novel combination of niraparib and anlotinib in patients with platinum-resistant recurrent ovarian cancer (PROC), and the primary analysis results have been reported previously.14 For this patient population with outstanding needs for more efficacious and better tolerated treatment options, niraparib and anlotinib were chosen on the basis of their single-agent antitumor activities in platinum-resistant or recurrent diseases and their potential synergy, and indeed the primary analysis of ANNIE showed considerable clinical benefits with an overall response rate (ORR) of 50.0% (20/40; 95% confidence interval [CI]: 33.8%–66.2%).14 However, it had been noted that cardiovascular and metabolic abnormalities were among the commonly reported TEAEs for both niraparib and anlotinib in their respective clinical trials.15,16 Niraparib could lead to hypertension and palpitations in approximately 17%–19% and 10%–15% of patients,15 respectively, due to effects on dopamine, norepinephrine, and serotonin metabolism.17 Anlotinib could cause hypertension in up to 68% of patients,16 possibly by reducing nitric oxide production and inducing elevation in vasoconstrictor endothelin-1, among other potential mechanisms for vascular endothelial growth factor receptor (VEGFR) inhibitor-induced hypertension.16,18,19
Considering the known TEAE profiles of the study drugs and the patient population’s propensity for cardiovascular and metabolic comorbidities, the ANNIE study made provision for potentially heightened TEAE management needs by incorporating a multidisciplinary comorbidity/TEAE management team, with the hope of pilot-testing the effectiveness of more holistic patient management in ovarian cancer. In this updated analysis, we hypothesize that the niraparib–anlotinib combination extends survival in platinum-resistant ovarian cancer through synergistic inhibition of vascular endothelial growth factor (VEGF) and poly (ADP-ribose) polymerase (PARP), while a multidisciplinary adverse event management model optimizes treatment tolerability. These findings aim to validate the long-term efficacy and safety of this novel regimen and provide a practical care model for integrating comprehensive toxicity management into clinical practice.
Materials and Methods
Study Design
This study was a multi-center, single-arm, phase 2 trial (NCT04376073) to evaluate the efficacy and safety of the niraparib–anlotinib combination in patients with PROC. The full methodologic details have been published previously.14 Briefly, eligible patients were 18 to 70 years old with histologically confirmed ovarian epithelial, fallopian tube, or primary peritoneal cancer that recurred within six months of the last platinum-based therapy, regardless of their biomarker status. Patients who previously received antiangiogenic treatment were eligible, whereas patients previously exposed to poly (ADP-ribose) polymerase (PARP) inhibitors were excluded.
The study was conducted in adherence to the Declaration of Helsinki, Good Clinical Practice, and all local legal and regulatory requirements. This study has been approved by the Ethics Committees of the Sun Yat-Sen University Cancer Center, Qilu Hospital of Shandong University, and Fujian Provincial Cancer Hospital. All patients provided written and informed consent before enrollment.
Procedure
The full details of the study procedure were described in the primary analysis.14 Eligible patients received oral niraparib plus anlotinib in successive 21-day cycles until disease progression or intolerable toxicities. Anlotinib was administered on days 1–14 of each cycle at 10 mg (12 mg before the protocol amendment on November 25, 2020) once a day (QD). Niraparib was administered at 300 mg QD (if baseline bodyweight ≥77kg) or 200 mg QD (if baseline bodyweight <77kg). Dose reductions and interruptions of niraparib and/or anlotinib were permitted for the management of adverse events, the details of which are provided in the protocol. Patients with dose interruptions longer than 28 days were discontinued from the study.
Tumor assessments were conducted at baseline and once every three cycles thereafter by computed tomography or magnetic resonance imaging. Complete blood count (CBC) test was conducted weekly during treatment cycle 1 and at least once a month thereafter. Blood biochemistry, blood lipids, and thyroid hormone levels were closely monitored at each follow-up, and interventions were implemented when appropriate. An additional follow-up had been conducted since the completion of the primary analysis, whereby the survival status and event time were updated for some of the censored patients in the primary analysis.
Multidisciplinary TEAE Management Team
Team Design
Considering the known adverse event profiles of niraparib and anlotinib and the patient population’s susceptibility to multiple chronic comorbidities, complex management needs were anticipated with respect to TEAEs and comorbidities. A multidisciplinary team (MDT) was established to alleviate the impact of TEAEs, to reduce treatment interruptions or discontinuations and, in turn, prolong patients’ effective treatment durations. The MDT included gynecologic oncologists, cardiologists and radiologists, with an endocrinologist and a psychologist engaged as clinical consultants when necessary. Training was provided before study initiation to all MDT members to ensure seamless collaboration. Study cardiologists were introduced to background knowledge of ovarian cancer and, after learning about the pharmacological and toxicological profiles of niraparib and anlotinib, recommended the appropriate classes of medications for managing cardiovascular TEAEs.
Baseline Assessment
During the screening period, medical history information was collected from all patients, including 1) ovarian cancer-related information, such as radiology records, treatment history, and relevant biomarker status; 2) medical records of common chronic comorbidities, such as cardiovascular, metabolic, and neurological conditions and the associated medications. Examinations of CBC, blood biochemistry, liver and kidney functions, thyroid functions, and electrocardiogram were performed.
The MDT assessed patients’ medical history and baseline examination results to identify patients with comorbidities or abnormalities but otherwise meeting the eligibility criteria. Comorbidity medications were evaluated by the internists for compatibility with the study drugs and adjusted in the case of potential drug–drug interactions. Patients whose comorbidity medications could not be adjusted satisfactorily before the end of the screening period were excluded.
Integrated TEAE Monitoring and Early Intervention
For all enrolled patients, an integrated TEAE management strategy was employed, where continuous self-monitoring, regular on-site follow-up, and as-needed remote management were coordinated via a WeChat group comprising a study assistant, internists, gynecologic oncologists, and radiologists. In accordance with cardiovascular disease management guidelines,20 patients were trained to self-monitor and record daily blood pressure and heart rates in the morning and before bedtime. During the on-site follow-up conducted once every cycle, patients were required to submit the self-monitoring records to the study assistant, who then circulated these records to the WeChat group for internist’s inspection, along with patients’ blood biochemistry results from the on-site follow-up. If patients sought consultation and undertook any medical examination at third-party institutions during the study, they were urged to report to the study assistant, who collated and sent the third-party test results to the WeChat group.
Within the WeChat group, the MDT comprehensively evaluated the information from the abovementioned sources. For any signs of abnormality identified, the oncologist investigators were promptly alerted, the internists provided specialist input for intervention, and cases of serious concern were escalated for the attention of the sub-principal investigator. Particularly, if an elevating trend was detected in the daily blood pressure or heart rate records, even if not yet reaching the thresholds for clinical diagnosis of hypertension (defined as systolic blood pressure ≥140 mmHg and diastolic blood pressure ≥90 mmHg at two or more post-baseline timepoints) or tachycardia (defined as ≥100 beats per minute), early intervention with appropriate medications was implemented as per the internist’s instruction.
For patients residing outside the cities of the investigation centers and especially during the coronavirus disease 2019 (COVID-19) pandemic, telemedicine and remote management were provided to enable them to obtain TEAE management medications from local pharmacies. Nonetheless, face-to-face follow-ups at the investigation centers in addition to the scheduled study visits were arranged where necessary and feasible to facilitate TEAE management.
Outcomes and Statistical Analysis
The key efficacy endpoint in this analysis was the updated OS in intention-to-treat (ITT) population (all patients who received at least one dose of study medication). Safety endpoints included the updated incidence, severity, and management of TEAEs in the ITT population.
OS and two-sided 95% CI were estimated using the Kaplan–Meier method. Adverse events were graded using the Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. The safety results were summarized by numbers and percentages of patients. Statistical analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC, USA).
Results
Patient Disposition and Baseline Characteristics
Between May 22, 2020, and April 22, 2021, 69 patients were screened and 40 patients were enrolled. The median duration of follow-up was 19.0 months. By data cut-off (July 10, 2022), one patient was still on treatment. Among the 39 patients who discontinued treatment, 27 were due to disease progression, five due to adverse events, six due to patient request, and one due to protocol violation (received chemotherapy).
Baseline demographics and characteristics have been reported previously (Table 1).14 The median age was 54 years (range 37—69 years). The predominant tumor pathology was high-grade serous carcinoma (n=34, 85%). Most patients were diagnosed with stage III (n=31, 78%) or IV (n=6, 15%) diseases. Twenty-seven (68%) patients received prior antiangiogenic treatments. Five (13%) patients carried germline BRCA mutations.
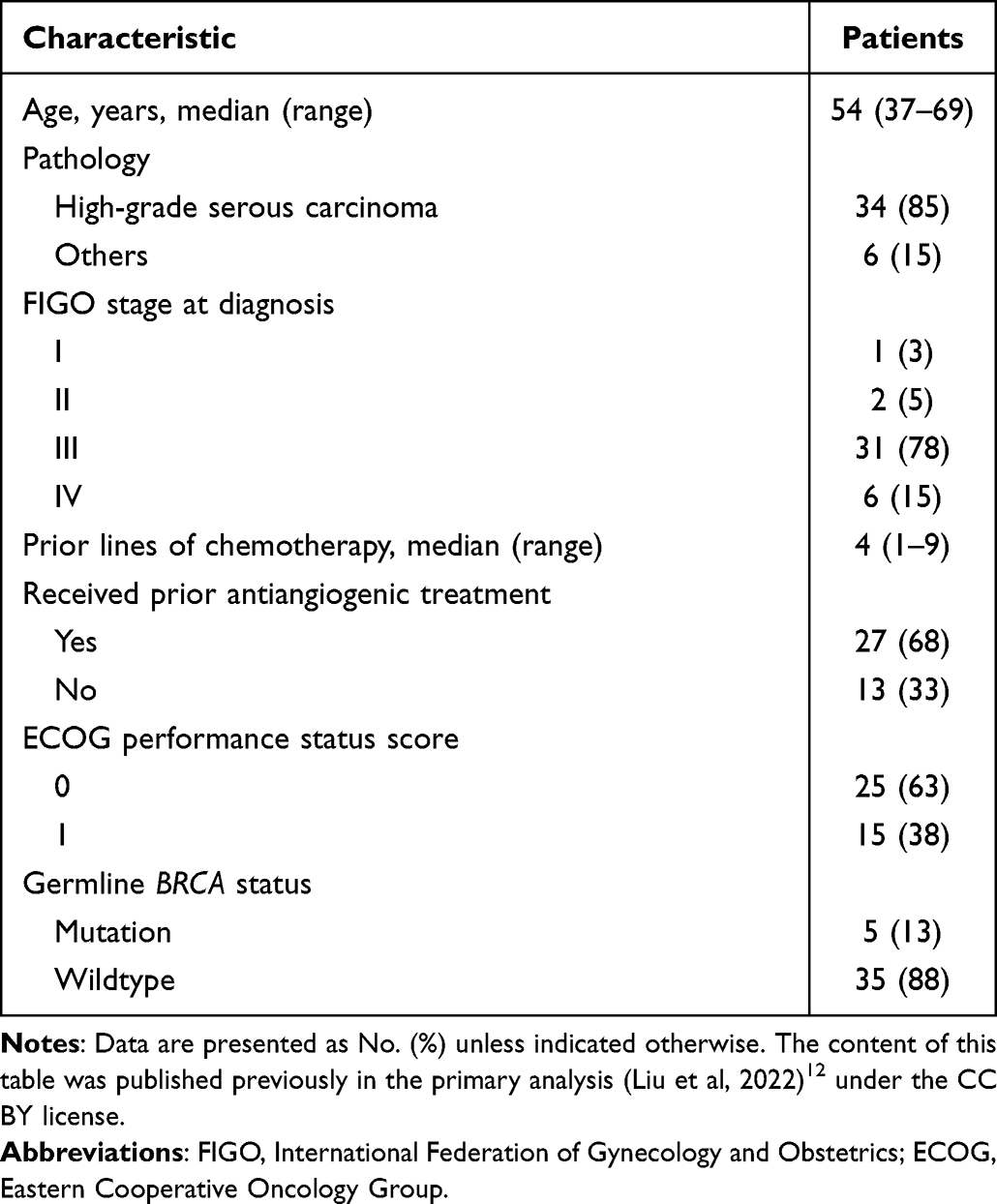 |
Table 1 Demographic and Baseline Clinical Characteristics (N=40) |
Efficacy Update
By data cut-off, 18 deaths had occurred and the final OS analysis yielded a median OS of 18.2 months (95% CI: 12.1–not evaluable) (Figure 1).
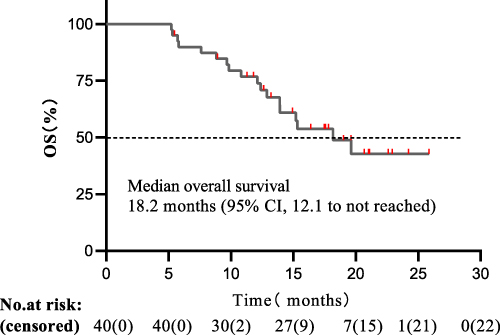 |
Figure 1 Kaplan–Meier curve for final overall survival (intention-to-treat population). Abbreviation: OS, overall survival. |
Overall Safety Update
All 40 patients received at least one dose of study drug and were included for the safety analysis. The most common TEAEs of any grade were hypertension (n=22, 55%), leukopenia (n=18, 45%), hand-foot syndrome (n=17, 43%), thrombocytopenia (n=15, 38%), neutropenia (n=14, 35%), and hypertriglyceridemia (n=12, 30%) (Table 2). Drug-related TEAEs of grade ≥3 occurring in more than one patient were neutropenia (n=7, 18%), hand-foot syndrome (n=6, 15%), anemia (n=5, 13%), hypertension (n=5, 13%), thrombocytopenia (n=4, 10%), leukopenia (n=4, 10%), hypertriglyceridemia (n=3, 8%), and intestinal obstruction (n=3, 8%). No drug-related death or myelodysplastic syndrome was reported. Patients’ on-study worst-state Eastern Cooperative Oncology Group (ECOG) performance scores showed a similar distribution to that at baseline (Supplementary Table S1), with majority of patients scoring 0 (69.4% at baseline, 77.8% at worst-state).
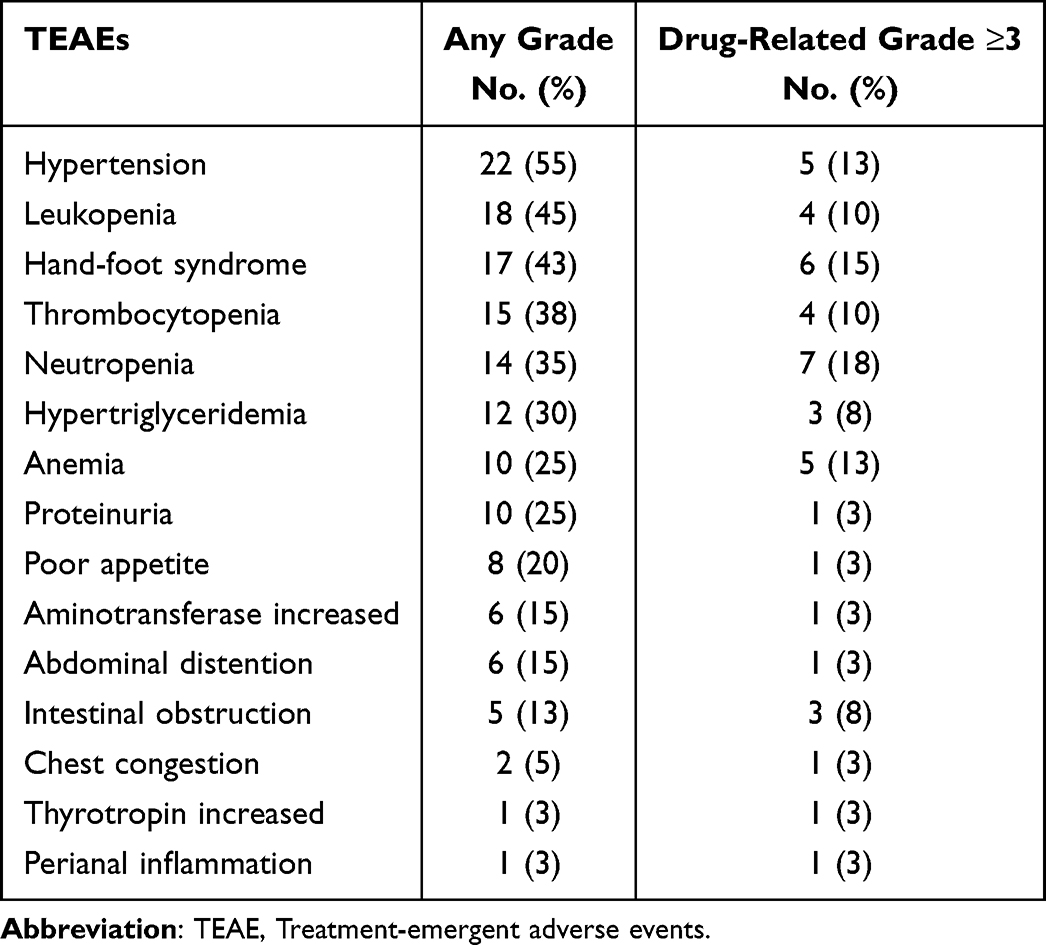 |
Table 2 Summary of TEAEs (N=40) |
Dose modification and treatment discontinuation due to TEAEs were analyzed for niraparib and anlotinib. Niraparib dose reductions occurred in 19 (48%) patients (median time to first dose reduction: 6.29 weeks), among whom 14 were able to revert to the original dose after a median duration of 5.29 weeks. Twenty-one (53%) patients experienced niraparib dose interruptions (median time to first dose interruption: 5.29 weeks), and 16 patients resumed niraparib treatment after a median of 3.36 weeks. Of the 21 (53%) patients receiving anlotinib dose reductions (median time to first dose reduction: 9.29 weeks), five reverted to the original dose after a median of three weeks. Fourteen patients had anlotinib dose interruptions (median time to first dose interruption: 7.43 weeks), and ten resumed anlotinib treatment after a median of two weeks. Eleven and six patients experienced TEAE-driven dose reductions and interruptions, respectively, for both drugs. Five patients discontinued treatment due to TEAE, with two patients discontinuing both drugs, one patient discontinuing niraparib only and two patients discontinuing anlotinib only.
Characteristics and Management of Hypertension and Other Cardiovascular Events
At baseline, 15 patients had pre-existing hypertension, and all were under medical control by study cardiologists. Treatment-emergent clinical hypertension events occurred in 22 (55%) patients. Daily blood pressure surveillance data of all 40 patients showed that during the course of study treatment patients’ average systolic and diastolic blood pressure increased from baseline but remained within the upper limit of the normal ranges (Figure 2). Table 3 summarizes the distribution of patients’ post-baseline worst-state blood pressure and heart rate data. In total, 29 (73%) patients had a worst-state systolic blood pressure of ≥140 mmHg, and 39 (98%) patients had a worst-state diastolic blood pressure of ≥90 mmHg.
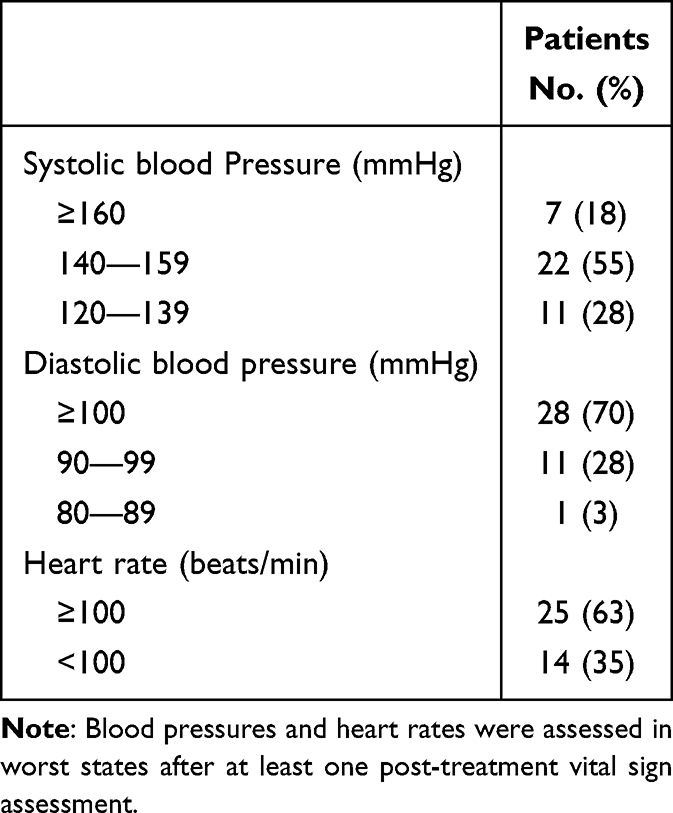 |
Table 3 Post-Baseline Worst-State Blood Pressure and Heart Rate (N=40) |
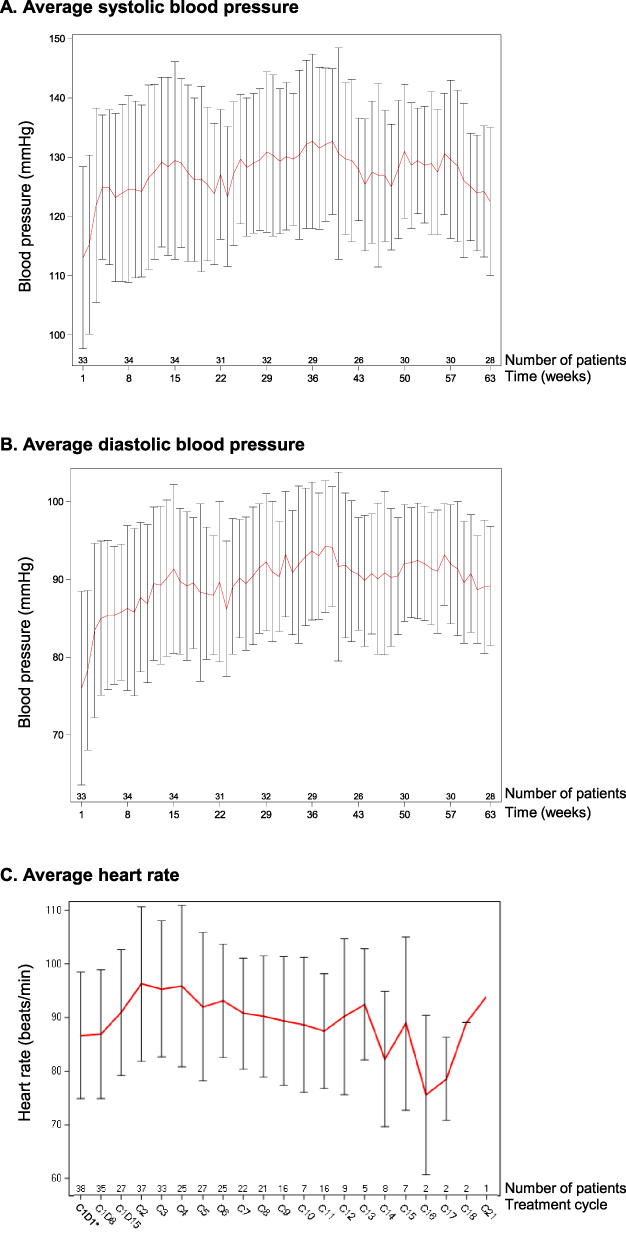 |
Figure 2 Average blood pressure and heart rate over time in the intention-to-treat population. (A) Average systolic blood pressure, (B) Average diastolic blood pressure, (C) Average heart rate, *For some patients, the data used was from the screening period. |
As partly reflected in the worst-state data, the increase in blood pressure experienced by patients was characterized by high diastolic blood pressure and accompanying increase in heart rate (see below for detailed heart rate data). Beta-blockers (metoprolol or bisoprolol) were the main antihypertensive used, which would simultaneously control the heart rate. If beta-blockers alone were ineffective, a combination antihypertensive regimen was administered, in most cases by adding calcium channel blockers (CCB) (amlodipine/levamlodipine/nifedipine, etc.) or angiotensin receptor blockers (ARB) (valsartan/irbesartan). Eight patients required only one antihypertensive (beta-blockers: n=6; ARB: n=2). Eight patients required dual therapy, including seven patients receiving beta-blockers plus CCB/ARB or angiotensin-converting enzyme inhibitors (ACEI) and one patient receiving ARB plus CCB. Five patients required triple therapy or beyond (beta-blockers, CCB, and ARB/diuretics) to regulate their blood pressure.
Patients’ average heart rate increased by approximately 10 beats per minute (bpm) from baseline during the first three treatment cycles, plateaued for subsequent cycles, and remained within the normal range throughout the study (Figure 2). Twenty-five patients (63%) had a worst-state heart rate of ≥100 bpm. Twenty-five patients (63%) experienced sinus tachycardia, all of which were of grade 1–2 and required no urgent medical attention. Starting from cycle 1, 18 patients received beta-blockers for heart rate control. No clinical symptoms were recorded due to tachycardia.
Dyslipidemia and Management with Immediate Lipid-Lowering Therapy
Of the 12 patients experiencing hypertriglyceridemia, 21 recurrent triglyceride elevation events were recorded, and three patients had drug-related grade ≥3 hypertriglyceridemia. Increased cholesterol level (all of which was grade 1–2) was observed in five patients, three of whom also experienced hypertriglyceridemia. Ten patients received immediate lipid-lowering medications, mostly using atorvastatin and simvastatin. One patient experiencing grade ≥3 hypertriglyceridemia received fenofibrate.
Hematologic Toxicities Consistent with Prior Studies
Consistent with previous reports, the most common hematological toxicities were leukopenia (n=18, 45%), thrombocytopenia (n=15, 38%), neutropenia (n=14, 35%), and anemia (n=10, 25%). Drug-related hematological TEAEs of grade ≥3 were neutropenia (n=7, 18%), anemia (n=5, 13%), thrombocytopenia (n=4, 10%), and leukopenia (n=4, 10%). Overall, the patients’ white blood cell counts fluctuated mostly within the normal range, showing a declining trend during C1D15–C4, stabilizing around the lower limit of normal during C4–C18, and returning to normality by the end of the study. Platelet counts showed mild fluctuation within the normal range during treatment. Red blood cell counts were slightly below baseline but stable during C4–C19 and returned to the lower limit of normal at the end of the study (Supplemental Figure S1).
Hand-Foot Syndrome and Anlotinib Dosage
Seventeen patients (43%) reported a total of 42 hand-foot syndrome occurrences, with six patients experiencing drug-related grade ≥3 events. A higher incidence of hand-foot syndrome was observed among the first 23 patients enrolled, and (together with a higher incidence of hypertension) led to the protocol amendment reducing the anlotinib dose from 12 mg QD to 10 mg QD. The following topical glucocorticoids and non-steroidal anti-inflammatory drugs (NSAIDs) were used in the 13 patients presenting with apparent symptoms of hand-foot syndrome, and most patients achieved significant relief: dexamethasone cream (n=6); urea ointment (n=6); celecoxib or ibuprofen (n=7) for pain relief; codeine or tramadol (n=4) for pain relief.
Discussion
Patients with PROC face severe unmet needs for efficacious treatment options, as the platinum-free chemotherapies currently recommended by the National Comprehensive Cancer Network (NCCN) and European Society for Medical Oncology (ESMO) guidelines only offer limited efficacy in terms of response rate (10%–15%) and durability (3–4 months).21–23 This challenge is further underscored by molecular mechanisms driving chemoresistance, such as frequent upregulation of the PI3K pathway in epithelial ovarian cancer. The PI3K pathway plays a critical role in maintaining genomic stability and promoting chemoresistance by regulating DNA replication and cell cycle checkpoints. For example, PI3K inhibition has been shown to disrupt spindle assembly checkpoint function (eg, Aurora kinase B activity), leading to genomic instability and mitotic catastrophe during prometaphase, which may sensitize cells to certain therapies.24 The ANNIE study evaluated the niraparib–anlotinib combination in 40 patients with PROC. The primary analysis previously published showed promising antitumor activity of niraparib-anlotinib in this patient population, achieving an ITT ORR of 50% (including 1 case of complete response), together with encouraging results for median duration of response (6.9 months), platinum-free interval (13.2 months), progression-free survival (9.2 months), and OS (15.3 months).14 In this analysis, the updated median OS of 18.2 months (95% CI: 12.1–not evaluable) provided further evidence on the persistent clinical benefit of niraparib-anlotinib.
For PROC patients, the quest for more efficacious treatments is integrally related to drug safety and tolerability, as the latter is crucial for ensuring treatment adherence and sustainability and, therefore, a prerequisite for optimally translating drug activity into clinical efficacy. Ovarian cancer patients are often at risk of chronic and metabolic comorbidities and face high levels of mental stress.1,7 For patients with PROC, the cumulative toxicities of multiple prior lines of platinum-based chemotherapy would have exacerbated their general health.25 Additionally, with an estimated overall survival of less than one year,26 maintaining the quality of life is considered an important principle in PROC care. Prior to ANNIE, olaparib plus cediranib is another combination of PARP inhibitor-antiangiogenic that has been studied for treating PROC.27–29 However, this combination faced the challenge of high toxicity. In two clinical studies of olaparib-cediranib, grade ≥3 adverse events occurred in over 70% of the patients, and safety concerns prevented the use of both agents at full clinical doses.27,28 In the ANNIE study, the safety results from both the primary analysis and the current update indicate that overall the niraparib–anlotinib combination can be safely used in PROC patients with both agents at usual clinical doses; TEAEs were well managed, and all death events were due to disease progression.
Hypertension is commonly observed in patients receiving VEGFR inhibitors, occurring in 30%–80% of patients.30 With olaparib-cediranib, the incidence of hypertension was reported at 66.7%,27 mainly attributable to the VEGFR inhibitor cediranib. Among the major guideline-recommended classes of hypertension medication (CCB, ACEI, ARB, beta-blockers, and diuretics31), vasodilators such as CCB and renin-angiotensin-aldosterone system inhibitors such as ACEI and ARB would be suitable for relieving hypertension induced through VEGFR inhibitors’ on-target vasoconstriction effects.30,32 However, most CCBs are metabolized via the CYP3A pathway, interacting with most small-molecule tyrosine kinase inhibitors such as cediranib, anlotinib, and apatinib.30 For olaparib-cediranib, the situation is compounded by olaparib also being CYP3A-metabolized, making the management of blood pressure increasingly challenging. The use of CCBs would render the plasma concentrations of both olaparib and cediranib unpredictable, potentially causing uncertainty to both efficacy and safety.33,34
The design of the ANNIE study similarly anticipated a heightened need for blood pressure management, because in addition to anlotinib, which shares the hypertension-inducing class effect of VEGFR inhibitors,16,19 niraparib can also cause hypertension and increased heart rate due to inhibition of dopamine, norepinephrine, and serotonin receptors.17 In the NOVA trial, 19.3% patients reported hypertension, with grade ≥3 hypertension in 8.2% patients, and 10.4% patients reported palpitations.35 Upon adopting an individualized starting dose for niraparib, the NORA study conducted in Chinese patients saw a lower rate of all-grade and grade ≥3 hypertension (11.3% and 1.1%, respectively), and 18.1% patients experienced palpitations.36 On the other hand, unlike olaparib, niraparib is not metabolized by CYP3A, and this would reduce the constraints on the choice of antihypertensives. Based on these considerations, the ANNIE study designed and implemented close monitoring and preventive/early interventive measures for blood pressure management, and the results were satisfactory: 22 patients experienced post-baseline clinical hypertension events, with increased heart rate and diastolic blood pressure being the predominant symptoms. As such, beta-blockers, a class of potent heart rate controllers, were adopted as the mainstay for blood pressure and heart rate management. Early interventions with beta-blocker-based monotherapy or combination therapy achieved effective blood pressure control in most patients, with only five patients requiring triple therapy. No intensive antihypertensive therapy (<120/80 mmHg) was conducted. No cardiovascular events were recorded during the post-study treatment safety follow-up.
Lipid metabolism should be another focus in managing ovarian cancer patients, who are subject to multiple dyslipidemia risk factors including aging, hormonal alterations due to natural or ovariectomy-induced mesopause, and elevated cardiovascular risks.10 TEAEs of increases in triglycerides and cholesterol have been reported in studies of anlotinib, occurring in approximately 20%–60% of patients.37–39 In this study, patient lipid levels were closely monitored. Hypertriglyceridemia occurred in 12 patients, including grade ≥3 hypertriglyceridemia in three. Five patients experienced hypercholesterolemia, all of which were of grade 1–2. In standard clinical practice, the choice of therapeutic modalities for blood lipid management depends on the patient’s profile: lifestyle therapies constitute the primary treatment for patients with mild blood lipid elevation and without other cardiovascular or metabolic risk factors, while lipid-lowering medications are used for patients with persistently elevated blood lipid levels despite lifestyle therapies and patients with multiple other risk factors. However, for the middle-aged and elderly post-operative PROC patients in this study, lifestyle therapies such as weight control and physical activities would be unrealistic and might increase the patients’ physical burdens. As such, blood lipid TEAEs were primarily managed using lipid-lowering medications, which were prescribed based on physicians’ instruction and immediately upon detecting a trend of blood lipid elevation in any patient. Ten patients received immediate lipid-lowering medications, mostly using atorvastatin and simvastatin. One patient experiencing grade ≥3 hypertriglyceridemia received fenofibrate. These management measures successfully maintained patients’ blood lipid levels at normal or CTCAE grade 1–2 level. No pancreatitis or cardio-cerebrovascular events occurred.
Hematologic toxicities have always been noted as a common class effect of PARP inhibitors and with niraparib, the incidence of hematologic TEAEs reported in clinical trials is approximately 60%.35,36,40 Notably, myelodysplastic syndrome has been reported in patients receiving niraparib, with an incidence of 0.2%–1.4%.15 Once this occurs, patients would face severe hematological damage and need to permanently stop using PARP inhibitors, leaving them with restricted treatment options. Some studies of anlotinib also reported hematologic adverse events.38,39 As such, it was crucial to conduct comprehensive tracking of blood system indicators when these two drugs that could cause hematologic adverse events were administered in combination. In this study, patients’ CBC was closely monitored, with focused follow-up for leukocyte, red blood cell, hemoglobin, and platelet levels. Overall, the hematological adverse events were manageable, without new signals identified.
This study had several limitations. Firstly, information was incomplete on patients’ treatment history for pre-existing hypertension and the use of other concomitant medications. While timely and effective interventions were implemented during the study for hypertension TEAEs, it was difficult to determine whether prior medications influenced the efficacy of these interventions. Secondly, the study did not assess the quality of life or patient-reported outcomes (PRO), which are important parameters for late-stage ovarian cancer patients in addition to survival. While the study provided multidisciplinary interventions for controlling patients’ somatic symptoms, the effectiveness of this management process could not be evaluated in a more intuitive or in-depth manner due to the lack of PRO data. Thirdly, insomnia should have been pre-specified as a key TEAE for investigation in addition to the vascular, metabolic, and hematologic TEAEs discussed above. Later, in the study, it was found that five patients used sleep aids and four patients experienced insomnia events. This incidence of insomnia at 10% is lower than that in the general population (33%),41 suggesting possible under-reporting of insomnia TEAEs and, by extension, possible under-recording of the use of sleep aids. Additionally, although the small sample size was understandable given the patient population, it hindered meaningful subgroup analysis, this should be recognized as a limitation of the study, and such analyses need to be conducted in future large-scale trials.
Conclusion
In conclusion, the updated OS analysis of the ANNIE study showed sustained long-term efficacy of niraparib-anlotinib PROC patients, and the safety data reflected satisfactory tolerability and adverse event management. TEAEs related to niraparib-anlotinib mainly concerned the cardiovascular, metabolic, and hematologic systems. Cardiovascular adverse events primarily manifested as clinically apparent symptoms such as tachycardia and hypertension, which required preventive monitoring and intervention. Adverse events of the metabolic system are mainly manifested in dyslipidemia. Experience from this study suggests that the involvement of an MDT comprising physicians from cardiology and other relevant disease areas can provide integrated interventions and achieve comprehensive adverse event management for PROC patients. This mode of collaborative care could benefit ovarian cancer patients, who are often of advanced age and high comorbidity burdens, by improving patient experience and in turn, promoting treatment effectiveness in late-line ovarian cancer.
Abbreviations
ACEI, angiotensin-converting enzyme inhibitors; ARB, angiotensin receptor blockers; bpm, beats per minute; CBC, complete blood count; CCB, calcium channel blockers; CI, confidence interval; COVID-19, corona virus disease 2019; CTCAE, Common Terminology Criteria for Adverse Events; ECOG, Eastern Cooperative Oncology Group; ESMO, European Society for Medical Oncology; ITT, intention-to-treat; MDT, multidisciplinary team; NCCN, National Comprehensive Cancer Network; NSAIDs, non-steroidal anti-inflammatory drugs; ORR, overall response rate; OS, overall survival; PARP, poly (ADP-ribose) polymerase; PRO, patient-reported outcomes; PROC, platinum-resistant recurrent ovarian cancer; QD, once a day; TEAEs, treatment-emergent adverse events; VEGFR, vascular endothelial growth factor receptor.
Data Sharing Statement
The authenticity of this article has been validated by uploading the key raw data onto the Research Data Deposit public platform (www.researchdata.org.cn), with the approval RDD number RDDA2022410532. Further inquiries can be directed to the corresponding author. Deidentified individual participant data will be made available to researchers who provide a methodologically sound proposal, subject to approval by the ethics committee at Sun Yat-Sen University Cancer Center, to achieve aims in the approved proposal. Proposals should be directed at the corresponding author.
Acknowledgments
The authors would like to thank the patients, their families, and all other investigational site staff who took part in this study. Prof. Liang Biling and Prof. Zhang Xiaoling conducted an independent review of all tumor evaluation results from the Central Radiology Committee in the study. Statistician Jia Huixun conducted a quality check of all endpoint calculations. Study assistant Xian Bingna ran all the data and materials management. Professor Guo Lan worked as an external consultant for cardiovascular event management. Medical writing assistance for this article was provided by Bo Lyu, PhD (Costello Medical) and Peng Lei (Costello Medical) in accordance with Good Publication Practice (GPP 2022) guidelines (https://www.ismpp.org/gpp-2022). This paper has been uploaded to ResearchSquare as a preprint: https://www.researchsquare.com/article/rs-3577949/v1.
Funding
This work was sponsored by Zai Lab (Shanghai) Co., Ltd; Jiangsu Chia Tai-Tianqing Pharmaceutical Co., Ltd, and was also supported by funds from the National Natural Science Foundation of China [grant number 82102783] and Science and Technology Projects in Guangzhou [No. SL2022A04J01644]. The manuscript was written by the authors with medical writing support, which was funded by Zai Lab. The sponsors were not involved in the study design, the collection, analysis, and interpretation of data, the writing of the manuscript, or the decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Michels KA, McNeel TS, Trabert B. Metabolic syndrome and risk of ovarian and fallopian tube cancer in the United States: an analysis of linked SEER-medicare data. Gynecol Oncol. 2019;155(2):294–300. doi:10.1016/j.ygyno.2019.08.032
2. National Cancer Institute. Cancer stat facts: ovarian cancer. Available from: https://seer.cancer.gov/statfacts/html/ovary.html.
3. Liu X, Yu S, Mao Z, et al. Dyslipidemia prevalence, awareness, treatment, control, and risk factors in Chinese rural population: the Henan rural cohort study. Lipids Health Dis. 2018;17(1):119. doi:10.1186/s12944-018-0768-7
4. Prince MJ, Wu F, Guo Y, et al. The burden of disease in older people and implications for health policy and practice. Lancet. 2015;385(9967):549–562. doi:10.1016/S0140-6736(14)61347-7
5. Rodgers JL, Jones J, Bolleddu SI, et al. Cardiovascular risks associated with gender and aging. J Cardiovasc Dev Dis. 2019;6(2):19. doi:10.3390/jcdd6020019
6. Saani I, Raj N, Sood R, et al. Clinical challenges in the management of malignant ovarian germ cell tumours. Int J Environ Res Public Health. 2023;20(12):6089. doi:10.3390/ijerph20126089
7. Hu S, Baraghoshi D, Chang CP, et al. Mental health disorders among ovarian cancer survivors in a population-based cohort. Cancer Med. 2023;12(2):1801–1812. doi:10.1002/cam4.4976
8. Ozga M, Aghajanian C, Myers-Virtue S, et al. A systematic review of ovarian cancer and fear of recurrence. Palliat Support Care. 2015;13(6):1771–1780. doi:10.1017/S1478951515000127
9. Ryder AL, Cohen BE. Evidence for depression and anxiety as risk factors for heart disease and stroke: implications for primary care. Fam Pract. 2021;38(3):365–367. doi:10.1093/fampra/cmab031
10. Saeaib N, Peeyananjarassri K, Liabsuetrakul T, Buhachat R, Myriokefalitaki E. Hormone replacement therapy after surgery for epithelial ovarian cancer. Cochrane Database Syst Rev. 2020;1:CD012559.
11. Neves KB, Montezano AC, Lang NN, Touyz RM. Vascular toxicity associated with anti-angiogenic drugs. Clin Sci. 2020;134(18):2503–2520. doi:10.1042/CS20200308
12. Cameron AC, Touyz RM, Lang NN. Vascular complications of cancer chemotherapy. Can J Cardiol. 2016;32(7):852–862. doi:10.1016/j.cjca.2015.12.023
13. Ghose A, McCann L, Makker S, et al. Diagnostic biomarkers in ovarian cancer: advances beyond CA125 and HE4. Ther Adv Med Oncol. 2024;16:17588359241233225. doi:10.1177/17588359241233225
14. Liu G, Feng Y, Li J, et al. A novel combination of niraparib and anlotinib in platinum-resistant ovarian cancer: efficacy and safety results from the phase II, multi-center ANNIE study. EClinicalMedicine. 2022;54:101767. doi:10.1016/j.eclinm.2022.101767
15. Monk BJ, Gonzalez-Martin A, Buckley L, et al. Safety and management of niraparib monotherapy in ovarian cancer clinical trials. Int J Gynecol Cancer. 2023;33(6):971–981. doi:10.1136/ijgc-2022-004079
16. Bing L, Jing C, Xiao-Liang L. Anlotinib-induced hypertension: current concepts and future prospects. Curr Pharm Des. 2022;28(3):216–224. doi:10.2174/1381612827666211006145141
17. Heo YA, Duggan ST. Niraparib: a review in ovarian cancer. Target Oncol. 2018;13(4):533–539. doi:10.1007/s11523-018-0582-1
18. Pandey AK, Singhi EK, Arroyo JP, et al. Mechanisms of VEGF (vascular endothelial growth factor) inhibitor-associated hypertension and vascular disease. Hypertension. 2018;71(2):e1–e8. doi:10.1161/HYPERTENSIONAHA.117.10271
19. Butel-Simoes LE, Haw TJ, Williams T, et al. Established and emerging cancer therapies and cardiovascular system: focus on hypertension-mechanisms and mitigation. Hypertension. 2023;80(4):685–710. doi:10.1161/HYPERTENSIONAHA.122.17947
20. The joint task force for guideline on the assessment and management of cardiovascular risk in China. Guideline on the assessment and management of cardiovascular risk in China. Chin J Prevent Med. 2019;53:13–35.
21. National Comprehensive Cancer Network. NCCN Guidelines for Patients Ovarian Cancer; 2022.
22. Ledermann JA, Raja FA, Fotopoulou C, et al. Newly diagnosed and relapsed epithelial ovarian carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(Suppl 6):vi24–vi32. doi:10.1093/annonc/mdt333
23. Pujade-Lauraine E, Banerjee S, Pignata S. Management of platinum-resistant, relapsed epithelial ovarian cancer and new drug perspectives. J Clin Oncol. 2019;37(27):2437–2448. doi:10.1200/JCO.19.00194
24. Aliyuda F, Moschetta M, Ghose A, et al. Advances in ovarian cancer treatment beyond PARP inhibitors. Curr Cancer Drug Targets. 2023;23(6):433–446. doi:10.2174/1568009623666230209121732
25. Fotopoulou C. Limitations to the use of carboplatin-based therapy in advanced ovarian cancer. EJC Suppl. 2014;12(2):13–16. doi:10.1016/S1359-6349(15)70005-4
26. Davis A, Tinker AV, Friedlander M. “Platinum resistant” ovarian cancer: what is it, who to treat and how to measure benefit? Gynecol Oncol. 2014;133(3):624–631. doi:10.1016/j.ygyno.2014.02.038
27. Lee JM, Moore RG, Ghamande S, et al. Cediranib in combination with olaparib in patients without a germline BRCA 1/2 mutation and with recurrent platinum-resistant ovarian cancer: phase IIB CONCERTO trial. Clin Cancer Res. 2022;28(19):4186–4193. doi:10.1158/1078-0432.CCR-21-1733
28. Liu JF, Barry WT, Birrer M, et al. Combination cediranib and olaparib versus olaparib alone for women with recurrent platinum-sensitive ovarian cancer: a randomised phase 2 study. Lancet Oncol. 2014;15(11):1207–1214. doi:10.1016/S1470-2045(14)70391-2
29. Colombo N, Tomao F, Benedetti Panici P, et al. Randomized Phase II trial of weekly paclitaxel vs. cediranib-olaparib (continuous or intermittent schedule) in platinum-resistant high-grade epithelial ovarian cancer. Gynecol Oncol. 2022;164(3):505–513. doi:10.1016/j.ygyno.2022.01.015
30. Robinson ES, Khankin EV, Karumanchi SA, Humphreys BD. Hypertension induced by vascular endothelial growth factor signaling pathway inhibition: mechanisms and potential use as a biomarker. Semin Nephrol. 2010;30(6):591–601. doi:10.1016/j.semnephrol.2010.09.007
31. World Health Organization. Guideline for the Pharmacological Treatment of Hypertension in Adults; 2021.
32. de Jesus-Gonzalez N, Robinson E, Moslehi J, Humphreys BD. Management of antiangiogenic therapy-induced hypertension. Hypertension. 2012;60(3):607–615. doi:10.1161/HYPERTENSIONAHA.112.196774
33. Chase DM, Patel S, Shields K. Profile of olaparib in the treatment of advanced ovarian cancer. Int J Women’s Health. 2016;8:125–129. doi:10.2147/IJWH.S55906
34. Lassen U, Miller WH, Hotte S, et al. Phase I evaluation of the effects of ketoconazole and rifampicin on cediranib pharmacokinetics in patients with solid tumours. Cancer Chemother Pharmacol. 2013;71(2):543–549. doi:10.1007/s00280-012-2038-0
35. Mirza MR, Monk BJ, Herrstedt J, et al. Niraparib maintenance therapy in platinum-sensitive, recurrent ovarian cancer. N Engl J Med. 2016;375(22):2154–2164. doi:10.1056/NEJMoa1611310
36. Wu XH, Zhu JQ, Yin RT, et al. Niraparib maintenance therapy in patients with platinum-sensitive recurrent ovarian cancer using an individualized starting dose (NORA): a randomized, double-blind, placebo-controlled Phase III trial(☆). Ann Oncol. 2021;32(4):512–521. doi:10.1016/j.annonc.2020.12.018
37. Chi Y, Fang Z, Hong X, et al. Safety and efficacy of anlotinib, a multikinase angiogenesis inhibitor, in patients with refractory metastatic soft-tissue sarcoma. Clin Cancer Res. 2018;24(21):5233–5238. doi:10.1158/1078-0432.CCR-17-3766
38. Lan CY, Zhao J, Yang F, et al. Anlotinib combined with TQB2450 in patients with platinum-resistant or -refractory ovarian cancer: a multi-center, single-arm, phase 1b trial. Cell Rep Med. 2022;3(7):100689. doi:10.1016/j.xcrm.2022.100689
39. Sun Y, Niu W, Du F, et al. Safety, pharmacokinetics, and antitumor properties of anlotinib, an oral multi-target tyrosine kinase inhibitor, in patients with advanced refractory solid tumors. J Hematol Oncol. 2016;9(1):105. doi:10.1186/s13045-016-0332-8
40. Moore KN, Secord AA, Geller MA, et al. Niraparib monotherapy for late-line treatment of ovarian cancer (QUADRA): a multicentre, open-label, single-arm, phase 2 trial. Lancet Oncol. 2019;20(5):636–648. doi:10.1016/S1470-2045(19)30029-4
41. Bhaskar S, Hemavathy D, Prasad S. Prevalence of chronic insomnia in adult patients and its correlation with medical comorbidities. J Family Med Prim Care. 2016;5(4):780–784. doi:10.4103/2249-4863.201153
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.