")
Back to Journals » Clinical Ophthalmology » Volume 16
Advantages of Double Running Sutures in Astigmatism After Penetrating Keratoplasty
Authors Nuzzi R , Burato C, Tridico F , Nuzzi A , Caselgrandi P
Received 3 January 2022
Accepted for publication 22 February 2022
Published 15 March 2022 Volume 2022:16 Pages 797—802
DOI https://doi.org/10.2147/OPTH.S355538
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Raffaele Nuzzi,1 Claudio Burato,1 Federico Tridico,1 Alessia Nuzzi,2 Paolo Caselgrandi1
1Eye Clinic Section, Department of Surgical Sciences, University of Turin, Turin, Italy; 2Department of Clinical Sciences and Community Health, Eye Clinic San Giuseppe Hospital, IRCCS Multimedica, University of Milan, Milan, Italy
Correspondence: Raffaele Nuzzi, Eye Clinic Section, Department of Surgical Sciences, University of Turin, Turin, Italy, Email [email protected]
Background: The purpose of this prospective study is to evaluate the effects of different suturing techniques in perforating keratoplasty surgery, in order to identify the most effective in reducing post-operative astigmatism.
Methods: We analysed data from patients who underwent penetrating keratoplasty for different indications. All interventions were performed by the same surgeon. Patients were subjected to a follow-up of at least 12 months after surgery, during which astigmatism (assessed by keratometry, topography and refraction) best-corrected visual acuity (BCVA) and complications were evaluated. A total of 100 eyes from 100 patients were included and were randomly assigned to five different groups, each one featuring a different suturing technique: interrupted (INT), single running (SRS), double running with two 10– 0 sutures (DRS), double running antitorque with two 10– 0 sutures (DRSa), double running with both 10– 0 and 11– 0 sutures (DRS with 11– 0).
Results: There is a statistically significant difference in astigmatism after surgery between the double running sutures groups and the others with different techniques. However, there is no statistically significant difference between the INT and the SRS group; moreover, there is no statistically significant difference between the different groups with double running sutures (DRS, DRSa, DRS with 11– 0). There is no statistically significant difference in BCVA values among the five groups. The wound leak rate was 10% in the INT group, 5.3% in the SRS group and 0% in all groups with double running sutures.
Conclusion: In penetrating keratoplasty surgery, the double running suture technique reduces postoperative astigmatism, provides faster visual rehabilitation and features lower complication rates when compared to techniques featuring single running and interrupted sutures. No significant difference in terms of postoperative astigmatism or complication rates was observed among patients receiving double running suture techniques.
Keywords: astigmatism, penetrating keratoplasty, corneal suture technique, running suture, interrupted suture
Introduction
The cornea can be affected by several pathological conditions that may lead to blindness. Despite the increasing need for donors, corneal transplant is still the most effective treatment for restoring corneal physio-anatomical integrity and, consecutively, visual function. Perforating keratoplasty (PK) has made history as the cornerstone of corneal graft techniques, and as of today, it is still one of the most versatile and adoptable surgical strategy for the treatment of most corneal diseases.1
Residual astigmatism following perforating keratoplasty represents an important limitation of this procedure. In fact, while advances in surgical techniques, materials and instruments led to a considerable improvement in anatomical results, especially in terms corneal graft transparency over time, on the other hand, high or irregular post-operative astigmatism may bring poor and unsatisfactory functional results in a not negligible percentage of patients.
Factors affecting postoperative astigmatism are represented mainly by healing processes and the adopted suturing technique.2–5 Over the years, several suture techniques have been proposed for this procedure. This has led to a search for the best technique in terms of risk-benefit ratio. Currently, the mainly used techniques are represented by interrupted suture (INT), single running suture (SRS) and double running sutures (DRS).
The purpose of this prospective study is to evaluate the effects of different suture techniques in penetrating keratoplasty surgery, in order to identify the most effective in reducing post-operative astigmatism.
Materials and Methods
This prospective study has been approved by our institutional ethics committee and written consent to participate was collected from all participants of the study. All procedures in this study relating to its conduct and documentation were carried out in accordance with the ethical principles established in the Declaration of Helsinki and its revisions.
In this prospective study we collected data from patients requiring penetrating keratoplasty in the period between May 2014 and January 2018. Every surgical procedure featured in this study were performed by the same surgeon.
Every recruited subject underwent a complete ophthalmological examination before surgery. The main indications for surgery in the study population were represented by keratoconus, central corneal scarring, corneal oedema due to Fuchs’ dystrophy and corneal oedema secondary to cataract surgery. In this case, penetrating keratoplasty was required given the presence of severe corneal conditions with important degenerative and scarring outcomes that contraindicated lamellar surgery. Surgical indications are listed in Table 1.
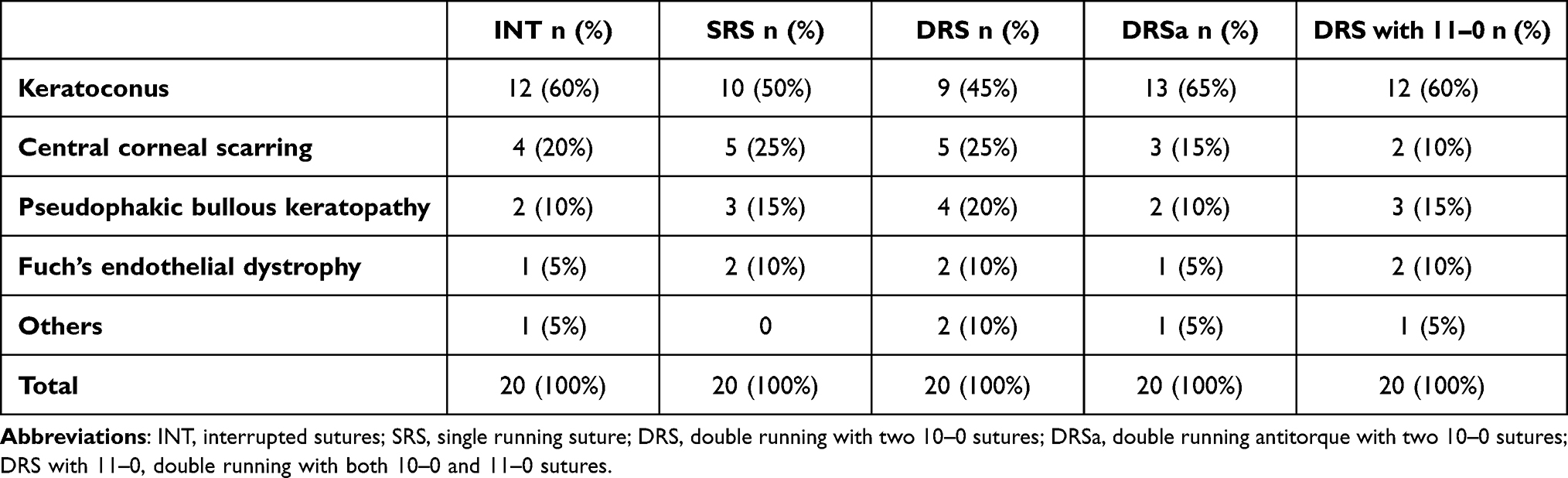 |
Table 1 Indications for Penetrating Keratoplasty (PK) Surgery in Each Group |
Patients undergoing combined surgery for cataracts or glaucoma were excluded. Patients were subjected to follow-up for 12 months after surgery, during which astigmatism (measured by keratometry, topography and refraction) best-corrected visual acuity (BCVA) and complication rates were assessed. Follow-up evaluations were scheduled at 1, 3, 6 and 12 months.
100 Eyes from 100 patients were included and randomly assigned to five different groups, each featuring a different suturing technique: interrupted (INT), single running (SRS), double running with two 10–0 sutures (DRS), double running antitorque with two 10–0 sutures (DRSa), double running with both 10–0 and 11–0 sutures (DRS with 11–0). Randomization was carried out with sequentially numbered cases provided by a computerized sequence before the start of the study. Patients’ characteristics are listed in Table 2.
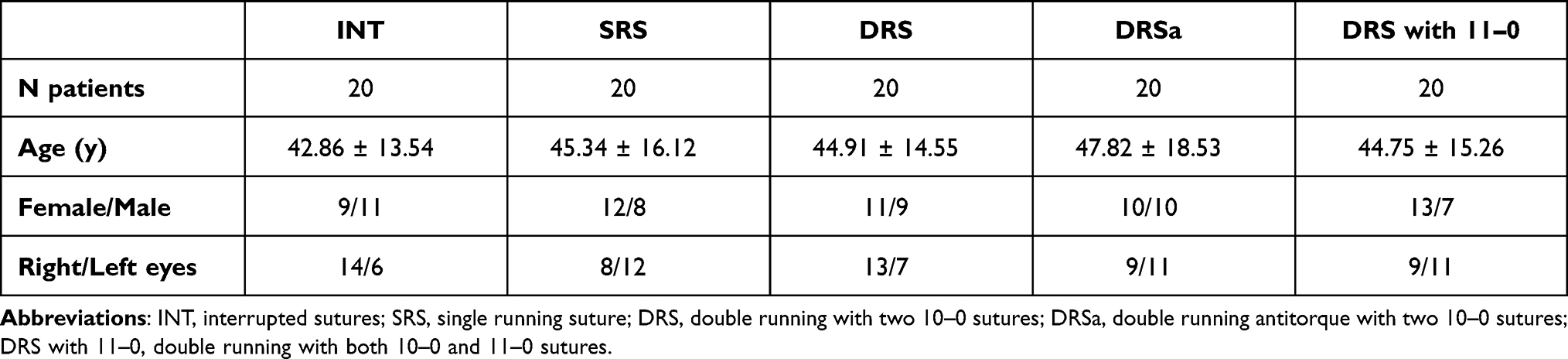 |
Table 2 Demographic Characteristics of Patients Included in the Study |
The mean trephine size of the recipient cornea was 7.50 mm, while the one relative to donor cornea was 7.75 mm. Penetrating keratoplasty was performed with a standard technique using the Hanna trephine6 in all study groups.
For the interrupted suture group, a 10–0 nylon thread was applied on 16 bites. In case of an astigmatism greater than 3 diopters detected during the follow-up period, a selective suture removal was performed along the corresponding meridian at about 2–3 months after surgery. A continuous Nylon 10–0 suture with 16–24 bites was used for the single running group. In case of postoperative astigmatism greater than 3 diopters, the continuous suture in these patients was adjusted right after surgery or in later follow-up visits.
Finally, in the groups featuring double running sutures, two continuous sutures with 12–16 bites were applied in accordance to the diameter of the graft. Patients receiving double running sutures were split in three groups according to different techniques: double 10–0 nylon suture, double antitorque 10–0 nylon suture (cross-stitch sutures in opposite direction), and 10–0 nylon suture in association with nylon 11–0 suture (Figure 1).
 |
Figure 1 The two main suturing techniques used in penetrating keratoplasty: single running suture (SRS) (A) and double running sutures (DRS) (B). |
In the latter three groups the depth of the first suture was about 90% of the cornea thickness and 50–90% for the second suture. The sutures were applied with equally spaced bites (0.75 mm) with minor extension on the donor side of the wound and greater extension on the recipient side.
For groups featuring double running suture techniques, postoperative suture adjustments for high postoperative astigmatism (> 3 diopters) were not possible, to avoid suture damage and failure. Therefore, in these cases, we opted for the complete removal of a single 10–0 suture at 2–3 months after surgery, leaving the second suture in place. Given this, especially in cases featuring 11–0 nylon suture application, the remaining suture is allowed to dissolve spontaneously, starting at 15–20 months after its application, with possible gradual astigmatism reduction.
Mean best-corrected visual acuity (BVCA) and mean residual astigmatism at 12 months after surgery (detected with refraction, keratometry and corneal topography) were compared among all study groups. The Mann–Whitney U-test was used to compare data between two groups, while the Wilcoxon matched pairs signed ranks test was used to compare more than two groups. Statistical significance was considered for a p-value < 0.05. Also, complications rates among all groups were compared.
Results
Mean post-surgical keratometric astigmatism values at the 12 months follow-up were 5.86 ± 1.87 diopters in the interrupted suture (INT) group, 5.34 ± 1.99 diopters in the single running suture group (SRS), 3.00 ± 1.38 diopters in the double 10–0 running suture group (DRS), 2.89 ± 1.11 diopters in the double 10–0 running antitorque suture group (DRSa) and 3.06 ± 1.22 diopters in the group featuring the double running suture with both 10–0 and 11–0 nylon threads (DRS with 11–0) (Table 3).
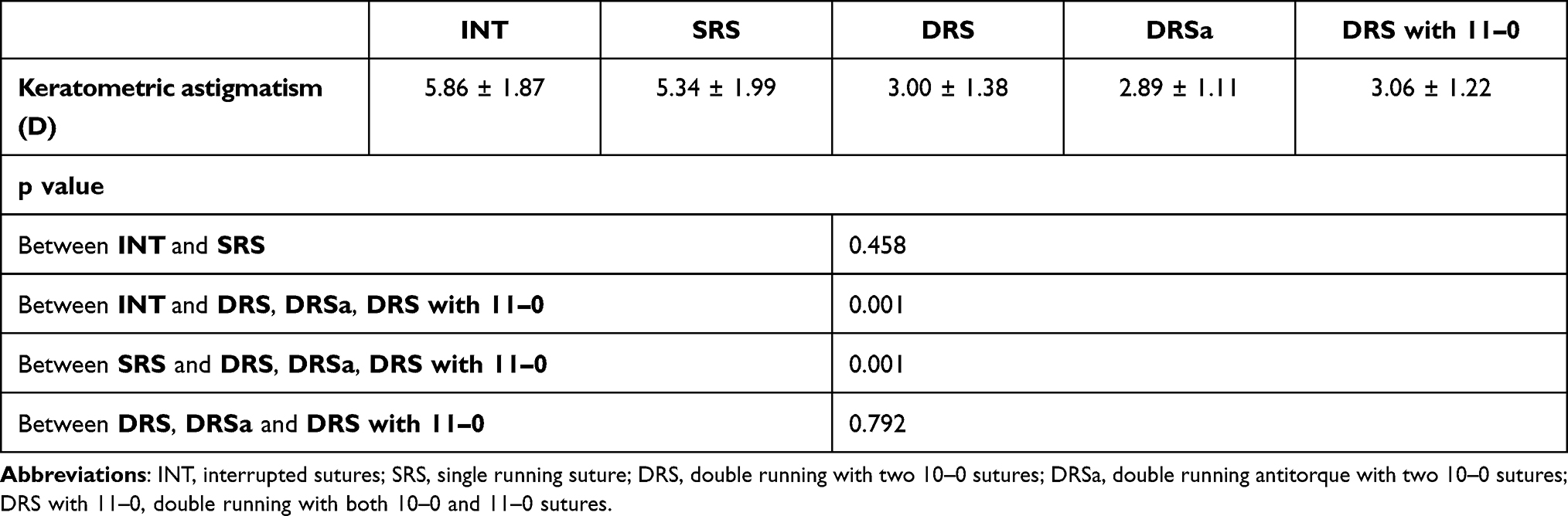 |
Table 3 Astigmatism (Diopters) Measured by Keratometry in Each Suturing Technique Groups at 12 Months of Follow-Up |
Mean post-surgical topographic astigmatism was 5.95 ± 1.69 diopters in the INT group, 5.62 ± 1.95 diopters in the SRS group, 3.18 ± 1.44 diopters in the DRS group, 3.02 ± 1.27 diopters DRSa group and 3.12 ± 1.08 diopters DRS with 11–0 group (Table 4).
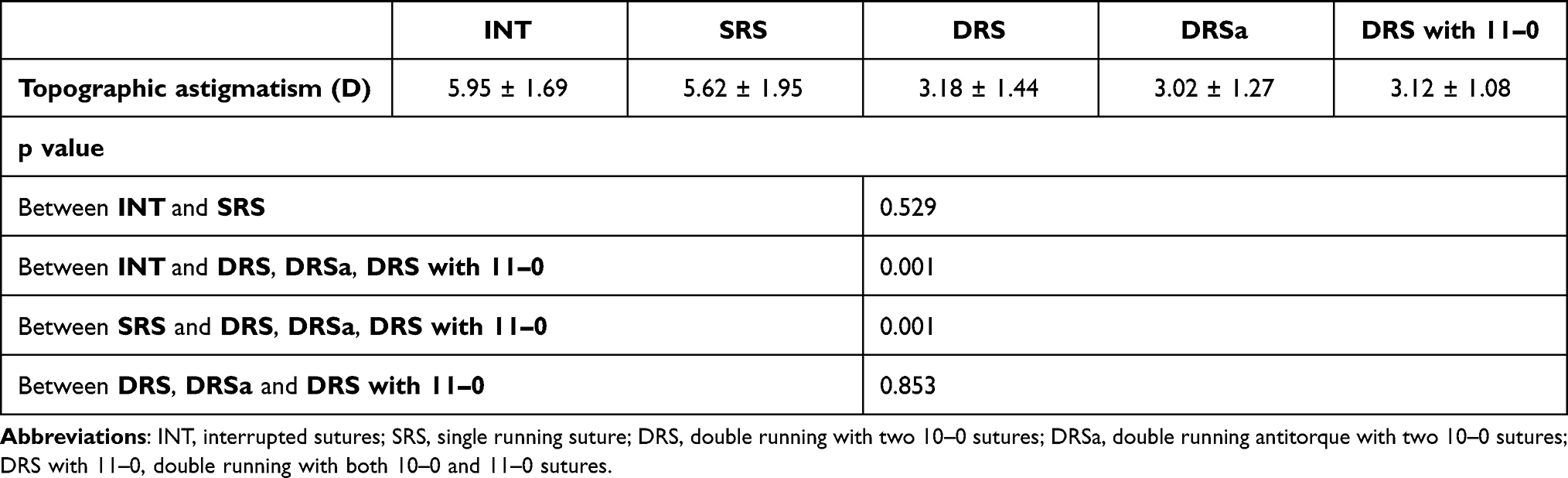 |
Table 4 Astigmatism (Diopters) Measured by Topography in Each Suturing Technique Groups at 12 Months of Follow-Up |
The values measured by refraction showed a slightly lower astigmatism for all groups compared to the values obtained with keratometry and topography.
From these results it emerges that there is no statistically significant difference in the postoperative astigmatism between the INT and the SRS group, while the difference between each of these two groups and the remaining three groups featuring double running sutures is statistically significant. There was no statistically significant difference in mean astigmatism between the groups with double running sutures (DRS, DRSa, DRS with 11–0).
Mean BCVA values at 12 months after surgery were 0.37 ± 0.11 in the INT group, 0.36 ± 0.13 in the SRS group, 0.39 ± 0.09 in the DRS group, 0.42 ± 0.12 in the DRSa group and 0.40 ± 0.14 in the DRS with 11–0 group. No statistically significant BVCA differences were detected among the five study groups.
In terms of complications, no endophthalmitis or graft ulceration was recorded in any group, while wound leak rate was 10% in the INT group, 5.3% in the SRS group and 0% in all groups with double running sutures (DRS, DRSa, and DRS with 11–0).
Discussion
The purpose of this prospective study was to investigate the effects of different suturing techniques on residual postoperative corneal astigmatism after penetrating keratoplasty (PK) surgery. In particular, it compared five different suturing techniques: interrupted, single running, double running 10–0 suture, double running 10–0 antitorque suture and double running suture with both 10–0 and 11–0 nylon threads.
The results show that at 12 months after surgery, the double running suture technique is the one associated with minor corneal astigmatism if compared with interrupted sutures or single running suture, regardless of whether two 10–0 nylon sutures are used, or one of them is a 11–0 suture or whether they are placed in antitorque mode. Furthermore, the double running technique, unlike the alternative techniques, was associated with a lower rate of postoperative complications, with no cases of wound leak or dehiscence. This phenomenon can be explained by a greater need of postoperative suture manipulation in the INT and SRS groups, while sutures in the DRS technique tend to be adjusted less, or not at all, especially in case of a double continuous suture with both 10–0 and 11–0 nylon threads.
The fact that the interrupted suture technique leads to increased postoperative astigmatism compared to single running suture or double running suture techniques is widely described in the current literature.7–9 However, a comparison between the single running and double running suture technique is still controversial. Assil et al state that the double running suture technique induces less astigmatism and leads to faster visual rehabilitation and a steeper cornea.10 Other authors report that the DRS technique induces less astigmatism than SRS, but only in the first postoperative months while there is no difference after a complete suture removal.11,12 This last aspect can be explained as the complete suture removal is usually associated with a marked reduction of astigmatism in the SRS technique, unlike with the DRS one. Jonas et al, however, underline that the DRS technique could be superior given the reduced risk of loosening sutures.13 Moreover, other authors report that SRS induces a lower degree of astigmatism compared to DRS starting from the very first postoperative months as it allows selective suture manipulation.14
Although there is no agreement in the literature on which suture technique is the one associated with minor astigmatism, it is widely accepted that double running sutures allow faster rehabilitation of visual function after penetrating keratoplasty. In fact, it is possible to remove one of the two sutures after just 2–3 months after surgery, leaving the second one in place. Moreover, especially in case of 11–0 suture application, the remaining thread will begin to spontaneously dissolve at 15–20 months. Additionally, DRS is a safer technique as it comes with a lower risk of complications.
In conclusion, the results of our study show that in penetrating keratoplasty surgery the double running suture technique can provide better outcomes as it is associated with minor postoperative astigmatism, leads to faster visual rehabilitation and has a lower complication rate if compared with techniques featuring single running and interrupted sutures. There are no differences in terms of postoperative astigmatism or complication rates between the different double running suture techniques examined. In conclusion, with the results reported in this study, we aim to provide further insights regarding the effects of different suture techniques for penetrating keratoplasty, in order to reduce possible concerns about this topic.
Ethics and Consent to Participate
All procedures in this study concerning his conduction and documentation were performed in conformity with the ethical principles set out in the Helsinki Declaration and its revisions. This prospective study was approved by the Ethics Committee of “Città della Salute e della Scienza di Torino” (University of Turin). Consent to participate was obtained in written form and has been registered for all subjects of this study. All participants were informed about the purpose of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
1. Naumann GOH. The bowman lecture. Eye. 1995;9(4):395–421. doi:10.1038/EYE.1995.98
2. Swinger CA. Postoperative astigmatism. Surv Ophthalmol. 1987;31(4):219–248. doi:10.1016/0039-6257(87)90023-3
3. Hoppenreijs VPT, van Rij G, Beekhuis WH, Rijneveld WJ, Rinkel-van Driel E. Causes of high astigmatism after penetrating keratoplasty. Doc Ophthalmol. 1993;85(1):21–34. doi:10.1007/BF01268097
4. Seitz B, Langenbucher A, Küchle M, Naumann GOH. Impact of graft diameter on corneal power and the regularity of postkeratoplasty astigmatism before and after suture removal. Ophthalmology. 2003;110(11):2162–2167. doi:10.1016/S0161-6420(03)00659-6
5. Murta JN, Amaro L, Tavares C, Mira JB. Astigmatism after penetrating keratoplasty. Role of the suture technique. Doc Ophthalmol. 1994;87(4):331–336. doi:10.1007/BF01203342
6. Waring GO, Hanna KD. The Hanna suction punch block and trephine system for penetrating keratoplasty. Arch Ophthalmol. 1989;107(10):1536–1539. doi:10.1001/ARCHOPHT.1989.01070020610051
7. Filatov V, Steinert RF, Talamo JH. Postkeratoplasty astigmatism with single running suture or interrupted sutures. Am J Ophthalmol. 1993;115(6):715–721. doi:10.1016/S0002-9394(14)73637-2
8. Frost NA, Wu J, Lai TF, Coster DJ. A review of randomized controlled trials of penetrating keratoplasty techniques. Ophthalmology. 2006;113(6):942–949. doi:10.1016/J.OPHTHA.2006.03.003
9. Busin M, Mönks T, Al’Nawaiseh I. Different suturing techniques variously affect the regularity of postkeratoplasty astigmatism. Ophthalmology. 1998;105(7):1200–1205. doi:10.1016/S0161-6420(98)97021-X
10. Assil KK, Zarnegar SR, Schanzlin DJ. Visual outcome after penetrating keratoplasty with double continuous or combined interrupted and continuous suture wound closure. Am J Ophthalmol. 1992;114(1):63–71. doi:10.1016/S0002-9394(14)77414-8
11. Spadea L, Cifariello F, Bianco G, Balestrazzi E. Long-term results of penetrating keratoplasty using a single or double running suture technique. Graefes Arch Clin Exp Ophthalmol. 2002;240(5):415–419. doi:10.1007/S00417-002-0444-4
12. Jonas JB, Heyer C, Budde WM. Effect of single- and double-running sutures on corneal astigmatism and suture loosening after PKP. J Cataract Refract Surg. 2002;28(9):1709–1710. doi:10.1016/S0886-3350(02)01592-4
13. Ramirez M, Hodge DO, Bourne WM. Keratometric results during the first year after keratoplasty: adjustable single running suture technique versus double running suture technique. Ophthalmic Surg Lasers Imaging Retina. 2022;32(5):370–374. doi:10.3928/1542-8877-20010901-04
14. Solano JM, Hodge DO, Bourne WM. Keratometric astigmatism after suture removal in penetrating keratoplasty: double running versus single running suture techniques. Cornea. 2003;22(8):716–720. doi:10.1097/00003226-200311000-00002
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.