Back to Journals » Advances in Medical Education and Practice » Volume 16
Advancing Rural Generalist Training: The Northern Regional Integrated Clerkship, a Blended Longitudinal Integrated Clerkship Innovation in Northern British Columbia
Authors Maurice SB ![]() , Watt M
, Watt M ![]() , Gingerich A
, Gingerich A ![]() , Winwood PJ
, Winwood PJ
Received 11 June 2025
Accepted for publication 7 October 2025
Published 18 October 2025 Volume 2025:16 Pages 1917—1928
DOI https://doi.org/10.2147/AMEP.S542705
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Dr Md Anwarul Azim Majumder
Sean B Maurice,1,2 Maggie Watt,3 Andrea Gingerich,1 Paul J Winwood1,3
1Northern Medical Program, Division of Medical Sciences, University of Northern British Columbia, Prince George, BC, Canada; 2Department of Cellular and Physiological Sciences, Faculty of Medicine, University of British Columbia, Vancouver, BC, Canada; 3Faculty of Medicine, University of British Columbia, Vancouver, BC, Canada
Correspondence: Paul J Winwood, Northern Medical Program, Division of Medical Sciences, University of Northern British Columbia, 3333 University Way, Prince George, BC, V2N4Z9, Canada, Email [email protected]
Abstract: The Northern Medical Program (NMP) is the most rural site of the University of British Columbia’s distributed medical school. Situated in northern British Columbia, Canada, the NMP strives for health equity by training physicians to meet the needs of northern, rural and Indigenous patients with innovative approaches to curriculum delivery which maintain comparability to the rest of the program and alignment with the assessment structure. Medical schools have a social accountability mandate to train physicians to serve the needs of rural and Indigenous peoples, to address the challenges of rural recruitment and retention, and to eliminate health inequities. Here we describe the creation of a new blended clerkship which places students in a small rural community for a 6-month longitudinal integrated clerkship and in a small urban community for a 6-month rotational clerkship. This new clerkship provides a unique opportunity for learners to learn and experience rural generalist medicine while meeting the accreditation standard of comparability. Early implementation has shown promise in enhancing rural medical education while maintaining curricular comparability, with positive reception from students and faculty.
Keywords: rural population, Indigenous peoples, health equity, social responsibility, health workforce, medical education, clinical clerkship
Introduction
Recruitment and retention of healthcare providers in rural areas is challenging. Despite widespread adoption of Distributed Medical Education (DME) throughout Canada, there remains a significant geographic maldistribution of healthcare providers relative to the population. While 18% of Canadians live rurally, their needs are served by only 8% of physicians who live rurally,1 and similar maldistributions exist for other healthcare professionals.2 The shortage of healthcare providers leads to inequities in health outcomes for rural peoples, compared with their urban counterparts.3 Ensuring equitable healthcare access and outcomes is a social accountability imperative, and a UN Sustainable Development Goal.4,5 It is also critically important for the health of Indigenous peoples, many of whom live rurally, and continue to suffer significant health inequities due to past and ongoing effects of colonization.6,7
In Canada, like other regions of the world with sparse populations spread across large geographies, DME programs have been created to allow training of medical students in rural regions in order to increase the odds that students trained at these sites will stay in the region.8,9 Many medical schools with DME programs involve Longitudinal Integrated Clerkships (LICs) as a component of the clinical education. Students training at rurally located DME sites in Canada and other countries are 2–5 times more likely to practice rurally than their counterparts who trained at urban sites.10–13 Students who choose to train in a rural LIC are 2–12 times more likely to practice rurally than their counterparts who participated in a block rotation.11,14–16 When students train at a rural DME site and participate in an LIC based in rural primary care, they are 5–19 times more likely to practice rurally than their counterparts trained at an urban tertiary care university hospital.11,13 Thus, developing rural DME sites and rural LICs are critical strategies for building the rural health workforce.
Correcting the maldistribution of physicians requires that physicians are taught how medicine is practiced in places other than academic medical centres and large urban areas. However, our curricula continue to under-represent generalist-specific teaching and community contexts, while over-representing discipline-specific specialist teaching and metropolitan medical contexts, despite evidence that the majority of patients seek care outside of academic medical centres.17 In Canada, accreditation standards dictate that across distributed sites of the same medical school, learning experiences must be comparable and assessment must be equivalent, to ensure all learners achieve the same learning outcomes.18 As such, there is a tension between capitalizing on the potential for unique learning opportunities provided by the diverse contexts of a distributed medical school, and the need to ensure that curriculum delivery is comparable.19 Navigating this grey area is important when developing innovations in DME. Here we describe an innovation to increase training in rural generalist medicine in small rural communities, offered at one site in a DME program while maintaining comparability to the rest of the sites of our provincially distributed program.
Our Context
The province of British Columbia (BC) is the Westernmost province in Canada, with its population of 5.5 million people mostly concentrated near the southern border. The province is currently served by a single medical school, with four academic sites distributed across a vast geography.20 Located in Prince George, a small urban community, the Northern Medical Program (NMP) is the most northern and rural site of the University of British Columbia’s (UBC) MD Undergraduate Program (MDUP),21 located on the traditional, ancestral, and unceded territories of the Lheidli T’enneh First Nation.22 In comparison to the other 3 MDUP sites, the NMP serves the largest landmass (Figure 1), the sparsest population (Figure 2A), the highest Indigenous population (Figure 2B), with the poorest health indicators and outcomes (Figure 2C–F).23–27 In addition, it has far fewer physicians (Figure 2G) and in comparison to the population, it has the second lowest ratio of physicians to population (Figure 2H).28 These data illustrate that people in the north have worse access to care and worse health outcomes than those in the more urban regions of the province.
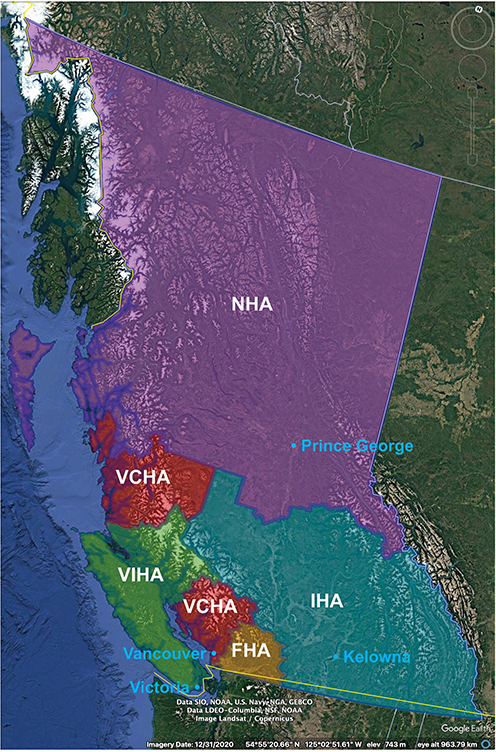 |
Figure 1 Map of British Columbia, Canada, illustrating the regions covered by the five regional health authorities, and the locations of the four academic sites of the distributed MD Undergraduate program as of 2023. NHA represents two thirds of the landmass of the province with an area of 605,525 square kilometers, similar in size to the country of France. VCHA = Vancouver Coastal Health Authority; FHA = Fraser Health Authority; VIHA = Vancouver Island Health Authority; IHA = Interior Health Authority; NHA = Northern Health Authority.23–25 |
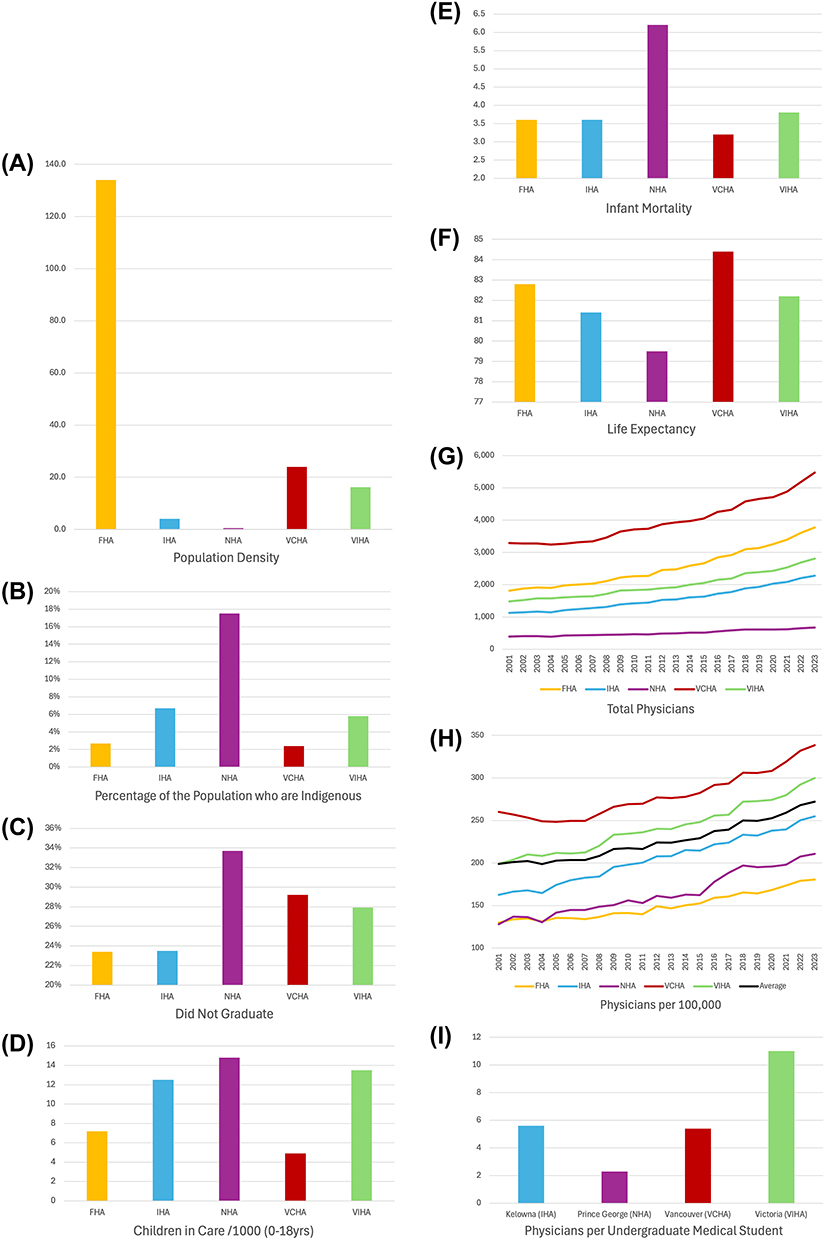 |
Figure 2 Representative demographic and population health indicators across British Columbia’s health authorities. (A) Population density (people/km2) by health authority.26,27 (B) Percentage of the population who are Indigenous by health authority.27 (C) Percentage of 18-year-olds who did not graduate high school by health authority.27 (D) Children in Care per 1000 (0–18yrs) by health authority.27 (E) Infant mortality per 1000 live births (2011–2015) by health authority.27 (F) Life expectancy at birth by health authority (2011–2015).27 (G) Total Physicians by health authority, 2001–2023.28 (H) Physicians per 100,000 residents by health authority, 2001–2023.28 (I) Physicians per undergraduate medical student, living within 100 kms of each site.29 Note the Vancouver site of the medical school is called the Vancouver-Fraser Medical Program (VFMP), indicating its responsibility to the FHA as well as VCHA. In recent years much work has been done to strengthen the VFMPs role in the FHA. The health authorities indicated here reflect the physical location of the academic site, and for all but the VFMP, the sites are responsible for training physicians to serve the needs of the health authority in which they are located. |
There is a clear connection between access to healthcare and health outcomes.3 In many ways, rural living can be healthier than urban living,30,31 and Indigeneity is clearly a strength,32,33 yet inadequate access to care counteracts these strengths and leaves rural and Indigenous peoples with health inequities. The idea that some people in urban locations do not find it concerning that rural and Indigenous peoples experience inequitable access to healthcare and inequitable health outcomes has been described as Geographic Narcissism; the devaluing of rural peoples and their lived realities, whether consciously or subconsciously.34 Similarly, the idea that rural and Indigenous peoples do not deserve health equity because of where they live, is described as an entrenched rural deficit discourse.31
Social Accountability
The UBC MDUP has a social accountability commitment to rural and Indigenous peoples as priority populations based on unmet needs and poorer health outcomes, and in accordance with accreditation requirements.35,36 With the goal to admit more rural and Indigenous students into medical school, and with the hope that these students would return to their hometowns or rural areas to practice medicine and reduce health inequities, the University of British Columbia (UBC) MD Undergraduate Program (MDUP) implemented admissions pathways for Northern and Rural students and Indigenous students in 2004.37 All students at the NMP are admitted through one of these two admission pathways. To date, the NMP has been successful in training students for northern and rural practice, with graduates 70% more likely to enter family medicine than their counterparts at the main urban campus, and 5 times as likely to practice rurally.12 At the same time, the NMP has built social and cultural capital within the clinical teaching workforce.38 It has also had broader impacts on the community within the education and health sectors, and the economy in general.39 However, these successes have required extraordinary teaching involvement from local physicians in a region that has less than half the number of physicians per medical student, compared with other sites of the MDUP (Figure 2I).29
Integrated Clerkships at UBC
If we are to attain health equity for rural and Indigenous peoples, we must not accept that their health is less important than the health of their urban counterparts. We must build capacity, address all barriers40 and ensure we are teaching the right type of medicine for practice in rural, northern, and Indigenous communities. To train students to be successful in this type of practice, which is increasingly understood to be distinct from urban family medicine, we need to ensure we are teaching the skills of rural generalist medicine.41,42
We know that providing medical students with exposure to rural communities increases their interest in practicing in those areas.43,44 This is why all students in the UBC MDUP are required to do a one-month rural family medicine rotation as part of their year 3 clinical training. However, this rotation is a short period of time within the 18 months of clinical training in the MDUP, and is not long enough for students to form connections in community or truly learn the skills of rural generalism. Longer term immersive clinical training in rural communities such as is typically provided in LICs, is associated with increased likelihood of students choosing to practice rurally, with a minimum of 6 months appearing to be required for students to achieve competence and confidence.45,46 Extended periods of time in rural clinical training allow for continuity with preceptors, patients, and location, which collectively support student learning wholistically and support development of generalist competencies.47,48 LICs are also effective in supporting student transformation and professional identity formation, due to the relationships formed between preceptors and students.48–50
Since 2004, the UBC MDUP has offered the option for a small number of students to participate in LICs, which, at UBC are referred to as Integrated Community Clerkships (ICCs).51 These sites have the capacity to provide all of the training required during clerkship, with exposure to the core clinical disciplines and the same tracking and assessment as at other sites in the provincial program, while immersing learners in a large rural or small urban community for 12 months.
Assessment in our ICCs is the same as for the rotational clerkships, except that learners in the ICC program write Comprehensive Written Exams (CWEs) twice per year, instead of block exams four times per year. These two different exams are developed from the same exam question bank and cover all the same disciplines, but the CWEs are meant to assess learning more wholistically, for learners not rotating through discipline specific “blocks.” Since 2004, UBC ICC grads have been as successful as their rotational counterparts academically, and as strong if not stronger with procedural and problem-solving skills, similar to the outcomes of other LICs.52–54
The Northern Regional Integrated Clerkship
The Northern Regional Integrated Clerkship (NRIC) was envisioned to build on the strengths of the rotational (traditional) clerkship and the ICCs, in a way that could support training in rural generalism at smaller sites across northern BC. It is a blended clerkship55 consisting of 6 months of LIC with a focus on training in rural generalism, and 6 months of rotational clerkship at the University Hospital of Northern BC (Figure 3).56 NRIC learners will be assessed using the ICC assessment plan. At full implementation in 2026, NRIC will more than double the percentage of students across the provincial program who spend time learning in an LIC.
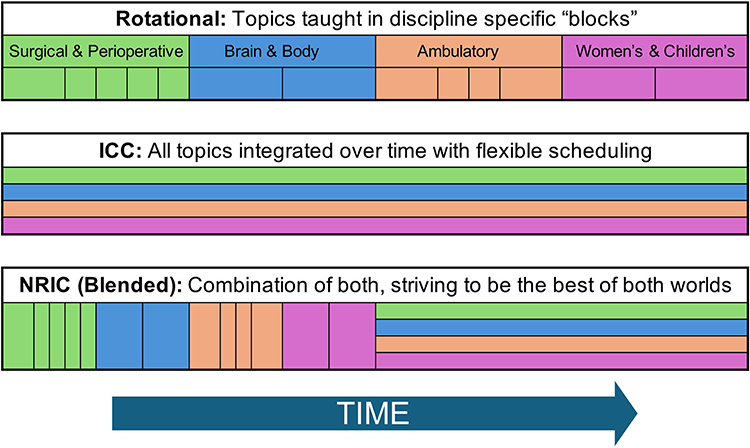 |
Figure 3 The Northern Regional Integrated Clerkship (NRIC) illustrated schematically, as compared to the traditional rotation clerkship, and the Integrated Community Clerkship offered at other sites within the University of British Columbia, MD Undergraduate Program. Note students in NRIC will either start or finish with rural community placement, such that the one half of the class will always be at the tertiary hospital (the University Hospital of Northern BC, in Prince George) for the northern site, while the other half are in rural communities. Reproduced with permission from University of Northern British Columbia. Available from: https://www.unbc.ca/northern-medical-program/northern-regional-integrated-clerkship.56 |
Various versions of blended clerkships exist around the world. Within Canada the primary example is the Northern Ontario School of Medicine’s (NOSM) blended clerkship which provides training in large rural and small urban communities, with an emphasis on family medicine and rural generalism.57,58 NRIC will build on the success of models like NOSM, using smaller rural communities, and ensure comparability to other sites (including large urban sites) of our provincial medical school. Sites were chosen based on physician availability and readiness for teaching, based on our collective experience working with these colleagues in the north, and based on the experiences of students in shorter rotations in these communities, over the past several years.
Learning Environment
The NRIC rural community sites are communities where the physicians are predominantly family physicians who are rural generalists. While the ICC sites which offer 12 months of clerkship training are in large rural or small urban communities of 15,000–80,000 people, similar to those employed by NOSM,57,58 NRIC offers clinical training in small rural communities of 600–5000 people (serving regions of 2500–8000 people)(Figure 4).56
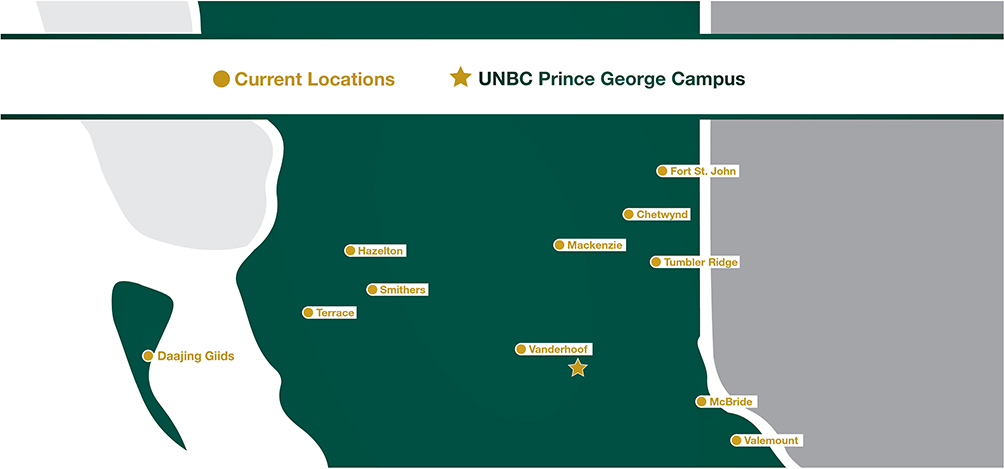 |
Figure 4 Map of the southern portion of the northern health authority, showing the main academic site (star - Prince George), the integrated community clerkships (Terrace and Fort St. John), and the NRIC rural communities (Daajing Giids, Hazelton, Smithers, Vanderhoof, Mackenzie, Chetwynd, Tumbler Ridge, McBride, and Valemount).56 Reproduced with permission from University of Northern British Columbia. Available from: https://www.unbc.ca/northern-medical-program/nric-communities. |
Site leads have been hired in each community as the point community faculty leads to interact with the program, and administrative support is being provided. A new rural faculty leadership position has also been created to provide leadership and support rural learners and faculty. All rural faculty involved are UBC clinical faculty and have access to the vast resources of our provincial faculty development office.59 Additionally, the new site leads and rural faculty lead will monitor faculty development needs in each of these communities and ensure they are met. Our experience is that faculty development is most useful when the content and facilitators understand and meet the needs expressed by the rural communities; an end user approach. Thus, we anticipate reciprocal learning as we increasingly bring rural perspectives to the central UBC (urban) office and faculty development from the large academic centre to our rural communities. Likewise, we aspire to build a community of practice amongst educators in our region, such that best practices can be shared among those working in relative isolation from one another. Through this community of practice, we aim to help sustain and support rural clinical educators. In addition to the benefits of teaching, we know that such a community of practice itself can be helpful in rural recruitment and retention.60,61
We likewise aspire to create and maintain community amongst our learners. We recognize that learners can be cautious about any new innovation and thus we will provide information and support in transition to this new clerkship. We are trying to increase rural learning opportunities along the continuum from pre-clinical learning opportunities to postgraduate education, such that the benefits of rural clinical teaching will be more familiar and attractive to our learners. We will also help the class maintain connections through the use of virtual whole class learning opportunities (described further below).
Community Consultation and Pilot Launch
The idea for developing this hybrid clerkship came as a result of consultations with rural generalist physicians in northern BC. Initial consultation was done electronically, with rural physicians known to the NMP site who were already involved in many forms of teaching for the undergraduate and postgraduate programs. Following initial enthusiasm from physicians across the region, a brief proposal was submitted to the medical school and permission was granted to begin planning in earnest (Table 1).
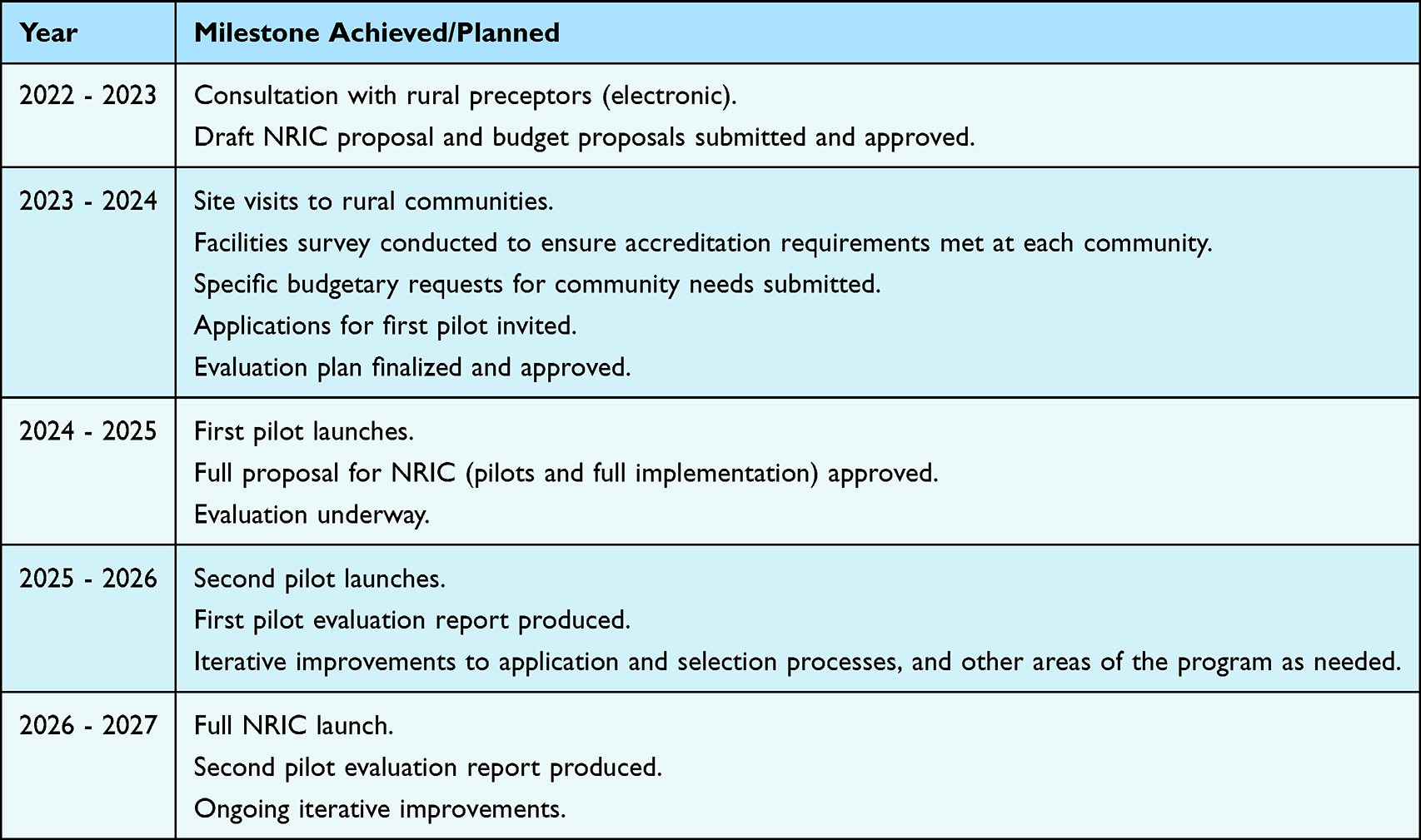 |
Table 1 Timeline of the Development and Launch of the Northern Regional Integrated Clerkship, 2022–2027 |
During the 2023–24 academic year, site visits were performed with a team of senior academic and administrative leaders from the NMP to seek input and further build community with rural physicians, and to ensure adequacy of clinical teaching and learning spaces. The rural physicians described a dissatisfaction with the current year 3 rural family medicine offering, which involves students from all sites of the UBC MDUP. This rural family medicine rotation was felt to be too short (at just 4 weeks), for anything more than just giving medical students a taste of rural medicine. Some physicians expressed that they provide students with a good time in their rural community, and the students are largely grateful, but they never come back. They were clearly concerned about the rural health workforce and their motivations to be involved in teaching were connected to the desire to recruit future colleagues. Physicians were passionate about focusing their supervisory efforts on longer clerkship experiences with students in the northern and rural pathway, who had a realistic chance of choosing to return to the same or similarly sized community.
Rural physicians unanimously, and without prompting, asked whether they could not just have one person to contact for all teaching requests. They expressed that they do a lot of different teaching at different levels of the undergraduate and postgraduate programs (Figure 5). In most small rural communities, the clinical team of 4 to 6 physicians are all involved in teaching that happens in community. These physicians are generally all keen to teach and to share with learners the special type of medical practice that they provide, yet from their perspective it is confusing working with different teams of academic and administrative leads from different areas of the medical school. They requested a single contact for their region who could coordinate all clinical teaching at that site. In response to this request, we have created an academic and administrative leadership structure that supports a local academic physician site lead and a regional administrative lead, who will be responsible for determining capacity at each small site and working with NMP staff to determine what types of teaching can be offered throughout the year. By streamlining our leadership structure to better support our clinical preceptors, we hope to expand rural clinical training for our learners throughout undergraduate and postgraduate medical training in our region.
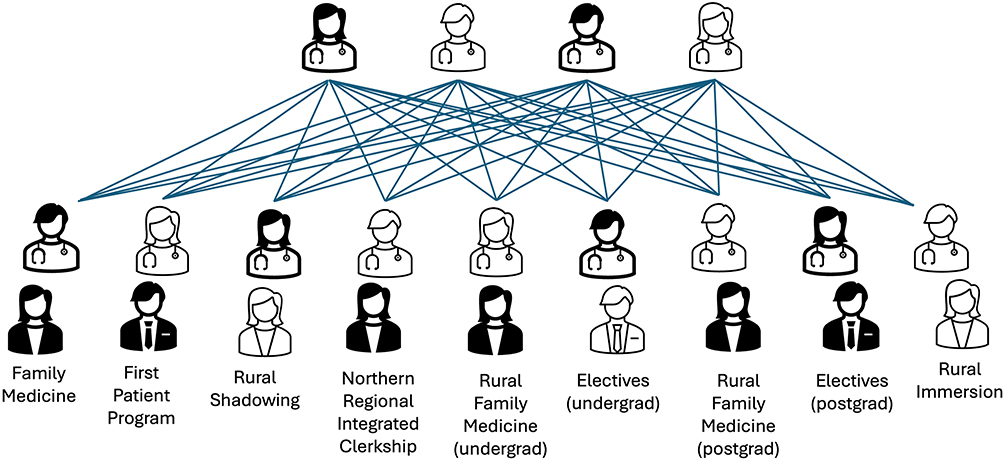 |
Figure 5 Graphical representation of the variety of academic and administrative leads associated with different types of rural teaching requested by the undergraduate MD program and postgraduate Family Medicine residency programs, and their connections to a small group of preceptors in a given rural community. Not all rural communities participate in all of these different types of teaching, but some do. Family Medicine is scheduled 1 day at a time (years 1 and 2), the First Patient program is 2 half-days in a year (years 1 and 2), Rural Shadowing is 1 weekend at a time (years 1 and 2), the Northern Regional Integrated Clerkship is 6 months (year 3), Rural Family Medicine is 4 weeks (year 3) or 4 months (postgraduate/residency), Electives are 2 or 4 weeks (year 4) or 2 or 4 months (postgraduate/residency), and Rural Immersion is 2 years (postgraduate/residency). |
The first NRIC pilot was launched during the 2023–24 academic year, largely in response to the enthusiasm of rural physicians (initial plans were to launch the first pilot the following year). It was optional, and 3 students volunteered to participate. Their experiences thus far, and the experiences of the preceptors involved, have been uniformly positive based on anecdotal evidence. We are using the resources of the UBC Faculty of Medicine Evaluation Studies Unit to assist in collecting data on the NRIC pilot. This will include assessment of the design and delivery, and outcomes. For the design and delivery, semi-structured interviews will take place with students, faculty, staff, the clerkship director, and senior administration, along with surveys for the hospital-based discipline specific site leads, after students have completed their rotations. Outcomes data will compare assessment data across all year 3 assessment modalities, between NRIC students and non-NRIC students at the NMP site, and will also include data on student perceptions of achieving learning objectives in NRIC. This evaluation will confirm whether comparability has been achieved in the NRIC clerkship, as the assessment of year 3 includes assessment of academic, clinical, and professional competencies, along with tracking exposure to the breadth of medicine expected. We are also aware that overlapping relationships are a significant component of rural life and practice, and these can enrich the experience of working rurally if the practitioner is equipped to navigate this terrain.62,63 However, the curriculum does not currently prepare students well for this aspect of rural practice which can create significant challenges for both students and preceptors at our small sites. Thus, we are also conducting research on how learners learn to navigate overlapping relationships in the NRIC pilot, as well as at other rural sites.
Lessons Learned to Date
In the initial phases of planning, we recognized some important concerns to consider. The first was that we would need students to move to the rural community, or back to the main site, half-way through the year (late November). This would be a challenge for the purposes of securing accommodation at the rural site and maintaining accommodations in Prince George. It would be inappropriate for the program to expect students to pay rent at 2 different locations concurrently. Thus, in our initial proposal we secured funding to supply housing in the rural communities and reduce this barrier for students. Secondly, we anticipated that students might feel isolated if they were the only learner at a small rural community. We therefore discussed this with rural physicians during our site visits and agreed that we would ensure that NRIC students should never be the only learner in community. This could be achieved by having more than one NRIC student at a time, or by ensuring 4th year elective students or resident physicians would be training in each community at the same time.
Through conversation with the class at the time of the first pilot, several students offered their views on why NRIC was exciting, but not something they choose to participate in. These views included concerns regarding: separation from their peers and feeling isolated; inadequate exposure to the breadth of clinical presentations and specialist medicine; and not knowing what the rural communities are like.
Learner Isolation
In addition to ensuring NRIC learners are never the only learner in community, we also sought to find ways to connect the NMP class throughout the year. A change in our assessment and Academic Half Day (AHD) approach provided this opportunity. In the rotational clerkships, AHDs are scheduled for each rotation for the students in that rotation only. At the NMP this has meant that typically 3–4 students would be receiving a given AHD at a time, and that same AHD had to be repeated multiple times throughout the year. Since NRIC is a more longitudinal training approach, we had decided to use the CWEs to assess academic knowledge during NRIC, and therefore we had an opportunity to change the AHD schedule to focus towards the CWE exams. The entire NMP class would be writing CWEs concurrently, regardless of whether they were in rural community or in Prince George at a given time. This allowed us to develop a single AHD schedule for the entire class, which would also allow the class to be together virtually for one AHD per week throughout the year, while also reducing the demand on preceptors to teach the AHD content.
Breadth of Clinical Presentations
Students also expressed concerns about adequacy of exposure to the breadth of clinical presentations required during year 3. Part of the assessment for students in clerkship requires tracking of “Must See, Must Do’s;” an inventory of 159 clinical encounters and procedures that students are required to experience throughout the year. We consulted with our rural physicians and confirmed that clerks would likely be able to complete 80–90% of these during a given 6-month period across the small rural communities, and we shared this with the Class. While the inventory is cataloged by discipline (as appropriate in an urban context), this consultation established that, in addition to the expectations for Family Medicine, students in longitudinal rural generalist training in a small rural community for 6 months would experience: all “Must See’s and Must Do’s” required by the UBC MDUP for Dermatology, Emergency Medicine, and Internal Medicine; most of the requirements for Orthopedics, Pediatrics and Surgery; and many of the requirements for Anesthesiology, Obstetrics and Gynecology, Ophthalmology, and Psychiatry. The areas that rural communities were least able to provide exposure to are mostly focused around the operating room (observing general anesthesia, operating room surgical checklist, assisting with orthopedic surgery, assisting at a major surgery), in addition to normal or complicated labour and delivery, and psychiatric aspects of alcohol or substance use, abuse, and withdrawal. Students will have these clinical experiences during the 6 month rotational component of NRIC.
Knowledge of the Communities
To help our learners gain some insight into communities that they have not visited before, we developed a website with videos and resources for each community.56 Rural physicians in each community were interviewed and asked questions about what they like about rural practice and practice at their location specifically, what they like about teaching, and what the main industry in their area is. Short videos were created for each community showing the physician(s) interviewed, the hospital, the community, and a bit of the region surrounding the community including the surrounding industry. An overview page and video were created to showcase aspects of learning in northern rural communities in general (that may also be helpful for students outside of the medical program), and pages for each community were created.
Sustaining NRIC will require continued funding for housing and rural physician leadership positions, responsiveness to the changing teaching capacities of our rural communities, ongoing faculty development which is appropriate to the rural needs and context, along with structured learner recruitment strategies. If successful, this model should be adaptable to other underserved regions in Canada and globally, and should help sustain rural generalist medical practice.
Limitations
The DME model allows for a large urban centre to contribute to medical education in a location that would otherwise be too small to support a full medical school. The smaller location contributes to the medical schools’ social accountability mandate, while ensuring the medical school considers rural context in its curriculum, policies, and governance. Operating a medical school across diverse contexts increases the impact of the medical school and the benefits to society, but also increases the complexity of operations.9 Here we describe a new blended clerkship model, which allows an emphasis on rural generalism in a way that did not previously exist across our distributed medical school, while meeting the standard of comparability of learning experiences and outcomes.
We are in the early days of the NRIC blended clerkship at the NMP. We recognize that early pilot students have self-selected for the adventure, and thus there is a selection bias that may have skewed the anecdotal data we have to date. We have yet to see how well this blended clerkship will be received by NMP classes more broadly. We anticipate challenges may emerge as we scale the program and students may be less uniformly enthusiastic for the experience. In light of this, we are gathering more rigorous program evaluation data and conducting research to help ensure we identify opportunities to improve the clerkship, and act on these. As we learn more about the challenges and opportunities, we expect to make iterative changes to ensure that NRIC is living up to our expectations, along with the expectations of our students and rural preceptors.
Ethics
This is not a research study. Consultation with physicians and students was done for the purposes of program evaluation and development. This manuscript is written in accordance with Canada’s Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans—TCPS 2 (2022) and with the 1964 Helsinki Declaration and its later amendments.
Acknowledgments
The authors wish to thank the preceptors across Northern BC who have contributed to the vision for this new clerkship, the students who have offered feedback and been willing to try something new, along with the staff who have worked hard to help ensure the success of it.
Disclosure
The authors report no conflicts of interest in this work.
References
1. The rural road map for action: directions. mississauga, on: advancing rural family medicine: the canadian collaborative taskforce; 2017. Available from: https://www.cfpc.ca/CFPC/media/Resources/Rural-Practice/Rural-Road-Map-Directions-ENG.pdf.
2. MacPhail C, Maurice SB. Attractions and barriers to rural practice: impact of an interprofessional rural immersion experience, in British Columbia, Canada. Discov Health Syst. 2024;3:87. doi:10.1007/s44250-024-00153-y
3. Weinhold I, Gurtner S. Understanding shortages of sufficient health care in rural areas. Health Policy. 2014;118(2):201–214. doi:10.1016/j.healthpol.2014.07.018.
4. United Nations sustainable development goals [homepage on the Internet]. Goal 3: ensure healthy lives and promote well-being for all at all ages. United Nations. Available from: https://www.un.org/sustainabledevelopment/health/.
5. Boelen C, Heck JE. Defining and measuring the social accountability of medical schools. Geneva: World Health Organization; 1995. Available from: https://iris.who.int/handle/10665/59441.
6. United Nations [homepage on the Internet]. United Nations declaration on the rights of indigenous peoples (UNDRIP); 2008. Available from: https://www.un.org/esa/socdev/unpfii/documents/DRIPS_en.pdf.
7. Truth and reconciliation commission of Canada [homepage on the Internet]. Calls to action of the truth and reconciliation commission; 2015. Available from: https://www2.gov.bc.ca/assets/gov/british-columbians-our-governments/indigenous-people/aboriginal-peoples-documents/calls_to_action_english2.pdf.
8. Lee J, Walus A, Billing R, Hillier LM. The role of distributed education in recruitment and retention of family physicians. Postgrad Med J. 2016;92(1090):436–440. doi:10.1136/POSTGRADMEDJ-2015-133577.
9. Snadden D. Distributed medical education: what is the point? Med Educ. 2018;52(11):1108–1110. doi:10.1111/medu.13734.
10. Bates J, Grand’Maison P, Banner SR, Lovato CY, Eva KW. Exploring the contributions of combined model regional medical education campuses to the physician workforce. Acad Med. 2021;96(3):409–415. doi:10.1097/ACM.0000000000003560.
11. Campbell DG, McGrail MR, O’Sullivan B, Russell DJ. Outcomes of a 1-year longitudinal integrated medical clerkship in small rural Victorian communities. Rural Remote Health. 2019;19(2):4987. doi:10.22605/RRH4987.
12. Lovato CY, Hsu HCH, Bates J, Casiro O, Towle A, Snadden D. The regional medical campus model and rural family medicine practice in British Columbia: a retrospective longitudinal cohort study. CMAJ Open. 2019;7(2):E415–E420. doi:10.9778/cmajo.20180205.
13. Worley P, Martin A, Prideaux D, Woodman R, Worley E, Lowe M. Vocational career paths of graduate entry medical students at Flinders University: a comparison of rural, remote and tertiary tracks. Med J Aust. 2008;188(3):177–178. doi:10.5694/j.1326-5377.2008.tb01567.x.
14. Nichols D, Cockell J, Lemoine D, Konkin J. The rural integrated community clerkship: a vital stretch in the Alberta rural physician workforce pipeline. Can Med Educ J. 2023;14(5):59–63. doi:10.36834/cmej.73944.
15. Kitchener S, Day R, Faux D, et al. Longlook: initial outcomes of a longitudinal integrated rural clinical placement program. Aust J Rural Health. 2015;23(3):169–175. doi:10.1111/ajr.12164
16. Zink T, Center B, Finstad D, et al. Efforts to graduate more primary care physicians and physicians who will practice in rural areas: examining outcomes from the university of Minnesota–Duluth and the rural physician associate program. Acad Med. 2010;85(4):599–604. doi:10.1097/acm.0b013e3181d2b537
17. Green LA, Fryer GE, Yawn BP, Lanier D, Dovey SM. The Ecology of Medical Care Revisited. N Engl J Med. 2001;344(26):2021–2025. doi:10.1056/NEJM200106283442611.
18. Committee on accreditation of Canadian medical schools [homepage on the Internet]. CACMS standards and elements. 8.7 comparability of education/assessment; 2023. Available from: https://cacms-cafmc.ca/wp-content/uploads/2023/03/CACMS-Standards-and-Elements-AY-2024-2025.pdf.
19. Hsu HCH, Martin T, Teunissen PW, Eva KW. Conceptualizing educational comparability in distributed health professions education: a scoping review. Acad Med. 2024;99(6):691–698. doi:10.1097/ACM.0000000000005679.
20. UBC Faculty of Medicine, MD Undergraduate Program [homepage on the Internet]. Program Sites; 2025. Available from: https://mdprogram.med.ubc.ca/about/distributed-program-sites/.
21. University of Northern British Columbia [homepage on the Internet]. Northern Medical Program. 2025. Available from: https://www.unbc.ca/northern-medical-program.
22. Lheidli T’enneh [homepage on the Internet]. Welcome to Lheidli T’enneh first nation; 2025. Available from: https://www.lheidli.ca.
23. British Columbia ministry of health [homepage on the Internet]. B.C. Ministry of Health Geographies Portal; 2023. Available from: https://experience.arcgis.com/experience/5f44ce2df1e2471b8570f1a2ba2801a6/page/Page-1?views=Welcome.
24. British Columbia Data Catalogue [homepage on the Internet]. Health authority boundaries, download KML ground overlay file; 2023. Available from: https://catalogue.data.gov.bc.ca/dataset/health-authority-boundaries/resource/8baaeeb6-5692-42ff-9cca-a3dd43826458.
25. European Union [homepage on the Internet]. France. Available from: https://european-union.europa.eu/principles-countries-history/eu-countries/france_en.
26. BC Stats [homepage on the Internet]. Population estimates & projections for British Columbia. Available from: https://bcstats.shinyapps.io/popApp/.
27. BC Community Health Data [homepage on the Internet]. Search by Location. Available from: http://communityhealth.phsa.ca/GetTheData/SearchByLocation.
28. Canadian Institute for Health Information [homepage on the Internet]. Supply, distribution and migration of physicians in Canada, 1971-2023 — historical data (XLSX); 2024. Available from: https://www.cihi.ca/sites/default/files/document/supply-distribution-migration-physicians-in-canada-1971-2023-data-tables-en.xlsx.
29. The College of Physicians and Surgeons of BC [homepage on the Internet]. Serving the public by regulating physicians and surgeons; 2025. Available from: https://www.cpsbc.ca.
30. Goodwin RD, Taha F. Global health benefits of being raised in a rural setting: results from the national comorbidity survey. Psychiatry Clin Neurosci. 2014;68(6):395–403. doi:10.1111/pcn.12144.
31. Lueebe A, Rutherford Z, Diminic S, Roovers H, Patel M, Whiteford H. Taking a strengths-based approach to mental health in rural communities: a systematic literature review. Aust N Z J Public Health. 2024;48:6. doi:10.1016/j.anzjph.2024.100201
32. Chandler MJ, Lalonde CE. Cultural continuity as a protective factor against suicide in first nations youth. Horizons. 2008;10:68–72.
33. Aldred T. Indigeneity is healing. BCMJ. 2024;66:73.
34. Fors M. Geographical narcissism in psychotherapy: countermapping urban assumptions about power, space, and time. Psychoanal Psychol. 2018;35(4):446–453. doi:10.1037/pap0000179.
35. UBC Faculty of Medicine, Undergraduate Medical Education [homepage on the Internet]. Social responsibility and accountability of the ubc md undergraduate program, a renewal of our social responsibility and accountability commitment; 2021. Available from: https://mednet.med.ubc.ca/files/2022/11/Social-Responsibility-Accountability-MD-Undergraduate-Program.pdf.
36. Committee on Accreditation of Canadian Medical Schools [homepage on the Internet]. CACMS standards and elements. 1.1.1 Social accountability; 2023 Available from: https://cacms-cafmc.ca/wp-content/uploads/2023/03/CACMS-Standards-and-Elements-AY-2024-2025.pdf.
37. UBC Faculty of Medicine, MD Undergraduate PROGRAM [homepage on the Internet]. Pathways to medicine; 2025. Available from: https://mdprogram.med.ubc.ca/admissions/before-you-apply/pathways-to-medicine/.
38. Hanlon N, Halseth G, Snadden D. “We can see a future here”: place attachment, professional identity, and forms of capital mobilized to deliver medical education in an underserviced area. Health Place. 2010;16(5):909–915. doi:10.1016/j.healthplace.2010.04.016.
39. Toomey P, Lovato C, Hanlon N, Poole G, Bates J. Impact of a regional distributed medical education program on an underserved community: perceptions of community leaders. Acad Med. 2013;88(6):811. doi:10.1097/ACM.0b013e318290f9c7.
40. Maganty A, Byrnes ME, Hamm M, et al. Barriers to rural health care from the provider perspective. Rural Remote Health. 2023;23(2):7769. doi:10.22605/RRH7769
41. Schubert N, Evans R, Battye K, Gupta TS, Larkins S, McIver L. International approaches to rural generalist medicine: a scoping review. Hum Resour Health. 2018;16(1):62. doi:10.1186/s12960-018-0332-6.
42. Ross BM, Taylor K, Button B, Kilbertus F, Cameron E. How early clinical experiences in rural communities influence student learning about rural generalism considered through the lens of educational theory. Canadia Med Educ J. 2024;15(2):6–13. doi:10.36834/cmej.77409.
43. Woloschuk W, Tarrant M. Does a rural educational experience influence students’ likelihood of rural practice? Impact of student background and gender. Med Educ. 2002;36(3):241–247. doi:10.1046/j.1365-2923.2002.01143.x.
44. Brooks RG, Walsh M, Mardon RE, Lewis M, Clawson A. The roles of nature and nurture in the recruitment and retention of primary care physicians in rural areas: a review of the literature. Acad Med. 2002;77(8):790–798. doi:10.1097/00001888-200208000-00008.
45. Abid Y, Connell CJW, Sijnja B, Verstappen AC, Poole P. National study of the impact of rural immersion programs on intended location of medical practice in New Zealand. Rural Remote Health. 2020;20(4):5785. doi:10.22605/RRH5785
46. Woolley T. Intended rural career modalities of final-year James Cook university medical students. Aust J Rural Health. 2019;27(5):412–418. doi:10.1111/ajr.12546.
47. Hirsh DA, Ogur B, Thibault GE, Cox M. “Continuity” as an organizing principle for clinical education reform. N Engl J Med. 2007;356(8):858–866. doi:10.1056/NEJMsb061660.
48. Cuncic C, Regehr G, Frost H, Bates J. It’s all about relationships: a qualitative study of family physicians’ teaching experiences in rural longitudinal clerkships. Perspect Med Educ. 2018;7(2):100–109. doi:10.1007/s40037-018-0416-y.
49. Beattie J, Binder M, Beks H, Fuller L. Influence of a rural Longitudinal Integrated Clerkship on medical graduates’ geographic and specialty decisions: a constructivist grounded theory study. BMC Med Educ. 2024;24(1):795. doi:10.1186/s12909-024-05793-5.
50. Brown MEL, Whybrow P, Kirwan G, Finn GM. Professional identity formation within longitudinal integrated clerkships: a scoping review. Med Educ. 2021;55(8):912–924. doi:10.1111/medu.14461.
51. UBC Faculty of Medicine, MD Undergraduate Program [homepage on the Internet]. Integrated community clerkships; 2025. Available from: https://mdprogram.med.ubc.ca/about/integrated-community-clerkships/.
52. Fleming B, MacKenzie M. Integrated community clerkship: medical education at UBC and the challenge of underserved communities. BCMJ. 2013;55:192–195.
53. Thistlethwaite JE, Bartle E, Chong AAL, et al. A review of longitudinal community and hospital placements in medical education: BEME Guide No. 26. Med Teach. 2013;35(8):e1340–e64. doi:10.3109/0142159X.2013.806981
54. Walters L, Greenhill J, Richards J, et al. Outcomes of longitudinal integrated clinical placements for students, clinicians and society. Med Educ. 2012;46(11):1028–1041. doi:10.1111/j.1365-2923.2012.04331.x
55. Worley P, Couper I, Strasser R, et al. A typology of longitudinal integrated clerkships. Med Educ. 2016;50(9):922–932. doi:10.1111/medu.13084
56. University of Northern British Columbia [homepage on the Internet]. Northern Rural Clinical Learning. 2025. Available from: https://www.unbc.ca/northern-medical-program/northern-rural-clinical-learning.
57. Strasser R, Hogenbirk JC, Minore B, et al. Transforming health professional education through social accountability: canada’s Northern Ontario school of medicine. Med Teach. 2013;35(6):490–496. doi:10.3109/0142159X.2013.774334
58. Strasser R, Cheu H. Needs of the many: northern Ontario School of Medicine students’ experience of generalism and rural practice. Can Fam Physician. 2018;64(6):449–455.
59. UBC Faculty of Medicine, Faculty Development [homepage on the Internet]. Welcome to the office of faculty development; 2025. Available from: https://facdev.med.ubc.ca.
60. Soles TL, Ruth Wilson C, Oandasan IF. Family medicine education in rural communities as a health service intervention supporting recruitment and retention of physicians: advancing rural family medicine: the canadian collaborative taskforce. Can Fam Physician. 2017;63(1):32–38.
61. Hudson JN, Thomson B, Weston K, Knight-Billington P. When a LIC came to town: the impact of longitudinal integrated clerkships on a rural community of healthcare practice. Rural Remote Health. 2015;15(3):3333. doi:10.22605/RRH3333.
62. Gingerich A, Volkenburg KV, Maurice SB, Simpson C, Roots R. Urban ideals and rural realities: physiotherapists navigating paradox in overlapping roles. Med Educ. 2021;55(10):1183–1193. doi:10.1111/medu.14476.
63. Gingerich A, Simpson C, Roots R, Maurice SB. “Juggle the different hats we wear”: enacted strategies for negotiating boundaries in overlapping relationships. Adv Health Sci Educ. 2024;29(3):813–828. doi:10.1007/s10459-023-10282-3.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.