Back to Journals » Cancer Management and Research » Volume 17

Advancing Prognostic Accuracy Beyond Classical N Staging in Colorectal Cancer: An Observational Cohort Study to Define a Lymph Node Ratio Based Risk Score
Authors Mangone L ![]() , Morabito F, Tripepi G, D'Arrigo G, Bisceglia I
, Morabito F, Tripepi G, D'Arrigo G, Bisceglia I ![]() , Marinelli F
, Marinelli F ![]() , Pinto C, Giorgi Rossi P, Neri A
, Pinto C, Giorgi Rossi P, Neri A
Received 15 January 2025
Accepted for publication 22 July 2025
Published 15 November 2025 Volume 2025:17 Pages 2807—2819
DOI https://doi.org/10.2147/CMAR.S515434
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Lucia Mangone,1 Fortunato Morabito,2 Giovanni Tripepi,3 Graziella D’Arrigo,3 Isabella Bisceglia,1 Francesco Marinelli,1 Carmine Pinto,4 Paolo Giorgi Rossi,1 Antonino Neri5
1Epidemiology Unit, Azienda Unità Sanitaria Locale-IRCCS di Reggio Emilia, Reggio Emilia, 42122, Italy; 2Gruppo Amici Dell’Ematologia Foundation-GrADE, Reggio Emilia, 42122, Italy; 3Istituto di Fisiologia Clinica del CNR di Reggio Calabria, Consiglio Nazionale delle Ricerche, Reggio, Calabria, Italy; 4Medical Oncology Unit, Azienda Unità Sanitaria Locale-IRCCS Di Reggio Emilia, Reggio Emilia, 42122, Italy; 5Scientific Directorate, Azienda Unità Sanitaria Locale–IRCCS di Reggio Emilia, Reggio Emilia, 42122, Italy
Correspondence: Lucia Mangone, Epidemiology Unit, Azienda Unità Sanitaria Locale–IRCCS di Reggio Emilia, Reggio Emilia, 42122, Italy, Email [email protected]
Purpose: Lymph node involvement is critical for colorectal cancer (CRC) staging and prognosis. The lymph node ratio (LNR), defined as the ratio of metastatic to total examined lymph nodes, has shown promise as a superior prognostic metric compared to traditional TNM staging and total lymph node yield (LNY). This study compared the prognostic value of LNR, N staging, and LNY and developed an LNR-based survival risk score (LNR-SRSCRC). Secondary objectives included evaluating the impact of multidisciplinary team (MDT) care and molecular markers (KRAS, NRAS, BRAF) on survival.
Patients and Methods: A population-based cohort of 2013 CRC cases (2013– 2018) from the Reggio Emilia Cancer Registry was analyzed. Prognostic models, including T-LNR-M, TNM, and T-LNY-M, were compared using Harrell’s C-index, Akaike Information Criterion (AIC), and net reclassification improvement (NRI). Patients were randomly assigned to training (1026) and validation (987) cohorts. Multivariable analysis identified significant predictors, and a survival risk score (SRSCRC) was validated. The study also assessed the independent prognostic role of MDT care and molecular markers.
Results: The T-LNR-M model outperformed TNM (C-index 71% vs 70%; NRI 4.7%, P = 0.002) and T-LNY-M (C-index 71% vs 70%) with the lowest AIC (8356). Predictors of mortality included T4 stage, LNR, metastasis, and age > 78.6 years. LNR-SRSCRC stratified patients into low, intermediate, intermediate-high, and high-risk groups with distinct survival probabilities. Validation confirmed its prognostic accuracy (C-index 71.4%). MDT care was associated with significantly improved survival (HR = 1.63; P = 0.047), while molecular markers (KRAS, NRAS, BRAF) were not significant.
Conclusion: LNR provides superior prognostic value compared to N staging or LNY. The LNR-SRSCRC enhances risk stratification and, together with MDT care, may enhance personalized CRC management. Prospective validation is warranted.
Keywords: colorectal cancer, survival prediction, TNM staging, LNR-based survival risk score colorectal cancer, multidisciplinary team prognostic models
Introduction
Colorectal cancer (CRC) is a major global health concern and one of the leading causes of cancer-related morbidity and mortality.1 It ranks as the third most common malignancy worldwide, with approximately two million new cases annually.2 Incidence varies by region, with higher in developed countries, reflecting differences in lifestyle, diet, healthcare access, and screening programs.
CRC is clinically and molecularly heterogeneous, contributing to outcome variability.3 Between 2017 and 2021, incidence was 36.5 per 100,000 annually, with an age-adjusted mortality rate 12.9 per 100,000 per year.4 Prognosis is stage-dependent, with five-year survival rates ranging from 91% in early to just 16% in advanced-stages.4
The TNM (Tumor, Node, Metastasis) staging system, developed by the American Joint Committee on Cancer and the Union for International Cancer Control (AJCC-UICC), is central to CRC management informing prognosis and therapy, as reflected in international guidelines.5,6 It performs well in early and late stages, but prognosis is more heterogeneous in stage II and III disease.7
The “T” (Tumor) classification is based on the depth of invasion rather than on the tumor size Kornprat et al found that larger tumors were linked to worse outcomes, in colon cancer, stressing the need for site-specific size cut-offs.8 Feng et al supported this, especially in node-positive cases,9 while Crozier et al highlighted systemic inflammation, not size, as a survival predictor.10
The “N” (Node) classification is determined by the number of positive lymph nodes.11 More involved nodes predict poorer outcomes and guide adjuvant therapy decisions.
However, increasing evidence suggests that quantitative nodal metrics, such as the total number of lymph nodes retrieved (LNY)12–14 and the lymph node ratio (LNR),15 may offer enhanced prognostic accuracy by accounting for variability in surgical quality and pathological assessment. These measures are not yet included in standard nodal staging despite their clinical relevance.
Distant metastasis (M1) is a major predictor of poor outcomes, with 5-year OS rates below 10%.11 Identifying metastasis guides systemic treatments, including chemotherapy and targeted therapies.16,17 Advances in imaging (PET-CT, MRI) have enhanced detection of metastases¹7.
Histopathological features (grading, lymphovascular, and perineural invasion) refine CRC prognosis.18,19 Tumor location also matters: right-sided CRC exhibits different molecular profiles and clinical behavior compared to the left-sided or rectum.20
However, patient-specific factors also impact outcomes. Age influences both prognosis and treatment:21 younger patients often have aggressive disease, yet often respond more favorably to therapy, while older patients frequently present with comorbidities that complicate treatment and worsen survival.21 Socioeconomic factors, healthcare access, and disparities in screening contribute to mortality differences.22,23
Multidisciplinary teams (MDTs) have enhanced CRC outcomes by facilitating collaborative decisions and optimizing care: MDT involvement improves survival, especially in advanced CRC.24–27
Molecular and genetic profiling are now the key in personalized CRC care. New guidelines recommend testing molecular biomarkers like KRAS, NRAS, and BRAF to guide prognosis, and therapy.28,29 KRAS/NRAS mutations (∼40%) confer resistance to anti-EGFR therapy (eg, cetuximab, panitumumab) and worsen survival.28 BRAF V600E (8–10%) signals poor prognosis and aggressive disease, especially in metastasis.29
In this context, our study aims to evaluate whether nodal metrics beyond traditional TNM staging can improve prognostic stratification in CRC. Specifically, we compared the prognostic value of LNY and LNR to identify the most reliable indicator of overall survival and constructed a LNR-based survival risk score. We also explored the role of molecular alterations and MDT decision-making as complementary factors in refining risk prediction.
Materials and Methods
Study Setting
The data for this population-based cohort study were obtained from the Reggio Emilia Cancer Registry (RE-CR). The procedures for conducting epidemiological analyses of the RE-CR data have been approved by the Reggio Emilia Ethics Committee (Protocol no. 2014/0019740 dated 04/08/2014). The RE-CR, which has been updated until the end of 2021 and covers a population of 532,000 individuals, is considered a high-quality cancer registry. It boasts a high rate of microscopic confirmation (93.4% for CRC) and a Death Certificate Only (DCO) rate below 0.1%.30 In the province of Reggio Emilia, a screening program targeting women and men aged 50 to 69 with biennial FOBT (Fecal Occult Blood Test) has been implemented since 2005. The participation rate is over 65% and the impact on incidence, with a marked decrease, has been observed and described.31
Data Sources
The RE-CR study utilized a comprehensive array of data sources including pathology reports, discharge records, mortality statistics, and diagnostic reports obtained from general practitioners and laboratories. All incident CRC cases diagnosed from 2013 to 2018 were included. This population-based retrospective cohort consisted of 2013 CRC cases, classified according to the International Classification of Diseases for Oncology, 3rd Edition (ICD-O3). Colorectal cancer cases included in this study exhibited a relatively stable distribution over the examined years. Specifically, there were 316 cases reported in 2013 356 cases in 2014, 348 cases in 2015, 329 in 2016, 340 in 2017, and 324 in 2018. Patients underwent treatment following the guidelines in place at the time of diagnosis. Information regarding variables of interest is summarized in Table 1.
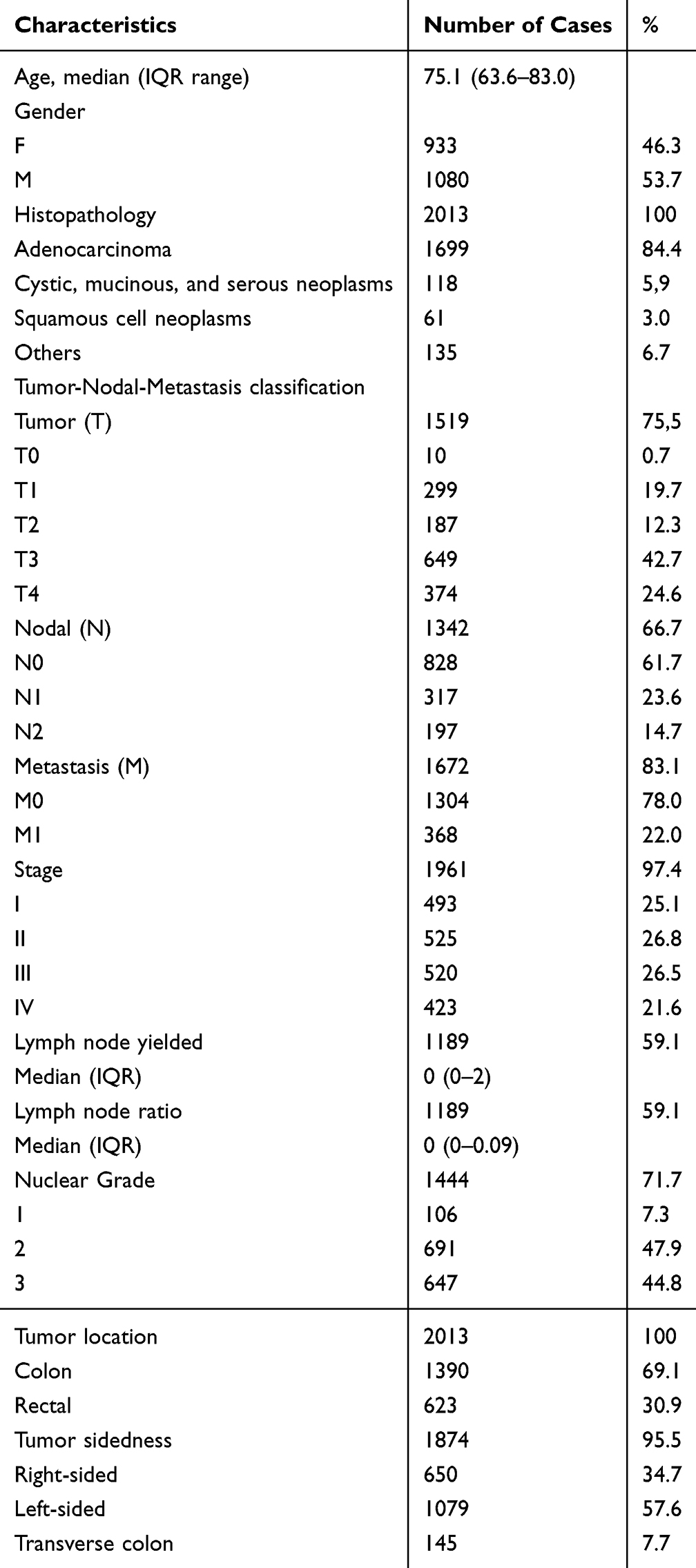 |
Table 1 Main Clinical and Histopathological Characteristics of the 2013 Colorectal Cancer Enrolled Between 2013–2018 in the Reggio Emilia Cancer Registry |
Multidisciplinary Team
In the years 2017–2018, diagnostic and therapeutic protocols for CRC were updated to enhance the MDT decision-making process. The revisions established evidence-based protocols, clarified roles among healthcare services, and ensured consistent cancer-specific MDT consultations. This framework aimed to integrate best practices, streamline provider communication, and promote patient-centered care. Process and outcome quality indicators are used to monitor care, with annual feedback provided to healthcare teams. The MDT, including oncologists, radiologists, surgeons, and other specialists, meets weekly to decide the best treatment for each patient, considering age, social factors, and tumor characteristics.27
Study Design and Statistical Analysis
In this study, all prognostic factors were collected from patient archives reflecting the status at diagnosis or MDT evaluation, to minimize bias related to retrospective data collection.
The analysis was conducted three phases. First, prognostic models incorporating the lymph node ratio (LNR) (T-LNR-M) were developed and compared to the conventional TNM and T-LNY-M (total lymph nodes yielded) models using the entire cohort of 1665 cases with complete data for all variables. Second, a survival risk score for colorectal cancer (SRSCRC) was developed by integrating additional variables into the prognostic model. This approach allowed us to assess the robustness and predictive accuracy of each model in a more comprehensive prognostic setting, incorporating factors that may influence outcomes beyond nodal metrics alone. The cohort was randomly divided into a training set (1026 patients) and a validation set (987 patients) in a 1:1 ratio using a computerized random number generator to minimize selection bias. The training cohort was used for model development and calibration, while the validation cohort was used to independently test model performance and generalizability. Finally, ancillary analyses were performed on the entire cohort to evaluate the contribution of mutations and MDT involvement to prognosis.
Data are expressed as absolute numbers and percentages, or median and interquartile range (IQR). OS was calculated from the date of diagnosis until death from any cause. OS was censored at the last date of patient follow-up. The relationship between risk factors and the outcome variables was investigated by univariable and multiple Cox regression analysis. On univariable models, tested covariates for death included patient age, gender, and each component of the TNM classification (tumor size [T], nodal involvement [N], other lymph node metrics such as LNY and LNR, and metastasis status [M]), as well as clinical stages (I–IV), nuclear grading (NG) and histological classification. All prognostic indicators significantly associated with univariable analysis were jointly introduced into the same multiple Cox regression model. Data were expressed as the hazard ratio (HR), 95% confidence interval (CI), and P-value. OS was estimated by the Kaplan-Meier method followed by a Log rank test. Given the multiple comparisons between survival curves (n=16), we applied a Bonferroni correction to adjust the significance threshold, setting it at 0.003 (0.05/16) to control for type I error. The optimal threshold of age for discriminating patients who died from those who survived was identified by the Receiver Operating Characteristic (ROC) curve analysis.
To calculate the survival risk score for CRC (SRSCRC), a regression coefficient-based scoring model was employed, following the methodology described by Mehta et al.32 In this approach, regression coefficients of independent prognostic factors identified through multivariable analysis were first summed. Each coefficient was then normalized by dividing by the total sum and multiplied by 100 to derive the percentage weight of each prognostic variable. This percentage weight ranged from 0 for unexposed patients to a value proportionate to the regression coefficient in exposed patients. Individual patient scores were calculated by summing these percentage weights across all relevant variables, generating a prognostic score from 0 (indicating no exposure to risk factors) to 100% (indicating full exposure to all risk factors). The prognostic accuracy of the models was quantified by calculating Harrell’s C-statistic, ranging from 0.5 (no discrimination) to 1.0 (perfect discrimination), the explained variation in mortality (R2, ie, an index combining calibration and discrimination), and Akaike information criterion (AIC).33,34 The net reclassification index (NRI) was also used to assess at what extent N, LNR, and LNY are useful to reclassify patients as at risk or not at risk of death when added to a simpler model based on T and M. A value of P<0.05 was considered statistically significant.
Statistical calculations were performed using SPSS for Windows v.21 (IBM, Chicago, Illinois, USA) and Stata 16 (StataCorp, Texas, USA).
Ethics
The Italian legislation identifies Cancer Registries as collectors of personal data for surveillance purposes without explicit individual consent. The approval of a research ethics committee was not required, as this study is a descriptive analysis of individual data without any intervention on patients.
Results
Patients’ Characteristics
Table 1 summarizes the clinical and histopathological features of 2013 CRC cases recorded from 2013 to 2018. The median age was 75.1 years, with a slight predominance of male sex (53.7%) and adenocarcinoma histology (84.4%) Among 1519 cases with T classification, T3 was most frequent (43%), followed by T4 (24.6%), T1 (19.7%), T2 (12.3%), and T0 (0.7%). Of the 1342 cases with N classification, 61.7% were N0, 23.6% N1, and 14.7% N2. Distant metastases (M1) were present in 22% of patients.Stage distribution (1961 cases) was balanced across stages I–IV (25.1%, 26.8%, 26.5%, and 21.6%, respectively). Grades 2 (47.9%) and 3 (44.8%) were most common.Colon tumors represented 69% of cases, with 1079 out of 1874 localized to the left side. Case numbers remained stable over time. Among cases with lymph node data (59.1%), both median LNY and LNR were 0 (IQR 0–2).
Comparative Prognostic Performance of TNM, T-LNY-M, and T-LNR-M Models
Given the prognostic potential of lymph node metrics, we compared three distinct Cox models—TNM, T-LNY-M, and T-LNR-M in 1165 colorectal cancer patients, (446 deaths). The TNM model had a Harrell’s C-index of 70%, explained variation of 29.5%, and NRI (due to N) of 3.8±1.0% (P=0.003). The T-LNY-M model performed similarly, (Harrell C-index of 70.0%, explained variation 29.1%, and NRI (due to LNY) 2.7±1.0%, (P=0.025). In contrast, the T-LNR-M model outperformed both with a Harrell C-index of 71%, explained variation of 31.2%, and NRI (due to LNR) 4.7±1.0% (P=0.002). Akaike weights confirmed T-LNR-M (AIC=5721.27) as the best model (>95% probability), outperforming TNM (AIC=5736.29) and T-LNY-M (AIC=5738.90). These findings support LNR as a stronger prognostic tool than both N stage and LNY in CRC.
Cross-Validation of Prognostic Model
Given the results of this comparison, we aimed to further evaluate the prognostic performance of the T-LNR-M model within a framework that included additional variables. A total of 1026 patients were assigned to the training cohort for model development, and the remaining 987 patients were assigned to the validation cohort for independent testing of model performance. A detailed comparison of the two cohorts did not show any significant differences in characteristics depicted in Table 1.
Training Cohort
Univariable Analyses of Overall Survival
After a median follow-up of 3.1 years (IQR range 1.0–5.2 years), 485 patients died. Median OS was 5.8 years (95% CI 4.9–6.7 years), with 60.8% of patients still alive at 3 years (Figure 1). Tumor extension significantly impacted OS: T4 tumors had the poorest outcomes, while T3 carried a 1.7-fold higher risk, than T0-T2 groups (grouped due to minor differences; Supplementary Figures 1 and 2). Median OS was not reached for the T0-T2 it was 7.5 years for T3 and 1.5 years for T4 patients. The 3-year OS rates were 86.7% for T0-T2 patients, 74.5% for those with T3, and markedly lower at 30.7% for the T4 group (Figure 2A).
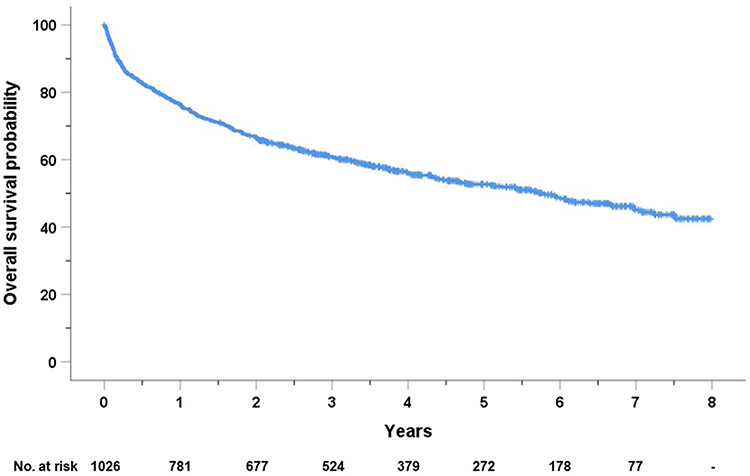 |
Figure 1 Kaplan-Maier curve of overall survival of the training cohort of 1026 colorectal cancer. |
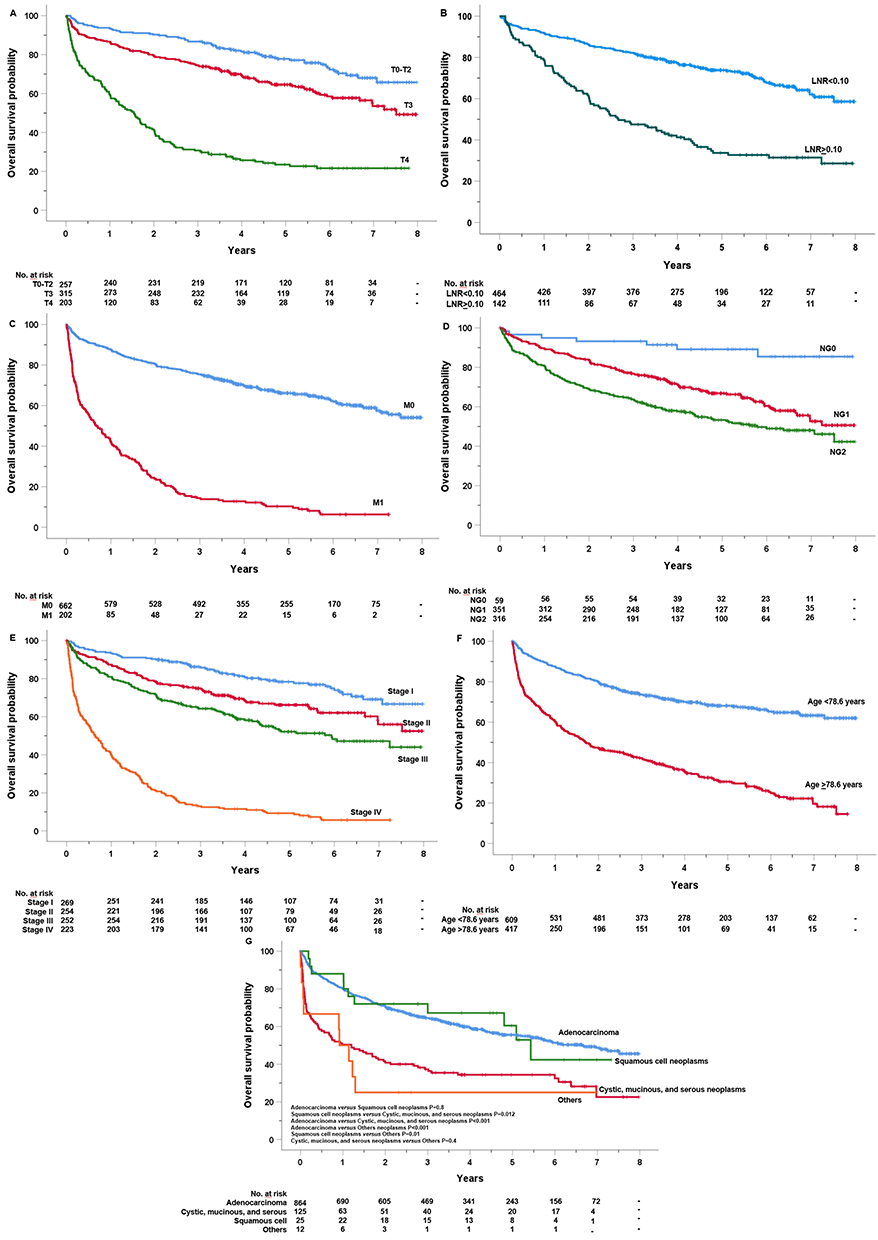 |
Figure 2 Kaplan-Maier curve of overall survival of the training cohort of colorectal cancer by (A) size and extend of the primary tumor (T) p<0.001, (B) lymphnode ratio (LNR) cut-off value p<0.001, (C) distant metastasis (M) p<0.001, (D) nuclear grade p<0.001, (E) stage p<0.001, (F) age threshold of 78.6 years p<0.001, and (G) histopathology. |
LNR, as a continuous variable, demonstrated strong association with OS (HR: 14.9, 95% 95% CI: 8.8–25.2, P<0.0001). ROC curve analysis identified an optimal LNR cut-off of 0.10 (Supplementary Figure 3). Below this threshold, 3-year OS rate was 82.3% versus 47.5% above. Median OS was not reached in the LNR<0.10 group, but was only 2.7 months in the >0.10 group (Figure 2B).
Distant metastasis (M1) conferred a 6-fold higher risk versus M0 (Supplementary Figure 1), with 3-year OS rate of 14.4% versus 75.4% (Figure 2C).
Nuclear grade (NG) was also predictive NG3 tumors had a 5.4-fold and a 3.5-fold increased risk compared to NG1 and NG2, respectively (Supplementary Figure 1). The 3-year OS rates were 93.2%, 76.6%, and 63.7% for NG1, NG2, and NG3, respectively, with the median OS not reached for NG1 or NG2, but significantly reduced to 5.8 months for NG3 (Figure 2D).
Stage IV was the most significant predictor of poor survival, with a 10.5-fold higher mortality risk compared to Stage I, while Stage II and III conferred respectively 1.7- and 2.0-fold higher risk (Supplementary Figure 1). The 3-year OS rates for Stages I, II, III, and IV were 85.8%, 74.9%, 64.2%, and 13%, respectively, with median OS unreached in I and II, 5.9 years in III and less than 7 months in IV (Figure 2E).
Age >78.6 years, as detected by ROC curve analysis (Supplementary Figure 4) tripled the mortality risk (HR 3.2, 95% CI 2.7–3.9, P < 0.001), with 3-year OS rate of 42.2% versus 73.6% in younger patients. The median OS was 1.7 years for older patients, while it was not reached for younger ones (Figure 2F).
Histological subtypes also influenced survival. Non-adenocarcinomas showed 2.3–3.1 times higher risk versus adenocarcinomas (Supplementary Figure 2). Median OS was notably lower across these subtypes: adenocarcinoma 6.6 years, squamous 5.4 years, cystic, mucinous, and serous 1.2 years, and those classified as “others” just 0.9 years (Figure 2G). Due to overlap, adenocarcinoma and squamous cell neoplasms were grouped for subsequent analyses; so were mucinous/serous and “other” types. This approach aimed to streamline the analysis and enhance statistical power by reducing subgroup heterogeneity.
After applying the Bonferroni correction (adjusted significance threshold: 0.003), all comparisons between survival curves remained statistically significant.
Multivariable Analysis of Overall Survival
When all variables having a significant impact on OS at univariable analysis were jointly introduced into the same multivariable Cox model, fitted in 573 out of 1026 patients (ie, 55.8% of total cases), tumor stages T4 (HR=3.8, 95% CI 1.7–8.3; P<0.001), LNR (HR=2.3, 95% CI 1.5–3.4; P<0.001), the presence of distant metastasis (M1) (HR=18.3, 95% CI 2.1–156; P=0.008), and age>78.6 years (HR=3.6, 95% CI 2.7–4.7; P<0.001), remained independently associated with death. Conversely, NG (P for trend=0.5), stage (P for trend=0.1), and histological subtypes (P for trend=0.1) failed to maintain their independent prognostic roles after multiple data adjustments.
Prognostic LNR-Based Survival Scoring System for Overall Survival
Next, based on the multivariable results, we calculated the LNR-derived survival risk scores for OS (referred to as LNR-SRSCRC, see Supplementary Table 1) in 603 cases from no risk to maximum risk exposure. Subsequently, cases were divided into four distinct risk categories: a low-risk group with 250 cases (41.4%); an intermediate-risk group comprising 159 cases (26.4%); an intermediate-high-risk group containing 138 cases (22.9%); and a high-risk group, with 56 cases (9.3%) (Figure 3). The 3- and 6-year OS probabilities were 94.4% and 86.9% for low-risk (HR=1, reference group), 76.7% and 57.1% for intermediate-risk (HR=4.7, 95% CI 3.0–7.4, P<0.001), 57.2% and 36.1% for intermediate-high-risk (HR=7.8, 95% CI 5.1–12.1, P<0.001), and 18.3% and 4.7% for high-risk (HR=24.4, 95% CI 15.2–39.4, P<0.001). Unlike the low-risk which did not reach the median timeline, the estimated median OS was 6.1 years (± 0.457 SEM) for intermediate-risk groups, 4.0 years (± 0.471) for intermediate-high risk, and 1.0 years (± 0.295 SEM) for high-risk cases. Of note, the LNR-SRSCRC had a Harrell C-index of 75.6% and an explained variation of 45.8% to predict mortality.
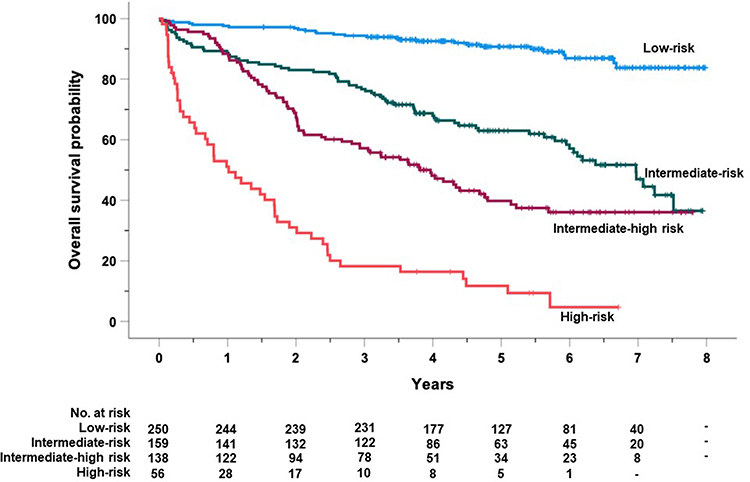 |
Figure 3 Kaplan-Maier curve of overall survival of 603 colorectal cancer (training cohort) clustered by the final LNR-derived survival risk score for colorectal cancer (LNR-SRSCRC). Low risk group: score=0; Intermediate risk group: score=20 p<0.001; Intermediate high risk group: score>20 <=55 p=0.002; high risk group: score >55 p<0.001. |
Validation of LNR-SRSCRC
This study included an additional validation cohort of 987 cases. Prognostic indicators based on the LNR-SRSCRC classification were assessed in 575 patients, with OS outcomes illustrated in Figure 4. Of these, 235 (40.9%) patients were categorized as low risk, 156 (27.1%) as intermediate risk, 143 (24.9%) as intermediate-high risk, and 41 (7.1%) as high risk. The 3- and 6-year OS probabilities were 92.3% and 82.8% for the low-risk group (HR=1, reference), 74.3% and 47.6% for the intermediate-risk group (HR=3.8, 95% CI: 2.5–5.7, P<0.001), 55.6% and 36.0% for the intermediate-high-risk group (HR=5.8, 95% CI: 3.9–8.7, P<0.001), and 26.8% and 22.0% for the high-risk group (HR=11.1, 95% CI: 6.8–17.9, P<0.001). Examining the survival curves, the estimated median OS was 5.7 years (± 0.448 SEM) for the intermediate-risk group, 3.4 years (± 0.500 SEM) for the intermediate-high-risk group, and 1.8 years (± 0.265 SEM) for the high-risk group, while the OS curve for the low-risk group did not reach the median OS. Remarkably, the LNR-SRSCRC had a Harrell C-index of 71.4% and an explained variation of 30.4% to predict mortality.
 |
Figure 4 Kaplan-Maier curve of overall survival of 575 colorectal cancer (validation cohort) clustered by the final LNR-derived survival risk score for colorectal cancer (LNR-SRSCRC). Intermediate risk group p<0.001; Intermediate high risk group p=0.002; high risk group p<0.001. |
Ancillary Analyses
We conducted ancillary analyses on the entire cohort, focusing on the impact of KRAS, NRAS, and BRAF mutations, and MDT management on mortality, and their potential to refine stratification within the LNR-SRSCRC. Due to limited complete data, findings should be interpreted cautiously.
Univariable analysis Cox analysis indicated that NRAS mutations (n=313) had an HR of 0.9 (95% CI: 0.7–1.2, P=0.7), KRAS mutations (n=361) had an HR of 1.7 (95% CI: 0.7–4.2, P=0.2), and BRAF mutations (n=310) showed an HR of 1.0 (95% CI: 0.7–1.6, P=0.9). These findings suggest that none of these mutations were associated with mortality in our cohort.
Among 619 evaluable cases, 365 received MDT care, which was linked to better survival (HR 2.6, 95% CI 2.0–3.3, P<0.001). In the multivariable model (n=232) including LNR-SRSCRC and MDT, the score stratified risk effectively: intermediate- (HR 4.5), intermediate-high- (HR 9.1), and high-risk (HR 22.1) groups showed significantly increased mortality versus baseline (all P<0.001). MDT also retained independent prognostic value (HR 1.626; 95% CI: 1.006–2.629; p = 0.047).
Discussion
Evaluating lymph node involvement is pivotal in CRC staging and prognosis, with the current N classification serving as a central determinant of the TNM system to predict patient outcomes and treatment decisions. However, the N classification, based solely on the absolute number of metastatic lymph nodes (N0–N2), has some limitations. It fails to consider variability in lymphadenectomy quality and the total lymph node yield, both of which significantly impact staging accuracy and prognostic reliability. Recent research suggests that alternative metrics, such as total LNY and LNR should be taken into consideration.12–15
Emerging evidence highlights the lymph node ratio (LNR)—the ratio of metastatic to total examined lymph nodes—as a more refined metric LNR captures not only the extent of nodal metastasis but also the adequacy of surgical lymph node harvest, providing a more accurate reflection of tumor burden and surgical quality.15,35–38 The Rosenberg et al study36 identified different LNR cut-off values that stratify patients into distinct prognostic groups. Schiffmann et al37 demonstrated that LNR allows for superior stratification of CRC patients compared to N staging, particularly when comprehensive lymphadenectomy ensures a sufficient total lymph node yield. LNR allows for finer stratification of patient outcomes compared to N staging alone, addressing the variability in total lymph node yield. This finding underscores the importance of establishing optimal cutoffs for LNR to ensure its broad applicability across clinical and research settings.
Our data confirm and extend these observations. The LNR-based T-LNR-M model outperformed both the traditional TNM and the LNY-based T-LNY-M models in prognostic accuracy, achieving higher discrimination (Harrell’s C-index 71% vs 70%) and explained variation (31.2% vs 29.5%). Moreover, the net reclassification improvement (NRI) of 4.7% (P=0.002) compared to TNM highlights the added value of LNR in refining risk predictions. Remarkably, the analysis of Akaike weights reveals that the model including LNR (AIC=5721.27) has >95% chance to be the best model when compared to the other two candidate models (TMN, AIC=5736.29; LNY, AIC=5738.90). These results are consistent with studies such as Naidu et al,38 which found that LNR provided superior survival predictions across both early and late-stage CRC, particularly in stage IV patients. The study calls for integrating LNR into staging systems to improve risk stratification in advanced CRC.
Building on the insights provided by LNR, we developed and validated a LNR-based survival risk score (LNR-SRSCRC) incorporating age as the sole additional prognostic factor. This score categorizes patients into four risk groups—low, intermediate, intermediate-high, and high risk—each with distinct survival trajectories. Validation in an independent, population-based cohort reinforced the robustness of this system, with 3-year OS rates ranging from 94.4% in the low-risk group to 18.3% in the high-risk group, providing a tool that can more accurately stratify patients based on OS outcomes. The distinct risk categories identified by the score are highly informative, allowing clinicians to predict survival trajectories with greater precision. For example, the low-risk group exhibited 3- and 6-year OS probabilities of 94.4% and 86.9%, respectively, with no median OS reached, signaling an excellent prognosis. On the other hand, patients in the high-risk group had significantly worse survival probabilities, with a 3-year OS rate of just 18.3% and an estimated median OS of only 1.0 year. This stark difference in survival underscores the model’s potential to identify patients who may benefit from more aggressive interventions as well as those who can safely avoid unnecessary treatments.
The intermediate- and intermediate-high-risk groups also revealed clear distinctions in outcomes, with median OS for these groups estimated at 6.1 years and 4.0 years, respectively. These results demonstrate that the LNR-SRSCRC goes beyond the simplicity of traditional staging systems by providing a more refined, personalized risk assessment. The model’s ability to stratify patients within these groups based also on a simple yet powerful metric like lymph node ratio significantly enhances prognostic accuracy. Moreover, the calculated HRs—4.7 for the intermediate-risk group and up to 24.4 for the high-risk group—further validate the model’s strength in predicting mortality, highlighting its clinical applicability.
Validation of the LNR-SRSCRC in a separate cohort of 987 cases adds to the robustness of the model, confirming its ability to generalize across diverse patient populations. In the validation cohort, the OS probabilities remained consistent with the initial findings, supporting the tool’s reliability. The Harrell C-index of 71.4% in the validation cohort demonstrates that the LNR-SRSCRC is effective in distinguishing between patients at different levels of risk, while the explained variation of 30.4% indicates that the model can account for a substantial portion of the variance in mortality risk. These findings further strengthen the credibility of the LNR-SRSCRC and its potential as a clinically useful prognostic tool.
Despite its strengths, the LNR-SRSCRC has areas for potential optimization. The reliance on lymph node yield (LNY) for calculating LNR highlights the need to standardize lymphadenectomy techniques across institutions. Variability in lymph node harvesting quality can impact LNR accuracy, and the incomplete reporting of LNY further complicates its use; in our cohort, LNY data were unavailable for approximately 30% of cases. Harmonizing surgical practices and improving reporting standards are essential to enhance the model’s reliability and reproducibility.
As an ancillary observation, this study reaffirms the association between MDT participation and improved CRC outcomes. Consistent with our previous findings,27 patients managed within an MDT framework demonstrated significantly improved OS. The analysis of the process indicators suggests that the better outcomes are attributable to coordinated treatment planning, timely interventions, and comprehensive follow-up care. In this new analysis, we have shown that MDT management retained its independent prognostic value even when integrated into a multivariable model that included our scoring system. On the other hand, the LNR-SRSCRC scoring system maintained its granular ability to stratify patients across different risk levels in this multivariable analysis, further enhancing its predictive accuracy for prognosis. Moreover, the lack of association between NRAS, and BRAF mutations and OS in this study should be considered in light of the relatively small sample size, as well as the rather imprecise estimate of the KRAS effect. Furthermore, while these mutations are well-established prognostic markers in CRC,28,29 the limited and extremely selected number of cases analyzed here may have introduced a selection bias possibly hindering meaningful associations. The decision to test patients is probably a negative prognostic factor itself, thus not allowing to correctly assess the prognostic value of the mutations in the population of all CRC patients. Additionally, treatment heterogeneity, including the use of targeted therapies, may have influenced survival outcomes and confounded the relationship between these mutations and OS. These limitations highlight the need for further research on the prognostic role of molecular markers in CRC.
Conclusion
In conclusion, this study underscores the clinical utility of LNR and the LNR-SRSCRC in CRC management, introducing a refined TNM staging system that substitutes the N component with LNR and integrates age as a key prognostic factor. Looking forward, the adoption of LNR-based metrics and risk scores into clinical guidelines will require international consensus on optimal cutoffs and standardization of lymphadenectomy practices and reporting. Exploring the integration of LNR-based tools into electronic health records and decision-support systems could also enhance their adoption in clinical practice. Incorporating emerging biomarkers and leveraging digital health technologies will also be crucial for enhancing the precision and scalability of these tools.
Data Sharing Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to ethical and privacy issues; requests for data must be approved by the Ethics Committee after the presentation of a study protocol.
Ethics Statement
The data accessed complied with relevant data protection and privacy regulations.
According to the Italian legislation (Presidente del Consiglio dei Ministri. Decreto del Presidente del Consiglio dei Ministri, 3/3/2017,41 Identificazione dei sistemi di sorveglianza e dei registri di mortalità, di tumori e di altre patologie.17A03142, GU Serie Generale n.109 del (12-05-2017). Available at: https://www.gazzettaufficiale.it/eli/id/2017/05/12/17A03142/sg last access: January 14, 2025), population-based cancer registries collect pseudonymised personal data for surveillance purposes that do not need the collection of explicit individual consent, without any direct or indirect intervention on patients, therefore the approval of a research ethics committee was not required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was partially supported by the Italian Ministry of Health - Ricerca Corrente Annual Program 2026.
Disclosure
Dr Paolo Giorgi Rossi reports non-financial support from Roche, Hologic, Becton Dickinson, ICAD, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Bray F, Laversanne M, Sung H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–263. doi:10.3322/caac.21834
2. Baidoun F, Elshiwy K, Elkeraie Y, et al. Colorectal cancer epidemiology: recent trends and impact on outcomes. Curr Drug Targets. 2021;22:998–1009. doi:10.2174/18735592MTEx9NTk2y
3. Yang Z, Wang X, Zhou H, Jiang M, Wang J, Sui B. Molecular complexity of colorectal cancer: pathways, biomarkers, and therapeutic strategies. Cancer Manag Res. 2024;16:1389–1403. doi:10.2147/CMAR.S481656
4. National Cancer Institute. Cancer Stat Facts: colorectal Cancer. Available online: https://seer.cancer.gov/statfacts/html/colorect.html. (
5. Amin MB, Greene FL, Edge SB, et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67:93–99. doi:10.3322/caac.21388
6. Quirke P, Williams GT, Ectors N, Ensari A, Piard F, Nagtegaal I. The future of the TNM staging system in colorectal cancer: time for a debate? Lancet Oncol. 2007;8:651–657. doi:10.1016/S1470-2045(07)70205-X
7. Schneider NI, Langner C. Prognostic stratification of colorectal cancer patients: current perspectives. Cancer Manag Res. 2014;6:291. doi:10.2147/CMAR.S38827
8. Kornprat P, Pollheimer MJ, Lindtner RA, Schlemmer A, Rehak P, Langner C. Value of tumor size as a prognostic variable in colorectal cancer: a critical reappraisal. Am J Clin Oncol. 2011;34(1):43–49. doi:10.1097/COC.0b013e3181cae8dd
9. Feng H, Lyu Z, Zheng J, et al. Association of tumor size with prognosis in colon cancer: a Surveillance, Epidemiology, and End Results (SEER) database analysis. Surgery. 2021;169:1116–1123. doi:10.1016/j.surg.2020.11.011
10. Crozier JE, McMillan DC, McArdle CS, et al. Tumor size is associated with the systemic inflammatory response but not survival in patients with primary operable colorectal cancer. J Gastroenterol Hepatol. 2007;22:2288–2291. doi:10.1111/j.1440-1746.2006.04792.x
11. Brierley JD, Gospodarowicz MK, Wittekind C. TNM Classification of Malignant Tumours. Hoboken, NJ, USA: John Wiley & Sons; 2017.
12. Chang GJ, Rodriguez-Bigas MA, Skibber JM, Moyer VA. Lymph node evaluation and survival after curative resection of colon cancer: systematic review. J Natl Cancer Inst. 2007;99:433–441. doi:10.1093/jnci/djk092
13. Le Voyer TE, Sigurdson ER, Hanlon AL, et al. Colon cancer survival is associated with increasing number of lymph nodes analyzed: a secondary survey of intergroup trial INT-0089. J Clin Oncol. 2003;21:2912–2919. doi:10.1200/JCO.2003.05.062
14. Chen K, Collins G, Wang H, Toh JWT. Pathological features and prognostication in colorectal cancer. Curr Oncol. 2021;28:5356–5383. doi:10.3390/curroncol28060447
15. Pyo JS, Kim JH, Lee SY, Baek TH, Kang DW. Metastatic lymph node ratio (mLNR) is a useful parameter in the prognosis of colorectal cancer; a meta-analysis for the prognostic role of mLNR. Medicina. 2019;55:673. doi:10.3390/medicina55100673
16. Mainali BB, Valenzuela CD, Moaven O, et al. Resection versus resection with ablation: analysis from the colorectal liver operative metastasis international collaborative. J Surg Oncol. 2024;130(3):516–522. doi:10.1002/jso.27789
17. Guimarães RB, Pacheco EO, Ueda SN, et al. Evaluation of colon cancer prognostic factors by CT and MRI: an up-to-date review. Abdom Radiol. 2024;49(11):4003–4015. doi:10.1007/s00261-024-04373-x
18. Barresi V, Reggiani Bonetti L, Ieni A, Caruso RA, Tuccari G. Histological grading in colorectal cancer: new insights and perspectives. Histol Histopathol. 2015;30:1059–1067. doi:10.14670/HH-11-633
19. Johncilla M, Yantiss RK. Histology of colorectal carcinoma: proven and purported prognostic factors. Surg Pathol Clin. 2020;13(3):503–520. doi:10.1016/j.path.2020.05.008
20. Petrelli F, Tomasello G, Borgonovo K, et al. Prognostic survival associated with left-sided vs right-sided colon cancer: a systematic review and meta-analysis. JAMA Oncol. 2017;3:211–219. doi:10.1001/jamaoncol.2016.4227
21. Kellokumpu I, Kairaluoma M, Mecklin JP, et al. Impact of age and comorbidity on multimodal management and survival from colorectal cancer: a population-based study. J Clin Med. 2021;10(8):1751. doi:10.3390/jcm10081751
22. Maida M, Dahiya DS, Shah YR, et al. Screening and surveillance of colorectal cancer: a review of the literature. Cancers. 2024;16(15):2746. doi:10.3390/cancers16152746
23. Rouhafzay A, Yousefi J. Geographical disparities in colorectal cancer in canada: a review. Curr Oncol Rep. 2024;26(10):1249–1257. doi:10.1007/s11912-024-01574-x
24. Munro A, Brown M, Niblock P, Steele R, Carey F. Do Multidisciplinary Team (MDT) processes influence survival in patients with colorectal cancer? A population-based experience. BMC Cancer. 2015;15:686. doi:10.1186/s12885-015-1683-1
25. Segelman J, Singnomklao T, Hellborg H, Martling A. Differences in multidisciplinary team assessment and treatment between patients with stage IV colon and rectal cancer. Color Dis. 2009;11:768–774. doi:10.1111/j.1463-1318.2008.01648.x
26. Rollet Q, Bouvier V, Moutel G, et al. Multidisciplinary team meetings: are all patients presented and does it impact quality of care and survival—A registry-based study. BMC Health Serv Res. 2021;21:1032. doi:10.1186/s12913-021-07022-x
27. Mangone L, Marinelli F, Bisceglia I, et al. Characteristics and outcomes of colorectal cancer patients cared for by the multidisciplinary team in the Reggio Emilia Province, Italy. Cancers. 2024;16(13):2390. doi:10.3390/cancers16132390
28. Koncina E, Haan S, Rauh S, Letellier E. Prognostic and predictive molecular biomarkers for colorectal cancer: updates and challenges. Cancers. 2020;13:12. doi:10.3390/cancers13010012
29. Seligmann JF, Fisher D, Smith CG, et al. Investigating the poor outcomes of BRAF-mutant advanced colorectal cancer: analysis from 2530 patients in randomised clinical trials. Ann Oncol. 2017;28(3):562–568. doi:10.1093/annonc/mdw645
30. Mangone L, Borciani E, Michiara M, et al. I tumori nelle province dell’Area Vasta Emilia Nord: piacenza, Parma, Reggio Emilia e Modena: anni 2013–2014. Registri Tumori. 2025;111(1):71–78. doi:10.1177/03008916241298810
31. Mangone L, Marinelli F, Bisceglia I, Braghiroli MB, Damato A, Pinto C. Five-year relative survival by stage of breast and colon cancers in northern Italy. Front Oncol. 2022;12:982461. doi:10.3389/fonc.2022.982461
32. Mehta HB, Mehta V, Girman CJ, Adhikari D, Johnson ML. Regression coefficient-based scoring system should be used to assign weights to the risk index. J Clin Epidemiol. 2016;79:22–28. doi:10.1016/j.jclinepi.2016.03.031
33. Tripepi G, Heinze G, Jager KJ, Stel VS, Dekker FW, Zoccali C. Risk prediction models. Nephrol Dial Transplant. 2013;28(8):1975–1980. doi:10.1093/ndt/gft095
34. D’Arrigo G, Gori M, Pitino A, Torino C, Roumeliotis S, Tripepi G. Statistical methods to assess the prognostic value of risk prediction rules in clinical research. Aging Clin Exp Res. 2021;33(2):279–283. doi:10.1007/s40520-020-01542-y
35. Vaccaro CA, Im V, Rossi GL, et al. Lymph node ratio as prognosis factor for colon cancer treated by colorectal surgeons. Dis Colon Rectum. 2009;52(7):1244–1250. doi:10.1007/DCR.0b013e3181a65f0b
36. Rosenberg R, Friederichs J, Schuster T, et al. Prognosis of patients with colorectal cancer is associated with lymph node ratio: a single-center analysis of 3026 patients over a 25-year time period. Ann Surg. 2008;248(6):968–978. doi:10.1097/SLA.0b013e318190eddc
37. Schiffmann L, Eiken AK, Gock M, Klar E. Is the lymph node ratio superior to the union for international cancer control (UICC) TNM system in prognosis of colon cancer? World J Surg Oncol. 2013;11:79. doi:10.1186/1477-7819-11-79
38. Naidu K, Chapuis PH, Connell L, Chan C, Mjfx R, Ng KS. Lymph node ratio prognosticates overall survival in patients with stage IV colorectal cancer. Tech Coloproctol. 2024;28(1):115. doi:10.1007/s10151-024-02984-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Alcohol Use, Coronary Heart Disease and Hypertension Modify the Predictive Accuracy of Pre-Operative CEA for TNM Staging in Chinese Colorectal Cancer Patients
Kuai D, Cheng J, Li R, Gao X, Sun L, Li Y, Sun W, Hu Y, Li C, Xu B
Cancer Management and Research 2025, 17:3373-3382
Published Date: 31 December 2025