Back to Journals » Cancer Management and Research » Volume 18

Advancing Precision Medicine in Non-Small Cell Lung Cancer Diagnostics in a Southeast Asian Country
Authors Poh ME ![]() , Thiagarajan M, Tho LM, Ho GF, Mohammad N, Tan WC, How SH
, Thiagarajan M, Tho LM, Ho GF, Mohammad N, Tan WC, How SH
Received 29 October 2025
Accepted for publication 30 December 2025
Published 13 January 2026 Volume 2026:18 570997
DOI https://doi.org/10.2147/CMAR.S570997
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Mau Ern Poh,1 Muthukkumaran Thiagarajan,2 Lye Mun Tho,3 Gwo Fuang Ho,4 Norhasanah Mohammad,5 Wuan Chin Tan,5 Soon Hin How6
1Department of Medicine, Faculty of Medicine, Universiti Malaya, Kuala Lumpur, Wilayah Persekutuan, Malaysia; 2Department of Radiotherapy and Oncology, Hospital Kuala Lumpur, Kuala Lumpur, Wilayah Persekutuan, Malaysia; 3Oncology Department, Beacon Hospital, Petaling Jaya, Selangor, Malaysia; 4M. Kandiah Faculty of Medicine and Health Sciences, Universiti Tunku Abdul Rahman, Kuala Lumpur, Wilayah Persekutuan, Malaysia; 5Medical Affairs, Pfizer, Kuala Lumpur, Wilayah Persekutuan, Malaysia; 6Faculty of Medicine, International Islamic University Malaysia Medical Centre, Kuantan, Pahang, Malaysia
Correspondence: Mau Ern Poh, Department of Medicine, Faculty of Medicine, Universiti Malaya, Kuala Lumpur, Wilayah Persekutuan, Malaysia, Tel +6 03-79494422, Email [email protected]
Purpose: Next-generation sequencing (NGS) has transformed molecular diagnostics and precision oncology by enabling broad genomic profiling and informed treatment selection for non-small cell lung cancer (NSCLC). However, adoption in Southeast Asia remains limited, particularly in public healthcare settings. This study aimed to assess the landscape of NGS testing for NSCLC in Malaysia, identify barriers, and explore strategies clinicians use to improve patient access.
Patients and Methods: A descriptive, cross-sectional survey comprising 18 questions was distributed to clinical oncologists and respiratory physicians across Malaysia over an eight-week period. The survey collected data on clinical experience with NGS, testing practices, perceived barriers, and access strategies. Descriptive statistics were used for analysis, and associations between healthcare sectors (public vs private) and NGS usage frequency were evaluated using the Chi-square test.
Results: Seventy-one clinicians participated - 67.6% clinical oncologists and 32.4% respiratory physicians. Private hospitals had the highest NGS uptake (38.5% testing all NSCLC patients), with the lowest in Ministry of Health (MoH) institutions (8.3%) (p< 0.0001). Among oncologists, 45.8% used NGS for all or nearly all patients. For respiratory physicians, 35.3%, mainly from MoH, used it most of the time. NGS results were more frequently available in private referrals. Most private clinicians (84.6%) rated NGS accessibility as excellent. Key barriers included cost of testing and therapies, limited availability, long turnaround times, insufficient tissue, and unclear guidelines. Strategies to improve access included industry-subsidized programs, insurance coverage, and clinical trial enrolment.
Conclusion: NGS adoption for NSCLC in Malaysia varies significantly across healthcare settings. Public hospitals face substantial barriers, particularly related to cost and access to testing and therapies. Addressing these challenges will require coordinated efforts across policy, infrastructure, clinician training, and public-private partnerships. This study offers key insights into the Malaysian NGS landscape and supports broader access to precision oncology.
Keywords: genomic access, next generation sequencing, non-small cell lung cancer, Southeast Asia
Introduction
Non-small cell lung cancer (NSCLC) accounts for a significant proportion of lung cancer cases and encompasses three main subtypes: adenocarcinoma, squamous cell carcinoma (SCC), and large cell carcinoma (LCC). Despite significantly contributing to the Malaysian cancer burden,1,2 national data specifying the different lung cancer subtypes is limited. A review of lung cancer research estimated that 80% of patients with lung cancer in Malaysia have NSCLC.3 The prevalence of lung adenocarcinoma has increased significantly, making it the most common subtype regardless of sex or smoking status.4
Advances in targeted therapies have improved outcomes for advanced NSCLC, supported by biomarker testing for epidermal growth factor receptor (EGFR) mutations, anaplastic lymphoma kinase (ALK) rearrangement, and other less common alterations.5–8 EGFR mutations are estimated to occur more frequently in Asians than in the Western population (up to 30% vs 14%, respectively).9,10 While ALK rearrangements are reported in 4–5% in the Asian and non-Asian populations, some studies suggest that up to 7% of the lung cancer population in Asia harbor the mutation.8,11–13 In Malaysia, ALK-positive advanced NSCLC was reported in 4.1% of 1581 NSCLC patients registered in the National Cardiovascular and Thoracic Surgical Database.8 EGFR mutations were found in up to 45.7% of NSCLC cases,2,14 and ALK rearrangements occurred in 13% of EGFR wild-type lung adenocarcinoma patients.2 However, testing for targetable mutations in Malaysia is limited by the high cost of targeted therapies,8,14 and if done, is commonly performed using single-gene assays, polymerase chain reaction (PCR) for EGFR and fluorescence in situ hybridization (FISH) and immunohistochemistry (IHC) for ALK.2,8 Single-gene testing is limited by its narrow scope, sequential workflow, potential tissue depletion, and higher overall costs, particularly when using methods like Sanger sequencing, which require additional assays for exon-level alterations.15–18
Next-generation sequencing (NGS), introduced in 2005, has transformed molecular diagnostics by enabling high-throughput, parallel sequencing in a single run.19 Compared to traditional methods, NGS is faster, more cost-effective, and provides broader genomic insights, supporting matched targeted therapies that have improved outcomes in cancers such as NSCLC.5,20 It also conserves tissue, identifies resistance mechanisms, and offers multi-panel testing that can inform treatment selection, response prediction, and prognosis.21–24 NGS has also shown potential for early detection in early-stage lung cancer.6
The clinical utility of NGS in NSCLC has been increasingly demonstrated across Asia. Studies from countries such as India,21 Korea,25 China,26,27 and Taiwan28 highlight its ability to identify actionable mutations and improve overall survival through precision oncology. In Malaysia, targeted NGS panels identified actionable targets in 76.2% of solid tumor cases, including NSCLC, with rapid turnaround times of three days.22 In Singapore, upfront NGS was shown to be cost-effective, enabling faster access to personalised therapies in an EGFR-mutant predominant population.29 In Malaysia, a joint consensus by the College of Pathologists, Academy of Medicine Malaysia, the Malaysian Thoracic Society (MTS), and the Malaysian Oncological Society (MOS) recommends using multiplexed NGS panels over single-gene tests to identify actionable mutations beyond EGFR, ALK, and ROS proto-oncogene 1 (ROS1).30
However, despite its clinical value and endorsement, NGS uptake in Malaysia remains limited, potentially due to cost and accessibility barriers, as the test is only available in private laboratories. This reflects a broader regional pattern where. Although countries such as Japan and South Korea offer reimbursement for NGS in metastatic cancers, the degree of financial support differs. In Japan, coverage is provided mainly for patients with advanced disease who have already undergone standard therapy, with individuals contributing roughly 10–30% of the test cost and the remainder subsidized by the government according to age and income level. In South Korea, national schemes cover about 50% for selected solid tumors when testing is performed at diagnosis or recurrence. By comparison, uptake remains low in settings such as Thailand, Hong Kong, Malaysia, and the Philippines, where NGS is not reimbursed and patients must bear the full out-of-pocket expense.31
This study aims to determine the current landscape of NGS testing for NSCLC in Malaysia, ascertain major barriers in the utilization of NGS testing, explore strategies clinicians use to improve patient access to NGS, and propose additional initiatives to enhance accessibility. While clinicians and stakeholders have widely recognized limited uptake, no formal studies have quantified these challenges in the Malaysian context. By addressing this gap, the study seeks to provide evidence to guide ongoing discussions and initiatives aimed at strengthening precision oncology services for NSCLC in Malaysia, while also offering insights that could support future national cancer control planning or reimbursement-related considerations.
Materials and Methods
This descriptive study utilized a survey to assess the clinical experience, current practices and opinions regarding NGS testing in the management of NSCLC in Malaysia.
A survey of 18 questions was developed using Microsoft Forms to gather information on the NSCLC clinical experience, NGS testing practices, and clinicians’ opinions on NGS. The survey targeted clinical oncologists, respiratory physicians, and internal medicine specialists. It was distributed via the MTS, Lung Cancer Network Malaysia (LCNM), and a professional WhatsApp group for clinical oncologists. The survey period lasted eight weeks.
To maintain respondent anonymity, demographic information was limited to the clinician’s specialty, years of experience in their specialty, and primary place of work. The choice of primary place of work was either in the public sector, which comprises the Ministry of Health (MoH), Ministry of Higher Education (MoHE), or Ministry of Defense (MoD) hospitals or private hospitals. The survey explored three main areas: clinical experience with NGS, opinions on its utility, and strategies to overcome challenges in accessing it.
To assess clinical experience, respondents were asked about their frequency of performing NGS in the first-line treatment settings, the proportion of referred patients presenting with completed NGS testing, and the accessibility of NGS tests at their primary place of work. Additionally, clinicians were asked to identify the primary reasons for not performing NGS for their patients.
Opinions on NGS were evaluated through questions on whether respondents would use NGS if cost and accessibility were not barriers, their assessment of NGS accessibility within their practice, and the main challenges encountered in accessing it for patients. To understand how clinicians overcame challenges in accessing NGS, respondents were asked about strategies used, such as applying for special requests through their hospitals or patients’ insurance, utilizing pharmaceutical industry patient access programs, or employing other methods. Clinicians were also asked to rank the importance of multi-stakeholder collaborations in improving NGS access and identify initiatives or programs that have enhanced NGS availability in Malaysia.
This study was approved by the Medical Research Ethics Committee (MREC) of Universiti Malaya Medical Centre (UMMC) (MECID No. 20201115–9217) and was conducted in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived by the Medical Research Ethics Committee of UMMC as the survey was non-interventional and collected no identifiable personal data.
All survey data were created and stored on Microsoft OneDrive with restricted access limited to the study administrator. As part of the data security and confidentiality measures, the anonymized dataset was downloaded for analysis, and all original survey responses were subsequently deleted.
Statistical Analysis
Descriptive statistical analyses were conducted using Microsoft Excel to summarize the survey responses. Results are presented as percentages and frequencies to provide an overview of clinicians’ demographics, NGS testing practices, opinions on accessibility, and strategies for overcoming challenges.
The Chi-square test function within Microsoft Excel was used to evaluate associations between the primary place of work (public vs private sectors) and the frequency of NGS testing performed in the first-line setting for NSCLC patients. Observed frequencies were tabulated into contingency tables for public (MoH and MoHE/MoD combined) and private sectors, with testing categorized as “All (100%),” “Almost always (91–99%),” “Most of the time (50–90%),” “Sometimes (10–49%),” “Rarely (<10%),” and “None.”
Expected frequencies were calculated assuming no association between workplace and testing frequency, using E = (Row total × Column total) ÷ Grand total. The Chi-square statistic for each cell was computed as χ2 = (O – E)2 ÷ E, with the total statistic obtained by summing all contributions. The P-values were calculated using Excel’s CHISQ.TEST (actual range, expected range) function. A significance level of 0.05 was applied because it is the standard threshold for determining statistical significance.
Results
Respondents’ Baseline Characteristics
Table 1 summarizes the characteristics of the survey respondents. Seventy-one clinicians participated in the survey, with the majority being clinical oncologists (67.6%). Clinical oncologists were evenly distributed between public (MoH and MoHE/MoD, 54.1%) and private practice (45.8%), whereas most respiratory physicians were based in MoH settings (60.9%).
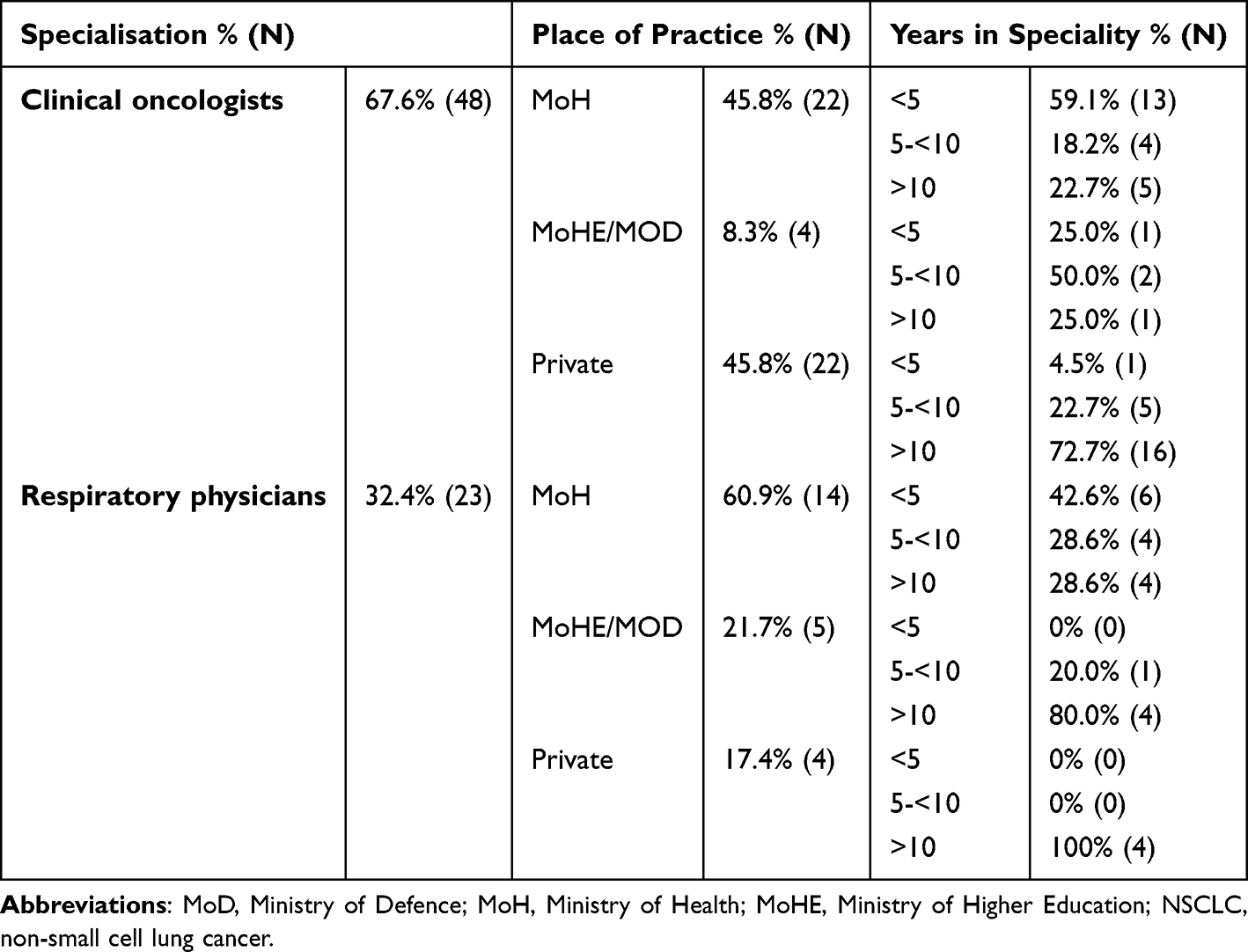 |
Table 1 Baseline Characteristics of Respondents |
All respiratory physicians (n=19) from MoHE/MoD hospitals reported treating NSCLC patients, however only 78.6% of those in MoH and only one from private hospitals treated patients with NSCLC, highlighting a distinction between diagnostic and treatment roles of respiratory physicians in public and private practice. Conversely, all the oncologist respondents in both settings were involved in the treatment of NSCLC.
NGS Testing in the First-Line Setting
The adoption of NGS testing in the first-line setting varied across healthcare sectors. Private hospitals demonstrated the highest uptake, with 80.5% of respondents reporting that >90% of NSCLC patients received NGS testing. In contrast, 22.2% of respondents from MoHE/MoD and only 8.3% from MoH institutions reported sending >90% of their NSCLC patients for NGS routinely (Figure 1). A statistically significant difference in NGS testing distribution between the public and private sectors was observed (P<0.0001).
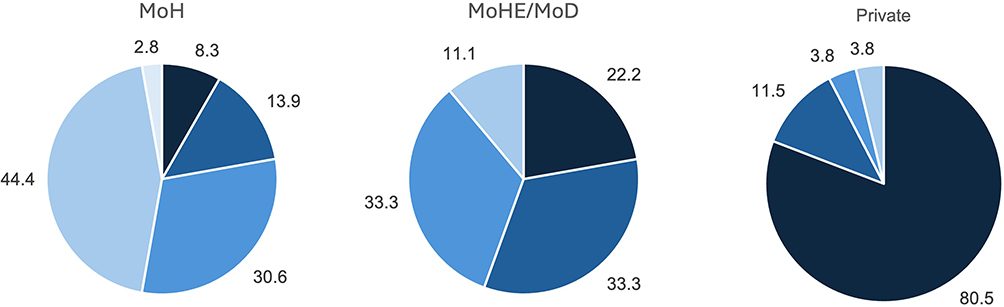





Among oncologists, 20.8% reported performing NGS testing in all NSCLC patients in the first-line setting, while 25.0% indicated testing in almost all cases. A smaller proportion (10.4%) perform NGS testing most of the time, whereas 14.6% test only sometimes. It is worth noting that almost 1/3rd (29.2%) of oncologists, all but one of whom were from MoH hospitals, rarely or never send their patients for NGS testing.
Though no respiratory physicians reported sending all (100%) their NSCLC patients for NGS testing, all of them indicated that at least a portion of their patients were tested with NGS. Among those who diagnose and treat NSCLC (n=17), 47.1% (n=8) reported sending NGS for >50% of their patients. This included two respiratory physicians from public hospitals reporting NGS use in >90% of cases. The remaining 52.9% (n=9), all from public hospitals, reported sending NGS for <50% of their NSCLC patients. Among those who only diagnose NSCLC (n=6), respiratory physicians from private hospitals (n=2) reported sending NGS in >90% of their cases whereas the remaining four physicians from public hospitals reported NGS usage in <50% of their patients.
These findings suggest higher overall adoption of NGS testing among oncologists compared to respiratory physicians, with oncologists were more likely to conduct NGS testing in a larger proportion of their patients. However, barriers to universal adoption remain, as 60.6% of the respondents across both specialties still perform testing infrequently or not at all.
Referrals with NGS Testing
The availability of NGS test results in patient referrals varied across healthcare settings, with referrals to MoH facilities least likely to include prior NGS testing. Two-thirds (66.7%) of MoH respondents reported that NGS results were rarely available, while 16.7% indicated that it was available sometimes. Only a small fraction (2.8–5.6%) received referrals with NGS results most of the time, almost always, or all the time, highlighting the limited integration of NGS in referrals to MoH hospitals.
In MoHE/MoD institutions, referrals with NGS results were slightly more common, though 55.6% of respondents still reported receiving them rarely. A third (33.3%) noted NGS was available sometimes, and 11.1% reported that referrals had NGS results most of the time.
Among private hospital respondents, 38.5% rarely received referrals with NGS results, 34.6% received them sometimes, and 15.4% received them most of the time. Although higher than in public institutions, this pattern reflects the overall low rates of NGS testing at referring centers.
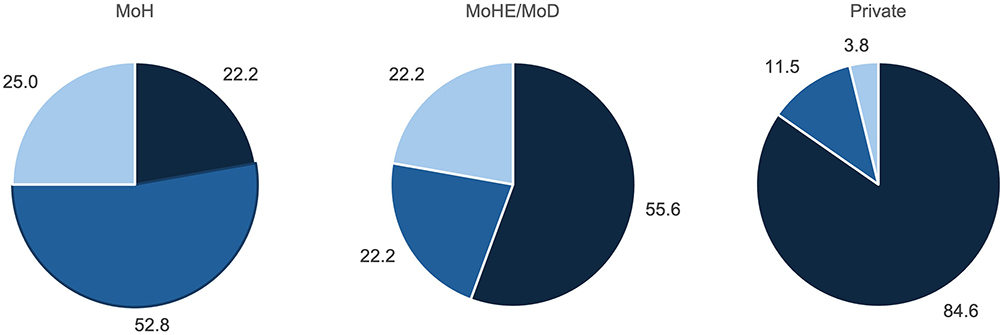
NGS Accessibility by Different Healthcare Settings
NGS accessibility varied across healthcare settings, with private hospitals reporting the highest access, followed by MoHE/MoD institutions, while MoH facilities faced the greatest challenges (Figure 2). Most respondents from private hospitals (84.6%) rated NGS accessibility as excellent. In contrast, respondents from MoHE/MoD and MoH hospitals generally indicated lower levels of accessibility. These differences underscore the disparity in NGS availability between the public and private sectors, with private hospitals demonstrating the most consistent access to testing.



Barriers to NGS Testing
Cost emerged as the most frequently reported barrier to NGS testing, with 36 respondents identifying the price of the test itself and 33 citing the expense of targeted treatments. Additionally, 10 respondents noted that NGS was unavailable at their institutions, particularly within MoH facilities, while five highlighted limited access to clinical trials offering NGS as a challenge.
Open-text responses highlighted additional challenges, including long turnaround times of NGS, limited tissue availability after prior multiple IHC stains, and a lack of clear testing guidelines.
Overcoming NGS Accessibility Challenges
Respondents reported various strategies to improve NGS access. In MoH and MoHE/MoD institutions, industry-subsidized access programs were most commonly used, often combined with hospital or insurance support. In private hospitals, access was more flexible and evenly distributed across industry-driven, insurance, and hospital-supported mechanisms.
Discussion
The Malaysian healthcare system is divided into public (MoH, MoHE and MoD hospitals) and private sectors, with public hospitals bearing a significantly higher patient load.32 For every patient admitted to a private hospital, two are admitted to public hospitals, while for every outpatient visit in the private sector, approximately 16 patients are seen in public healthcare facilities.27 The government heavily subsidizes public healthcare that typically caters for the lower socioeconomic status and rural populations,33 whereas private sector patients, who are typically from the mid-to-high socioeconomic status, rely on out-of-pocket (OOP) payments or insurance reimbursement. However, with only six MoH oncology centers and four MoHE hospitals catering to the majority of cancer patients, resource limitations in infrastructure, workforce, and funding pose significant challenges.34 These structural differences provide context for the observed differences in NGS access between public and private institutions.
Most studies on NGS adoption and its barriers have centered on Western countries or East Asian settings such as China, Japan, and South Korea.35–37 Research remains limited in Southeast Asia, including Malaysia, reflecting the region’s ongoing development in NGS implementation. While local studies have demonstrated the efficacy of NGS in identifying actionable mutations,22 this is the first to assess variations in NGS use across Malaysian healthcare settings and to identify specific barriers to its adoption. These findings are consistent with real-world Malaysian data, which show that first-line diagnostics continue to rely primarily on PCR for EGFR and FISH or IHC for ALK, rather than NGS.8,14 Both studies cited cost as the main obstacle to broader NGS adoption. MoH and MoHE hospitals currently do not offer in-house NGS testing, however, in Universiti Malaya Medical Centre, NGS is only available through off-site private laboratory services that are partially sponsored by industry.
Our study revealed clear differences in NGS adoption across healthcare settings. Private hospitals reported the highest levels of routine first-line NGS use, while MoH institutions demonstrated the lowest, with MoHE/MoD hospitals showing moderate uptake. Findings from international studies are consistent with these results. A 2017 US survey found that three-quarters of clinicians using NGS to guide treatment decisions were affiliated with academic institutions,35 which aligns with our findings that NGS use was more common in academic settings (MoHE/MoD hospitals). Although access in the private setting was generally highest, many referrals to private clinicians arrived without prior NGS results. This reflects low testing rates at referring institutions, rather than restricted availability within the private setting, highlighting broader upstream gaps in NGS use. Studies from Asia examining NGS adoption across public, private, and academic healthcare sectors are lacking. By addressing this gap, our study provides new insights into how healthcare settings influence NGS utilization, particularly highlighting higher adoption in private institutions where insurance funding is more accessible.
There is no doubt that NGS adoption is the way forward as evidence suggests comprehensive molecular profiling enables more accurate treatment decisions and improved outcomes. Studies have shown that patients receiving NGS-guided targeted therapies have significantly better outcomes, with median overall survival (OS) of 18.3 months versus 14.1 months,38 and progression-free survival (PFS) of 19.4 months compared to 6.4 months.39 However, real-world data from Malaysia underscore the difficulty in achieving comparable outcomes, with How et al (2022)14 reporting that the high cost of targeted therapies, often unaffordable for patients, has hindered wider adoption of NGS.
Moreover, the continued reliance on sequential single-gene testing in Malaysia may further delay time-to-treatment. Consistent with global findings highlighting the inefficiencies of stepwise testing,37 a Malaysian real-world study reported that delays in ALK testing due to sequential workflows led to missed treatment opportunities, reinforcing the need for multiplex approaches such as NGS.8 These delays are particularly critical in aggressive cancers like NSCLC, where timely treatment can significantly influence outcomes.
In addition to causing delays, PCR-based testing may miss actionable mutations. Studies have shown that up to 11.3% of EGFR mutations, such as exon 20 insertions, can go undetected with PCR.40 NGS not only addresses this gap but has also identified driver mutations in nearly 40% of patients initially classified as EGFR/ALK wild-type. For the reasons above, 59% of patients receive broad-panel NGS compared to 31% undergoing single-gene testing in the United States of America (USA),37 supporting the case for adopting NGS in the first-line setting. This proportion is likely much lower in Southeast Asia.
Barriers that shape NGS uptake include clinician hesitancy to test, restrictive testing guidelines, and high testing costs.41 Our findings confirmed that cost was the most common barrier, with testing and treatment expenses frequently cited. Additionally, NGS availability was limited in several institutions, particularly within MoH facilities. Testing rates are not always aligned with treatment accessibility. For example, despite South Korea reporting high EGFR testing rates approximately 25% of NSCLC patients were not prescribed tyrosine kinase inhibitors (TKIs).42 Public institutions face significant obstacles to NGS implementation, including infrastructure constraints and prolonged turnaround times, issues also raised by respondents in our study, especially those from high-volume MoH hospitals. Similar delays have been reported in other resource-limited settings.43
Insufficient tissue samples are another critical limitation, particularly in NSCLC, where low tumor cellularity and evolving biopsy techniques, such as endobronchial ultrasound, often yield inadequate specimens. Studies estimate that up to 20% of cases may not be suitable for NGS.22,44 This challenge was also reflected in our study, where concerns about tissue adequacy, sometimes caused by previous multiple IHC stains, were noted. A retrospective study done in the USA likewise identified limited tissue availability as a major barrier.37
Even when NGS is available, integrating genomic findings into clinical practice can be difficult, particularly when corresponding targeted therapies are unaffordable or unavailable.45 This issue was evident in our data, with some clinicians hesitating to order NGS due to treatment access limitations, especially in public hospitals. These observations are supported by Malaysian real-world data indicating similar clinician concerns.8
While targeted therapies remain costly, these drugs could still be innovatively delivered in resource-limited real world settings, offering a potential approach to managing costs without compromising efficacy.46,47 Additionally, similar studies are needed for other targeted therapies, such as those directed at B-Raf proto-oncogene (BRAF) and Kirsten rat sarcoma virus (KRAS) mutations, to explore cost-reduction strategies, particularly in developing countries, since the value of NGS is limited if patients cannot afford the corresponding treatments.
Improving NGS accessibility requires multifaceted efforts. Our respondents described using industry-subsidized access programs, insurance support, and hospital funding to offset costs, with private hospitals benefiting from more flexible access mechanisms. Expanding clinical trial enrolment was seen as another potential solution, though only a few respondents currently used this pathway. In the USA, 25% of oncologists referred patients to academic centers or trial networks for molecular testing.35 Limited-panel testing also provides a pragmatic alternative when broader profiling is not feasible. Increasing clinician awareness of these options is critical for optimizing molecular testing use. Public-private partnerships like the lung cancer screening collaborations involving pharmaceutical partners, Lung Cancer Network Malaysia (LCNM), and Qure.ai could serve as scalable models for future NGS expansion.48
Institutional support is equally essential, where oncologists have highlighted the importance of robust frameworks and resources for integrating genomic data into practice.37,38 National cancer genomic registries could help identify clinically significant variant patterns and improve targeted therapy use while attracting industry-sponsored trials. Including NSCLC-targeted therapies in the WHO Essential Medicines List, as has been done for some breast cancer treatments, could further improve affordability and testing uptake.42,43
The Malaysian National Strategic Plan for Cancer Control (2021–2025) aligns with many of these stakeholder-driven recommendations to advance precision oncology.34 It outlines priorities such as integrating molecular diagnostics, expanding targeted therapy access, and personalizing cancer treatment based on biomolecular profiles. Strengthening clinical trial participation and promoting research into companion diagnostic biomarkers are core to the strategic plan’s vision. These findings can help inform policy by highlighting gaps in molecular testing access, while future work incorporating patient outcomes and cost-effectiveness analyses would further support policy and resource planning.
Limitations
This study has several limitations. As recruitment was carried out mainly through professional societies and WhatsApp groups, the sample may lean towards clinicians who are more connected to academic circles or private sector networks, which could result in limited representation of practitioners working in rural or resource-constrained settings. In addition, all findings reflect clinicians’ own reports rather than institutional records, which may affect the accuracy of the reported practices. As a Malaysia-focused survey, applicability to other settings may be limited. While key barriers to NGS adoption were identified, operational and logistical challenges in public healthcare were not explored in depth, and the study did not assess the direct impact on patient outcomes. More extensive statistical analyses, such as regression modelling, were not performed because the study was not powered for this and such analyses were beyond its intended scope. Nonetheless, it offers valuable insights into the NGS landscape in Malaysia and highlights areas for improving access and adoption.
Conclusion
This study highlights significant disparities in NGS adoption for NSCLC across Malaysian healthcare settings, with public hospitals reporting limited uptake primarily due to testing costs and restricted access to targeted therapies. The continued use of single-gene testing and low rebiopsy rates further restricts the timely initiation of targeted treatments in first- or second-line settings. Overcoming these challenges will require coordinated efforts across policy, infrastructure, and research, supported by public-private partnerships between government and industry. Better NGS access may enhance identification of actionable mutations, expand clinical trial opportunities, and improve treatment outcomes. More detailed statistical modelling was not performed as the study was not powered for such analyses and they were beyond its intended scope. Further research incorporating patient outcomes or cost-effectiveness could help inform future policy decisions.
Funding
This work is supported in part by Pfizer (Malaysia) for editorial support.
Disclosure
Mau Ern Poh and Soon Hin How declare no conflicts of interest.
Muthukkumaran Thiagarajan is the President of the Malaysian Oncological Society for 2025 – 2027 term, which is an honorary post with no payment.
Lye Mun Tho declares receiving payments for lectures delivered on behalf of and participation as an expert in advisory board meetings for AstraZeneca, Janssen, Merck, Novartis, Pfizer, Amgen, Roche and MSD. He has also received support for attending meetings from AstraZeneca, Merck, Novartis, Pfizer, Amgen and Roche.
Gwo-Fuang Ho declares receiving grants paid to his affiliated institutions from EliLily, Regeneron Pharmaceuticals, Merck Sharp & Dohme, AB Science, Astellas, Tessa Therapeutics, Roche, Arcus Bioscience, AstraZeneca, Pfizer, Janssen Research & Development, Mirati Therapeutics, Novartis, Amgen, Boehringer Ingelheim, mAbxience. He has also received honoraria for presenting lectures for MSD, Novartis, F. Hoffmann-La Roche AG, AstraZeneca, Boehringer Ingelheim, Pfizer, Merck & Co., Inc, and Eisai. Honoraria for presenting lectures for Gene Solutions were paid to the affiliated institution. Dr Ho has also received support for attending meetings from IPSEN, AstraZeneca, Bristol Myers Squibb, MSD, Regeneron Pharmaceuticals, Dr Reddy’s, Roche, Servier, Zuellig Pharma, Pfizer. His affiliated institution has also received equipments, materials and other services from Pfizer, Novartis, Janssen Pharmaceuticals, Taiho, and EliLily.
Norhasanah Mohammad and Wuan Chin Tan declare that they are salaried full-time employees of Pfizer (Malaysia).
The authors report no other conflicts of interest in this work.
References
1. World Health Organization, International Agency for Research on Cancer. Global Cancer Observatory (GLOBOCAN) Malaysia. 2022. Available from: https://gco.iarc.who.int/media/globocan/factsheets/populations/458-malaysia-fact-sheet.pdf.
2. Rajadurai P, How SH, Liam CK, et al. Lung cancer in Malaysia. J Thorac Oncol. 2020;15(3):317–10. doi:10.1016/j.jtho.2019.10.021
3. Kan CS, Chan KM. A review of lung cancer research in Malaysia. Med J Malaysia. 2016;71(Suppl 1):70–78.
4. Liam CK, Pang YK, Leow CH, et al. Changes in the distribution of lung cancer cell types and patient demography in a developing multiracial Asian country: experience of a university teaching hospital. Lung Cancer. 2006;53(1):23–30. doi:10.1016/j.lungcan.2006.03.009
5. Benjamin DJ, Haslam A, Gill J, et al. Targeted therapy in lung cancer: are we closing the gap in years of life lost? Cancer Med. 2022;11(18):3417–3424. doi:10.1002/cam4.4703
6. Cainap C, Balacescu O, Cainap SS, et al. Next generation sequencing technology in lung cancer diagnosis. Biology. 2021;10(9):864. doi:10.3390/biology10090864
7. Greenhalgh J, Boland A, Bates V, et al. First-line treatment of advanced epidermal growth factor receptor (EGFR) mutation positive non-squamous non-small cell lung cancer. Cochrane Database Syst Rev. 2021;3(3):Cd010383. doi:10.1002/14651858.CD010383.pub3
8. Poh ME, How SH, Ho GF, et al. Real-world treatment and outcomes of ALK-positive metastatic non-small cell lung cancer in a Southeast Asian country. Cancer Manag Res. 2023;15:31–41. doi:10.2147/CMAR.S393729
9. Sekine I, Yamamoto N, Nishio K, et al. Emerging ethnic differences in lung cancer therapy. Br J Cancer. 2008;99(11):1757–1762. doi:10.1038/sj.bjc.6604721
10. Zhou W, Christiani DC. East meets West: ethnic differences in epidemiology and clinical behaviors of lung cancer between East Asians and Caucasians. Chin J Cancer. 2011;30(5):287–292. doi:10.5732/cjc.011.10106
11. Lee VHF, Mok TSK, Goto Y, et al. Differences between the East and the West in managing advanced-stage non-small cell lung cancer. Clin Oncol. 2020;32(1):e1–e9. doi:10.1016/j.clon.2019.07.014
12. Soda M, Choi YL, Enomoto M, et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature. 2007;448(7153):561–566. doi:10.1038/nature05945
13. Saito M, Shiraishi K, Kunitoh H, et al. Gene aberrations for precision medicine against lung adenocarcinoma. Cancer Sci. 2016;107(6):713–720. doi:10.1111/cas.12941
14. How SH, Liam CK, Zainal Abidin MA, et al. Outcomes of patients with EGFR-mutant advanced NSCLC in a developing country in Southeast Asia. Cancer Manag Res. 2022;14:1995–2005. doi:10.2147/CMAR.S364713
15. Bestvina CM, Waters D, Morrison L, et al. Cost of genetic testing, delayed care, and suboptimal treatment associated with polymerase chain reaction versus next-generation sequencing biomarker testing for genomic alterations in metastatic non-small cell lung cancer. J Med Econ. 2024;27(1):292–303. doi:10.1080/13696998.2024.2314430
16. Muzzey D, Evans EA, Lieber C. Understanding the basics of NGS: from mechanism to variant calling. Curr Genet Med Rep. 2015;3(4):158–165. doi:10.1007/s40142-015-0076-8
17. Ortendahl JD, Cuyun Carter G, Thakkar SG, et al. Value of next generation sequencing (NGS) testing in advanced cancer patients. J Med Econ. 2024;27(1):519–530. doi:10.1080/13696998.2024.2329009
18. Zheng Y, Vioix H, Liu FX, et al. Diagnostic and economic value of biomarker testing for targetable mutations in non-small-cell lung cancer: a literature review. Future Oncol. 2022;18(4):505–518. doi:10.2217/fon-2021-1040
19. Kchouk M, Gibrat J-F, Elloumi M. Generations of sequencing technologies: from first to next generation. Biol Med. 2017;9(03):1–8. doi:10.4172/0974-8369.1000395
20. Mok T, Camidge DR, Gadgeel SM, et al. Updated overall survival and final progression-free survival data for patients with treatment-naive advanced ALK-positive non-small-cell lung cancer in the ALEX study. Ann Oncol. 2020;31(8):1056–1064. doi:10.1016/j.annonc.2020.04.478
21. Aggarwal A, Sharma S, Brar Z, et al. Comprehensive molecular analysis of driver mutations in non-small cell lung carcinomas and its correlation with PD-L1 expression, an Indian perspective. Pathol Res Pract. 2024;253:155013. doi:10.1016/j.prp.2023.155013
22. Ahmad AR, Toh YL, Tan W, et al. Tissue-based next generation sequencing (NGS) testing in solid tumors: a single-center experience in Malaysia [abstract]. J Clin Oncol. 2022;40(16 Suppl):e15121. doi:10.1200/JCO.2022.40.16_suppl.e15121
23. Qin K, Hou H, Liang Y, et al. Prognostic value of TP53 concurrent mutations for EGFR- TKIs and ALK-TKIs based targeted therapy in advanced non-small cell lung cancer: a meta-analysis. BMC Cancer. 2020;20(1):328. doi:10.1186/s12885-020-06805-5
24. Takahashi K, Seto Y, Okada K, et al. Overcoming resistance by ALK compound mutation (I1171S + G1269A) after sequential treatment of multiple ALK inhibitors in non-small cell lung cancer. Thorac Cancer. 2020;11(3):581–587. doi:10.1111/1759-7714.13299
25. Byeon S, Lee B, Park WY, et al. Benefit of targeted DNA sequencing in advanced non-small-cell lung cancer patients without EGFR and ALK alterations on conventional tests. Clin Lung Cancer. 2020;21(3):e182–e190. doi:10.1016/j.cllc.2019.11.006
26. Zhang Y, Shen WX, Zhou LN, et al. The value of next-generation sequencing for treatment in non-small cell lung cancer patients: the observational, real-world evidence in China. Biomed Res Int. 2020;2020:29387167.
27. Cao L, Long L, Li M, et al. The utilization of next-generation sequencing to detect somatic mutations and predict clinical prognosis of Chinese non-small cell lung cancer patients. Onco Targets Ther. 2018;11:2637–2646. doi:10.2147/OTT.S155995
28. Lai W-A, Huang Y-S, Chang K-C, et al. Next-generation sequencing in lung cancers - a single-center experience in Taiwan. Medicina. 2024;60(2):236. doi:10.3390/medicina60020236
29. Tan AC, Lai GGY, Tan GS, et al. Utility of incorporating next-generation sequencing (NGS) in an Asian non-small cell lung cancer (NSCLC) population: incremental yield of actionable alterations and cost-effectiveness analysis. Lung Cancer. 2020;139:207–215. doi:10.1016/j.lungcan.2019.11.022
30. Rajadurai P, Cheah PL, How SH, et al. Molecular testing for advanced non-small cell lung cancer in Malaysia: consensus statement from the College of Pathologists, Academy of Medicine Malaysia, the Malaysian Thoracic Society, and the Malaysian Oncological Society. Lung Cancer. 2019;136:65–73. doi:10.1016/j.lungcan.2019.08.005
31. Loong HH, Shimizu T, Prawira A, et al. Recommendations for the use of next-generation sequencing in patients with metastatic cancer in the Asia-Pacific region: a report from the APODDC working group. ESMO Open. 2023;8(4):101586. doi:10.1016/j.esmoop.2023.101586
32. Ministry of Health Malaysia. Health facts 2024. Available from: https://www.moh.gov.my/moh/resources/Penerbitan/Penerbitan%20Utama/HEALTH%20FACTS/Health_Facts_2024_updt_23012025.pdf.
33. Samsudin MF, Lim YC, Rochmah TN, et al. Revisiting the policy implications of medical tourism in the post-COVID-19 pandemic from a Malaysian perspective: a qualitative study. Cureus. 2024;16(7):e64308. doi:10.7759/cureus.64308
34. Ministry of Health Malaysia. National strategic plan for cancer control programme 2021-2025. Available from: https://www.moh.gov.my/moh/resources/Penerbitan/Rujukan/NCD/Kanser/National_Strategic_Plan_for_Cancer_Control_Programme_2021-2025.pdf.
35. Freedman AN, Klabunde CN, Wiant K, et al. Use of next-generation sequencing tests to guide cancer treatment: results from a nationally representative survey of oncologists in the United States. JCO Precis Oncol. 2018;2(2):1–13. doi:10.1200/PO.18.00169
36. Jung HA, Lee DH, Lim SM, et al. Epidemiology and outcomes of non-small cell lung cancer in South Korea. JAMA Network Open. 2024;7(2):e2355331. doi:10.1001/jamanetworkopen.2023.55331
37. Simpson L, Mathew A, Stapp J. Study of practice patterns in NGS vs single gene testing, provider-identified barriers to biomarker testing and utilization of liquid biopsy across multiple hospital-based cancer centers [abstract]. J Clin Oncol. 2023;41(16 Suppl):e18743. doi:10.1200/JCO.2023.41.16_suppl.e18743
38. Cifuentes C, Lombana M, Vargas H, et al. Application of comprehensive genomic profiling-based next-generation sequencing assay to improve cancer care in a developing country. Cancer Control. 2023;30:1–11. doi:10.1177/10732748231175256
39. Hernandez-Martinez J-M, Guijosa A, Flores‐Estrada D, et al. Real-world survival outcomes in non–small cell lung cancer: the impact of genomic testing and targeted therapies in a Latin American middle-income country. JCO Glob Oncol. 2024;10:e2400338. doi:10.1200/GO-24-00338
40. Shen CI, Chiang CL, Shiao TH, et al. Real-world evidence of the intrinsic limitations of PCR-based EGFR mutation assay in non-small cell lung cancer. Sci Rep. 2022;12(1):13566. doi:10.1038/s41598-022-17394-7
41. Levent A, Richter PD, Bender H. Patient access to precision medicine: identifying barriers to biomarker testing in non-small cell lung cancer [poster]. J Clin Oncol. 2023;41(16_suppl):3131. doi:10.1200/JCO.2023.41.16_suppl.3131
42. Chambers P, Man KKC, Lui VWY, et al. Understanding molecular testing uptake across tumor types in eight countries: results from a multinational cross-sectional survey. JCO Oncol Pract. 2020;16(8):e770–e778. doi:10.1200/JOP.19.00507
43. Mantilla WA, Sanabria-Salas MC, Baldion AM, et al. NGS in lung, breast, and unknown primary cancer in Colombia: a multidisciplinary consensus on challenges and opportunities. JCO Glob Oncol. 2021;7(7):1012–1023. doi:10.1200/GO.21.00046
44. Hiley CT, Le Quesne J, Santis G, et al. Challenges in molecular testing in non-small-cell lung cancer patients with advanced disease. Lancet. 2016;388(10048):1002–1011. doi:10.1016/S0140-6736(16)31340-X
45. Szamreta EA, Kaminski A, Shah R, et al. Survey study of barriers to evidence-based decision-making in oncology care using next-generation sequencing. J Clin Oncol. 2021;39(15_suppl):e18757. doi:10.1200/JCO.2021.39.15_suppl.e18757
46. Poh ME, Balakrishnan S, Tan SN, et al. Real-world efficacy of low dose osimertinib as second-line treatment in patients with epidermal growth factor receptor-mutated advanced non-small cell lung cancer. Transl Lung Cancer Res. 2024;13(7):1649–1659. doi:10.21037/tlcr-24-243
47. Poh ME, Chai CS, Liam CK, et al. Does dose reduction of Afatinib affect treatment outcomes of patients with EGFR-mutant metastatic non-small cell lung cancer in real-world clinical practice? Transl Lung Cancer Res. 2024;13(2):307–320. doi:10.21037/tlcr-23-691
48. Combating lung cancer in the Asia Pacific Region. Malaysia. Available from: https://combatinglungcancerasiapacific.com/roche-fpa/malaysia-case-study/.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.