Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
Advancing Hepatocellular Carcinoma Therapy with Next-Generation Molecular and Immunotherapeutics
Authors Hassan M, Hussain I, Ahmad K, Zafar S, Khalid A, Haseeb M, Hussain N, Ghafar MA
Received 21 September 2025
Accepted for publication 16 December 2025
Published 24 December 2025 Volume 2025:12 Pages 2907—2918
DOI https://doi.org/10.2147/JHC.S569017
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Gerber
Mudassir Hassan,1 Ijaz Hussain,2 Kafeel Ahmad,3 Saima Zafar,2 Adeel Khalid,4 Muhammad Haseeb,5 Nazim Hussain,3 Muhammad Adeel Ghafar3
1Department of Zoology, Baba Guru Nanak University, Nankana Sahib, Punjab, Pakistan; 2Department of Zoology, Government College University Faisalabad, Faisalabad, Punjab, Pakistan; 3Department of Botany, Baba Guru Nanak University, Nankana Sahib, Punjab, Pakistan; 4Department of Zoology, University of Sialkot, Sialkot, Punjab, Pakistan; 5Department of Veterinary Sciences, University of Veterinary and Animal Sciences, Lahore, Punjab, Pakistan
Correspondence: Mudassir Hassan, Department of Zoology, Baba Guru Nanak University, Nankana Sahib, Punjab, Pakistan, Email [email protected]
Abstract: Hepatocellular carcinoma (HCC), the most prevalent form of primary liver cancer, remains a major global health concern due to its high incidence and mortality rates. Driven by factors such as chronic hepatitis B and C infections, alcohol-related liver disease, and metabolic-associated fatty liver disease (MAFLD), HCC is often diagnosed at advanced stages, limiting therapeutic options and prognosis. Recent advances in understanding the molecular mechanisms and tumor microenvironment of HCC, particularly disruptions in key pathways like Ras-Raf-MEK, PI3K-Akt/mTOR, and Wnt/β-catenin, have catalyzed the development of novel treatment strategies. This review synthesizes findings from over 80 recent peer-reviewed studies to explore the evolution of HCC therapy, including targeted therapies, immune checkpoint inhibitors, combination regimens, surgical techniques, and locoregional treatments. Special emphasis is placed on the role of tumor immunology, emerging biomarkers, and the impact of precision medicine in tailoring treatment strategies. These innovations collectively offer promising avenues for improving survival and quality of life in patients with HCC.
Keywords: hepatocellular carcinoma, HCC, primary liver cancer, tumor microenvironment, tumor immunology, apoptosis
Introduction
The most prevalent kind of liver cancer and the third most common cause of cancer-related deaths globally is hepatocellular carcinoma (HCC). Between 1990 and 2015, the number of liver cancer cases rose by 75%, largely due to an aging population and overall population growth. In 2015, about 854,000 new cases were reported, with approximately 810,000 deaths. By 2020, estimates indicated around 905,700 new cases and 830,200 deaths globally.1,2 In 2022, the American Cancer Society reported approximately 20 million new cancer diagnoses globally, with the disease claiming around 9.7 million lives. In 2022, approximately 866,136 new liver cancer cases were identified globally. The highest age-adjusted incidence rates per 100,000 people were observed in Mongolia (96.1), Egypt (32.0), Cambodia (25.1), Laos (24.9), and Thailand (22.7).3 Figure 1 illustrates the temporal patterns in the global liver cancer problem, depicting the increasing incidences and mortality reported between 1990 and 2022. The graph represents yearly frequency rates, while the superimposed line graph depicts corresponding mortality trends. As a whole, the data show a sustained upward trajectory in hepatocellular carcinoma (HCC) worldwide, driven largely by aging populations, persistent viral hepatitis, alcohol-related liver disease, and the rapid rise of metabolic-associated fatty liver disease (MAFLD). The figure highlights the widening gap between incidence and mortality, reflecting limited improvement in early detection and curative treatment access. Several factors contribute to the onset of HCC, such as chronic liver disease like hepatitis B and C, liver damage caused by alcohol consumption, and non-alcoholic fatty liver disease. These conditions often hinder timely diagnosis and treatment.4,5
 |
Figure 1 Trends in global liver incidence and mortality. |
The growth of HCC is strongly influenced by disruptions in key molecular systems, including the Ras-Raf-MEK, PI3K-Akt/mTOR, and Wnt-β-catenin pathways. For instance, when the Wnt/β-catenin pathway becomes overactive, it can trigger the expression of genes that drive excessive cell growth, leading to tumor development.6,7
In a similar vein, HCC is often associated with activation of the Phosphoinositide 3-Kinase-Protein Kinase B-Mammalian Target of Rapamycin pathway, which is necessary for cell life, growth, and blood vessel formation.8 Aggressive tumor behavior is linked to alterations in the Ras-Raf-MEK.
Pathway, which aids in cell proliferation and differentiation.9 In HCC, the tumor microenvironment (TME) is a complex ecosystem made up of extracellular matrix components, fibroblasts, immune cells, and tumor cells.10 The effectiveness of treatment and the development of tumors are greatly influenced by this complex interaction. Tumor-associated macrophages and regulatory T cells are two examples of immunological cells that might induce immunosuppression inside the TME, impeding the effectiveness of anti-tumor immune responses.11
Additionally, cancer-associated fibroblasts aid in extracellular matrix remodeling, which promotes angiogenesis and tumor invasion.12 Metabolically associated fatty-liver disease (MAFLD) is now recognized as a growing risk factor for HCC, largely due to changing dietary patterns and lifestyle habits worldwide.13 Genetic and epigenetic changes are key in liver cancer development, affecting how tumors grow and respond to treatment. In the past, treatment choices were limited, leading to poor survival rates. However, recent progress in understanding tumor biology, early detection and prognosis, immune responses, and molecular pathways has led to improved therapies.14 The introduction of targeted treatments, personalized approaches, and combined treatment strategies has greatly enhanced the management of hepatocellular carcinoma (HCC), offering better survival prospects.15 This review aims to elucidate these recent developments, providing a detailed analysis of current and emerging treatments for liver cancer.
The studies for this review were collected through a systematic literature search. The search was carried out from different major scientific databases, including PubMed, Scopus, Web of Science, and Google Scholar. The keywords used in the search included “Hepatocellular carcinoma,” “HCC,” “Primary liver cancer,” “Tumor microenvironment,” “Tumor immunology,” “Apoptosis,” and “advancement in liver cancer treatment.” Publications considered were up to the year 2024. Studies were selected based on predefined inclusion criteria, requiring the publications to be peer-reviewed, in English, and directly focused on hepatocellular carcinoma biology, progression, tumor microenvironment, immunology, apoptosis, or therapeutic advancements. Non-research articles, or research on areas not specifically related to either mechanisms of liver cancer or its treatments, and those lacking a specific and adequate methodological description, were to be excluded. The titles, abstracts, and full texts of all identified articles were screened for relevance and scientific quality. Other studies were identified from the reference lists of selected articles. This approach provided an assurance that the synthesis undertaken on hepatocellular carcinoma was comprehensive and reliable.
Advances in Immunotherapy
Immunotherapy has revolutionized most cancer treatments by harnessing the affected person’s immune system to recognize and smash tumor cells. In hepatocellular carcinoma (HCC), immune checkpoint inhibitors and adoptive mobile treatments boost T-cellular activation, overcoming tumor-caused immune suppression and enhancing medical consequences. This approach not simplest goals malignant cells especially however also gives durable responses and capacity synergy with conventional remedies.
Immune Checkpoint Inhibitors
Immune checkpoint blockers aid in treating hepatocellular carcinoma (HCC) by preventing signals that weaken the body’s defense system, allowing it to fight cancerous cells more effectively. In 2022, the US Food and Drug Administration (FDA) approved the use of tremelimumab, which targets CTLA-4, in combination with durvalumab, a PD-L1 inhibitor, for patients with liver cancer that cannot be surgically removed. This decision was supported by clinical trials showing that the combination led to better overall survival rates than sorafenib, the prior standard treatment.16 Blocking both CTLA-4 and PD-L1 pathways boosts T-cell activity and growth, strengthening the body’s ability to fight tumors. Another significant development is the use of atezolizumab, which targets PD-L1, along with bevacizumab, which restricts blood vessel growth. Research indicates that this combination increases survival rates and slows disease progression in patients affected with liver cancer, making it a preferred first-line treatment.17,18 Inhibiting immune checkpoints and tumor blood supply weakens the tumor’s defenses, allowing the immune system to target it more effectively. Immune checkpoint inhibitors, like anti-PD-1, PD-L1, and anti-CTLA-4 antibodies, work by blocking signals that suppress immune responses, allowing T cells to function properly. T cells become inactive when PD-1 proteins on their surface interact with PD-L1 and PD-L2 proteins found on tumor cells. This relationship is broken by anti-PD-1/PD-L1 antibodies, which boost T-cell activation against tumor cells.19 Another T-cell inhibitory receptor is CTLA-4. It prevents T-cell activation by binding with B7 ligands on antigen-presenting cells, blocking CD28 from attaching. By preventing this inhibitory contact, anti-CTLA-4 antibodies improve T-cell priming and activation.20 Figure 2 summarizes the main oncogenic signaling cascades involved in hepatocellular carcinoma (HCC) pathogenesis and highlights current therapeutic intervention points. The diagram shows aberrant activation of Wingless/Integrated-β-catenin (Wnt/β-catenin), Rat sarcoma/rapidly accelerated fibrosarcoma/mitogen-activated protein kinase kinase/extracellular signal-regulated kinase (Ras/Raf/MEK/ERK), phosphatidylinositol 3-kinase/protein kinase B/mammalian target of rapamycin (PI3K/AKT/mTOR), and growth factor receptor pathways, indicating their roles in tumorigenesis, angiogenesis, cell survival, and immune evasion. Immune checkpoint pathways, including programmed cell death protein-1/programmed cell death ligand-1 (PD-1/PD-L1) and cytotoxic T-lymphocyte-associated protein 4 (CTLA-4), as well as angiogenic circuits such as the vascular endothelial growth factor–vascular endothelial growth factor receptor (VEGF–VEGFR) axis, are shown with inhibitory “T-bars” representing approved drugs such as immune checkpoint inhibitors and antiangiogenic agents. This figure provides a mechanistic overview of how cross-talk promotes treatment resistance and how targeted therapies disrupt these signaling nodes.
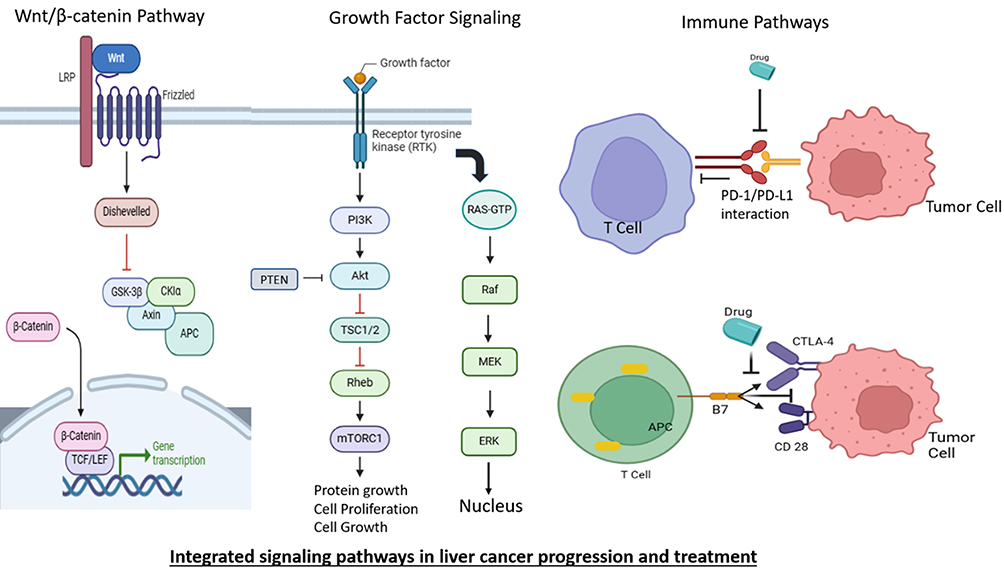 |
Figure 2 Integrated Signaling Pathways in Liver Cancer, Mechanisms and Therapeutic Targets. Abbreviations: LRP, Low-density lipoprotein receptor-related protein; Dvl, Dishevelled; GSK-3β, Glycogen synthase kinase-3 beta; CK1α, Casein kinase 1 alpha; Axin, Axis inhibition protein; APC, Antigen-presenting cell; β-Catenin, Beta-catenin; TCF/LEF, T-cell factor/Lymphoid enhancer-binding factor; RTK, Receptor tyrosine kinase; PI3K, Phosphoinositide 3-kinase; Akt, Protein kinase B; RAS-GTP, Ras bound to guanosine triphosphate; Raf, Rapidly accelerated fibrosarcoma kinase; MEK, Mitogen-activated protein kinase kinase; ERK, Extracellular signal-regulated kinase; PD-1, Programmed cell death protein 1; PD-L1, Programmed death-ligand 1; CTLA-4, Cytotoxic T-lymphocyte-associated protein 4; B7, B7 family co-stimulatory molecules. |
Combination Therapies
Using immune checkpoint inhibitors (ICIs) alongside other treatments has proven more effective in managing hepatocellular carcinoma (HCC). A key study found that patients with intermediate-stage HCC experienced better progression-free survival when treated with a combination of lenvatinib, pembrolizumab, and transarterial chemoembolization (TACE) compared to those who received TACE alone.21 The complementary biological actions of transarterial chemoembolization (TACE), lenvatinib, and pembrolizumab are used in aggregate for intermediate-stage HCC. TACE induces ischemic necrosis by obstructing arterial tumor delivery, producing antigen release and inflammatory signaling. Lenvatinib inhibits VEGFR, FGFR, and additional seasoned-angiogenic kinases, restricting neovascularization and tumor regrowth following embolization. Pembrolizumab complements cytotoxic T-cellular responses by way of blocking PD-1–mediated immune suppression. The schematic illustrates how the integrated method augments antitumor immunity, reduces vascular assist, and enhances tumor control in comparison with monotherapy in Figure 3.
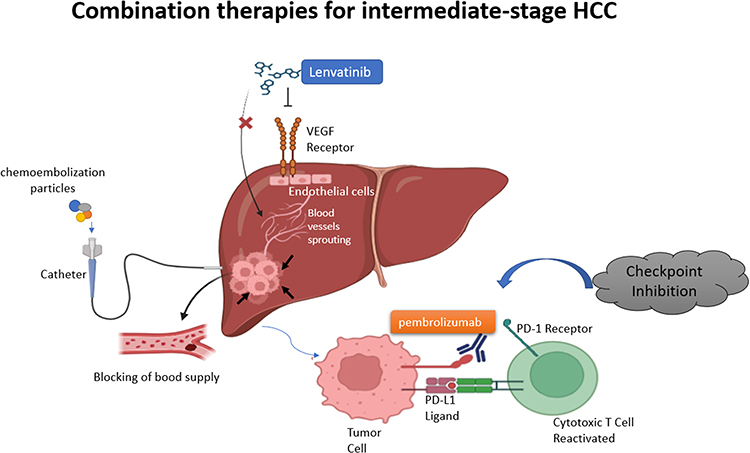 |
Figure 3 The illustration shows treatment options synergized for treating intermediate-stage HCC: TACE prevents the flow of blood to the tumor, lenvatinib blocks the building of new blood vessels, and pembrolizumab energizes Tcells by blocking checkpoint molecules. |
Surgical Interventions and Liver Transplantation
The main treatments for early-stage HCC include surgery and liver transplantation. Improvements in surgical methods and patient selection have led to better results and increased the number of eligible patients.
Liver Transplantation
Transplantation is a potential treatment for patients with early-stage HCC, particularly those with liver damage. Recent research has improved the criteria for selecting patients by considering tumor size, quantity, and alpha-fetoprotein levels to assess the likelihood of recurrence and enhance recovery outcomes.22–24 Advancements in organ harvesting and distributing them more efficiently have made more grafts available, leading to fewer deaths among patients on the waiting list.25
Minimally Invasive Surgical Techniques
Surgical techniques like robotic-assisted and laparoscopic procedures have decreased post-surgery complications and promoted fast recovery. These methods are especially advantageous for patients with cirrhosis as they reduce surgical strain and help preserve liver function.26,27 Improved imaging techniques and surgical navigation tools have made tumor removal more precise, resulting in better treatment outcomes.28
Locoregional Therapies
Therapies associated with Locoregional are crucial in hepatocellular carcinoma (HCC) management, particularly for patients who are ineligible for surgical intervention. These treatments precisely target tumor cells while preserving the integrity of surrounding healthy tissue, thereby reducing collateral damage and improving patient outcomes. Some of the therapies that are commonly practiced are given below.
Transarterial Chemoembolization (TACE)
Transarterial chemoembolization (TACE) targets tumor cells while reducing systemic toxicity by delivering chemotherapeutic drugs and embolic materials straight into the hepatic artery. Ischemia and necrosis are brought on by embolic particulates that stop blood flow to the tumor. The effectiveness of TACE is increased by drug-eluting beads, which release chemotherapeutic drugs in a regulated manner.29 Transarterial chemoembolization remains a primary treatment for intermediate-stage hepatocellular carcinoma (HCC). Recent advancements, such as drug-eluting beads, enable the controlled release of chemotherapy agents, improving their effectiveness in targeting tumor cells while minimizing systemic toxicity.30,31 Pairing transarterial chemoembolization (TACE) with whole-body treatments, such as drugs that help the immune system recognize and attack harmful cells, has shown promising improvements in survival rates. When used alongside PD-1 inhibitors, TACE may help slow tumor growth and potentially reduce disease severity in appropriately chosen patients.32,33 Ongoing research evaluates the most effective sequencing and combination of therapies to enhance treatment outcomes.
Ablative Therapies
Tumor cell death is caused by thermal injury in radiofrequency (RFA) and microwave ablation (MWA). MWA generates energy using microwave energy, whereas RFA uses radiofrequency energy. Both methods kill tumor cells by causing localized areas of coagulative necrosis.34 The RFA and MWA are widely used minimally invasive techniques for treating small tumors, including hepatocellular carcinoma (HCC). Advances in probe technology and imaging guidance have improved the accuracy and effectiveness of these treatments. Comparative studies indicate that both RFA and MWA achieve similar therapeutic outcomes and safety profiles. However, MWA has certain advantages over RFA, including shorter procedure times and a reduced number of sessions required to achieve complete tumor ablation, making it a more efficient option in clinical practice.35,36 Comparative studies on microwave ablation (MWA) and radiofrequency ablation (RFA) suggest that both techniques are equally effective and safe for tumor treatment. However, MWA appears to offer certain advantages, including reduced procedure time and fewer sessions required to achieve complete tumor ablation.35
Selective Internal Radiation Therapy (SIRT)
Selective Internal Radiation Therapy (SIRT), also known as radioembolization, is a targeted treatment that delivers radioactive microspheres directly into the liver’s blood to eliminate cancerous cells while reducing harm to healthy tissue. This approach has shown effectiveness in treating unresectable hepatocellular carcinoma and liver metastases from colorectal cancer. Recent research indicates that using SIRT along with immune checkpoint inhibitors could be beneficial, enhancing the body ability to recognize and attack tumors, potentially improving treatment outcomes. Ongoing clinical trials are investigating the most effective ways to integrate these therapies for better patient survival and disease management.37,38 By injecting radioactive microspheres straight into the hepatic artery, selective internal radiation therapy (SIRT) can provide high radiation doses to tumor cells while preserving healthy liver tissue. Beta radiation from the microspheres damages DNA and kills cells.39
Systemic Therapies
The treatment options for hepatocellular carcinoma (HCC) have expanded, introducing new medications and combined approaches that have improved patient survival rates.
Targeted Therapies
Targeted treatments interfere with specific molecular pathways that drive tumor growth and survival. Lenvatinib, a multi-kinase inhibitor, is an established first-line therapy for advanced HCC, showing survival benefits comparable to sorafenib.40 Regorafenib and cabozantinib are now approved as second-line treatments, helping patients which not respond to initial therapy live longer.41,42 Doctors are now using molecular profiling to choose targeted therapies, making treatments better suited to individual patients.6
VEGFR/VEGF Pathway Suppression
A major therapeutic approach for HCC is the suppression of the Vascular Endothelial Growth Factor Receptor (VEGFR) and Vascular Endothelial Growth Factor (VEGF) pathway, which is essential for tumor angiogenesis. By blocking VEGF-A from attaching to its receptors, the monoclonal antibody bevacizumab suppresses angiogenesis.10 Multi-kinase inhibitors like lenvatinib and sorafenib target VEGFRs as well as other kinases like FGFR and PDGFR that are implicated in tumor growth and angiogenesis.43,44
mTOR Pathway Inhibition
The mTOR (mechanistic Target of Rapamycin) pathway, which promotes cell survival and proliferation, is commonly dysregulated in HCC. Everolimus is a mTOR inhibitor that inhibits mTOR activity, which inhibits angiogenesis and cell growth.45
c-MET Pathway Inhibition
The c-MET (Mesenchymal-Epithelial Transition Factor) pathway is linked to the metastasis and progression of HCC. A multi-kinase inhibitor called cabotinib inhibits tumor development and angiogenesis by targeting c-MET and other kinases like VEGFRs and AXL.46
Mechanism of Resistance
Number of mechanisms, including pathway bypass, compensatory signaling, and the activation of alternative signaling pathways, might result in resistance to targeted therapy in HCC. For example, the PI3K-Akt and mTOR pathway becomes active, or the overexpression of alternative angiogenic factors can result in resistance to VEGFR inhibitors. Multiple pathway-targeting combination treatments can overcome resistance and enhance treatment results.47
Biomarker-Based Treatment
Molecular profiling with proteomics and genomics can find certain biomarkers that indicate how well HCC patients will respond to targeted treatments. For example, patients those are more likely to benefit from specific targeted medicines can be chosen based on the expression of particular gene signatures or protein markers. This individualized approach to cancer care can reduce toxicity and increase therapeutic efficacy.48
Immunotherapy
Immunotherapy has significantly transformed the approach to treating advanced hepatocellular carcinoma (HCC). Research indicates that using immune checkpoint inhibitors like tremelimumab (which targets CTLA-4) and durvalumab (which blocks PD-L1) has led to better patient survival rates compared to conventional treatments.17 This combined immunotherapy method boosts T-cell activity and growth, strengthening the body’s ability to fight tumors. Researchers are currently investigating how immunotherapy can be used alongside localized treatments and targeted drugs to improve patient outcomes.17,49,50
Natural killer (NK) and other immune cells play a vital role in detecting and responding to tumors. NK cells use a variety of methods, such as the release of cytotoxic-granules and the activation of death receptors, to identify and destroy tumor cells. NK cell failure is commonly seen in HCC, which aids in the growth of the tumor. To improve the results of HCC treatment, therapeutic approaches that target NK cell function, like cytokine therapy and NK cell-based immunotherapy, are being investigated.51
Emerging Therapies and Future Directions
The progression of hepatocellular carcinoma (HCC) treatment involves emerging therapies that are undergoing evaluation in both preclinical research and clinical trials, offering potential improvements in patient care.
Personalized Cancer Vaccines
Personalized cancer vaccines help the immune system detect and attack proteins that are specific to tumor cells. Recent clinical research indicates that integrating a customized anti-tumor vaccine with standard immunotherapy is safe and can nearly double the treatment response rate in patients with HCC compared to immunotherapy alone.52–54 This approach has the potential to enhance the effectiveness of existing treatments and promote more sustained therapeutic responses. Personalized cancer vaccines target neoantigens, which are distinct mutations expressed on tumor cells, to trigger an immune response specific to a given tumor. These neoantigens are found using next-generation sequencing technologies, and customized vaccinations are made to encourage T cells to identify and target tumor cells that express these neoantigens. Neoantigen-based vaccinations have shown promise in boosting anti-tumor immunity in clinical studies, proving their viability and potential effectiveness in HCC.55
An integrated conceptual model of the tumor microenvironment (TME) and key molecular pathways riding HCC progression and therapeutic resistance. The diagram indicates interactions among angiogenic elements (VEGF), immunosuppressive mediators (TGF-β, regulatory T cells, tumor-related macrophages), and oncogenic signaling pathways (PI3K/AKT/mTOR, Ras/Raf/MEK/ERK, Wnt/β-catenin). These networks together promote immune evasion, out of control proliferation, and resistance to focused agents and immune checkpoint inhibitors. Therapeutic classes—which include anti-VEGF marketers, ICIs, and multi-kinase inhibitors—are positioned along their respective objectives, illustrating rational combinations designed to triumph over resistance and enhance remedy results (Figure 4). The TME supports tumor development by promoting blood vessel formation (angiogenesis), suppressing immune responses, and interacting with surrounding stromal cells, making it a critical target for therapy.10,56 Vascular endothelial growth factor helps maintain the tumor’s bloodsupply while transforming growth factor-β (TGF-β), which weakens the immune system, reduces the effectiveness of immune checkpoint inhibitors (ICIs) such as PD-1/PD-L1 and CTLA-4 inhibitors.57 The Wnt/β-catenin pathway further increases immune resistance and tumor survival, complicating immunotherapy.58,59 Additionally, disruptions in the PI3K-Akt/mTOR and Ras/Raf/MEK/ERK pathways accelerate uncontrolled cell growth, reducing the success of targeted treatments.60 Combining ICIs with VEGF inhibitors and drugs that block these pathways may help overcome resistance, improving treatment outcomes for HCC.
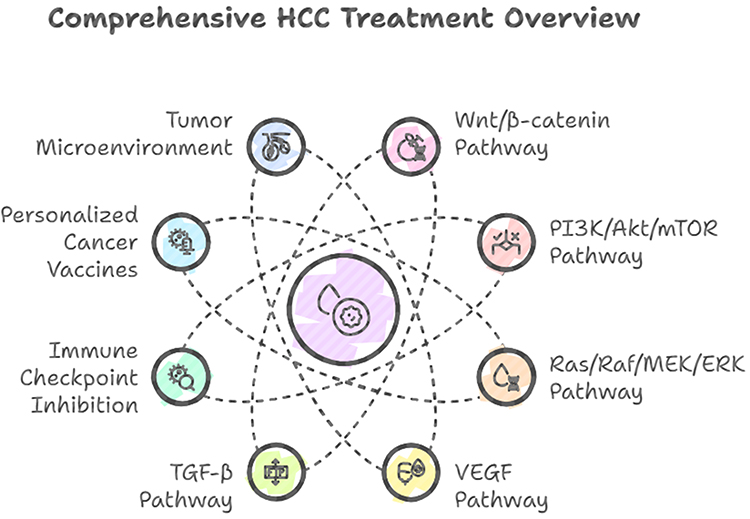 |
Figure 4 Interconnected Pathways in HCC: A Comprehensive Treatment Landscape (Header removed and quality improved). |
Artificial Intelligence in Radiation Therapy
The artificial intelligence (AI) in radiation therapy aims to improve accuracy and minimize harmful effects. By processing real-time imaging data, AI can modify radiation delivery in response to tumor shifts and anatomical changes. AI algorithms are being explored for monitoring tumor movement in the chest, abdomen, and pelvis during radiation therapy. Research highlights their role in improving dose accuracy and tracking tumors in real time. By reducing radiation exposure to healthy tissues, this approach aims to enhance treatment safety and effectiveness. Though still under investigation, AI-assisted radiation therapy shows promise in refining cancer treatment strategies.61,62
Histotripsy
Histotripsy is a medical procedure that uses sound waves to break apart tumor tissue without surgery. Research indicates that this method can effectively target liver tumors while minimizing damage to nearby healthy cells.63 This approach provides a potential option for patients who cannot undergo conventional surgery. Clinical trials are assessing how safe and effective histotripsy is in treating more patients.64
Gene Therapy
Gene therapy has emerged as a compelling therapeutic approach for hepatocellular carcinoma (HCC), leveraging viral vectors to supply functional genetic cloth at once into tumor cells.19 This approach permits specific modulation of oncogenic signaling via introducing cytotoxic genes, seasoned-apoptotic molecules, or tumor-suppressor genes, thereby inducing centered tumor cellular loss of life or restoring misplaced regulatory mechanisms. Viral vectors—most typically adenoviral, adeno-associated, or lentiviral structures—provide high transduction efficiency and the capability to acquire selective gene expression inside malignant tissue, minimizing off-goal consequences.19
A specifically promising course is the development of engineered oncolytic adenoviruses capable of both replicating selectively within tumor cells and delivering therapeutic transgenes. One such method includes arming adenoviruses with genes encoding tumor necrosis component–associated apoptosis-inducing ligand (TRAIL) and interleukin-12 (IL-12). Preclinical investigations confirmed that these twin-function constructs exerted robust anti-tumor hobby in human HCC fashions both in vitro and in murine systems.57 Delivery of TRAIL more suitable apoptosis by activating extrinsic death receptor pathways, while IL-12 promoted sturdy anti-tumor immunity thru stimulation of cytotoxic T cells and herbal killer cell responses. Additionally, IL-12–mediated immune activation suppressed tumor-associated angiogenesis, further impairing tumor progression.
Collectively, these findings underscore the multiple therapeutic capability of gene-armed oncolytic adenoviruses—concurrently inducing direct tumor mobile lysis, amplifying immunomodulation, and disrupting vascular aid systems.57
Viruses That Cause Cancer
Oncolytic viruses are a category of healing marketers engineered or certainly decided on to preferentially infect, replicate within, and lyse tumor cells at the same time as sparing normal tissues.20 Their tumor selectivity arises from the compromised antiviral defenses characteristic of cancer cells, consisting of impaired interferon signaling, altered apoptotic pathways, and dysregulated mobile metabolism, which together render malignant cells rather permissive to viral replication. Beyond direct oncolysis, those viruses act as powerful in situ vaccines by using eliciting strong anti-tumor immune responses.20
Cancer cells show off weakened innate immune surveillance and faulty viral recognition mechanisms, making them significantly extra vulnerable to viral access and replication. Oncolytic viruses take advantage of this vulnerability with the aid of the usage of distinct routes of mobile entry: adenoviruses, measles virus, and herpes simplex virus make use of overexpressed or tumor-related floor receptors, while vaccinia virus and Newcastle ailment virus typically input via endocytic pathways.58 Once within the tumor cell, the virus undergoes replication till cellular integrity is misplaced, leading to lytic destruction.
The resulting oncolysis releases a diverse array of tumor-associated antigens, neoantigens, and risk-related molecular patterns into the tumor microenvironment. These immunogenic indicators recruit and prompt antigen-presenting cells such as dendritic cells and macrophages, which system and gift tumor-derived peptides to T lymphocytes.59 This cascade ultimately initiates a systemic, tumor-specific immune reaction capable of spotting and putting off malignant cells, thereby amplifying the therapeutic efficacy of oncolytic virotherapy and improving its compatibility with immunotherapies.
Nanotechnology
The specificity and effectiveness of cancer treatments can be increased by using nanoparticles to deliver medications and imaging agents to HCC tumors. Nanoparticles can be designed to distribute medications in a regulated way or to target certain tumor cells.24 Tiny carriers like liposomes, micelles, and polymer-based particles are used to deliver chemotherapy drugs directly to liver cancerous cells. Studies show that nanoparticles carrying drugs such as doxorubicin and sorafenib can slow liver cancer cell growth while reducing harm to healthy tissues.65 Besides treatment, nanoparticles help enhance the imaging of HCC tumors. Iron oxide nanoparticles with magnetic properties help improve MRI scans, making detecting tumors easier. This multiple role supports mutually the diagnosis and management of liver cancer.66
Biopsies in Liquid
A non-invasive method of tracking therapy response and identifying recurrence in HCC is provided by liquid biopsies, such as circulating tumor DNA (ctDNA) analysis. Personalized cancer treatment is made possible by the useful information that ctDNA can offer regarding the genetics and dynamics of tumors.25 Circulating tumor DNA is at a higher level in individuals with hepatocellular carcinoma (HCC) than in those with chronic liver conditions, aiding early detection and monitoring. Chung et al observed the genome-wide genetic alterations in cell-free DNA were linked to patient outcomes. A greater number of these changes increased the risk of disease progression and mortality, especially with sorafenib treatment.67
Conclusion
The treatment of hepatocellular carcinoma (HCC) has improved drastically, main to stepped forward affected person outcomes. Developments in systemic healing procedures, locoregional interventions, and novel medical technology have expanded remedy alternatives, permitting extra specific and powerful care. Continuous studies and scientific trials are refining those strategies, with emerging procedures including personalized vaccines and AI-assisted treatment options showing promise. Looking ahead, future studies have to focus on overcoming key challenges, along with remedy resistance, intratumoral heterogeneity, and the shortage of reliable predictive biomarkers. Integrating multi-omics profiling, liquid biopsy–primarily based monitoring, and superior computational evaluation may further enhance early detection and individualized treatment choice. Strengthening translational pathways—from preclinical modeling to medical implementation—will be vital for developing long-lasting, mechanism-based, totally healing procedures. As understanding of HCC biology advances, persevering innovation will be crucial to extending survival and enhancing the overall best of life for sufferers.
Abbreviations
HCC, Hepatocellular Carcinoma; MAFLD, Metabolically Associated Fatty Liver Disease; RFA, Radiofrequency Ablation; MWA, Microwave Ablation; TACE, Transarterial Chemoembolization; SIRT, Selective Internal Radiation Therapy; SBRT, Stereotactic Body Radiotherapy; FDA, Food and Drug Administration; CTLA-4, Cytotoxic T-Lymphocyte-Associated Protein 4; PD-1, Programmed Cell Death Protein-1; PD-L1, Programmed Cell Death Ligand-1; VEGF, Vascular Endothelial Growth Factor; VEGFR, Vascular Endothelial Growth Factor Receptor; FGFR, Fibroblast Growth Factor Receptor; mTOR, Mechanistic Target of Rapamycin; c-MET, Mesenchymal-Epithelial Transition Factor; ICIs, Immune Checkpoint Inhibitors; NK, Natural Killer (cells); TRAIL, Tumor Necrosis Factor–Related Apoptosis-Inducing Ligand; IL-12, Interleukin-12; TME, Tumor Microenvironment; TGF-β, Transforming Growth Factor-Beta; PI3K, Phosphoinositide 3-Kinase; AKT, Protein Kinase B; ERK, Extracellular Signal-Regulated Kinase; MEK, Mitogen-Activated Protein Kinase Kinase; Ras, Rat Sarcoma (protein); Raf, Rapidly Accelerated Fibrosarcoma (protein); Wnt, Wingless/Integrated; AI, Artificial Intelligence; ctDNA, Circulating Tumor DNA.
Acknowledgment
The authors gratefully acknowledge colleagues and researchers whose work contributed to the insights discussed in this review.
Disclosure
The authors declare that there are no conflicts of interest related to this work. All research was conducted independently, and the findings reported here have not been influenced by any financial, personal, or professional relationships.
References
1. Oh JH, Jun DW. The latest global burden of liver cancer: a past and present threat. Clin Mol Hepatol. 2023;29(2):355. doi:10.3350/cmh.2023.0070
2. Rumgay H, Arnold M, Ferlay J, et al. Global burden of primary liver cancer in 2020 and predictions to 2040. J Hepatol. 2022;77(6):1598–1606. doi:10.1016/j.jhep.2022.08.021
3. Valery PC, Laversanne M, Clark PJ, et al. Projections of primary liver cancer to 2030 in 30 countries worldwide. Hepatology. 2018;67(2):600–611. doi:10.1002/hep.29498
4. Behrouzifar S. Identifying downregulated hub genes and key pathways in HBV-related hepatocellular carcinoma using systems biology approach. 2023.
5. Guo W-P, Zhang H-Y, Liu L-X. Risk factors of hepatocellular carcinoma in non-alcoholic fatty liver disease: a systematic review and meta-analysis. Eur Rev Med Pharmacol Sci. 2023;27(24).
6. Llovet JM, Montal R, Sia D, et al. Molecular therapies and precision medicine for hepatocellular carcinoma. Nat Rev Clin Oncol. 2018;15(10):599–616. doi:10.1038/s41571-018-0073-4
7. Shi Y, Wang Y, Niu K, et al. How CLSPN could demystify its prognostic value and potential molecular mechanism for hepatocellular carcinoma: a crosstalk study. Computer Biol Med. 2024;172:108260. doi:10.1016/j.compbiomed.2024.108260
8. Cervello M, McCubrey JA, Cusimano A, et al. Targeted therapy for hepatocellular carcinoma: novel agents on the horizon. Oncotarget. 2012;3(3):236.
9. Dimri M, Satyanarayana A. Molecular signaling pathways and therapeutic targets in hepatocellular carcinoma. Cancers. 2020;12(2):491. doi:10.3390/cancers12020491
10. Hassan M, Tutar L, Sari-Ak D, et al. Non-genetic heterogeneity and immune subtyping in breast cancer: implications for immunotherapy and targeted therapeutics. Translational Oncol. 2024;47:102055. doi:10.1016/j.tranon.2024.102055
11. Feng H, Zhuo Y, Zhang X, et al. Tumor microenvironment in hepatocellular carcinoma: key players for immunotherapy. J Hepatocell Carcinoma. 2022;9:1109–1125. doi:10.2147/JHC.S381764
12. Roy AM, Iyer R, Chakraborty S. The extracellular matrix in hepatocellular carcinoma: mechanisms and therapeutic vulnerability. Cell Rep Med. 2023;4(9):101170. doi:10.1016/j.xcrm.2023.101170
13. Younossi ZM, Golabi P, de Avila L, et al. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: a systematic review and meta-analysis. J Hepatol. 2019;71(4):793–801. doi:10.1016/j.jhep.2019.06.021
14. Shi Y, Wang J, Huang G, et al. A novel epithelial–mesenchymal transition gene signature for the immune status and prognosis of hepatocellular carcinoma. Hepatology International. 2022;16(4):906–917. doi:10.1007/s12072-022-10354-3
15. Sangro B, Sarobe P, Hervás-Stubbs S, et al. Advances in immunotherapy for hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol. 2021;18(8):525–543. doi:10.1038/s41575-021-00438-0
16. Patel TH, Brewer JR, Fan J, et al. FDA approval summary: tremelimumab in combination with durvalumab for the treatment of patients with unresectable hepatocellular carcinoma. Clin Cancer Res. 2024;30(2):269–273. doi:10.1158/1078-0432.CCR-23-2124
17. Abou-Alfa GK, Lau G, Kudo M, et al. Tremelimumab plus durvalumab in unresectable hepatocellular carcinoma. NEJM Evidence. 2022;1(8):2100070. doi:10.1056/EVIDoa2100070
18. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
19. Zheng J, Wang S, Xia L, et al. Hepatocellular carcinoma: signaling pathways and therapeutic advances. Signal Transduct Target Therap. 2025;10(1):35. doi:10.1038/s41392-024-02075-w
20. Wang Z, Wang Y, Gao P, et al. Immune checkpoint inhibitor resistance in hepatocellular carcinoma. Cancer Lett. 2023;555:216038. doi:10.1016/j.canlet.2022.216038
21. Llovet J, Finn RS, Ren Z, et al. LBA3 Transarterial chemoembolization (TACE) with or without lenvatinib (len)+ pembrolizumab (pembro) for intermediate-stage hepatocellular carcinoma (HCC): phase III LEAP-012 study. Ann Oncol. 2024;35:S1229. doi:10.1016/j.annonc.2024.08.2277
22. Sha M, Wang J, Cao J, et al. Criteria and prognostic models for patients with hepatocellular carcinoma undergoing liver transplantation. Clin Mol Hepatol. 2024;31(1):S285.
23. Li PJ, Shah S, Mehta N. Recent advances in liver transplantation for hepatocellular carcinoma. Curr Treatment Options Oncol. 2024;25(9):1153–1162. doi:10.1007/s11864-024-01247-8
24. Mazzaferro V, Regalia E, Doci R, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996;334(11):693–700. doi:10.1056/NEJM199603143341104
25. Kwong AJ, Mannalithara A, Heimbach J, et al. Migration of patients for liver transplantation and waitlist outcomes. Clin Gastroenterol Hepatol. 2019;17(11):2347–2355.e5. doi:10.1016/j.cgh.2019.04.060
26. Vitale A, Angelico R, Sensi B, et al. What is the role of minimally invasive liver surgery in treating patients with hepatocellular carcinoma on cirrhosis? Cancers. 2024;16(5):966. doi:10.3390/cancers16050966
27. Coelho FF, Herman P, Kruger JAP, et al. Impact of liver cirrhosis, the severity of cirrhosis, and portal hypertension on the outcomes of minimally invasive left lateral sectionectomies for primary liver malignancies. Surgery. 2023;174(3):581–592. doi:10.1016/j.surg.2023.04.057
28. Haddad AF, Aghi MK, Butowski N. Novel intraoperative strategies for enhancing tumor control: future directions. Neuro-Oncology. 2022;24(Supplement_6):S25–S32. doi:10.1093/neuonc/noac090
29. Wu M, Luo Z, Cai Z, et al. Spleen‐targeted neoantigen DNA vaccine for personalized immunotherapy of hepatocellular carcinoma. EMBO Mol Med. 2023;15(10):e16836. doi:10.15252/emmm.202216836
30. Golfieri R, Giampalma E, Renzulli M, et al. Randomised controlled trial of doxorubicin-eluting beads vs conventional chemoembolisation for hepatocellular carcinoma. Br J Cancer. 2014;111(2):255–264. doi:10.1038/bjc.2014.199
31. Oh JS, Chun HJ. The update on transcatheter arterial chemoembolization using drug-eluting beads: optimization for best response. Intl J Gastrointestinal Intervention. 2021;10(4):161–164. doi:10.18528/ijgii210045
32. Marinelli B, Kim E, D’Alessio A, et al. Integrated use of PD-1 inhibition and transarterial chemoembolization for hepatocellular carcinoma: evaluation of safety and efficacy in a retrospective, propensity score-matched study. Journal for Immunotherapy of Cancer. 2022;10(6):e004205. doi:10.1136/jitc-2021-004205
33. Hu Y, Pan T, Cai X, et al. Addition of transarterial chemoembolization improves outcome of tyrosine kinase and immune checkpoint inhibitors regime in patients with unresectable hepatocellular carcinoma. J Gastrointestinal Oncol. 2023;14(4):1837. doi:10.21037/jgo-23-486
34. Aravalli RN. Role of innate immunity in the development of hepatocellular carcinoma. World J Gastroenterol. 2013;19(43):7500. doi:10.3748/wjg.v19.i43.7500
35. Suwa K, Seki T, Aoi K, et al. Efficacy of microwave ablation versus radiofrequency ablation for hepatocellular carcinoma: a propensity score analysis. Abdom Radiol. 2021;46(8):3790–3797. doi:10.1007/s00261-021-03008-9
36. Campbell WA, Makary MS. Advances in image-guided ablation therapies for solid tumors. Cancers. 2024;16(14):2560. doi:10.3390/cancers16142560
37. Garcia-Reyes K, Gottlieb RA, Menon KM, et al. Radioembolization plus immune checkpoint inhibitor therapy compared with radioembolization plus tyrosine kinase inhibitor therapy for the treatment of hepatocellular carcinoma. J Vasc Interv Radiol. 2024;35(5):722–730.e1. doi:10.1016/j.jvir.2024.02.004
38. Food U, Administration D. FDA approves tremelimumab in combination with durvalumab for unresectable hepatocellular carcinoma. 2022.
39. Okikawa S, Morine Y, Saito Y, et al. Inhibition of the VEGF signaling pathway attenuates tumor‑associated macrophage activity in liver cancer. Oncol Rep. 2022;47(4):1–11. doi:10.3892/or.2022.8282
40. Kudo M, Finn RS, Qin S, et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: a randomised Phase 3 non-inferiority trial. Lancet. 2018;391(10126):1163–1173. doi:10.1016/S0140-6736(18)30207-1
41. Bruix J, Qin S, Merle P, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;389(10064):56–66. doi:10.1016/S0140-6736(16)32453-9
42. Abou-Alfa GK, Meyer T, Cheng A-L, et al. Cabozantinib in patients with advanced and progressing hepatocellular carcinoma. N Engl J Med. 2018;379(1):54–63. doi:10.1056/NEJMoa1717002
43. Li X, Li Y, Wang Y, et al. Sinensetin suppresses angiogenesis in liver cancer by targeting the VEGF/VEGFR2/AKT signaling pathway. Exp Ther Med. 2022;23(5):360. doi:10.3892/etm.2022.11287
44. Xue Y, Ruan Y, Wang Y, et al. Signaling pathways in liver cancer: pathogenesis and targeted therapy. Mol Biomed. 2024;5(1):20. doi:10.1186/s43556-024-00184-0
45. Sun EJ, Wankell M, Palamuthusingam P, et al. Targeting the PI3K/Akt/mTOR pathway in hepatocellular carcinoma. Biomedicines. 2021;9(11):1639. doi:10.3390/biomedicines9111639
46. Goyal L, Muzumdar MD, Zhu AX. Targeting the HGF/c-MET pathway in hepatocellular carcinoma. Clin Cancer Res. 2013;19(9):2310–2318. doi:10.1158/1078-0432.CCR-12-2791
47. Zhu Y-J, Zheng B, Wang H-Y, et al. New knowledge of the mechanisms of sorafenib resistance in liver cancer. Acta Pharmacol Sin. 2017;38(5):614–622. doi:10.1038/aps.2017.5
48. Harris WP, Wong KM, Saha S, et al. Biomarker-driven and molecular targeted therapies for hepatobiliary cancers. In: Seminars in Oncology. Elsevier; 2018. 116–123.
49. Rimassa L, Finn RS, Sangro B. Combination immunotherapy for hepatocellular carcinoma. J Hepatol. 2023;79(2):506–515. doi:10.1016/j.jhep.2023.03.003
50. Zhang X-C, Zhou Y-W, Wei G-X, et al. Locoregional therapies combined with immune checkpoint inhibitors for liver metastases. Can Cell Inter. 2024;24(1):302. doi:10.1186/s12935-024-03484-1
51. Wu S-Y, Li C, Zhang L, et al. Natural killer cells in cancer biology and therapy. Mol Cancer. 2020;19:1–26. doi:10.1186/s12943-019-1085-0
52. Castro-Alejos C, Sarobe P. Personalized neoantigen vaccines for patients with advanced hepatocellular carcinoma. AME Clin Trials Rev. 2024;2:49. doi:10.21037/actr-24-76
53. Yang H, Liu Y, Zhang N, et al. Therapeutic advances in hepatocellular carcinoma: an update from the 2024 ASCO annual meeting. Front Oncol. 2024;14:1453412. doi:10.3389/fonc.2024.1453412
54. Yarchoan M, Gane EJ, Marron TU, et al. Personalized neoantigen vaccine and pembrolizumab in advanced hepatocellular carcinoma: a Phase 1/2 trial. Nature Med. 2024;30(4):1044–1053. doi:10.1038/s41591-024-02894-y
55. Reynolds CR, Tran S, Jain M, et al. Neoantigen cancer vaccines: generation, optimization, and therapeutic targeting strategies. Vaccines. 2022;10(2):196. doi:10.3390/vaccines10020196
56. Hanahan D, Coussens LMJCC. Accessories to the crime: functions of cells recruited to the tumor microenvironment. Cancer Cell. 2012;21(3):309–322. doi:10.1016/j.ccr.2012.02.022
57. Batlle E, Massagué JJI. Transforming growth factor-β signaling in immunity and cancer. Immunity. 2019;50(4):924–940. doi:10.1016/j.immuni.2019.03.024
58. Li X, Rasul A, Sharif F, et al. PIAS family in cancer: from basic mechanisms to clinical applications. Front Oncol. 2024;14:1376633. doi:10.3389/fonc.2024.1376633
59. Stortelers C, Pinto-Espinoza C, Van Hoorick D, et al. Modulating ion channel function with antibodies and nanobodies. Curr Opinion Immunol. 2018;52:18–26. doi:10.1016/j.coi.2018.02.003
60. Fruman DA, Chiu H, Hopkins BD, et al. The PI3K pathway in human disease. Cell. 2017;170(4):605–635. doi:10.1016/j.cell.2017.07.029
61. Zhao W, Shen L, Islam MT, et al. Artificial intelligence in image-guided radiotherapy: a review of treatment target localization. Quantitative Imaging Med Surg. 2021;11(12):4881. doi:10.21037/qims-21-199
62. Sava J. Evolution of personalized cancer care with molecular profiling. 2025.
63. Vlaisavljevich E, Greve J, Cheng X, et al. Non-invasive ultrasound liver ablation using histotripsy: chronic study in an in vivo rodent model. Ultrasound Med Biol. 2016;42(8):1890–1902. doi:10.1016/j.ultrasmedbio.2016.03.018
64. Worlikar T, Zhang M, Ganguly A, et al. Impact of histotripsy on development of intrahepatic metastases in a rodent liver tumor model. Cancers. 2022;14(7):1612. doi:10.3390/cancers14071612
65. Xu M, Yang L, Lin Y, et al. Emerging nanobiotechnology for precise theranostics of hepatocellular carcinoma. J Nanobiotechnol. 2022;20(1):427. doi:10.1186/s12951-022-01615-2
66. Ruman U, Fakurazi S, Masarudin MJ, et al. Nanocarrier-based therapeutics and theranostics drug delivery systems for next generation of liver cancer nanodrug modalities. Int J Nanomed. 2020;15:1437–1456. doi:10.2147/IJN.S236927
67. Ding J, Zhao W. The application of liquid biopsy techniques in high-risk population for hepatocellular carcinoma. Cancer Manage Res. 2022;Volume 14:2735–2748. doi:10.2147/CMAR.S373165
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Design and Mechanism Study of 6c, a Novel Artesunate Derivatives, for Anti-Hepatocellular Carcinoma

Xiong SS
Journal of Hepatocellular Carcinoma 2025, 12:149-167
Published Date: 25 January 2025