Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
Advances in the Application of Brain–Computer Interface-Based Neurofeedback Training in the Rehabilitation of Patients with Major Depressive Disorder
Authors Liu J ![]() , Liu L, Chen H, Xuan S, Leng X
, Liu L, Chen H, Xuan S, Leng X
Received 17 March 2026
Accepted for publication 11 June 2026
Published 25 June 2026 Volume 2026:22 609788
DOI https://doi.org/10.2147/NDT.S609788
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Junting Liu,1 Lingyu Liu,2 Han Chen,1 Shu Xuan,1 Xinke Leng1
1School of Physical Education, Hunan University, Changsha, Hunan, People’s Republic of China; 2School of Acupuncture, Rehabilitation and Clinical Medicine, Guangzhou University of Chinese Medicine, Guangzhou, Guangdong, People’s Republic of China
Correspondence: Xinke Leng, School of Physical Education, Hunan University, Changsha, Hunan, People’s Republic of China, Email [email protected]
Abstract: Major depressive disorder is a highly prevalent affective disorder worldwide, and existing pharmacological and psychological treatments continue to demonstrate notable limitations in terms of therapeutic stability, adverse effects, and relapse prevention. Brain–computer interface-based neurofeedback training (BCI‑NFT) guides patients to actively regulate abnormal neural functional states through real‑time feedback of brain activity signals, thereby providing a precise interventional pathway that acts directly at the level of neural function. This narrative review examines the theoretical foundations, neural mechanisms, and clinical application modalities of BCI‑NFT in depression rehabilitation, encompassing advances in both non‑invasive and invasive neurofeedback technologies, diverse combined intervention paradigms, and the application prospects of a concurrent intervention approach integrating wearable BCI technology with aerobic exercise at the interdisciplinary intersection of sports neuroscience and psychiatric rehabilitation medicine. Preliminary evidence suggests that BCI‑NFT may facilitate neural functional recovery in patients with major depressive disorder through three primary mechanisms: remodeling of emotion‑regulation‑related brain regions, correction of aberrant EEG activity patterns, and improvement of large‑scale brain network connectivity; however, given the sample sizes and methodological heterogeneity of existing studies, these conclusions still require further validation through large-scale randomized controlled trials. Nevertheless, the widespread clinical implementation of BCI‑NFT remains constrained by a lack of standardized training protocols, insufficient clarity regarding suitable patient populations, and a paucity of large‑sample clinical data. Future research should, within a precision psychiatry framework and through the integration of multimodal neuroimaging and large‑scale randomized controlled trials, further advance the standardized clinical translation of BCI‑NFT.
Keywords: brain–computer interface, neurofeedback training, major depressive disorder, sports neuroscience, neuromodulation, neuroplasticity, psychiatric rehabilitation
Introduction
In recent years, mental health and psychological well-being have received increasing priority in global and Chinese public health agendas. According to data published by the World Health Organization, major depressive disorder (MDD) has become the second most prevalent disease worldwide, surpassed only by cardiovascular disease, and is characterized by a prominent and persistent depressed mood.1 Epidemiological surveys indicate that approximately 350 million individuals are affected globally,2 while the lifetime prevalence of depressive disorders among Chinese adults is estimated at 6.8%.3 Moreover, among middle-aged and elderly populations in China, the prevalence of depressive disorders is even more pronounced and its underlying mechanisms more complex. A nationally representative study by Zhang et al (2025) systematically characterized the epidemiological features and multidimensional determinants of depression among middle-aged and older Chinese adults, further underscoring the pressing real-world importance of precision interventions tailored to such special populations in the context of population aging.4 Internationally, MDD constitutes a major contributor to disability and productivity loss.5 Furthermore, the disorder not only severely impairs patients’ social functioning but also significantly elevates suicide risk and increases the likelihood of comorbid physical conditions such as cardiovascular and cerebrovascular disease, thereby imposing a substantial burden on public healthcare systems.6
Conventional therapeutic approaches for MDD primarily encompass pharmacotherapy, psychotherapy, and physical treatment modalities; however, each of these standard interventions demonstrates notable limitations in clinical practice.7 Conventional antidepressants, for instance, may induce significant adverse effects—including weight gain and cardiotoxicity—as well as withdrawal reactions upon discontinuation.8 Psychotherapy, while facilitating emotional and cognitive restructuring, is highly dependent on patient adherence and the therapeutic environment. Physical treatment modalities likewise exhibit considerable inter-individual variability in efficacy.9 Accordingly, the investigation of novel, safer, and more effective therapeutic strategies capable of directly targeting aberrant neural activity at the level of brain function has emerged as a pivotal research priority in psychiatric rehabilitation.10
Against this backdrop, brain–computer interface-based neurofeedback training (BCI-NFT) has attracted considerable attention as an emerging neuromodulatory intervention.11 This technology aims to overcome the shortcomings of conventional approaches by providing individuals with real-time feedback of their own neural activity characteristics, thereby guiding active self-regulation of aberrant brain functional states and promoting neuroplasticity-based reorganization and functional recovery.12 It is also noteworthy that BCI-based neurofeedback technology has sparked broad exploration in the field of sports neuroscience—researchers have begun applying it to the optimization of athletes’ psychological performance and competitive state regulation, accumulating in the process a neuromodulatory methodology that shares common mechanisms with depression rehabilitation training.13 This cross-disciplinary accumulation of research provides an important methodological reference for the standardized application of BCI-NFT in psychiatric rehabilitation. It should be noted that the brain–computer interface (BCI), neurofeedback (NF), and brain–computer interface-based neurofeedback training (BCI-NFT) are conceptually related yet distinct: the BCI is a general technical framework that establishes a communication channel between the brain and external devices; NF is a training method that guides self-regulation through real-time feedback of brain activity; and BCI-NFT is a specific intervention modality that deeply integrates the real-time decoding capabilities of the BCI with the closed-loop learning mechanisms of NF, and it constitutes the core analytical focus of this review. Although several reviews have addressed the application of NF or the BCI in psychiatry, the existing literature still lacks a systematic comparison of non-invasive and invasive technical pathways, an integration of the cross-disciplinary perspective of sports neuroscience, and a synthesis of the evidence on combined intervention paradigms; this review aims to fill these gaps. This review successively addresses the theoretical foundations, neural mechanisms, principal technical modalities (non-invasive and invasive), and combined intervention paradigms of BCI-NFT; explores emerging research directions from the intersecting perspectives of sports neuroscience and psychiatric rehabilitation medicine; and finally discusses current limitations and future development pathways, with the goal of informing the positioning of BCI-NFT within a comprehensive treatment framework and advancing the standardization of neuromodulatory intervention pathways.
Literature Search Strategy
This review was conducted as a narrative review to synthesize current evidence on the application of brain–computer interface-based neurofeedback training (BCI-NFT) in the rehabilitation of major depressive disorder (MDD). A comprehensive literature search was performed in PubMed, Web of Science, and PsycINFO databases, covering publications from January 2000 to February 2026. The following search terms were used, either individually or in combination: “brain–computer interface,” “neurofeedback,” “neurofeedback training,” “major depressive disorder,” “depression rehabilitation,” “EEG neurofeedback,” “fMRI neurofeedback,” “fNIRS neurofeedback,” “real-time fMRI,” “deep brain stimulation,” “closed-loop neuromodulation,” “neuroplasticity,” “functional connectivity,” “default mode network,” “aerobic exercise,” and “sports neuroscience.”
Inclusion criteria were: (1) peer-reviewed original research articles, randomized controlled trials, systematic reviews, or meta-analyses; (2) studies directly addressing BCI or neurofeedback interventions in human participants diagnosed with MDD or related depressive disorders; (3) studies reporting neurophysiological outcomes, clinical symptom measures, or mechanistic findings relevant to depression rehabilitation. Studies were excluded if they were (1) case reports with fewer than five participants (unless of exceptional methodological significance), (2) conference abstracts without full-text availability, or (3) studies exclusively focused on non-depressive psychiatric or neurological conditions without relevance to the themes of this review. Additional references were identified through manual screening of bibliographies of retrieved articles and highly cited reviews in the field. A total of 84 references were ultimately included. Given the narrative nature of this review, no formal risk-of-bias assessment was conducted; however, methodological quality was considered qualitatively when interpreting the strength of evidence.
Theoretical Foundations of Brain–Computer Interface-Based Neurofeedback Training
The brain–computer interface (BCI) is an emerging technology in the field of neural rehabilitation that establishes a direct communication channel between the brain and external devices for real-time information exchange and control.14 By creating a direct interactive pathway between neural signals and external hardware, BCIs enable the acquisition, decoding, and feedback of neural information, thereby opening novel avenues for the modulation of brain function.15 BCIs are generally classified into two categories: invasive BCIs and non-invasive BCIs. Invasive BCIs typically employ stereotactic neurosurgical implantation of microelectrode arrays into the cerebral cortex or deep brain structures, enabling direct acquisition of neural signals with high spatiotemporal resolution.16 While offering significant advantages in signal fidelity and decoding efficiency, their clinical application is constrained by surgical risks, ethical concerns, and long-term safety considerations, and thus they are primarily investigated in the context of severe neural dysfunction such as treatment-resistant depression.17
Non-invasive BCIs, represented by electroencephalography (EEG) and functional near-infrared spectroscopy (fNIRS), facilitate real-time acquisition and feedback of brain activity without neurosurgical intervention, offering high safety, strong reproducibility, and favorable patient compliance (Figure 1).18 Consequently, they have been more widely adopted in rehabilitation research targeting MDD and other psychiatric and emotion-related disorders.19
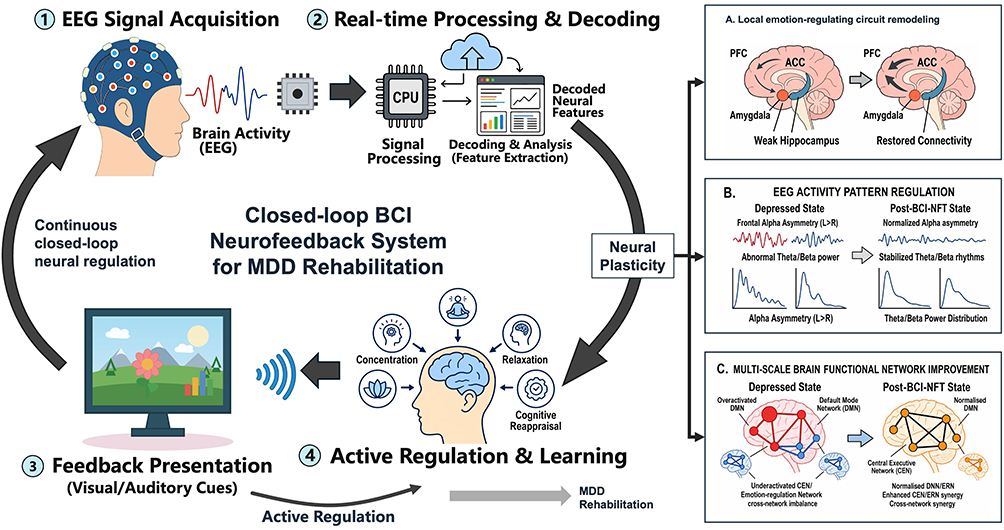 |
Figure 1 Closed-loop BCI neurofeedback system for MDD rehabilitation. This figure illustrates the closed-loop architecture and therapeutic logic of a brain–computer interface-based neurofeedback training (BCI-NFT) system for major depressive disorder (MDD) rehabilitation. The system continuously acquires EEG signals reflecting ongoing brain activity, processes and decodes neural features in real time, and transforms the decoded information into visual or auditory feedback cues that can be perceived by the patient. Through repeated feedback-guided practice, patients engage in active self-regulation strategies such as concentration, relaxation, and cognitive reappraisal, thereby forming a continuous cycle of neural signal acquisition, decoding, feedback presentation, and adaptive regulation. This closed-loop process is proposed to promote neuroplasticity and support MDD rehabilitation through multiple interconnected pathways, including remodeling of local emotion-regulating circuits, normalization of aberrant EEG activity patterns, and improvement of multi-scale brain functional network connectivity. Abbreviations: BCI-NFT, brain–computer interface-based neurofeedback training; MDD, major depressive disorder; EEG, electroencephalography; PFC, prefrontal cortex; ACC, anterior cingulate cortex; DMN, default mode network; CEN, central executive network; ERN, emotion-regulation network. |
In recent years, a growing consensus has emerged in psychiatric and neuroscientific research on MDD that brain function is not immutably fixed. Under specific training and feedback conditions, the brain is capable of undergoing significant neuroplastic change.20 This premise enables neural activity to transition from a static pathological marker to an interventional and trainable functional target. Neurofeedback training is grounded in this principle: it presents an individual’s own neural activity state in real time through intuitive visual or auditory modalities, allowing trainees to progressively acquire volitional control over their own brain activity through repeated practice.21
At its core, neurofeedback constitutes a learning process in which brain activity serves as the locus of regulation, with the ultimate therapeutic outcome contingent upon the neural self-regulation strategies developed by the individual under feedback conditions.22 BCI-NFT represents a modality of neural functional modulation developed at the intersection of neurofeedback and modern BCI technology. It tightly integrates the learning mechanisms of neurofeedback with the real-time decoding capabilities of BCIs, transforming the training process from experience-based heuristic regulation to a closed-loop control paradigm driven by neural signals.23
In practice, EEG or cerebral blood flow signals are decoded online and presented instantaneously, fostering a dynamic cycle of “neural activity – system feedback – active self-regulation” in the trainee.24 This closed-loop architecture establishes, across the temporal dimension, a stable correspondence between changes in neural activity and self-regulation strategies—a defining feature that distinguishes BCI-NFT from conventional psychological training.25
From a theoretical genealogy perspective, the closed-loop control learning framework of BCI-NFT is highly congruent with the classical motor skill acquisition theories in sports science. Adams’ pioneering closed-loop theory of motor learning revealed the central role of sensory feedback signals in motor error correction and skill consolidation;26 biofeedback training, as a traditional practice tool in sports science, has for decades continuously used peripheral physiological parameters—such as electromyography and heart rate—to guide athletes in real time toward optimized movement patterns and psychological competitive states. BCI-based neurofeedback can be regarded as a deepened extension of this methodological framework at the level of central neural signals—upgrading the feedback target from peripheral physiological indices to the electrophysiological or hemodynamic characteristics of the brain, thereby achieving closed-loop regulation of internal states at a more refined neural level.27 This methodological inheritance not only provides a sports science perspective to support the theoretical explanation of BCI-NFT in depression rehabilitation, but also endows the operational learning optimization experience accumulated in sports neuroscience with direct reference value.
From a theoretical perspective, the core rationale underlying BCI-NFT resides in its capacity to promote neuroplasticity and facilitate the reorganization of brain functional networks.28 Through the systematic and repeated reinforcement of activity in target brain regions or networks, this training modality can induce synaptic plasticity and promote rebalancing of functional connectivity.29
The integration of multimodal technical approaches further provides spatial localization and temporal synchronization information, enhancing the correspondence between training targets and feedback signals.30 Importantly, BCI-NFT places strong emphasis on active participation by the trainee throughout the regulatory process. This subject-centered, participatory approach not only induces changes in neurotransmitter systems and synaptic structure, but also fosters an enhanced sense of self-efficacy.31 The physiological changes attributable to neuroplasticity and the psychological gains in perceived self-control operate synergistically during training, jointly constituting the theoretical foundation through which this technology exerts its interventional effects.25
Neural Mechanisms Underlying the Facilitation of MDD Rehabilitation by BCI-NFT
Patients with MDD exhibit characteristic neurophysiological features including functional imbalances in emotion-regulation-related brain regions, aberrant EEG rhythms, and disrupted functional connectivity within brain networks. Neurofeedback training provides a novel technical approach for precise intervention at the level of neural function.32 Unlike conventional treatments, BCI-NFT does not exert its effects through direct exogenous stimulation of the nervous system. Rather, it guides patients to actively regulate aberrant neural functional states through real-time feedback of their own brain activity characteristics.33 This regulatory process promotes neural functional remodeling and neuroplastic change (Figure 2).34 Based on current neuroscientific frameworks, the facilitative effects of BCI-NFT on MDD rehabilitation are primarily manifested across three dimensions: the remodeling of function in emotion-regulation-related brain regions, the modulation of aberrant EEG activity patterns, and the improvement of functional network connectivity.35 Mechanistically, these three dimensions constitute a continuum progressing from the restoration of local regulatory function and the stabilization of rhythmic activity to the reconstruction of cross-network coordination.36
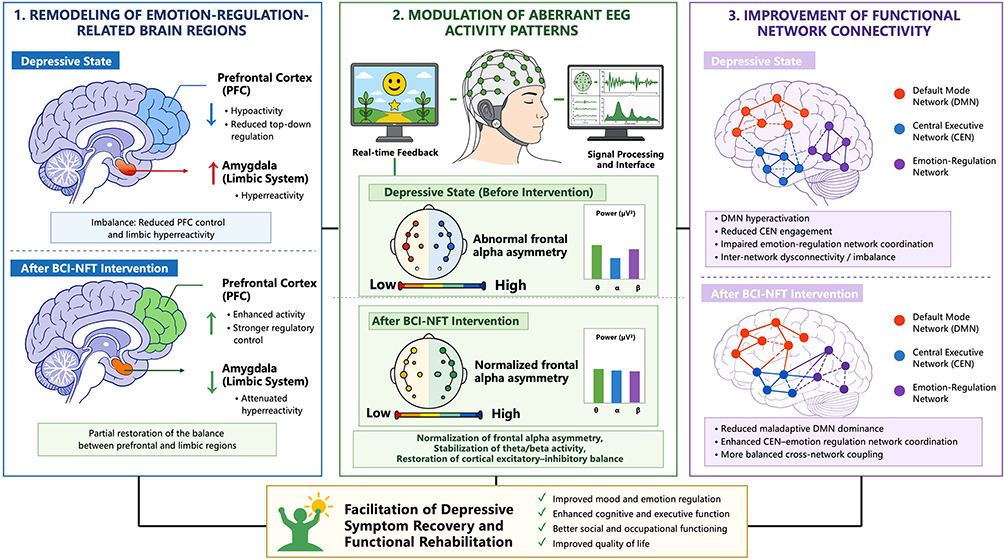 |
Figure 2 Mechanistic pathways through which BCI-NFT facilitates MDD rehabilitation. This figure illustrates the proposed neural remodeling mechanisms through which brain–computer interface-based neurofeedback training (BCI-NFT) may facilitate rehabilitation in major depressive disorder (MDD). In the depressive state, impaired prefrontal regulatory control, limbic hyperactivity, aberrant EEG rhythmic activity, and disrupted large-scale functional network connectivity jointly contribute to emotional dysregulation, repetitive negative thinking, and impaired cognitive–affective functioning. Through closed-loop acquisition, processing, and real-time feedback of neural signals, BCI-NFT enables patients to actively regulate abnormal brain activity and gradually promotes neuroplastic reorganization. This process may enhance prefrontal top-down control, attenuate amygdala and limbic hyperreactivity, normalize frontal alpha asymmetry and theta/beta activity, reduce maladaptive default mode network dominance, and strengthen coordination between central executive and emotion-regulation networks. Collectively, these regional, rhythmic, and network-level changes may support depressive symptom recovery and broader functional rehabilitation, including improvements in mood regulation, cognitive and executive function, social and occupational functioning, and quality of life. Abbreviations: BCI-NFT, brain–computer interface-based neurofeedback training; MDD, major depressive disorder; PFC, prefrontal cortex; EEG, electroencephalography; DMN, default mode network; CEN, central executive network. |
Remodeling of Function in Emotion-Regulation-Related Brain Regions
Functional dysregulation of emotion-regulation-related brain regions constitutes a fundamental neural substrate of MDD.37 Patients with MDD broadly exhibit functional imbalances across the prefrontal cortex (PFC), amygdala, cingulate cortex, and hippocampus, with the most characteristic pattern being a concurrent reduction in PFC activity alongside limbic system hyperreactivity.38 This combined state of diminished regulatory capacity and heightened reactivity substantially impairs cognitive control over negative emotions, rendering patients more susceptible to persistent low mood and ruminative negative thinking.39
BCI-NFT delivers the activity states of these emotion-related brain regions in real time to the trainee via visual or auditory feedback.40 Because patients cannot directly perceive activity changes in deep brain structures, the BCI system computes and presents signal intensity in real time, providing the brain with precise reward signals.41 Through repeated closed-loop training sessions, patients gradually acquire internal strategies for volitionally modulating the activity levels of target brain regions.42
At the neural mechanistic level, this active regulation enhances activation of the dorsolateral and ventromedial PFC while concurrently suppressing the amygdala’s exaggerated response to negative emotional stimuli.43 This process augments prefrontal regulatory signaling and induces inverse coupling changes relative to limbic system reactivity.44 The resulting reestablishment of prefrontal–limbic system functional balance directly repairs the neural circuitry underlying emotion regulation,45 and further influences overall cortical excitatory–inhibitory balance, thereby exerting an upstream modulatory effect on the subsequent stabilization of rhythmic neural activity.46
Modulation of Aberrant EEG Activity Patterns
Beyond structural and functional abnormalities in specific brain regions, patients with MDD also broadly exhibit disrupted EEG activity patterns, most notably characterized by frontal alpha-wave asymmetry and aberrant theta- and beta-band power.47 These rhythmic alterations reflect a shift in the cortical excitatory–inhibitory balance.48 For example, a relative increase in left frontal alpha power indicates insufficient activity in that region—an EEG asymmetry closely associated with negative affective processing and reduced motivation, consistent with the observed decline in prefrontal regulatory capacity.49
BCI-NFT can directly target these characteristic EEG indices to exert its mechanistic effects.50 By continuously monitoring patients’ EEG signals, it guides them to consciously regulate neural activity in specific frequency bands.51 Mechanistically, this volitional modulation of aberrant neural rhythms may be viewed as the rhythmic expression of restored prefrontal regulatory function.52 Through active engagement in feedback-driven regulation, patients bring about a physiologically meaningful correction of frontal alpha asymmetry while guiding theta- and beta-band power distributions toward greater stability.53
This transition of EEG rhythms from a pathological to a relatively balanced state marks the progressive restoration of the brain’s overall emotion-regulation capacity.54 The stabilization of neural rhythms not only depends on improvements in higher-level regulatory brain regions but also furnishes a coherent and consistent temporal structure for inter-network information transmission.
Improvement of Functional Network Connectivity
In recent years, large-scale brain functional network dysregulation has emerged as an important framework for understanding the neural mechanisms of MDD.55 Patients with MDD typically manifest hyperactivation of the default mode network (DMN) accompanied by significant hypofunction of the central executive network and emotion-regulation-related networks.56 This inter-network imbalance predisposes patients to excessive internally focused, negative self-referential processing while undermining attentional and executive engagement with external tasks.57
BCI-NFT, through feedback-driven regulation of activity in specific brain regions or individual networks, can promote the reintegration of functional connectivity at the higher-dimensional level of network organization.58 Modern BCI systems are increasingly capable of computing inter-nodal phase synchrony or functional coupling strength in real time, thereby providing feedback for complex network connectivity.59
The mechanistic basis for this rests upon the enhanced prefrontal regulatory capacity and the temporal synchronization conditions afforded by EEG rhythm stabilization.60 At the level of network modulation, repeated reinforcement via neurofeedback effectively attenuates DMN hyperactivation while strengthening the coordinated interaction between the PFC-dominated central executive network and emotion-regulation networks.61
This improvement in cross-network functional coupling disrupts the ruminative thought cycle and provides a network topology foundation for enhanced cognitive control.62 From a neuroscientific standpoint, BCI-NFT offers a scientifically grounded interventional pathway for MDD rehabilitation—one that originates from localized brain region modulation and progressively extends to global network reorganization.63 Together with the restoration of regional brain function and the stabilization of EEG activity, this constitutes a complete, bottom-up, hierarchically progressive neural remodeling mechanism.
Application Modalities of BCI-NFT in MDD Rehabilitation
The application of BCI-NFT in MDD rehabilitation has, in recent years, advanced beyond the early stage of technical feasibility exploration and entered a new phase of evidence-based data accumulation and intervention paradigm standardization.64 With the introduction of precision psychiatry concepts for MDD, the volume of related research has grown exponentially.65 Study designs have progressively evolved from small, uncontrolled open-label trials to rigorous randomized clinical trials employing sham feedback as a double-blind control condition.66 In parallel, systematic reviews and meta-analyses of this technology have proliferated substantially.67
This signals a paradigmatic shift in research focus from preliminary evaluation of single-technology efficacy toward cross-modal comparative analysis, quantification of intervention dosage, and stratification of eligible patient populations according to distinct neurobiological subtypes.68 In terms of specific clinical application pathways, BCI-based neurofeedback is primarily divided into two broad categories based on differences in the physical barrier of neural signal acquisition and the depth of the targeted network: non-invasive and invasive modalities.69 Table 1 summarizes the key characteristics, advantages, limitations, and clinical applicability of non-invasive and invasive BCI-NFT modalities in MDD rehabilitation.
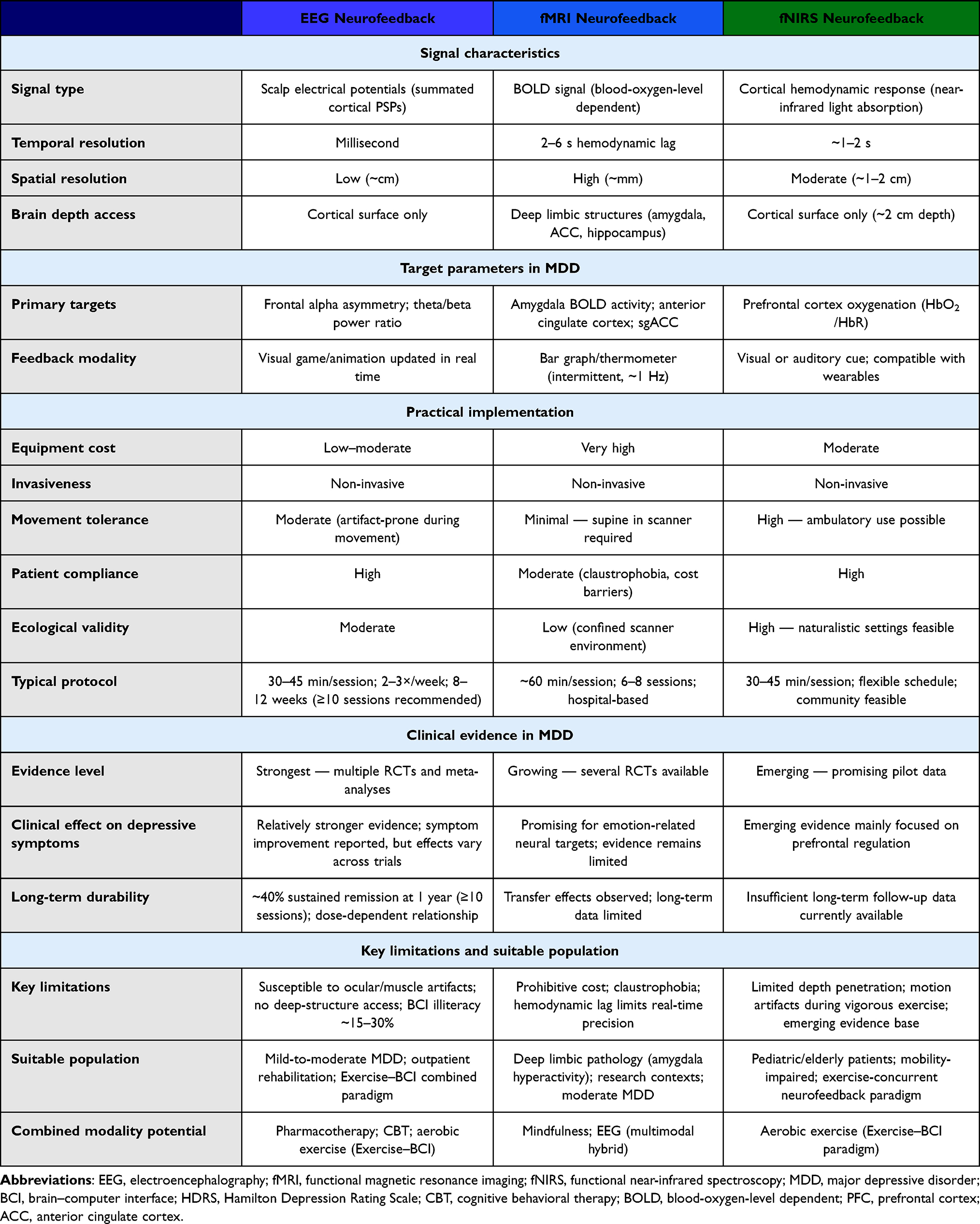 |
Table 1 Comparative Analysis of Non-Invasive BCI-Based Neurofeedback Modalities for MDD Rehabilitation. The Three Modalities are Compared Across Five Domains: Signal Characteristics, Primary Targets in MDD, Practical Implementation, Clinical Evidence, and Suitable Patient Populations |
These two technical pathways fulfill distinctly different roles within a comprehensive treatment framework: non-invasive modalities are highly safe and better suited for long-term, high-frequency repeated training during the rehabilitation phase,70 whereas invasive modalities are constrained by ethical considerations and procedural risks and are primarily reserved as a last-resort intervention for cases of treatment-resistant depression.71 Furthermore, as interdisciplinary integration deepens, combined application paradigms that incorporate BCI with conventional psychotherapy and pharmacotherapy are increasingly emerging as a clinical trend for strengthening individual neuroregulatory capacity and reducing disease recurrence.72
Non-Invasive BCI Neurofeedback Training Modalities
Non-invasive BCIs represent the most central and extensively applied mainstream direction in MDD neurofeedback research. EEG, fMRI, and fNIRS constitute the three most commonly employed non-invasive technical pathways,63 forming a complementary triad in terms of temporal resolution, spatial localization precision, and equipment accessibility. EEG detects weak potential changes on the scalp surface and, with millisecond-level temporal resolution, reflects the summated postsynaptic potentials of cortical pyramidal cells, making it the most clinically operable modality currently available. fMRI, through measurement of blood-oxygen-level-dependent (BOLD) signals, enables precise localization of deep limbic structures such as the amygdala and hippocampus with millimeter-level spatial resolution. fNIRS, as an intermediate solution, leverages the absorption and scattering properties of near-infrared light in biological tissue to monitor cerebral cortical hemodynamic changes, and—unconstrained by the confined MRI scanner bore—demonstrates considerable flexibility in naturalistic ecological environments and during movement.
Additionally, fNIRS, by virtue of its capacity to monitor cerebral hemodynamic changes in naturalistic movement states, has been widely applied in the field of sports neuroscience to study the relationships among physical activity, cognitive function, and brain function.73 Given its favorable tolerance to movement, fNIRS has been extensively used for monitoring cerebral cortical hemodynamic changes during walking, cycling, and other exercise tasks, thereby becoming an important technical tool in sports neuroscience research on the physical activity–cognition–brain function relationship.74 This characteristic also provides the technical foundation for constructing an “exercise-concurrent neurofeedback”75 intervention paradigm, enabling participants to simultaneously receive real-time feedback training on prefrontal cortex activity while performing moderate-intensity aerobic exercise.76
Implementation of non-invasive neurofeedback is a highly complex process of human–machine interaction and neural learning, typically comprising four intensive closed-loop steps: neural signal acquisition, feature extraction, real-time computation, and feedback presentation. Taking the clinically most prevalent EEG pathway as an example: trainees first don an EEG cap equipped with 32 to 128 electrode nodes in a quiet treatment room shielded from electromagnetic interference. Following impedance reduction with conductive gel, the system continuously records weak scalp electrical activity across multiple regions in real time. Backend signal-processing algorithms must then, within a minimal delay (typically strictly controlled to under 300 milliseconds), employ mathematical tools such as independent component analysis or fast Fourier transform to eliminate physiological artifacts—including ocular and myoelectric signals—and decompose the complex time-domain signal into power spectral density across frequency bands. The extracted target EEG features are then transformed into perceptually accessible multimedia signals for the patient—for example, a three-dimensional racing game, a gradually blossoming lotus flower, or a rising-and-falling thermometer displayed on screen—wherein the animation speed or color saturation is precisely synchronized with the degree to which target EEG indices approach the healthy range.
Driven by this closed-loop feedback, trainees must exercise considerable volitional engagement, continuously attempting various internal psychological strategies—such as recalling positive autobiographical memories, practicing diaphragmatic breathing, or applying mindful awareness—in response to the on-screen visual cues. Through this process of operant conditioning—repeated tens of thousands of times as “attempt–system feedback–strategy modification”—the trainee’s cerebral cortex gradually establishes new synaptic connections, progressively learning to stabilize its own neural rhythms within the prescribed healthy threshold, either consciously or non-consciously. In standard clinical practice, a single BCI-NFT session generally lasts 30 to 45 minutes; to counteract neural forgetting mechanisms and consolidate long-term potentiation effects, intervention frequency is typically set at two to three sessions per week, with the overall treatment course spanning six to twelve weeks.
Existing clinical intervention data increasingly reveal patterns of outcomes based on different technical targets and control conditions. Among EEG-based feedback paradigms, frontal alpha-wave asymmetry training has the highest level of supporting evidence. A rigorous double-blind randomized controlled trial enrolling 60 patients with mild-to-moderate MDD demonstrated that following 12 sessions of active EEG neurofeedback training, participants in the experimental group showed a mean reduction of 7.2 points on the Hamilton Depression Rating Scale (HDRS), compared with a decline of only 3.1 points in the sham-feedback control group, which received randomized video playback.53 Multiple large-scale meta-analyses encompassing hundreds of patients further confirmed that EEG neurofeedback yields an overall effect size of approximately 0.6 for improving core depressive symptoms, corresponding to a medium-to-large clinical effect.54 Long-term follow-up data also reveal a significant dose–response relationship: when the number of training sessions falls below eight, neuroplastic changes tend to be insufficiently consolidated and symptom relapse is common;60 however, when systematic training reaches or exceeds ten sessions, synaptic-level changes stabilize, and studies with follow-up durations of up to one year report that approximately 40% of patients maintain significant symptom remission following cessation of training, demonstrating the durable anti-relapse potential of actively learned neural self-regulation strategies.61
By contrast, fMRI-based feedback paradigms demonstrate an overwhelming advantage in spatial targeting precision. In a typical fMRI-guided training session, patients lying in the MRI scanner perform emotion-regulation tasks while the system—accounting for the natural hemodynamic response lag of 2 to 6 seconds—dynamically feeds back activation levels in deep brain structures such as the amygdala or anterior cingulate cortex, typically via intermittent bar graphs. A randomized controlled trial directly targeting “reduced left amygdala hyperactivation” showed that after only eight sessions of high-precision regional BOLD feedback training, participants in the experimental group achieved a mean HDRS reduction of points.65 As an emerging alternative, fNIRS technology has also demonstrated impressive efficacy in remodeling prefrontal cortex function,67 while avoiding the prohibitive costs and claustrophobia risks associated with fMRI and exhibiting particularly high compliance during extended continuous training in pediatric and elderly depressed populations.
Invasive BCI Neurofeedback Training Modalities
In contrast to non-invasive approaches, which leverage the compensatory and reorganizational capacity of the cerebral cortex, invasive BCIs directly target the deep subcortical nuclei that exert decisive influence over emotion generation—structures that remain largely inaccessible to conventional non-invasive modalities.64 In terms of signal acquisition stability, dynamic range across high-frequency bands, and absolute spatial localization accuracy, this modality possesses physical advantages unmatched by any other currently available technology. At the level of clinical implementation, the system requires stereotactic neurosurgical implantation of multi-contact microelectrode arrays with sub-millimeter precision into the cortical surface or deep structures of the basal ganglia and limbic system, along with subcutaneous implantation of a pulse generator beneath the clavicle. Following implantation, these electrodes—embedded within brain tissue—serve as continuous neural activity sentinels, recording local field potentials or discharge sequences of neuronal ensembles in target nuclei. An onboard embedded computer system performs uninterrupted real-time decoding of these raw signals, analyzing amplitude, phase coupling, and high-frequency gamma-band power fluctuations to identify specific “neuropathological biomarkers” closely correlated with acute worsening of depressive symptoms, anxiety episodes, or surges in ruminative thinking.
Fundamentally distinct from non-invasive systems—which rely heavily on the patient’s concentrated attention for “active learning and regulation”—modern invasive closed-loop systems operate as fully automated, covert intervention devices. When the background artificial intelligence classification algorithm detects an abnormal neural signal pattern highly consistent with a depressive episode, the system automatically triggers the embedded micro-current stimulation device within milliseconds, delivering precisely calibrated electrical pulses to forcibly interrupt pathological network synchronous oscillations and restore the target brain region from a state of hyperactivation or inhibition to a preset healthy physiological baseline. This intervention pathway entirely bypasses the patient’s subjective cognition and behavioral effort, constituting a purely automated, neural-biomarker-driven modulation of physical parameters. Consequently, the individualized configuration of stimulation frequency, pulse width, and output current intensity to accommodate each patient’s heterogeneous neural phenotype represents the core technical challenge determining treatment success or failure.
Given the inevitable procedural trauma of cranial surgery, the risk of foreign-body-induced immunological responses, and the uncertain effects of chronic electrical stimulation on the brain microenvironment, the clinical application of invasive BCIs has been strictly restricted by international medical ethics committees to the context of orphan-drug-equivalent rescue treatment for patients with treatment-resistant depression (TRD). More recently, with the introduction of genuinely closed-loop neuromodulation systems, both the efficacy and dropout rates of invasive treatment have improved qualitatively. Cutting-edge small-sample closed-loop studies targeting TRD report that, by delivering electrical stimulation only upon detection of depressive neural signatures, not only was device power consumption and the risk of long-term stimulation-related side effects substantially reduced, but approximately 50% of patients achieved complete symptom remission at 12-month follow-up,62 with precipitous declines in depression rating scale scores. Overall, invasive closed-loop systems can produce rapid and dramatic symptom reversal within days to weeks, with the therapeutic mechanism closely tied to the direct disruption of abnormal electrophysiological oscillations within pathological neural circuits. Nevertheless, large-scale dissemination remains confronted with formidable challenges relating to ethics, health economics, and long-term safety.
Combined Application of BCI-NFT with Conventional Rehabilitation Modalities
MDD is not a simple disorder attributable to a single neurotransmitter deficit or isolated brain region pathology; rather, it is a complex, multi-level systemic functional dysregulation spanning molecular, cellular, network, psycho-cognitive, and social-environmental dimensions. Therefore, organically integrating BCI-NFT into existing comprehensive psychiatric treatment frameworks—building neurological modulatory target-specific training on top of established conventional therapies—is rapidly becoming the leading edge of current clinical rehabilitation translational research. The underlying logic of this combined modality rests on exploiting differences in temporal windows, mechanistic targets, and action pathways across interventions to produce synergistic effects that exceed the sum of their individual contributions.
First, in combined application with classical antidepressant pharmacotherapy, the mechanistic complementarity of the two modalities is pronounced. Antidepressants elevate global cerebral monoaminergic neurotransmitter concentrations over several weeks by inhibiting presynaptic reuptake, effectively managing severe psychomotor retardation and suicidal ideation. However, pharmacotherapy is ill-suited to the precise correction of aberrant connectivity between specific brain regions. The introduction of BCI-NFT at this stage enables targeted editing of plastic neural networks: neurofeedback specifically remodels the dynamic balance between the PFC and the limbic system, compensating for the limitations of pharmacotherapy in localized functional regulation.
The seamless, synchronized integration of BCI with cognitive behavioral therapy (CBT) is regarded as the most conceptually innovative intensification paradigm in current psychotherapeutic practice. The core of conventional CBT lies in cognitive restructuring—training patients to identify, challenge, and replace the negative automatic thoughts that perpetuate depression. In a novel combined clinical protocol, patients sit in the treatment room with a high-precision BCI device while simultaneously receiving guidance from a psychotherapist. The system continuously monitors the real-time state of the patient’s PFC in the background. When the patient successfully applies a CBT technique to counter a negative cognition, and the system simultaneously detects a substantive increase in frontal activity indicative of rational control, an immediate, salient positive visual reward is triggered on screen. This mechanism—which binds covert mental processes to visible physiological indicators—enables the formation of a robust conditioned association between cognitive strategies and specific neural states. Clinical evidence indicates that patients receiving this synchronized combined intervention achieve markedly greater improvements on self-rated depression scales than those undergoing CBT alone, with their baseline frontal cortex activation levels also demonstrably elevated at a neurophysiological level.71
A further relatively novel modality involves combining BCI-NFT with mindfulness meditation and attentional regulation training, addressing the longstanding difficulty of objectively quantifying whether patients have genuinely achieved states of focused attention or present-moment awareness during traditional contemplative practices. Patients with MDD are highly susceptible to unconscious mind-wandering and negative ruminative cycles, characterized by hyperactivation of the DMN. In the combined intervention, patients perform mindfulness breathing or body scan practices with eyes closed while the BCI system employs algorithms to specifically monitor EEG rhythms indicative of DMN activity levels. As soon as the patient’s thoughts begin to wander, the system immediately delivers a gentle but unambiguous corrective signal, enabling patients to detect attentional lapses at their earliest onset and redirect focus to the present moment with minimal cognitive load. In sum, within the comprehensive treatment landscape for MDD and related psychiatric disorders, the pharmacotherapy-combined modality serves as the bedrock for stabilizing and sustaining therapeutic gains; the CBT-combined modality functions as a precision instrument for enhancing cognitive executive capacity; and the mindfulness-combined modality operates as a surgical tool for severing the chains of ruminative ideation. These three modalities form a perfectly complementary closed loop along the neural intervention chain.72
Beyond the three combined intervention modalities described above, the interdisciplinary convergence of sports neuroscience and BCI technology is giving rise to an emerging combined intervention paradigm that warrants dedicated attention. With the ongoing miniaturization of portable wireless EEG and fNIRS devices and improvements in their tolerance to movement,77 researchers have begun attempting to implement neurofeedback concurrently while patients perform aerobic exercise (eg., stationary cycling or treadmill walking), constructing an “Exercise–BCI” concurrent intervention paradigm. In this paradigm, lightweight dry-electrode EEG caps or wearable fNIRS probes continuously acquire prefrontal cortical neural signals during exercise and transmit them wirelessly to a compact display screen or augmented reality glasses within the patient’s visual field, where the real-time feedback interface is presented,78 enabling patients to receive targeted neuromodulatory reinforcement training while simultaneously performing aerobic exercise tasks. The theoretical rationale of this combined paradigm lies in the aerobic exercise-induced increase in prefrontal cortical blood perfusion and elevation of cortical excitability, which provides a more favorable neurophysiological window for the active learning mechanisms of neurofeedback. It is anticipated to systematically improve the neuroregulatory learnability of patients who—due to executive dysfunction and reduced motivation—are unable to effectively engage in traditional static closed-loop training (the so-called “BCI-illiterate” population).79,80 At present, clinical evidence for this combined modality remains in its early accumulation phase, and technical challenges persist in ensuring signal quality during exercise, allocating dual-task attentional resources, and matching optimal exercise intensity parameters. Nevertheless, the cross-disciplinary integration prospects it demonstrates have attracted widespread attention from both the sports neuroscience and psychiatric rehabilitation communities.
Limitations and Future Directions of BCI-NFT in MDD Rehabilitation
Although BCI-NFT has demonstrated enormous potential in the domain of non-invasive neuromodulation for MDD, substantial challenges remain before it can achieve large-scale clinical implementation.
First, the heterogeneity of clinical evidence and the absence of standardized experimental design represent a fundamental obstacle. Most existing randomized controlled trials involve relatively small sample sizes (typically fewer than 100 participants), and different research teams adopt divergent protocols for key training parameters, including the selection of target brain regions, feedback frequency band definitions, baseline calibration methods, session duration, and total treatment course; in addition, some studies lack clearly defined inclusion and exclusion criteria as well as formal methodological quality assessment, which reduces comparability across studies. This methodological inconsistency significantly limits cross-study comparison and synthesis and also makes it difficult to conduct systematic risk-of-bias assessments of existing studies. Consequently, systematic reviews and meta-analyses have repeatedly highlighted that such heterogeneity substantially weakens the reliability of current clinical evidence55 and greatly complicates the development of standardized clinical practice guidelines.56
Second, the attribution of therapeutic efficacy remains a persistent methodological challenge in neurofeedback research. In complex clinical environments, it is difficult to determine whether symptom improvement results from genuine neural rhythm modulation or from non-specific psychosocial influences. The use of advanced technological equipment, strong psychological expectations associated with cutting-edge therapies, frequent therapist–patient interactions, and the novelty of the treatment environment may all produce significant placebo-like therapeutic effects.81 Moreover, implementing rigorous sham-feedback control conditions is technically difficult and may raise ethical concerns; in some studies, participants are even able to identify the sham-feedback condition, making true double-blinding difficult to achieve. Therefore, developing stricter double-blind experimental paradigms capable of distinguishing neurobiologically specific treatment effects from psychosocial influences remains an essential methodological task in the current stage of clinical validation.
Third, the phenomenon of BCI illiteracy and substantial inter-individual variability further constrain the universal applicability of neurofeedback interventions. Empirical studies suggest that approximately 15%–30% of patients with MDD fail to acquire effective strategies for self-regulating neural signals even after repeated closed-loop training sessions.82 Core symptoms of MDD, including anhedonia, attentional impairment, executive dysfunction, and reduced motivation, may significantly hinder patients’ ability to engage in cognitively demanding neurofeedback learning tasks. This large degree of inter-individual variability indicates that uniform training protocols cannot be universally applied across patient populations. In addition, modality-specific technical limitations remain evident. EEG signals are highly susceptible to ocular artifacts, muscle activity, and subtle head movements, which may be incorrectly interpreted by algorithms as successful neural regulation. Meanwhile, the high operational costs of fMRI and the confined scanning environment limit its scalability in primary healthcare systems and community rehabilitation settings.
At the technical challenge level, the motion artifact interference problem confronting wearable BCIs in exercise-concurrent neurofeedback settings constitutes the core engineering bottleneck constraining further advancement of the “Exercise–BCI” combined modality. Artifacts arising during exercise—including head movement, surface electromyographic activity, and blood flow pulsation—can readily contaminate the specificity of target neural signals. Breakthrough advances are urgently needed in adaptive filtering, independent component analysis, and deep learning denoising algorithms83 to ensure the quality and reliability of neurofeedback signals during exercise, thereby establishing the hardware and algorithmic foundation for standardizing the “Exercise–BCI” combined intervention paradigm. Furthermore, how to systematically evaluate the optimal sequencing and integration schemes for different exercise types, intensities, and neurofeedback training protocols remains an important issue that the deep cross-disciplinary fusion of sports neuroscience and psychiatric rehabilitation medicine must clarify through rigorous randomized controlled trials.
Fourth, advances in interdisciplinary integration are beginning to provide new opportunities to overcome these limitations. The convergence of neuroscience, artificial intelligence, and clinical medicine is fundamentally transforming neural signal decoding technologies. Machine learning and deep learning approaches are increasingly replacing traditional linear filtering and feature extraction methods, with architectures such as convolutional neural networks enabling more precise extraction of non-linear neural features from complex EEG signals.59 In addition, reinforcement learning–based adaptive closed-loop systems are emerging as an important research direction. These systems may dynamically adjust feedback difficulty and reward mechanisms by continuously monitoring patients’ cognitive load, fatigue levels, and learning trajectories, thereby improving engagement and potentially reducing the impact of BCI illiteracy.
Fifth, hardware evolution and multimodal integration are gradually overcoming the limitations of single-modality neural recording. Multimodal neurofeedback systems that combine EEG with fMRI or fNIRS are increasingly used in mechanistic studies.57 This approach integrates the millisecond-level temporal resolution of EEG with the high spatial resolution of hemodynamic imaging techniques. As a result, researchers can simultaneously observe electrophysiological dynamics in cortical oscillations and hemodynamic responses in deeper emotional circuits, providing a more comprehensive spatiotemporal understanding of whole-brain functional network modulation.
Finally, from the perspective of clinical translation, future neurofeedback research is likely to shift toward a precision psychiatry framework. Given the considerable neurobiological heterogeneity of MDD, individualized treatment strategies will become increasingly important. In this paradigm, resting-state fMRI or high-density EEG data may first be used to stratify patients into distinct neurobiological subtypes before intervention. Neurofeedback targets, feedback modalities, and treatment dosage could then be tailored according to specific neural characteristics, such as default mode network hyperactivity or deficits in dorsolateral prefrontal cortex cognitive control circuits.58 With the continued development of large-scale multicenter randomized controlled trials and long-term outcome studies, BCI-NFT may gradually transition from an exploratory experimental technique to a standardized clinical intervention for MDD and related psychiatric disorders.84
Conclusion
Brain–computer interface‑based neurofeedback training represents a rapidly developing neuromodulatory approach for the rehabilitation of major depressive disorder. By enabling patients to actively regulate neural activity through real‑time feedback, BCI‑NFT targets the neurophysiological substrates of depression rather than focusing solely on symptomatic treatment. The preliminary evidence synthesized in this narrative review suggests that BCI‑NFT may facilitate recovery through the remodeling of emotion‑regulation‑related brain regions, normalization of abnormal EEG rhythms, and restoration of functional connectivity within large‑scale neural networks; however, it should be noted that this evidence derives mainly from early studies with limited sample sizes, and the generalizability of these conclusions remains to be tested in large-scale randomized controlled trials. Compared with traditional therapeutic approaches, this technology offers the advantage of patient‑centered neural self‑regulation and the potential for personalized intervention. However, important challenges remain, including heterogeneity in training protocols, limited large‑scale clinical trials, placebo effects that are difficult to fully exclude, and uncertainty regarding optimal target signals and feedback strategies. Future research integrating multimodal neuroimaging, advanced machine‑learning algorithms, and precision psychiatry frameworks may further improve the efficacy and standardization of BCI‑NFT interventions. Overall, BCI-NFT demonstrates the potential to become an important component of comprehensive treatment strategies for major depressive disorder; however, its broad adoption in routine clinical practice will still depend on the continued accumulation and validation afforded by larger-scale multicenter randomized controlled trials, the establishment of standardized training protocols, and long-term follow-up outcome studies.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Malhi GS, Mann JJ. Depression. Lancet. 2018;392(10161):2299–16. doi:10.1016/S0140-6736(18)31948-2
2. World Health Organisation. Depression and Other Common Mental Disorders: global Health Estimates. 2017. Available from: https://apps.who.int/iris/handle/10665/254610.
3. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/S2215-0366(18)30511-X
4. Zhang J, Zhang D, Xue X, Wang X, Ding S, Ma Y. Intergenerational Psychological Capital, Disability, and Depressive Symptoms in the Shadow of Functional Deprivation Among Middle-Aged and Older Adults in China. Psychol Res Behav Manag. 2025;2025:2237–2257.
5. Collaborators GBDMD. Global, regional, and national burden of 12 mental disorders in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Psychiatry. 2022;9(2):137–150. doi:10.1016/S2215-0366(21)00395-3.
6. Correll CU, Solmi M, Veronese N, et al. Prevalence, incidence and mortality from cardiovascular disease in patients with pooled and specific severe mental illness: a large-scale meta-analysis of 3,211,768 patients and 113,383,368 controls. World Psychiatry. 2017;16(2):163–180. doi:10.1002/wps.20420
7. Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. 2018;391(10128):1357–1366. doi:10.1016/S0140-6736(17)32802-7
8. Fava GA, Gatti A, Belaise C, Guidi J, Offidani E. Withdrawal Symptoms after Selective Serotonin Reuptake Inhibitor Discontinuation: a Systematic Review. Psychother Psychosom. 2015;84(2):72–81. doi:10.1159/000370338
9. Brunoni AR, Sampaio-Junior B, Moffa AH, et al. Noninvasive brain stimulation in psychiatric disorders: a primer. Braz J Psychiatry. 2019;41(1):70–81. doi:10.1590/1516-4446-2017-0018
10. Williams LM. Precision psychiatry: a neural circuit taxonomy for depression and anxiety. Lancet Psychiatry. 2016;3(5):472–480. doi:10.1016/S2215-0366(15)00579-9
11. Sitaram R, Ros T, Stoeckel L, et al. Closed-loop brain training: the science of neurofeedback. Nat Rev Neurosci. 2017;18(2):86–100. doi:10.1038/nrn.2016.164
12. Ros T, Enriquez-Geppert S, Zotev V, et al. Consensus on the reporting and experimental design of clinical and cognitive-behavioural neurofeedback studies (CRED-nf checklist). Brain. 2020;143(6):1674–1685. doi:10.1093/brain/awaa009
13. Mirifar A, Beckmann J, Ehrlenspiel F. Neurofeedback as supplementary training for optimizing athletes’ performance: a systematic review with implications for future research. Neurosci Biobehav Rev. 2017;75:419–432. doi:10.1016/j.neubiorev.2017.02.005
14. Wolpaw JR, Wolpaw EW. Brain-Computer Interfaces: Principles and Practice. Oxford University Press; 2012.
15. Millan JD, Rupp R, Muller-Putz GR, et al. Combining Brain-Computer Interfaces and Assistive Technologies: state-of-the-Art and Challenges. Front Neurosci. 2010;4:1. doi:10.3389/fnins.2010.00161
16. Chaudhary U, Birbaumer N, Ramos-Murguialday A. Brain-computer interfaces for communication and rehabilitation. Nat Rev Neurol. 2016;12(9):513–525. doi:10.1038/nrneurol.2016.113
17. Figee M, Riva-Posse P, Choi KS, Bederson L, Mayberg HS, Kopell BH. Deep Brain Stimulation for Depression. Neurotherapeutics. 2022;19(4):1229–1245. doi:10.1007/s13311-022-01270-3
18. Lotte F, Bougrain L, Cichocki A, et al. A review of classification algorithms for EEG-based brain-computer interfaces: a 10 year update. J Neural Eng. 2018;15(3):031005. doi:10.1088/1741-2552/aab2f2
19. Daly JJ, Wolpaw JR. Brain-computer interfaces in neurological rehabilitation. Lancet Neurol. 2008;7(11):1032–1043. doi:10.1016/S1474-4422(08)70223-0
20. Koralek AC, Jin X, Long II JD, Costa RM, Carmena JM. Corticostriatal plasticity is necessary for learning intentional neuroprosthetic skills. Nature. 2012;483(7389):331–335. doi:10.1038/nature10845
21. Enriquez-Geppert S, Huster RJ, Herrmann CS. EEG-Neurofeedback as a Tool to Modulate Cognition and Behavior: a Review Tutorial. Front Hum Neurosci. 2017;11:51. doi:10.3389/fnhum.2017.00051
22. Thibault RT, Lifshitz M, Raz A. The self-regulating brain and neurofeedback: experimental science and clinical promise. Cortex. 2016;74:247–261. doi:10.1016/j.cortex.2015.10.024
23. Marzbani H, Marateb HR, Mansourian M. Neurofeedback: a Comprehensive Review on System Design, Methodology and Clinical Applications. Basic Clin Neurosci. 2016;7(2):143–158. doi:10.15412/J.BCN.03070208
24. Gruzelier JH. EEG-neurofeedback for optimising performance. I: a review of cognitive and affective outcome in healthy participants. Neurosci Biobehav Rev. 2014;44:124–141. doi:10.1016/j.neubiorev.2013.09.015
25. Ros T, Jb B, Lanius RA, Vuilleumier P. Tuning pathological brain oscillations with neurofeedback: a systems neuroscience framework. Front Hum Neurosci. 2014;8:1008. doi:10.3389/fnhum.2014.01008
26. Adams JA. A closed-loop theory of motor learning. J Mot Behav. 1971;3(2):111–149. doi:10.1080/00222895.1971.10734898
27. Sulzer J, Haller S, Scharnowski F, et al. Real-time fMRI neurofeedback: progress and challenges. Neuroimage. 2013;76:386–399. doi:10.1016/j.neuroimage.2013.03.033
28. Draganski B, Gaser C, Busch V, Schuierer G, Bogdahn U, May A. Neuroplasticity: changes in grey matter induced by training. Nature. 2004;427(6972):311–312. doi:10.1038/427311a
29. Hebb DO, Daly CB. The organization of behavior: a neuropsychological theory. In: A Wiley Book in Clinical Psychology. Vol. xix. Wiley; 1949:335.
30. Fazli S, Mehnert J, Steinbrink J, et al. Enhanced performance by a hybrid NIRS-EEG brain computer interface. Neuroimage. 2012;59(1):519–529. doi:10.1016/j.neuroimage.2011.07.084
31. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037//0033-295x.84.2.191
32. Disner SG, Beevers CG, Haigh EA, Beck AT. Neural mechanisms of the cognitive model of depression. Nat Rev Neurosci. 2011;12(8):467–477. doi:10.1038/nrn3027
33. Kaiser RH, Andrews-Hanna JR, Wager TD, Pizzagalli DA. Large-Scale Network Dysfunction in Major Depressive Disorder: a Meta-analysis of Resting-State Functional Connectivity. JAMA Psychiatry. 2015;72(6):603–611. doi:10.1001/jamapsychiatry.2015.0071
34. Drysdale AT, Grosenick L, Downar J, et al. Resting-state connectivity biomarkers define neurophysiological subtypes of depression. Nat Med. 2017;23(1):28–38. doi:10.1038/nm.4246
35. Mulders PC, van Eijndhoven PF, Schene AH, Beckmann CF, Tendolkar I. Resting-state functional connectivity in major depressive disorder: a review. Neurosci Biobehav Rev. 2015;56:330–344. doi:10.1016/j.neubiorev.2015.07.014
36. Sheline YI, Barch DM, Price JL, et al. The default mode network and self-referential processes in depression. Proc Natl Acad Sci U S A. 2009;106:1942–1947.
37. Drevets WC, Savitz J, Trimble M. The subgenual anterior cingulate cortex in mood disorders. CNS Spectr. 2008;13(8):663–681. doi:10.1017/s1092852900013754
38. Mayberg HS. Limbic-cortical dysregulation: a proposed model of depression. J Neuropsychiatry Clin Neurosci. 1997;9(3):471–481. doi:10.1176/jnp.9.3.471
39. Etkin A, Buchel C, Gross JJ. The neural bases of emotion regulation. Nat Rev Neurosci. 2015;16(11):693–700. doi:10.1038/nrn4044
40. Young KD, Siegle GJ, Zotev V, et al. Randomized Clinical Trial of Real-Time fMRI Amygdala Neurofeedback for Major Depressive Disorder: effects on Symptoms and Autobiographical Memory Recall. Am J Psychiatry. 2017;174(8):748–755. doi:10.1176/appi.ajp.2017.16060637
41. Zotev V, Krueger F, Phillips R, et al. Self-regulation of amygdala activation using real-time FMRI neurofeedback. PLoS One. 2011;6(9):e24522. doi:10.1371/journal.pone.0024522
42. Zotev V, Yuan H, Misaki M, et al. Correlation between amygdala BOLD activity and frontal EEG asymmetry during real-time fMRI neurofeedback training in patients with depression. Neuroimage Clin. 2016;11:224–238. doi:10.1016/j.nicl.2016.02.003
43. Ochsner KN, Gross JJ. The cognitive control of emotion. Trends Cognit Sci. 2005;9(5):242–249. doi:10.1016/j.tics.2005.03.010
44. Etkin A, Egner T, Kalisch R. Emotional processing in anterior cingulate and medial prefrontal cortex. Trends Cognit Sci. 2011;15(2):85–93. doi:10.1016/j.tics.2010.11.004
45. Arnsten AF. Stress signalling pathways that impair prefrontal cortex structure and function. Nat Rev Neurosci. 2009;10(6):410–422. doi:10.1038/nrn2648
46. Coan JA, Allen JJ. Frontal EEG asymmetry as a moderator and mediator of emotion. Biol Psychol. 2004;67(1–2):7–49. doi:10.1016/j.biopsycho.2004.03.002
47. Olbrich S, Arns M. EEG biomarkers in major depressive disorder: discriminative power and prediction of treatment response. Int Rev Psychiatry. 2013;25(5):604–618. doi:10.3109/09540261.2013.816269
48. Davidson RJ. Anterior cerebral asymmetry and the nature of emotion. Brain Cogn. 1992;20(1):125–151. doi:10.1016/0278-2626(92)90065-t
49. Mennella R, Patron E, Palomba D. Frontal alpha asymmetry neurofeedback for the reduction of negative affect and anxiety. Behav Res Ther. 2017;92:32–40. doi:10.1016/j.brat.2017.02.002
50. Quaedflieg CW, Smulders FT, Meyer T, Peeters F, Merckelbach H, Smeets T. The validity of individual frontal alpha asymmetry EEG neurofeedback. Soc Cogn Affect Neurosci. 2016;11:33–43.
51. Peeters F, Oehlen M, Ronner J, van Os J, Lousberg R. Neurofeedback as a treatment for major depressive disorder--a pilot study. PLoS One. 2014;9:e91837. doi:10.1371/journal.pone.0091837
52. Wang SY, Lin IM, Fan SY, et al. The effects of alpha asymmetry and high-beta down-training neurofeedback for patients with the major depressive disorder and anxiety symptoms. J Affect Disord. 2019;257:287–296. doi:10.1016/j.jad.2019.07.026
53. Trambaiolli LR, Kohl SH, Linden DEJ, Mehler DMA. Neurofeedback training in major depressive disorder: a systematic review of clinical efficacy, study quality and reporting practices. Neurosci Biobehav Rev. 2021;125:33–56. doi:10.1016/j.neubiorev.2021.02.015
54. Fernandez-Alvarez J, Grassi M, Colombo D, et al. Efficacy of bio- and neurofeedback for depression: a meta-analysis. Psychol Med. 2022;52(2):201–216. doi:10.1017/S0033291721004396
55. Roy Y, Banville H, Albuquerque I, Gramfort A, Falk TH, Faubert J. Deep learning-based electroencephalography analysis: a systematic review. J Neural Eng. 2019;16(5):051001. doi:10.1088/1741-2552/ab260c
56. Vidaurre C, Blankertz B. Towards a cure for BCI illiteracy. Brain Topogr. 2010;23(2):194–198. doi:10.1007/s10548-009-0121-6
57. Scangos KW, Khambhati AN, Daly PM, et al. Closed-loop neuromodulation in an individual with treatment-resistant depression. Nat Med. 2021;27(10):1696–1700. doi:10.1038/s41591-021-01480-w
58. Lozano AM, Lipsman N, Bergman H, et al. Deep brain stimulation: current challenges and future directions. Nat Rev Neurol. 2019;15(3):148–160. doi:10.1038/s41582-018-0128-2
59. Insel TR. The NIMH Research Domain Criteria (RDoC) Project: precision medicine for psychiatry. Am J Psychiatry. 2014;171(4):395–397. doi:10.1176/appi.ajp.2014.14020138
60. Misaki M, Tsuchiyagaito A, Guinjoan SM, Rohan ML, Paulus MP. Whole-brain mechanism of neurofeedback therapy: predictive modeling of neurofeedback outcomes on repetitive negative thinking in depression. Transl Psychiatry. 2024;14(1):354. doi:10.1038/s41398-024-03066-9
61. Khaleghi A, Samiei H, Zarafshan H, Baloochi SA, Mohammadi MR. Effectiveness of fMRI-based Neurofeedback Therapy on Depression: a Systematic Review. Clin Psychopharmacol Neurosci. 2025;23(3):337–355. doi:10.9758/cpn.25.1295
62. Dobbins ICS, Bastos M, Ratis RC, Silva W, Bonini JS. Effects of neurofeedback on major depressive disorder: a systematic review. Einstein. 2023;21:eRW0253. doi:10.31744/einstein_journal/2023RW0253
63. Mehler DMA, Sokunbi MO, Habes I, et al. Targeting the affective brain-a randomized controlled trial of real-time fMRI neurofeedback in patients with depression. Neuropsychopharmacology. 2018;43(13):2578–2585. doi:10.1038/s41386-018-0126-5
64. Mathiak K, Keller M. Clinical Application of Real-Time fMRI-Based Neurofeedback for Depression. Adv Exp Med Biol. 2021;1305:275–293. doi:10.1007/978-981-33-6044-0_15
65. Zahn R, Weingartner JH, Basilio R, et al. Blame-rebalance fMRI neurofeedback in major depressive disorder: a randomised proof-of-concept trial. Neuroimage Clin. 2019;24:101992. doi:10.1016/j.nicl.2019.101992
66. Tsuchiyagaito A, Misaki M, Kirlic N, et al. Real-Time fMRI Functional Connectivity Neurofeedback Reducing Repetitive Negative Thinking in Depression: a Double-Blind, Randomized, Sham-Controlled Proof-of-Concept Trial. Psychother Psychosom. 2023;92(2):87–100. doi:10.1159/000528377
67. Mel’nikov MY, Bezmaternykh DD, Savelov AA, et al. Real-time fMRI neurofeedback compared to cognitive behavioral therapy in a pilot study for the treatment of mild and moderate depression. Eur Arch Psychiatry Clin Neurosci. 2023;273:1139–1149.
68. Bloom PA, Pagliaccio D, Zhang J, et al. Mindfulness-based real-time fMRI neurofeedback: a randomized controlled trial to optimize dosing for depressed adolescents. BMC Psychiatry. 2023;23(1):757. doi:10.1186/s12888-023-05223-8
69. Lee YJ, Lee GW, Seo WS, Koo BH, Kim HG, Cheon EJ. Neurofeedback Treatment on Depressive Symptoms and Functional Recovery in Treatment-Resistant Patients with Major Depressive Disorder: an Open-Label Pilot Study. J Korean Med Sci. 2019;34(42):e287. doi:10.3346/jkms.2019.34.e287
70. Patil AU, Lin C, Lee SH, et al. Review of EEG-based neurofeedback as a therapeutic intervention to treat depression. Psychiatry Res Neuroimaging. 2023;329:111591. doi:10.1016/j.pscychresns.2023.111591
71. Voigt JD, Mosier M, Tendler A. Systematic review and meta-analysis of neurofeedback and its effect on posttraumatic stress disorder. Front Psychiatry. 2024;15:1323485. doi:10.3389/fpsyt.2024.1323485
72. von Altdorf L, Bracewell M, Cooke A. Effectiveness of Electroencephalographic Neurofeedback for Parkinson’s Disease: a Systematic Review and Meta-Analysis. J Clin Med. 2025;14(19):6929. doi:10.3390/jcm14196929
73. Herold F, Wiegel P, Scholkmann F, Muller NG. Applications of Functional Near-Infrared Spectroscopy (fNIRS) Neuroimaging in Exercise(-)Cognition Science: a Systematic, Methodology-Focused Review. J Clin Med. 2018;7:466.
74. Herold F, Gronwald T, Scholkmann F, et al. New Directions in Exercise Prescription: is There a Role for Brain-Derived Parameters Obtained by Functional Near-Infrared Spectroscopy? Brain Sci. 2020;10(6):342. doi:10.3390/brainsci10060342
75. Scholkmann F, Kleiser S, Metz AJ, et al. A review on continuous wave functional near-infrared spectroscopy and imaging instrumentation and methodology. Neuroimage. 2014;85(1):6–27. doi:10.1016/j.neuroimage.2013.05.004
76. Vitorio R, Stuart S, Rochester L, Alcock L, Pantall A. fNIRS response during walking - Artefact or cortical activity? A systematic review. Neurosci Biobehav Rev. 2017;83:160–172. doi:10.1016/j.neubiorev.2017.10.002
77. Niso G, Romero E, Moreau JT, Araujo A, Krol LR. Wireless EEG: a survey of systems and studies. Neuroimage. 2023;269:119774. doi:10.1016/j.neuroimage.2022.119774
78. Wei TY, Chang DW, Liu YD, et al. Portable wireless neurofeedback system of EEG alpha rhythm enhances memory. Biomed Eng Online. 2017;16(1):128. doi:10.1186/s12938-017-0418-8
79. Kleinloog JPD, Mensink RP, Ivanov D, Adam JJ, Uludag K, Joris PJ. Aerobic Exercise Training Improves Cerebral Blood Flow and Executive Function: a Randomized, Controlled Cross-Over Trial in Sedentary Older Men. Front Aging Neurosci. 2019;11:333. doi:10.3389/fnagi.2019.00333
80. Won J, Callow DD, Pena GS, et al. Evidence for exercise-related plasticity in functional and structural neural network connectivity. Neurosci Biobehav Rev. 2021;131:923–940. doi:10.1016/j.neubiorev.2021.10.013
81. Bassett DS, Sporns O. Network neuroscience. Nat Neurosci. 2017;20(3):353–364. doi:10.1038/nn.4502
82. Deco G, Jirsa VK, McIntosh AR. Emerging concepts for the dynamical organization of resting-state activity in the brain. Nat Rev Neurosci. 2011;12(1):43–56. doi:10.1038/nrn2961
83. Schmoigl-Tonis M, Schranz C, Muller-Putz GR. Methods for motion artifact reduction in online brain-computer interface experiments: a systematic review. Front Hum Neurosci. 2023;17:1251690. doi:10.3389/fnhum.2023.1251690
84. Zhai L, Zhao M, Zhang J, Jamil M, Naz R, Li C. A systematic review of EEG-based biomarkers for depression, anxiety, and bipolar disorder: trends in explainable artificial intelligence (XAI). BMC Psychiatry. 2025;26(1):90. doi:10.1186/s12888-025-07589-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sodium-Glucose Cotransporter-2 Inhibitors in Mood Disorders: A Narrative Review of Mechanisms, Evidence, and Challenges
Guo X, Yang T, Fang Y, Chen J
Neuropsychiatric Disease and Treatment 2026, 22:599108
Published Date: 8 April 2026