Back to Journals » Cancer Management and Research » Volume 17

Advances in PSMA-Targeted Radionuclide Therapy for Metastatic Castration-Resistant Prostate Cancer
Authors Wang J, Yuan H, Xu J, Yang C
Received 4 May 2025
Accepted for publication 11 August 2025
Published 1 September 2025 Volume 2025:17 Pages 1859—1869
DOI https://doi.org/10.2147/CMAR.S538367
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Yong Teng
Jie Wang, Hui Yuan, Jianan Xu, Chongyi Yang
Department of Urology, Ninghai First Hospital, Zhejiang, People’s Republic of China
Correspondence: Chongyi Yang, Email [email protected]
Abstract: Prostate cancer (PCa) is the most common tumor for men in the genital system. Despite several new therapies approved in the past decades, 34,700 patients die on a regular basis in 2023 in America. Recently radioisotopic therapies have shown the delightful results in the PCa treatment, which made FDA approved lutetium-177 for adult patients with prostate-specific membrane antigen (PSMA)-positive metastatic castrate-resistant prostate cancer (mCRPC). Many other clinical trials are also in progress in various settings. Both monotherapy and combination studies are underway. However, because of several limitations existed in these clinical trials and alarmed long-term nephrotoxicity of PSMA-targeted therapy, we should be more prudent to this therapy. In this review, we evaluates the evolving clinical and preclinical landscape of PSMA-targeted therapy, as well as the potential biomarkers for evaluating the therapeutic response.
Keywords: prostate cancer, prostate-specific membrane antigen, radioligand therapy, lutetium-177, actinium-225
Introduction
Prostate cancer (PCa), a solid malignant tumor originating from the prostate epithelium, is the most common tumor affecting the male genitourinary system and represents a significant public health concern. In 2020, approximately 1.4 million new cases of PCa were diagnosed worldwide, including 288,300 new cases and 34,700 related deaths in the United States in 2023.1,2 Despite numerous advances in the treatment of PCa, a substantial number of patients present with locally advanced or metastatic disease, contributing to ongoing mortality. There remains a critical need for novel, individualized, and effective targeted therapies to address the unmet medical needs of this population.
Although the exact function of prostate-specific membrane antigen (PSMA) in PCa is not fully understood, it is markedly overexpressed in PCa tissues compared to normal tissues.3 Notably, elevated PSMA expression is associated with increased prostate-specific antigen (PSA) levels, higher Gleason scores, and poorly differentiated, metastatic, and castration-resistant PCa, suggesting a potential role for PSMA in the differentiation and progression of metastatic castration-resistant prostate cancer (mCRPC).3–6 PSMA has the ability to internalize bound molecules, making it a potential target for both diagnostic imaging and targeted therapeutic strategies.7 The FDA approved 68Ga-PSMA-11 for staging and restaging of PCa in December 2020 and Lutetium-177 (177Lu)-PSMA-617 for the treatment of adult patients with PSMA-positive mCRPC in March 2022. Numerous other PSMA-targeting molecules and antibodies are currently being investigated in preclinical and clinical studies. In this review, we summarize current research on PSMA and its applications in iatreusiology.
Current Clinical Experience with PSMA-Targeted RLT
β-Emitting Radionuclides
The β particle is an electron emitted from the nucleus of a decaying radioactive atom.8 DNA damage caused by β particles is dose-dependent; at low doses, the damage may be sublethal. However, owing to the relatively long range over which β particles deposit their energy, reactive oxygen species (ROS) produced from cytotoxic damage in adjacent non-tumor cells can also contribute to DNA damage.9,10 Among the various β particles investigated for PCa targeted therapy, 177Lu, Iodine-131, and Terbium-161 have shown potential.11–16
Among all β-emitting radioisotopes, 177Lu is the most commonly used in PCa treatment.7,17 In 2015, 10 patients with metastatic castration-resistant prostate cancer (mCRPC) received one cycle of 177Lu-PSMA-617.18 Following an eight-month follow-up, seven patients (70%) showed a decline in PSA levels, including six and five patients who experienced PSA reductions of ≥30% and ≥50%, respectively. Subsequent studies have confirmed the therapeutic benefits of 177Lu-PSMA-617 in mCPRC.19–21 In a meta-analysis of 1,338 patients, 44% of those treated with 177Lu-PSMA radioligand therapy (RLT) had a ≥50% decline in PSA, compared with 22% of patients treated with enzalutamide or cabazitaxel (p = 0.0002).21 Another meta-analysis involving 3,958 patients across seven randomized controlled trials (RCTs) showed that 177Lu-PSMA-617 treatment resulted in a 1.3-fold higher rate of ≥50% PSA decline compared to treatment with abiraterone, enzalutamide, mitoxantrone, or cabazitaxel (p < 0.001).20 Despite these positive outcomes, several concerns remain. Most studies used PSA decline as the primary outcome rather than overall survival. Given that many enrolled patients had limited life expectancy, it is notable that only a few studies reported survival data. Subsequently, two large RCTs (VISON and TheraP trials) reported outcomes for 177Lu-PSMA-617 in mCPRC treatment (Table 1). The VISON trial, an open-label Phase III trial, enrolled 581 patients in the treatment arm who had progressed after at least one androgen receptor pathway inhibitor and one or two taxane regimens. Patients treated with 177Lu-PSMA-617 plus standard care had longer median imaging-based progression-free survival (PFS) (8.7 vs 3.4 months, p < 0.001) and overall survival (15.3 vs 11.3 months, p < 0.001) than those receiving standard care.22 These results were consistent with findings from a recent real-world study, which reported a median overall survival and PFS of 13.5 and 8.2 months, respectively, in mCRPC patients treated with 177Lu-PSMA-617.23 The TheraP trial, an open-label Phase II trial, enrolled 200 patients with mCPRC for whom cabazitaxel was considered the next appropriate standard treatment. In this trial, patients treated with 177Lu-PSMA-617 showed a higher PSA response rate than those receiving cabazitaxel.24 177Lu-PSMA RLT was well-tolerated, with no acute or subacute nephrotoxicity observed, even in patients with chronic renal failure, a single functioning kidney, or those who underwent 5–6 treatment cycles.25–28 Only a small number of patients experienced grade 3/4 hematological toxicity, and no treatment-related deaths occurred.19,22,24,29,30 Hematological toxicity was typically transient and self-limiting, involving decreases in hemoglobin, neutrophil, and platelet levels. Grade 1/2 non-hematological events included xerostomia, nausea, vomiting, and bone pain.24,30 Based on these findings, agencies such as the Food and Drug Administration (FDA) and European Medicines Agency (EMA) have approved 177Lu-PSMA-617 as a third-line treatment for patients with mCRPC. However, the rigor of these RCTs has been questioned. In the VISON trial, three-quarters of patients in the control arm had previously received enzalutamide, a group unlikely to benefit from abiraterone—resulting in a suboptimal control group. Additionally, an updated analysis of the TheraP trial showed no significant difference in overall survival between the 177Lu-PSMA-617 and cabazitaxel arms (19.1 vs 19.6 months).31 Concerns about long-term nephrotoxicity associated with 177Lu-PSMA-617 have also emerged. A recent retrospective study reported that 45% (48/106) of patients receiving four or more cycles of 177Lu-PSMA RLT experienced moderate decreases in estimated glomerular filtration rate (eGFR) one year after initiating treatment, and 24% (25/106) experienced severe eGFR decline.32
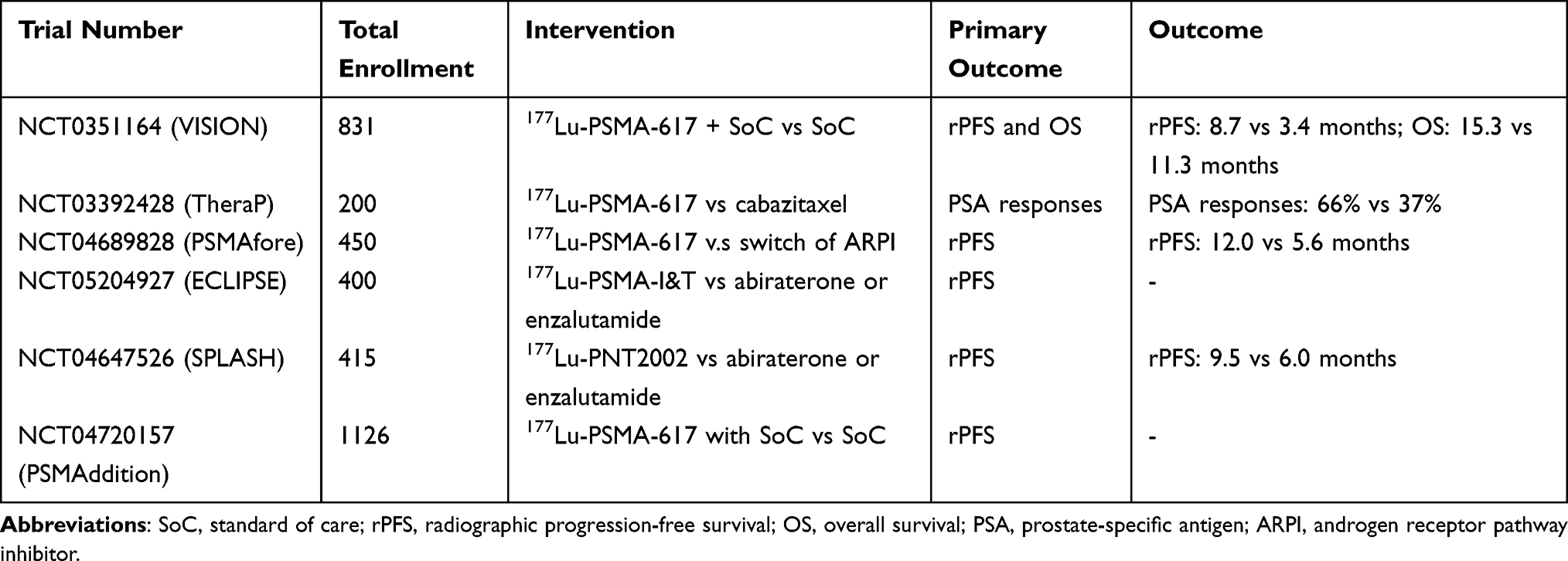 |
Table 1 Current Active or Recruiting Phase III Prostate Cancer Trials Involving 177Lu-PSMA RLT |
Several clinical trials have shown that earlier use of PSMA-targeted RLT in the mCRPC treatment yields better responses than when used after multiple prior treatments. Banda et al reported that 83% (15/18) of patients with metastatic hormone-sensitive prostate cancer (mHSPC) achieved a ≥50% PSA response following 177Lu-PSMA-617 therapy.33 However, it remains unclear whether PSMA-targeted RLT offers superior efficacy compared to currently approved first- or second-line agents. A clinical trial (PSMAfore, NCT04689828) is ongoing to evaluate whether 177Lu-PSMA-617 improves radiographic PFS compared with a change in androgen deprivation therapy (ADT) in patients with mCRPC previously treated with an alternate ADT and not exposed to a taxane-containing regimen in the CRPC or mHSPC setting.34 Preliminary results from the PSMAfore trial indicated a longer median radiographic PFS in the 177Lu-PSMA-617 arm compared with the ADT-switch group (12.0 vs 5.6 months, p < 0.05). However, similar concerns apply: patients in the control arm who had already received enzalutamide were unlikely to respond favorably.
The urea-based small molecule PSMA I&T is another frequently used RLT agent. Recent studies have found no significant differences in survival outcomes between PSMA I&T and PSMA-617.35–37 Whole-body and lacrimal gland absorbed doses were higher with 177Lu-PSMA-617 than with 177Lu-PSMA I&T, while renal absorbed doses were lower in patients treated with 177Lu-PSMA-617.38 Schäfer et al recently reported that three patients who underwent 8–10 cycles of 177Lu-PSMA I&T developed radiation-induced nephropathy.39 Therefore, the potential nephrotoxicity of 177Lu-PSMA I&T must be carefully considered during treatment.
α-Emitting Radionuclides
The α particle—a 4He nucleus consisting of two neutrons and two protons—releases all its energy over a very short distance, resulting in higher efficiency against cancer cells and reduced toxicity to surrounding tissues compared with β particles.40,41 Therefore, targeted α therapy is a promising alternative to β therapy, as it induces lethal DNA double-strand breaks with high efficacy.42 Unlike β particles, which may cause sublethal damage and depend on ROS produced by adjacent non-tumor cells, α particles kill cancer cells independently of oxygenation status or cell cycle phase, leading to enhanced therapeutic effectiveness.43,44
Actinium-225 (225Ac) decays, through a series of daughter radionuclides, to Francium-221, Astatine-217, Bismuth-213 (213Bi), and finally Bismuth-209, with a half-life of 10 days.45,46 Owing to the nephrotoxicity associated with 213Bi, 225Ac was previously limited in its clinical application for targeted α therapy.47,48 However, since the development of stable chelators such as 225Ac-PSMA-617 and 225Ac-PSMA-I&T, 225Ac has significantly improved its potential for treating mCRPC.49–51 These chelators facilitate rapid tumor uptake and efficient clearance of unbound conjugates from circulation, thereby reducing hematologic toxicity and nephrotoxicity. Furthermore, owing to its limited tissue penetration, 225Ac causes minimal hematologic toxicity, even in patients with bone marrow infiltration.
In 2016, Kratochwil et al reported the first clinical use of 225Ac-PSMA-617 in two patients, one who could not receive β-emitters owing to diffuse bone marrow involvement and another who was resistant to 177Lu-PSMA-617. Both patients exhibited PSA levels below 0.1 ng/mL, with minimal hematological toxicity except for dose-dependent xerostomia.52 Since then, several studies have demonstrated the promising antitumor effects of 225Ac-PSMA-617.53–57 In a retrospective study involving 73 patients with mCPRC who had exhausted standard therapies with 225Ac-PSMA-617,57 82% demonstrated a PSA response, with 70% achieving a 50% PSA decline. Xerostomia was the most common adverse event but was generally manageable and not severe enough to warrant treatment discontinuation. However, five cases of grade 3/4 renal failure have been reported. A meta-analysis of nine studies involving 263 patients demonstrated that 60.99% (95% confidence interval [CI], 54.92–66.83%) experienced a ≥50% PSA decline, with a mean PFS and mean overall survival of 9.15 and 11.77 months, respectively.58 A multicenter retrospective study (WARMTH Act) involving 488 patients further confirmed the efficacy of 225Ac-PSMA RLT,58 with a mean overall survival of 15.5 months and a mean PFS of 7.9 months.59 However, notable toxicities included grade 3/4 anemia (13%), leukopenia (4%), thrombocytopenia (7%), and renal toxicity (5%). Another stable chelator, 225Ac-PSMA-I&T has shown an efficacy comparable to 225Ac-PSMA-617 in a recent retrospective analysis.60
Generally, 225Ac-PSMA-617 is used as a salvage therapy for end-stage mCRPC or to overcome resistance to β-emitting radionuclides. Recent studies have explored its potential earlier in the treatment paradigm. In one study, 53 patients with mCRPC were treated with 225Ac-PSMA-617 immediately following ADT, and 91% exhibited a ≥50% PSA reduction.61 Notably, after a median follow-up of 55 months, overall survival had not yet been reached in patients with a ≥50% PSA reduction, suggesting that 225Ac-PSMA-617 may serve as an alternative to standard therapies such as enzalutamide or abiraterone post-ADT. Another retrospective study revealed that among 21 patients with mHSPC, 95% had a PSA response and 86% achieved a ≥50% PSA decline.62 225Ac-PSMA-617 is not a substitute for ADT; however, its encouraging disease control rates suggest potential synergy when used in combination with ADT in HSPC. However, toxicity remains a major limitation in its routine clinical use. Xerostomia is currently the most common dose-limiting side effect for PSMA-targeted RLT. Salivary gland toxicity appears more frequent and severe following 225Ac-PSMA treatment. In a retrospective study involving 26 patients with mCPRC previously treated with 177Lu-PSMA, all developed grade 1/2 xerostomia, with six discontinuing therapy due to the severity.55 Another study reported grade 1/2 xerostomia in 94% of patients following 225Ac-PSMA-617 therapy.62 Previous studies indicate that the antitumor efficacy of RLT increases with higher radiation doses;63,64 thus, severe toxicity may limit therapeutic intensification and reduce overall response. Currently, no RCT has documented that the benefits of 225Ac-PSMA outweigh its adverse effects.
Other α-targeted therapies have also been studied. 213Bi-PSMA-617 has been administered to patients with progressive mCPRC despite conventional therapy; however, its clinical utility is limited by the short half-life of 213Bi.65 Thorium-227 (227Th), with a more suitable half-life for targeted α therapy, has shown promising preclinical results with the PSMA-targeted conjugate PSMA-TTC.66,67 223Ra, another α-emitting radioisotope with a half-life of 11.4 days, emits 93.5% of its decay energy as α particles and eventually decays to stable lead-207 (207Pb). However, its clinical application is restricted to patients with PCa and osteoblastic metastases owing to its affinity for bone tissue.68
Combination Therapy
Androgen Receptor Pathway Inhibitors
Although 177Lu-PSMA RLT has demonstrated positive outcomes in mCPRC treatment, an increasing number of studies suggest that 177Lu-PSMA RLT is not limited to third-line therapy. Several clinical trials are currently underway, evaluating PSMA-targeted RLT at various stages of PCa and in earlier lines of therapy. In an observational study comparing the efficacy of combined 177Lu-PSMA-617 and abiraterone acetate versus 177Lu-PSMA-617 monotherapy in patients with mCRPC, the combination group exhibited significant improvements in symptomatic response, PFS, and overall survival.69 In a real-world study, patients receiving 177Lu-PSMA-617 in combination with androgen receptor pathway inhibitors had a longer overall survival compared to those receiving 177Lu-PSMA-617 alone; however, the difference was not statistically significant (18.2 vs 12.3 months, p = 0.265).23
Docetaxel/Cabazitaxel
In a prospective study comparing the efficacy of 177Lu-PSMA-617 and docetaxel in chemotherapy-naïve patients with mCRPC, 60% (9/15) of those receiving 177Lu-PSMA-617 experienced a ≥50% PSA decline, while 40% (8/20) of patients treated with docetaxel showed a similar PSA response.70 Moreover, 177Lu-PSMA RLT demonstrated good tolerability. Grade 3/4 adverse events were less frequent in the 177Lu-PSMA-617 group than in the docetaxel group, suggesting the potential of 177Lu-PSMA-617 for use earlier in the disease course, rather than reserving it solely for advanced-stage treatment. An RCT (UpFrontPSMA, NCT04343885) is currently evaluating the efficacy of sequential treatment with 177Lu-PSMA-617 followed by docetaxel versus docetaxel monotherapy in patients with metastatic hormone-naïve PCa.71
A prospective, single-arm clinical trial (LuCAB, NCT05340374) is also ongoing to determine the maximum tolerated dose, dose-limiting toxicities, and recommended phase II dose of cabazitaxel in combination with 177Lu-PSMA-617 in patients with mCRPC.72
Olaparib
A Phase I open-label clinical trial (LuPARP, NCT03874884) is underway to evaluate the safety and tolerability of combining olaparib with 177Lu-PSMA-617 in patients with mCRPC.73
Immunotherapy
A phase Ib trial (NCT03805594) is ongoing to evaluate the objective response of pembrolizumab in combination with 177Lu-PSMA-617 in patients with mCRPC.74 Similarly, a phase I/II trial (PRINCE, NCT03658447) is investigating the safety and tolerability of pembrolizumab administered every 3 weeks alongside 177Lu-PSMA-617 every 6 weeks for up to six cycles, beginning at 8.5 GBq with 0.5 GBq dose reduction per cycle.75
A phase II study (EVOLUTION, NCT05150236) was conducted to evaluate the activity and safety of 177Lu-PSMA-617 alone and in combination with ipilimumab and nivolumab in patients with mCRPC.76
Radium-223
A single-arm phase I/II trial (AlphaBet, NCT05383079) enrolled 36 patients to determine the maximum tolerated dose of 223Ra in combination with 177Lu-PSMA I&T.77
Radiosensitizer
The combination of 177Lu-PSMA-617 with radiosensitizers has demonstrated enhanced survival benefit.78,79 Among patients with mCRPC, 86% of those treated with 177Lu-PSMA-617 and Idronoxil (NOX66) experienced a PSA reduction, while 61% achieved a maximum PSA decline of ≥50%.80
β-Emitting and α-Emitting Radionuclides
Despite promising outcomes with targeted α and β therapies, a notable proportion (approximately 30%) of patients either do not respond to PSMA-targeted RLT or develop early resistance.81,82 Furthermore, many patients cannot tolerate the associated adverse effects, with xerostomia currently being the most common dose-limiting side effect. Combination therapies employing β-emitting radionuclides have been proposed to minimize toxicity and overcome drug resistance. In a study involving 20 patients with mCRPC who showed no improvement with 177Lu-PSMA monotherapy, a combination of low-activity 225Ac-PSMA-617 and full-activity 177Lu-PSMA-617 was administered. Of these patients, 65% exhibited a maximum PSA decline of ≥50%, with a median PFS of 19 weeks and overall survival of 48 weeks.83 Additionally, 17 patients who had progressed after 177Lu-PSMA-617 monotherapy received one cycle of tandem therapy with 225Ac-PSMA-617 and 177Lu-PSMA-617; 71% of these patients demonstrated partial remission or stable disease.78
Characteristics Predicting Biochemical Response Following PSMA-Targeted RLT
A growing body of evidence suggests that RLT is not limited to advanced, end-stage diseases. Both 225Ac-PSMA-617 and 177Lu-PSMA-617 have been investigated in patients with mHSPC, as well as in combination with other therapies such as abiraterone acetate.62,69 However, a considerable number of patients still fail to respond to RLT.59,79 Therefore, understanding the limitations and resistance mechanisms to RLT remains a critical challenge. While several promising studies have identified potential biomarkers and predictive characteristics, there remains an unmet need for optimal patient selection.
PSA remains the most prevalent biomarker to predict PCa recurrence and therapeutic response. A decline in PSA levels following RLT is generally considered an effective marker of response;17,84–88 however, no consensus exists regarding the degree of PSA decline necessary to serve as a reliable prognostic marker. Most studies suggest that any PSA decline after the first RLT cycle is associated with prolonged overall survival.84–86 A recent meta-analysis reported a pooled hazard ratio of 0.29 (0.18–0.46) for overall survival among patients with any PSA decline, and 0.67 (0.43–1.07) for those with >50% PSA decline.86 Some studies have indicated that a PSA decline of ≥50% after the first RLT cycle is a strong predictor of prolonged overall survival.17 Assessing PSA changes six weeks after RLT initiation has also been proposed as an early predictor of long-term clinical outcomes. A PSA reduction of ≥30% at six weeks has been linked to a longer overall survival of 16.7 months, compared with 11.8 months in patients with stable PSA and 6.5 months in those with PSA progression.89 However, this correlation has not been consistently observed.90 For instance, Ahmadzadehfar et al reported that PSA declines of >50% or <50% after the first cycle did not significantly impact median overall survival, which was 14.3 and 13.9 months, respectively.7 Furthermore, a considerable proportion of patients (30–50%) who exhibited no PSA decline after the first cycle went on to show decreased PSA levels after the second or third cycle. This suggests that relying solely on PSA response after the first RLT cycle may exclude patients who ultimately derive significant long-term benefit. Variability in therapeutic dosages, patient characteristics, and the timing of PSA assessments contributes to heterogeneity across studies.
Ahmadzadehfar et al also reported that prior chemotherapy was a significant predictor of reduced overall survival, based on both univariate and multivariate analyses.7 The median overall survival was 10.9 months in patients who had received one round of chemotherapy with docetaxel and 8.9 months in those treated sequentially with docetaxel and cabazitaxel—both notably shorter than in patients without prior chemotherapy.7 Another retrospective study involving 167 patients with mCRPC revealed that prior taxane chemotherapy was associated with worse overall survival.91 However, the association was not significant in multivariate analysis, suggesting that poor baseline characteristics post-chemotherapy may influence prognosis. Another study verified that treatment with docetaxel or cabazitaxel did not affect survival or response rates to RLT.87 Similarly, prior treatment with abiraterone, corticosteroids, or radiotherapy was not a predictor of PFS or overall survival in patients undergoing RLT.87,92
Other factors, such as bone metastases, elevated lactate dehydrogenase, and alkaline phosphatase levels, have also been proposed as biomarkers for predicting RLT efficacy;91,93,94 however, their predictive value remains controversial. Furthermore, most of these biomarkers are only measurable after treatment has already commenced, requiring patients to undergo expensive therapy prior to evaluation. Given the need for individualized treatment approaches, the identification of novel predictive biomarkers is urgently needed.
Advancements in whole-exome sequencing have led to the identification of numerous candidate biomarkers at the genomic, transcriptomic, proteomic, and metabolomic levels for evaluating RTL response. A 2021 study involving nine patients with mCRPC verified that PSMA protein expression in biopsy-confirmed metastatic lesions was an unreliable predictor of response to 177Lu-PSMA-617.95 Similarly, a retrospective analysis of 19 patients showed no correlation between PSMA expression and response to 177Lu-PSMA-617.96 However, the full-length androgen receptor and its splice variant AR-V7 were identified as prognostic biomarkers for predicting response to 177Lu-PSMA-617.96 Genomic instability, primarily associated with defects in DNA repair pathways, suggests that DNA damage-repair (DDR) mutations may serve as potential indicators of RLT response. Studies have shown that patients who are resistant to RLT despite PSMA positivity often carry DDR or checkpoint gene alterations.97 Conversely, other research suggests that patients harboring DDR defects may experience longer overall survival following 225Ac-PSMA-617 treatment compared to those without such mutations. Additionally, decreased DDR gene expression, such as 53BP1 and γ-H2AX, has been associated with progressive PCa.98
Discussion
Despite the demonstrated efficacy of PSMA-targeted RLT as a therapeutic option for patients with mCRPC, several challenges must be addressed before it can be widely adopted in clinical practice. Although α-emitting radionuclides exhibit superior cytotoxicity toward cancer cells and reduced toxicity to surrounding tissues compared to β particles, issues such as the variable chemistry of daughter radionuclides and the recoil effect must be carefully considered.99 Toxicity remains a major limiting factor in the routine clinical use of α-emitting radionuclides. Many patients experience significant side effects from 225Ac-PSMA-617 treatment. While tandem treatments have been proposed to minimize toxicity, only a limited number of cases have been reported. The mechanism by which PSMA-targeted radioligands accumulate in the salivary glands is not yet fully understood. This accumulation does not appear to result primarily from PSMA-mediated uptake, thereby limiting available interventions for alleviating xerostomia.100 Another major concern involves long-term side effects, including respiratory, hepatic, and renal failure, as well as the potential development of secondary malignancies and genetic disorders due to unintended radiation exposure to healthy tissues.101 Data on the nephrotoxicity of 177Lu-PSMA-617 remain inconclusive, underscoring the need for caution when considering PSMA-targeted RLT in patients with early-stage mCRPC or HSPC. Discrepancies between preclinical and clinical studies also present significant barriers to broader RLT application. Differences in molecular expression patterns between human subjects and animal models can skew estimations of efficacy and toxicity.102,103 For instance, PSMA-targeted radioligand accumulation in human salivary glands is notably higher than in mice and is often negligible in preclinical models, potentially leading to underestimation of toxicity risks in human applications.89,104 Moreover, only those PSMA-targeted radioligands deemed optimal and safe in preclinical evaluations have progressed to clinical testing. This selective advancement may inadvertently exclude novel radioligands with promising clinical potential owing to incomplete preclinical assessments. In many RCTs, including VISON, TheraP, PSMAfore, UpFrontPSMA, PSMAddition, ANZUP2001, LuCAB, LuPARP, and AlphaBet, patients received a homogeneous dose and number of cycles: 7.4 GBq of 177Lu-PSMA-617 or 177Lu-PSMA I&T on Day 1 of every six-week cycle, for up to six cycles. However, the optimal dose and administration schedule of these agents remain undetermined. It also remains unclear whether PSMA RLT is superior to currently approved first- or second-line therapies. Furthermore, there are no validated biomarkers to predict RLT response, and the limited production capacity of 225Ac-PSMA has further constrained its clinical development.
To overcome these challenges, efforts must focus on reducing treatment-related side effects. One promising strategy is the development of novel radioligands and chelators that improve tumor uptake of targeting moieties while minimizing radiation exposure to healthy tissues. Several clinical trials are currently investigating the stability, efficacy, and toxicity of these ligands.105–107 Other strategies include combination therapies and the use of salivary gland protectors to reduce toxicity;82,108 however, further research is necessary to confirm the toxicity endpoints associated with these approaches and to evaluate the balance between therapeutic effectiveness and toxicity. Simultaneously, future studies should aim to elucidate the genotypic and phenotypic characteristics of patients, as well as their tumor immune microenvironments, to enable rational design of combination therapies that yield optimal clinical outcomes. Finally, innovative methods to increase the production of radioligands must be investigated to meet the growing demand.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Siegel RL, Miller KD, Wagle NS, et al. Cancer stat, 2023. CA Cancer J Clin. 2023;73:17–48. doi:10.3322/caac.21763
2. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249.
3. Kasperzyk JL, Finn SP, Flavin R, et al. Prostate-specific membrane antigen protein expression in tumor tissue and risk of lethal prostate cancer. Cancer Epidemiol Biomarkers Prev. 2013;22(12):2354–2363. doi:10.1158/1055-9965.EPI-13-0668
4. Queisser A, Hagedorn SA, Braun M, et al. Comparison of different prostatic markers in lymph node and distant metastases of prostate cancer. Mod Pathol. 2015;28(1):138–145. doi:10.1038/modpathol.2014.77
5. Derlin T, Riethdorf S, Schumacher U, et al. PSMA-heterogeneity in metastatic castration-resistant prostate cancer: circulating tumor cells, metastatic tumor burden, and response to targeted radioligand therapy. Prostate. 2023;83(11):1076–1088. doi:10.1002/pros.24549
6. Bravaccini S, Puccetti M, Bocchini M, et al. PSMA expression: a potential ally for the pathologist in prostate cancer diagnosis. Sci Rep. 2018;8(1):4254. doi:10.1038/s41598-018-22594-1
7. Ahmadzadehfar H, Rahbar K, Baum RP, et al. Prior therapies as prognostic factors of overall survival in metastatic castration-resistant prostate cancer patients treated with [(177)Lu]Lu-PSMA-617. A WARMTH multicenter study (the 617 trial). Eur J Nucl Med Mol Imaging. 2021;48(1):113–122. doi:10.1007/s00259-020-04797-9
8. Asadian S, Mirzaei H, Kalantari BA, et al. β-radiating radionuclides in cancer treatment, novel insight into promising approach. Pharmacol Res. 2020;160:105070. doi:10.1016/j.phrs.2020.105070
9. Chen J, Qi L, Tang Y, et al. Current role of prostate-specific membrane antigen-based imaging and radioligand therapy in castration-resistant prostate cancer. Front Cell Develop Biol. 2022;10:958180. doi:10.3389/fcell.2022.958180
10. Jang A, Kendi AT, Sartor O. Status of PSMA-targeted radioligand therapy in prostate cancer: current data and future trials. Therapeut Adv Med Oncol. 2023;15:17588359231157632. doi:10.1177/17588359231157632
11. Strosberg J, El-Haddad G, Wolin E, et al. Phase 3 trial of 177 lu-dotatate for midgut neuroendocrine tumors. New Engl J Med. 2017;376(2):125–135. doi:10.1056/NEJMoa1607427
12. Ruigrok EAM, van Vliet N, Dalm SU, et al. Extensive preclinical evaluation of lutetium-177-labeled PSMA-specific tracers for prostate cancer radionuclide therapy. Euro J Nuclear Med Molecular Imaging. 2021;48(5):1339–1350. doi:10.1007/s00259-020-05057-6
13. Gafita A, Calais J, Grogan TR, et al. Nomograms to predict outcomes after (177)Lu-PSMA therapy in men with metastatic castration-resistant prostate cancer: an international, multicentre, retrospective study. Lancet Oncol. 2021;22(8):1115–1125. doi:10.1016/S1470-2045(21)00274-6
14. Kramer K, Pandit-Taskar N, Kushner BH, et al. Phase 1 study of intraventricular (131)I-omburtamab targeting B7H3 (CD276)-expressing CNS malignancies. J Hematol Oncol. 2022;15(1):165. doi:10.1186/s13045-022-01383-4
15. Qian Y, Liu Q, Li P, et al. Highly tumor-specific and long-acting iodine-131 microbeads for enhanced treatment of hepatocellular carcinoma with low-dose radio-chemoembolization. ACS Nano. 2021;15(2):2933–2946. doi:10.1021/acsnano.0c09122
16. Borgna F, Haller S, Rodriguez JMM, et al. Combination of terbium-161 with somatostatin receptor antagonists-a potential paradigm shift for the treatment of neuroendocrine neoplasms. Eur J Nucl Med Mol Imaging. 2022;49(4):1113–1126. doi:10.1007/s00259-021-05564-0
17. Yadav MP, Ballal S, Bal C, et al. Efficacy and safety of 177Lu-PSMA-617 radioligand therapy in metastatic castration-resistant prostate cancer patients. Clin Nucl Med. 2020;45(1):19–31. doi:10.1097/RLU.0000000000002833
18. Ahmadzadehfar H, Rahbar K, Kürpig S, et al. Early side effects and first results of radioligand therapy with (177) Lu-DKFZ-617 PSMA of castrate-resistant metastatic prostate cancer: a two-centre study. EJNMMI Research. 2015;5(1):114. doi:10.1186/s13550-015-0114-2
19. von Eyben FE, Bauman G, von Eyben R, et al. Optimizing PSMA radioligand therapy for patients with metastatic castration-resistant prostate cancer. a systematic review and meta-analysis. Int J Mol Sci. 2020;21(23):9054. doi:10.3390/ijms21239054
20. von Eyben FE, Kairemo K, Paller C, et al. (177)Lu-PSMA radioligand therapy is favorable as third-line treatment of patients with metastatic castration-resistant prostate cancer. A systematic review and network meta-analysis of randomized controlled trials. Biomedicines. 2021;9(8):1042.
21. von Eyben FE, Roviello G, Kiljunen T, et al. Third-line treatment and (177)Lu-PSMA radioligand therapy of metastatic castration-resistant prostate cancer: a systematic review. Eur J Nucl Med Mol Imaging. 2018;45(3):496–508. doi:10.1007/s00259-017-3895-x
22. Sartor O, de Bono J, Chi KN, et al. Lutetium-177-PSMA-617 for metastatic castration-resistant prostate cancer. New Engl J Med. 2021;385(12):1091–1103. doi:10.1056/NEJMoa2107322
23. Almuradova E, Seyyar M, Arak H, et al. The real-world outcomes of lutetium-177 PSMA-617 radioligand therapy in metastatic castration-resistant prostate cancer: Turkish oncology group multicenter study. Int J Cancer. 2024;154(4):692–700. doi:10.1002/ijc.34749
24. Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): a randomised, open-label, Phase 2 trial. Lancet. 2021;397(10276):797–804. doi:10.1016/S0140-6736(21)00237-3
25. Gallyamov M, Meyrick D, Barley J, et al. Renal outcomes of radioligand therapy: experience of (177)lutetium-prostate-specific membrane antigen ligand therapy in metastatic castrate-resistant prostate cancer. Clin Kidney J. 2020;13(6):1049–1055. doi:10.1093/ckj/sfz101
26. Rosar F, Kochems N, Bartholomä M, et al. Renal safety of [(177)Lu]Lu-PSMA-617 radioligand therapy in patients with compromised baseline kidney function. Cancers. 2021;14(1):13. doi:10.3390/cancers14010013
27. Zhang J, Kulkarni HR, Singh A, et al. 177 Lu-PSMA-617 radioligand therapy in metastatic castration-resistant prostate cancer patients with a single functioning kidney. J Nucl Med. 2019;60(11):1579–1586. doi:10.2967/jnumed.118.223149
28. Chi KN, Armstrong AJ, Krause BJ, et al. Safety analyses of the phase 3 VISION trial of [177Lu]Lu-PSMA-617 in patients with metastatic castration-resistant prostate cancer. Europ urol. 2024;S0302-2838(23):3297.
29. Kesavan M, Turner JH, Meyrick D, et al. Salvage radiopeptide therapy of advanced castrate-resistant prostate cancer with lutetium-177-labeled prostate-specific membrane antigen: efficacy and safety in routine practice. Cancer Biother Radiopharm. 2018;33(7):274–281. doi:10.1089/cbr.2017.2403
30. Heck MM, Tauber R, Schwaiger S, et al. Treatment outcome, toxicity, and predictive factors for radioligand therapy with (177)Lu-PSMA-I&T in metastatic castration-resistant prostate cancer. Europ urol. 2019;75(6):920–926. doi:10.1016/j.eururo.2018.11.016
31. Hofman MS, Emmett L, Sandhu S, et al. TheraP: 177 Lu-PSMA-617 (LuPSMA) versus cabazitaxel in metastatic castration-resistant prostate cancer (mCRPC) progressing after docetaxel—Overall survival after median follow-up of 3 years (ANZUP 1603). JCO. 2022;40(16_suppl):5000. doi:10.1200/JCO.2022.40.16_suppl.5000
32. Steinhelfer L, Lunger L, Cala L, et al. Long-term nephrotoxicity of 177 Lu-PSMA radioligand therapy. J Nucl Med. 2024;65(1):79–84. doi:10.2967/jnumed.123.265986
33. Banda A, Privé BM, Allach Y, et al. PSMA-RLT in patients with metastatic hormone-sensitive prostate cancer: a retrospective study. Cancers. 2022;15(1):297. doi:10.3390/cancers15010297
34. 177Lu-PSMA-617 vs. Androgen receptor-directed therapy in the treatment of progressive metastatic castrate resistant prostate cancer - full text view -ClinicalTrials.gov.
35. Hartrampf PE, Weinzierl FX, Buck AK, et al. Matched-pair analysis of [(177)Lu]Lu-PSMA I&T and [(177)Lu]Lu-PSMA-617 in patients with metastatic castration-resistant prostate cancer. Eur J Nucl Med Mol Imaging. 2022;49(9):3269–3276. doi:10.1007/s00259-022-05744-6
36. Demirkol MO, Esen B, Seymen H, et al. Radioligand therapy with 177 Lu-PSMA-I&T in patients with metastatic prostate cancer: oncological outcomes and toxicity profile. Clin Nucl Med. 2023;48(12):e564–e569. doi:10.1097/RLU.0000000000004901
37. Tauber R, Knorr K, Retz M, et al. Safety and efficacy of [177Lu]-PSMA-I&T radioligand therapy in octogenarians with metastatic castration-resistant prostate cancer: report on 80 patients over the age of 80 years. J Nucl Med. 2023;64(8):1244–1251. doi:10.2967/jnumed.122.265259
38. Schuchardt C, Zhang J, Kulkarni HR, et al. Prostate-specific membrane antigen radioligand therapy using 177 Lu-PSMA I&T and 177 Lu-PSMA-617 in patients with metastatic castration-resistant prostate cancer: comparison of safety, biodistribution, and dosimetry. J Nucl Med. 2022;63(8):1199–1207. doi:10.2967/jnumed.121.262713
39. Schäfer H, Mayr S, Büttner-Herold M, et al. Extensive 177Lu-PSMA radioligand therapy can lead to radiation nephropathy with a renal thrombotic microangiopathy-like picture. Eur Urol. 2023;83(5):385–390. doi:10.1016/j.eururo.2022.05.025
40. Juzeniene A, Stenberg VY, Bruland ØS, et al. Preclinical and clinical status of PSMA-targeted alpha therapy for metastatic castration-resistant prostate cancer. Cancers. 2021;14(1):13.
41. Patel CM, Wadas TJ, Santiago-Toribio A, Sánchez A. Progress in targeted alpha-particle-emitting radiopharmaceuticals as treatments for prostate cancer patients with bone metastases. Molecules. 2021;27(1):26. doi:10.3390/molecules27010026
42. Schumann S, Eberlein U, Muhtadi R, et al. DNA damage in leukocytes after internal ex-vivo irradiation of blood with the α-emitter Ra-223. Sci Rep. 2018;8(1):2286. doi:10.1038/s41598-018-20364-7
43. Aghevlian S, Boyle AJ, Reilly RM. Radioimmunotherapy of cancer with high linear energy transfer (LET) radiation delivered by radionuclides emitting α-particles or Auger electrons. Adv Drug Deliv Rev. 2017;109:102–118. doi:10.1016/j.addr.2015.12.003
44. Seidl C. Radioimmunotherapy with α-particle-emitting radionuclides. Immunotherapy. 2014;6(4):431–458. doi:10.2217/imt.14.16
45. Kossert K, Takács MP, Nähle O. Determination of the activity of 225Ac and of the half-lives of 213Po and 225Ac. Appl Radiat Isot. 2020;156:109020. doi:10.1016/j.apradiso.2019.109020
46. Stokke C, Kvassheim M, Blakkisrud J. Radionuclides for targeted therapy: physical properties. Molecules. 2022;27(17):5429. doi:10.3390/molecules27175429
47. Tamborino G, Nonnekens J, Struelens L, et al. Therapeutic efficacy of heterogeneously distributed radiolabelled peptides: influence of radionuclide choice. Phys Med. 2022;96:90–100. doi:10.1016/j.ejmp.2022.02.021
48. Banerjee SR, Lisok A, Minn I, et al. Preclinical evaluation of 213Bi- and 225Ac-labeled low-molecular-weight compounds for radiopharmaceutical therapy of prostate cancer. J Nucl Med. 2021;62(7):980–988. doi:10.2967/jnumed.120.256388
49. Kratochwil C, Bruchertseifer F, Rathke H, et al. Targeted α-therapy of metastatic castration-resistant prostate cancer with 225 Ac-PSMA-617: swimmer-plot analysis suggests efficacy regarding duration of tumor control. J Nucl Med. 2018;59(5):795–802. doi:10.2967/jnumed.117.203539
50. Unterrainer LM, Beyer L. Total tumor volume on (18)F-PSMA-1007 PET as additional imaging biomarker in mCRPC patients undergoing PSMA-targeted alpha therapy with (225)Ac-PSMA-I&T. Biomedicines. 2022;11(1):10. doi:10.3390/biomedicines11010010
51. Sathekge M, Bruchertseifer F, Knoesen O, et al. (225)Ac-PSMA-617 in chemotherapy-naive patients with advanced prostate cancer: a pilot study. Eur J Nucl Med Mol Imaging. 2019;46(1):129–138. doi:10.1007/s00259-018-4167-0
52. Kratochwil C, Bruchertseifer F, Giesel FL, et al. 225 Ac-PSMA-617 for PSMA-targeted α-radiation therapy of metastatic castration-resistant prostate cancer. J Nucl Med. 2016;57(12):1941–1944. doi:10.2967/jnumed.116.178673
53. Yadav MP, Ballal S, Sahoo RK, et al. Efficacy and safety of 225 Ac-PSMA-617 targeted alpha therapy in metastatic castration-resistant prostate cancer patients. Theranostics. 2020;10(20):9364–9377. doi:10.7150/thno.48107
54. Sanli Y, Kuyumcu S, Simsek DH, et al. 225Ac-prostate-specific membrane antigen therapy for castration-resistant prostate cancer: a single-center experience. Clin Nucl Med. 2021;46(12):943–951. doi:10.1097/RLU.0000000000003925
55. Sen I, Thakral P, Tiwari P, et al. Therapeutic efficacy of (225)Ac-PSMA-617 targeted alpha therapy in patients of metastatic castrate resistant prostate cancer after taxane-based chemotherapy. Ann Nuclear Med. 2021;35(7):794–810. doi:10.1007/s12149-021-01617-4
56. Feuerecker B, Tauber R, Knorr K, et al. Activity and adverse events of actinium-225-PSMA-617 in advanced metastatic castration-resistant prostate cancer after failure of lutetium-177-PSMA. Europ urol. 2021;79(3):343–350. doi:10.1016/j.eururo.2020.11.013
57. Sathekge M, Bruchertseifer F, Vorster M, et al. Predictors of overall and disease-free survival in metastatic castration-resistant prostate cancer patients receiving 225 Ac-PSMA-617 radioligand therapy. J Nucl Med. 2020;61(1):62–69. doi:10.2967/jnumed.119.229229
58. Lee DY, Kim YI. Effects of 225 Ac-labeled prostate-specific membrane antigen radioligand therapy in metastatic castration-resistant prostate cancer: a meta-analysis. J Nucl Med. 2022;63(6):840–846. doi:10.2967/jnumed.121.262017
59. Sathekge MM, Lawal IO, Bal C, et al. Actinium-225-PSMA radioligand therapy of metastatic castration-resistant prostate cancer (WARMTH Act): a multicentre, retrospective study. Lancet Oncol. 2024;25(2):175–183. doi:10.1016/S1470-2045(23)00638-1
60. Zacherl MJ, Gildehaus FJ, Mittlmeier L, et al. First clinical results for PSMA-targeted α-therapy using 225 Ac-PSMA-I&T in advanced-mCRPC patients. J Nucl Med. 2021;62(5):669–674. doi:10.2967/jnumed.120.251017
61. Sathekge M, Bruchertseifer F, Vorster M, et al. mCRPC patients receiving 225 Ac-PSMA-617 therapy in the post–androgen deprivation therapy setting: response to treatment and survival analysis. J Nucl Med. 2022;63(10):1496–1502. doi:10.2967/jnumed.121.263618
62. Sathekge M, Bruchertseifer F, Vorster M, et al. (225)Ac-PSMA-617 radioligand therapy of de novo metastatic hormone-sensitive prostate carcinoma (mHSPC): preliminary clinical findings. Eur J Nucl Med Mol Imaging. 2023;50(7):2210–2218. doi:10.1007/s00259-023-06165-9
63. Violet J, Jackson P, Ferdinandus J, et al. Dosimetry of 177 Lu-PSMA-617 in metastatic castration-resistant prostate cancer: correlations between pretherapeutic imaging and whole-body tumor dosimetry with treatment outcomes. J Nucl Med. 2019;60(4):517–523. doi:10.2967/jnumed.118.219352
64. Kletting P, Thieme A, Eberhardt N, et al. Modeling and predicting tumor response in radioligand therapy. J Nucl Med. 2019;60(1):65–70. doi:10.2967/jnumed.118.210377
65. Sathekge M, Knoesen O, Meckel M, et al. (213)Bi-PSMA-617 targeted alpha-radionuclide therapy in metastatic castration-resistant prostate cancer. Eur J Nucl Med Mol Imaging. 2017;44(6):1099–1100. doi:10.1007/s00259-017-3657-9
66. Hammer S, Hagemann UB, Zitzmann-Kolbe S. Preclinical efficacy of a PSMA-targeted thorium-227 conjugate (PSMA-TTC), a targeted alpha therapy for prostate cancer. Clin Cancer Res. 2020;26(8):1985–1996. doi:10.1158/1078-0432.CCR-19-2268
67. Hammer S, Schlicker A, Zitzmann-Kolbe S. Darolutamide potentiates the antitumor efficacy of a PSMA-targeted thorium-227 conjugate by a dual mode of action in prostate cancer models. Clin Cancer Res. 2021;27(15):4367–4378. doi:10.1158/1078-0432.CCR-21-0342
68. Wale DJ, Viglianti BL, Gross MD, Ferretti A, Rubello D, Wong KK. Nuclear medicine therapy with 223Radium-dichloride for osseous metastases in prostate carcinoma. Am J Clin Oncol. 2019;42(1):99–106. doi:10.1097/COC.0000000000000479
69. Suman S, Parghane RV, Joshi A, et al. Combined 177 Lu-PSMA-617 PRLT and abiraterone acetate versus 177 Lu-PSMA-617 PRLT monotherapy in metastatic castration-resistant prostate cancer: an observational study comparing the response and durability. Prostate. 2021;81(15):1225–1234. doi:10.1002/pros.24219
70. Satapathy S, Mittal BR, Sood A. (177)Lu-PSMA-617 versus docetaxel in chemotherapy-naïve metastatic castration-resistant prostate cancer: a randomized, controlled, phase 2 non-inferiority trial. Eur J Nucl Med Mol Imaging. 2022;49(5):1754–1764. doi:10.1007/s00259-021-05618-3
71. Dhiantravan N, Emmett L, Joshua AM, et al. UpFrontPSMA: a randomized phase 2 study of sequential 177 Lu-PSMA-617 and docetaxel vs docetaxel in metastatic hormone-naïve prostate cancer (clinical trial protocol). BJU Int. 2021;128(3):331–342. doi:10.1111/bju.15384
72. Cabazitaxel in combination with 177Lu-PSMA-617 in metastatic castration-resistant prostate cancer (LuCAB) - full text view -ClinicalTrials.gov.
73. 177Lu-PSMA-617 therapy and olaparib in patients with metastatic castration resistant prostate cancer - full text view -ClinicalTrials.gov.
74. 177Lu-PSMA-617 and pembrolizumab in treating patients with metastatic castration-resistant prostate cancer - full text view -ClinicalTrials.gov.
75. PRINCE (PSMA-lutetium radionuclide therapy and immunotherapy in prostate CancEr) - full text view -ClinicalTrials.gov.
76. EVOLUTION: 177Lu-PSMA therapy versus 177Lu-PSMA in combination with ipilimumab and nivolumab for men with mCRPC - full text view -ClinicalTrials.gov.
77. Kostos L, Buteau JP, Yeung T, et al. AlphaBet: combination of radium-223 and [177Lu]Lu-PSMA-I&T in men with metastatic castration-resistant prostate cancer (clinical trial protocol). Front Med Lausanne. 2022;9:1059122. doi:10.3389/fmed.2022.1059122
78. Rahbar K, Boegemann M, Yordanova A, et al. PSMA targeted radioligandtherapy in metastatic castration resistant prostate cancer after chemotherapy, Abiraterone and/or enzalutamide. A retrospective analysis of overall survival. Eur J Nucl Med Mol Imaging. 2018;45(1):12–19. doi:10.1007/s00259-017-3848-4
79. Satapathy S, Sood A, Das CK, Mittal BR. Evolving role of (225)Ac-PSMA radioligand therapy in metastatic castration-resistant prostate cancer-a systematic review and meta-analysis. Prostate Cancer Prostatic Dis. 2021;24(3):880–890. doi:10.1038/s41391-021-00349-w
80. Pathmanandavel S, Crumbaker M, Yam AO, et al. 177 Lu-PSMA-617 and idronoxil in men with end-stage metastatic castration-resistant prostate cancer (LuPIN): patient outcomes and predictors of treatment response in a phase I/II Trial. J Nucl Med. 2022;63(4):560–566. doi:10.2967/jnumed.121.262552
81. Crumbaker M, Pathmanandavel S, Yam AO, et al. Phase I/II trial of the combination of (177)lutetium prostate specific membrane antigen 617 and Idronoxil (NOX66) in men with end-stage metastatic castration-resistant prostate cancer (LuPIN). European Urol Oncol. 2021;4(6):963–970. doi:10.1016/j.euo.2020.07.002
82. Khreish F, Ebert N, Ries M, et al. (225)Ac-PSMA-617/(177)Lu-PSMA-617 tandem therapy of metastatic castration-resistant prostate cancer: pilot experience. Eur J Nucl Med Mol Imaging. 2020;47(3):721–728. doi:10.1007/s00259-019-04612-0
83. Rosar F, Hau F, Bartholomä M, et al. Molecular imaging and biochemical response assessment after a single cycle of [225 Ac]Ac-PSMA-617/[177 Lu]Lu-PSMA-617 tandem therapy in mCRPC patients who have progressed on [177 Lu]Lu-PSMA-617 monotherapy. Theranostics. 2021;11(9):4050–4060. doi:10.7150/thno.56211
84. Mader N, Groener D, Tselis N. Outcome of (177)Lu-PSMA-617 radioligand therapy in chemo-refractory patients with metastatic castration-resistant early-onset prostate cancer. Cancers. 2021;13(16):4193. doi:10.3390/cancers13164193
85. Gadot M, Davidson T, Aharon M, et al. Clinical variables associated with PSA response to lutetium-177-PSMA ([177Lu]-PSMA-617) radionuclide treatment in men with metastatic castration-resistant prostate cancer. Cancers. 2020;12(5):1078. doi:10.3390/cancers12051078
86. Sadaghiani MS, Sheikhbahaei S, Werner RA, et al. A systematic review and meta-analysis of the effectiveness and toxicities of lutetium-177-labeled prostate-specific membrane antigen-targeted radioligand therapy in metastatic castration-resistant prostate cancer. Europ urol. 2021;80(1):82–94. doi:10.1016/j.eururo.2021.03.004
87. Rasul S, Hartenbach M, Wollenweber T, et al. Prediction of response and survival after standardized treatment with 7400 MBq (177)Lu-PSMA-617 every 4 weeks in patients with metastatic castration-resistant prostate cancer. Eur J Nucl Med Mol Imaging. 2021;48(5):1650–1657. doi:10.1007/s00259-020-05082-5
88. Gafita A, Heck MM, Rauscher I, et al. Early prostate-specific antigen changes and clinical outcome after 177 Lu-PSMA Radionuclide treatment in patients with metastatic castration-resistant prostate cancer. J Nucl Med. 2020;61(10):1476–1483. doi:10.2967/jnumed.119.240242
89. Benešová M, Umbricht CA, Schibli R, et al. Albumin-binding PSMA ligands: optimization of the tissue distribution profile. Mol Pharm. 2018;15(3):934–946. doi:10.1021/acs.molpharmaceut.7b00877
90. Yadav MP, Ballal S, Sahoo RK, et al. Radioligand therapy with 177 Lu-PSMA for metastatic castration-resistant prostate cancer: a systematic review and meta-analysis. AJR. 2019;213(2):275–285. doi:10.2214/AJR.18.20845
91. Barber TW, Singh A, Kulkarni HR, et al. Clinical outcomes of 177 Lu-PSMA radioligand therapy in earlier and later phases of metastatic castration-resistant prostate cancer grouped by previous taxane chemotherapy. J Nucl Med. 2019;60(7):955–962. doi:10.2967/jnumed.118.216820
92. Suman S, Parghane RV, Joshi A, et al. Therapeutic efficacy, prognostic variables and clinical outcome of (177)Lu-PSMA-617 PRLT in progressive mCRPC following multiple lines of treatment: prognostic implications of high FDG uptake on dual tracer PET-CT vis-à-vis Gleason score in such cohort. British J Radiol. 2019;92(1104):20190380. doi:10.1259/bjr.20190380
93. Yordanova A, Linden P, Hauser S, et al. The value of tumor markers in men with metastatic prostate cancer undergoing [177 Lu]Lu-PSMA therapy. Prostate. 2020;80(1):17–27. doi:10.1002/pros.23912
94. Karimzadeh A, Heck M, Tauber R, et al. 177 Lu-PSMA-I&T for treatment of metastatic castration-resistant prostate cancer: prognostic value of scintigraphic and clinical biomarkers. J Nucl Med. 2023;64(3):402–409. doi:10.2967/jnumed.122.264402
95. Stangl-Kremser J, Rasul S, Tosoian JJ, et al. Single-lesion prostate-specific membrane antigen protein expression (PSMA) and response to [(177)Lu]-PSMA-ligand therapy in patients with castration-resistant prostate cancer. Euro Urolog Open Sci. 2021;30:63–66. doi:10.1016/j.euros.2021.06.007
96. Kessel K, Seifert R, Weckesser M, et al. Molecular analysis of circulating tumor cells of metastatic castration-resistant prostate cancer patients receiving 177 Lu-PSMA-617 radioligand therapy. Theranostics. 2020;10(17):7645–7655. doi:10.7150/thno.44556
97. van der Doelen MJ, Mehra N, van Oort IM, et al. Clinical outcomes and molecular profiling of advanced metastatic castration-resistant prostate cancer patients treated with 225Ac-PSMA-617 targeted alpha-radiation therapy. Urol Oncol. 2021;39(10):729.e7–729. doi:10.1016/j.urolonc.2020.12.002
98. Widjaja L, Werner RA, Krischke E, et al. Individual radiosensitivity reflected by γ-H2AX and 53BP1 foci predicts outcome in PSMA-targeted radioligand therapy. Eur J Nucl Med Mol Imaging. 2023;50(2):602–612. doi:10.1007/s00259-022-05974-8
99. Roscher M, Bakos G, Benešová M. Atomic nanogenerators in targeted alpha therapies: curie’s legacy in modern cancer management. Pharmaceuticals. 2020;13(4):76.
100. Rupp NJ, Umbricht CA, Pizzuto DA, et al. First clinicopathologic evidence of a non–psma-related uptake mechanism for 68 Ga-PSMA-11 in salivary glands. J Nucl Med. 2019;60(9):1270–1276. doi:10.2967/jnumed.118.222307
101. Poty S, Francesconi LC, McDevitt MR, et al. α-emitters for radiotherapy: from basic radiochemistry to clinical studies-part 1. J Nucl Med. 2018;59(6):878–884. doi:10.2967/jnumed.116.186338
102. Simons BW, Turtle NF, Ulmert DH, et al. PSMA expression in the Hi-Myc model; extended utility of a representative model of prostate adenocarcinoma for biological insight and as a drug discovery tool. Prostate. 2019;79(6):678–685. doi:10.1002/pros.23770
103. Roy J, Warner BM, Basuli F, et al. Comparison of prostate-specific membrane antigen expression levels in human salivary glands to non-human primates and rodents. Cancer Biother Radiopharm. 2020;35(4):284–291. doi:10.1089/cbr.2019.3079
104. Stenberg VY, Juzeniene A, Bruland ØS, et al. In situ generated 212 Pb-PSMA ligand in a 224 Ra-solution for dual targeting of prostate cancer sclerotic stroma and PSMA-positive cells. Curr Radiopharm. 2020;13(2):130–141. doi:10.2174/1874471013666200511000532
105. Kramer V, Fernández R, Lehnert W, et al. Biodistribution and dosimetry of a single dose of albumin-binding ligand [(177)Lu]Lu-PSMA-ALB-56 in patients with mCRPC. Eur J Nucl Med Mol Imaging. 2021;48(3):893–903. doi:10.1007/s00259-020-05022-3
106. Tschan VJ, Borgna F, Busslinger SD, et al. Preclinical investigations using [(177)Lu]Lu-Ibu-DAB-PSMA toward its clinical translation for radioligand therapy of prostate cancer. Eur J Nucl Med Mol Imaging. 2022;49(11):3639–3650. doi:10.1007/s00259-022-05837-2
107. Yusufi N, Wurzer A, Herz M, et al. Comparative preclinical biodistribution, dosimetry, and endoradiotherapy in metastatic castration-resistant prostate cancer using 19F/ 177 Lu-rhPSMA-7.3 and 177 Lu-PSMA I&T. J Nucl Med. 2021;62(8):1106–1111. doi:10.2967/jnumed.120.254516
108. Chan TG, O’Neill E, Habjan C, et al. Combination strategies to improve targeted radionuclide therapy. J Nucl Med. 2020;61(11):1544–1552. doi:10.2967/jnumed.120.248062
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.