")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Advancements in the Study of Biologic Agents in Comorbidities of Psoriasis: A Literature Review
Authors Wang Y, Zhang P, Lv Y, Deng Y, Yao M, Wang L, Pan G
Received 7 September 2023
Accepted for publication 21 November 2023
Published 4 December 2023 Volume 2023:16 Pages 3487—3495
DOI https://doi.org/10.2147/CCID.S439110
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Yuhan Wang,1,* Ping Zhang,1,* Yu Lv,1 Yu Deng,2 Ming Yao,3 Lin Wang,1 Guangtao Pan3
1College of Traditional Chinese Medicine, Hubei University of Chinese Medicine, Wuhan, Hubei Province, People’s Republic of China; 2Department of Encephalopathy, Guangzhou Hospital of Integrated Traditional and West Medicine Affiliated to Guangzhou University of Chinese Medicine, Guangzhou, People’s Republic of China; 3Department of Dermatology, Yancheng Hospital of Traditional Chinese Medicine Affiliated to Nanjing University of Chinese Medicine, Yancheng, Jiangsu Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guangtao Pan, Department of Dermatology, Yancheng Hospital of Traditional Chinese Medicine Affiliated to Nanjing University of Chinese Medicine, No. 53, Renmin North Road, Tinghu District, Yancheng, Jiangsu Province, People’s Republic of China, Tel +86-17612738767, Email [email protected]
Abstract: This literature review systematically searched relevant literature from the past 10 years using various medical databases, including PubMed, Medline, Cochrane, China National Knowledge Infrastructure (CNKI), Wanfang, and Weipu. As a chronic inflammatory disease, psoriasis is associated with various cells and cytokines of the body’s immune system, making them more susceptible to various systemic comorbidities than the general population. At a time when conventional regimens are ineffective and there is a lack of personalized treatment options for such comorbidities, the development of biologics has revolutionized the treatment of psoriasis comorbidities, and a number of biologic combination therapies have been incorporated into first-line treatments in many countries. The focus of this review was to investigate the relationship between psoriasis and comorbidities, such as metabolic syndrome, psoriatic arthritis, cardiovascular diseases, mental disorders, infectious diseases, digestive system diseases, and renal diseases. Furthermore, the study explored the significance of biologic therapies in the management of these comorbidities. Also this paper suggests current conditions and precautions for the use of biologic therapies to minimize the occurrence of adverse effects. This review was performed to provide guidance for clinical drug selection in patients with psoriasis and comorbidities, as well as serve as a reference for the development and application of biologic therapies.
Keywords: psoriasis, biologics, comorbidity, research advancements
Psoriasis is a chronic inflammatory disease characterized by skin and joint manifestations. Due to the persistent inflammatory state observed in patients with psoriasis, they are more prone to develop various systemic comorbidities compared to the general population. The commonly recognized pathogenic mechanisms include excessive epidermal proliferation triggered by TH1 and TH17 responses, chronic neovascularization, and chronic inflammatory reactions.1 The use of biologic agents has become a trend for individuals with psoriasis who have suboptimal responses to conventional therapies and concurrent comorbidities. Biologic therapies for psoriasis primarily target tumor necrosis factor-alpha (TNF-α), interleukin (IL)-17A, and IL-23. The selection of biologic agents is of significant importance for patients with psoriasis who have complications and comorbidities, as it provides the optimal personalized treatment approach and harnesses the maximum benefits of biologic therapies. This study provides a comprehensive review of the research progress in the treatment strategies of biologics for the comorbidities of psoriasis, based on the classification and summarization of studies conducted both domestically and internationally.
Metabolic Syndrome
Metabolic syndrome (MS) is a syndrome characterized by obesity, hyperglycemia, hypertension, and other major features. In recent years, the correlation between psoriasis and metabolic syndrome has emerged as an important topic in dermatology.
Obesity
Kim et al2 pointed out that obesity is an independent risk factor affecting the development and exacerbation of psoriasis. Chronic inflammation has been identified as a mechanism linking psoriasis and obesity.3 Weight loss has been demonstrated to alleviate psoriatic lesions, and the occurrence of psoriasis increases the prevalence of obesity among patients. Optimal responses with fixed dose biological agents are less frequent in patients with increasing weight, especially above 100 kg, who account for approximately 25% to 30% of patients in clinical trials.4 Multiple biologics have limited efficacy in the management of obesity, with the exception of infliximab, which is the only medication administered per kilogram of body weight. It is one of the options for patients with severe obesity. For obese patients who do not respond to standard dosage, increasing the dosage or shortening the dosing interval may be considered.5 Therefore, infliximab can be used to treat psoriasis with comorbid obesity. The direct effects of IL-17 inhibitors on obesity have not been clearly documented.6
Diabetes
The study conducted by Kong et al7 revealed a significantly higher incidence of type 2 diabetes (28.77%) in patients with psoriasis compared to the normal population (8.97%). In its pathogenesis, research has shown that inflammatory factors, such as tumor necrosis factor-alpha (TNF-α), interleukin (IL)-1, and IL-6, in patients with psoriasis can promote insulin resistance and induce β-cell apoptosis, leading to elevated blood glucose levels.8 In the clinical application of biologics, TNF-α inhibitors have been suggested to enhance insulin resistance by modulating the interaction between insulin receptors and adipokines or inflammatory factors.9 Notably, ustekinumab has been highlighted to ameliorate insulin resistance and reduce levels of C-reactive protein.10 Meanwhile a study from Pirowska M’s team found that serum levels of IL-17 were significantly elevated in psoriasis patients with comorbid MS, and that blocking this pathway lowered blood glucose levels in psoriasis patients and in a mouse model11
Hypertension
The prevalence of hypertension is significantly increased in patients with moderate to severe psoriasis. Experimental studies abroad have indicated that the occurrence of hypertension and susceptibility to psoriasis are associated with such genes as endothelial nitric oxide synthase (eNOS), leucyl and cystinyl aminopeptidase (LNPEP), and human leukocyte antigen (HLA). TNF-α inhibitors and IL-17 inhibitors can reduce hypertension-related arterial inflammation and benefit endothelial cells, leading to a lowered incidence of hypertension.12
Psoriatic Arthritis (PsA)
PsA is a specific inflammatory disease associated with peripheral and axial joints, skin, tendons, and nails. PsA is a common comorbidity associated with psoriasis and can lead to permanent disability. The pathogenesis of PsA is still poorly understood, but evidence suggests that the IL-23/17 pathway is a key driving factor of inflammation. IL-23 influences the expression of helper T cell-derived IL-17, IL-22, and TNF-α, leading to inflammation, tissue damage, and the production of other cytokines.13 In clinical practice, early treatment is of paramount importance in preventing complications and improving the quality of life for patients with PsA. The number of disease-modifying antirheumatic drugs (DMARDs) indicated for PsA has increased during the last decade. The armamentarium now includes not only conventional synthetic DMARDs (csDMARDs) such as methotrexate (MTX), leflunomide and tumour necrosis factor inhibitors (TNFi), but also other targeted biological agents (bDMARDs) aimed at different cytokines, such as TNF, interleukin (IL)-12/23 and IL-17A.14 Biologic therapies for psoriasis have different efficacy in treating skin and joint diseases. Therefore, selecting the appropriate treatment method is highly important and should be tailored to individual patients. If axial symptoms of PsA cannot be controlled by nonsteroidal anti-inflammatory drugs (NSAIDs), guidelines developed by the Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA), the European League Against Rheumatism (EULAR), the American College of Rheumatology (ACR), and the National Psoriasis Foundation (NPF) recommend the use of biologic disease-modifying antirheumatic drugs. The current approach for treating PsA typically involves the use of TNF inhibitors. However, in cases with significant skin involvement, IL-17A inhibitors are favored over TNF inhibitors.14 Recent research indicates that IL-23 inhibitors may be effective in treating axial symptoms in patients with PsA. Data from axial spondyloarthritis (axSpA) studies suggest that conventional synthetic disease-modifying antirheumatic drugs (such as methotrexate) and systemic corticosteroids are not recommended for the treatment of axial PsA.15 Overall, TNF inhibitors are recommended as first-line therapy for patients with severe PsA, regardless of the presence of severe skin involvement. As a second-line treatment, IL-17 inhibitors are advised, followed by IL-23 inhibitors.
Cardiovascular Diseases (CVDs)
The pathogenesis of the comorbid CVDs in psoriasis involves genetic factors, lipid factors, insulin resistance, lipoproteins, angiogenesis, oxidative stress, and hypercoagulability. Consequently, the treatment of psoriasis with comorbid CVDs has become one of the recent research hotspots. Biologic therapies for psoriasis and concurrent CVDs are commonly employed in clinical practice. Hjuler et al16 demonstrated in a controlled clinical study that biologic therapy can attenuate the progression of coronary artery disease to a certain extent in patients with psoriasis. Among them, the use of TNF inhibitors in the treatment of psoriasis is associated with a reduction in the incidence of CVDs in patients with psoriasis. TNF-α inhibitors improve endothelial function and reduce the risk of myocardial infarction. In a previous study, the risk of comorbid CVDs and major adverse cardiovascular events (MACEs) was assessed in psoriasis patients receiving TNF inhibitor therapy compared to those receiving oral/topical therapies and local treatment. The results demonstrated a significant reduction in the risk for MACEs among psoriasis patients receiving TNF inhibitor therapy compared to other control groups. These findings suggest a potentially protective effect of TNF inhibitor therapy on the risk for MACEs in patients with psoriasis.17 In the study of Wu et al18 a comparison was made in the therapeutic efficacy between methotrexate and TNF inhibitor treatment for psoriasis-related CVDs. The findings indicated that TNF inhibitor therapy may contribute to a reduction in the risk of CVDs in patients with psoriasis. Furthermore, other studies have uncovered that the use of ustekinumab could potentially lower the occurrence of cardiovascular events.19 Current guidelines for the management of patients with psoriasis and cardiovascular comorbidities recommend the use of IL-17 inhibitors and IL-23 inhibitors (such as ustekinumab). Nevertheless, for patients with severe heart failure classified as New York Heart Association (NYHA) class III/IV, the use of TNF inhibitors should be avoided.20
Mental Disorders
Mental disorders are common comorbidities of psoriasis, including depression, suicidal behaviors, and suicidal ideation. Patients with psoriasis are at a higher risk of depression compared to the general population.21 Hence, the management and treatment of mental disorders in patients with psoriasis are also crucial to provide comprehensive care. In addition to conventional antidepressant treatment, biologics have profound effects on depression in patients with psoriasis. A randomized controlled trial of adalimumab, etanercept, and ustekinumab has demonstrated statistically significant reductions in depression symptom scores among patients with moderate to severe psoriasis.22 A prior foreign study has found that psoriasis patients with upregulated IL-17A levels carry an increased risk of depression and anxiety. In a mouse model of psoriasis, administration of anti-IL-17A treatment led to a decline in depressive-like symptoms.23 Nonetheless, caution should be exercised before using IL-17 inhibitors (such as brodalumab) in psoriasis patients with depression or suicidal ideation.24 On the other hand, clinical trials have demonstrated the antidepressant effects of anti-inflammatory drugs, such as TNF-α antagonists, in the treatment of depression. Furthermore, research is underway to explore new directions targeting inflammatory mechanisms, including the use of IL-6 inhibitors.25
Infectious Diseases
Psoriasis is an inflammatory response caused by excessive activation of the natural immune system, which often manifests as various types of infections. The extent of skin involvement and the Psoriasis Area and Severity Index (PASI) are commonly used indicators to measure the severity of psoriasis, with severe PASI itself susceptible to infection. Research conducted by Takeshita et al in the UK revealed an increased risk of pneumonia in patients with severe PASI scores.26 In clinical practice, a combination of methotrexate and biologics is commonly used for the treatment of psoriasis. However, methotrexate carries the risks of hepatotoxicity and myelosuppression, while the use of biologics also poses the risk of infection. Concurrent administration of these medications may lead to varicella-zoster virus infection. Prior research has highlighted that the use of infliximab increases the risk of Pneumocystis pneumonia,27 while secukinumab and ixekizumab are prone to upper respiratory tract infections. There have also been reports indicating that secukinumab carries the risk of interstitial pneumonia during its use.28
Tuberculosis Infection
For patients with latent tuberculosis infection (LTBI), the use of TNF-α inhibitors can activate the tuberculosis infection.29 TNF-α inhibitors and IL-23 inhibitors (such as ustekinumab) should be initiated for biologic treatment at least one month after preventive treatment with isoniazid. However the risk is lower with the fusion protein-based TNF-α inhibitor etanercept. Because its half-life is only 3 days, its cycle of TNF-α inhibition is relatively brief and its effect is incomplete, the risk of potential tuberculosis infection during use is low. As interleukin inhibitors, IL-17 inhibitors are considered relatively safe during application, and there have been no reported cases of LTBI activation following their use.29 More clinical data are needed for the application of IL-23 inhibitors.
Human Immunodeficiency Virus (HIV) Infection
HIV infection is an independent risk factor for the development of psoriasis, and in such patients, immunosuppressants may reactivate or induce infections.30 Biologic agents can be used in conjunction with highly active antiretroviral therapy (HAART) for HIV-positive patients with moderate to severe psoriasis who are resistant to conventional systemic treatments. Regarding the application of biologic agents, research has demonstrated that elevated levels of TNF-α are associated with high levels of HIV replication and disease progression. Therefore, psoriasis patients with HIV infection may be prioritized for TNF-α inhibitor therapy.31 For IL-17 inhibitors, a foreign team32 has reported the use of ixekizumab and secukinumab in the treatment of HIV-positive patients with comorbid psoriasis. Significant clearance of skin lesions was observed, with no relapses or opportunistic infections reported. These findings suggest that IL-17 inhibitors could be a promising and safe treatment option for managing psoriasis in HIV-positive patients. In IL-23 inhibitors,33 ustekinumab can be used for HIV-infected patients who have already received antiretroviral therapy.34 There have also been case reports abroad on the use of risankizumab for treating HIV-positive patients with psoriasis.35 Currently, more data are needed to validate the application of IL-23 inhibitors. However, it is evident that compared to TNF-α inhibitors, the risk of opportunistic infections is lower with IL-23 inhibitors treatment.33 This result implies that the use of IL-23 inhibitors could be a novel therapeutic approach for such comorbidities.
Viral Hepatitis
Studies conducted in China, a country with a high prevalence of viral hepatitis, have established an association between the severity of psoriasis (measured by PASI) and various liver diseases, such as alcoholic liver disease, non-alcoholic liver disease, and chronic hepatitis. However, the use of certain biologic agents in the treatment of psoriasis with comorbid hepatitis carries some risks. TNF-α plays an essential role in the clearance of hepatitis viruses, so patients with psoriasis and hepatitis may experience worsened liver conditions when treated with TNF-α inhibitors. During the active phase of hepatitis B virus (HBV) infection, the application of biologic agents for psoriasis treatment is contraindicated.36 For patients with chronic hepatitis C, the use of TNF-α inhibitors carries a relatively low risk, but regular monitoring of hepatitis C virus (HCV)-RNA viral load and comprehensive liver function assessment is necessary. In cases where hepatitis B has been resolved, the concurrent use of biologic agents requires close monitoring of liver function. A previous study conducted abroad has demonstrated no elevation in liver enzymes or viral load when using secukinumab to treat psoriasis combined with HBV/HCV infection.37 Similarly, relevant data in China has highlighted favorable therapeutic outcomes when using secukinumab to treat psoriasis with comorbid chronic hepatitis B.38
Diseases of the Digestive System
Inflammatory bowel disease (IBD), a non-specific chronic inflammatory disorder of the gastrointestinal tract, is primarily categorized into two subtypes: ulcerative colitis (UC) and Crohn’s disease (CD). These subtypes affect the small intestine, colon, and rectum. Although research has demonstrated that psoriasis significantly increases the incidence of CD, there are only a few reports regarding its association with UC.39 Both psoriasis and IBD are immune-mediated systemic inflammatory diseases, sharing common pathogenic pathways involving TNF-α, IL-23, and IL-17. TNF-α inhibitors, such as infliximab and adalimumab, are commonly used foundational medications for treating both conditions, but they carry a risk of inducing paradoxical psoriasis in 2–5% of cases.40 Ustekinumab has been found to be an effective treatment option for this scenario, with sufficient evidence supporting its efficacy in simultaneously managing TNF-α-induced paradoxical psoriasis and controlling IBD symptoms.41 Currently, IL-23 serves as a therapeutic target for the treatment of IBD. The administration of IL-23 inhibitors has been supported by a series of clinical trials, demonstrating their sufficient safety.42 In contrast, the efficacy of IL-17 inhibitors is relatively poor, and their use increases the risk of IBD in patients with psoriasis. This condition may be related to the role of IL-17 in regulating the balance of intestinal microbiota and maintaining the integrity of the intestinal mucosal barrier.43 Furthermore, research has also indicated that dupilumab (trade name: Dupixent) is safe and effective in treating dermatitis in patients with IBD, whether it is atopic dermatitis or dermatitis induced or exacerbated by anti-TNF therapy.44
Renal Diseases
Psoriatic nephropathy, as a comorbidity pattern identified in recent years, can manifest as hematuria, proteinuria, increased blood pressure, renal insufficiency, and other symptoms on the basis of psoriatic skin lesions. The incidence of chronic kidney disease (CKD) is positively correlated with the severity of psoriasis, as prior evidence has indicated a notable increase in the risk of CKD in patients with psoriasis.45 Furthermore, existing data have reflected that patients with moderate to severe psoriasis have an elevated risk of glomerular diseases, particularly IgA nephropathy.46 An experiment conducted by Ren et al47 observed significant inflammatory responses in patients with psoriasis. These inflammatory reactions result in damage to renal tubules, glomerular cells, podocytes, and glomerular membrane cells in the kidneys, ultimately leading to renal injury. By inhibiting the expression of inflammatory factors, the damage to podocytes is reduced, thereby alleviating psoriatic nephropathy. Nonetheless, certain conventional treatments confer nephrotoxic effects, which can further exacerbate the kidney burden and affect renal function. The use of biologics, on the other hand, addresses this issue. In international guidelines for the treatment of psoriasis, biologic agents, particularly TNF-α inhibitors or IL-23 inhibitors, are recommended as the first-line therapy for patients with psoriasis and comorbid CKD.48 In China, there have been cases of using ustekinumab for the treatment of psoriasis comorbid with renal insufficiency. It has also been indicated that the use of adalimumab may induce the comorbid IgA nephropathy of psoriasis during its administration.49 However, further data validation is required to substantiate these findings. Psoriasis comorbid with end-stage renal disease is a common cause of mortality. For general patients with psoriasis, it is advisable to avoid the use of nephrotoxic drugs whenever possible, choose biologics rationally, monitor renal function regularly, assess the risk of renal disease, and reduce the mortality rate associated with such conditions. For patients with renal disease requiring hemodialysis, it is suggested to use IL-23 inhibitors (such as ustekinumab), TNF-α inhibitors, and IL-17 inhibitors as first-line biologics.50
Novel Coronavirus Pneumonia
The coronavirus disease 2019 (COVID-19) has become a widespread epidemic worldwide in recent years, and it is particularly common for patients with psoriasis to have concurrent infections of the novel coronavirus. Based on this observation, a retrospective cohort study conducted in Brazil has indicated that systemic treatment does not exacerbate COVID-19 in patients with psoriasis.51 Furthermore, surveys have revealed that the majority of patients feel they have received effective treatment to a great extent (67.0%) and overall feel safe with their treatment (76.4%).52 Existing data have demonstrated that in patients with moderate to severe psoriasis, non-biologic systemic treatments are associated with a higher risk of hospitalization due to COVID-19 than biologic treatments.53 Meanwhile, carotid atherosclerosis as a risk factor for COVID-19, TNF-α, IL-1β, and IL-17 play an important role in promoting the development of atherosclerosis.54 Such inflammatory factor inhibitors can be considered to be put into the treatment of psoriasis patients with combined COVID-19. It should not be concluded that TNF-α inhibitors are necessarily safer than biologic agents targeting IL-17 and IL-23 in terms of the risk of respiratory tract and novel coronavirus infections.55 Furthermore, concerning COVID-19 vaccine administration, the current main types available are inactivated vaccines and recombinant protein vaccines. Patients with psoriasis who are using biologic agents can be vaccinated while on treatment, or they can choose to temporarily pause the use of biologic agents before vaccination based on their individual immune status. For instance, in the case of TNF-α inhibitors, it is recommended to discontinue the medication for 14–28 days prior to vaccination and resume treatment 7–14 days after vaccine administration.56 On the other hand, there is no need to discontinue IL-17 inhibitors during vaccine administration. Although there are no obvious contraindications to the use of inactivated vaccines, the risk-benefit ratio of maintaining immunosuppressive therapy must be evaluated prior to vaccine administration.57
Conclusion
Psoriasis, as a chronic disease, remains incurable to date due to its complex multifactorial etiology. It is prone to concurrent or comorbid diseases. Early detection, timely treatment, and appropriate medication are crucial in improving the prognosis and enhancing the quality of life for patients with psoriasis and comorbid diseases. Previous treatment strategies primarily involved the use of oral administration of chemical drugs, topical therapies, and phototherapy. However, these approaches were often accompanied by various adverse effects and inadequate efficacy, thereby limiting patient satisfaction. With the further advancement in understanding the mechanisms underlying psoriasis, the development and utilization of biologic agents have significantly improved the treatment landscape. As an emerging therapeutic approach, this study aims to summarize the current clinical efficacy of biologic agents in treating complications and comorbidities associated with psoriasis through a series of literature searches and analyses. The objective is to provide guidance for clinical drug selection in patients with such conditions and serve as a reference for the development and utilization of biologic agents. Currently, the main targets of biologic agents for psoriasis, both domestically and internationally, are TNF-α, IL-17A, and IL-23 (detailed summary information can be found in Table 1). The efficacy of these targeted therapies in treating psoriasis and its comorbidities has been confirmed (Table 2). In general, there is very little talk about the anti IL-23 p19 class. But, Some studies have found that selective IL-23p19 inhibition is an attractive therapeutic approach and may offer important advantages in terms of efficacy and safety. Several IL-23p19 inhibitors are currently being developed for the treatment of psoriasis, such as tildrakizumab, guselkumab, and risankizumab. Although clinical data on risankizumab is still scarce, it has shown characteristics that signify a major advance in the treatment of this disease, offering comparable or higher efficacy than IL-17 inhibitors.58 However, it is important to note that the biologic agents also carry a risk of causing related infections during their use. Therefore, routine screening for tuberculosis, hepatitis, anti-nuclear antibody (ANA), HIV, and other infections should be conducted before their administration. It is also necessary to select biologic agents appropriately based on the specific comorbidities present. Close monitoring of the conditions of patients is also required during the use of biologic agents. For future research and application of biologic agents, several aspects should be considered. Firstly, as time progresses, the long-term efficacy and side effects of biologic agents can be effectively evaluated, leading to potential improvements of existing agents. Secondly, by studying the common pathways between psoriasis and its comorbidities, more targeted drugs can be developed, aiming for individualized treatments by precisely targeting specific factors and minimizing toxicity and side effects. Thirdly, with continuous investment in research and development, more signaling pathways can be uncovered. The advancement can lead to the identification of more specific targets with reduced side effects and the availability of biologic agents that are better tailored for individual patients. This continuous effort can provide safer and more effective biologic treatment options for patients with psoriasis.
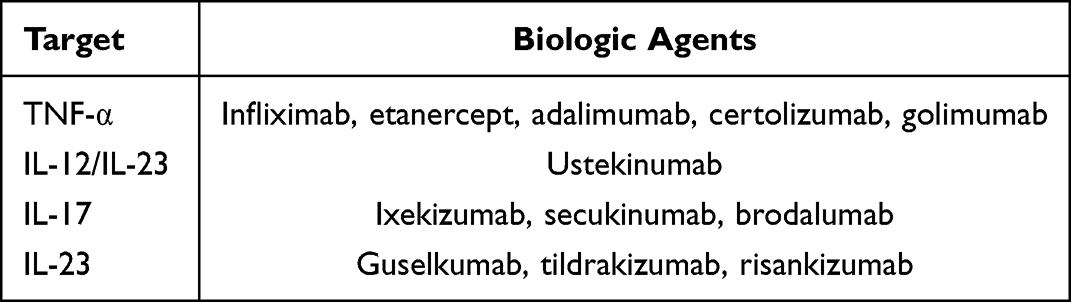 |
Table 1 Biologic Agents Used for the Treatment of Psoriasis Domestically and Internationally |
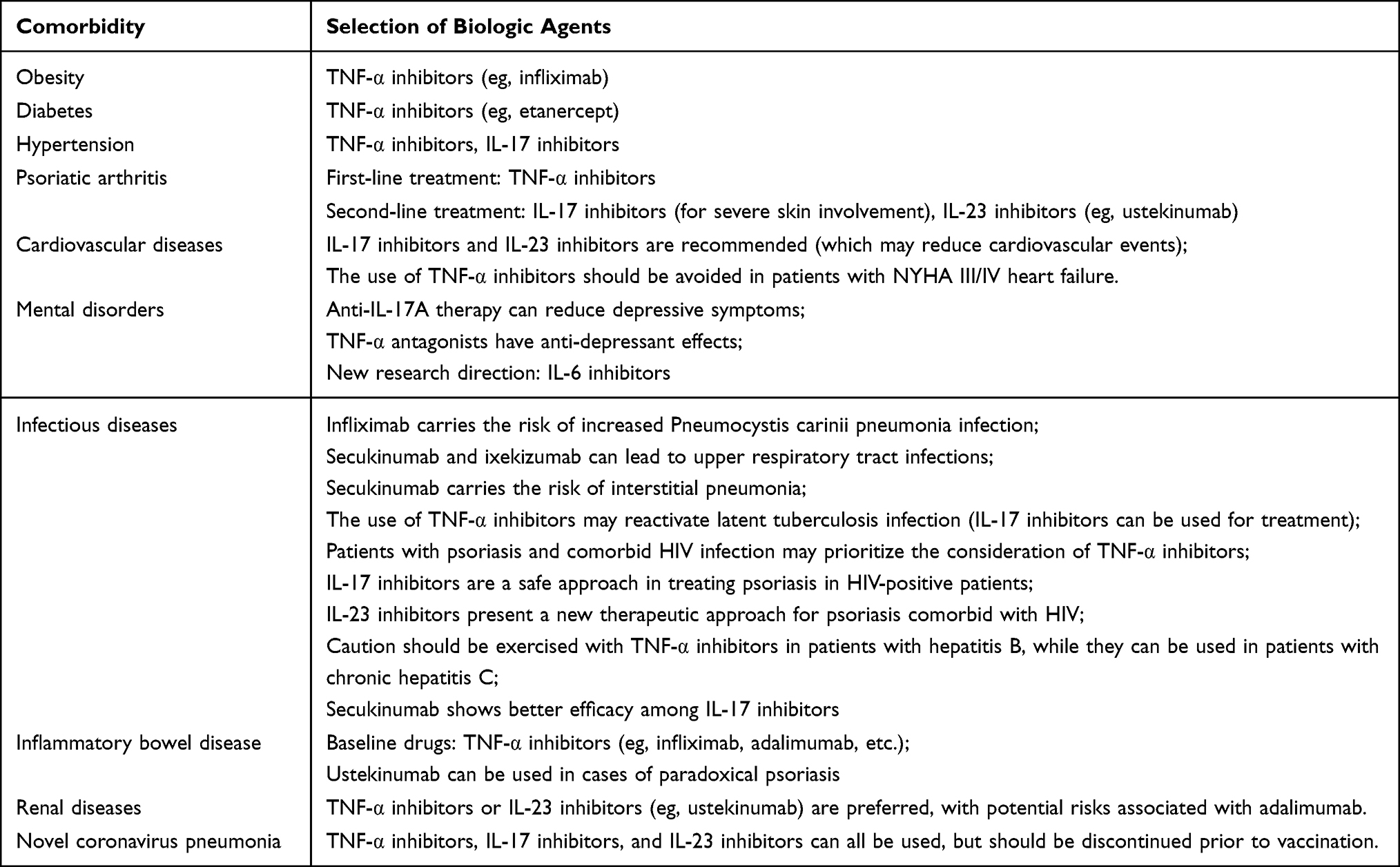 |
Table 2 Biologic Agents Used for the Treatment of the Comorbidities of Psoriasis |
Acknowledgments
We gratefully thank research assistant Yu LV and Yu DENG, Dr.Ming YAO and Dr.Lin WANG for their contributions to this study.
Funding
This work was supported by the Fund of Young Scientific and Technological Talents Support Project by Jiangsu Association for Science and Technology (No. TJ-2022-097), People’s Republic of China.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Gelfand JM, Mehta NN. Aortic valve stenosis: a new cardio-vascular comorbidity of psoriasis? Eur Heart J. 2015;36(32):2134–2135. doi:10.1093/eurheartj/ehv271
2. Kim M, Han K, Lee J. Bodyweight variability and the risk of psoriasis: A nationwide population-based cohort study. J Eur Acad Dermatol. 2020;34(5):1019–1025. doi:10.1111/jdv.16099
3. Brembilla NC, Boehncke WH. Dermal adipocytes’ claim forfame in psoriasis. Exp Dermatol. 2017;26(5):392–393. doi:10.1111/exd.13074
4. Puig L. Obesity and psoriasis: body weight and body mass index influence the response to biological treatment. J Eur Acad Dermatol Venereol. 2011;25(9):1007–1011. PMID: 21492252. doi:10.1111/j.1468-3083.2011.04065.x
5. Podoswa-Ozerkovsky N, maya-Guerra M, Barba-Gómez JF, et al. Expert recommendations for biological treatment in patients with psoriasis. Gac Med Mex. 2020;156(5):446–453. doi:10.24875/GMM.M20000441
6. Zafiriou E, Daponte A, Siokas V, et al. Depression and obesity in patients with psoriasis and psoriatic arthritis: is IL-17-mediated immune dysregulation the connecting link? Front Immunol. 2021;12:699848. doi:10.3389/fimmu.2021.699848
7. Kong ZL, Jiao TT, Zhang FR. Analysis of factors associated with psoriasis comorbid with type 2 diabetes. Chin J Lepros Skin Dis. 2021;37(2):80–84.
8. Gelfand J, Wan M. Psoriasis: A novel risk factor for type2 diabetes. Lancet Diabetes Endo. 2018;6(12):919–921. doi:10.1016/S2213-8587(18)30127-X
9. Cai J, Cui L, Wang Y, et al. Cardiometabolic comorbidities in patients with psoriasis: focusing on risk, biological therapy, and pathogenesis. Front Pharmacol. 2021;12:774808. doi:10.3389/fphar.2021.774808
10. Mikhaylov D, Hashim PW, Nektalova T, et al. Systemic psoriasis therapies and comorbid disease in patients with psoriasis: a review of potential risks and benefits. J Clin Aesthet Dermatol. 2019;12:46–54.
11. Pirowska M, Obtulowicz A, Lipko-Godlewska S, et al. The level of proinflammatory cytokines: interleukins 12,23,17 and tumor necrosis factor alpha in patients with metabolic syndrome accompanying severe psoriasis and psoriatic arthritis. Postepy Dermatol Alergol. 2018;35(4):360–366. doi:10.5114/ada.2018.77665
12. Warren R, Blauvelt A, Bagel J, et al. Bimekizumab versus Adalimumab in plaque psoriasis. New Engl J Med. 2021;385(2):130–141. doi:10.1056/NEJMoa2102388
13. Sieper J, Poddubnyy D, Miossec P. The IL-23–IL-17 pathway as a therapeutic target in axial spondyloarthritis. Nat Rev Rheumatol. 2019;15(12):747–757. doi:10.1038/s41584-019-0294-7
14. Gossec L, Baraliakos X, Kerschbaumer A, et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann Rheum Dis. 2020;79(6):700–712. doi:10.1136/annrheumdis-2020-217159
15. Poddubnyy D, Jadon DR, Bosch FVD, et al. Axial involvement in psoriatic arthritis: an update for rheumatologists. Semin Arthritis Rheumatism. 2021;51(4):880–887. doi:10.1016/j.semarthrit.2021.06.006
16. Hjuler KF, Bøttcher M, Vestergaard C, et al. Association between changes in coronary artery disease progression and treatment with biologic agents for severe psoriasis. JAMA dermatol. 2016;152(10):1173–1174. doi:10.1001/jamadermatol.2016.1984
17. Wu JJ, Joshi AA, Reddy SP, et al. Anti-inflammatory therapy with tumour necrosis factor inhibitors is associated with reduced risk of major adverse cardiovascular events in psoriasis. J Eur Acad Dermatol Venereol. 2018;32:1320–1326. doi:10.1111/jdv.14951
18. Wu JJ, Guérin A, Sundaram M, Dea K, Cloutier M, Mulani P. Cardiovascular event risk assessment in psoriasis patients treated with tumor necrosis factor-α inhibitors versus methotrexate. J Am Acad Dermatol. 2017;76:81–90. doi:10.1016/j.jaad.2016.07.042
19. Gelfand JM, Shin DB, Alavi A, et al. A Phase IV, randomized, double-blind, placebo-controlled crossover study of the effects of ustekinumab on vascular inflammation in psoriasis (the VIP-U Trial). Invest Dermatol. 2020;140:85–93. doi:10.1016/j.jid.2019.07.679
20. Thatiparthi A, Martin A, Liu J, et al. Biologic treatment algorithms for moderate-to-severe psoriasis with comorbid conditions and special populations: a review. Am J Clin Dermatol. 2021;22:425–442. doi:10.1007/s40257-021-00603-w
21. Wu JJ, Penfold RB, Primatesta P, et al. The risk of depression, suicidal ideation, and suicide attempt in patients with psoriasis, psoriatic arthritis, or ankylosing spondylitis. J Eur Acad Dermatol Venereol Jeadv. 2017;31:1168–1175. doi:10.1111/jdv.14175
22. Fleming P, Roubille C, Richer V, et al. Effect of biologics on depressive symptoms in patients with psoriasis: a systematic review. J Eur Acad Dermatol Venereol. 2015;29:1063–1070. doi:10.1111/jdv.12909
23. Nadeem A, Ahmad SF, Al-Harbi NO, et al. IL-17A causes depression-like symptoms via NFκB and p38MAPK signaling pathways in mice: implications for psoriasis associated depression. Cytokine. 2017;97:14–24. doi:10.1016/j.cyto.2017.05.018
24. Lebowitz E, Lebwohl M. Review of suicide and depression in psoriasis and management of suicide warnings in patients treated with psoriasis drugs. Skin J Cutan Med. 2019;3:72–81. doi:10.25251/skin.3.2.39
25. Hölsken S, Krefting F, Schedlowski M, Sondermann W. Common fundamentals of psoriasis and depression. Acta Derm Venereol. 2021;101(11):adv00609. doi:10.2340/actadv.v101.565
26. Takeshita J, Shin DB, Ogdie A, et al. 191 Increased risk of serious infection among patients with psoriasis: a population-based cohort study in the United Kingdom. J Invest Dermatol. 2016;136(5):S34. doi:10.1016/j.jid.2016.02.219
27. Podlipnik S, de la Mora L, Alsina M, et al. Pneumocystis jirovecii pneumonia in a patient with pustular psoriasis with an IL −36 RN deficiency treated with infliximab: case report and review of the literature. Australas J Dermatol. 2017;58(2):e44–e47. doi:10.1111/ajd.12489
28. Hayashi M, Igarashi A, Okamura K, et al. Paradoxical exacerbation of latent interstitial pneumonia by secukinumab in a patient with psoriasis vulgaris. Br J Dermatol. 2019;180:684–685. doi:10.1111/bjd.17424
29. Kammüller M, Tsai TF, Griffiths CE, et al. Inhibition of IL–17A by secukinumab shows no evidence of increased My-cobacterium tuberculosis infections. Clin Transl Immunol. 2017;6(8):e152. doi:10.1038/cti.2017.34
30. Bardazzi F, Magnano M, Campanati A, et al. Biologic therapies in HIV-infected patients with psoriasis: an Italian experience. Acta Derm Venereol. 2017;97(8):989–990. doi:10.2340/00015555-2698
31. Nakamura M, Abrouk M, Farahnik B, et al. Psoriasis treatment in HIV–positive patients: a systematic review of systemic immunosuppressive therapies. Cutis. 2018;101(1):38.
32. Pangilinan MCG, Sermswan P, Asawanonda P. Use of Anti-IL-17 monoclonal antibodies in HIV patients with erythrodermic psoriasis. Case Rep Dermatol. 2020;12(2):132–137. doi:10.1159/000508781
33. Kaushik SB, Lebwohl MG. Psoriasis: which therapy for which patient: focus on special populations and chronic infections. J Am Acad Dermatol. 2019;80(1):43–53. doi:10.1016/j.jaad.2018.06.056
34. Montes-Torres A, Aparicio G, Rivera R, et al. Safety and effectiveness of conventional systemic therapy and biological drugs in patients with moderate to severe psoriasis and HIV infection: a retrospective multicenter study. Dermatol Treat. 2019;30(5):461–465. doi:10.1080/09546634.2018.1535690
35. Rob F, Rozsypal H. Successful treatment of psoriasis with risankizumab in an HIV positive patient with sexually transmitted infection comorbidities. Dermatol Ther. 2022;35(3):e15277. doi:10.1111/dth.15277
36. Bonifati C, Lora V, Graceffa D, et al. Management of psoriasis patients with hepatitis B or hepatitis C virus infection. World Gastroenterol. 2016;22(28):6444–6455.
37. Snast I, Atzmony L, Braun M, et al. Risk for hepatitis B and C virus reactivation in patients with psoriasis on biologic therapies: a retrospective cohort study and systematic review of the literature (Article). J Am Acad Dermatol. 2017;77(1):
38. Zhao XQ, Zhu WJ, Mu Y, Xu M, Xia JX. Treatment of two cases of psoriasis comorbid with chronic hepatitis B using secukinumab [J/OL]. Chin J Dermatology Venereol. 2023;158:236–242. doi:10.23736/S2784-8671.23.07499-6
39. Freuer D, Linseisen J, Meisinger C. Association between inflammatory bowel disease and both psoriasis and psoriatic arthritis: a bidirectional 2-sample mendelian randomization study. JAMA Dermatol. 2022;158(11):1262–1268. doi:10.1001/jamadermatol.2022.3682
40. Mylonas A, Conrad C. Psoriasis: classical vs.paradoxical. The yin-yang of TNF and type I interferon. Front Immunol. 2018;9:2746. doi:10.3389/fimmu.2018.02746
41. Revankar R, Patel H, Rojas M, Walsh S, McGee JS. Systematic review of TNFα-induced paradoxical psoriasis: treatment outcomes of switching to alternative biologic therapies in inflammatory bowel disease patients. J Dermatolog Treat. 2022;18:1–4.
42. Al-Bawardy B, Shivashankar R, Proctor DD. Novel and emerging therapies for inflammatory bowel disease. Front Pharmacol. 2021;12:651415. doi:10.3389/fphar.2021.651415
43. Fauny M, Moulin D, D′Amico F, et al. Paradoxical gastrointestinal effects of interleukin-17 blockers. Ann Rheum Dis. 2020;79(9):1132–1138. doi:10.1136/annrheumdis-2020-217927
44. Spencer elizabeth A, Dolinger Michael T, Dubinsky Marla CA. Single-center experience with dupilumab for atopic or psoriasiform dermatitis in patients with inflammatory bowel disease. Dig Dis Sci. 2022;68:1121–1124. doi:10.1007/s10620-022-07684-5
45. Liu KL, Tsai WC, Tu HP, Lee CH. Statin use and the risk of chronic kidney disease in patients with psoriasis: a nationwide cohort study in Taiwan. PLoS One. 2020;15:8.
46. Grewal SK, Wan J, Denburg MR, Shin DB, Takeshita J, Gelfand JM. The risk of IgA nephropathy and glomerular disease in patients with psoriasis: a population-based cohort study. Br J Dermatol. 2017;176(5):1366–1369. doi:10.1111/bjd.14961
47. Ren F, Zhang M, Zhang C, Sang H. Psoriasis-like inflammation induced renal dysfunction through the TLR/NF-κB signal pathway. Biomed Res Int. 2020;2020:3535264. doi:10.1155/2020/3535264
48. Amatore F, Villani AP, Tauber M, et al. French guidelines on the use of systemic treatments for moderate-to-severe psoriasis in adults. J Eur Acad Dermatol Venereol. 2019;33(3):464–483. doi:10.1111/jdv.15340
49. Liu T, Fan XH, Zeng YP, Qin Y, Ai SX, Li XM. Adalimumab-induced IgA nephropathy and erythroderma in a patient with psoriasis. J Adverse Drug React. 2022;24(6):332–334.
50. Larquey M, Girard C, Sbidian E, Richard MA, Aubin F, Schmutz JL. Efficacy of biologics in psoriasis patients under hemodialysis. Eur J Dermatol. 2017;27:531–533. doi:10.1684/ejd.2017.3064
51. Lima XT, Cueva MA, Lopes EM, Alora MB. Severe Covid-19 outcomes in patients with psoriasis. J Eur Acad Dermatol Venereol. 2020;34(12):e776–e8.
52. Loft ND, Halling AS, Iversen L, et al. Concerns related to the coronavirus disease 2019 pandemic in adult patients with atopic dermatitis and psoriasis treated with systemic immunomodulatory therapy: A Danish questionnaire survey. J Eur Acad Dermatol Venereol. 2020;34(12):e773–e6. doi:10.1111/jdv.16863
53. Mahil SK, Dand N, Mason KJ, et al. Factors associated with adverse Covid-19 outcomes in patients with psoriasis-insights from a global registry-based. Study J Allergy Clin Immunol. 2021;147(1):60–71. doi:10.1016/j.jaci.2020.10.007
54. Han YM. Aziguli·abudureheman. Study on the relationship between serum TNF-α, IL-1β, IL-17 levels and atherosclerosis in patients with rheumatoid arthritis. Int J Lab Med. 2018;39(03):371–373.
55. Syed MN, Shah M, Shin DB, Wan MT, Winthrop KL, Gelfand JM. Effect of anti-tumor necrosis factor therapy on the risk of respiratory tract infections and related symptoms in patients with psoriasis-A meta-estimate of pivotal phase 3 trials relevant to decision making during the covid-19. Pandemic J Am Acad Dermatol. 2021;84(1):161–163. doi:10.1016/j.jaad.2020.08.095
56. Menter A, Strober BE, Kaplan DH, et al. Joint AAD–NPF guidelines of care for the management and treatment of psoriasis with biologics. J Am Acad Dermatol. 2019;80(4):1029–1072. doi:10.1016/j.jaad.2018.11.057
57. Diotallevi F, Campanati A, Radi G, et al. Vaccination against sars-Cov-2 and psoriasis: the three things every dermatologist should know. J Eur Acad Dermatol Venereol. 2021;35(7):e428–e30. doi:10.1111/jdv.17256
58. Torres T. Selective Interleukin-23 p19 inhibition: another game changer in psoriasis? Focus on risankizumab. Drugs. 2017;77(14):1493–1503. doi:10.1007/s40265-017-0794-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.