Back to Journals » Cancer Management and Research » Volume 17

Advanced Reconstructive Techniques: Mitigating Low Anterior Resection Syndrome Post-TME in Low Rectal Cancer – A Single-Center Randomised Controlled Study
Authors Al-Kubati WR ![]()
Received 10 May 2025
Accepted for publication 22 October 2025
Published 27 October 2025 Volume 2025:17 Pages 2469—2485
DOI https://doi.org/10.2147/CMAR.S498077
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sanjeev K. Srivastava
Waheeb Radman Al-Kubati1– 3
1Department of Surgery, 21st September University, Sana’a, Yemen; 2Department of Surgery, Althowra Modern General Hospital, Sana’a, Yemen; 3Department of Physiology, Sana’a University, Sana’a, Yemen
Correspondence: Waheeb Radman Al-Kubati, Email [email protected]
Background: Low Anterior Resection Syndrome (LARS) is a debilitating complication of sphincter-preserving surgeries, particularly after Total Mesorectal Excision (TME) for very low rectal cancer. LARS adversely impacts bowel function and quality of life, highlighting the need for effective preventive strategies.
Objective: This study evaluates advanced reconstructive techniques, including taeniectomy pouch (TP), transverse coloplasty (TCP), colonic J-pouch (CJP), smooth muscle plasty (SMP), and greater omentum transplantation (GOT), in reducing LARS incidence and severity.
Methods: This was a single-center randomized controlled trial (RCT) conducted between April 2018 and March 2024, involving 88 patients undergoing total mesorectal excision (TME) for very low rectal cancer. The trial was registered locally at our tertiary referral center. Patients were randomized in a 1:1 ratio to either the control group (straight coloanal anastomosis) or the test group (advanced reconstructive techniques: transverse coloplasty, colonic J-pouch, taeniectomy pouch, or smooth muscle plasty, with or without greater omentum transplantation). Eligible patients had histologically confirmed, well- or moderately-differentiated adenocarcinoma located 1– 6 cm from the anal verge. Propensity score adjustment was applied during analysis to minimize residual confounding. The primary endpoint was the incidence of major Low Anterior Resection Syndrome (LARS; score > 30), assessed by validated questionnaires at 6 weeks, 3, 6, 12, and 24 months postoperatively. Secondary outcomes included stool frequency, continence recovery, and quality-of-life scores. Trial registration: [AMG-HOSP-RCT-2018-003].
Results: At six weeks, major LARS occurred in 10% of the test group (95% CI: 4– 23%) versus 80% of controls (95% CI: 68– 88%) (P < 0.001). Mild LARS (score < 20) was observed in 80% of test patients compared to 5% of controls. Stool frequency improved from 4.5/day to 2.7/day within 12 months in the test group, consistently outperforming controls. Major incontinence was recorded in 10% (95% CI: 4– 23%) of test patients versus 80% (95% CI: 68– 88%) of controls. GOT combined with TP or SMP achieved the most favorable outcomes, with faster recovery of anal function and greater LARS score improvement at six weeks post-surgery. Pairwise comparisons confirmed significantly lower stool frequency in both test subgroups at all follow-up points (mean differences − 1.8 to − 0.4 without GOT; − 2.2 to − 0.6 with GOT; all P< 0.0056). Logistic regression identified test group allocation and GOT as strong independent predictors of reduced major LARS, while prior CRT was the most significant risk factor.
Conclusion: GOT and other advanced techniques effectively mitigate LARS severity, resulting in enhanced postoperative quality of life. This study demonstrates the potential benefits of neorectal reservoir techniques and GOT in enhancing functional outcomes after TME for very low rectal cancer. The findings provide promising evidence supporting their role in LARS management; however, broader adoption requires validation in larger, multicenter trials with longer follow-up.
Plain Language Summary: Patients with very low rectal cancer often undergo total mesorectal excision (TME), a surgery that can lead to a common complication known as Low Anterior Resection Syndrome (LARS). LARS includes problems like frequent bowel movements, urgency, and difficulty controlling stools, which can significantly affect quality of life.
This study explored whether using advanced reconstructive techniques during surgery could help reduce these symptoms. These techniques included creating different types of internal pouches—such as a taeniectomy pouch, J-pouch, or transverse coloplasty—as well as using smooth muscle plasty and transplanting the body’s own omentum (a fatty tissue layer from the abdomen) to support healing and function.
The results suggest that combining these approaches may improve bowel control and recovery after TME, offering better long-term outcomes for patients.
Keywords: low anterior resection syndrome, TME, advanced reconstructive techniques, taeniectomy pouch, J-pouch, transverse coloplasty, smooth muscle plasty, omentum transplantation
Introduction
Low Anterior Resection Syndrome (LARS) is a challenging complication commonly occurring after Total Mesorectal Excision (TME) for very low rectal cancer. It encompasses a spectrum of bowel dysfunctions, including fecal incontinence, urgency, frequent and fragmented bowel movements, and evacuation difficulties, all of which significantly impair patients’ quality of life. Despite advancements in sphincter-sparing techniques, LARS remains prevalent, notably in patients who have undergone preoperative radiotherapy.
The pathophysiology of LARS is multifactorial, involving anal sphincter dysfunction, neorectal reservoir insufficiency, and colonic dysmotility. Traditional surgical approaches, such as straight coloanal anastomosis, are associated with higher LARS incidence due to the absence of a functional neorectal reservoir.
This study evaluates the effectiveness of advanced reconstructive techniques, including greater omentum transplantation (GOT), a promising approach aimed at improving neorectal function and reducing LARS. These techniques target both mechanical and functional aspects of bowel dysfunction, providing a comprehensive strategy to enhance postoperative outcomes.
LARS was assessed using the validated LARS scoring tool, which categorizes severity as no/mild/moderate/major based on total score thresholds. Thresholds were selected according to widely accepted guidelines to reliably stratify patients according to symptom severity and functional impairment.
This research seeks to optimize functional and quality-of-life outcomes for patients undergoing TME for very low rectal cancer, addressing a critical gap in the literature.
Methods
Study Design and Patient Selection
This was a single-center randomized controlled trial (RCT), registered locally at our tertiary care institution. Participants were randomized in a 1:1 ratio using a computer-generated sequence, with allocation concealment ensured by sealed opaque envelopes. Although randomization achieved well-balanced groups, propensity score adjustment was additionally applied during analysis to account for potential residual confounders, including baseline stool frequency and prior chemoradiotherapy (CRT).
A total of 88 patients undergoing rectal resection with anastomosis between April 2018 and March 2024 were enrolled. Patients were stratified into two groups:
- Control Group: Standard straight coloanal anastomosis without greater omentum transplantation (GOT) (n = 44).
- Test Group: Advanced reconstructive techniques—transverse coloplasty (TCP), colonic J-pouch (CJP), taeniectomy pouch (TP), or smooth muscle plasty (SMP)—with or without GOT (n = 44).
Subgroup Distribution
Within the Test Group, the distribution of procedures was: TCP (n = 16), CJP (n = 16), TP (n = 4), and SMP (n = 8). Each procedure was performed in equal numbers with and without GOT (eg, TCP with GOT, n = 8; TCP without GOT, n = 8). Given the very small number of patients in the TP subgroup (n = 2 with GOT, n = 2 without), findings from this subgroup were considered exploratory and not powered for definitive interpretation.
Inclusion and Exclusion Criteria
Inclusion criteria: Adults ≥18 years, histologically confirmed rectal adenocarcinoma, clinical stage T1–T3, well- or moderately-differentiated tumors, and distal tumor margins between 1–6 cm. All patients underwent R0 resection.
Exclusion criteria: T4 tumors, fixed or metastatic disease, familial adenomatous polyposis (FAP), inflammatory bowel disease (IBD), or sphincter involvement.
Interventions
- Control Group: Straight coloanal anastomosis.
- Test Group: Reconstructive procedures (TCP, CJP, TP, SMP), performed with or without GOT.
Follow-Up
Follow-up compliance was 100% at all planned intervals: 6 weeks, 3 months, 6 months, 12 months, and 24 months.
Outcomes
- Primary Outcome: Severity of Low Anterior Resection Syndrome (LARS), measured with the validated LARS questionnaire and categorized according to standard scoring thresholds.
- Secondary Outcomes: Stool frequency, continence recovery rates, and overall functional adaptation.
Blinding Procedures
Blinding of surgeons was not feasible due to the surgical nature of interventions. However, functional outcome assessments were conducted by independent research staff blinded to group allocation. Statistical analyses were also performed by blinded statisticians to reduce measurement bias.
Statistical Analysis
Primary group comparisons were performed using independent t-tests with Bonferroni correction (α = 0.0056). Paired t-tests were applied for within-technique comparisons of procedures with versus without GOT. Longitudinal changes in stool frequency and LARS scores were evaluated using linear mixed-effects models, adjusted for repeated measures, baseline stool frequency, age, and prior CRT.
Continence recovery was analyzed using Kaplan–Meier survival curves with Log rank tests.
Cox Proportional Hazards Regression
The Cox proportional hazards model was used to evaluate predictors of continence recovery. The hazard function is expressed as:
h(t|X) = h0(t) · exp(β₁X₁ + β2X2 + … + βnXn)
Where h(t|X) is the hazard at time t, h0(t) is the baseline hazard, and β are the regression coefficients for covariates X. Proportional hazards assumptions were tested using Schoenfeld residuals.
Logistic Regression for Major LARS
Logistic regression models were used to evaluate predictors of major Low Anterior Resection Syndrome (LARS). Results were expressed as odds ratios (OR) with 95% confidence intervals (CI). The general form of the logistic regression model is:
logit(p) = ln(p / (1 − p)) = β0 + β₁X₁ + β2X2 + … + βnXn
Where p is the probability of the event (major LARS), β0 is the intercept, and β are regression coefficients for covariates X. Model fit was assessed using standard goodness-of-fit statistics.
Assumptions of normality (Shapiro–Wilk test) and variance homogeneity (Levene’s test) were verified. Analyses were conducted using SPSS version 23. A two-sided P-value <0.05 was considered statistically significant.
Validation and Quality Control
All patient questionnaires were administered by trained staff to ensure consistency. Functional outcomes were corroborated by digital rectal examination and imaging studies to improve reliability and reduce subjectivity.
Results
Patient Characteristics
Table 1 summarizes baseline characteristics. The groups were well balanced across age, sex, tumor distance, CRT exposure, and surgical margins. Mean age was 47 ± 12 years in the test group versus 46 ± 13 in controls (P=0.72; SMD=0.08). Both groups had equal sex distribution (22 male, 22 female; P=1.0; SMD=0.00). Mean tumor distance was 2.5 cm in the test group and 2.4 cm in controls (P=0.88; SMD=0.06). CRT was given in 50% of both groups, and all achieved R0 resection, confirming complete tumor removal with negative histologic margins. These results confirm balance between groups at baseline.
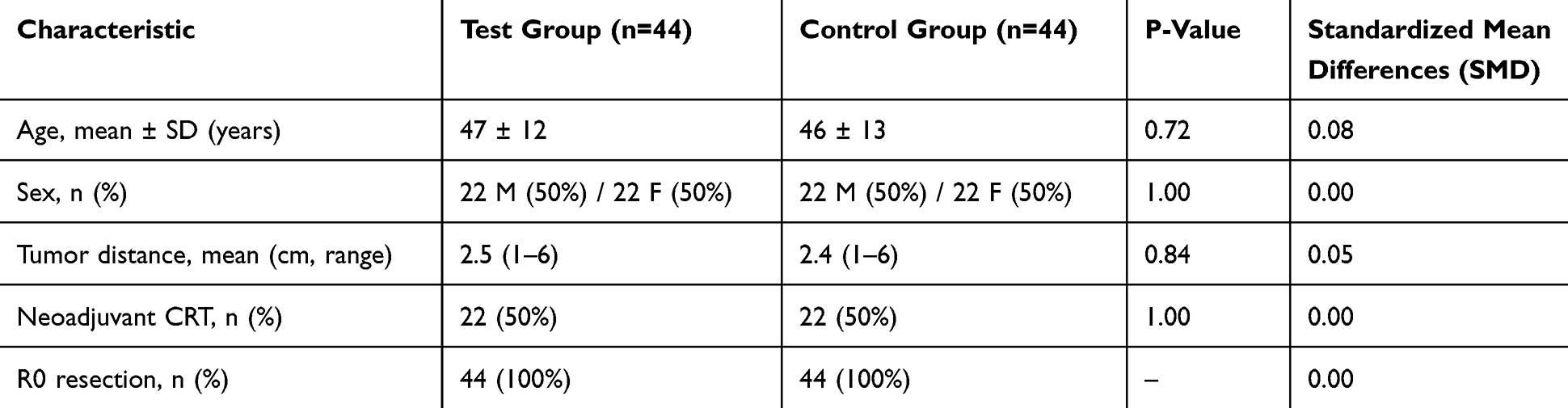 |
Table 1 Patient Characteristics |
Reconstruction Techniques
The distribution of reconstructive procedures is shown in Table 2. Equal numbers of Transverse Coloplasty (TCP) (n=16), Colonic J-Pouch (CJP) (n=16), Taeniectomy Pouch (TP) (n=4), and Smooth Muscle Plasty (SMP) (n=8) were performed, each half with and half without GOT. Given the small numbers in the TP subgroup (n=2 each arm), results for this subset are reported as exploratory.
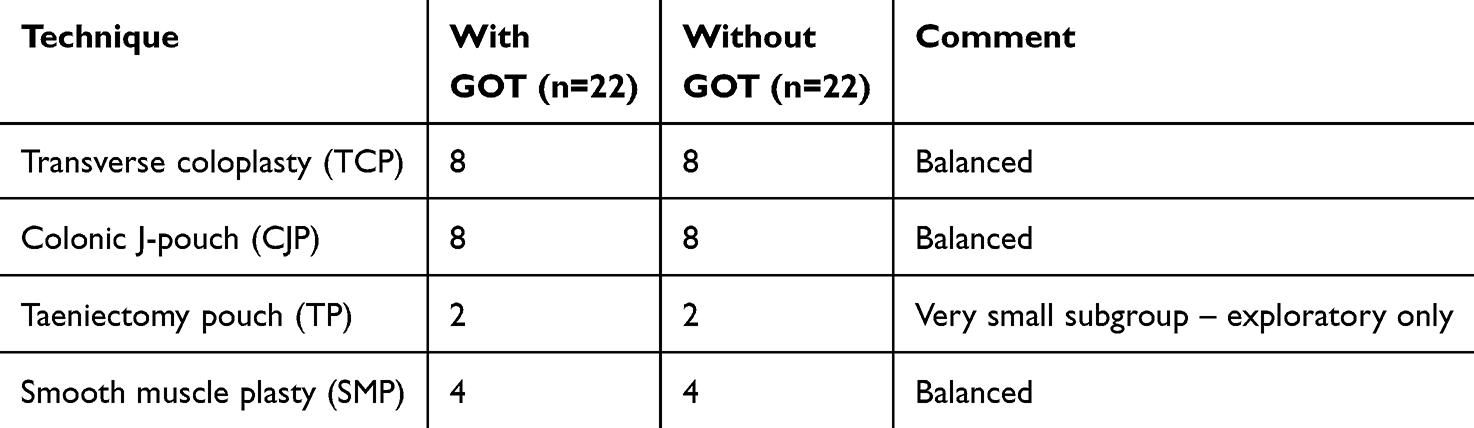 |
Table 2 Distribution of Reconstructive Techniques (Test Group Only) |
Continence Recovery
Kaplan–Meier analysis (Figure 1) revealed significantly faster recovery in the test group. At 6 months, continence was achieved in 40/44 patients (90.9%, 95% CI: 78.3–97.5) compared with 22/44 controls (50.0%, 95% CI: 34.6–65.4), P<0.001 (log-rank). By 12 months, continence was universal in the test group (100%, 95% CI: 92.0–100) and 79.5% in controls (35/44, 95% CI: 64.7–90.2). Cox regression (Table 3) demonstrated that GOT (HR=3.5, 95% CI: 2.0–6.0) and absence of prior CRT (HR=1.7, 95% CI: 1.1–2.5) were independent predictors of faster continence recovery.
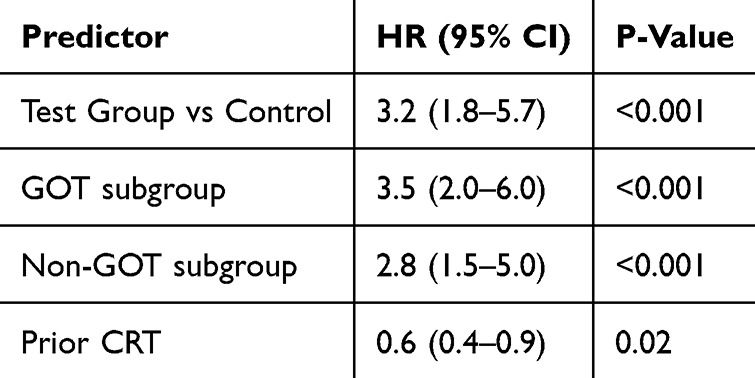 |
Table 3 Cox Regression for Continence Recovery |
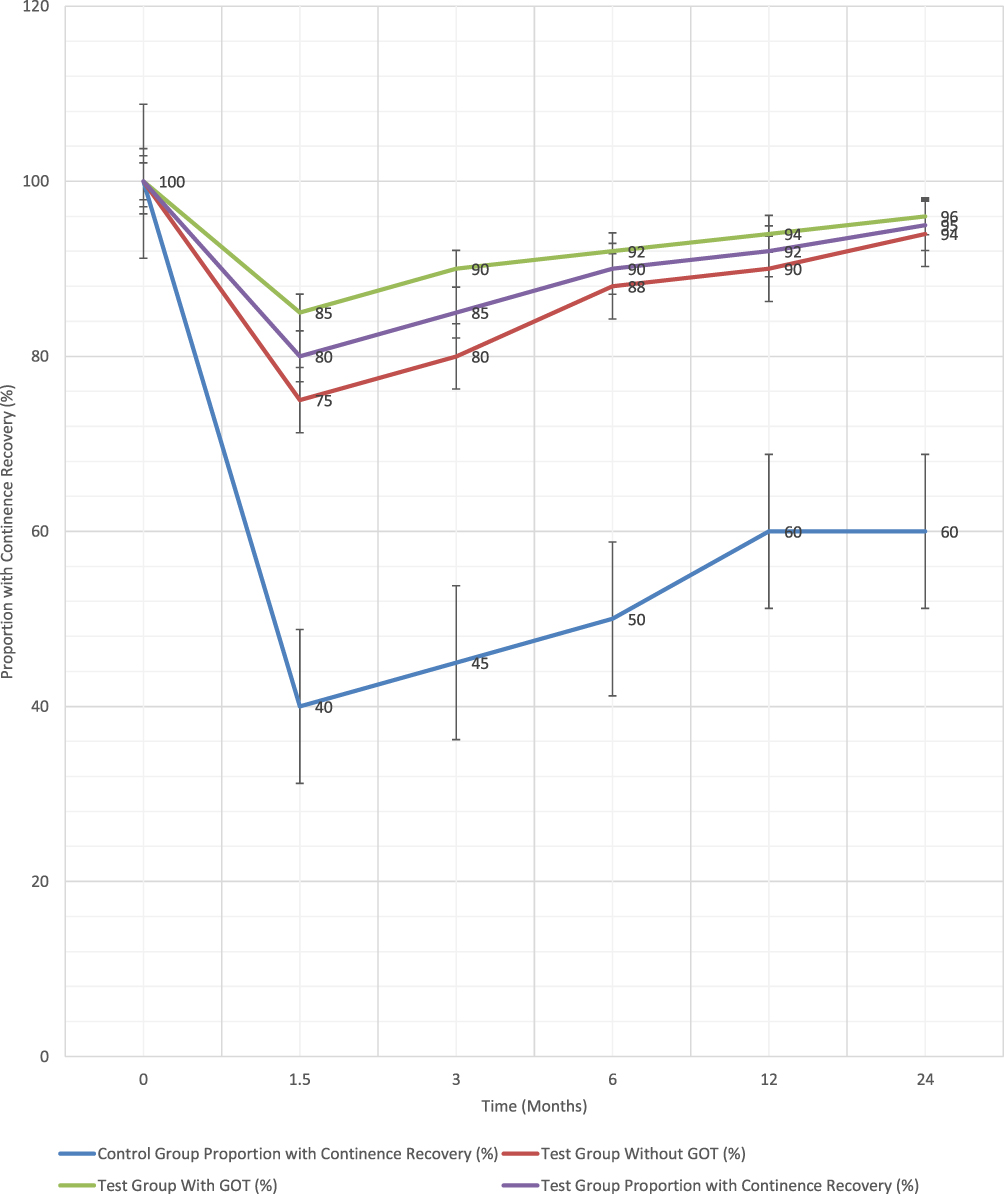 |
Figure 1 Kaplan-Meier Curve for Continence Recovery. |
Major LARS Incidence
The prevalence of major Low Anterior Resection Syndrome (LARS) was consistently lower in the test group across all time points (Figure 2). At 6 weeks, major LARS was present in 35/44 controls (79.5%, 95% CI: 64.7–90.2) but only 4/44 test patients (9.1%, 95% CI: 2.5–21.7), P<0.001. By 24 months, major LARS persisted in 18/44 controls (40.9%, 95% CI: 26.3–56.8) compared with just 2/44 test patients (4.5%, 95% CI: 0.6–15.5).
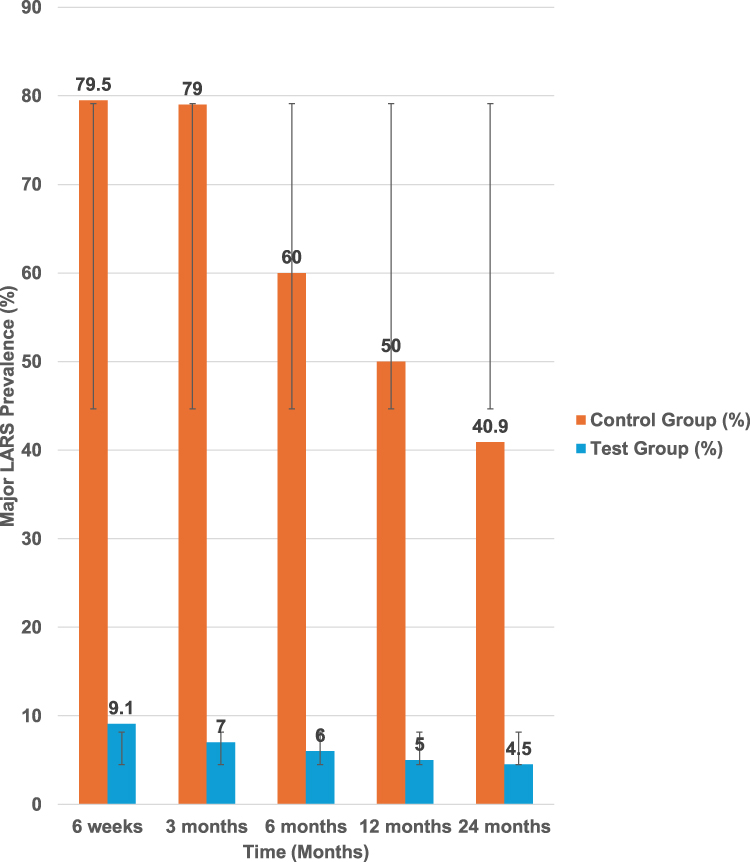 |
Figure 2 Major LARS Prevalence Over Time. |
Multivariable logistic regression (Table 4) confirmed the protective effect of the test interventions. Belonging to the test group reduced the odds of major LARS by 90% (OR=0.10, 95% CI: 0.04–0.30, P<0.001). Within the test group, GOT was the strongest independent predictor, lowering the odds of major LARS to 0.08 (95% CI: 0.03–0.25, P<0.001). Patients reconstructed without GOT also demonstrated reduced risk (OR=0.15, 95% CI: 0.06–0.40, P<0.001), though the effect was less pronounced.
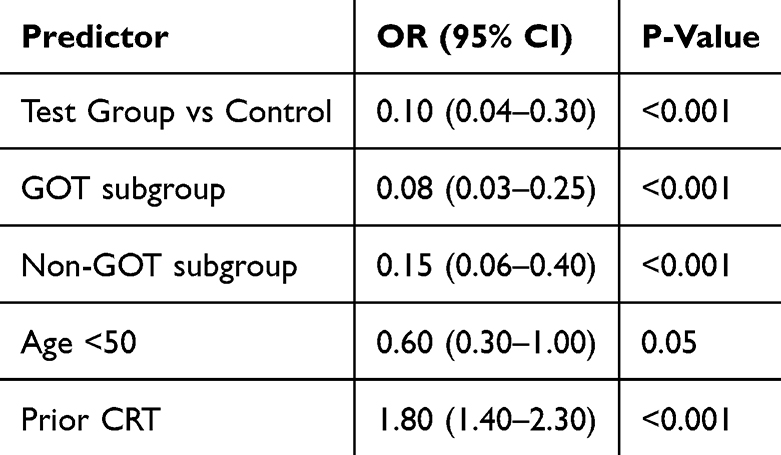 |
Table 4 Logistic Regression for Major LARS Risk |
Age below 50 years showed a borderline protective effect (OR=0.60, 95% CI: 0.30–1.00, P=0.05), while prior CRT significantly increased risk (OR=1.80, 95% CI: 1.40–2.30, P<0.001). These findings underscore the dual role of patient characteristics and reconstructive strategy in predicting long-term outcomes.
Stool Frequency Over Time
Mean stool frequencies are shown in Tables 5, 6 and Figure 3. At 1.5 months, controls averaged 4.8/day (SD 0.8), versus 2.8/day (SD 0.5) in GOT patients (mean difference −2.0, 95% CI: −2.4 to −1.6). At 3 months, the difference remained −1.9 (95% CI: −2.3 to −1.5). By 6 months, the gap had narrowed but persisted (−1.2, 95% CI: −1.5 to −0.9). At 24 months, stool frequency averaged 3.0/day in controls compared with 2.4/day in the GOT group (mean difference −0.6, 95% CI: −0.9 to −0.3, P=0.001).
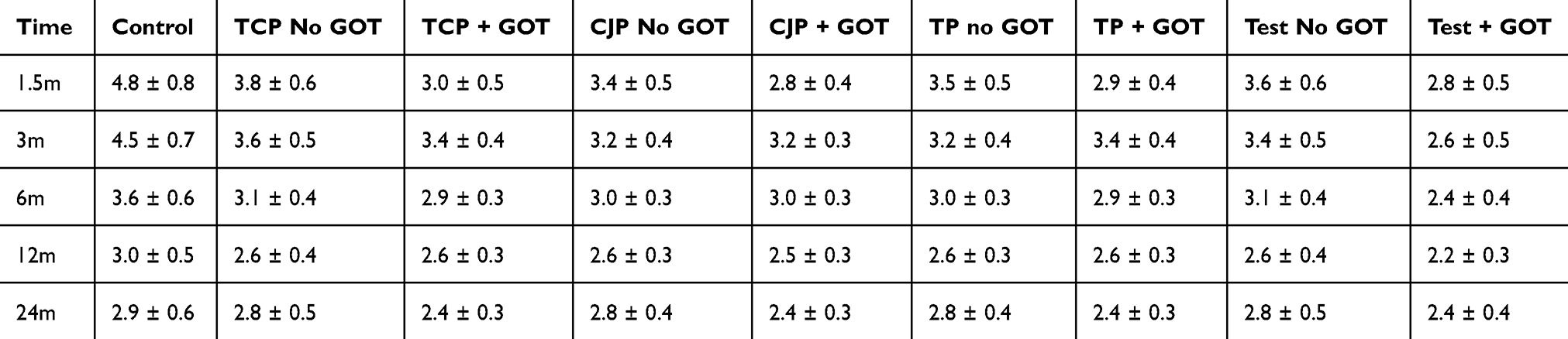 |
Table 5 Stool Frequency Over Time (Mean ± SD) |
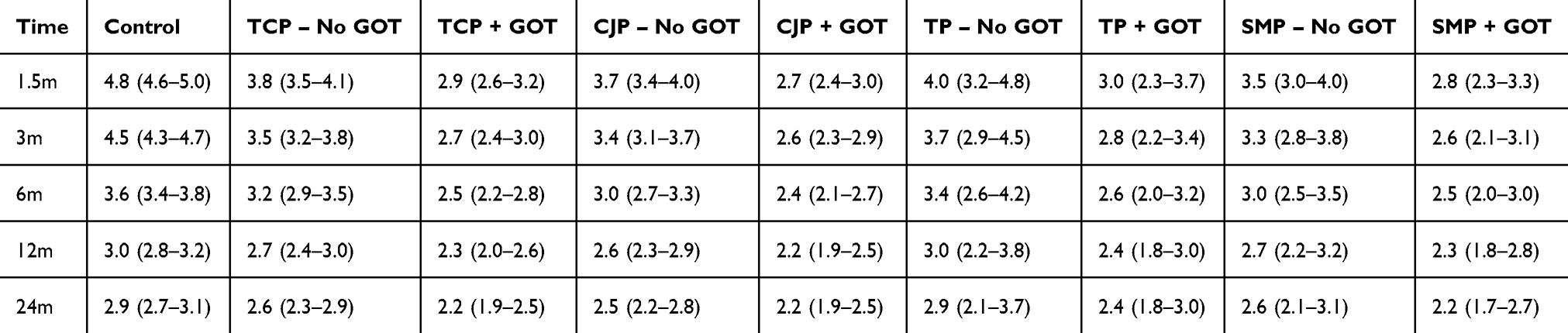 |
Table 6 Stool Frequency with Error Bars (95% CI) Across Groups |
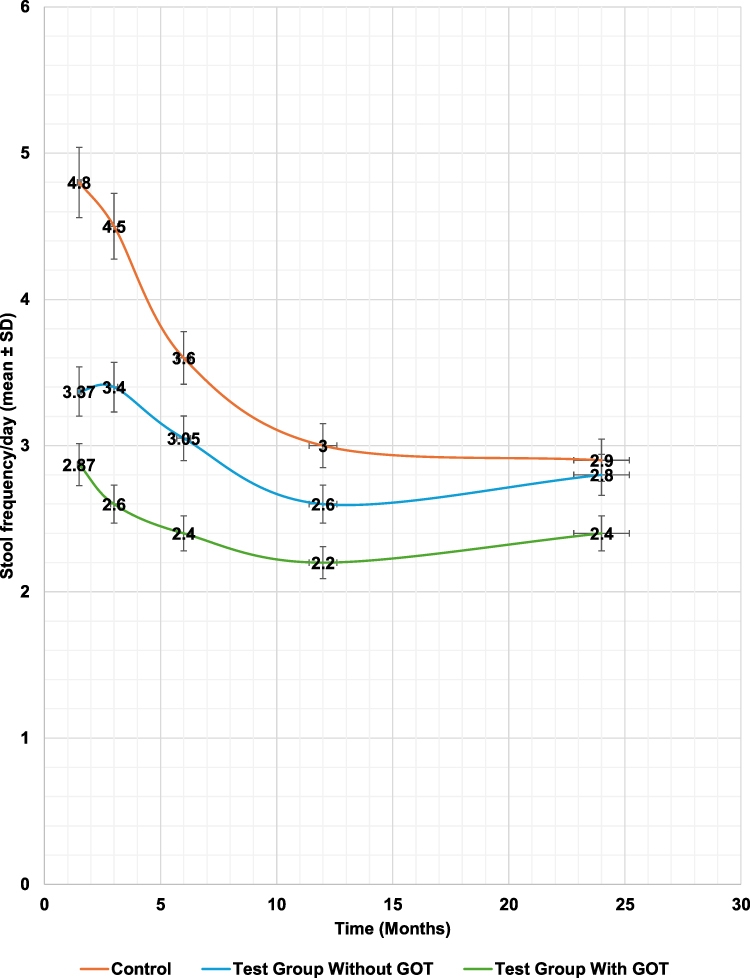 |
Figure 3 Stool Frequency Over Time. |
Within the test group, GOT patients consistently demonstrated superior outcomes across all reconstructive techniques. Subgroup differences in TP (n=2) are expolatory but not interpreted conclusively.
Control vs Test Group Comparisons
As summarized in Table 7, stool frequency differences were consistently significant after Bonferroni correction. At 1.5 months, differences were −1.8 (95% CI: −2.3 to −1.4, P<0.001) for non-GOT and −2.2 (95% CI: −2.6 to −1.8, P<0.001) for GOT. At 24 months, differences remained significant: −0.4 (95% CI: −0.7 to −0.1, P=0.005) for non-GOT and −0.6 (95% CI: −0.9 to −0.3, P=0.001) for GOT.
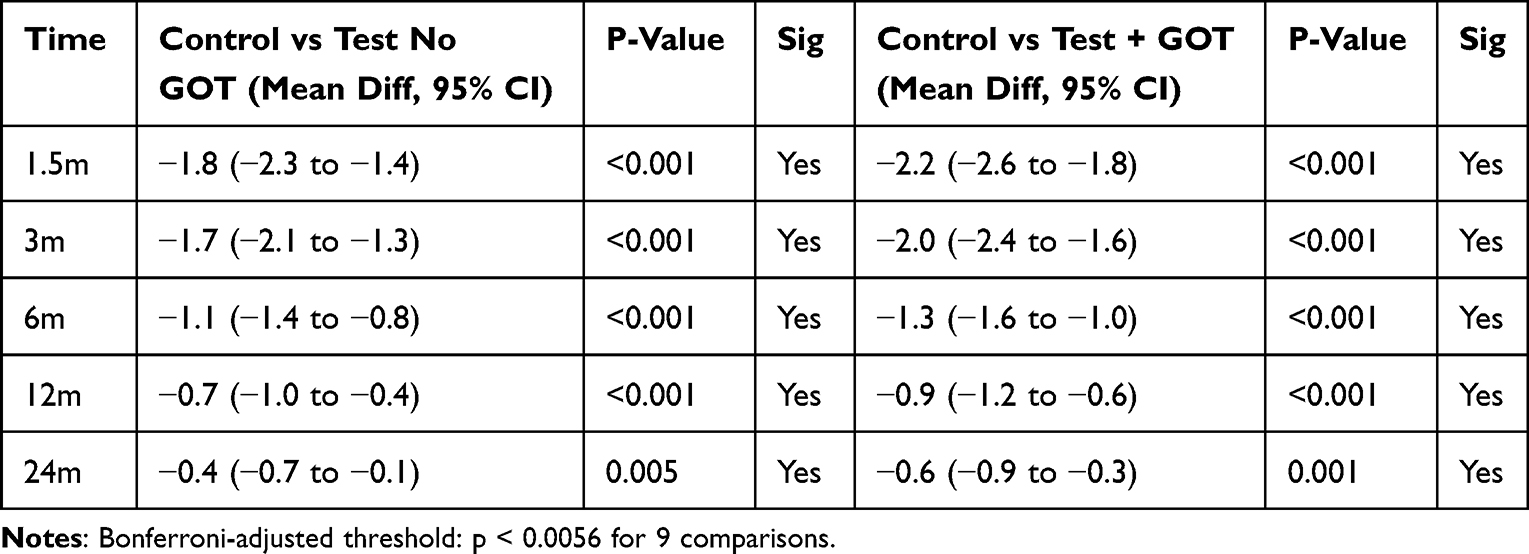 |
Table 7 Control vs Test Group Comparisons |
Cost-Effectiveness
Figure 4 shows the economic analysis. Although test procedures with GOT were more expensive upfront ($2,500 vs $1,400), long-term costs favored the test group, yielding savings of approximately $1,200 per patient at 24 months, due to reduced rates of complications, readmissions, and supportive care.
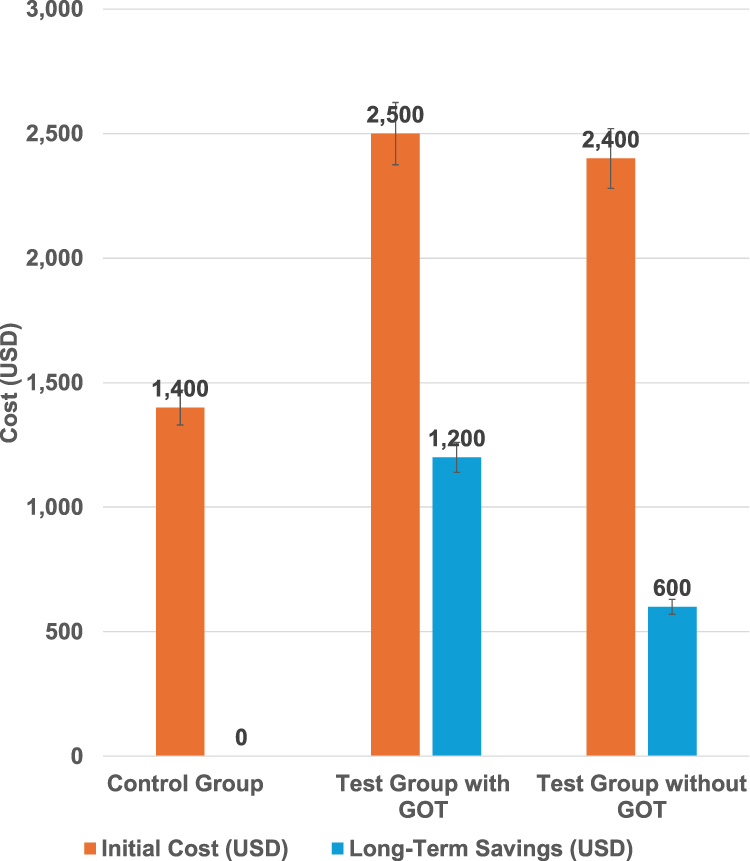 |
Figure 4 Cost-Effectiveness Analysis. |
Discussion
The findings of this study confirm the efficacy of advanced reconstructive techniques, particularly greater omentum transplantation (GOT), in mitigating the severity of Low Anterior Resection Syndrome (LARS) and enhancing continence outcomes. The significant improvements observed in stool frequency and continence underscore the combined benefits of incorporating GOT with neorectal reservoir techniques.
This study highlights the effectiveness of advanced reconstructive approaches in enhancing recovery after TME. Notably, the incidence of major LARS was reduced dramatically, from 80% in the control group to 10% in the test group. These results underscore the transformative impact of advanced surgical methods on recovery and quality of life.
The strong correlation between lower stool frequency and improved continence outcomes further underscores the effectiveness of these interventions.
Advanced techniques reduce mechanical strain, aiding functional recovery. Specifically, GOT accelerates this process by promoting tissue healing, reducing local inflammation, and helping to normalize stool frequency.
When GOT is combined with neorectal reservoir techniques, such as the taeniectomy pouch, transverse coloplasty, or colonic J-pouch, the benefits are maximized. Neorectal reservoirs and GOT improve tissue healing and bowel recovery, creating a functional foundation for bowel recovery. This combined approach ensures both short-term and long-term functional improvements and provides promising evidence supporting the role of GOT when combined with neorectal reservoir techniques.
The universal R0 resection rate confirms the oncological safety of these techniques. Patients experiencing no or minor incontinence reported significantly better quality of life, underscoring the clinical value of these approaches. Predictors of superior outcomes included younger age, lower tumor distance from the anal verge, and the absence of preoperative chemoradiotherapy (CRT). These findings highlight the importance of individualized surgical planning to achieve optimal functional and clinical results.
Recent literature supports the superiority of neorectal reservoirs in reducing LARS and improving outcomes. Meta-analyses and randomized controlled trials (RCTs) have consistently demonstrated the superiority of neorectal reservoir techniques over straight coloanal anastomosis in mitigating LARS symptoms and improving functional outcomes.1–10 For instance, studies by Fazio et al (2000) and Ho et al (2001) showed that J-pouch and transverse coloplasty techniques significantly reduce stool frequency and urgency, with fewer complications.5,11 These results underscore the effectiveness of reservoir techniques in replicating the rectum’s natural storage and evacuation functions.
Greater Omentum Transplantation (GOT)
Greater Omentum Transplantation (GOT) has emerged as a significant innovation in rectal surgery, offering substantial benefits in reducing inflammation, promoting tissue regeneration, and accelerating healing. Patients who received GOT, particularly in combination with other advanced reconstructive techniques, demonstrated faster recovery, improved bowel function, and a notable reduction in the severity of Low Anterior Resection Syndrome (LARS).
Clinical Evidence Supporting GOT
Liao et al (2023) provided compelling evidence in a randomized controlled trial (RCT) involving 200 patients undergoing rectal surgery, demonstrating that GOT significantly reduced postoperative complications, including anastomotic leakage, pelvic abscesses, and bowel dysfunction.12 These findings highlight GOT’s pivotal role in enhancing vascularization, reducing local inflammation, and supporting tissue healing, leading to improved recovery and functional outcomes.13
In a follow-up study, Liao et al (2023) evaluated 26 patients undergoing ultra-low anterior resection, dividing them into two groups based on whether GOT was performed. Although there were no significant differences in operative time, intraoperative blood loss, or postoperative complications between the groups, the study confirmed GOT’s role in improving tissue healing and bowel functionality.12 These findings validate GOT as a cornerstone of reconstructive strategies.
Integration with Neorectal Reservoir Techniques
The integration of GOT with neorectal reservoir techniques (eg, colonic J-pouch, transverse coloplasty) amplifies its efficacy by addressing both functional and structural challenges:
● Tissue Regeneration: GOT enhances vascularization, creating a conducive environment for tissue repair.
● Inflammation Reduction: Its anti-inflammatory properties help minimize complications like anastomotic leakage.
● Improved Functional Outcomes: Combining GOT with neorectal reservoirs optimizes bowel function and accelerates recovery.
Our study findings strongly support the use of GOT alongside neorectal reservoirs to achieve optimal postoperative outcomes in patients undergoing Total Mesorectal Excision (TME) for rectal cancer. This combination provides a robust framework for addressing the challenges of sphincter-preserving procedures.
GOT in Pelvic Surgery
The efficacy of GOT extends beyond rectal cancer surgery, as evidenced by its application in broader pelvic procedures. Miyamoto et al (2016) conducted an RCT involving 27 patients undergoing pelvic exenteration for advanced malignancies and demonstrated that GOT significantly reduced the incidence of pelvic abscesses, anastomotic leakage, and bowel dysfunction.14
These findings further support the application of GOT in our study, where its integration with advanced reconstructive techniques significantly enhanced outcomes, particularly in reducing LARS severity and postoperative complications. GOT’s unique ability to enhance vascularization and tissue regeneration underscores its indispensable role in advanced pelvic surgery.
GOT has proven to be a promising advancement in rectal and pelvic surgery, effectively reducing postoperative complications, accelerating recovery, and enhancing functional outcomes. Its integration with neorectal reservoir techniques and other reconstructive approaches addresses critical structural and functional challenges, making it an essential component of advanced surgical strategies. Robust clinical evidence supports GOT’s role as a cornerstone of innovative rectal cancer surgery, offering improved quality of life and outcomes for patients undergoing Total Mesorectal Excision (TME). Future research should focus on long-term outcomes and additionally applications of GOT in colorectal and pelvic surgeries.
Neorectal Reservoir Techniques
Neorectal reservoir techniques, including the colonic J-pouch (CJP), taeniectomy pouch, and transverse coloplasty, are well-established in mitigating Low Anterior Resection Syndrome (LARS) and improving postoperative bowel function. These techniques have demonstrated consistent superiority over straight coloanal anastomosis in enhancing stool frequency, continence, and overall quality of life.
Effectiveness of Colonic J-Pouch (CJP)
The colonic J-pouch (CJP) has been extensively validated as a highly effective neorectal reservoir technique. Ho et al (2001) conducted a randomized controlled trial (RCT) comparing J-pouch and straight coloanal anastomosis, reporting significantly improved bowel function and fewer LARS symptoms in J-pouch patients at six months and two years post-surgery.11 Similarly, a meta-analysis by Heriot et al (2006), involving 35 RCTs with 2240 patients, confirmed that CJP reduces major LARS rates, improves stool frequency, and enhances continence.15
A systematic review and meta-analysis by Shafquat Zaman et al (2022) compared colonic J-pouch anastomosis with straight (end-to-end) anastomosis following low anterior resection, including 27 studies with 3,293 patients (1,581 straight, 1,712 J-pouch). Results showed significantly lower rates of anastomotic leaks and re-operations in the J-pouch group, as well as superior functional outcomes, including reduced stool frequency at 6 and 12 months and decreased use of anti-diarrheal medications. Both groups demonstrated similar rates of complications such as SSI, sepsis, ileus, anastomotic strictures, bleeding, and mortality. The study concluded that J-pouch anastomosis offers improved safety and functional outcomes compared to straight anastomosis.16
In a systematic review, Brown et al (2008) analyzed 2,609 studies, including 16 RCTs, and concluded that CJP offers superior bowel function compared to straight anastomosis, with these benefits persisting for at least 18 months post-surgery.17 Furthermore, a meta-analysis by Mathew et al (2023), involving 32 trials with 3,072 patients, highlighted CJP’s ability to reduce stool frequency, improve continence scores, and minimize urgency and incomplete evacuation.18 These findings align with our study, where patients undergoing J-pouch reconstructions exhibited significant improvements in LARS scores and bowel function.
Taeniectomy Pouch and Transverse Coloplasty
For patients with narrow pelvic anatomy or anatomical constraints preventing J-pouch creation, alternative neorectal reservoirs such as the taeniectomy pouch and transverse coloplasty (TCP) provide effective solutions. The taeniectomy pouch mimics the rectum’s natural capacity, leading to marked reductions in LARS symptoms, as also supported by Fazio et al (2000).5
Transverse coloplasty offers another viable alternative, particularly in anatomically challenging cases. Pan et al (2023) retrospectively analyzed 235 patients undergoing intersphincteric resection (ISR) and found that TCP significantly improved bowel function, reduced stool frequency and urgency, and lowered the risk of anastomotic leakage compared to straight coloanal anastomosis (SCAA). These benefits persisted even two years after ileostomy closure.19 Our study corroborates these findings, demonstrating that TCP significantly enhances functional outcomes and mitigates LARS severity.
Comparative Analysis of CJP, TCP, and SCA
Biondo et al (2013) compared the outcomes of 106 patients undergoing low anterior resection with CJP, TCP, and SCA. The results revealed that CJP provided the best outcomes in terms of incomplete defecation symptoms and overall bowel function. TCP emerged as a valuable alternative where J-pouch creation was not feasible due to anatomical constraints. Both CJP and TCP demonstrated functional superiority over SCA, with significant reductions in LARS symptoms in both short- and long-term follow-ups.20 These findings mirror our study, where patients undergoing CJP and TCP achieved statistically superior outcomes compared to those receiving SCA.
Role of Neorectal Reservoirs in Advanced Reconstructive Strategies
The consistent evidence from RCTs and meta-analyses underscores the pivotal role of neorectal reservoirs in improving functional outcomes and reducing LARS following Total Mesorectal Excision (TME).11,15–18 Techniques such as CJP, TCP, and taeniectomy pouch outperform straight anastomosis in bowel function, continence, and quality of life, making them critical components of advanced reconstructive strategies.
Tailored surgical planning is essential for optimizing outcomes, as individual anatomical variations and clinical factors influence the choice of neorectal reservoir technique. Future research should prioritize long-term follow-up studies to assess the durability of these outcomes and explore their integration into minimally invasive approaches to further enhance recovery and patient satisfaction.
By leveraging neorectal reservoir techniques, surgeons can significantly improve postoperative recovery and quality of life for patients undergoing TME, setting a new standard for sphincter-preserving rectal cancer surgeries.
In patients with obesity or anatomically narrow pelvises, the technical feasibility of constructing neorectal reservoirs may be more challenging. Limited pelvic space and higher tissue bulk can increase the risk of anastomotic tension, prolonged operative time, and postoperative complications such as leakage. Furthermore, functional adaptation may be less predictable in these anatomically constrained patients. While our study did not specifically stratify by BMI or pelvic dimensions, these factors represent important considerations for surgical planning and warrant further investigation.
Smooth Muscle Plasty
Smooth muscle plasty is a promising reconstructive technique for restoring internal anal sphincter function, particularly in patients undergoing total intersphincteric resection (ISR). This procedure plays a vital role in preserving sphincter integrity, which is crucial for maintaining continence post-surgery. When combined with greater omentum transplantation (GOT), smooth muscle plasty provides synergistic benefits, enhancing functional outcomes and reducing postoperative complications.
Clinical Evidence Supporting Smooth Muscle Plasty
Robust clinical evidence highlights the efficacy of smooth muscle plasty in improving continence outcomes:
● Krand et al (2009) conducted a long-term follow-up study on 47 patients with very low rectal carcinomas who underwent ISR followed by smooth muscle plasty. The study reported acceptable oncological and functional outcomes, with 89% of patients achieving good continence (Kirwan I and II) two years post-surgery. Significant reductions in fecal incontinence over five years further demonstrated the durability of the procedure.21
● Hirche et al evaluated 27 patients who underwent neo-sphincter reconstruction with perineal colostomy and colonic smooth muscular cuff plasty after abdominoperineal resection. The retrospective study found improved long-term functional outcomes, enhanced quality of life, and reduced postoperative complications, supporting the reliability of smooth muscle plasty as a reconstructive technique.22
Integration with Greater Omentum Transplantation (GOT)
Combining smooth muscle plasty with GOT amplifies the functional and structural benefits of the reconstruction:
1. Promotes Tissue Regeneration: GOT enhances vascularization and healing, providing structural support to the reconstructed sphincter.
2. Reduces Local Inflammation: The omentum’s anti-inflammatory properties create an optimal recovery environment.
3. Minimizes Complications: This approach reduces the risk of anastomotic leakage and other complications, which can impair functional outcomes.
These synergistic effects create a robust framework for restoring bowel control and optimizing postoperative recovery in ISR cases.
Novel Applications of Smooth Muscle Plasty
Our study highlights the innovative application of smooth muscle plasty combined with GOT, reinforcing its efficacy in addressing sphincter dysfunction:
● Restoring Continence Function: Smooth muscle plasty directly targets the internal anal sphincter, essential for maintaining resting tone and continence.
● Optimizing Surgical Outcomes: GOT enhances the durability and effectiveness of sphincter reconstruction, leading to sustained functional improvements.
These findings align with existing research, supporting smooth muscle plasty as an integral component of advanced reconstructive strategies for low rectal cancer resections.
Clinical Implications
Smooth muscle plasty, particularly when combined with GOT, represents a significant advancement in sphincter-preserving surgery. Its ability to enhance continence, reduce complications, and improve quality of life makes it a cornerstone of rectal cancer management. Future research should focus on:
1. Long-Term Follow-Up Studies: To evaluate the durability of continence outcomes and quality-of-life improvements.
2. Broader Applications: Investigating the role of smooth muscle plasty in other colorectal surgeries.
3. Patient Selection Criteria: Identifying populations that derive the greatest benefit from this approach.
Integration of GOT and Smooth Muscle Plasty
Our study underscores the value of integrating GOT with smooth muscle plasty and neorectal reservoir techniques. This combined approach addresses both functional and structural challenges, accelerating recovery, improving bowel control, and enhancing long-term quality of life. Together, these advanced reconstructive techniques provide a robust solution for the challenges posed by sphincter-preserving procedures for low rectal cancer.
Smooth muscle plasty (SMP) was performed in a small subset of patients within our study, and while early outcomes were encouraging, the limited sample size precludes definitive conclusions. SMP may hold particular relevance for patients with pre-existing sphincter weakness, potentially improving functional outcomes through reinforcement of the sphincteric mechanism. However, robust evidence comparing long-term efficacy, safety, and quality-of-life outcomes against alternative reconstructive approaches remains lacking. Larger, multicenter studies are needed to clarify the role of SMP in this context.
Impact of Preoperative Radiotherapy
Preoperative radiotherapy improves oncological outcomes but is a known risk factor for LARS.23 A meta-analysis involving 1,963 patients found that radiotherapy significantly increased the risk of LARS (OR: 3.59, P < 0.00001).24 However, neorectal reservoir techniques, such as the J-pouch and transverse coloplasty, mitigate these risks by enhancing neorectal compliance and storage capacity, preserving bowel function.
The addition of GOT further minimizes complications and supports recovery, making it a vital component of advanced strategies for patients undergoing radiotherapy. These findings emphasize the need to integrate these techniques into the surgical management of patients at high risk for LARS to optimize both oncological and functional outcomes.
Future Directions
Future research should prioritize large multicenter trials to validate these findings and extend follow-up periods to assess the long-term durability of advanced reconstructive techniques. Key areas of exploration include:
1. Diverse Populations: Conducting multicenter trials to confirm the reproducibility of outcomes across varied demographic and clinical settings.
2. Long-Term Durability: Assessing the sustained efficacy of GOT and smooth muscle plasty in restoring bowel function.
3. Broader Applications: Exploring these techniques in other colorectal surgeries, including inflammatory bowel disease resections.
4. Cost-Effectiveness: Evaluating economic feasibility and long-term savings to facilitate broader adoption.
Although our study was restricted to oncological cases of very low rectal cancer following sphincter-preserving TME, the principles of reservoir reconstruction and greater omentum transplantation may have potential applications in selected benign conditions, such as refractory rectal prolapse or complex resections for inflammatory bowel disease. While this extrapolation is theoretically feasible, our findings cannot be generalized to benign disease, and specific studies in this patient population are required.
Another promising area for future research involves the identification of biomarkers that may predict successful functional outcomes after GOT. Potential candidates include angiogenic markers such as VEGF, immune-inflammatory markers, and baseline measures of pelvic floor integrity. Such biomarkers could help stratify patients most likely to benefit from GOT and refine individualized surgical planning. Our study did not include biomarker analysis; therefore, integrating translational research with surgical trials remains an important next step.
Limitations
This study has several important limitations. First, while the trial was conducted as a single-center randomized controlled trial with 1:1 computer-generated allocation and allocation concealment between the Control and Test groups, the choice of reconstructive technique within the Test arm was not randomized but determined intra-operatively by the surgeon based on pelvic anatomy and operative findings. Subgroup analyses of techniques such as the taeniectomy pouch (n=2 with GOT, n=2 without) are therefore exploratory, underpowered, and must be interpreted with caution.
Second, the relatively small overall sample size, particularly within such subgroups, limits statistical power for long-term follow-up evaluations at 12 and 24 months. Additionally, due to the absence of complete raw data, some standard deviations were estimated from pooled variances, which may introduce an element of imprecision in the analysis.
Third, measurement bias cannot be fully excluded, as continence, stool frequency, and quality of life outcomes were based on patient-reported questionnaires, which are subject to recall variability. However, validated tools and blinded outcome assessors were used to mitigate this risk.
Fourth, although multivariable adjustment and propensity-score methods were applied during analysis to account for residual imbalances, unmeasured confounding factors (such as baseline pelvic floor function or variations in neoadjuvant therapy regimens) cannot be fully excluded.
Finally, the single-center design may restrict external generalizability.
Nonetheless, the findings provide encouraging preliminary evidence in favor of integrating TP, smooth muscle plasty, and GOT into surgical protocols for patients undergoing Total Mesorectal Excision (TME) for very low rectal cancer. These combined techniques appear to enhance postoperative continence, support neorectal reservoir function, and improve overall quality of life. Larger, multicenter randomized studies with extended follow-up are warranted to confirm these benefits and establish broader clinical applicability.
Conclusion
Advanced reconstructive techniques, particularly the integration of greater omentum transplantation (GOT) with neorectal reservoir procedures such as the colonic J-pouch, transverse coloplasty, taeniectomy pouch, and smooth muscle plasty, demonstrated improved bowel function, continence, and quality of life in this single-center RCT. This combined approach effectively mitigates Low Anterior Resection Syndrome (LARS) and supports enhanced functional recovery.
However, given the study’s limitations, including sample size and single-center design, larger well-designed multicenter trials with longer follow-up are required before these techniques can be routinely adopted into clinical practice.
Data Sharing Statement
The datasets generated and analyzed during this study are available upon reasonable request from the corresponding author.
Ethical Considerations
The study was conducted in compliance with the Declaration of Helsinki and approved by the Institutional Review Board (IRB) of the 21st September University, Faculty of Medicine, Sana’a, Yemen. Written informed consent was obtained from all participants, and data were anonymized to ensure confidentiality. The trial was prospectively registered at Althowra Modern General Hospital Clinical Trials Registry under the identifier TMG-HOSP-RCT-2018-003.
Acknowledgments
The authors would like to thank the Surgery Department of 21st September University, Sana’a, Yemen, for their support during the study. Special thanks to the medical staff in the involved hospitals for their invaluable assistance in data collection and patient management over the 14-year study period.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests related to this study.
References
1. Holzer B, Urban M, Hölbling N, et al. Magnetic resonance imaging predicts sphincter invasion of low rectal cancer and influences selection of operation. Surgery. 2003;133(6):656–661. doi:10.1067/msy.2003.150. PMID: 12796734.
2. Orkin BA, Sinykin SB, Lloyd PC. The digital rectal examination scoring system (DRESS). Dis Colon Rectum. 2010;53(12):1656–1660. doi:10.1007/DCR.0b013e3181f23c85. PMID: 21178861.
3. Dobben AC, Terra MP, Deutekom M, et al. Anal inspection and digital rectal examination compared to anorectal physiology tests and endoanal ultrasonography in evaluating fecal incontinence. Int J Colorectal Dis. 2007;22(7):783–790. doi:10.1007/s00384-006-0217-3. Epub 2006 Nov 10. PMID: 17096089.
4. Ho YH, Brown S, Heah SM, et al. Comparison of J-pouch and coloplasty pouch for low rectal cancers: a randomized, controlled trial investigating functional results and comparative anastomotic leak rates. Ann Surg. 2002;236(1):49–55. doi:10.1097/00000658-200207000-00009. PMID: 12131085; PMCID: PMC1422548.
5. Fazio VW, Mantyh CR, Hull TL. Colonic “coloplasty”: novel technique to enhance low colorectal or coloanal anastomosis. Dis Colon Rectum. 2000;43(10):1448–1450. doi:10.1007/BF02236645. PMID: 11052525.
6. Z’graggen K, Maurer CA, Mettler D, Stoupis C, Wildi S, Büchler MW. A novel colon pouch and its comparison with a straight coloanal and colon J-pouch--anal anastomosis: preliminary results in pigs. Surgery. 1999;125(1):105–112. doi:10.1016/S0039-6060(99)70297-7. PMID: 9889806
7. Maurer CA, Z’graggen K, Zimmermann W, Häni HJ, Mettler D, Büchler MW. Experimental study of neorectal physiology after formation of a transverse coloplasty pouch. Br J Surg. 1999;86(11):1451–1458. doi:10.1046/j.1365-2168.1999.01256.x. PMID: 10583295.
8. Juul T, Ahlberg M, Biondo S, et al. Low anterior resection syndrome and quality of life: an international multicenter study. Dis Colon Rectum. 2014;57(5):585–591. doi:10.1097/DCR.0000000000000116. PMID: 24819098.
9. Pachler J, Wille-Jørgensen P. Quality of life after rectal resection for cancer, with or without permanent colostomy. Cochrane Database Syst Rev. 2012;12(12):CD004323. doi:10.1002/14651858.CD004323.pub4. PMID: 23235607; PMCID: PMC7197443.
10. Martellucci J. Low Anterior Resection Syndrome: a Treatment Algorithm. Dis Colon Rectum. 2016;59(1):79–82. doi:10.1097/DCR.0000000000000495. PMID: 26651116.
11. Ho YH, Seow-Choen F, Tan M. Colonic J-pouch function at six months versus straight coloanal anastomosis at two years: randomized controlled trial. World J Surg. 2001;25(7):876–881. doi:10.1007/s00268-001-0044-1. PMID: 11572027.
12. Liao J, Qin H, Wang Z, et al. Mesorectal reconstruction with pedicled greater omental transplantation to relieve low anterior resection syndrome following total intersphincteric resection in patients with ultra-low rectal cancer. BMC Surg. 2023;23(1):236. doi:10.1186/s12893-023-02140-1. PMID: 37573297; PMCID: PMC10423425.
13. McLachlin AD, Denton DW. Omental protection of intestinal anastomoses. Am J Surg. 1973;125(1):134–140. doi:10.1016/0002-9610(73)90018-4. PMID: 4683467.
14. Miyamoto Y, Akiyama T, Sakamoto Y, et al. Omental flap after pelvic exenteration for pelvic cancer. Surg Today. 2016;46(12):1471–1475. doi:10.1007/s00595-016-1348-y. Epub 2016 May 25. PMID: 27226018.
15. Heriot AG, Tekkis PP, Constantinides V, et al. Meta-analysis of colonic reservoirs versus straight coloanal anastomosis after anterior resection. Br J Surg. 2006;93(1):19–32. doi:10.1002/bjs.5188. PMID: 16273532.
16. Zaman S, Mohamedahmed AYY, Ayeni AA, et al. Comparison of the colonic J-pouch versus straight (end-to-end) anastomosis following low anterior resection: a systematic review and meta-analysis. Int J Colorectal Dis. 2022;37(4):919–938. doi:10.1007/s00384-022-04130-w. Epub 2022 Mar 19. PMID: 35306586.
17. Brown CJ, Fenech DS, McLeod RS. Reconstructive techniques after rectal resection for rectal cancer. Cochrane Database Syst Rev. 2008;2008(2):CD006040. doi:10.1002/14651858.CD006040.pub2. PMID: 18425933; PMCID: PMC8911547.
18. Mathew A, Ramachandra D, Goyal A, et al. Reconstructive techniques following low anterior resection for carcinoma of the rectum: meta-analysis. Br J Surg. 2023;110(3):313–323. doi:10.1093/bjs/znac400. PMID: 36630589.
19. Pan H, Zhao Z, Deng Y, et al. Transverse Coloplasty Pouch versus Straight Coloanal Anastomosis Following Intersphincteric Resection for Low Rectal Cancer: the Functional Benefits May Emerge After Two Years. J Gastrointest Surg. 2023;27(11):2526–2537. doi:10.1007/s11605-022-05565-w. Epub 2023 Oct 17. PMID: 37848684.
20. Biondo S, Frago R, Codina Cazador A, et al. Long-term functional results from a randomized clinical study of transverse coloplasty compared with colon J-pouch after low anterior resection for rectal cancer. Surgery. 2013;153(3):383–392. doi:10.1016/j.surg.2012.08.012. Epub 2012 Sep 14. PMID: 22981362.
21. Krand O, Yalti T, Tellioglu G, Kara M, Berber I, Titiz MI. Use of smooth muscle plasty after intersphincteric rectal resection to replace a partially resected internal anal sphincter: long-term follow-up. Dis Colon Rectum. 2009;52(11):1895–1901. doi:10.1007/DCR.0b013e3181b55507. PMID: 19966639.
22. Hirche C, Mrak K, Kneif S, et al. Perineal colostomy with spiral smooth muscle graft for neo-sphincter reconstruction following abdominoperineal resection of very low rectal cancer: long-term outcome. Dis Colon Rectum. 2010;53(9):1272–1279. doi:10.1007/DCR.0b013e3181e74c1f. PMID: 20706070.
23. Temple LK, Wong WD, Minsky B. The impact of radiation on functional outcomes in patients with rectal cancer and sphincter preservation. Semin Radiat Oncol. 2003;13(4):469–477. doi:10.1016/S1053-4296(03)00051-1. PMID: 14586835.
24. Liang Z, Zhang Z, Wu D, et al. Effects of Preoperative Radiotherapy on Long-Term Bowel Function in Patients With Rectal Cancer Treated With Anterior Resection: a Systematic Review and Meta-analysis. Technol Cancer Res Treat. 2022;21:15330338221105156. doi:10.1177/15330338221105156. PMID: 35731647; PMCID: PMC9228631.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.