Back to Journals » International Journal of Nanomedicine » Volume 21
Advanced Multiscale Inhalation Platforms for Treatment of Pulmonary Diseases
Authors Zhou S, Ran S, Zhang F, Ma H, Jiang C, Li S, Zhang Q ![]()
Received 17 April 2026
Accepted for publication 17 June 2026
Published 26 June 2026 Volume 2026:21 617811
DOI https://doi.org/10.2147/IJN.S617811
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Kamakhya Prakash Misra
Siyu Zhou,1 Shasha Ran,1 Fang Zhang,1 Haotian Ma,1 Chunling Jiang,2 Shanshan Li,1 Qixiong Zhang3,4
1College of Pharmacy and Food, Key Laboratory of Research and Application of Ethnic Medicine Processing and Preparation on the Qinghai-Tibet Plateau, Southwest Minzu University, Chengdu, People’s Republic of China; 2Department of Pharmacy, Dachuan District People’s Hospital, Dazhou, People’s Republic of China; 3Department of Pharmacy, Personalized Drug Research and Therapy Key Laboratory of Sichuan Province, Sichuan Academy of Medical Science & Sichuan Provincial People’s Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China; 4Department of Pharmacy, Sichuan Provincial People’s Hospital East Sichuan Hospital & Dazhou First People’s Hospital, Dazhou, People’s Republic of China
Correspondence: Qixiong Zhang, Department of Pharmacy, Personalized Drug Research and Therapy Key Laboratory of Sichuan Province, Sichuan Academy of Medical Sciences & Sichuan Provincial People’s Hospital, School of Medicine, University of Electronic Science and Technology of China, Chengdu, People’s Republic of China, Email [email protected]; [email protected] Shanshan Li, College of Pharmacy and Food, Key Laboratory of Research and Application of Ethnic Medicine Processing and Preparation on the Qinghai-Tibet Plateau, Southwest Minzu University, Chengdu, People’s Republic of China, Email [email protected]
Abstract: Pulmonary diseases, including chronic obstructive pulmonary disease, asthma, pneumonia, pulmonary fibrosis, and lung cancer, pose a significant threat to global health. Their high incidence and mortality rates highlight the urgency for novel therapeutic approaches. Traditional treatments such as oral and injection administrations face limitations like first-pass effects, low bioavailability, and systemic toxicity, which restrict their therapeutic efficacy. Inhaled preparations, with advantages such as uniform drug distribution, rapid onset, high bioavailability, and avoidance of hepatic first-pass effects, have become effective means for treating lung diseases. This article reviews the research progress of novel inhaled preparations (nanoparticles, liposomes, microspheres, biomimetic platforms) in treating lung diseases, aiming to explore the development and application of novel inhaled formulations driven by advancements in nanotechnology, biomaterials and preparation processes, thereby providing new possibilities for lung disease treatment. Overall, the research and application prospects of novel inhaled preparations are broad, promising more effective and safer treatment options for patients with pulmonary diseases.
Keywords: pulmonary diseases, inhalation preparations, nanoparticles, liposomes, microspheres, biomimetic platforms
Introduction
Pulmonary diseases are among the major threats to global health, severely impacting human quality of life and longevity. High-incidence diseases such as chronic obstructive pulmonary disease (COPD),1 asthma,2 pneumonia,3 pulmonary fibrosis,4 and lung cancer5,6 not only cause respiratory difficulties and organ dysfunction but are also closely associated with systemic complications (eg., cardiovascular diseases). For example, COPD is characterized by partially irreversible progressive airflow limitation, primarily caused by abnormal lung inflammation due to long-term exposure to harmful gases or particles (eg., smoking, air pollution). Typical symptoms include chronic cough, sputum production, dyspnea, and recurrent acute exacerbations. Its harmfulness manifests as high mortality, accelerated lung function decline, systemic complications, and significantly reduced quality of life and lifespan due to frequent acute exacerbations.7,8 Idiopathic pulmonary fibrosis (IPF) is another type of lung disease characterized by fibroblast proliferation, excessive extracellular matrix accumulation, accompanied by inflammatory damage and structural destruction, with an average survival of only 3–5 years post-diagnosis.9,10 Survey data indicate that respiratory diseases cause millions of deaths annually, with their high incidence, mortality, and substantial socioeconomic burden underscoring the urgency of prevention and treatment.11
Traditional lung disease treatments primarily rely on oral or injection administration. While they can alleviate symptoms to some extent, they have significant limitations: Oral administration for lung diseases is affected by first-pass effects, leading to low bioavailability and suboptimal efficacy.12 For instance, nintedanib and pirfenidone (PFD) are currently approved drugs for treating IPF,13,14 both exhibiting low oral bioavailability and limited therapeutic potential, requiring higher doses to enhance efficacy, which in turn causes severe hepatic and gastrointestinal toxicity.15,16 Intravenous injection is a systemic administration method where systemic drug distribution leads to non-target organ exposure, causing metabolic burden and adverse reactions,17 such as immunosuppression in hormone therapy18 and nephrotoxicity from intravenous antibiotics.19 Low effective drug concentrations in the lungs necessitate dose increases, exacerbating side effects. For example, intravenous chemotherapy for lung cancer results in drug distribution across various organs, thus requiring high doses to achieve therapeutic concentrations at the lesion site, resulting in severe adverse effects, especially in hair, skin, spleen, and liver that with rapidly dividing cells.20 Additionally, poor patient compliance (particularly in long-term users) further limits the efficacy.21 Therefore, developing more efficient and safe targeted therapeutic strategies is imperative.
Inhalation delivery has been considered a promising choice for treating lung diseases because it can shuttle therapeutic payloads directly to lung lesions via simple and noninvasive procedures while reducing systemic toxicity. With uniform drug distribution, rapid onset, high bioavailability, and avoidance of hepatic first-pass effects, inhaled preparations reduce systemic adverse reactions, providing more effective and safer options for lung disease treatment (Figure 1).22–24 Research has shown that the pharmacokinetics and tissue distribution of curcumin (Cur) in rats differ significantly among three routes of administration: inhalation, oral, and intravenous injection.25 After inhalation at 100 mg/kg, the peak concentration (Cmax) of Cur reached 93.15 ng/mL. At the same dose, the bioavailability and Cmax by inhalation were approximately 54-fold and 92-fold higher than those by oral route. Although intravenous injection at a lower dose (2.5 mg/kg) yielded a Cmax of 63.01 ng/mL, the drug was rapidly distributed throughout the body and eliminated quickly. Tissue distribution results further revealed that inhalation led to a pronounced accumulation of Cur in the lung, with extremely low concentrations in the heart, liver, spleen, kidneys, and brain, demonstrating remarkable lung-targeting specificity. However, the drug concentration in lung by intravenous injection was far lower, revealing more significant systemic exposure. Similarly, when sinapine thiocyanate (ST) was formulated as inhaled dry powder for the treatment of acute lung injury (ALI),26 the absolute bioavailability reached as high as 79.12%, approximately 2.7-fold that of the oral route. Overall, inhalation, combining non-invasiveness, lung targeting, and relatively high bioavailability, offers more pronounced advantages.
 |
Figure 1 Schematic diagram of applications of advanced inhalation platforms. |
In recent years, with advancements in nanotechnology, biomaterials, and preparation processes, novel inhaled preparations continue to emerge, offering new possibilities for lung disease treatment.27–30 This article aims to review the latest research progress in inhaled preparations for treating lung diseases, focusing on the development and application of novel inhaled formulations, to provide references for related research and clinical practice.
Advanced Inhalation Platforms for Pulmonary Diseases
Nanoparticles
Active Targeting Nanocarriers
Active targeting nanocarriers refer to nanocarriers modified or designed to actively recognize and bind to target cells or tissues, achieving precise drug delivery. Active targeting strategies are based on the specific receptors on cell surface. For instance, tumor cells overexpress specific receptors like folate (FA) receptor,31 transferrin (Tf) receptor,32 and epidermal growth factor receptor (EGFR).33 By modifying nanocarrier surfaces with ligands that specifically bind these receptors enabling active targeting.34 An EGFR-targeted nanoparticles (EGFC/DLPNs) co-delivering cisplatin and doxorubicin was developed for lung carcinoma therapy. In vitro and in vivo results showed good stability, sustained drug release, significant anticancer effects and low toxicity.35 Another smart chitosan-PLGA nanocarrier (CPSF) functionalized with FA ligands was developed for targeted delivery of sorafenib (SRF) to lung cancer cells. CPSF efficiently accumulated in cancer tissues bypassing cancer cell membrane barriers through high-affinity binding to FA receptors, thus reducing systemic distribution, increasing cytotoxic doses to tumor cells and minimizing inhibition of normal cells.36 Researchers anchored Tf to nanomicelle surfaces through the coordination effect between surface carboxyl groups and Fe3+ to develop an inhalable nanomimosa (Tf-Mic@SD) to enhance ferroptosis therapy for lung cancer based on lysosome hijacking strategy (Figure 2).37 The Fenton-like reaction substrate dihydroartemisinin (DHA) and SRF were further encapsulated. After inhalation, Tf-Mic@SD is captured by tumor cells through Tf receptor recognition, then endocytosed by lysosomes. Under acidic conditions, the conformation of Tf changes, releasing Fe3+, DHA, and SRF, triggering Fenton-like reactions to rapidly generate reactive oxygen species, accelerating ferroptosis and effectively eliminating tumor cells. Results showed Tf-Mic@SD effectively inhibited lung tumor growth with good biosafety for normal cells, offering new methods for lung cancer treatment and potential application in other Tf recepter-high cancers.
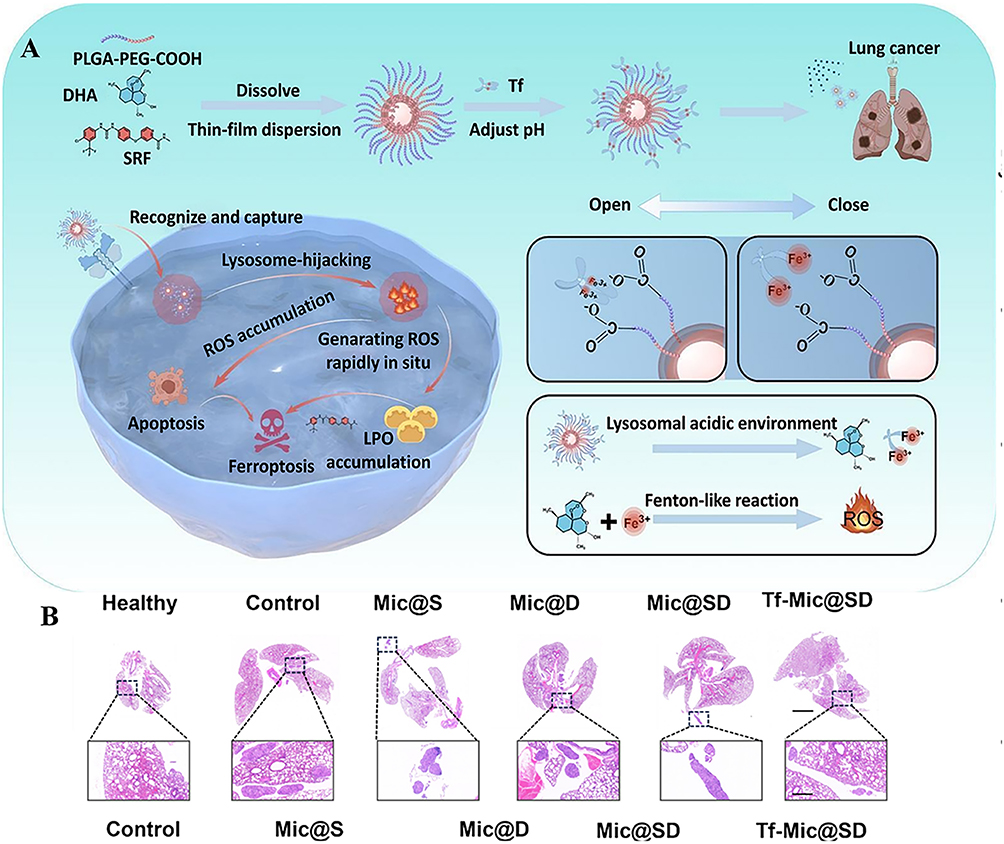 |
Figure 2 (A) Tf-Mic@SD presents a schematic of the optimized ferroptosis-based therapy for lung cancer; (B) H&E-stained sections of lung tumor tissue.37 Reprinted with permission from Journal of Controlled Release, 386 (2025) 114101. Copyright 2025, with permission from Elsevier. |
Targeting peptides, which are able to recognize and bind to specific cell or tissue surface receptors, is another kind of anchor to modify the nanoparticles for enhancing targeting.38 A neonatal-Fc-receptor-targeted peptide (FcBP) was anchored on polyethylene glycol (PEG) nanoparticles (PEG-NP) to form FcBP-NP for ameliorated transepithelial transport and prolonged pulmonary retention.39 By FcBP-functionalization, the mucus-permeability of PEG-NP was not impaired. Moreover, the cellular internalization and exocytosis via specific receptor-mediated processes were enhanced. Loaded with dexamethasone (Dex), FcBP-NP@Dex could effectively cross the airway epithelial layer and be endocytosed by inflammatory cells, then significantly reduce inflammatory cytokine levels and relieve asthma symptoms (Figure 3). This study provided a promising strategy for inhalation therapy with prolonged pulmonary retention of drugs.
 |
Figure 3 (A) Schematic illustration of FcBP-NP@Dex to ameliorate airway inflammation in asthma. (B) Uptake of transported nanoparticles by RAW 264.7 cells. (C) Uptake of nanoparticles and mucin. **p < 0.01. Mean ± SD, n = 3. (D) Apparent permeability (Papp) values of nanoparticles in expectorated human sputum. ns p > 0.05, **p < 0.01. Mean ± SD, n = 3.39 Reprinted with permission from Journal of Controlled Release, 367 (2024) 223–234. Copyright 2024, with permission from Elsevier. |
Stimulus-Responsive Nanoparticles
Responsive nanocarriers are nanomaterials that alter their properties in response to external environmental changes (eg., pH, temperature, magnetic fields, enzymes) or specific physiological/pathological signals, enabling targeted drug delivery and controlled release.40,41 The tumor microenvironment features low pH, enhanced enzyme activity (eg., MMP-2, cathepsin B), and altered redox status (ROS/GSH imbalance), supporting stimulus-responsive nanoparticles in cancer therapy.42,43 An inhalable pH-responsive core-shell nanocarrier (PEG-CS/Alg@MSNs) for sequential release of drugs in lung cancer therapy was established via layer-by-layer self-assembly.44 In this study, aminated mesoporous silica (MSNs) loaded with docetaxel (DTX) was used as a core, then sequentially coated with polyanionic alginate (Alg) as an intermediary sellotape layer to prevent drug leaking. The outermost shell is polycationic PEGylated-chitosan (PEG-CS) loaded with gemcitabine (GMC). Under neutral to weakly acidic physiological conditions, the PEG-CS and Alg layers prevent premature drug release and ensure the stability of the nanocarrier; while in the acidic environment of the tumor microenvironment, the amino groups in chitosan undergo protonation, destroying the shell structure, thereby triggering the rapid release of GMC, followed by the slow release of DTX from MSNs. Experimental results showed the good lung deposition, biosafety and significant anticancer effects of PEG-CS/Alg@MSNs on A549 cells, providing a new and effective drug delivery system for lung cancer treatment.
Besides, an inhalable mucoadhesive proteinic nanoparticles with redox responsibility were conducted to realize noninvasive, localized treatment of lung cancer in a highly biocompatible, site-specific manner. Specifically, the thiolated mussel adhesive protein (thMAP) containing 3,4-dihydroxyphenylalanine (DOPA) based nanoparticles (thMAP NPs) were administered to target lung tissues via nebulization process. Cur-loaded thMAP NPs (thMAP@Cur NPs) showed efficient cellular uptake through the thiol-mediated pathway and controlled intracellular release of Cur in response to the high glutathione (GSH) concentration in tumor microenvironment (Figure 4).45 This study proposes a novel precision therapy strategy for lung cancer that addresses the poor mucosal absorption of hydrophobic drugs in traditional inhalation by enabling efficient local pulmonary delivery and long-term retention, reducing systemic toxicity, while a redox-specific response mechanism enhances intracellular drug release efficiency and therapeutic outcomes, indicating broad application potential.
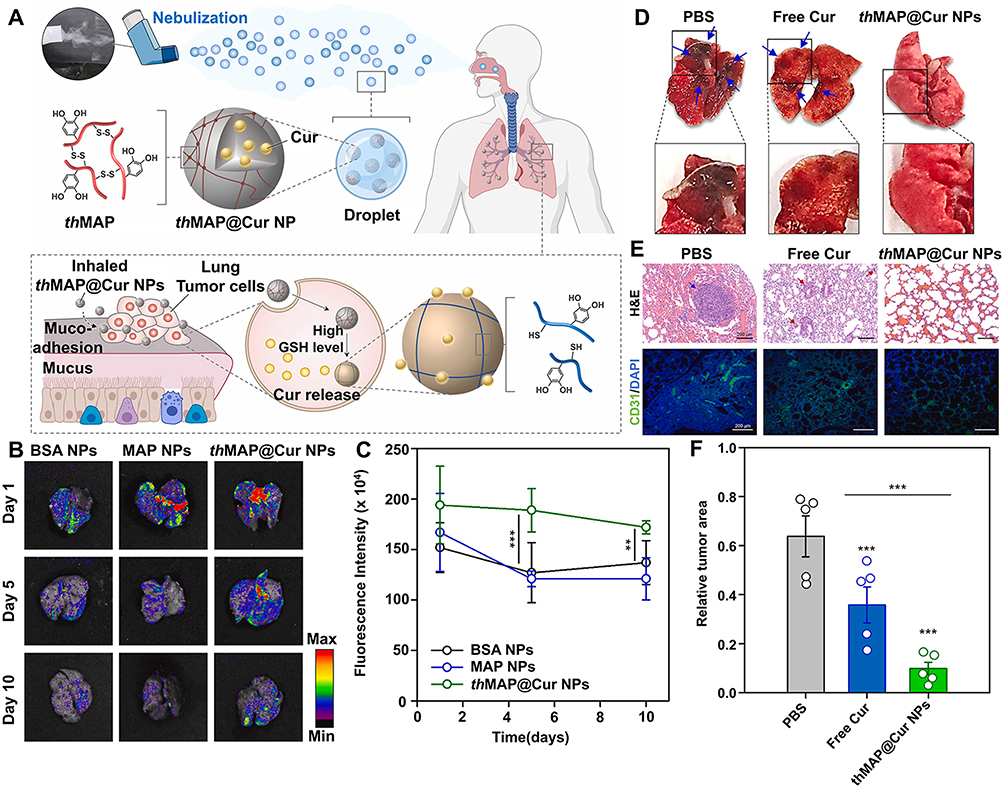 |
Figure 4 (A) Schematic illustration of the inhalable thMAP@Cur NPs for targeted lung cancer therapy. (B) In vitro fluorescence images of lung tissue at 1, 5, and 10 days after nebulization. Rhodamine-labeled BSA and MAP NPs were used as controls. (C) The integrated fluorescence intensity of the resected lung tissue area. (D) Optical images of lung tissue resected at the end of the study. The blue arrow indicates the tumor. (E) H&E and CD31 staining images of lung tissues. Blue arrows indicate metastatic melanoma nodules, red arrows denote epithelial hyperplasia. Green represents CD31-positive cells, blue indicates nuclei (DAPI). (F) Relative tumor area (tumor area/total area). Data represent mean ± s.e.m. (n ≥ 5), with statistical significance indicated by **p < 0.01 and ***p < 0.005.45 Reprinted with permission from Biomaterials, 316 (2025) 123004. Copyright 2025, with permission from Elsevier. |
The management of severe bacterial pneumonia remains a formidable clinical problem, primarily due to the compromised antibiotic efficacy resulting from the obstructive mucus barrier in the lower respiratory tract. A nano-agent (OTP) containing natural polysaccharide oxidized soluble starch (OSS), tobramycin (TOB) and m-PEG-NH2, with mucus-penetrating and infection-responsive releasing capabilities, was designed and fabricated (Figure 5).46 Due to its hydrophilicity, small molecular size, and positively charged surface, OTP exhibits enhanced mucosal permeability, enabling it to overcome mucociliary clearance and reach pulmonary lesions. Then TOB was responsively released by the triggering of slightly acidic environment of infection (pH = 5.4), owning to the pH-sensitive imine bond. The efficacy of OTP was further validated in a pneumonia mice model. This study presents a versatile and effective strategy for constructing inhalable drug delivery systems to treat pneumonia, highlighting its considerable potential for clinical management of severe pulmonary infections. Other researches on the treatment of lung diseases by inhalable nanoparticle systems were summarized in Table 1.
 |
Figure 5 (A) Schematic diagram illustrating the preparation process of OTP21 and its application in suppressing pulmonary infection therapy. (B) pH-responsive release kinetics of TOB from OTP21 and OTP21-R. (C) Images of OTP21 and OT21 samples penetrating artificial mucus. (D) Bioluminescence images of mice at day 1 and day 3 (“×” indicates death of the experimental animal due to infection). (E) Bacterial colonies from lung homogenates from Staphylococcus aureus-infected lung tissues. (F) Lung tissues collected from mice sacrificed 72 hours post-bacterial challenge, subjected to histological analysis via H&E staining and immunohistochemical (IHC) staining.46 Reprinted with permission from Nano Today, 44 (2022) 44. Copyright 2022, with permission from Elsevier. |
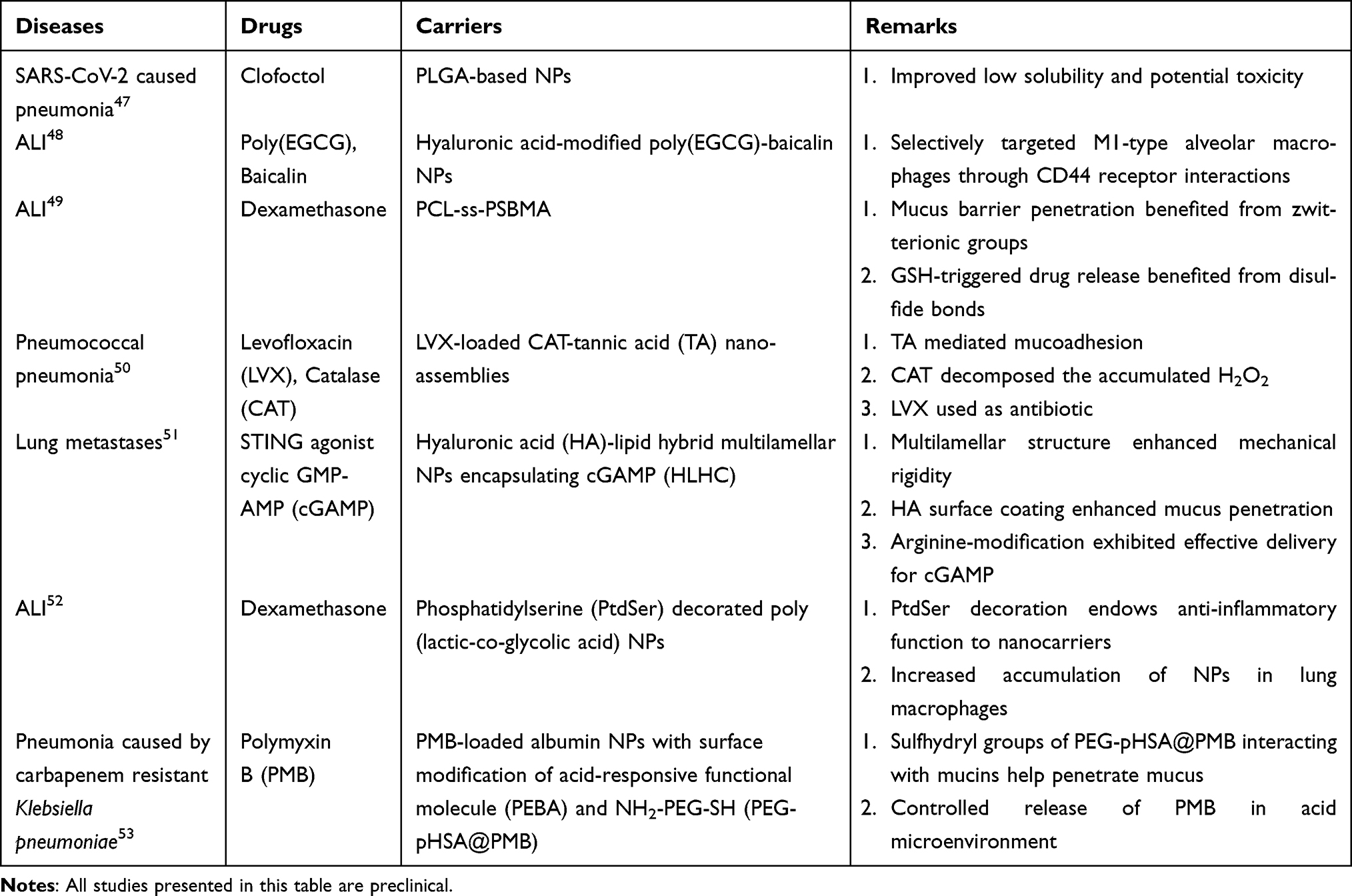 |
Table 1 Summary of Inhalable Nanoparticles for Treating Pulmonary Diseases |
Liposomes
Inhaled liposomes are microcapsules composed of phospholipid bilayers, capable of encapsulating both hydrophilic and hydrophobic drugs. They have good biocompatibility, can protect drugs from degradation, and achieve sustained release. In recent years, the potential of liposome technology in the treatment of pulmonary diseases has been continuously explored. Research has found that liposomes composed of saturated neutral and anionic phospholipids possessed high stability and permeability.54 The following will introduce several innovative studies based on liposomes, which explore from different perspectives how to enhance drug delivery efficiency and therapeutic effect through liposome technology.
Alveolar macrophages (AMs) possess a unique ability to infiltrate tumor tissue and play an important role in pulmonary metastasis. Specifically, AMs are prone to be polarized into immunosuppressive M2 phenotype in pulmonary metastasis, while immune-promoting M1 phenotype is effective in immunotherapy. Based on the capacity of AMs for non-specific phagocytosis and the specific binding with phosphatidylserine on the surface of apoptotic cell, a phosphatidylserine-decorated liposome was fabricated for both passive and active targeted delivery of TLR7/8 agonists (R848) and SHP2 inhibitor (SHP099), which could polarize AMs into immune-promoting M1 phenotype and restore the phagocytosis.55 This kind of inhalable and AM targeted immunostimulants (I-AM-IMs) could promote the phagocytic elimination of pulmonary metastatic tumor cells and activate CD8+ T cell specific anti-tumor immunity through phenotype reprogramming of AMs, then eradicate pulmonary metastasis.
Given the high collagen content in IPF lesions, collagen-targeted drug delivery systems can be used for the treatment of IPF. A pathological collagen targeting and penetrating liposome (DP-CC) for delivery of anti-fibrotic dual drugs including pirfenidone (PFD) and dexamethasone (DEX) have been constructed (Figure 6). With co-decoration of collagen binding peptide (CBP) and collagenase (COL) on the surface of DP-CC, the vehicle could efficiently target the fibrotic lesions and break through the collagen barrier then deep deliver to the injured alveoli. Subsequently, the released PFD and DEX exhibited a synergistic anti-fibrotic effect, capable of repairing damaged epithelial tissues and remodeling the extracellular matrix, thereby reconstructing the lung structure.56
 |
Figure 6 Pathological collagen targeting and penetrating liposomes (DP-CC) for deep injured alveoli drug delivery. (A) Components and construction of the DP-CC. (B) Proposed mechanism of the DP-CC in vivo. i) Pathological collagen is exposed to the bloodstream around fibrotic sites, DP-CC targeted the pathological collagen and delivered PFD/DEX to the fibrotic lungs through intravenous injection. ii) Pathological collagen is accumulated to obstruct foreign liposomes, while DP-CC could break through the collagen barrier. iii) After reaching the deep injured alveoli, PFD and DEX exert a synergistic anti-fibrotic effect to reverse IPF.56 Reprinted with permission from Journal of Controlled Release, 351 (2022) 623–637. Copyright 2022, with permission from Elsevier. |
In addition to the above two innovative strategies, the basic liposome drug delivery system also demonstrates great potential. The effect of liposomal prostaglandin E2 (PGE2) delivered by inhalation in the treatment of IPF was studied.57 In a murine model, the therapeutic potential of pulmonary-delivered liposomal PGE2 was assessed. Inhalation led to greater lung-specific accumulation and less systemic distribution compared to intravenous administration. Experimental results demonstrated that liposomal PGE2 significantly attenuated inflammation and fibrotic damage in lung tissue, prevented weight loss, reduced hydroxyproline accumulation, and markedly reduced mortality in mice. These findings indicate that pulmonary delivery of liposomal PGE2 via inhalation is an effective therapeutic approach for IPF. This study provides critical evidence supporting the development of novel IPF treatments, particularly by enhancing local drug concentrations while mitigating systemic side effects.
Although inhaled lipid-based delivery systems hold significant promise for IPF treatment, their applicability extends beyond this condition. Ongoing research explores their potential for other pulmonary diseases to benefit broader patient populations. For instance, Jiang et al58 proposed an innovative inhaled lipid-based strategy for treating ALI and its progression to acute respiratory distress syndrome (ARDS). Recognizing the central role of macrophages, particularly pro-inflammatory M1 polarization, in the pathogenesis of ALI/ARDS, the researchers designed L-arginine-modified liposomes targeting M1 macrophages via their highly expressed CAT-2 receptors. Curcumin was encapsulated as a model drug (Figure 7). The modification was achieved by conjugating L-arginine’s carboxyl groups to liposomal amines via EDC/NHS chemistry. Results demonstrated that this targeted system significantly enhanced curcumin’s efficacy against ALI/ARDS. By enabling direct lung deposition, it bypasses hepatic/splenic first-pass metabolism, increases local drug concentration, and minimizes systemic adverse effects. This approach offers novel insights for treating acute pulmonary inflammation, including cytokine storms associated with COVID-19, presenting a safer and more effective therapeutic option.
 |
Figure 7 (A) Preparation of Arg-Cur-Lip and its treatment for ALI/ARDS. L-arginine functionalized Cur-Lip was used to target M1 macrophages in the lung after aerosol inhalation and release the drug for treatment after accumulation in the inflamed lung. (B) In vivo fluorescence images of a rat ALI model using DiR loaded liposomes via pulmonary nebulization. (C) In vitro fluorescence images of excised organs 24 hours after using DiR loaded liposomes. Measure the protein expression levels of TNF-α (D) and IL-6 (E) in lung tissue using ELISA.58 Data are represented as means ± SD (n = 4). *P < 0.05 compared with the model group, **P < 0.01 compared with the model group, ##P < 0.01 compared with the control group, &P < 0.05 compared with Cur-Lip group. Reprinted with permission from European Journal of Pharmaceutics and Biopharmaceutics, 182 (2023) 21–31. Copyright 2023, with permission from Elsevier. |
Other researches on the treatment of lung diseases by inhalable liposomal preparations were summarized in Table 2.
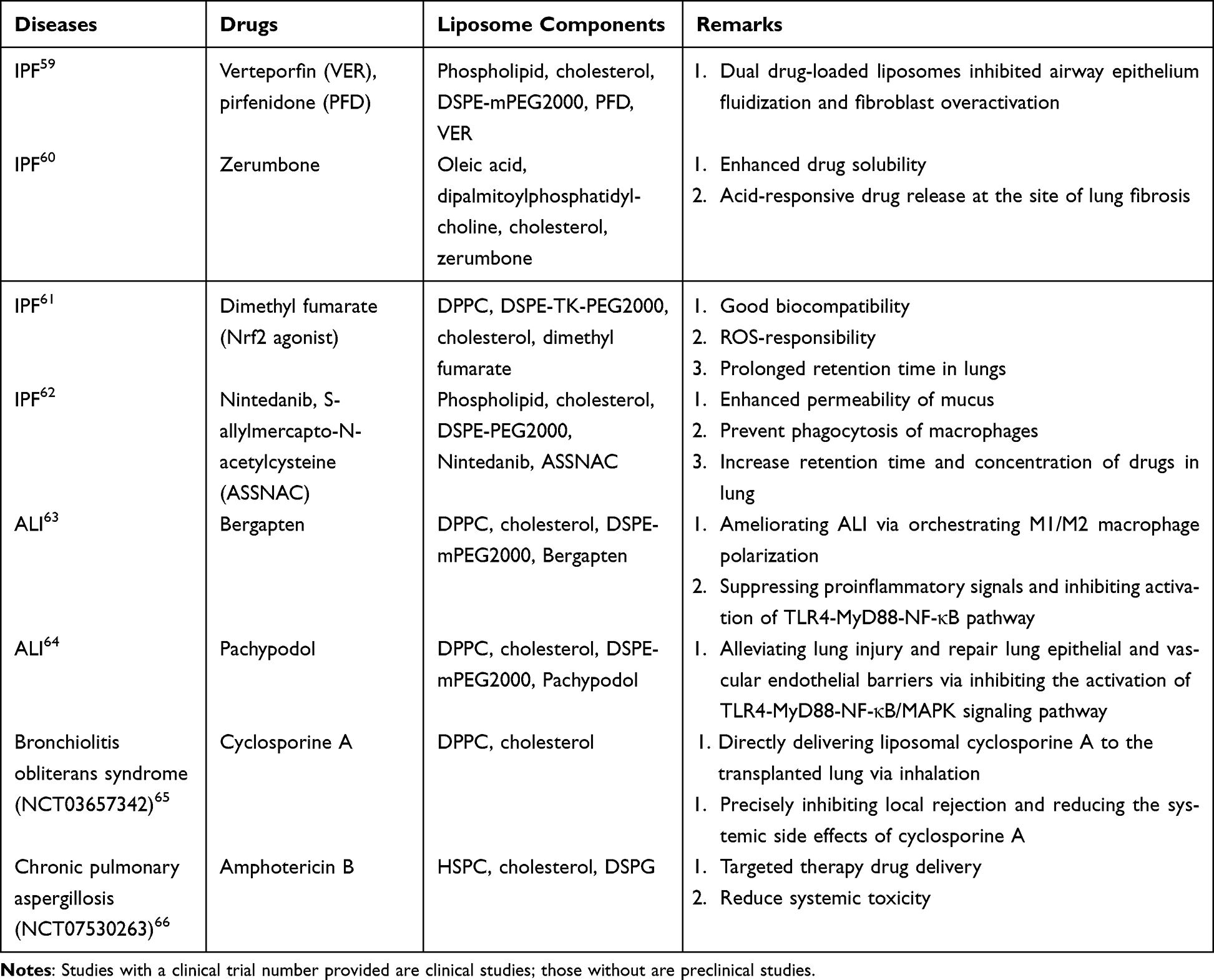 |
Table 2 Summary of Inhalable Liposomal Preparations for Treating Pulmonary Diseases |
Microspheres
Microsphere inhalation agents are a new type of drug delivery system, where drugs are precisely encapsulated within microsphere carriers constructed from biodegradable polymers.67 Their core advantage lies in the precise control over particle size, which ensures targeted pulmonary deposition at lesion sites following inhalation. This facilitates local drug enrichment, thereby enhancing therapeutic efficacy while minimizing off-target side effects.68 Furthermore, inhaled microspheres exploit a distinctive sustained-release mechanism based on the gradual degradation of polymeric matrices within the physiological environment.69 This process ensures continuous and stable drug elution, sustaining effective drug concentrations in the lungs over extended periods. Consequently, it prolongs the duration of pharmacological action and reduces dosing frequency, which may enhance patient compliance. These attributes underscore the significant clinical potential of microsphere-based systems for pulmonary diseases, offering innovative strategies for precision medicine.70,71
In the investigation of inhalable microspheres for pulmonary diseases, Cheng et al developed an aerosol platform of inhalable honeycomb-shaped microsphere (HCLplga-Ab) composed of FDA-approved PLGA and pore-forming agent for the targeted delivery of Andrographolide, a bioactive compound derived from traditional Chinese medicine. The microsphere was coated by chitosan-ambroxol to facilitate mucosal penetration, sequential drug release, and prolonged lung retention (Figure 8). Characterization revealed a geometric diameter of ~10–15 μm and an aerodynamic diameter of ~2.57 μm, enabling deep lung deposition while evading alveolar macrophage clearance. In murine models of ALI, bacterial pneumonia, and fungal pneumonia, the aerosol exhibited potent mucosal penetration and biofilm destruction capabilities, markedly reducing inflammation and pathogen loads while improving survival rates. Notably, compared with conventional PLGA microspheres, the HCLplga-Ab variant demonstrated staged release kinetics: ambroxol was released first to compromise the mucosal barrier, followed by sustained Andrographolide release to exert anti-inflammatory and antibacterial effects. This work presents a novel strategy integrating traditional medicine with advanced aerosol technology, highlighting significant translational potential for treating respiratory diseases such as pneumonia, asthma, and pulmonary fibrosis.72
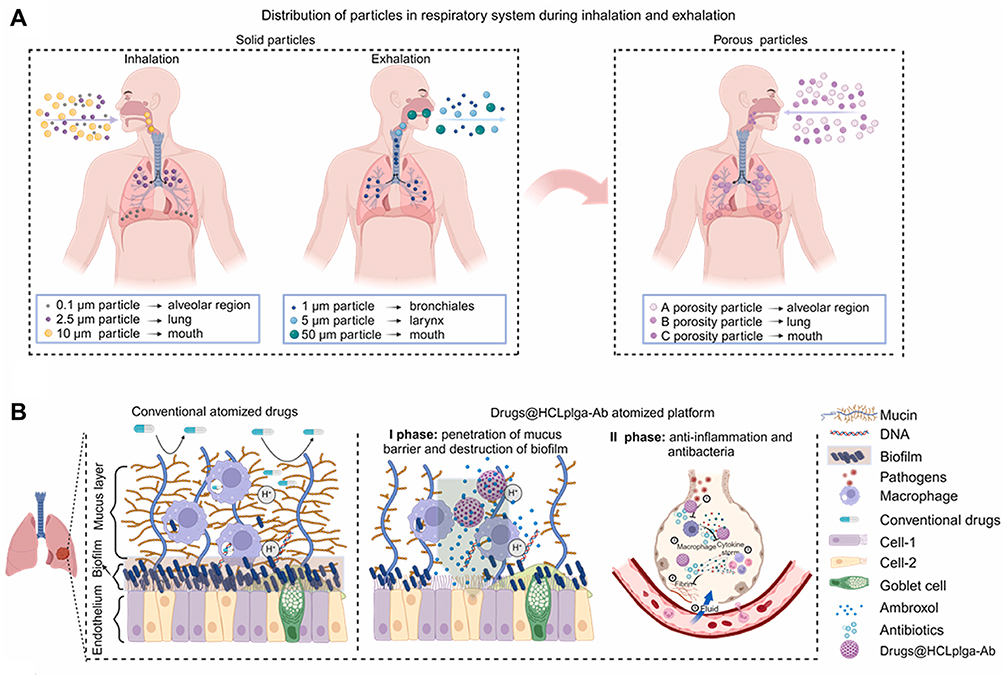 |
Figure 8 Schematic illustration of a honeycomb-inspired porous microsphere as an inhalable drug delivery platform. (A) Particle deposition in the respiratory tract depends on aerodynamic size, which is tunable by adjusting microsphere porosity, enabling targeted lung delivery. (B) Sequential drug release: The inhalable dry powder aerosol penetrates the mucus barrier and disrupts biofilms during the first phase, followed by anti-inflammatory and antibacterial effects in the second phase.72 Reprinted with permission from Biomaterials, 322 (2025) 123401. Copyright 2025, with permission from Elsevier. |
To address metastatic lung cancer, porous PLGA microspheres fabricated via double emulsion/solvent evaporation were employed for the inhalational co-delivery of icariin (ICA) and miR-23b (Figure 9).73 These microspheres exhibited favorable aerodynamic properties, high drug loading and encapsulation efficiencies, and sustained release kinetics. Results demonstrated that porous PLGA microspheres serve as an effective inhalation platform for combined drug/gene delivery, highlighting their potential for treating lung cancer and other pulmonary diseases. Following inhalation, the microspheres directly deposited in lung tissue, achieving elevated local concentrations and controlled release, which enhanced therapeutic efficacy while minimizing systemic toxicity. Furthermore, the biodegradable and low-toxicity nature of PLGA underpins the safety and clinical feasibility of this system. This delivery strategy holds promise for developing novel therapeutic approaches against lung cancer and related respiratory disorders.
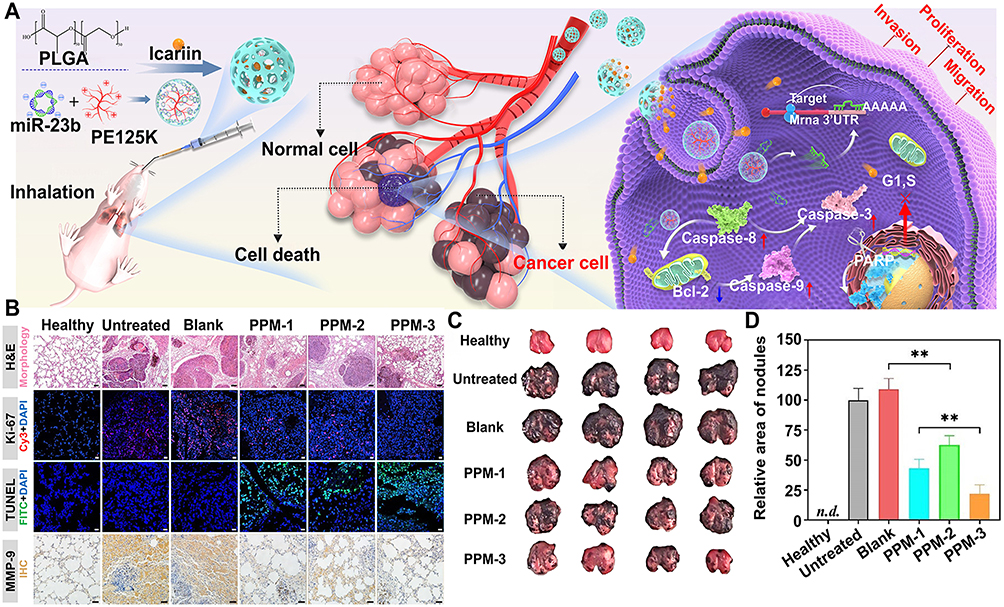 |
Figure 9 (A) Preparation and atomization of porous PLGA microspheres. Porous PLGA microspheres harboring icariin and PEI/miR-23b nanoparticles were prepared by double emulsification/solvent evaporation method. They could be well inhaled and deposited in the lungs after the proper aerolization, thereby obtaining favorable efficacy in the treatment of metastatic lung cancer. (B) H&E staining, Ki-67 and TUNEL immunofluorescence analysis, and IHC analysis of MMP-9 expression in melanoma metastatic lung tissue after treatment with different porous PLGA microspheres. Black scale bar: 100μm; White scale bar: 20μm. (C) Lung photos obtained from mice treated with different PLGA microspheres. (D) Relative area of melanoma nodules. Data were presented as mean ± SD (n = 4, n.d. not determined, **P < 0.01).73 Reprinted with permission from Asian Journal of Pharmaceutical Sciences, 20 (2025) 101008. Copyright 2025, with permission from Elsevier. |
Beyond lung cancer applications, inhalable swellable microspheres were explored for asthma therapy.74 The study developed a system for the concomitant pulmonary delivery of naringenin (NRG) and doxofylline (DOX). The formulation involved loading NRG onto glycerol tristearate-based solid lipid nanoparticles (NRG SLN), which were then co-encapsulated with DOX into chitosan-tripolyphosphate-based swellable microspheres (NRG SLN DOX sMS). Comprehensive characterization confirmed excellent swelling behavior and favorable aerodynamic properties. In a murine asthma model, the system significantly reduced serum bicarbonate levels and eosinophil counts while improving respiratory flow, tidal volume, and bronchial wall integrity compared to asthmatic controls. Collectively, this inhalable dual-drug platform represents a promising strategy for effective asthma management, offering a novel approach to co-deliver therapeutics locally, potentially enhancing efficacy while minimizing systemic side effects. Other researches on the treatment of lung diseases by inhalable microspheres were summarized in Table 3.
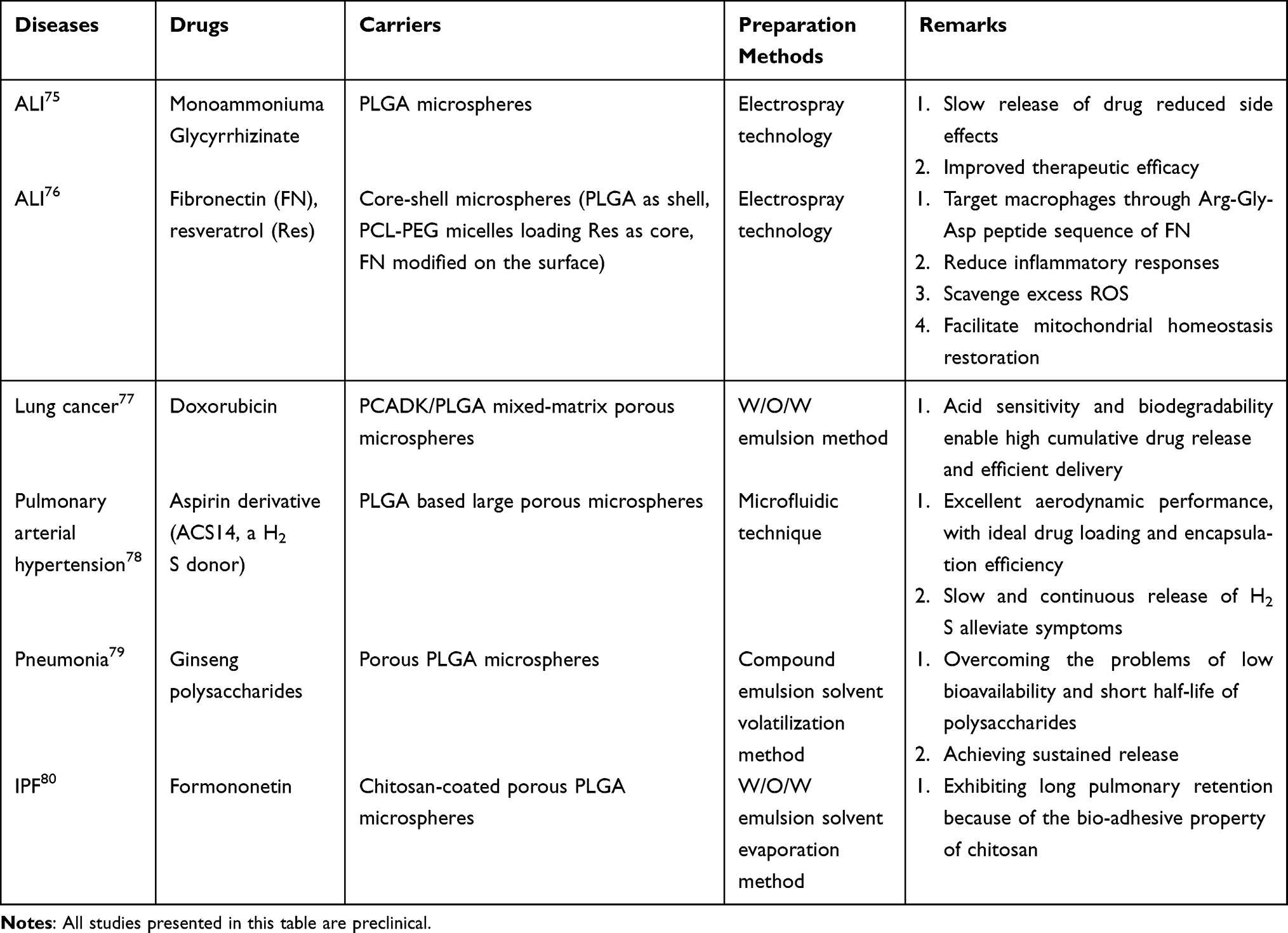 |
Table 3 Summary of Microspheres for Treating Pulmonary Diseases |
Biomimetic Platforms
Biomimetic inhalation platforms are a class of inhalable formulations engineered through biomimetic strategies that mimic biological substances or structures, such as cell membranes or pulmonary surfactants. They are designed with optimized physicochemical properties, most notably a particle size ranging from 1 to 1000 nm. This size range facilitates effective lung deposition while enabling the particles to evade clearance by alveolar macrophages. A neutrophil membrane-modified inhalable nanoparticle (LVX@PLGA@Mem) was developed for the treatment of COPD (Figure 10).81 The nanocarrier was constructed by coating levofloxacin (LVX)-loaded PLGA nanoparticles with a neutrophil membrane, endowing it with mucus-penetrating, anti-inflammatory, and antibacterial capabilities. The membrane coating preserved most native proteins and functions. Its near-neutral surface charge reduced electrostatic repulsion with mucus, enhancing penetration of the mucosal barrier. Moreover, targeting proteins on the membrane enabled active migration to inflammatory sites, improving pulmonary drug distribution and retention. These nanoparticles also evaded immune cell phagocytosis, prolonging their circulation time. Experimental results demonstrated that this system effectively alleviated COPD symptoms by reducing pro-inflammatory cytokines, inflammatory immune cells, and bacterial load. Its unique combination of mucus penetration, anti-inflammatory, and antibacterial actions highlights its therapeutic potential for COPD. Furthermore, the nanoparticles exhibited good biocompatibility and low systemic toxicity, supporting their translational prospects. This work provides an innovative nanomedicine-based strategy for COPD management, with the potential to enhance therapeutic outcomes and patient compliance.
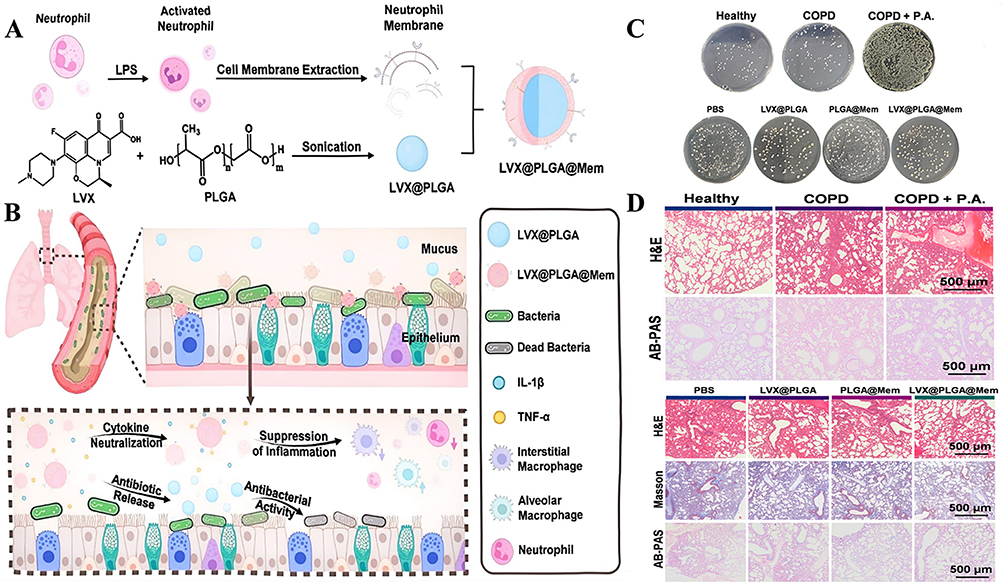 |
Figure 10 (A) Schematic diagram illustrating the fabrication process of LVX@PLGA@Mem. (B) its application for treatment of bacteria-infected COPD. (C) Representative images of bacterial colonies after different treatments. (D) H&E, Masson and AB-PAS images of lungs after different treatments.81 Reprinted with permission from Journal of Controlled Release, 381 (2025) 113648. Copyright 2025, with permission from Elsevier. |
Wang et al reported a synergistic inhalation strategy for IPF treatment using pulmonary surfactant-biomimetic liposomes (PSBs).82 The team designed PSBs composed of DPPC/POPG/DPPG/CHO to mimic natural pulmonary surfactant (PS) transport, co-loading the ROS scavenger astaxanthin (AST) and the anti-fibrotic drug pirfenidone (PFD) for precise aerosol delivery (Figure 11). Results demonstrated that PSBs, by fusing with the endogenous pulmonary surfactant membrane, efficiently targeted alveolar epithelial cells (AECs). Subsequently, released PFD penetrated the lung tissue barrier, significantly improving lung function, reducing collagen deposition and inflammatory factors, and promoting repair of damaged AECs in IPF mouse models. This study pioneers the use of the pulmonary surfactant recycling mechanism for cooperative drug delivery, offering a novel targeted platform for IPF. By optimizing PSB composition and delivery, this strategy may overcome the limited efficacy and systemic side effects of current anti-fibrotic drugs, presenting a potential clinical solution for IPF and informing new directions for inhaled therapies of other pulmonary diseases.
 |
Figure 11 (A) Schematic diagram of the synergistic therapeutic effect of PSBs on IPF. After nebulization inhalation, PSBs gradually fuse with the PS layer, promoting the adsorption of AECs on AST. Simultaneously, PFD is released bypassing the PS barrier and effectively enters the lungs. (B) The anti-fibrotic effect of PSBs@AST/PFD on bleomycin-induced pulmonary fibrosis in mice. (C) The anti-fibrotic effect of PSBs@AST/PFD on silicosis-induced mice.82 Reprinted with permission from Biomaterials, 303 (2023) 122404. Copyright 2023, with permission from Elsevier. |
The field of biomimetic inhalation for pulmonary disease therapy continues to advance with innovative delivery technologies. By mimicking endogenous substances or structures, inhalable formulations with tailored properties can be engineered to achieve targeted delivery and synergistic effects. Concurrently, cell-derived platforms are expanding the scope of this approach. For instance, the clinical potential of nebulized extracellular vesicles from human umbilical cord mesenchymal stem cells (hUCMSC-EVs) for treating pulmonary fibrosis was evaluated.83 Through a rigorous quality control system, high-quality hUCMSC-EVs were produced and comprehensively characterized by miRNA, protein, and metabolite profiles. In murine models, nebulized hUCMSC-EVs predominantly accumulated in the lungs, markedly ameliorating bleomycin-induced fibrosis: survival increased from 20% to 80%, lung volume recovered, tissue damage was alleviated, and oxygenation and lung function improved. A subsequent Phase I trial involving 24 randomized patients demonstrated good tolerance to nebulized hUCMSC-EVs with no serious adverse events. Patients receiving hUCMSC-EVs combined with standard care showed significant improvements in lung function and respiratory health. Notably, two patients with advanced post-inflammatory fibrosis exhibited marked regression on serial CT scans (Figure 12). These findings indicate the potential of nebulized hUCMSC-EVs as a novel therapeutic strategy for pulmonary fibrosis. However, further large-scale trials are warranted to confirm their long-term safety and efficacy. Other researches on the treatment of lung diseases by inhalable biomimetic nanoparticles were summarized in Table 4.
 |
Figure 12 (A) Process roadmap for the preparation of hUCMSC-EVs. (B) Representative histological lung sections of mice stained with H&E and Masson trichrome 21 days after injury. (C) Representative HRCT images of the lungs of three participants.83 Reprinted with permission from Signal Transduction and Targeted Therapy, 10 (2025) 179. Copyright 2025, with permission from Springer Nature. |
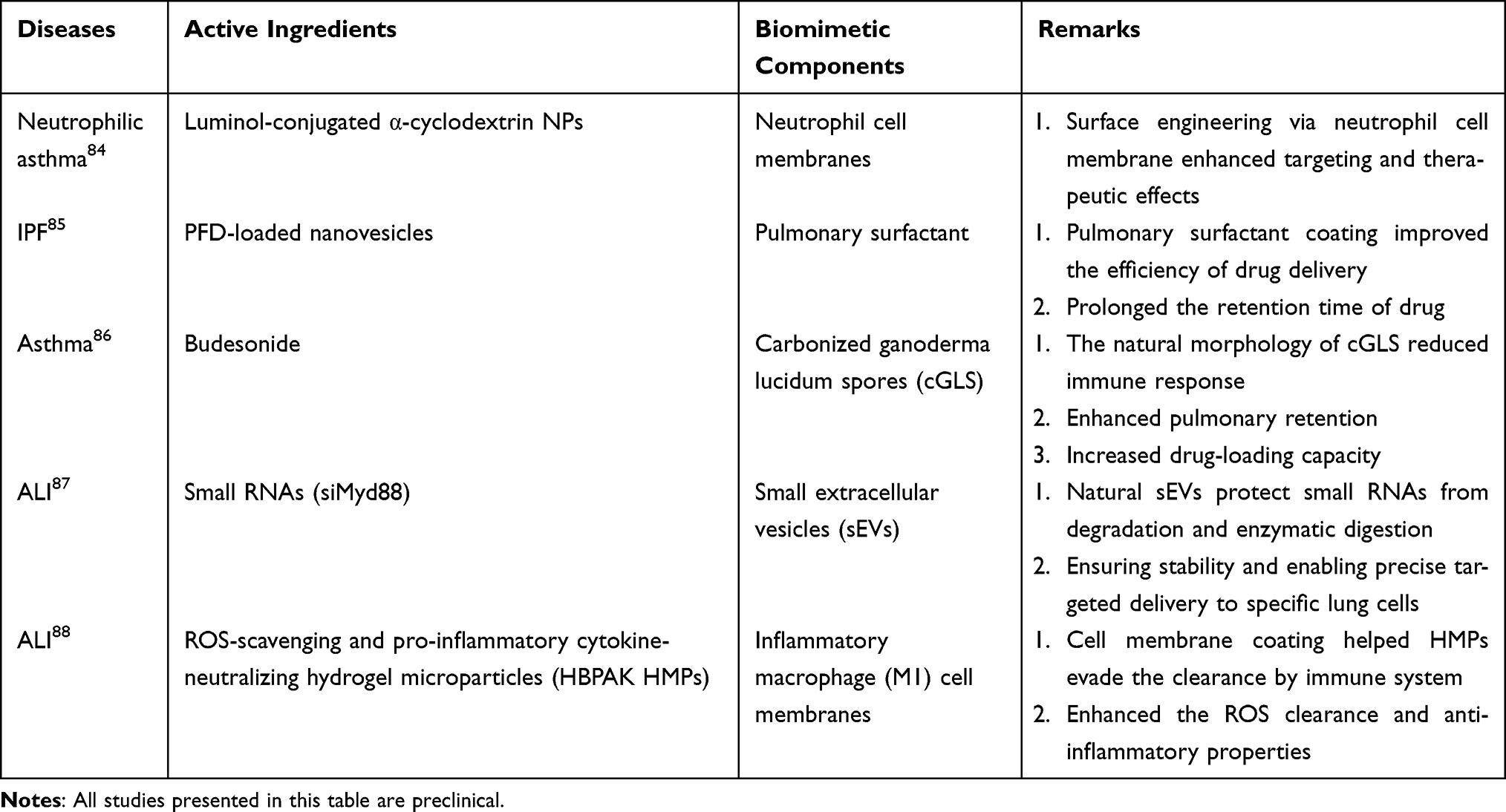 |
Table 4 Summary of Inhalable Biomimetic Nanoparticles for Treating Pulmonary Diseases |
Others
Beyond the prominent roles played by nanoparticles, liposomes, microspheres, and biomimetic preparations in treating pulmonary diseases, other innovative inhalation strategies continue to emerge, such as gel-based and dry powder inhalers (DPIs). These systems enrich the repertoire of inhalation formulations, offering novel therapeutic perspectives. Gel-based inhalers can enhance bioavailability and reduce systemic side effects. Through specific preparation methods, they can be engineered to possess multi-stimuli responsiveness, as well as synergistic antioxidant and anti-inflammatory efficacy.89–91 DPIs often prepared via technologies like spray drying, address challenges related to drug stability, hepatic metabolism, and oral bioavailability. They facilitate direct drug deposition in the deep lung, thereby improving local bioavailability and minimizing systemic risks.92–94 Furthermore, innovative formulations such as inclusion complexes and advanced aerosol systems contribute multi-faceted therapeutic effects. Collectively, these developments inject new vitality into pulmonary disease treatment and broaden the development pathways for novel inhalation therapies. The details were summarized in Table 5.
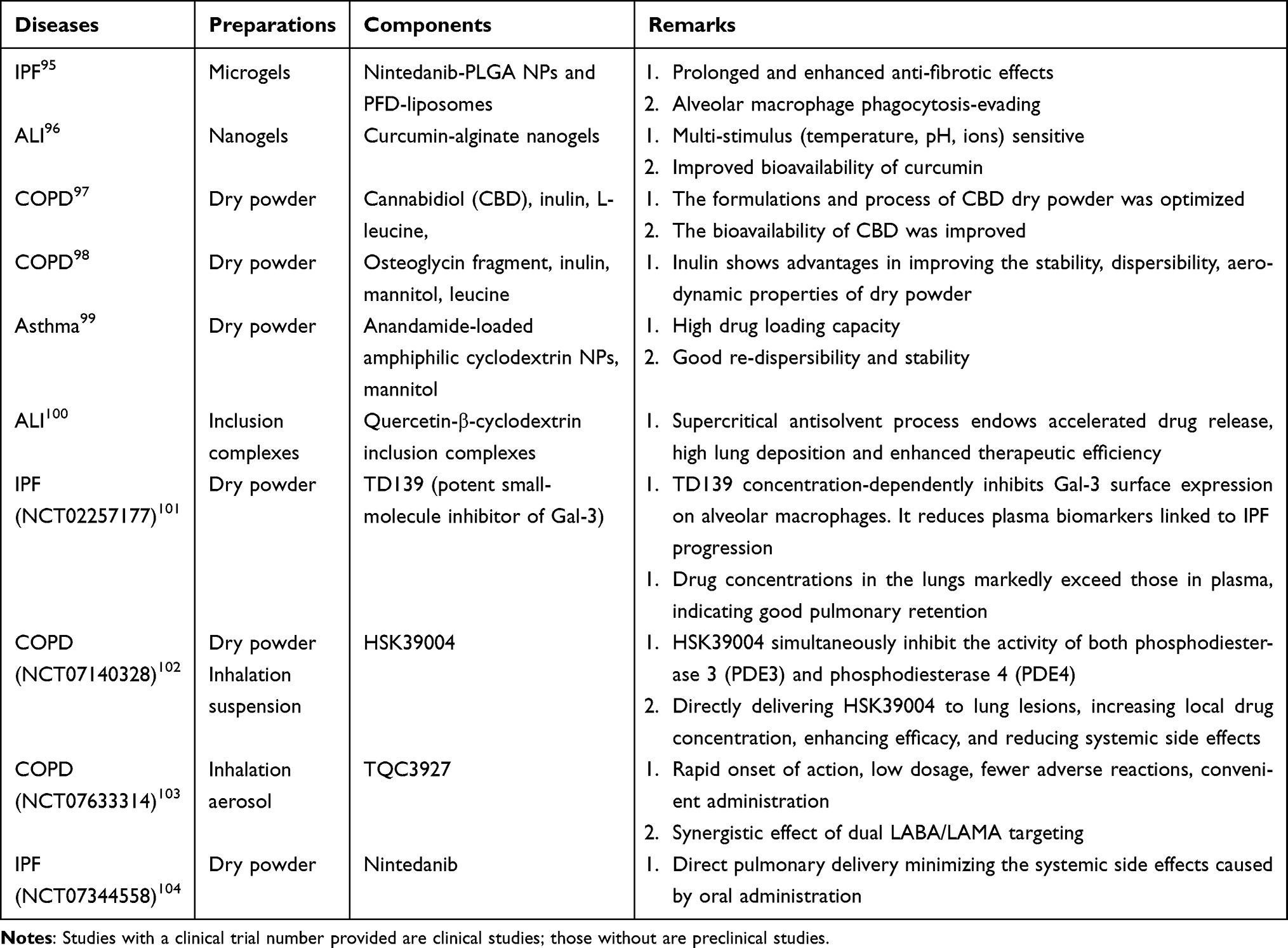 |
Table 5 Summary of Other Inhalation Preparations for Treating Pulmonary Diseases |
Discussion
Although inhalation platforms hold great promise, their clinical translation still faces a series of critical hurdles that call for a more balanced and in-depth examination. Beyond the requirements of precise delivery to diseased lung regions, several other core bottlenecks (eg., dependence on device handling, limited pulmonary retention time) in the translation process are often underestimated. Variability in airway deposition, influenced by breathing patterns, airway geometry, and disease state, leads to unpredictable dose distribution. Meanwhile, the viscous mucus barrier, rapid mucociliary clearance, and phagocytic clearance by alveolar macrophages further shorten the effective residence time of the drug at the target site. Differences in inhaler device design and inadequate patient adherence frequently cause significant deviations between the actual delivered dose and the intended dose, exacerbating uncertainty in therapeutic efficacy. In terms of long-term safety, greater vigilance is required for risks that may emerge after repeated administration, such as cumulative toxicity, immunogenicity, excessive nanocarrier burden on alveolar macrophages, local irritation, and even chronic lung injury. These factors constitute major barriers to bench-to-bedside translation.
Notably, nanoscale inhaled formulations have entered the market recently, providing an important window for evaluating the real-world performance of such platforms. For example, amikacin liposome inhalation suspension has demonstrated targeted therapeutic advantages in refractory pulmonary mycobacterial infections. However, its clinical application has also revealed potential concerns such as local irritation (eg., coughing, hemoptysis) and long-term lipid loading in macrophages,105–107 indicating that even marketed products still have room for improvement in delivery efficiency, mucus penetration, and long-term safety. Moreover, scaling up nano-inhaled formulations from the laboratory to industrial production is extremely challenging. It requires precise control of particle size, drug loading, and release behavior under large-scale conditions, while ensuring batch-to-batch consistency and sterility requirements. Processes such as spray drying and microfluidics are prone to particle aggregation, degradation, or polymorphic transformation during scale-up, creating another barrier to product translation.
Conclusion and Prospect
Pulmonary diseases, including COPD, asthma, pneumonia, pulmonary fibrosis, and lung cancer, present a serious threat to human health. While conventional therapies have certain limitations, inhalation formulations have emerged as an effective strategy for the treatment of these conditions, owing to their ability to achieve uniform lung distribution, rapid onset of action, high bioavailability, and avoidance of hepatic first-pass metabolism. This article reviews recent advances in novel inhalation drug delivery systems, with a focus on cutting-edge formulations such as nanoparticles, liposomes, microspheres, and biomimetic inhalers. By leveraging nanotechnology, advanced carrier materials, and biomimetic strategies, these novel systems significantly enhance drug stability, lung deposition efficiency, and targeting capability. They can also effectively overcome physiological barriers such as mucus, achieve sustained and controlled drug release, and ultimately improve therapeutic outcomes while reducing dosing frequency. Furthermore, other innovative inhalation platforms, including gel-based formulations, continue to broaden the scope and potential of inhalation therapy.
Despite their promising prospects, the clinical translation of inhalation formulations still faces several challenges. However, technological advancements, significant clinical demand, the rise of personalized medicine, and supportive regulatory policies collectively provide strong momentum for the innovation and clinical adoption of these systems. Looking ahead, the future development of inhalation therapy will achieve breakthroughs by deeply integrating nanoengineering, biomimetic design, and smart devices, building on existing experience and lessons from current obstacles. To overcome bottlenecks such as the mucus barrier, macrophage phagocytosis, and rapid mucociliary clearance, cell membrane-coated nanoparticles, exosome-based carriers, and smart nanosystems capable of sensing the pathological microenvironment and releasing drugs in response are expected. Smart inhaler devices need to be deeply integrated with formulation properties to address variability in patient handling. By recognizing breathing patterns in real time and providing feedback, they will ensure controllable aerosol deposition even in the presence of variations in airway geometry, truly establishing an integrated “device-formulation-patient” precision delivery system. At the industrialization level, the combination of continuous spray drying, highly reproducible microfluidic processes, and AI-driven process analytical technology will effectively overcome the core challenges, thereby supporting the commercial translation of personalized inhalation regimens. On this basis, inhalation therapy is poised to progress from broad-spectrum drug delivery to intelligent, personalized targeted interventions against specific pathological microenvironments in diseases, ultimately reshaping the overall landscape of pulmonary disease treatment. Notably, the application scope of inhalation delivery is expanding beyond pulmonary conditions, demonstrating considerable potential for treating systemic diseases (eg., diabetes,108,109 Parkinson’s disease110,111), intervening in central nervous system disorders (eg., depression, anxiety),112,113 and even enabling novel approaches in cell therapy and other cutting-edge areas.114–117
In summary, the ongoing development and innovation of advanced inhalation formulations are poised not only to transform the clinical management of lung diseases but also to open new therapeutic avenues for a broader range of disorders, ultimately benefiting a larger patient population worldwide.
Author Contributions
Qixiong Zhang and Shanshan Li were responsible for the design of conception and critically reviewing the article. Siyu Zhou, Shashan Ran and Fang Zhang contributed to the formation of the draft of the manuscript. Haotian Ma and Chunling Jiang are responsible for the design of figures in the manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by National Natural Science Foundation of China [82404874], Natural Science Foundation of Sichuan [2026NSFSC0626, 2025ZNSFSC1733], Scientific and Technological Innovation Team for Qinghai-Tibetan Plateau Research in Southwest Minzu University [2024CXTD15], Sichuan Province Traditional Chinese Medicine Research Project [25MSZX428], Dazhou Science and Technology Project [25YYJC0026], and Dazhou Traditional Chinese Medicine Research Project [2025LHZRZD02].
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Kim V, T J, Rogers G, Criner J. New concepts in the pathobiology of chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2008;5(4).
2. Lambrecht BN, Hammad H, Fahy JV. The cytokines of asthma. Immunity. 2019;4:50. doi:10.1016/j.immuni.2019.05.005
3. Singh V, Aneja S. Pneumonia–management in the developing world. Paediatric Respiratory Rev. 2011;12(1):52–24. doi:10.1016/j.prrv.2010.09.011
4. Noble PW, Barkauskas CE, Jiang D. Pulmonary fibrosis: patterns and perpetrators. J Clin Invest. 2012;122(8):2756–2762. doi:10.1172/JCI60323
5. Tanoue LT, Matthay RA, Matthay RA. Lung cancer: epidemiology, etiology, and prevention. Clinics Chest Med. 2011;32:605–644. doi:10.1016/j.ccm.2011.09.001
6. Nasim F, Sabath B, Eapen G. The medical clinics of North America. Lung Cancer. 103(3):463–473.
7. Bhutani M, Müllerová H, Patel D, et al. Disease burden and health-related outcomes of patients discharged from hospital following a COPD exacerbation in the United States. Respir Med. 2025;248(c):108337. doi:10.1016/j.rmed.2025.108337
8. Wang Z, Cao W, You Z, et al. Factors influencing the prevalence and death rate of COPD: a pan-database ecological study covering 201 countries and regions from 1990 to 2021. EClinicalMedicine. 2025;86:000. doi:10.1016/j.eclinm.2025.103347
9. Richeldi L, Collard HR, Jones MG. Idiopathic pulmonary fibrosis. Lancet. 2017;389(10082):1941–1952. doi:10.1016/S0140-6736(17)30866-8
10. Spagnolo P, Kropski JA, Jones MG, et al. Idiopathic pulmonary fibrosis: disease mechanisms and drug development. Pharmacol Ther. 2021;222:107798. doi:10.1016/j.pharmthera.2020.107798
11. Soriano JB, Kendrick PJ, Paulson KR, GBD Chronic Respiratory Disease Collaborators. Prevalence and attributable health burden of chronic respiratory diseases, 1990-2017: a systematic analysis for the global burden of disease study 2017. Lancet Respir Med. 2020;8(6):585–596. doi:10.1016/S2213-2600(20)30105-3
12. Azarmi S, Roa WH, Löbenberg R. Targeted delivery of nanoparticles for the treatment of lung diseases. Adv Drug Deliv Rev. 2008;60(8):863–875. doi:10.1016/j.addr.2007.11.006
13. Hughes G, Toellner H, Morris H, Leonard C, Chaudhuri N. Real world experiences: pirfenidone and nintedanib are effective and well tolerated treatments for idiopathic pulmonary fibrosis. J Clin Med. 2016;5(9):78. doi:10.3390/jcm5090078
14. Rivera-Ortega P, Hayton C, Blaikley J, Leonard C, Chaudhuri N. Nintedanib in the management of idiopathic pulmonary fibrosis: clinical trial evidence and real-world experience. Ther Adv Respir Dis. 2018;12:1753466618800618. doi:10.1177/1753466618800618
15. Ruwanpura SM, Thomas BJ, Bardin PG. Pirfenidone: molecular mechanisms and potential clinical applications in lung disease. Am J Respir Cell Mol Biol. 2020;62(4):413–422. doi:10.1165/rcmb.2019-0328TR
16. Cheema S, Saddique MN, Jha A, et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis: a systematic review and meta-analysis. Heart Lung. 2025;73:114–122. doi:10.1016/j.hrtlng.2025.05.008
17. Jin Z, Gao Q, Wu K, Ouyang J, Guo W, Liang X-J. Harnessing inhaled nanoparticles to overcome the pulmonary barrier for respiratory disease therapy. Adv Drug Deliv Rev. 2023;202:115111. doi:10.1016/j.addr.2023.115111
18. Xu W, Ye J, Cao Z, Zhao Y, Zhu Y, Li L. Glucocorticoids in lung cancer: navigating the balance between immunosuppression and therapeutic efficacy. Heliyon. 2024;10(12):e32357. doi:10.1016/j.heliyon.2024.e32357
19. Wood GC. Aerosolized antibiotics for treating hospital-acquired and ventilator-associated pneumonia. Expert Rev Anti Infect Ther. 2011;9(11):993–1000. doi:10.1586/eri.11.126
20. Mangal S, Gao W, Li T, Zhou QT. Pulmonary delivery of nanoparticle chemotherapy for the treatment of lung cancers: challenges and opportunities. Acta Pharmacol Sin. 2017;38(6):782–797. doi:10.1038/aps.2017.34
21. Jain H, Bairagi A, Srivastava S, Singh SB, Mehra NK. Recent advances in the development of microparticles for pulmonary administration. Drug Discov Today. 2020;25(10):1865–1872. doi:10.1016/j.drudis.2020.07.018
22. Abdelaziz HM, Gaber M, Abd-Elwakil MM, et al. Inhalable particulate drug delivery systems for lung cancer therapy: nanoparticles, microparticles, nanocomposites and nanoaggregates. J Control Release. 2018;269:374–392. doi:10.1016/j.jconrel.2017.11.036
23. El-Sherbiny IM, El-Baz NM, Yacoub MH. Inhaled nano- and microparticles for drug delivery. Glob Cardiol Sci Pract. 2015;2015:2. doi:10.5339/gcsp.2015.2
24. Liu Q, Guan J, Qin L, Zhang X, Mao S. Physicochemical properties affecting the fate of nanoparticles in pulmonary drug delivery. Drug Discov Today. 2020;25(1):150–159. doi:10.1016/j.drudis.2019.09.023
25. Hu Y, Sheng Y, Liu P, Sun J, Tang L. The pharmacokinetics and tissue distribution of curcumin following inhalation administration in rats-a comparative analysis with oral and intravenous routes. Biomed Chromatogr. 2024;38(12):e6003. doi:10.1002/bmc.6003
26. Li Z, Wang C, Xu H, et al. Three-compartment pharmacokinetics of inhaled and injected sinapine thiocyanate manifest prolonged retention and its therapeutics in acute lung injury. Pharmaceutics. 2025;17(7):909. doi:10.3390/pharmaceutics17070909
27. Ito T, Suzuki T, Sakai Y, et al. Engineered ACE2 decoy in dry powder form for inhalation: a novel therapy for SARS-CoV-2 variants. Mol Ther Methods Clin Dev. 2025;33(2):101459. doi:10.1016/j.omtm.2025.101459
28. Jin W, Yang H, Zhang M, et al. Inhalable cyclodextrin metal-organic framework dry powder enhanced direct pulmonary delivery of paclitaxel for the treatment of lung cancer. J Drug Delivery Sci Technol. 2024;101(No. Pt.B):106310. doi:10.1016/j.jddst.2024.106310
29. Mei C, Cai X, Li P, et al. Preparation and comprehensive preclinical study of peramivir inhalation solution: achieving accurate drug delivery. Biomed Pharmacother. 2025;186:118029. doi:10.1016/j.biopha.2025.118029
30. Yuan M, Wang J, Lakerveld R, et al. Advanced particle technologies in the preparation of dry powders for inhalation. Particuology. 2025;102:118–140. doi:10.1016/j.partic.2025.04.007
31. Scaranti M, Cojocaru E, Banerjee S, Banerji U. Exploiting the folate receptor α in oncology. Nat Rev Clin Oncol. 2020;17(6):349–359. doi:10.1038/s41571-020-0339-5
32. Wu Y, Xu J, Chen J, Zou M, Rusidanmu A, Yang R. Blocking transferrin receptor inhibits the growth of lung adenocarcinoma cells in vitro. Thorac Cancer. 2018;9(2):253–261. doi:10.1111/1759-7714.12572
33. Kwon YW, Jo HS, Bae S, et al. Application of proteomics in cancer: recent trends and approaches for biomarkers discovery. Front Med Lausanne. 2021;8:747333. doi:10.3389/fmed.2021.747333
34. Batool S, Sohail S, Ud Din F, et al. A detailed insight of the tumor targeting using nanocarrier drug delivery system. Drug Deliv. 2023;30(1):2183815. doi:10.1080/10717544.2023.2183815
35. Nan Y. Lung carcinoma therapy using epidermal growth factor receptor‑targeted lipid polymeric nanoparticles co‑loaded with cisplatin and doxorubicin. Oncol Rep. 2019;42(5):2087–2096. doi:10.3892/or.2019.7323
36. Narmani A, Ganji S, Amirishoar M, Jahedi R, Kharazmi MS, Jafari SM. Smart Chitosan-PLGA nanocarriers functionalized with surface folic acid ligands against lung cancer cells. Int J Biol Macromol. 2023;245:125554. doi:10.1016/j.ijbiomac.2023.125554
37. Guo M, Liang Y, Zhang M, et al. Lysosome-hijacking inhalable nanomimosa enhances ferroptosis for lung cancer therapy. J Control Release. 2025;386:114101. doi:10.1016/j.jconrel.2025.114101
38. Warthen JL, Lueckheide MJ. Peptides as targeting agents and therapeutics: a brief overview. Biomacromolecules. 2024;25(11):6923–6935. doi:10.1021/acs.biomac.4c00518
39. Yu Y, Ni M, Zheng Y, Huang Y. Airway epithelial-targeted nanoparticle reverses asthma in inhalation therapy. J Control Release. 2024;367:223–234. doi:10.1016/j.jconrel.2024.01.044
40. Ghasemi Z, Maleki A, Jafari T, Naghib SM. A review of multimodule stimuli-responsive chitosan-incorporated lipid-based micro/nanocarriers for drug delivery in cancer therapy: promises, outlooks, and prospects. Int J Biol Macromol. 2025;317(Pt 1):144587. doi:10.1016/j.ijbiomac.2025.144587
41. Liu X, He F, Liu M. New opportunities of stimulus-responsive smart nanocarriers in cancer therapy. Nano Materi Sci. 2024.
42. Jia R, Teng L, Gao L, et al. Advances in multiple stimuli-responsive drug-delivery systems for cancer therapy. Int J Nanomed. 2021;16:1525–1551. doi:10.2147/IJN.S293427
43. Tapponi S, Yusuf A, Alsaafin F, Hussain Z. Breaking barriers with ph-responsive nanocarriers: a new frontier in precision oncology. Int J Pharm. 2025;682:125931. doi:10.1016/j.ijpharm.2025.125931
44. Eldin MH, Arafa KK, Gamal O, Keshk S, El-Sherbiny IM. Inhalable pH-Responsive core-shell nanocarriers with PEGylated chitosan/alginate layer-by-layer coating for sequential drug release in lung cancer therapy. Int J Biol Macromol. 2025;307(Pt 1):141851. doi:10.1016/j.ijbiomac.2025.141851
45. Jeong Y, Shim YS, Jo YK, Cha HJ. Redox-activatable inhalable mucoadhesive proteinic nanotherapeutics for targeted treatment of lung cancer. Biomaterials. 2025;316:123004. doi:10.1016/j.biomaterials.2024.123004
46. Ren HM, Han L, Zhang L, et al. Inhalable responsive polysaccharide-based antibiotic delivery nanoparticles to overcome mucus barrier for lung infection treatment. Nano Today. 2022;(44):44.
47. Bourguignon T, Godinez-Leon JA, Pochet A, et al. Pulmonary delivery of clofoctol-loaded nanoparticles inhibits SARS-CoV-2 replication and reduces pneumonia. Int J Pharm. 2025;677:125634. doi:10.1016/j.ijpharm.2025.125634
48. Pang P, Liu W, Ma S, et al. Self-assembling natural flavonoid nanomedicines for alveolar macrophage reprogramming by restoring mitochondrial function in acute lung injury therapy. Chem Eng J. 2025;506:000. doi:10.1016/j.cej.2025.160171
49. Chen R, Dai X, Sun R, et al. Inhalable dexamethasone-loaded zwitterionic nanomicelles enabling effective penetration of the mucus barrier for acute lung injury treatment. Chem Eng J. 2010;520(000):12.
50. Dong H, Zhao Y, Li S, et al. An inhalable nanoparticle enabling virulence factor elimination and antibiotics delivery for pneumococcal pneumonia therapy. J Control Release. 2024;375:698–711. doi:10.1016/j.jconrel.2024.09.036
51. Zhang R, Wu C, Yu L, Peng C, Li S, Kuai R. Low-dose inhalable amino acid-modified multilamellar nanoparticles activate sting for safe and effective regression of lung metastases. J Control Release. 2025;386:114061. doi:10.1016/j.jconrel.2025.114061
52. Li Y, Li H, Hu Z, et al. Phosphatidylserine-decorated delivery platform helps alleviate acute lung injury via potentiating macrophage targeting. J Lipid Res. 2025;66(5):100799. doi:10.1016/j.jlr.2025.100799
53. Li Z, Lei H, Hu J, et al. Inhaled pH-responsive polymyxin b-loaded albumin nanoparticles against pneumonia caused by carbapenem resistant Klebsiella pneumoniae. Mater Today Bio. 2025;31:101590. doi:10.1016/j.mtbio.2025.101590
54. Peng J, Wang Q, Sun R, Zhang K, Chen Y, Gong Z. Phospholipids of inhaled liposomes determine the in vivo fate and therapeutic effects of salvianolic acid B on idiopathic pulmonary fibrosis. J Control Release. 2024;371:1–15. doi:10.1016/j.jconrel.2024.05.026
55. Chen X, Liu Q, Yu B, et al. Phosphatidylserine decorated inhalable immunostimulants to eradicate pulmonary metastasis through alveolar macrophage polarization and phagocytosis restoration in situ. Nano Today. 2025;61.
56. Yang M-Y, Lin Y-J, Han -M-M, et al. Pathological collagen targeting and penetrating liposomes for idiopathic pulmonary fibrosis therapy. J Control Release. 2022;351:623–637. doi:10.1016/j.jconrel.2022.09.054
57. Ivanova V, Garbuzenko OB, Reuhl KR, Reimer DC, Pozharov VP, Minko T. Inhalation treatment of pulmonary fibrosis by liposomal ProstaglandinE2. Eur J Pharm Biopharm. 2013;84(2):335–344. doi:10.1016/j.ejpb.2012.11.023
58. Jiang L, Guo P, Ju J, Zhu X, Wu S, Dai J. Inhalation of L-arginine-modified liposomes targeting M1 macrophages to enhance curcumin therapeutic efficacy in ALI. Eur J Pharm Biopharm. 2023;182:21–31. doi:10.1016/j.ejpb.2022.11.017
59. Han -M-M, Tang L, Huang B, et al. Inhaled Nanoparticles for treating idiopathic pulmonary fibrosis by inhibiting honeycomb cyst and alveoli interstitium remodeling. J Control Release. 2024;366:732–745. doi:10.1016/j.jconrel.2024.01.032
60. N E, Cw H, Jb F. Development and characterization of ph-sensitive zerumbone-encapsulated liposomes for lung fibrosis via inhalation route. Eur J Pharm Biopharm. 2025;207. doi:10.1016/j.ejpb.2024.114599
61. Liu J, Wu Z, Liu Y, et al. ROS-responsive liposomes as an inhaled drug delivery nanoplatform for idiopathic pulmonary fibrosis treatment via Nrf2 signaling. J Nanobiotechnol. 2022;20(1):213. doi:10.1186/s12951-022-01435-4
62. Zhang Q, Li G, Zhao G, et al. Preparation and evaluation of inhalable S-allylmercapto-N-acetylcysteine and nintedanib Co-loaded liposomes for pulmonary fibrosis. Eur J Pharm Sci. 2024;197:106779. doi:10.1016/j.ejps.2024.106779
63. Liao R, Sun ZC, Wang L, et al. Inhalable and bioactive lipid-nanomedicine based on bergapten for targeted acute lung injury therapy via orchestrating macrophage polarization. Bioact Mater. 2024;43:406–422. doi:10.1016/j.bioactmat.2024.09.020
64. Sun Z-C, Liao R, Xian C, et al. Natural pachypodol integrated, lung targeted and inhaled lipid nanomedicine ameliorates acute lung injury via anti-inflammation and repairing lung barrier. J Control Release. 2024;375:300–315. doi:10.1016/j.jconrel.2024.09.013
(65.) Zambon SpA. A Phase III clinical trial to demonstrate efficacy / safety of liposomal cyclosporine A + standard of care (SoC) vs SoC alone in treating chronic lung allograft dysfunction / bronchiolitis obliterans in patients post single lung transplant. Clinical trial registration NCT03657342; clinicaltrials.gov. 2025. Available from: https://clinicaltrials.gov/study/NCT03657342.
(66.) Radboud University Medical Center. Nebulised lIposomal aMphotericin B in Chronic pUlmonary aSpergillosis: a deposition study. Clinical trial registration NCT07530263; clinicaltrials.gov. 2026. Available from: https://clinicaltrials.gov/study/NCT07530263.
67. Ruan L, Su M, Qin X, et al. Progress in the application of sustained-release drug microspheres in tissue engineering. Mater Today Bio. 2022;16:100394. doi:10.1016/j.mtbio.2022.100394
68. Yj L, Ms K. Advances in drug-loaded microspheres for targeted, controlled, and sustained drug delivery: potential, applications, and future directions. Biomed Pharmacothe. 2025;189. doi:10.1016/j.biopha.2025.118244
69. Cadinoiu AN, Rata DM, Atanase LI, et al. Physicochemical characterization and in vitro evaluation of peptide-functionalized microspheres based on carboxymethyl chitosan and poly(vinyl alcohol) as promising pulmonary drug delivery system. Appl Mater Today. 2025;44.
70. Bao S, Zou Y, Firempong CK, et al. Preparation and evaluation of sustained release pirfenidone-loaded microsphere dry powder inhalation for treatment of idiopathic pulmonary fibrosis. Eur J Pharm Sci. 2023;188:106509. doi:10.1016/j.ejps.2023.106509
71. Xiong B, Chen Y, Liu Y, Hu X, Han H, Li Q. Artesunate-loaded porous PLGA microsphere as a pulmonary delivery system for the treatment of non-small cell lung cancer. Colloids Surf B Biointerfaces. 2021;206:111937. doi:10.1016/j.colsurfb.2021.111937
72. Cheng D, Pan T, Wang X, et al. An advanced inhalable dry powder, mucus-penetrating aerosol platform: bridging andrographolide delivery with clinical translation. Biomaterials. 2025;322:123401. doi:10.1016/j.biomaterials.2025.123401
73. Xiong B, Shao X, Fang G, Dong M, Han H, Li Q. Porous PLGA microspheres for the inhalation delivery of icariin and mir-23b in the treatment of metastatic lung cancer. Asian J Pharm Sci. 2025;20(2):101008. doi:10.1016/j.ajps.2024.101008
74. Pareek A, Kothari R, Pareek A, et al. Development of a new inhaled swellable microsphere system for the dual delivery of naringenin-loaded solid lipid nanoparticles and doxofylline for the treatment of asthma. Eur J Pharm Sci. 2024;193:106642. doi:10.1016/j.ejps.2023.106642
75. Jin J, chen J, Shou X, et al. MAG-encapsulated PLGA microspheres for lipopolysaccharide-induced acute lung injury. J Drug Delivery Sci Technol. 2023;86:104632. doi:10.1016/j.jddst.2023.104632
76. Huang Y, Zhan M, Sun H, et al. Electrosprayed core-shell microspheres co-deliver fibronectin and resveratrol for combined treatment of acute lung injury. J Colloid Interface Sci. 2025;686:498–508. doi:10.1016/j.jcis.2025.01.249
77. Li W, Chen S, Zhang L, et al. Inhalable functional mixed-polymer microspheres to enhance doxorubicin release behavior for lung cancer treatment. Colloids Surf B Biointerfaces. 2020;196:111350. doi:10.1016/j.colsurfb.2020.111350
78. Zhang H, Hao L-Z, Pan J-A, et al. Microfluidic fabrication of inhalable large porous microspheres loaded with H2S-releasing aspirin derivative for pulmonary arterial hypertension therapy. J Control Release. 2021;329:286–298. doi:10.1016/j.jconrel.2020.11.060
79. Lan W, Tao L, Mao K, et al. Porous poly (lactic-co-glycolic acid) microspheres loaded with neutral and acidic ginseng polysaccharides ameliorate pneumonia in mice. Carbohydr Polym. 2025;362:123697. doi:10.1016/j.carbpol.2025.123697
80. Zhao C, Ji L, Wang X, et al. Intratracheal instillation of chitosan-coated formononetin-loaded porous microspheres prolongs lung retention and improves the treatment in bleomycin-induced pulmonary fibrosis. Eur J Pharm Sci. 2025;215:107347. doi:10.1016/j.ejps.2025.107347
81. Yu Q, Zhang Q, Zhu J, et al. Inhalable neutrophil-mimicking nanoparticles for chronic obstructive pulmonary disease treatment. J Control Release. 2025;381:113648. doi:10.1016/j.jconrel.2025.113648
82. Wang B, Gao Y, sun L, et al. Inhaled pulmonary surfactant biomimetic liposomes for reversing idiopathic pulmonary fibrosis through synergistic therapeutic strategy. Biomaterials. 2023;303:122404. doi:10.1016/j.biomaterials.2023.122404
83. Li M, Huang H, Wei X, et al. Clinical investigation on nebulized human umbilical cord msc-derived extracellular vesicles for pulmonary fibrosis treatment. Signal Transduct Target Ther. 2025;10(1):179. doi:10.1038/s41392-025-02262-3
84. Cai J, Tao H, Liu H, et al. Intrinsically bioactive and biomimetic nanoparticle-derived therapies alleviate asthma by regulating multiple pathological cells. Bioact Mater. 2023;28:12–26. doi:10.1016/j.bioactmat.2023.04.023
85. Kim CG, Jang M, Oh C, et al. Pulmonary surfactant-based pirfenidone-loaded nanovesicles for inhalation therapy of idiopathic pulmonary fibrosis. J Control Release. 2025;385:114005. doi:10.1016/j.jconrel.2025.114005
86. Tong M, Kuang X, Jiang Q, et al. Spore-inspired inhalation drug delivery system for asthma therapy. Bioact Mater. 2025;53:801–818. doi:10.1016/j.bioactmat.2025.07.045
87. Han Y, Zhu Y, Youngblood HA, et al. Nebulization of extracellular vesicles: a promising small RNA delivery approach for lung diseases. J Control Release. 2022;352:556–569. doi:10.1016/j.jconrel.2022.10.052
88. Song L, Zhai Z, Ouyang W, et al. Inhalation of macrophage membrane-coated hydrogel microparticles for inflammation alleviation of acute lung injury in vivo. Acta Biomater. 2025;192:409–418. doi:10.1016/j.actbio.2024.12.015
89. Su M, Zhu Y, Chen J, et al. Microfluidic synthesis of manganese-alginate nanogels with self-supplying H2O2 capability for synergistic chemo/chemodynamic therapy and boosting anticancer immunity. Chem Eng J. 2022;435:134926. doi:10.1016/j.cej.2022.134926
90. Zhu X, He Q, He S, et al. Facile manganese ion-coordination assembly of nanogels for synergistic cancer chemo–chemodynamic-immunotherapy. Chem Eng J. 2024;485:149752. doi:10.1016/j.cej.2024.149752
91. Fu W, Liu Y, Xia L, et al. A clinical pilot study on the safety and efficacy of aerosol inhalation treatment of IFN-κ plus TFF2 in patients with moderate COVID-19. EClinicalMedicine. 2020;25:100478. doi:10.1016/j.eclinm.2020.100478
92. Shi T, Jin M, Li H, et al. Inhaled nintedanib dry powder formulation for the treatment of idiopathic pulmonary fibrosis: pharmacodynamic and pharmacokinetic study. Int J Pharm. 2025;683:126088. doi:10.1016/j.ijpharm.2025.126088
93. Singh S, Francis F, Barsain M. Dry powder inhalation of nintedanib in dibasic calcium phosphate for targeting the lungs in pulmonary fibrosis. Mol Pharm. 2025;22(3):1471–1479. doi:10.1021/acs.molpharmaceut.4c01190
94. Lu P, Li J, Liu C, et al. Salvianolic acid B dry powder inhaler for the treatment of idiopathic pulmonary fibrosis. Asian J Pharm Sci. 2022;17(3):447–461. doi:10.1016/j.ajps.2022.04.004
95. Lee WT, Lee H, Kim J, et al. Alveolar macrophage phagocytosis-evading inhaled microgels incorporating nintedanib-PLGA nanoparticles and pirfenidone-liposomes for improved treatment of pulmonary fibrosis. Bioact Mater. 2024;33:262–278. doi:10.1016/j.bioactmat.2023.11.005
96. Cai J, Zhong H, Luo J, Huang X, Xu Q, Li P. Inhalable multi-stimulus sensitive curcumin-alginate nanogels for scavenging reactive oxygen species and anti-inflammatory co-ordination to alleviate acute lung injury. Int J Biol Macromol. 2024;283:137816. doi:10.1016/j.ijbiomac.2024.137816
97. Komal K, Chen S, Hanton LR, Glass M, Das SC. Preparation and in vitro characterization of inhalable cannabidiol dry powder for treating chronic obstructive pulmonary disease. Int J Pharm. 2025;682:125892. doi:10.1016/j.ijpharm.2025.125892
98. van der Koog L, Jansen EM, Elferink RAB, et al. Development of a stable inhalable dry powder formulation with osteoglycin fragment for alveolar epithelial repair. Int J Pharm. 2025;682:125913. doi:10.1016/j.ijpharm.2025.125913
99. Hübl A, Brettner FEB, Vogel-Kindgen S, et al. Inhalable spray-dried nano-in-microparticles encapsulating anandamide: a novel approach for the treatment of asthma. Int J Pharm. 2025;683:126014. doi:10.1016/j.ijpharm.2025.126014
100. Wang W, Liu Y, Zhang H, et al. Preparation of inhalable quercetin-β-cyclodextrin inclusion complexes using the supercritical antisolvent process for the prevention of smoke inhalation-induced acute lung injury. J CO2 Util. 2023;69:102414. doi:10.1016/j.jcou.2023.102414
101. Galecto Biotech AB. A placebo-controlled RCT in HV’s investigating the safety, tolerability and PK (Pharmacokinetic) of TD139, a galectin-3 inhibitor, followed by an expansion cohort treating subjects with Idiopathic Pulmonary Fibrosis (IPF). Clinical trial registration NCT02257177; clinicaltrials.gov. 2023. https://clinicaltrials.gov/study/NCT02257177.
102. Haisco Pharmaceutical Group Co. Ltd. A multicenter, randomized, double-blind, placebo-controlled, parallel-group phase II clinical study to evaluate the efficacy and safety of HSK39004 Dry powder inhaler and HSK39004 inhalation suspension in the treatment of Chronic Obstructive Pulmonary Disease (COPD). Clinical trial registration NCT07140328; clinicaltrials.gov. 2026. Available from: https://clinicaltrials.gov/study/NCT07140328.
103. Chia Tai Tianqing Pharmaceutical Group Co. Ltd. A Multicenter, Randomized, Open-Label, Active-Controlled Phase II Clinical Trial to Explore the Efficacy and Safety of Different Doses of TQC3927 Inhaled Powder in Patients With Chronic Obstructive Pulmonary Disease. Clinical trial registration NCT07633314; clinicaltrials.gov. 2026. Available from: https://clinicaltrials.gov/study/NCT07633314.
104. Mannkind Corporation. A randomized, double-blind, placebo-controlled, phase 1b clinical study of the safety, tolerability, and pharmacokinetics of MNKD-201 (nintedanib dry powder inhalation) in patients with idiopathic pulmonary fibrosis. Clinical trial registration NCT07344558; clinicaltrials.gov. 2026. Available from: https://clinicaltrials.gov/study/NCT07344558.
105. Dorgan D, Waweru C, Cocks K, et al. A simultaneous assessment of efficacy and safety of amikacin liposome inhalation suspension for refractory mycobacterium avium complex lung disease. Clin. Ther. 2026;48(7):610–614. doi:10.1016/j.clinthera.2026.04.007
106. Griffith DE, Eagle G, Thomson R, et al; CONVERT Study Group. Amikacin liposome inhalation suspension for treatment-refractory lung disease caused by mycobacterium avium complex (CONVERT). A prospective, open-label, randomized study. Am J Respir Crit Care Med. 2018;198(12):1559–1569. doi:10.1164/rccm.201807-1318OC
107. Yanagihara T, Osaki Y, Ikeda T, et al. Challenges and efficacy of amikacin liposome inhalation in real-world refractory mycobacterium avium complex pulmonary disease. Cureus. 2025;17(10):e95192. doi:10.7759/cureus.95192
108. Kugler AJ, Fabbio KL, Pham DQ, Nadeau DA. Inhaled technosphere insulin: a novel delivery system and formulation for the treatment of types 1 and 2 diabetes mellitus. Pharmacotherapy. 2015;35(3):298–314. doi:10.1002/phar.1555
109. Khan AB, Ahmad A, Ahmad S, et al. Comparative analysis of inhaled insulin with other types in type 1 diabetes mellitus: a systematic review and meta-analysis. Cureus. 2022;14(4):e23731. doi:10.7759/cureus.23731
110. Hu Y, Zhao Y, Mao Z, et al. Inhalation of acori tatarinowii rhizoma essential oil alleviates dyskinesia in parkinson’s disease rats through the regulation of neuroinflammation. J Ethnopharmacol. 2025;348:119705. doi:10.1016/j.jep.2025.119705
111. Paul M, Lau R. Potentials and challenges of levodopa particle formulation for treatment of parkinson’s disease through intranasal and pulmonary delivery. Adv Powder Technol. 2020;31(6):9. doi:10.1016/j.apt.2020.03.028
112. Feng M, Cheng S, Fang Y, et al. Augmentation of sevoflurane inhalation for treatment-resistant depression with different features: a case series. Asian J Psychiatr. 2023;82:103495. doi:10.1016/j.ajp.2023.103495
113. Song H, Yang A, Wang Y, Xu R, Hu W. Potential roles of inhalation aromatherapy on stress-induced depression by inhibiting inflammation in the peripheral olfactory system. Neurochem Int. 2025;186:105967. doi:10.1016/j.neuint.2025.105967
114. Chen S, Gao J, Zhang T. From mesenchymal stem cells to their extracellular vesicles: progress and prospects for asthma therapy. Asian J Pharm Sci. 2024;19(4):100942. doi:10.1016/j.ajps.2024.100942
115. Feng Y, Guo K, Jiang J, Lin S. Mesenchymal stem cell-derived exosomes as delivery vehicles for non-coding rnas in lung diseases. Biomed Pharmacother. 2024;170(000):13. doi:10.1016/j.biopha.2023.116008
116. He XY, Han MM, Zhao YC, et al. Surface-engineered mesenchymal stem cell for refractory asthma therapy: reversing airway remodeling. J Control Release. 2024;376:972–984. doi:10.1016/j.jconrel.2024.10.056
117. Niimi Y, Baljinnyam T, Fukuda S, et al. Effects of nebulized adipose-derived mesenchymal stem cells on acute lung injury following smoke inhalation in sheep. Int Immunopharmacol. 2023;123:110638. doi:10.1016/j.intimp.2023.110638
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.