Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Advance Care Plans and the Potentially Conflicting Interests of Bedside Patient Agents: A Thematic Analysis
Authors Craig DP ![]() , Ray R
, Ray R ![]() , Harvey D
, Harvey D ![]() , Shircore M
, Shircore M ![]()
Received 31 May 2021
Accepted for publication 15 July 2021
Published 6 August 2021 Volume 2021:14 Pages 2087—2100
DOI https://doi.org/10.2147/JMDH.S314664
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Denise P Craig,1 Robin Ray,2 Desley Harvey,3,4 Mandy Shircore5
1College of Medicine and Dentistry, James Cook University, Cairns, Queensland, Australia; 2College of Medicine and Dentistry, James Cook University, Townsville, Queensland, Australia; 3Health Practitioner Research Capacity Building, Cairns and Hinterland Hospital and Health Service, Cairns, Queensland, Australia; 4College of Healthcare Sciences, James Cook University, Cairns, Queensland, Australia; 5College of Business, Law and Governance, James Cook University, Cairns, Queensland, Australia
Correspondence: Denise P Craig Email [email protected]
Aim: People diagnosed with a neurodegenerative disorder often contend with a threat to independence and control, leading some to complete an advance care plan. Advance care plans are commonly associated with treatment limitations; however, key patient agents (such as doctors, allied health, nurses and family) may instead make temporal, best interests or good medical practice decisions on behalf of the patient. Accordingly, there is a need to better understand ancillary decision-maker’s perspectives, particularly of doctors.
Purpose: To explain how the potentially conflicting interests of bedside patient agents operates as a factor which influences doctors’ application of advance care plans of people with a neurodegenerative disorder.
Participants and Methods: Using a constructivist grounded theory informed thematic analysis, 38 semi-structured interviews were conducted with hospital-based doctors, allied health, nurses and family of people with a neurodegenerative disorder who had an advance care plan. Data were inductively analysed using open and focused coding.
Results: Analysis revealed two main themes: dynamics of discerning best interests; and avoiding conflict. Rather than applying advance care plans, doctors largely involved families to attempt best interests decision-making partnerships on patients’ behalf. Bedside agents demonstrated significant intra and interpersonal challenges associated with their roles as patient agents. Doctors appeared protective of families and patients with neurodegenerative disorder.
Conclusion: Although bedside agents value advance care plans, doctors often favour temporal healthcare decisions in consultation with family. We suggest there are limitations to the effectiveness of advance care plans in practice, with application typically only occurring close to death. Despite the intentions of advance care planning, bedside agents may still experience considerable dissonance.
Keywords: advance directive, consent, end of life, hospital doctors, living will, patient agency
Introduction
People with neurodegenerative disorders (PWND) such as dementia live with clear prospects of disabling cognitive decline.1 Consequently, PWND often contend with a threat to independence and control,2 leading some to exercise their agency by completing an Advance Care Plan (ACP). The genesis of formal advance care planning lies in complex medical, ethical and legal debates associated with the potential juxtaposition of medical decision-making and patient autonomy.3 The mid-1900s saw an escalation of societal expectations that individuals should be allowed autonomy in healthcare decisions, which led to guardianship laws intended to preserve this right.4 By the 1990s, legislation and structured ACPs had commenced in the USA where personal autonomy is an accepted cultural norm.4 ACPs are now widely promoted around the world to both enhance patient autonomy and protect doctors from litigation.5
In Australia, advance care planning frameworks vary between states. Since the inception of advance care planning, legislative changes and iterations of ACPs have occurred to facilitate communication of patient rights, preferences or directions.4 In the state of Queensland, legally binding Advance Health Directives [AHD] have been in use for almost two decades. In 2015 the Government of Queensland introduced a new, non-binding Statement of Choices form through which people may communicate important healthcare information intended as a guide to substitute decision-makers (SDMs). In November 2020, the Queensland AHD (now Version 5) was amended to include values-based guidance statements as adjuncts to healthcare consent or refusal directions.
Accordingly, competent adults in Queensland have two formalised ACP options available: Statement of Choices and AHD. Adults have the right to express their wishes, values and beliefs in a Statement of Choices and/or record binding healthcare directions within an AHD. By law, where a PWND has given directions within an AHD, matters related to the provision of care must be dealt with under the AHD. Both ACPs may be completed without medical advice despite requiring medical doctor certification. Collectively, these ACPs have been most associated with treatment limitations,6 suggesting that failure to incorporate ACPs in decision-making may be associated with patients receiving unwanted interventions.
Where an AHD does not address the clinical issue at hand, a SDM is required. SDMs are tasked with making decisions in the patient’s best interests, broadly meaning taking account of the patient’s wishes and acting in a way least restrictive of the patient’s rights.7,8 Yet, medical advice can be contradictory and people may be confronted by choices in which they have little or no expertise.9 Consequently, for SDMs such as family, best interests decision-making can be a fraught proposition associated with emotional burden such as stress, guilt and doubt.10 Not surprisingly, reliability of SDM input appears variable, with discrepancies between SDM and patient decisions well documented.11,12 Even in the most well intended judgements, decisions may reflect implicit bias and conflicting interests.10,11,13–15 What is incumbent upon SDMs, however, is an authentic effort to incorporate what is known about the patient’s wishes or directions, such as those recorded within an ACP.
Hospital-based clinicians such as doctors, allied health and nurses (AH/N) are critical agents in patients’ healthcare. All clinicians have a professional duty to act in the patients’ best interests and respect patients’ known views and wishes. Clinicians are ideally positioned to familiarise themselves with ACPs, raise awareness of ACP existence, and advocate for concordant care.16 In so doing, the focus of the inpatients’ hospitalisation may transcend the question of what is wrong with the patient, to what matters most to the patient. However, a recent scoping review of hospital doctors’ application of ACP17 to medical decision-making indicated that although doctors held largely positive attitudes towards ACPs, they prefer temporal decision-making and often do not read patients’ ACPs.
To understand more about the reasons behind doctors’ application of ACPs to treatment decisions of PWND, this study sought to hear the voices of bedside agents: doctors, AH/N and family or friends of PWND with an ACP. Data collection occurred during the novel coronavirus disease 2019 (COVID-19) pandemic, at which time increased attention to ACPs and patient preferences appeared evident.18–20 We defined ACP as a patient-owned, written statement, articulating future healthcare wishes or directions applicable only during incapacity to consent. The Queensland AHD in effect during data collection was Version 4 and the Statement of Choices was Version 5.1. (Please see Supplemental Information). In line with study aims, AHD and Statement of Choices are specified only where relevant to distinguish legislated applicability.
Materials and Methods
Aims
The findings presented in this paper constitute part of a broader constructivist grounded theory [CGT] research project exploring enablers and barriers to hospital doctors’ application of ACPs of incapacitated PWND. Consistent with CGT methodology, the research team commenced this study with broad aims rather than specific objectives. This paper provides a thematic analysis explaining how the potentially conflicting interests of bedside patient agents operates as a factor which influences ACP application.
Study Design
An inductive thematic analysis informed by the CGT approach of Charmaz21 was chosen for its capacity to help develop a new understanding of the underlying phenomena associated with this study. Grounded theory has been recommended for its suitability to explanations of phenomenon about which little is known.22,23 CGT21 methodology was used to inductively describe the experiences of doctors, AH/N, family and friends regarding healthcare decision-making for an incompetent PWND with an ACP. The purpose of using CGT was to work towards the development of a theoretical framework for understanding the complex human experience of applying an ACP to life and death decisions on behalf of a PWND who sought to preserve their autonomy. The resulting theory will be published separately.
Ethical Approvals
Multisite approvals were granted by Townsville Hospital and Health Service Human Research Ethics Committee (54125) and James Cook University (H7930). Participant access to professional support if distress occurred was incorporated into approvals. This paper was informed by the Consolidated Criteria for Reporting Qualitative Research (COREQ), and data were maintained in accordance with the Declaration of Helsinki.
Participants and Recruitment
Three participant groups who had direct experience with treatment decisions for PWND who had an ACP during incapacity to consent were invited: hospital doctors, AH/N, and family or friend advocates (henceforth “family”). Doctors were the primary focus of this study, with AH/N and family participants theoretically sampled to achieve wider perspectives. All participants received written and oral information about the study and they provided informed consent to interviews being digitally recorded and anonymised responses published.
Doctors, Allied Health and Nurses
Doctors and AH/N clinicians were recruited via health service newsletters, snowball referral and emails disseminated by heads of departments. All had treatment experience in the context of AHDs and a small number had experience in the context of a Statement of Choices. Purposive sampling was undertaken from units most associated with care at the end-of-life [EOL] included palliative care, emergency, geriatrics, intensive care, medical oncology.24 In line with theoretical sampling techniques, some specialties (such as neurology, general medicine, psychiatry, respiratory and renal) and disciplines (such as social workers, speech pathologists, dietitians and nurses) were invited to participate. Doctors from the respiratory and renal subspecialty declined participation. In this manuscript, AH/N and doctors are referred to collectively as “clinicians”, however disciplines are separated for interpretation of data where necessary.
Family
Family responded to invitations during support group presentations, social media posts, or snowball referrals. Family members were invited to speak about their experience of hospitalisation of someone meeting the PWND criteria during illness and incapacity to directly consent.
Data Collection and Analysis
The authors developed a semi-structured interview guide based on professional experience and research, to flexibly explore factors such as attitudes towards patient agency through ACPs, and barriers or enablers to applying the ACPs completed by PWND (see Figure 1). The guide was piloted across all groups, then amended iteratively as theoretical concepts emerged. Interviews were conducted across two health service districts by the first author [DC] and primary advisor [RR], face-to-face or via telephone or “MS TEAMS” online software and ranged from 20 to 70 minutes (mean of 51.8 minutes).
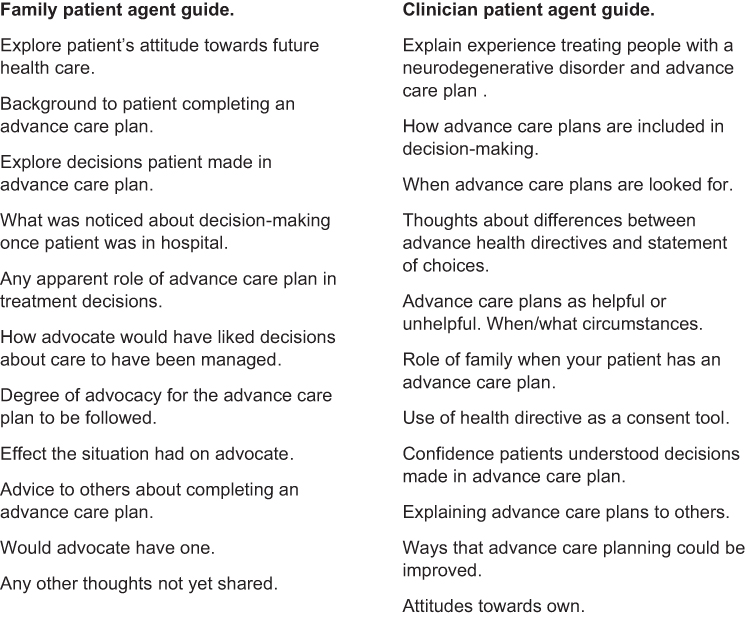 |
Figure 1 Example interview topics. |
Interviews were transcribed verbatim by either the first author (DC) or a professional transcription service. Early interviews were coded by two research team members (DC, RR) after which coding was compared and discussed. DC then coded all transcripts using a combination of open and in vivo codes, with QSR NVivo 12 software utilised to assist data management. In line with grounded theory, data and codes were constantly compared21 and codes discussed and revised during regular research team (DC, RR, DH, MS) meetings, increasing confirmability of the data. As the analysis progressed, codes were collapsed into categories which captured recurring themes and sub-themes. DC wrote reflexive memos to explore and interpret understanding of categories and used diagrams to document relationships between themes and to develop an overarching conceptual framework. Data collection and analysis continued concurrently until the research team were satisfied that no new ideas were emerging, and data saturation had occurred.
Results
Participants
A total of 38 bedside agents participated between November 2019 and November 2020. Of the 38, 32 were clinicians representing a broad range of specialties and clinical expertise, all with ACP experience. Doctors, predominantly senior medical officers, were from the subspecialties of emergency, general medicine, intensive care, neurology, medical oncology, geriatrics and psychiatry. Nurses ranged from bedside to management and nurse practitioner level, and allied health were senior clinicians. Six participants were family members of patients hospitalised with dementia, Motor Neurone Disease, stroke, Huntington’s Disease and Cerebral Amyloid Angiopathy (see Table 1).
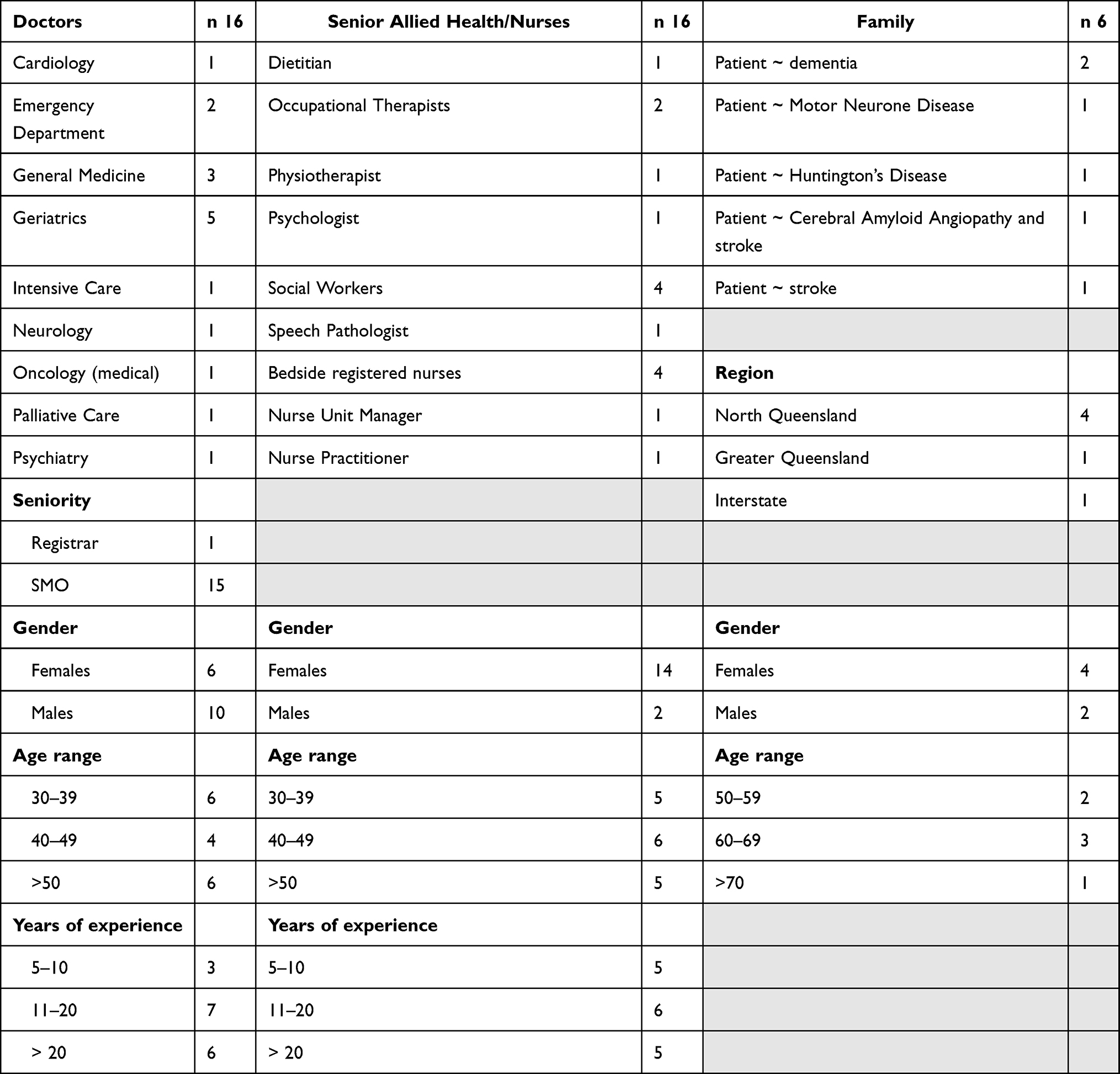 |
Table 1 Participant Characteristics |
Data analysis revealed two main themes: dynamics of discerning best interests; and avoiding conflict. Collectively, these themes formed the basis of the core category: conflicting interests of bedside patient agents (see Table 2). Participants are identified by letters: AH – Allied Health, D – Doctor, F – Family, RN – Registered Nurse.
 |
Table 2 Example of the Coding Process |
Conflicting interests among bedside agents encapsulates the competing influences, such as cognitive biases which impact decision-making. Conflicting interests may occur when agents encounter cognitive discord between possible choices, such as: loving family advocating for the patient’s right to treatment refusal, yet not wanting the patient to die; or clinicians seeking to ascertain the best interests of patients and provide good medical care, yet the patient has refused life-sustaining treatment within an AHD.
Dynamics of Discerning Best Interests
Discerning the best interests of another person, in this case an incapacitated PWND who sought agency through ACP, is a complex ethical position for agents. All bedside agent groups spoke of the essential role that doctors play in contributing medical expertise and guidance to both patients and families. Doctors recognised their profession as predisposed towards active treatment and trained to solve medical problems. Remarkably, some doctors identified that medicine is often not holistic or patient centred. Despite modern advances in medicine and technology, most of the doctors experienced difficulty prognosticating, including recognising EOL. When EOL is not recognised, the primary trigger to include the ACP in decision-making is diminished.
Doctors are technicians, they’re engineers, we’re not scientists … So we’re goal orientated, as doctors, we don’t enter into things with open scientific enquiry. We’re very outcome driven … we’re actually taught in medical school that doctors are very bad at identifying looming death … and I have come unstuck from a patient saying “I don’t think I’m going to live through this” and me going, “Oh, don’t worry about it, you’ll be fine, let’s crack on with the rehab”. And sure enough they have passed away from it. D3
Sometimes there is a benefit in not knowing the patient as well, because a familiarity has its own problems. And we can get a little attached to long term patients and develop cognitive biases. It’s highly individual-specific, highly experience-specific … but prognosticating is difficult … there’s good evidence that prognostic, except for the last 24 hours of life, even palliative care specialists are pretty rubbish at estimating prognosis and time. D4
So I think unless you’ve done time with palliative care, or ICU or even geriatrics, it can be quite challenging to actually recognise a dying patient. And people are very reluctant to diagnose patients with dying … When we are talking about someone … with extremely poor premorbid function and irreversible illness, stop doing lumbar puncture for these patients because that’s not going to change their trajectory at all. D7
Most doctors indicated that doctors tend to be perfectionistic and want control over medical decision-making. Interestingly, one doctor explicitly connected doctors’ perfectionism and desire for control with their vulnerability to feeling threatened when an AHD contradicts the doctor’s treatment decision. This suggests the potential for conflicting interests associated with decision-making responsibility, with both doctors and PWND seeking some control over the PWND’s healthcare.
But the other issue with doctors is that, that sense of control and not wanting to make a mistake. And if the Advance Health Directive doesn’t agree with them they’ll panic and ignore it. Or it’s just a – I don’t think there’d be any issue if it mirrors what they want to do, what the treatment says to do. It’s only ever going to be an issue when the patient’s wishes are against what the doctors think should be done. D16
Doctors appeared to respect their responsibility to provide good medical care which, in their judgment, would be care that is in the patient’s best interests. Accordingly, some valued their right to resist “futile”, unreasonable treatments associated with some patients’ AHDs which consented to death-delaying treatment. However, some doctors referred to judging good medical practice as a subjective process that challenges doctors. Therefore interpretation of applicability of AHDs also varies between doctors, with some influenced by the AHD to provide intervention which other doctors would not provide.
One does have to think of beneficence, not just autonomy, and make an overall judgement, what is the right thing for the patient, considering the spirit of the decision that they have conveyed [within an AHD]. D6
Fortunately in Australia we doctors have the latitude to provide the healthcare that they think is appropriate and in a way it doesn’t matter what the patient’s written in the Advance Health Directive … That being said, amongst my peers I fall at one extreme where there are some patients that I think I would not resuscitate whereas my closest peers would because the patient had expressed desire to be resuscitated. D11
At the same time doctors have rights, too, hospitals have rights, too, so you can’t compel me to do something that I think is futile or is against good medical practice. D3
Interestingly, most doctors appeared uncomfortable about their limited understanding of ACP related legislation, however most believed that applying good medical practice would afford them legal protection.
The line where you do and you don’t that is very difficult, but that, you see, the legislation in Queensland and I know it’s different elsewhere, but the legislation in Queensland clearly states it has to be consistent with good medical practice. Now if I’ve got someone who I can fix within a few hours and they’re going to be better the next day and back to where they were, it’s not consistent with good medical practice to let them die. D5
I haven’t specifically looked into Queensland Law because I haven’t had to … I think it’s like a national umbrella for healthcare workers and doctors that medical judgement is very important … we’re kind of protected in that we can make the decision to withdraw care on a patient against their will and against the family’s will if we feel like it is completely futile, or we’re inflicting pain and torture on a person for no reason, no benefit … my understanding is that we’re protected under that sort of circumstance. D15
One doctor acknowledged the impact of doctors’ personal values systems on clinical judgements.
So I think that there are biases between certain clinicians. I’ve seen biases from religious clinicians away from certain treatment pathways which don’t adhere to their value systems. I’ve seen people completely the opposite because of just personality I guess or difference of opinion … I think we apply our value systems to those documents. D8
All doctors spoke of inherent complexities of healthcare and consequently they perceived ACPs in isolation as of little value. Commonly, doctors asserted that medical decisions should be led by doctors in association with known patient preferences, typically ascertained in consultation with family rather than the ACP. All groups agreed that family contribute valuable personal knowledge about the patient’s situation and healthcare preferences. Most doctors appeared motivated to minimise family’s discomfort, in part because family “will live on” with the experience of the PWND’s death, potentially putting family’s interests in conflict with the PWND’s agency. Whilst a small number of doctors spoke of “trying” to prioritise patients’ needs over those of family, doctors generally interpreted family inclusion as an essential element of good patient care, implying difficulty negotiating boundaries between patients and families.
There’s a list of, I think, the health directive is supposed to be the number one before all else, but in reality, [we use] next of kin … And sometimes it’s a big negotiation between like whether or not they’d still be suitable for a [hospital unit] admission to give them a chance to turnaround versus not. D15
I don’t think you can treat patients independent from their families even though you want to at times. D16
I think we’ve got to take great caution in not treating the family, treating the person and their wishes. But … advance health directives are not clear cut quite often …. they cover a very finite set of circumstances and a finite set of treatments … they often don’t capture the person’s wishes and the person’s life history. D4
Sympathetically, some doctors tried to shield families by becoming paternalistic (also referred to empathetic) and making definitive recommendations.
And you’ve got somebody who’s unconscious and then it comes down to, I’m afraid, a certain doctor knows best paternalistic attitude …. I think paternalistic is the wrong word. I think it’s being empathetic and respecting the fact that that patient couldn’t possibly have envisaged this scenario, not being a doctor … discussion with the family has to be trust engendering, has to be accurate, honest and, in my view, should revolve around two things, which is prognosis and treatment and, secondly, the patient’s wishes and then try to intermingle all those together to get an outcome which is appropriate for everybody. D5
Despite the overarching responsibility which doctors maintain for patient care, data revealed AH/N contribute considerable power to influence the application of ACPs to treatment decisions. Clinician groups broadly endorsed AH/N as the most likely clinicians to identify the existence of an ACP, bring it to the attention of doctors, and to advocate for enacting patients’ documented wishes. When AH/N perceived a conflict between prescribed medical care and a patient’s ACP, some challenged doctors. Some doctors credited AH/N with making it difficult for doctors to overrule an AHD. Data suggested the potential influence of AH/N confidence, hierarchy or scope of practice and the possibility that these clinicians may be less constrained by their responsibilities than doctors. One nurse explicitly referred to the relative powerlessness of nurses, with a colleague reportedly ostracised by team members for raising a formal complaint when an AHD was not applied.
The non-medical multidisciplinary team [MDT] are more strong champions for implementation of advance care directives than the doctors …. It’s [MDT] very supportive until you want to do something other than what the ACD [Advance Care Directive] says, which is when you have to carry the whole team around with you. D6
[When persisting with life sustaining treatment against the patient’s wishes] I would have very clear debates with the doctors, “Why are you doing this? What’s this actually about?” AH2
What ended up happening is the nurses took charge and didn’t, [they] were advocating for their patients. So, they called Ryan’s Rule [process to escalate concern] … that person who took it further and … Ryan’s Ruled it, was then kind of ostracised by senior medical staff … But that was conflict of interest, conflict in beliefs, conflict of paperwork … it was everything all in one … we’re the first persons to get blamed because we’re the bottom of the food chain. RN1
Of the allied health clinicians, social workers were most often referred to as core patient advocates. Speech pathologists, dietitians, psychologists, physiotherapists, and occupational therapists described themselves, or were referred to by colleagues, as advocates who resist involvement in treatment considered counter to the PWND’s ACP. All clinician groups indicated that AH/N can develop rich insights about patients and families, enabling them to contribute considerable information which doctors agreed was advantageous.
The main people who are champions for this are nurses and the social workers. The physios and Ots [Occupational Therapists], their interest in that is “This patient says I don’t want treatment, why am I treating?” D6
Before you develop a holistic opinion, you’d take it to the MDT … They’ll tell you about their journey through the 24 hours because at the end of the day the doctors are not there, the nurses are with the patients far more than the doctors. And often the nurses are very good at, they have a lot of contact with families as well … physio will give you information ….that can help you prognosticate a bit … the occupational therapists. The social worker, and you know, dietitian and speechies can tell you about prognostic factors … But a lot of the times … it really comes back to the core of social work, nursing, and medicine. D4
Most clinicians perceived a potential conflict of interests associated with family’s power and role as partners in decision-making. Some clinicians expressed that although family had been supportive of the concept of PWND’s agency through ACP, when faced with the experience of applying it, families were emotionally conflicted.
There’s that dynamic of what the patient wants, and what the doctor thinks is reasonable, and then you’ve got the family. It’s a bit of a dance really. RN2
But often, when patients’ family are driving it, that is because they have some belief in something that they want to make sure is adhered to. It is very difficult to wade through this problem that is not yours and not adulterate the decision with your own views, and purely say “This is what this person would have done”. D6
The advanced health directive does obviate a lot of problems because there’s an inherent conflict … between families or next of kin, and the person’s wishes. On one hand, we all want our loved ones to live forever and be happy and do all those sorts of things. You know, there’s certainly, there’s some … you know, we all have those motivations that we don’t want to lose somebody. D4
Some clinicians were suspicious of family members’ motives, perceiving families as biased and unable to separate their own needs or beliefs (often emotional or religious in nature) from the patient’s.
I’ve seen tension … between families and medical teams … we’ve had family, like a lot of argy bargy between family and particularly, I’ve worried that the family don’t necessarily have the best interests of the patient at heart. I think in some situations it [ACP] can make things trickier for families in a time where their loved one is incapacitated … often people … are looking for a locus of control in a time where they really want control. I think that can actually be challenging. AH10
In a clear demonstration of the emotional conflict faced by families, these participants recalled considerable intra and interpersonal conflict between themselves and clinicians when presuming the PWND’s AHD should be applied, and when advocating for the patient. In all cases, the PWND, via their AHD, requested a palliative approach to EOL if their condition was considered by the doctor to be terminal, incurable or irreversible. Accordingly, advocating for application of the AHD was associated with the expected death of the PWND, and considerable distress for some family members. Two participants remarked that subsequent symptoms of anxiety had persisted years after the PWND’s death.
We then had to negotiate with the medical people and that’s where tensions came … [Doctor] came trying to encourage [PWND] to continue with the therapy that might save [PWND] … she even tried to argue the point … and I remember [Name] and I standing there in front her in effect trying to say as carefully and clearly as we could “the answer is no” … getting them to back down and then just stay out of it. They were no longer going to be part of the treatment, and just to stay away from us. F3
That’s a dreadful thing to have to do … I had to go to [Doctor] and say, “Well what about this advance healthcare directive ….”. it’s like, you’ve got to go and precipitate the demise of your loved one, just [expletive] awful … I didn’t know what the hell was going on … and find out two days later, “Oh we’re not doing that because of some advance healthcare directive”, off the nurse’s aid in casual conversation … which was exactly why [PWND] got an advance healthcare directive … I know that at the time I was too uncomfortable, ashamed, guilty, grief-stricken, absolutely devastated, whatever, to tell our friends who visited [PWND] daily that I had just had to virtually insist that the doctors follow the directive and cease artificial feeding. Still haven’t told them to this day. Instead I told them “The doctors have decided”, which is what should have happened but really did not. F1
A couple of the younger doctors were nice. The older sort of treating doctors were just, you know “I know more than you do”. And you’d ask a question and they make you out to be a bit of a nong … I don’t like even going past the hospital at the moment. F2
Avoiding Conflict
An unexpected theme arising from most participants’ data across all groups, was that doctors often appear uncomfortable with, and avoidant of, conflict. As a profession trained to treat and solve medical problems, doctors appeared to experience intra-personal conflict when faced with a patient’s death. Doctors generally demonstrated high expectations of themselves as good doctors and appeared authentically committed to patient outcomes. Whilst doctors expressed agreement with their legal and ethical responsibilities as medical officers, they also appeared sensitive to expectations of them. Some doctors experienced considerable discomfort associated with patients dying, and some had endured emotional challenges discerning the philosophical boundary between prolonging life and prolonging death. Several doctors reasoned that death is broadly perceived as a failure of care, adding to their sense of failure or blame upon a patient’s death. Accordingly, transitioning patients from life-sustaining medical interventions to EOL care (potentially as a consequence of an ACP) was linked with inner conflict that required a significant, often uncomfortable, cognitive shift of focus.
If you just say “for goodness sake, the family are really not able to make this decision and this person asked for this, this is what we need – we need to go by their wishes” they find that really hard. They don’t like conflict, doctors. AH6
It’s like they didn’t want to be the ones that actively precipitated the end … and yet, in a way you’re the one who has to actively precipitate the end by sort of insisting that they follow the advance healthcare directive. So, it’s just, it’s a lot of mixed signals. F1
What I find really challenging is going from a very aggressive healthcare approach to a philosophical ‘we’re not prolonging death’ approach … D7
[Is death perceived as failure] Definitely in medicine. Especially in the junior ranks. Look, I mean, when you were in your formative ages, you thought your job to become a doctor is to save lives. That’s what people say “you save lives”, right? …. All my life I have been saying to my patients “You will not die, don’t worry, I am there for you”. D6
[Is death perceived as failure] For me, it’s a real cognitive shift. And unless you’re in that thought process to make that cognitive shift, it can be really hard. Because it’s philosophically opposed from a clinical perspective to really aggressively give medication to treat this, to treat that, to, “you know what, we’re actually not going to prolong your life. But, by doing that, we’re prolonging your death”. I say that to patients and patients’ families, perhaps not for their sake but perhaps for mine, to actually put me in the mood to make those decisions with them. D8
Because we’re not just automatons, you know … do we keep this non-life sustaining sub-cut fluid going or not? I mean put it in, take it out. But the emotional weight that was attached to removing that fluid was just awful. D9
Several clinicians described doctors appearing intimidated by outspoken patient advocates. Not surprisingly then, clinicians broadly endorsed that doctors typically seek to avoid conflict with families. Accordingly, despite a PWND tangibly seeking agency through an AHD, family members may be afforded considerable influence over treatment decisions, which may in fact reflect family’s needs and preferences.
But if there’s family involved, we have to, quite often, go by the family wishes as opposed to the patient’s wishes. There can be a bit of conflict there because they [PWND], obviously wrote the healthcare directive when they were well and when they had capacity. D15
There’s a lot of different reasons why a doctor may not adhere to an Advance Health Directive and pressure from families is definitely in there. Because sometimes the patient may say no, I don’t want anything done but the families don’t agree with that. And when the patient hasn’t got capacity then they assume substituted decision-making whatever so it does get extremely tricky to honour the patient’s wishes. D16
To some degree it’s how much responsibility you’re prepared to take in a patient’s care … They’re big life changes, yes. I think there’s – sometimes it is not feeling confident to weigh up all of those features and take a decision and be forthright about it because you may have to have conflict with family members and you may have to point out the futility that sometimes family members or patients don’t want to accept. But that’s what drives a whole lot of madness in healthcare is always trying to pass the buck. D11
To avoid conflict, most doctors emphasised the importance of establishing a cooperative relationship with family to enhance decision agreement. Nonetheless, all participant groups concurred that doctors often have difficulty communicating adequately with PWND or families. Few doctors thought they had been sufficiently trained for EOL conversations, resulting in a common reliance on social workers when difficult conversations, such as EOL prognosis, were expected.
So it just, it’s again, comes back to investing up front. If you invest time, talk with the family, everyone is aware, on the same page … I think you have to portray or display yourself as someone who is genuine, who is acting in the patient’s best interest. Once you’ve given them that confidence and they have started having faith in you I think things just happen a lot easier from there. D7
Because people don’t have the information to make the decisions …. nobody’s actually told them “Oh, they’re not going to get over this” … doctors don’t know how to do it, and because doctors don’t know how to really explain that, things are not going well. D10
That’s difficult and you probably need a few grey hairs to have that conversation a lot of the times. And it’s just not possible if you’re 23 to be trying to guide a conversation with highly emotional family members who just don’t want to hear that because they’re not going to take it from you. D11
[How do the doctors manage EOL conversations?] Terribly. Terribly. Oh my God, the medical doctors, it’s shameful, and that’s quite often why I or a social worker would follow up with them [patients]. They’ve really pushed in [hospital unit] for the social worker to be present for every single discussion about end of life. AH4
They’re very medical minded and “We can fix it.” … but let’s not tell you about all those other things that might go wrong. So I quite like to be in those family meetings because I’m then able to prompt the family to ask those questions. I don’t think the doctors do that well. They don’t like to tell people that – you know, “Well you’re going to die anyway”. AH6
Several family members recognised that some doctors may experience emotional challenges associated with treatment limitations and a PWND’s death. Only one provided an example of a positive experience of shared decision-making between family and doctor.
The people that work there were fantastic and nurses were great, the doctors were good … I’m sure they meant well and wanted perhaps to give us a little longer with [PWND] among us. F1
Well actually my brother-in-law is an orthopaedic surgeon and he said to me “They’re [AHD] a toothless tiger.” He said “If you’re in bed and you’ve got an Advance Health Directive and your two daughters stood at the foot of the bed and they demanded that you be resuscitated and be given antibiotics, no doctor will waive this in front of them and say but your mother didn’t want it”. F6
Look, there’s always going to be messy situations. So in fact, the ones with the [hospital unit] people, I think were good. They were constructive. They didn’t just back down immediately to anything that we said. In that sense they did their job properly to make sure that we understood. F3
The importance of leading temporal treatment plans with consent of families (as opposed to applying AHDs) reflected a means of avoiding potential conflict. Some doctors expressed that appeasing family can also be a source of discomfort, with some capitulating under pressure from family, or compromising treatment plans for a family’s benefit. Some doctors feared and sought to avoid complaints from families, or legal action against them.
And what we do is we just try and toe that line between making it a good experience for the EPOA [legally appointed SDM] /significant other as well as respect the wishes of the patient. If it were something really startlingly obviously like the EPOA was saying you need to intubate them and we’d be less – probably a lot more forceful in our views. But, to be honest, the majority of cases are subtleties that we can happily allow them to have. We’ll give them antibiotics for a week or we’ll give them fluids for a few days which is fine and as long as it comes under the banner of do no harm to the patient. When to play that, well, it’s not a game but to do the dance I suppose. D9
Like some of the stuff that we were having to do to like 80-year-old nannas that I just wanted to put a blanket on and put in a corner for some dignity, and yet their family want everything done … sometimes you also run into the problem that, yes, they want to go down a palliative pathway if they deteriorate but then when you talk to the family they’re like “No, you have to keep them alive for the next three days till I get there” … it definitely plays into your mind like, if you’ve got a highly objective family, like it’s hard to fight that because they’re the ones that are going to put in the complaint and the litigation. D15
Yes, I have pulled the “I am the doctor, I’ll make a decision on some issues”. Because when there’s a coronial it’s going to be my [responsibility], you know, I’m up there taking the rap. D16
Discussion
Exploring the perspectives of doctors, AH/N and families of hospitalised PWND who expressed agency through ACP, revealed that these agents often experienced intra and interpersonal conflicting interests when acting as patient agents. This research appears to be the first to investigate the potentially conflicting interests between agents when a PWND who has an ACP no longer has capacity to consent to healthcare. Broadly, doctors held a strong preference for leading temporal best interests decisions in the context of the PWND’s known illness status, and they prioritised partnerships with families to meet collective needs. Families sought inclusion in temporal decision-making whilst simultaneously advocating for AHD application to respect the PWNDs treatment limiting directions, and in one case, to alleviate guilt. AH/N maintained a unique position of influence to advocate for the PWND by promoting ACP application. Effectively, the agency of PWND may depend on the recursive relationship that exists between structures (such as hospital systems) and human agency (in this case clinicians and family)25,26 which can result in conflict as each of these actors retain considerable power when determining healthcare for PWND. Although well intended, temporal decision-making which favours family consent potentially conflicts with the rights of the PWND and raises questions about the utility of ACPs.
Dynamics of Discerning Best Interests
Given the complexity of healthcare and the relatively simplistic nature of ACPs, the realisation of agency through ACP is unavoidably impacted by a conflicting convergence of the hypothetical nature of ACPs and the responsibilities of bedside agents. Although PWND are encouraged to complete ACPs in their own best interests, when healthcare decisions were required, clinicians largely co-opted families to attempt best interests decision-making partnerships on patients’ behalf. PWND who develop an AHD have exercised a legislated right; hence, to overlook their agency by transferring power to family risks undermining a fundamental right of the patient.
Doctors in this study often presumed family’s knowledge of the patient’s intentions for ACP applicability and the appropriateness of including family in decision-making. Consistent with another study,10 both clinicians and families perceived family as powerful patient agents, however family members were at times conflicted about their authority as SDMs. This situation gives rise to a potential imbalance of power associated with individual capacities such as communication skills, health literacy, self-confidence, and emotional investment in decisions, and therefore intra and interpersonal conflict when discerning patients’ best interests.11,14
Similarly to other studies,27–32 doctors saw themselves as appropriate leaders of good medical practice, and advisors to healthcare decisions reflective of the PWND’s best interests. Importantly, in situations where family reported healthcare dissatisfaction, they contended that the prescribed healthcare contradicted an AHD because doctors chose to overrule the patient’s directive. This suggests philosophical inconsistencies in discerning best interests care. Although variable by subspecialty or individual’s practice culture, doctors demonstrated tendencies towards life-sustaining treatment, as though they perceived sustaining life as synonymous with their role and patients’ best interests. Through AHD, PWND had exercised their legislated power to give directions in what they believed to be their own best interests, yet our study revealed that doctors typically assumed clinical leadership over PWND’s best interests and prioritised temporal healthcare decisions.
Predictably, all clinician groups demonstrated high expectations of themselves and their colleagues as professional patient agents. Members of multidisciplinary teams made representation on patients’ behalf which sometimes gave rise to conflicting opinions. Doctors’ attitudes towards AH/N input ranged from appreciative to feeling challenged. AH/N attitudes towards their own contributions to treatment decisions ranged from self-doubting to confident. As noted by Olsson et al,33 doctors were typically identified as the key medical problem-solvers; however this study also revealed that AH/N and doctors associated doctors’ responsibilities with the highest expectations of excellence and vulnerability to moral distress. It seems plausible then that confident AH/N may feel empowered as patient agents, possibly because they are less constrained by the responsibilities of doctors. Collectively, clinicians from varied disciplinary perspectives shouldered considerable ethical and professional standards obligations as agents for PWND who sought to influence their healthcare through ACP.
Fear of litigation has been associated with non-adherence to ACP in intensive care physicians.34 Adding to this knowledge, numerous doctors in this study revealed their fear of misjudging situations, making critical clinical errors, and incurring litigation. Interestingly, despite significant advances in medicine and technology, or perhaps in part because of them, doctors conceded that prognostication is often challenging, a factor reported elsewhere.33,35 Difficulty recognising when a PWND is approaching death appeared closely aligned with delayed application of ACPs. Predictably, other research also associated doctors’ recognition of patients’ impending death with improved communication and EOL care,36 however, this often occurs close to death.33 Late application of ACPs suggests the potential for provision of unwanted medical intervention and therefore revision of ACPs to establish PWND preferences should occur early, when treatment decisions might better reflect patient’s agency.
Disturbingly, some agents in our study found that their responsibilities as a PWND’s agent triggered considerable inner conflict and or distress. Family members demonstrated both complementary and contradictory roles: they took responsibility for advocating for AHD adherence, whilst simultaneously asserting authority as SDMs. In reality, healthcare involves power imbalances, with exemplary communication of facts essential to achieve equitable empowerment of agents. Accordingly, when families in this study felt vulnerable to the authority held by the medical system, they exerted control and asserted their power to influence treatment decisions in line with their self-expectations.
However, roles remain unequal, with the capacity to advocate for application of AHDs compromised by inconsistent information sharing and uncertainty about the PWND’s prognosis. Nevin et al35 in their review described similar barriers to applying palliative care principles in acute care hospitals. They found prognostic uncertainties and EOL care were perceived as in conflict with acute care practice culture, leading some doctors to deflect and avoid difficult conversations. Similarly, this study identified a link between doctors’ prognostication uncertainties and avoidance of timely transition from active treatment to AHD application. Further research may be needed to establish means of supporting doctors in this regard.
Avoiding Conflict
Consistent with social theory, doctors today shoulder considerable responsibilities and are forced as never before to justify their actions.9 Patients and their families enjoy unprecedented access to healthcare information, and simultaneously, authority over healthcare consent. In response, it seems predictable that some doctors will develop fear-based, conflict avoidant behaviour patterns in the context of EOL healthcare consent. The degree to which doctors in this study appeared motivated to avoid conflict and extend their responsibilities beyond the care of the patient to incorporate families is noteworthy. Doctors appeared to have co-opted families, in part to mitigate potential reprisals but also on compassionate grounds. Doctors recognised that patient priorities must be respected, but they ascribed similar respect to the priorities of families, whom doctors noted would live on with memories of the PWND’s healthcare and death. Unlike an ACP which remains a static document that cannot be probed; doctors and families have opportunities to interact and negotiate care. However, when negotiations do not meet their needs, doctors can become threatened by agents questioning care decisions. Clearly, modern doctors practice within complex, powerful healthcare systems and relationships, wherein patient agency through ACP is influenced by multiple agent pressures and thus stands as an ideal yet to be achieved.
Interestingly, White et al24 found Australian doctors were more motivated by ethical than legal considerations; however when doctors doubted that a medical decision adhered to the law, family views were endorsed ahead of personal ethical principles. Accordingly, although justification of ACP non-application varies, doctors clearly exercise clinical judgement, leaving the door open to ethical reasoning. This study has highlighted doctors’ protective attitude not only towards PWND, but also their families, reflecting doctors’ sense of ethical responsibility which extends beyond their immediate patients. Further, these results may reflect treatment culture in a regional hospital context, which remains to be further explored.
Limitations
Whilst this study represents an important first step in the generation of a theory to explain factors associated with PWND’s agency through ACP, the data were collected from a specific region and in relation to neurodegenerative illnesses. Although our research drew on the rich perspectives of 38 individuals, their views are not representative of all agents. It is possible that clinicians who participated were sympathetic to the concept of ACPs. Despite extensive recruitment efforts, family participation was low. Family participants held strong views about AHD application, suggesting people with alternative views may not have participated. It appears feasible that some family may not have realised their eligibility, or perhaps they did not feel strongly or wish to discuss their experience. Further, in some cases participants were known to, or colleagues of, the first author, which may have biased their responses. However, it is possible that this element represents a study strength by improving participants’ reflexivity about their actions. Finally, efforts were made to engage doctors from other units and of junior status, however these potential participants declined invitations.
Conclusion
This study provides insights into the potentially conflicting interests experienced by beside patient agents who seek to represent the best interests of PWND. Although bedside patient agents endeavour to respect patient choices, doctors feel conflicted about relying on ACP as sources of truth. Doctors do not appear conflicted by patient agency when doctors and families agree with the decisions within the ACP. Generally doctors perceive that family cannot be excluded from a temporal decision-making partnership, elevating the needs of doctors and family beyond the agency of the PWND. Whilst not all ACPs are legally persuasive, doctors engage families and make decisions on behalf of PWND regardless of ACP legal status, thus placing bedside agents and patient agency in potential conflict. It appears that there are substantial limitations to the effectiveness of PWND’s agency expressed through ACP, and that bedside agents can experience considerable intra and interpersonal conflict. The complex interplay between healthcare systems and the realisation of agency through ACP warrants further research.
Acknowledgments
The authors sincerely thank participants who provided their valuable time and insights. This research was supported by the Australian Government Research Training Program (RTP) and James Cook University Cohort Doctoral Studies Program.
Disclosure
The results from this publication are to be included in the doctoral thesis of Denise P Craig which will be uploaded to: James Cook University repository URL: https://researchonline.jcu.edu.au/. See reference.37 Ms Denise P Craig was financially assisted by the Far North Queensland Hospital Foundation Paul and Dina Kamsler Memorial Award, and the Tropical Australian Academic Health Centre Clinician Researcher Fellowship Scheme. Funders had no further role in the study. The authors have no other conflicts to interest in this work.
References
1. Regan L, Preston NJ, Eccles FJR, Simpson J. The views of adults with neurodegenerative diseases on end-of-life care: a metasynthesis. Aging Mental Health. 2019;23(2):149–157. doi:10.1080/13607863.2017.1396578
2. Low L-F, Swaffer K, McGrath M, Brodaty H. Do people with early stage dementia experience prescribed disengagement®? A systematic review of qualitative studies. Int Psychogeriatr. 2018;30(6):807–831.
3. Russell S. Advance care planning: whose agenda is it anyway? Palliat Med. 2014;28(8):997–999.
4. Australian Health Ministers’ Advisory Council. A National Framework For Advance Care Directives. Australian Government Department of Health and Ageing; 2011. Available from: http://www.coaghealthcouncil.gov.au/Portals/0/A%20National%20Framework%20for%20Advance%20Care%20Directives_September%202011.pdf.
5. Thomas K, Lobo B, Detering K. Advance Care Planning in End of Life Care.
6. Queensland Government. Statewide Office of Advance Care Planning: Performance Report 2019–20. Queensland Health; 2020
7. Queensland Parliament. Guardianship and Administration Act 2000 (Qld). Available from: https://www.legislation.qld.gov.au/view/html/inforce/current/act-2000-008. Accessed July 24, 2021
8. Queensland Parliament. Powers of Attorney Act 1998 (Qld). Available from: https://www.legislation.qld.gov.au/view/pdf/2017-03-05/act-1998-022. Accessed July 24, 2021.
9. Kaspersen LB, Giddens A. An Introduction to a Social Theorist. Oxford: Blackwell; 2000.
10. Wendler D, Rid A. Systematic review: the effect on surrogates of making treatment decisions for others. Ann Intern Med. 2011;154(5):336–346. doi:10.7326/0003-4819-154-5-201103010-00008
11. Shah SGS, Farrow A, Robinson I. The representation of healthcare end users’ perspectives by surrogates in healthcare decisions: a literature review. Scand J Caring Sci. 2009;23(4):809–819. doi:10.1111/j.1471-6712.2008.00674.x
12. Pope TM. Legal fundamentals of surrogate decision making. Chest. 2012;141(4):1074–1081.
13. Schenker Y, Crowley-Matoka M, Dohan D, et al. Want to be the one saying ‘We should just let him die’: intrapersonal tensions experienced by surrogate decision makers in the ICU. J Gen Intern Med. 2012;27(12):1657–1665.
14. Smith AK, Lo B, Sudore R. When previously expressed wishes conflict with best interests. JAMA Intern Med. 2013;173(13):1241–1245.
15. Batteux E, Ferguson E, Tunney RJ. A mixed methods investigation of end-of-life surrogate decisions among older adults. BMC Palliat Care. 2020;19(1):44.
16. Queensland Government. Advance care planning clinical guidelines. Available from: https://clinicalexcellence.qld.gov.au/priority-areas/service-improvement/improving-care-end-life-queensland/care-plans-clinical-tools.
17. Craig DP, Ray R, Harvey D, Shircore M. Factors which influence hospital doctors’ advance care plan adherence. J Pain Symptom Manage. 2020;59(5):1109–1126.
18. Block BL, Smith AK, Sudore RL. During COVID-19, outpatient advance care planning is imperative: we need all hands on deck. J Am Geriatr Soc. 2020;68(7):1395–1397.
19. Martin‐Khan M, Bail K, Yates MW, et al. Interim guidance for health‐care professionals and administrators providing hospital care to adult patients with cognitive impairment, in the context of COVID‐19 pandemic. Australas J Ageing. 2020;39(3):283–286.
20. Curtis JR, Kross EK, Stapleton RD. The importance of addressing advance care planning and decisions about do-not-resuscitate orders during novel coronavirus 2019 (COVID-19). JAMA. 2020;323(18):1771–1772.
21. Charmaz K. Constructing Grounded Theory.
22. Wong RE, Weiland TJ, Jelinek GA. Emergency clinicians’ attitudes and decisions in patient scenarios involving advance directives. Emerg Med J. 2012;29(9):720–724.
23. Birks M, Mills J. Grounded Theory: A Practical Guide.
24. White B, Willmott L, Cartwright C, Parker M, Williams G. The knowledge and practice of doctors in relation to the law that governs withholding and withdrawing life-sustaining treatment from adults who lack capacity. J Law Med. 2016;24(2):356–370.
25. Giddens A, Pierson C. Conversations with Anthony Giddens: Making Sense of Modernity. Stanford University Press; 1998.
26. Clark J, Modgil C, Modgil S. Anthony Giddens: Consensus and Controversy. Vol. 2. Routledge; 1990.
27. Moore N, Detering KM, Low T, Nolte L, Fraser S, Sellars M. Doctors’ perspectives on adhering to advance care directives when making medical decisions for patients: an Australian interview study. BMJ Open. 2019;9(10):e032638.
28. Willmott L, White B, Tilse C, Wilson J, Purser K. Advance health directives: competing perceptions, intentions and use by patients and doctors in Queensland. QUT Law Rev. 2013;13:30.
29. White B, Willmott L, Williams G, Cartwright C, Parker M. The role of law in decisions to withhold and withdraw life-sustaining treatment from adults who lack capacity: a cross-sectional study. J Med Ethics. 2017;43(5):327–333.
30. Willmott L, White B, Parker M, Cartwright C, Williams G. Is there a role for law in medical practice when withholding and withdrawing life-sustaining medical treatment? Empirical findings on attitudes of doctors. J Law Med. 2016;24(2):342–355.
31. Corke C, Milnes S, Orford N, Henry MJ, Foss C, Porter D. The influence of medical enduring power of attorney and advance directives on decision-making by Australian intensive care doctors. Crit Care Resusc. 2009;11(2):122–128.
32. Bond CJ, Lowton K. Geriatricians’ views of advance decisions and their use in clinical care in England: qualitative study. Age Ageing. 2011;40(4):450–456.
33. Olsson MM, Windsor C, Chambers S, Green TL. A scoping review of end-of-life communication in international palliative care guidelines for acute care settings. J Pain Symptom Manage. 2020.
34. Gutierrez KM. Advance directives in an intensive care unit: experiences and recommendations of critical care nurses and physicians. Crit Care Nurs Q. 2012;35(4):396–409.
35. Nevin M, Hynes G, Smith V. Healthcare providers’ views and experiences of non-specialist palliative care in hospitals: a qualitative systematic review and thematic synthesis. Palliat Med. 2020;34(5):605–618.
36. Houttekier D, Witkamp FE, Van Zuylen L, Van Der Rijt CCD, Van Der Heide A. Is physician awareness of impending death in hospital related to better communication and medical care? J Palliat Med. 2014;17(11):1238–1243.
37. Craig DP, Ray R, Harvey D, Shircore M Advance care plans and the potentially conflicting interests of bedside patient agents: a thematic analysis [dissertation]. College of Medicine and Dentistry, James Cook University, Cairns; 2021.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.