Back to Journals » Patient Preference and Adherence » Volume 13
Adult Perceptions of Different Orthodontic Appliances
Authors Alansari RA ![]() , Faydhi DA, Ashour BS
, Faydhi DA, Ashour BS ![]() , Alsaggaf DH
, Alsaggaf DH ![]() , Shuman MT, Ghoneim SH
, Shuman MT, Ghoneim SH ![]() , Linjawi AI
, Linjawi AI ![]() , Marghalani HYA
, Marghalani HYA ![]() , Dause RR
, Dause RR
Received 15 October 2019
Accepted for publication 27 November 2019
Published 13 December 2019 Volume 2019:13 Pages 2119—2128
DOI https://doi.org/10.2147/PPA.S234449
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Reem A Alansari,1 Dimah A Faydhi,2 Basoum S Ashour,2 Doaa H Alsaggaf,1 Muhannad T Shuman,3 Salma H Ghoneim,1 Amal I Linjawi,1 Hussain YA Marghalani,1 Rania R Dause1
1Department of Orthodontics, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi Arabia; 2Dental Interns, Faculty of Dentistry, King Abdulaziz University, Jeddah, Saudi; 3Private Practice, Jeddah, Saudi Arabia
Correspondence: Reem A Alansari
King Abdulaziz University, Faculty of Dentistry, Department of Orthodontics, Alsulemaneya, PO Box 80209, Jeddah 21589, Saudi Arabia
Tel +966 505533276
Fax +966 12 692 1262
Email [email protected]
Introduction: Pursuing an esthetically-pleasing orthodontic outcome, orthodontic patients must consider and choose from the different available options of orthodontic appliance. Practitioners need to be better informed of their customers’ preferences to make better practice management decisions and satisfy their patients’ needs.
Purpose: To explore adult laypeople’s perceptions of the attractiveness, acceptability, preference and economic value of different orthodontic appliances when they consider these appliances for themselves and for their children.
Patients and methods: This cross-sectional survey included 199 adults (110 females). The average age of participants was 27.7 years. Participants answered a questionnaire evaluating and comparing multiple smiling images of an adult wearing different orthodontic appliances. Participants rated each appliance for: (1) attractiveness on a Likert scale; (2) acceptability of having the appliance placed for themselves and their children (with a yes/no response); (3) preference (by ranking all appliances in order); and (4) economic value (by providing the additional amount they are willing to pay for each appliance for themselves and their children).
Results: We found a statistically significant difference in the attractiveness scores between the different orthodontic appliances (p< 0.0001). The most attractive appliances were clear aligners and lingual brackets. The least attractive appliances were colored o-tied-brackets followed by shaped-brackets. Clear aligners were the most acceptable appliances among our participants to have placed on themselves (86.9%) and their children (84.9%). Shaped brackets were the least acceptable appliances among our participants to have placed on themselves (24.1%) and their children (36.2%). The most preferred appliances were lingual brackets (39.2%), followed by clear aligners (34.17%). The least preferred appliances were colored o-tied-brackets (4%). Participants varied with regards to how much more they were willing to pay for each of the different orthodontic appliances. The majority were willing to pay more for clear aligners and lingual brackets to have them placed on themselves but not to have them placed on their children.
Conclusion: Adults preferred more innovative esthetic appliances over traditional ones and were willing to pay more to have them placed on themselves but not on their children.
Keywords: smile, attractiveness, esthetics, value
Introduction
There are a variety of orthodontic appliances that are available for patients seeking orthodontic treatment and their orthodontists to choose from during treatment planning. The appliance choice is a dynamic process that depends on a myriad of factors.1 The functional properties of the appliances and their fit for the treatment needs play an important role but esthetic aspects of the appliances are equally important.2,3 Studies have shown that the esthetic appearance of orthodontic appliances may influence how others judge the intelligence, attractiveness and social competence of patients wearing the appliances.4 Non-visible, tooth-colored, and transparent appliances have been shown to be more attractive than other appliances.5
A tremendous effort goes into developing alternative appliances that are both therapeutically efficient and esthetically acceptable for patients. Technological advances over the past decades have enabled an evolution of orthodontic appliances with reduced visibility and increased acceptability.2 Plastic and ceramic brackets, lingual brackets, white-coated wires, and transparent tray aligners were introduced to the market to overcome the esthetic disadvantages of metal brackets.6 A study revealed that a third of Swedish adults who want to fix their malocclusion were unwilling to wear visible orthodontic appliances.5 A study conducted on adults from the central United States showed that clear aligners and lingual braces were the most acceptable appliances with 90% acceptance rates, followed by ceramic braces. On the other hand, the acceptability rates of traditional and self-ligating metal brackets were only at 55% and 58%, respectively.5 Another study looking into the acceptability, attractiveness and value of different orthodontic appliances in the Iranian population found that lingual brackets had the lowest acceptability despite high attractiveness ratings. This may be related to concerns the appliance may cause oral discomfort.7
Socioeconomic and cultural factors are also at play.5,8 The cost of the appliance and the patient’s willingness to pay (WTP) may determine whether a particular appliance is chosen.5,9 Rosvall showed that adults are willing to pay an additional $610 for lingual braces and clear aligners, $329 for ceramic and self-ligating appliances, and $167 for hybrid self-ligating appliances to be used either for themselves or their children.5 Another study found that adults are willing to pay more for themselves and for their children in order to get more esthetic treatment options like aligners and lingual brackets.10 The previously mentioned Iranian study also found that adults were willing to pay more for their children to have esthetically appealing appliances placed.7
The aforementioned factors (attractiveness, acceptability, patient preference, and monetary value attributed to various orthodontic appliances) may vary across different cultures and populations.11–14 This may affect the treatment planning discussions and decisions whether to make a given orthodontic appliances available for a given population. In Saudi Arabia, for example, perceptions of esthetic requirements were found to be highly variable among patients.15 A study asked Saudi adults to rank four different orthodontic appliances and it showed that they preferred ceramic braces and found lingual braces to be the least preferred.16 This is similar to the previously mentioned Iranian study but contradicts studies in other populations where clear trays and lingual appliances were among the most attractive treatments.10 As far as the authors are aware, this is the only study evaluating perceptions of orthodontic appliances in Saudi Arabia. Our knowledge about Saudi laypeople’s perceptions of esthetic properties, acceptability, and price value of different orthodontic appliances is therefore incomplete. The aim of this study is to evaluate Saudi adults’ perceptions of attractiveness, preferences, acceptance, and the price value they are willing to pay for different orthodontic appliances for themselves or for their children in Saudi Arabia.
Materials and Methods
The cross-sectional study was approved by the Institutional Review Board of the Faculty of Dentistry at King Abdulaziz University (project # 165-12-18) and adheres to the tenets of the Declaration of Helsinki. Each participant signed a written informed consent before participating in the study. We recruited a convenience sample of Saudi adults ages 18 and above from a shopping mall in the Jeddah, Saudi Arabia. We excluded dental health care professionals from the study as their personal perceptions and opinions may be influenced by their training and are not likely to represent those of lay persons. We also excluded adults who had previous orthodontic treatment as their personal experience with the orthodontic appliance they have had is likely to influence their judgment of the study parameters. We calculated the sample size using G*power, version 3.1.9.2. We estimated that the minimal sample size required to detect a 0.1 difference in the proportions of acceptability of orthodontic appliances, at a power=0.8 and an alpha=0.05, was 196 subjects. A total of 320 individuals were approached to participate in the study of whom 199 agreed to participate.
Participants were asked to fill out a questionnaire asking them to evaluate attractiveness, acceptability, order of preference and financial values of 9 different orthodontic appliances. To prepare the study questionnaire, we took standardized frontal oral smiling photographs of a Saudi, young adult, female model wearing different orthodontic appliances (Figure 1). The presented photographs of orthodontic appliances included: (1) metal brackets with colorless O-ties; (2) metal brackets with colored O-ties; (3) self-ligating metal brackets; (4) half-metal and half-ceramic (hybrid) brackets; (5) ceramic brackets; (6) self-ligating ceramic brackets; (7) shaped brackets (heart-shaped and superman logo-shaped); (8) Clear aligner trays; and (9) no appliance to resemble the lingual brackets. The chosen model had a near-ideal smile, good tooth alignment, and no malocclusion or midline shift. Her smile exposed the teeth between the right and left 2nd premolars. In order to prepare the different appliances, we fabricated upper and lower dental casts using maxillary and mandibular impressions of the model’s dentition and a bite registration in maximum intercuspation. We then fabricated multiple identical, 0.016x0.022”, stainless steel wires. These were adapted to the facial surfaces of the upper teeth at the level of the bracket points, with 2 bends towards the occlusal surfaces at the level of the 1st molars to allow the model to bite on each wire for stabilization. The appliances were not glued to the model’s teeth. Brackets were then tied to the wires with either o-ties or self-ligating gates secured in place with small pieces of orthodontic wax. We fabricated a vacuum-formed upper clear aligner tray using the upper dental cast. We captured smiling photographs with each appliance using a D5200 Nikon camera with an AF-S Micro-Nikkor 105mm lens. The camera was held by a tripod stand placed in a fixed location. The settings were manually adjusted to ISO=100, F=25, and Shutter=1/125. The source of light remained constant in all pictures. In order to have standard color and format of the images, we used Lightroom (version 6.0; Adobe). The quality of the images was set to RAW (NEF file). The model signed a written informed consent allowing the use of her photos for the study and for publication.
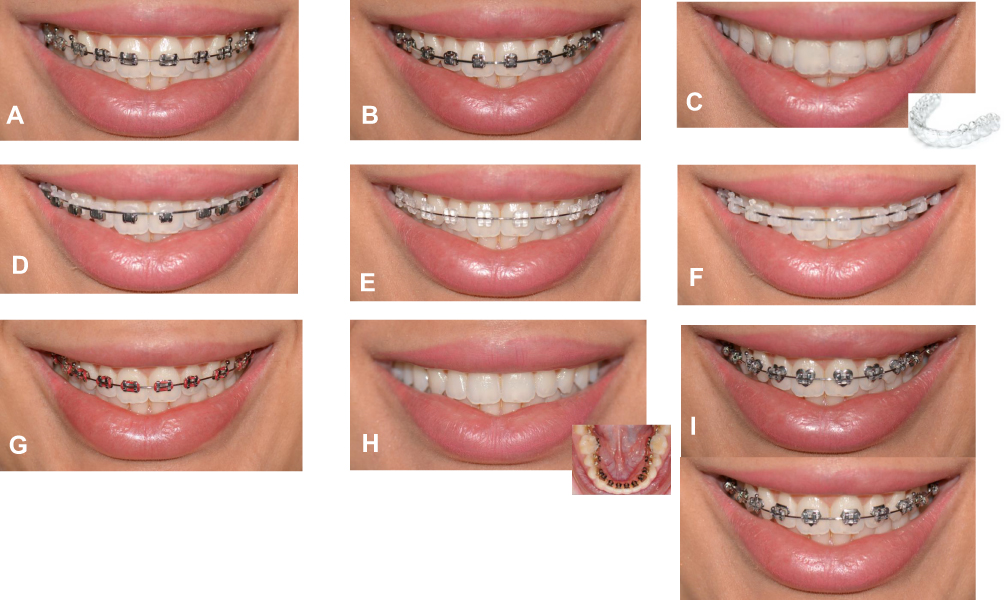 |
Figure 1 The different orthodontic appliances displayed in the questionnaire. |
Using a handheld electronic tablet, participants self-filled the study questionnaire on Google Forms, a web-based electronic survey tool. Two of the authors stood by the participants to answer potential inquiries. The questionnaire started with questions about the gender, age, education level, and marital and employment status. Subsequently, participants successively viewed the previously described 9 photographs depicting the orthodontic appliances. After each picture, participants rated the appliance for attractiveness on an 11-point Likert scale (ranging from 0 representing “extremely unattractive” to 10 representing “extremely attractive”). They then answered two yes/no questions about the acceptability of the appliance for themselves and for their children. The following set of questions were related to participant willingness to pay for each appliance for themselves and for their children. They viewed 8 successive pairs of photographs, the first labelled photographs A and the second labelled B. Photograph A was kept constant and showed standard metal brackets because it is the most commonly used orthodontic appliance. Photograph B changed with each successive pair to show one of the 8 other orthodontic appliances. Participants were told that the basic price to have the orthodontic appliance in photograph A was 20,000 Saudi riyals (SR) (around 5300 dollars). After viewing each pair, participants answered 2 questions asking how much more they would be willing to pay for the orthodontic appliance in photograph B for themselves and their children. They had 12 options to choose from: 1000SR to 10000SR, in 1000SR increments, “I will not pay more, I prefer braces in Picture A”, or “I will not pay more, both look the same”. The last section of the questionnaire showed pictures of all appliances labelled A to I (Figure 1) and participants were asked to rank them in their preference order.
We used IBM SPSS Statistics for Windows, Version 25.0. Intrarater reliability was evaluated by asking 20 participants to fill out the questionnaire a second time 2 weeks after their initial attempt. To assess attractiveness, we used the Intraclass Correlation Coefficient (ICC). For acceptability and value, we assessed reliability using Cohen kappa statistics. We calculated frequency distributions of demographic characteristics. We used the Friedman non-parametric test to assess if the differences in attractiveness scores between different appliances were statistically significant. To account for multiple comparisons, pairwise comparisons were done using the Wilcoxon Signed Rank test with Bonferroni corrections (significance set at P value = 0.05/36 =0.001). Assuming that 50% of adults would accept an orthodontic appliance, Binomial test was used to assess if the proportion of adults’ acceptability to each appliance is significantly different from 0.5. We used the Chi-square test to examine the association between the acceptability of each orthodontic appliance for adults and its acceptability for their children, as well as the associations between appliance acceptability and demographic characteristics of participants. We calculated frequency distributions of preference and economic value responses.
Results
The intrarater reliability of participant responses about the attractiveness of orthodontic appliances was strong, with a mean ICC of 0.81 (95% CI=0.41–0.95). The intrarater reliability for acceptability ranged from moderate (κ=0.6, 95% CI=0.2–1.05) to perfect agreement (κ=1, 95% CI=1-1), and that for WTP also ranged from moderate (κ=75, 95% CI = 0.46–1.04) to perfect agreement (κ=1, 95% CI=1-1).
Of the 199 adults who participated in the study, 44.7% were males and 55.3% were females. The mean age of the participants was 27.7± 7.7 years. Table 1 summarizes the demographic characteristics of the study participants. Almost half of the participants (49.2%) attained a bachelor’s degree, and 18.6% had a postgraduate degree. About 16% of the participants finished high school, and 2.5% finished middle school. Only 1 participant had no schooling. Approximately 41% of the participants were employed, 35.2% were students, 4.5% were self-employed and 19.6% were not employed. Almost two-thirds of the participants were single, while 33.7% were married.
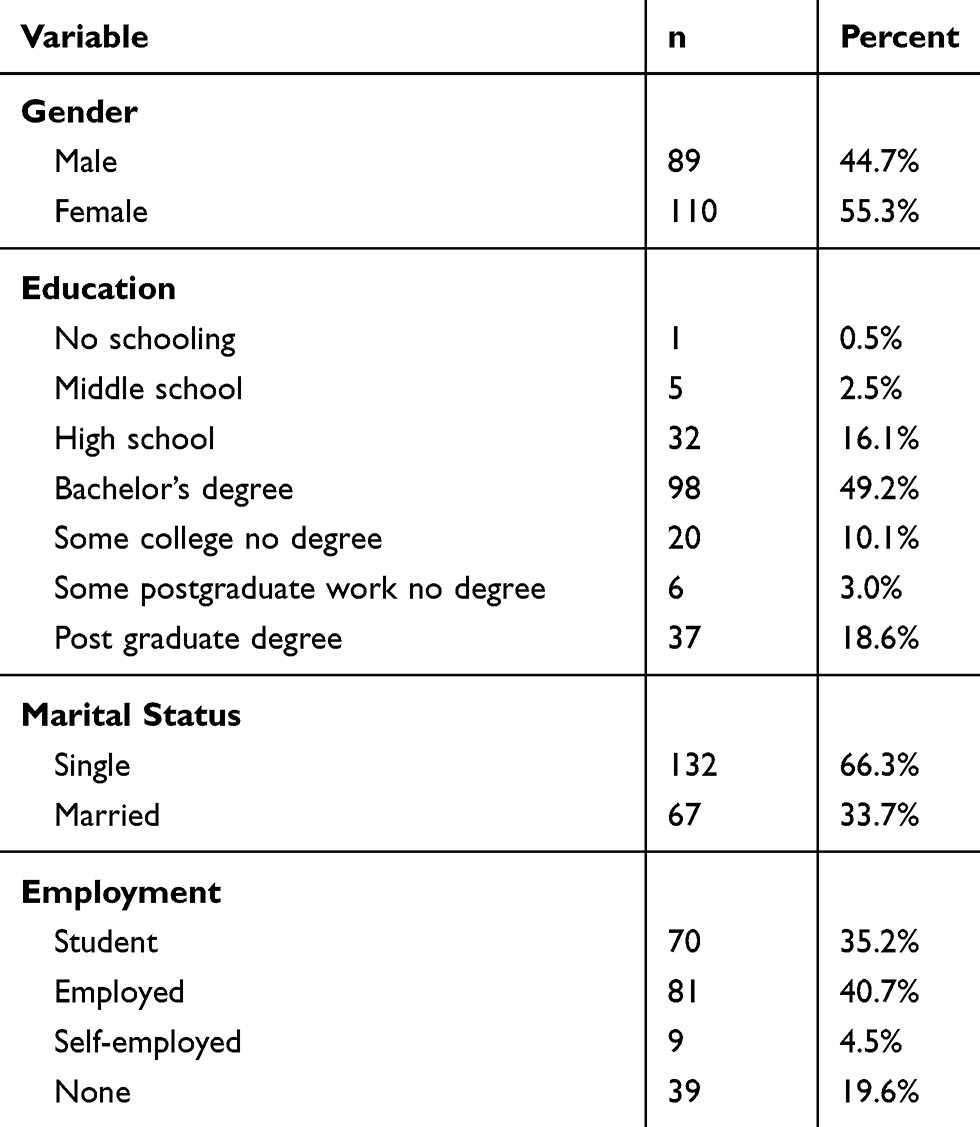 |
Table 1 Demographic Characteristics of the Study Participants (n=199) |
Figure 2 shows the distribution of the scores participants gave to rate the attractiveness of different orthodontic appliances evaluated in this survey. Clear aligners and lingual brackets had the highest median attractiveness scores (Mdn = 8, IQR 6 to 10, for both clear aligners and lingual brackets). On the other hand, shaped brackets had the lowest median attractiveness score (Mdn= 1, IQR= 0 to 5), followed by metal brackets with colored o-ties (Mdn=3, IQR= 0 to 5). Friedman’s test revealed statistically significant differences in the attractiveness scores of various orthodontic appliances (P< 0.0001). Results from pairwise comparisons with Wilcoxon Singed rank test with Bonferroni corrections showed that there was a significant difference between attractiveness scores of standard metal brackets compared to ceramic, ceramic self-ligating brackets, clear aligners and lingual brackets, with each of these appliances having higher median attractiveness scores compared to standard metal brackets (P< 0.0001 for each comparison). On the other hand, metal brackets with colored o-ties and shaped brackets had significantly lower scores of attractiveness compared to standard metal brackets (P< 0.0001). There were no statistically significant differences in scores of attractiveness of metal self-ligating and half metal-half ceramic brackets compared to standard metal brackets (P = 0.3 and P = 0.1 for metal self-ligating and half metal-half ceramic brackets respectively).
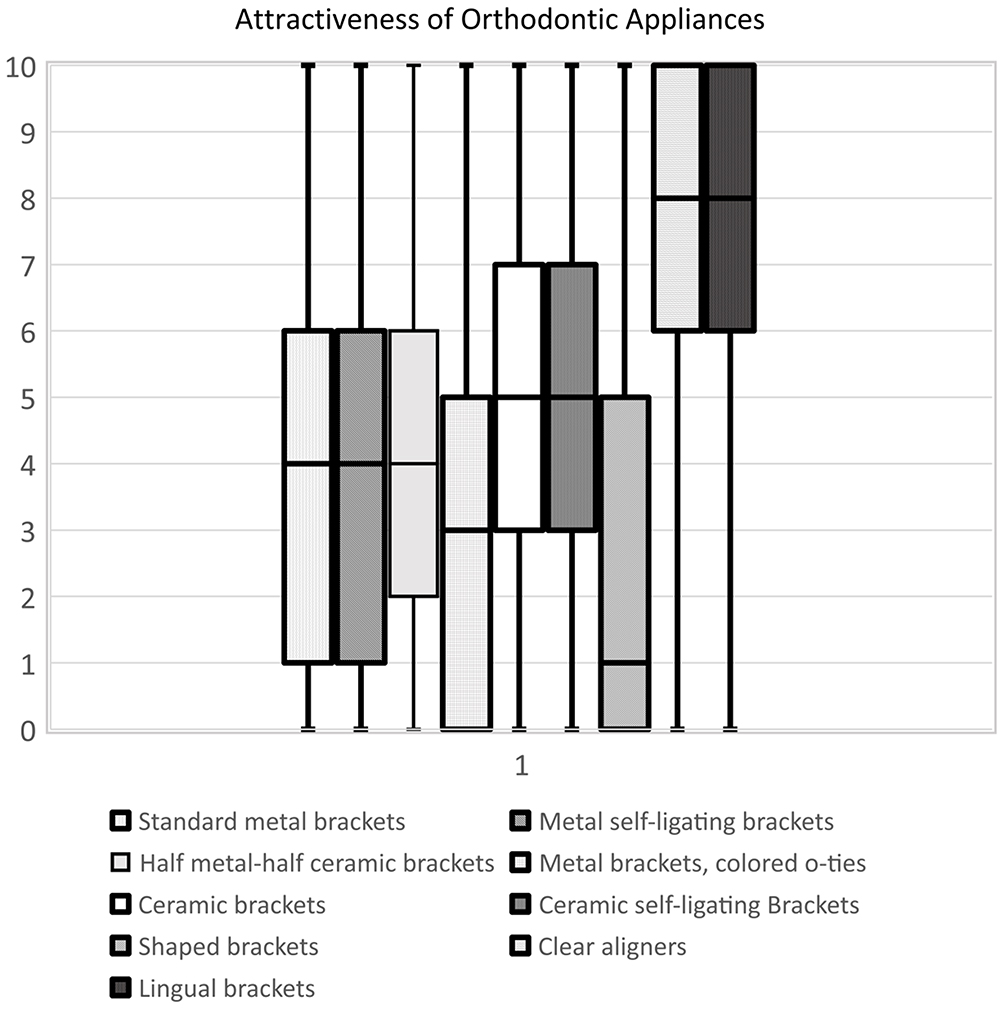 |
Figure 2 Box and whisker plot showing the median and interquartile range of the scores participants gave to rate attractiveness of different orthodontic appliances. |
The acceptability of different orthodontic appliances to adults are illustrated in Figure 3. Results from binomial tests showed that the percentage of adults accepting ceramic brackets, clear aligners, and lingual brackets was significantly higher than the expected 50% (P= 0.007 for ceramic brackets, and P< 0.0001 for clear aligners and P< 0.0001 for lingual brackets). On the contrary, the percentage of adults accepting metal brackets and that for shaped brackets were significantly lower than 50% (P< 0.0001 for metal brackets with colored o-ties and P< 0.0001 for shaped brackets). Figure 4 shows adults’ acceptability of orthodontic appliances for their children. For most orthodontic appliances included in the survey, the percentage of adults accepting the appliance for their children was significantly higher than 50%. However, the percentage of adults accepting shaped brackets for their children was %36, which is significantly lower than the expected 50% (P< 0.0001). Bivariate associations between adults’ acceptability of an orthodontic appliance to themselves and their acceptability of the same appliance for their children is presented in Table 2. For all evaluated appliances, there was a statistically significant association between adults’ acceptability of an orthodontic appliance for themselves and their acceptability of the same appliance for the treatment of their children. In general, adults accepting an appliance for themselves were more likely to accept if for their children, while those not accepting the appliance for themselves were more likely not to accept it for their children (P < 0.0001). There were no significant associations between the acceptability of orthodontic appliances and the demographic characteristics of the participants.
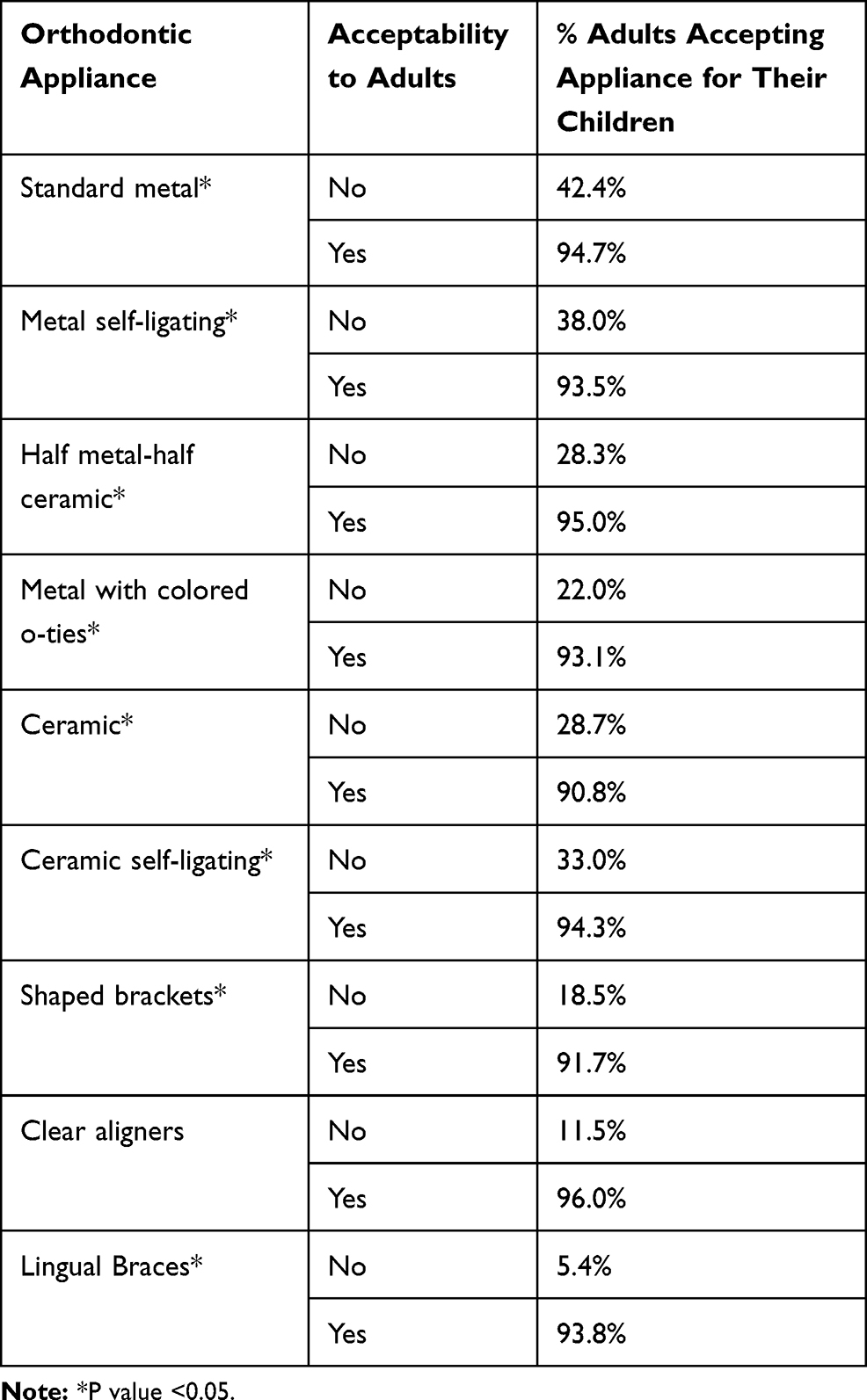 |
Table 2 Bivariate Associations Between Adults’ Acceptability of an Orthodontic Appliance for Themselves and Their Acceptability of the Same Appliance for Their Children (n=199) |
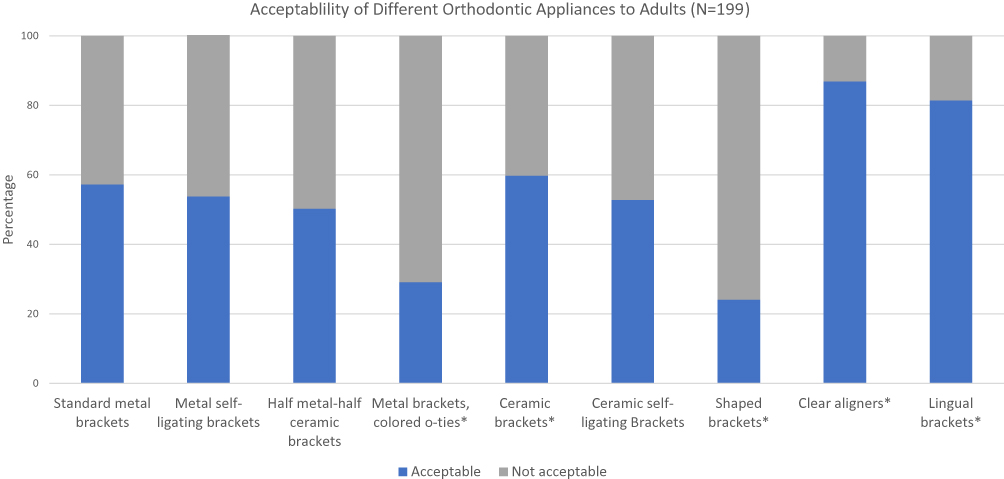 |
Figure 3 Adults’ acceptability of different orthodontic appliances for their themselves. *P value <0.05. |
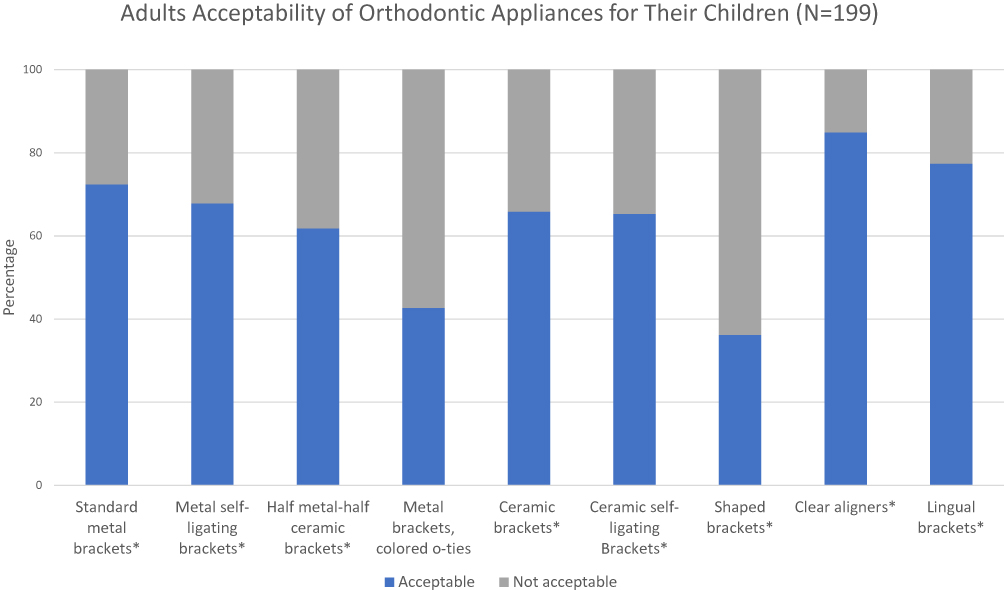 |
Figure 4 Adults’ acceptability of different orthodontic appliances for their children. *P value <0.05. |
The analysis shows that 38.2% of the participants thought that metal self-ligating brackets look the same as standard metal brackets, and 23.1% preferred the standard metal brackets over the metal self-ligating ones. Similar results were found for half metal-half ceramic brackets, with 31.2% of the participants reporting that those brackets and standard metal ones look the same, and 20.6% preferring standard metal brackets. Nonetheless, when they were asked how much more they were willing to pay for orthodontic appliances for themselves compared to the standard metal appliance, 25.6% and 31.2% of the participants considered paying an extra 1000–4000 SR for metal self-ligating and half metal-half ceramic brackets respectively. Almost a quarter of the participants preferred standard metal brackets over ceramic as well as ceramic self-ligating appliances. On the contrary, about 47.7% and 48.7% of the participants were willing to pay an extra 1000–4000 SR for ceramic and ceramic self-ligating appliances respectively. Only a few participants preferred standard metal brackets over clear aligners and lingual brackets. Furthermore, 35.7% of the participants were willing to pay extra 1000–4000 SR for clear aligners, and a higher percentage (50.2%) were willing to pay an extra 5000–10,000 SR for clear aligners. Lingual brackets were also valued by participants with 42.7% willing to pay an extra 1000–4000 SR for them, and 40.2% willing to pay extra 5000–10,000 SR for treatment with lingual brackets. Similar results were found when participants were asked how much they were willing to pay extra for orthodontic appliances for their children compared to the standard metal appliance. Table 3 summarizes the amount participants were willing to pay extra for treatment of themselves and their children with an orthodontic appliance compared to standard metal brackets.
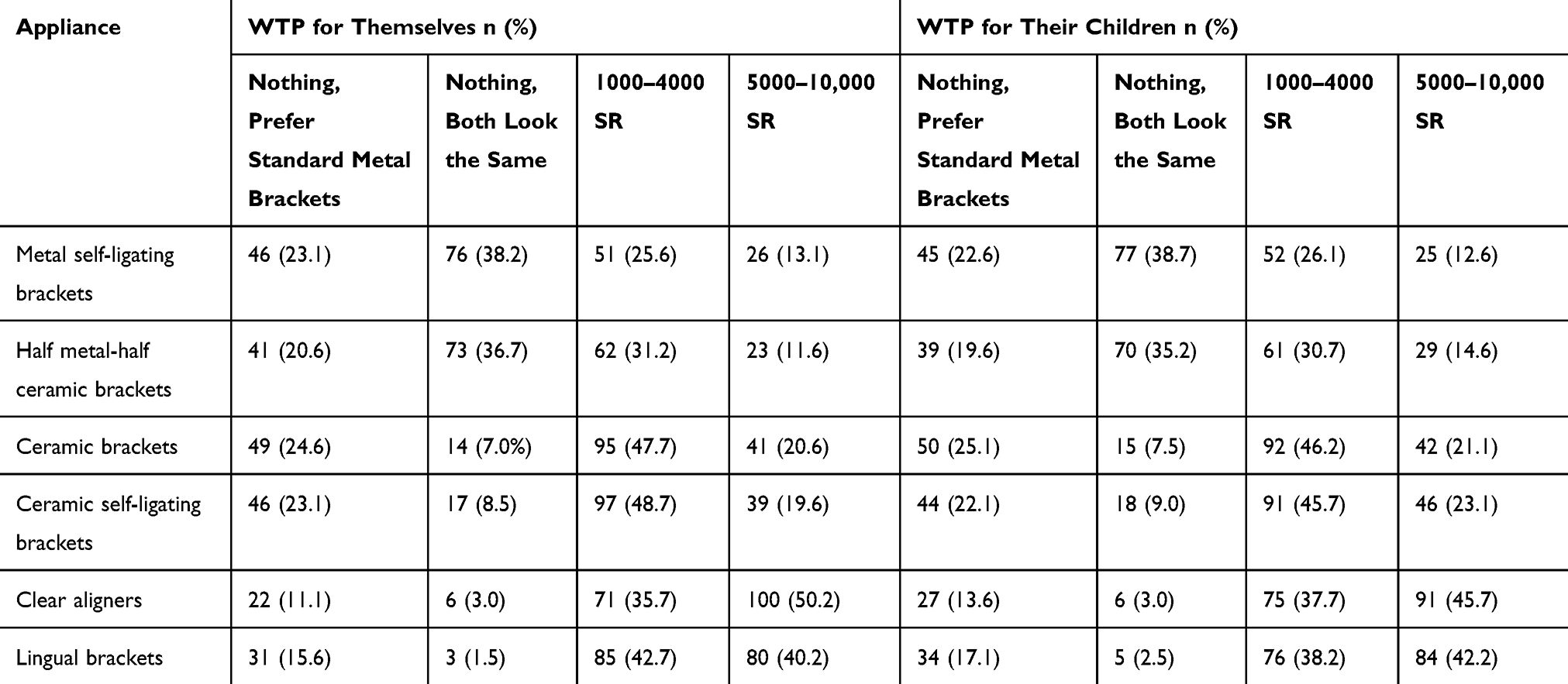 |
Table 3 Amount of Extra Money Participants Were Willing to Pay (WTP) for Treatment with an Orthodontic Appliance Compared to Standard Metal Brackets (n=199) |
Figure 5 shows adults orthodontic appliance preference, when asked to rate the appliances from most to least preferred, 39.2% of the participants rated lingual brackets as their most preferred orthodontic appliance, and 34.2% preferred clear aligners. About 16% of the participants preferred metal brackets. The least preferred orthodontic appliances to adults were ceramic brackets and metal brackets with colored o-ties with only 6.5% and 4% of the participants rating them as their most preferred orthodontic appliances respectively.
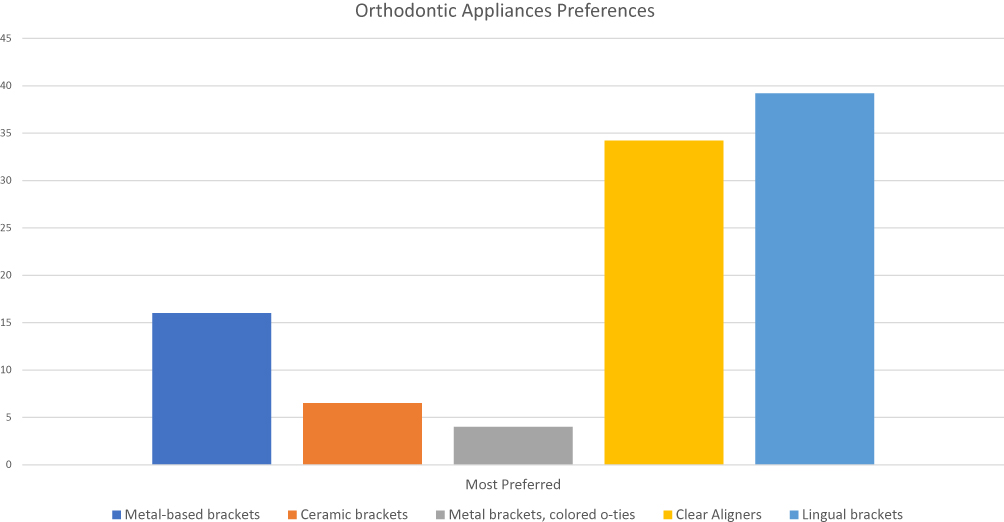 |
Figure 5 Adults’ preference of different orthodontic appliances. (n=199). |
Discussion
The values societies and cultures place on esthetics constantly evolve over time.2 These societal views influence perception of the esthetic and monetary values of different orthodontic appliances.5 Practitioners need to be informed of their consumers’ preferences to make better practice management decisions and to satisfy their patients’ needs.
The need for comprehensive orthodontic treatment in Saudi Arabia was reported to be as high as 77%17 with highly variable perceptions of their esthetic and functional needs.15 Our study showed that adult patients have a wide range of perceptions of the attractiveness of the various orthodontic appliances. The least attractive appliances were the most visible ones, namely the shaped-brackets followed by the metal brackets with colored o-ties. On the other hand, the most attractive appliances were the clear aligners and lingual brackets. There were also the appliances our participants preferred the most. These findings corroborate those of Rosvall and Ziuchkovski et al who found that the least visible appliances, clear trays and lingual appliances, were the most attractive treatments chosen by adults from the central United States.5,10 However, this contradicts the prior study of perception of Saudi adults of orthodontic appliances in 2018, which found that ceramic brackets were the most favored treatment choices, while lingual brackets were positioned the least in the ranking.16 While it is not clear to the authors why there is a difference in preference between the two studies, one may speculate the participants in the earlier study ranked their appliance preferences based on other parameter in addition to the esthetic value, which might have played a role.
Our findings showed that our participants were willing to pay more to have esthetically pleasing, least visible appliances placed for them rather than the standard metal braces. We speculate that this willingness to pay likely indicates that participants perceived impact orthodontic appliances on esthetic appearance and possibly how they are perceived in social situations. This has been reported.8 Participants also preferred less visible appliances for their children but were not willing to pay more for them to be worn by children. This may mean that parents perceive that it is not necessary for their children to have the most esthetically pleasing appliance. Parents may feel that their children will not suffer from negative self-perception or judgement in social situations as it is perhaps more common to see children wearing visible braces than adults. This contradicts Rosvall’s finding that adults were willing to pay more for less visible appliances for their children.5 Multiple factors may account for the different findings between the two studies. Societal values placed on the esthetic appearance of the appliances when used for children may simply be different across the two different cultures. Differences in socioeconomic circumstances of parents and the reimbursement plans in the two different healthcare systems may also play a role.
This study had limitations. First, the photographs presented to participants may not have been completely representative of how the appliances look in real life. This is because we chose a model with a near-ideal smile, good tooth alignment, and no malocclusion or midline shift. Therefore, the photographs shown do not represent how appliances will look on patients, especially in the beginning of orthodontic treatment.
This study does not reflect the opinion of children since parents answered the questionnaires. Even though adult participants preferred less visible appliances for their children, this may not be the case when children are given the choice. This study may not yield the same results in different cultures. Further investigations using different ways of measuring and understanding the monetary value adult patients give to different appliances may be warranted.
Conclusion
Adult laypeople vary in their esthetic and monetary perception of different orthodontic appliances. Regardless of their demographics, they seem to find commonly used metal brackets less attractive and less acceptable compared to the more esthetic options such as clear aligners and lingual brackets for themselves as well as for their children.
Adults preferred more innovative esthetic appliances over standardly used ones and were willing to pay more, for themselves but not for their children, for what they considered a more esthetic option. This study shows an array of preferences for the available orthodontic appliances.
Therefore, orthodontists should offer and explain all options for their patients to allow patients to make an informed decision.
Acknowledgments
The project was funded by the Deanship of Scientific Research (DSR), King Abdulaziz University, Jeddah, under grant No. (DF-076-254-1441). The author, therefore, acknowledges DSR technical and financial support.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Russell JS. Current products and practice: aesthetic orthodontic brackets. J Orthod. 2005;32(2):146–163. doi:10.1179/146531205225021024
2. Sarver DM, Ackerman JL. Orthodontics about face: the re-emergence of the esthetic paradigm. Am J Orthod Dentofacial Orthop. 2000;117(5):575–576. doi:10.1016/s0889-5406(00)70204-6
3. Bergström K, Halling A, Wilde B. Orthodontic care from the patients’ perspective: perceptions of 27-year-olds. Eur J Orthod. 1998;20(3):319–329. doi:10.1093/ejo/20.3.319
4. Jeremiah HG, Bister D, Newton JT. Social perceptions of adults wearing orthodontic appliances: a cross-sectional study. Eur J Orthod. 2010;33(5):476–482. doi:10.1093/ejo/cjq069
5. Rosvall MD, Fields HW, Ziuchkovski J, Rosenstiel SF, Johnston WM. Attractiveness, acceptability, and value of orthodontic appliances. Am J Orthod Dentofacial Orthop. 2009;135(3):276–e1. doi:10.1016/j.ajodo.2008.09.020
6. Walton DK, Fields HW, Johnston WM, Rosenstiel SF, Firestone AR, Christensen JC. Orthodontic appliance preferences of children and adolescents. Am J Orthod Dentofacial Orthop. 2010;138(6):698–e1. doi:10.1016/j.ajodo.2010.08.001
7. Moshkelgosha V, Salahi M, Rostami S. Evaluation of perceived acceptability, beauty and value of different orthodontic brackets. J Dent Biomater. 2015;2(1):33–38.
8. Fonseca LM, de Araújo TM, Santos AR, Faber J. Impact of metal and ceramic fixed orthodontic appliances on judgments of beauty and other face-related attributes. Am J Orthod Dentofacial Orthop. 2014;145(2):203–206. doi:10.1016/j.ajodo.2013.10.016
9. Zarnke KB, Levine MA, O’Brien BJ. Cost-benefit analyses in the health-care literature: don’t judge a study by its label. J Clin Epidemiol. 1997;50(7):813–822.
10. Ziuchkovski JP, Fields HW, Johnston WM, Lindsey DT. Assessment of perceived orthodontic appliance attractiveness. Am J Orthod Dentofacial Orthop. 2008;133(4):S68–S78. doi:10.1016/j.ajodo.2006.07.025
11. Kiyak HA. Comparison of esthetic values among caucasians and Pacific-Asians. Community Dent Oral Epidemiol. 1981;9(5):219–223. doi:10.1111/j.1600-0528.1981.tb00333.x
12. Mugonzibwa EA, Kuijpers-Jagtman AM, Van ’t Hof MA, Kikwilu EN. Perceptions of dental attractiveness and orthodontic treatment need among Tanzanian children. Am J Orthod Dentofacial Orthop. 2004;125(4):426–433. doi:10.1016/S088954060300948X
13. Miguel JAM, Sales HX, Quintão CC, Oliveira BH, Feu D. Factors associated with orthodontic treatment seeking by 12-15-year-old children at a state university-funded clinic. J Orthod. 2010;37(2):100–106. doi:10.1179/14653121042957
14. Feu D, Catharino F, Duplat CB, Capelli Junior J. Esthetic perception and economic value of orthodontic appliances by lay Brazilian adults. Dental Press J Orthod. 2012;17(5):102–114. doi:10.1590/S2176-94512012000500015
15. Akeel R. Attitudes of Saudi male patients toward the replacement of teeth. J Prosthet Dent. 2003;90(6):571–577. doi:10.1016/j.prosdent.2003.09.007
16. Bindayel NA. Awareness of orthodontic modalities and preference of appliance and payment options in Saudi Arabia. Saudi J Oral Sci. 2018;5(2):98–103.
17. Al-Jobair AM, Baidas LF, Al-Hamid AA, Al-Qahtani SG, Al-Najjar AT, Al-Kawari HM. Orthodontic treatment need among young Saudis attending public versus private dental practices in Riyadh. Clin Cosmet Investig Dent. 2016;8:121.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.