Back to Journals » Journal of Healthcare Leadership » Volume 17
Adopting an Integrative and Co-Design Process to Contextualize Management Capacity Building in Hospitals
Received 16 June 2025
Accepted for publication 27 October 2025
Published 12 November 2025 Volume 2025:17 Pages 721—736
DOI https://doi.org/10.2147/JHL.S547285
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Russell Taichman
Zhanming Liang,1 Hui Zhang2
1College of Business, Law and Governance, James Cook University, Townsville Campus, Townsville, Queensland, Australia; 2School of Public Health, Sun Yat-Sen University, Guangzhou, Guangdong, People’s Republic of China
Correspondence: Hui Zhang, School of Public Health, Sun Yat-sen University, No. 74, Zhongshan 2nd Road, Guangzhou, 510080, People’s Republic of China, Email [email protected]
Introduction: Context plays a critical role in shaping how interventions are designed and implemented, and must therefore be considered prior to implementation. There is consensus that the relationship between contextual factors and intervention outcomes is best understood using qualitative and quantitative methods, the process for considering and incorporating context remains unclear. Drawing on a recently completed study focusing on building hospital management capacity, this paper describes and discusses the benefits and learning from the implementation of an integrative and co-design approach.
Methods: This sequential mixed-methods study included managers and clinicians from two district hospitals in China. Focus Group Discussions [FGD] are a critical step in guiding the adaptation of several validated tools in the local hospital context. Data collected from FGDs and online surveys provides a comprehensive understanding of the current state of hospitals.
Results: This study identified a wide range of difficulties faced by mid-level managers and clinical staff in two hospitals. While managers reported hospital-specific challenges, staff across both sites consistently cited issues such as inadequate support, lack of recognition, and lack of patient trust. Survey results also revealed low levels of psychological empowerment, job satisfaction, and perceived leadership effectiveness. Self-assessment using the MCAP tool highlighted significant competency gaps among mid-level managers, particularly in operations management and leading change.
Discussion: The use of a co-design approach broadly engaging relevant key stakeholders from the design and implementation of the project and formulation of improvement strategies is key to enabling project success and maximizing and sustaining project impact.
Keywords: focus group discussions, health managers, leaders, competency, capability, hospitals
Introduction
Roles of Context
Context affects how intervention and change processes should be designed to generate pre-determined outcomes.1 At the same time, economic, cultural, and social factors at the system level and history, culture, specific structures, and processes at the organization level can influence how and the extent to which intervention can generate outcomes.2–5 The relationship between contextual factors and intervention outcomes can be understood through research using either qualitative or quantitative methods. Qualitative studies such as focus groups and interviews help understand the process and interaction between contextual factors, interventions and outcomes is best understood by qualitative studies such as focus groups and interviews.6 Hence, mixed-method studies can generate an in-depth understanding of the experiences of those affected by interventions and intervention outcomes gained from a much broader views.7,8 For applied and action research aimed at identifying solutions to problems and formulating strategies for service improvement, the consideration of the local context prior to the finalization of intervention is critical to ensure the relevance and applicability of the proposed actions that suit the local context.9 A qualitative approach, drawing on participants’ lived experiences through public forums, focus groups, or interviews, is one of the most appropriate ways to develop an insightful understanding of issues.10 Despite growing recognition of the importance of context, many improvement initiatives overlook local factors, organisational culture, and system-level dynamics. There is limited guidance on how to systematically identify, assess, and integrate contextual factors into the design phase of interventions/improvement strategies. Context is often not treated as a dynamic and evolving influence on implementation and outcomes. This can lead to misalignment between intervention strategies and the environments in which they are deployed, reducing their effectiveness and sustainability.2,4
Collaborative and Qualitative Approach in Intervention Design
Constructivism in qualitative research acknowledges multiple subjective realities and encourages exploration of multiple perspectives.11 In healthcare research, the pragmatic approach focuses on practical solutions that improve health and health outcomes12 and generate actionable knowledge to inform evidence-based interventions and policies.7 For its success, collaboration between key stakeholders such as practitioners, researchers, and policymakers is emphasized to ensure that the suggested solutions and research outcomes are relevant, applicable, and practical. A pragmatic approach is extremely useful for adapting solutions/interventions in the local context9 by understanding the perspectives of key stakeholders and the complex factors that may affect the outcomes of solutions/interventions. This pragmatic approach reinforces the importance of building trust between the project teams and key stakeholders (or collaborative partners) for its sustainability.9 However, the pragmatic approach may overemphasize practical outcomes which potentially conflict with the values and priorities of key stakeholders.7 Adopting a collaborative co-design approach creates opportunities for all key stakeholders to actively engage in project design, implementation, and evaluation processes to address concerns, solve conflicts, and develop a sense of ownership which is critical for addressing resistance and improving compliance.
Adopting a Co-Design Approach in Building Organization Management Capacity
Co-design has emerged as an effective approach in designing and implementing research that can inform the formulation of service improvement strategies and development of policies in health and community care.13 Going beyond the commonly known participatory approach,14 co-design is an active process of bringing key stakeholders together in partnership with each other throughout the research process. It is a powerful approach for taking local context into consideration, getting stakeholder buy in, developing ownership and ensuring the delivery of sustainable outcomes.15–17 It also empowers the more vulnerable and those who are often left out of the consultation process to become active partners.18,19 Typically, co-design is guided by the following principles: inclusive, participative, respectful, interactive and outcome-focused.20 Several frameworks have been proposed in previous studies. After studying these frameworks via a systematic literature review process, Greenhalgh et al,21 suggest the following five taxonomy for co-design framework: “power‐focused, priority‐setting, study‐focused, report‐focused, and partnership‐focused—based on their primary focus and intended purpose.” (p.796). Although many co-design toolkits have been developed by government and non-government agencies which are accessible online, the research co-design process and its associated benefits have not been adequately described or evaluated in detail.13 In addition, studies on co-design vastly focus on consumers’ and patients’ engagement in service design and delivery, as confirmed in the scoping review conducted by Slattery et al.13 In studies aiming at building organizational management capacity, where policymakers, managers, and clinicians are the key stakeholders, no study has yet been found that describes the use of the co-design approach.
Importance of Management Capacity Building
Hospital managers, particularly those with dual managerial and clinical roles, are instrumental in providing consistent and high-quality patient care.22,23 International evidence has positively linked a supportive work environment and a clear vision that empowers staff retention and job satisfaction.24–26 Globally, in both the developed and developing world over the past two decades, there has been increasing momentum and investment at both the system and organization levels in developing a competent health management workforce. Such investments can be demonstrated in the reinforcement of mandatory training for health managers, an increased number of management competency studies and relevant publications,27 transitioning management development from an ad hoc basis to more formal efforts. For example, a recent desktop search in Australia confirmed that 24 postgraduate health management programs are currently being offered, with the majority of them being established no more than 20 years ago.
Despite increasing efforts, health service managers, particularly those at the mid- and lower-management levels, often lack opportunities to develop their management capability before and after taking up management roles.28–30 This issue is more significant in countries where health management positions are generally filled by clinicians based on their clinical seniority rather than their competence and experience in managerial roles. This directly affects their confidence in their managerial role and their ability to lead both the organization and the team successfully.31,32 At the organizational level, developing managers’ capabilities and filling management positions with competent managers are core parts of human resource management policies. Creating an environment that enables managers to apply management competencies to their management roles and translate them into positive management outcomes is of utmost importance. Figure 1 illustrates how context may influence improvement efforts in management capabilities at the organisational level.
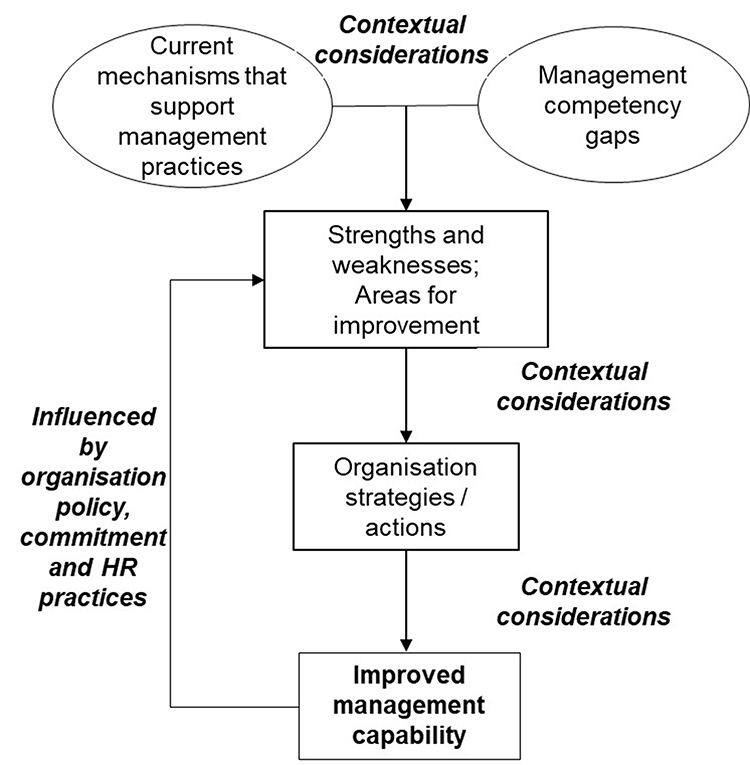 |
Figure 1 Contextualisation vs management capability development. |
Learning from Existing Evidence on Management Capability Development
In a resource-constrained healthcare environment, learning from the experiences gained and adopting tools that have been developed in other healthcare contexts are critical to improving the effectiveness and efficiency of managing healthcare organizations and quality care provision.33,34 In health service research, such as management competency studies, it is common and cost-effective to adopt tools and methods developed and tested in other target groups or countries.27 A systematic scoping review of management competency studies conducted by Kakemam and Liang27 in both the health and non-health industries reinforced the importance of learning and “borrowing” rather than recreating the wheel to propose a framework to guide future management competency studies. They developed a framework that supports the adoption of management competencies identified in studies in various healthcare contexts. It also highlights the importance of considering the context in which managerial tasks are performed by adopting either a qualitative or mixed-method process. The management competency assessment partnership tool (MCAP Tool) originally developed and validated in the Australian health context between 2011 and 2014 has been used globally to generate new knowledge and to guide the development of the health management workforce by leading professional institutions.27,31,32,35–37 The MCAP Tool has already been translated in Chinese language with both content validity and internal consistent being confirmed.31,32 Hence, it has been adopted by the current study. Focus groups are commonly adopted to elicit managers’ views on competency requirements and the difficulties they encounter in their roles. However, many studies failed to provide adequate details on how such studies were implemented, participants’ engagement strategies, and the applicability of the research results were considered.27
Focus of the Paper
Using a recently completed project aimed at building hospitals’ management capacity as an example, this paper describes and discusses the benefits and learning from the integration of a co-design, active engagement, and mixed-method process to ensure that the adapted tools and the developed improvement strategies have given the local context full consideration – an innovative approach in health management research. The integration process, which takes cultural, economic, social, and organization/system specifications into consideration, can guide contextual adaptation.
Contextual Background of Two Public Hospitals
To develop unified views on patient experience and staff job satisfaction in public hospitals, the Chinese Government implemented an annual National Public Hospital Patient Satisfaction Survey (NPHPSS) in 2017. The survey data from 2021 indicated that the mean satisfaction scores of both patients and staff at two local hospitals (ZXYH and RMH) located in the same District were well below the mean scores of the 496 hospitals that completed the survey in the same province. This District is one of the three regional health districts in a Level III city in Guangdong Province, China. District hospitals, ZXYH and RMH, are the only two hospitals that provide medical services to a population of 374,700 in the the District. The District Health Department identified the pressing need to address low staff job satisfaction and low patient satisfaction with care by building the management capacity of hospitals. The two authors of this paper were tasked with gathering evidence to guide strategy formulation via an active engagement approach, with broad engagement across hospitals.
Material and Methods
Guided by the principles of the co-design and qualitative research approach and the benefits of combining a quantitative approach in getting a much broader view, a sequential mixed-method study was implemented (refer to Figure 1) involving both managers and clinicians of both hospitals. The project also adopted a validated management competency development process35 with the inclusion of a number of validated tools. Figure 2 illustrates the conceptual framework and the project flow. Table 1 provides the details of each key step in terms of purpose and participants.
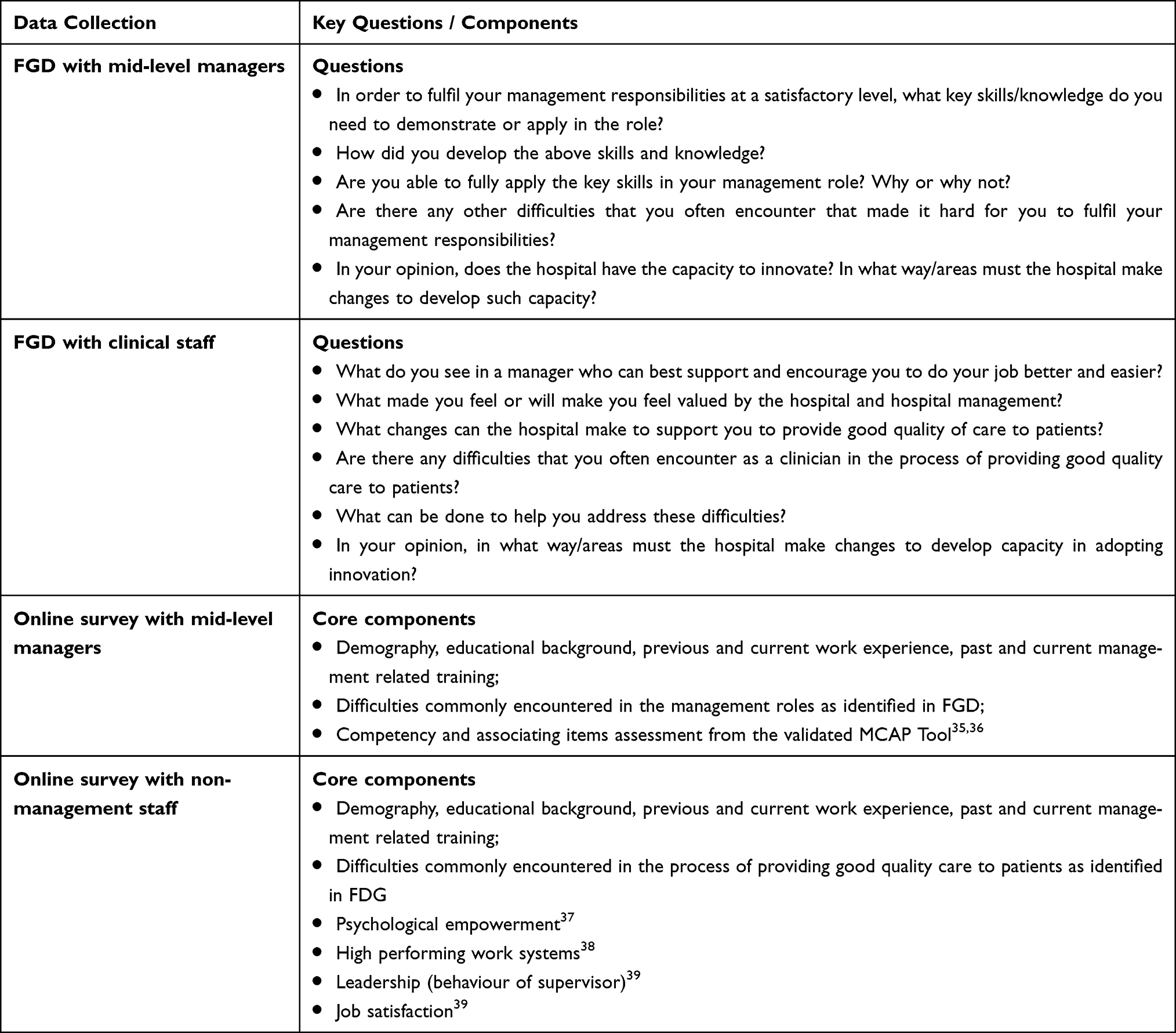 |
Table 1 Key Focus of the FGD and Online Survey |
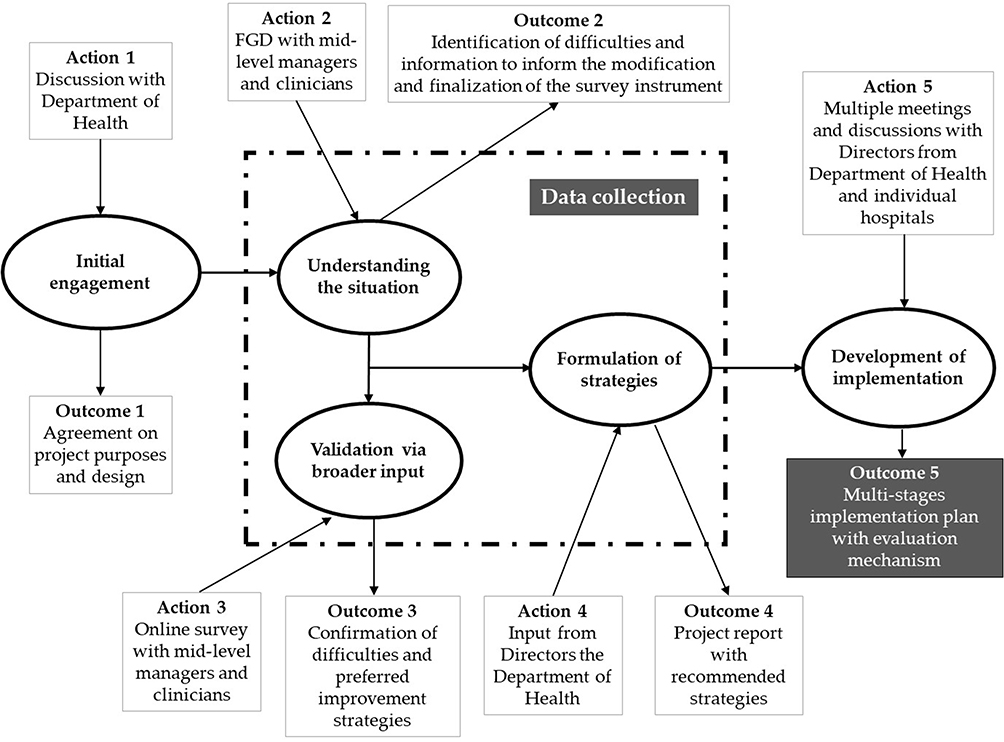 |
Figure 2 Multi-phase project design with associating actions and outcomes. |
Specific Consideration in the Design of the Study
The study included three primary target groups: mid-level managers, clinicians, and non-clinical staff (technicians and administrative staff). Data collected from these groups via focus group discussions (FGD) and online surveys provide a comprehensive understanding of the current state of hospitals. The two FGDs were conducted separately with mid-level managers and clinical/nonclinical staff in each hospital. All members of the primary target groups from both hospitals were invited to complete online surveys. To enhance the rigor of the study, selection and response bias and bias resulted by facilitation of focus group discussion were considered throughout the research design and implementation. All mid-level managers, clinicians, and non-clinical staff from both hospitals were invited to participate in the FGDs and online surveys. This inclusive approach would minimize selection bias. In addition, reinforcement of the voluntary nature of the study and confidentiality and anonymity in both FGDs and surveys encourage responses without coercion. The use of validated instruments (eg, MCAP Tool, psychological empowerment scale) further supported the reliability of responses. In addition, FGDs were facilitated by trained and experienced members of the research team who followed a semi-structured guide to ensure consistency across sessions. Facilitators were able to maintain neutrality, avoid leading questions, and encourage open dialogue.
The key questions for the FGD and the key components of the two survey instruments are included in Table 1.
Focus group discussions not only gathered important information that contributed to the development of the two online survey instruments but also increased the momentum of change and improvement across the organization. This momentum is directly attributed to the high response rate of both the online surveys. Focus group discussions and online surveys were conducted separately at each of the hospitals which were critical for gathering information to inform the formulation of plans for individual hospitals and at the District Health level. The details are shown in Figure 2 and Table 2.
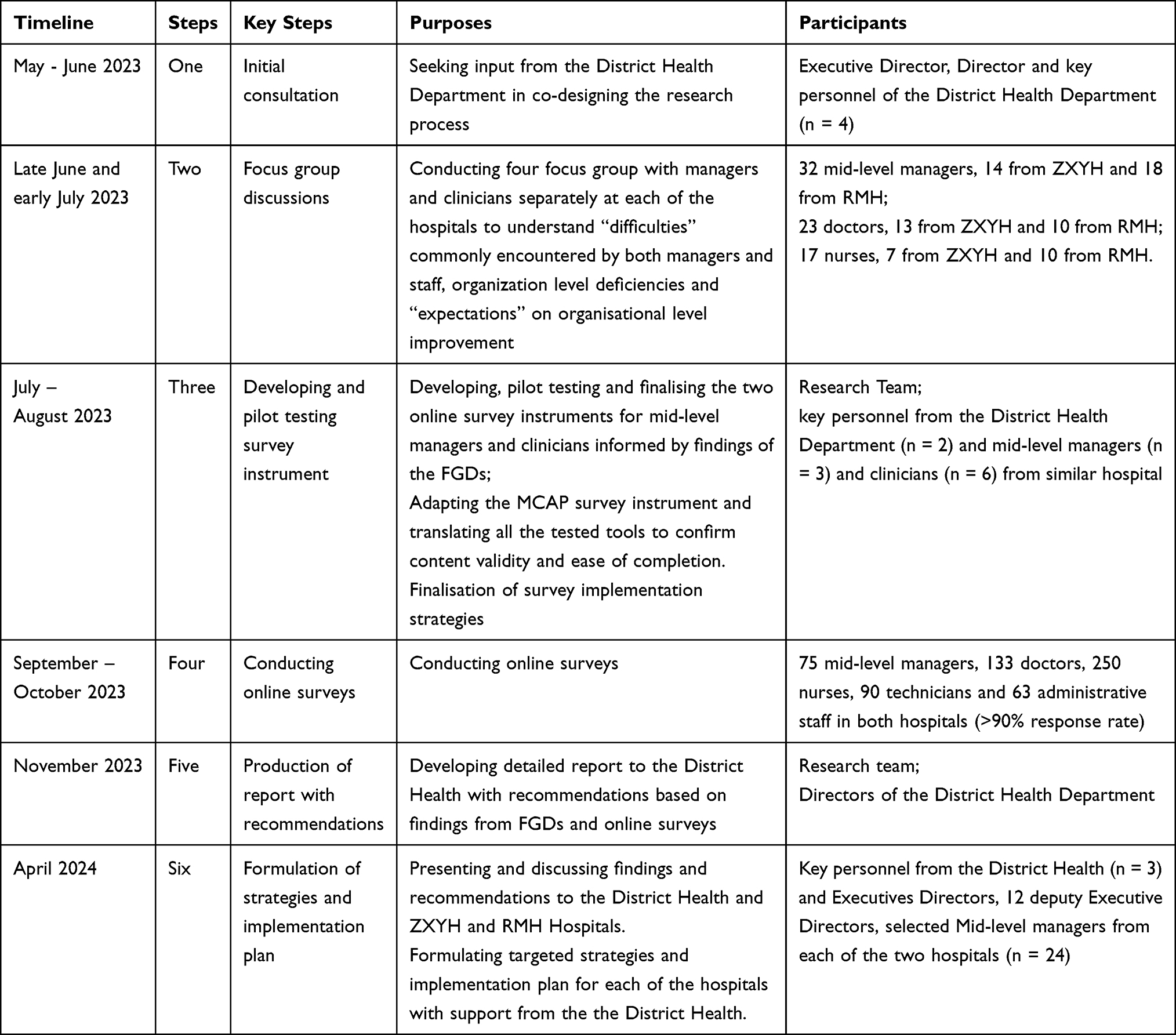 |
Table 2 Detailed Project Steps, Purposes and Participants |
The secondary target groups were officials from the Health District and the senior executives of both hospitals. The groups primarily contributed to project design, the process of formulating strategies, and the implementation plan. The groups did not participate in either the FGDs or online surveys but were engaged in interactive discussions and meetings with the research team.
Data Analysis
Common qualitative and quantitative data analysis techniques were applied, including thematic content analysis of qualitative data collected from FGDs, open-ended questions included in online surveys, and descriptive analysis of quantitative data collected from surveys.
Results
Confirmation of Difficulties via FGDs
This study generates a large amount of rich qualitative and quantitative data. The FGDs with mid-level managers identified 18 difficulties encountered in their management roles. The following five difficulties were consistent with the 13 difficulties included in the MCAP survey.
- Team conflicts
- Confronting higher managements level
- High staff turnover
- Losing high performing staff
- Changing team skills requirements
As a result, 26 difficulties were included in an online survey of mid-level managers. FGDs with clinicians (doctors and nurses) generated 27 difficulties that were included in online surveys with both clinical and non-clinical staff.
Confirmation of Difficulties via Online Survey
Survey participants were asked to select 5 −7 difficulties that they most commonly encountered in their roles from a list of 26 and 27 items for mid-level managers and clinical/non-clinical staff, respectively. Table 3 details the six difficulties most commonly encountered by the participants which were selected by more than 30% of the participants. The six difficulties most commonly encountered by mid-level managers differed vastly between the two hospitals. However, five of the six difficulties most commonly encountered by the non-management staff at the two hospitals were the same.
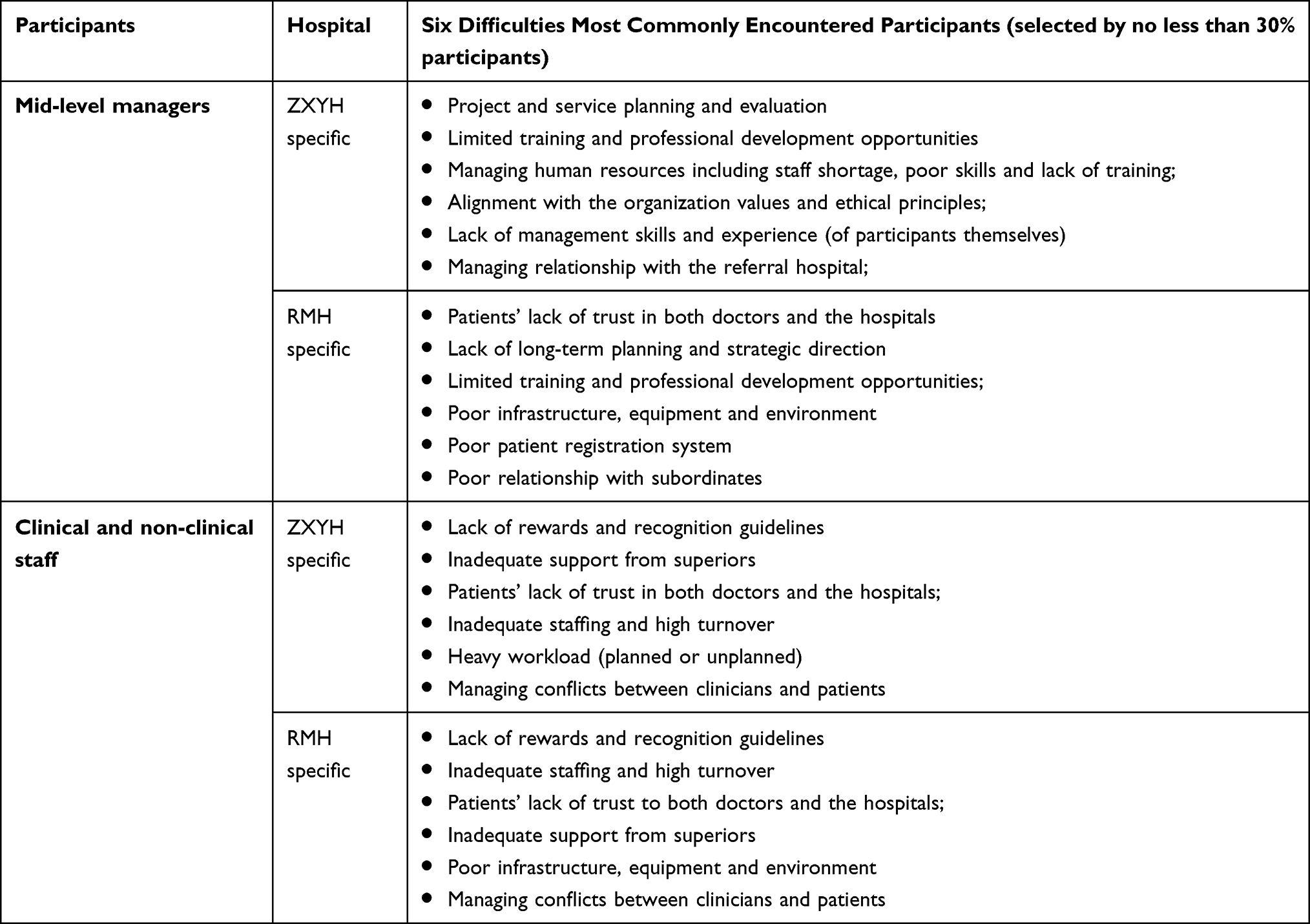 |
Table 3 Difficulties Commonly Encountered |
Lack of Support and Recognition from Management and Organization
The online survey with non-management staff, including doctors, nurses, technicians, and administrative staff, confirmed inadequate support and recognition from managers and the hospital as an organization. Figure 3, 4, and 5 present the proportion of non-management staff from each hospital who chose agree or strongly agree for each of the 12 psychological empowerment items, seven job satisfaction items, and 19 leadership behaviors demonstrated by mid-level managers. The details of these items are provided in Appendix 1.
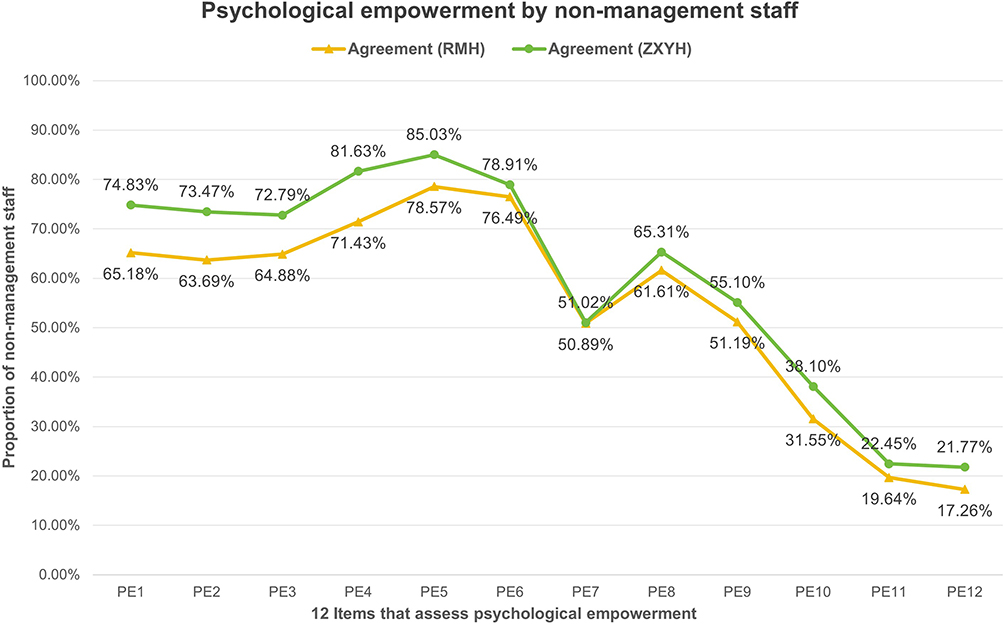 |
Figure 3 Psychological empowerment by non-management staff. |
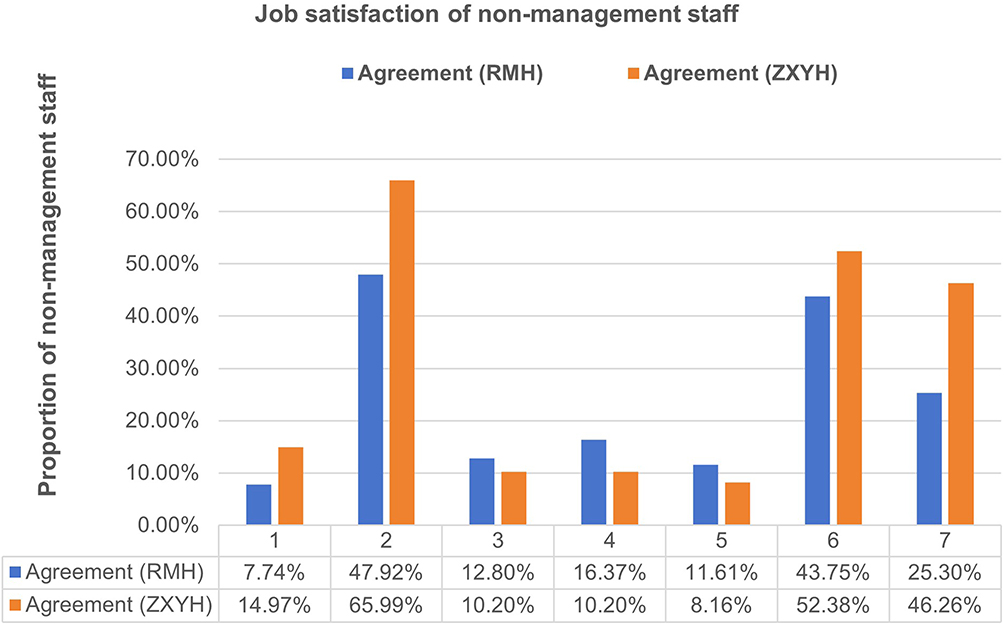 |
Figure 4 Job satisfaction of non-management staff. |
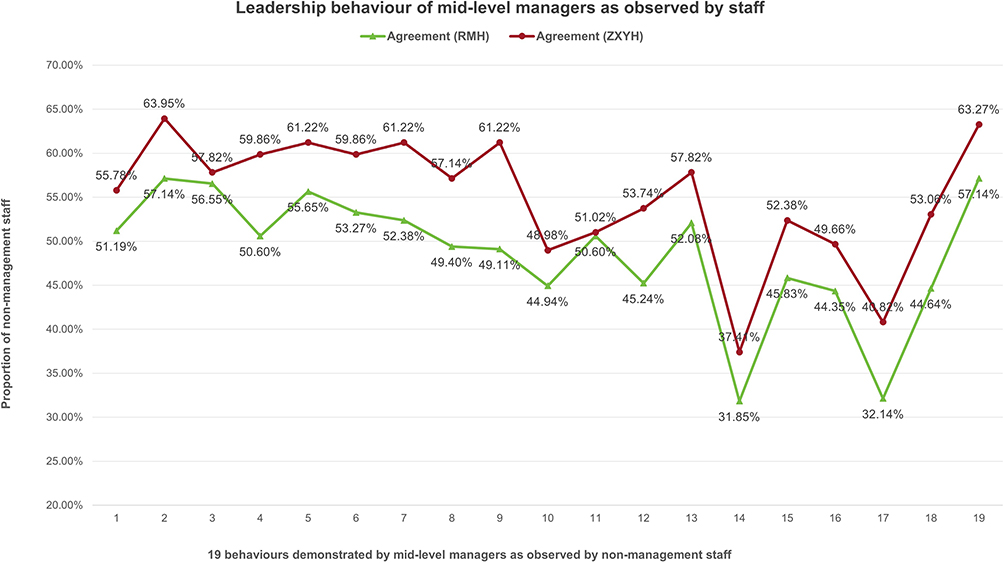 |
Figure 5 Leadership behaviour of mid-level managers as observed by staff. |
The results indicate that a significant proportion of non-management staff believed that they were not given the autonomy to do their jobs (items PE 7,8,9) and that the organization did not recognize their importance to the job and the organization. Their level of job satisfaction and perceived importance to the organizations were low (items PE 10,11,12) (See Figure 3). This trend was consistent across the two hospitals.
The results indicate that a significant proportion of non-management staff was not satisfied with their jobs, with 10–15% of them contemplating leaving the hospital (see Figure 4). Below are the details of the six job-satisfaction items.
The results indicate that less than 55% of non-management staff from RMH agreed that their immediate managers (mid-level managers) demonstrated each behavioral item (see Figure 5). Nine of the 19 items were agreed upon by less than 50% of the staff. Each of these leadership items was agreed upon by a slightly higher proportion of non-management staff from ZXYH, except for item 11, where the result is similar.
Low Competency Level Amongst Mid-Level Managers
Self-assessment of core management competencies and associating behavioral items based on the MCAP assessment tool35,36 confirmed competency gaps among mid-level managers. Figure 6 presents the mean scores for each of the six core management competencies from each hospital and shows the variation in the mean scores received. Competency 4 – “Interpersonal, communication qualities and relationship management” received the highest mean score of 4.60 and 5.20 for RMH and ZXYH, respectively. Competency 2 – “Operations, administration and resource management” and competency 6 – “Leading and managing change” received the lowest meant score from both hospitals. In addition, the mean scores received for each of the competencies for mid-level managers from ZXYH were all 0.5, which was higher than the mean scores from RMH. Details of the MCAP competencies and 13 behavioral items are included in Appendix 1.
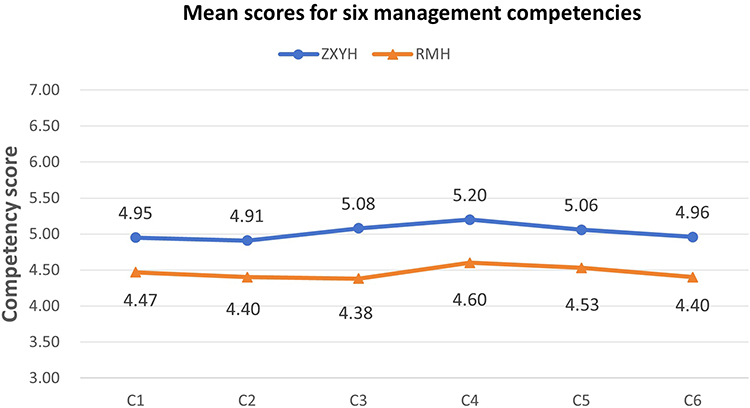 |
Figure 6 Mean scores for six management competency. |
In the MCAP tool, each of the six core management competencies is assessed using a number of behavioral items. Figure 7 shows the mean scores for each of the 13 behavioral items for assessing competency 5 – ‘Leading people and organizations received from mid-level managers from each hospital to demonstrate how strengths and weaknesses within each competency are identified. It clearly shows the variation in mean scores across the 13 behavioral items and consistently higher scores for ZXYH.
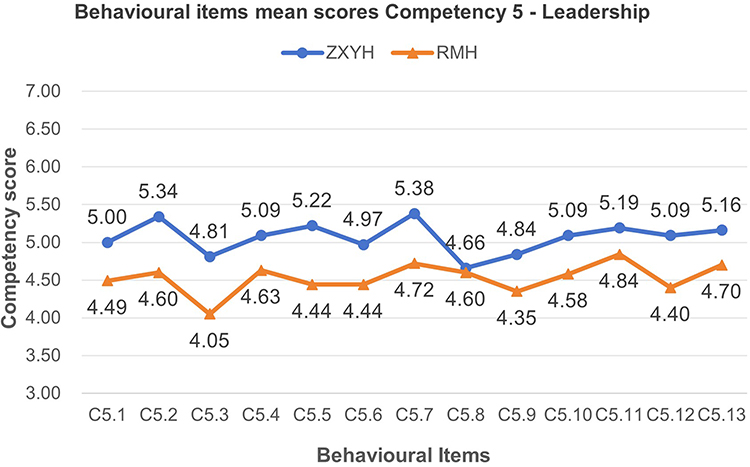 |
Figure 7 Behavioural items mean scores Competency 5 – Leadership. |
Discussion
This study reinforces the theoretical proposition that context affects the design and implementation of strategies that enhance management capability1,40 and demonstrates the benefits of adopting validated tools such as the MCAP Tool35,36 can be adapted through co-design to suit local organisational contexts. The findings contribute to the growing body of literature on contextualized competency development and organization capacity building. The study also advances the understanding of co-design as a strategic mechanism in organisational development, aligning with participatory design theories.13,15,17,20
Value of the Integrative and Co-Design Approach
Using a six-step integrative and co-design approach, the project successfully collected contextually sensitive evidence from two hospitals to guide the formulation of strategies for building hospital management capacity. In support of the concept of “management is context sensitive”.1,40 The project adopted internationally validated tools after testing content validity and actively engaging staff members across two hospitals during the data collection process. The project obtained information not only relevant to guiding individual hospitals to plan for their future actions, but also important to the District Health Department for developing actions in building hospitals’ capacity to provide quality health services collectively to the population in the district.
Using a mixed-method design to generate evidence that can guide strategy formulation in practice, improvement is not new in the healthcare context. However, the conceptual considerations and actual learning of using research to develop an improvement strategy via a co-design and qualitative process have not received adequate attention. The qualitative method, which is well recognized for its ability to understand the real-world context and dipping into actual experiences and thoughts of people whose opinions count,10,41 is also proven by the study as being powerful in guiding strategy formulation in building organizational management capacity and improving management practices and informs the adaptation of validating research tools in the local context. Additionally, creating an environment that encourages new ideas collaboratively has proven extremely beneficial for conducting robust research and development plans. Engaging end-users and decision makers as partners in ‘idea creation by taking on the preferences and experiences of “end-users” is critical.42 This study further demonstrates the value of utilizing existing expertise and experience to support new creation.
In addition to the active engagement and consultative approach adopted by the project aligning with the co-design principles,20,21 the project’s success is also vastly attributed to two key factors forming a very important part of learning which have implications for adaptation by future research and healthcare organizations in management capacity building:
- Gaining high-level support from District Health and hospital executives and their understanding of the urgency for change and formulation of management capacity-building strategies using an evidence-informed process
- Adopting change management principles, paying attention to change preparation, and motivating the momentum of change across hospitals has led to active participation in FGDs, extremely high survey response rates, and reliability of the data collected.
The Importance of Context
The study consistently identified differences between the two hospitals in terms of the competency levels of mid-level managers and the difficulties that managers encountered most often. Such consistent differences were also found in the job satisfaction of non-management staff and their perceived support and recognition of hospitals. On the other hand, studies also found that the difficulties most often encountered by non-management staff were consistent between the two hospitals. Both hospitals in the study are governed by the same District Health Department and are the only two hospitals providing healthcare services to people living in the same geographic locations; clinical staff qualifications and backgrounds and management staff’s selection criteria and processes are very similar. This confirms the importance of considering the “local context” by collecting evidence to understand organizational strengths and weaknesses when formulating improvement strategies. It also reinforces the importance of implementing a local adaptation process when learning from experiences gained from other organizations and sectors.5,34 In health service and health management research, considering research findings and their implications in the context in which data were collected is important to maximize the impact of the research as it guides adaptation for future studies.4 Therefore, researchers should share this understanding in publications that present research results. However, such efforts have not been common in many health management competency studies, as identified in a scoping review by.27
The completely different difficulties most commonly encountered by mid-level managers between the two hospitals further reinforced the role of organization context in affecting managers’ management competency and performance. Such findings are consistent with studies using the MCAP tool35,36 in assessing the management competencies of senior managers in three hospitals in another province which confirmed the variation in competency levels between different types of management positions and different categories of hospitals.31,32
Context and Framework discussion
The management literature has well accepted that management and management competencies are context sensitive.1,40 However, its application in organizational development and the building of managers’ capabilities is not well understood. The current study supports the notion that management tools, management improvement processes, and strategies cannot be “copied” without modification. Content validity must be considered during the local adaptation process43,44– a process of active engagement with key stakeholders, particularly local experts and study participants. In an organizational context, core components must be considered when formulating strategies and developing solutions.5 Hence, strategies for building management capabilities and improving management structures and processes should be formulated that align with the organizations strengths and weaknesses.45 Such considerations would ensure that the solutions are applicable and appropriate to the context in which such strategies and solutions may apply. The current study demonstrates a process for incorporating organisational context into consideration in developing an understanding of the current management challenges and management capacity-building strategies and in developing strategies that are specific to the two targeted hospitals with broad involvement across hospitals. The active and continuous engagement of mid-level managers, clinicians, senior hospital managers, and policymakers, who play a critical role in funding and supporting the development of both organizations, is key to success. The study piloted and tested a conceptual framework (Figure 1) that guides future evidence-based management capacity building in organizations.
Co-Design Organization Development Strategies
Co-design, a newly emerged concept, has taken “consumer participation” to a higher level with strategic importance.13,15,17 This study has proven its value in contributing to achieving the overall project aims by keeping key stakeholders fully engaged and getting senior management to buy in. The current study integrated a number of key steps, as described by20 in the co-design of the research process. The application of the co-design principles not only contributed to project success but also allowed the utilization of international and local expertise and adaptation of validated tools that improved project efficiency and the applicability of project findings. This study has made a significant contribution to the understanding of what co-designing management capacity building at the organisational level may look like, and the associated actions and expected outcomes. The study translated management capacity building and co-design theory into practice, allowing cross-learning. Considering the conceptual framework presented earlier and learning from the experience of the current study, the evidence-based framework (Figure 8) has the ability to guide healthcare organizations in co-designing organization improvement and management capacity building strategies.
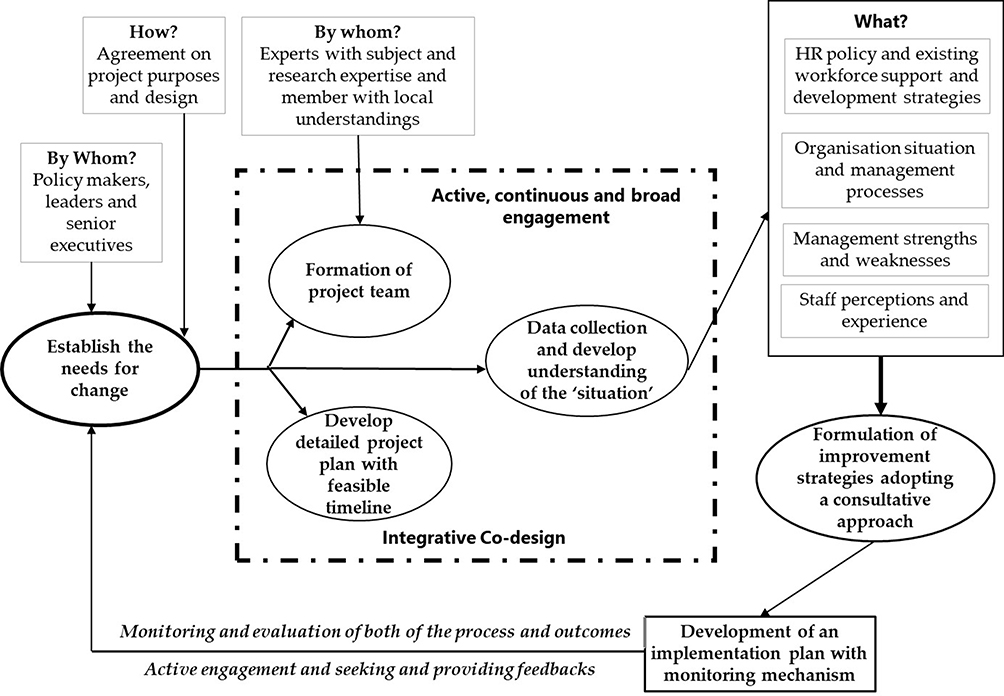 |
Figure 8 An integrative co-design framework for management capacity building in organizations. |
The framework begins by establishing the need for change to set the momentum of change and forming a project team with the required expertise which may include the engagement of experts in the field. Through an active and broad engagement and integrative co-design process, the team collects relevant data to develop an understanding of the organization’s policies, procedures, processes, strengths and weaknesses, and staff experience and perception. Improvement strategies are then developed with direct input from the organization’s decision-makers to ensure their relevance and feasibility of implementation. By continuously monitoring the implementation of strategies and outcomes, the extent to which strategies address needs and whether more actions are required can be determined. This cycle of change can continue if the needs have not been fully addressed.
Limitations
Although strategies have been implemented to mitigate bias, social desirability bias may have influenced self-reported competency levels and perceptions, particularly in the survey responses. Additionally, the study was conducted in only two hospitals within one single district, which may limit the generalizability of findings to other settings with different governance structures, organisational cultures, and health system configuration.
Practical Implications and Future Research
The project provides a replicable model for evidence-informed strategy formulation in hospital management capacity building. It demonstrates how engaging key stakeholders including clinical and non-clinical staff, managers, executives and health department officials in the co-design of improvement strategies can foster ownership, improve data quality, and catalyze organisational change. The high level of participation across both hospitals suggests that embedding change management principles can significantly improve the effectiveness of workforce development initiatives. These insights are applicable to other health systems, particularly those operating in resource-constrained or centralized settings, seeking to strengthen management capacity. Future research should expand the application of the co-design framework to diverse health service contexts, including rural and remote settings, to test scalability and adaptability.
Conclusion
This study reported an integrative and co-design process implemented in formulating strategies for developing the management capacity of two hospitals in a health district, a process that actively engaging policy makers, managers, and staff across hospitals and various research data collection stages. By explaining the associating actions and outcomes of each of the implementation stages and the presentation of selected results, this study confirms the important role that context plays in management functions, leadership behavior, and staff perceptions of their importance to the organization and level of support received. Learning from the integration of a co-design, active engagement, and mixed-method process, taking the organisational context into consideration, provides useful guidance for future health management research and capacity building projects. The integrative co-design framework created in this study provides step-by-step guidance for future evidence-based management capacity-building improvements in healthcare organizations.
Abbreviations
FGD, Focus Group Discussions; MCAP, Management Competency Assessment Partnership.
Ethical Approval and Consent to Participate
This study was approved by the Institutional Review Board of School of Public Health, Sun Yat-Sen University (No. 202370). All participants provided their consent to the participation of the study prior to the data collection process.
Acknowledgments
We would like to thank the National Natural Science Foundation of China and the Guangdong Basic and Applied Basic Research Foundation for their funding support of the project and all participants who contributed to the study. We would also like to thank and acknowledge the contribute to the project made by the following Higher Degree Research students: Zhilang Feng, Xuezhu Li.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Consent for Publication
The authors received consent from study participants in publishing the results in journals.
Funding
This project was supported by the National Natural Science Foundation of China (Grant No. 72274225) and the Guangdong Basic and Applied Basic Research Foundation (Grant No. 2023A1515011725).
Disclosure
The authors declare no potential conflicts of interest with respect to the research, authorship, or publication of this article.
References
1. Hailey VH, Balogun J. Devising context sensitive approaches to change: the example of Glaxo Wellcome. Long Range Plann. 2002;35(2):153–78
2. Kaplan HC, Brady PW, Dritz MC, et al. The influence of context on quality improvement success in health care: a systematic review of the literature. MilbankQ. 2010;88(4):500–59. doi:10.1111/j.1468-0009.2010.00611.x
3. McCormack B, Kitson A, Harvey G, Rycroft‐Malone J, Titchen A, Seers K. Getting evidence into practice: the meaning of ‘context’. J Adv Nurs. 2002;38(1):94–104.
4. Nilsen P, Bernhardsson S. Context matters in implementation science: a scoping review of determinant frameworks that describe contextual determinants for implementation outcomes. BMC Health Serv Res. 2019;19(189). doi:10.1186/s12913-019-4015-3
5. Williams B, Perillo S, Brown T. What are the factors of organisational culture in health care settings that act as barriers to the implementation of evidence-based practice? A scoping review. Nurs Educ Today. 2015;35(2):e34–e41. doi:10.1016/j.nedt.2014.11.012
6. Flemming K, Booth A, Garside R, Ö T, Noyes J. Qualitative evidence synthesis for complex interventions and guideline development: clarification of the purpose, designs and relevant methods. BMJ Glob Health. 2019;4(Suppl 1):e000882.
7. Biesta G, editor. Pragmatism and the Philosophical Foundations of Mixed Methods Research. California Sage Publications; 2010.
8. Creswell JW, Clark VLP. Designing and Conducting Mixed Methods Research.
9. Greenwood DJ, Levin M. Introduction to action research: social research for social change: Sage Publications; 2006. Available from https://books.google.com.au/books?id=PdtFBQAAQBAJ.
10. Patton MQ. Qualitative Research & Evaluation Methods: Integrating Theory and Practice. California: Sage Publications; 2002.
11. Breckenridge J, Jones D, Elliott I, Nicol M. Choosing a methodological path: reflections on the constructivist turn. Grounded Theory Review. 2012;11(1):64–71.
12. Charmaz K, editor. Grounded Theory as an Emergent Method. New York: Guildford Press; 2008.
13. Slattery P, Saeri AK, Bragge P. Research co-design in health: a rapid overview of reviews. Health Res Policy and Syst. 2020;18(17):1–13.
14. Haijes HA, Van Thiel GJMW. Participatory methods in pediatric participatory research: a systematic review. Pediat Res. 2016;79(5):676–83.’doi:10.1038/pr.2015.279.
15. Antonini M. An overview of co-design: advantages, challenges and perspectives of users’ involvement in the design process. J Des Think. 2021;2(1):45–60.’doi:10.22059/jdt.2020.272513.1018.
16. Bird M, McGillion M, Chambers E, et al. A generative co-design framework for healthcare innovation: development and application of an end-user engagement framework. Res Involv Engagem. 2021;7:1–12.
17. Salsberg J, Parry D, Pluye P, Macridis S, Herbert CP, Macaulay AC. Successful strategies to engage research partners for translating evidence into action in community health: a critical review. J Enivron Public Health. 2015;2015:191856. doi:10.1155/2015/191856
18. Blackwell RW, Lowton K, Robert G, Grudzen C, Grocott P. Using experience-based co-design with older patients, their families and staff to improve palliative care experiences in the emergency department: a reflective critique on the process and outcomes. Int J Nurs Stud. 2017;68:83–94. doi:10.1016/j.ijnurstu.2017.01.002
19. Pedersen J. War and peace in codesign. CoDesign. 2016;12(3):171–84.’doi.org/10.1016/j.ijnurstu.2017.01.002. doi:10.1080/15710882.2015.1112813
20. NSW Council of Social Services. The co-design principles. The Fair Deal Forum November 2016; Woolloomooloo, NSW. NSW Council of Social Services; Available from: https://www.ncoss.org.au/sites/default/files/public/resources/Codesign%20prinhttps://www.ncoss.org.au/wp-content/uploads/2017/06/Codesign-principles.pdff.
21. Greenhalgh T, Hinton L, Finlay T, et al. Frameworks for supporting patient and public involvement in research: systematic review and co‐design pilot. Health Expect. 2019;22(4):785–801.’doi:10.1111/hex.12888.
22. Mc Carthy VJ, Murphy A, Savage E, et al. Perceived importance and performance of clinical leadership in practice: a cross‐sectional study of nurses and midwives of all grades. J N Manag. 2019;27(8):1738–1746. doi:10.1111/jonm.12867
23. Ngabonzima A, Asingizwe D, Kouveliotis K. Influence of nurse and midwife managerial leadership styles on job satisfaction, intention to stay, and services provision in selected hospitals of Rwanda. BMC Nurs. 2020;19(35):1–11.
24. Almutairi H, Bahari G. A multisite survey of managerial competence and organizational commitment among nurses working at public hospitals in Saudi Arabia. J N Manag. 2022;30(1):179–186.
25. Vainieri M, Ferrè F, Giacomelli G, Nuti S. Explaining performance in health care: how and when top management competencies make the difference. Health Care Manage Rev. 2019;44(4):306–317. doi:10.1097/HMR.0000000000000164
26. Van Bogaert P, Clarke S, Wouters K, Franck E, Willems R, Mondelaers M. Impacts of unit-level nurse practice environment, workload and burnout on nurse-reported outcomes in psychiatric hospitals: a multilevel modelling approach. Int J Nurs Stud Adv. 2013;50(3):357.
27. Kakemam E, Liang Z. Guidance for management competency identification and development in the health context: a systematic scoping review. BMC Health Serv Res. 2023;23(1):421. doi:10.1186/s12913-023-09404-9
28. Becker WS. Starting new team operations: lessons from greenfield managers. Team Perform Manag in J. 2013;19(1/2):72–86. doi:10.1108/13527591311312105
29. Kendrick M, Kendrick K, Morton P, Taylor NF, Leggat SG. Hospital staff report it is not burnout, but a normal stress reaction to an uncongenial work environment: findings from a qualitative study. Int J Environ Res Public Health. 2020;17(11):4107. doi:10.3390/ijerph17114107
30. Nagle C, Omonaiye O, Bennett PN. Valuing nurse and midwifery unit managers’ voices: a qualitative approach. BMC Nurs. 2021;20(160):1–9.
31. Liang Z, Howard P, Wang J, Xu M. A call for leadership and management competency development for directors of medical services—evidence from the Chinese public hospital system. Int J Environ Res Public Health. 2020;17(18):6913. doi:10.3390/ijerph17186913
32. Liang Z, Howard P, Wang J, Xu M, Zhao M. Developing senior hospital managers: does ‘one size fit all’? – evidence from the evolving Chinese health system. BMC Health Serv Res. 2020;20(1):149–163. doi:10.1186/s12913-020-05116-6
33. Chambers DA, Norton WE. The Adaptome: advancing the science of intervention adaptation. Am J Prev Med. 2016;51(4):S124–S31. doi:10.1016/j.amepre.2016.05.011
34. Shelton RC, Cooper BR, Stirman SW. The sustainability of evidence-based interventions and practices in public health and health care. Annu Rev Public Health. 2018;39:55–76.
35. Liang Z, Howard PF, Leggat S, Bartram T. Development and validation of health service management competencies. J Health Organ Manag. 2018;32(2):157–175. doi:10.1108/JHOM-06-2017-0120
36. Howard PF, Liang Z, Leggat S, Karimi L. Validation of a management competency assessment tool for health service managers. J Health Organ Manag. 2018;32(1):113–134. doi:10.1108/JHOM-08-2017-0223
37. Spreitzer GM. Psychological empowerment in the workplace: dimensions, measurement, and validation. Academy Manag J. 1995;38(5):1442–1465. doi:10.2307/256865
38. Zachariae R, O’Connor M, Lassesen B, et al. The self-efficacy in patient-centeredness questionnaire–a new measure of medical student and physician confidence in exhibiting patient-centered behaviors. BMC Med Educ. 2015;15(150):1–13. doi:10.1186/s12909-015-0427-x
39. Bartram T, Karimi L, Leggat SG, Stanton P. Social identification: linking high performance work systems, psychological empowerment and patient care. Int J Human Res Manag. 2014;25(17):2401–19. doi:10.1080/09585192.2014.880152.
40. Epstein RM, Hundert EM. Defining and assessing professional competence. J American Med. 2002;287(2):226–235.
41. Creswell JW, Poth CN. Qualitative Inquiry and Research Design: Choosing Among Five Approaches. California: Sage Publications; 2016.
42. Canadian Institutes of Health Research. Canada’s strategy for patient oriented research: improving health outcomes through evidence-informed care. Ottawa, Canada: Canadian Institutes of Health Research; 2011. Available from https://cihr-irsc.gc.ca/e/44000.html.
43. Aithal A, Aithal P. Development and validation of survey questionnaire & experimental data–a systematical review-based statistical approach. Int J Manag Technol Soc Sci. 2020;5(2):233–51. doi:10.5281/zenodo.4179499.
44. Taherdoost H. Validity and reliability of the research instrument: how to test the validation of a questionnaire/survey in a research. Int J Acad Res Manag. 2016;5(3):28–36. doi:10.2139/ssrn.3205040.
45. Baumgartner RJ, Rauter R. Strategic perspectives of corporate sustainability management to develop a sustainable organization. J Clean Prod. 2017;140(1):81–92. doi:10.1016/j.jclepro.2016.04.146
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.