Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Admissions Due to Perinatal Respiratory and Cardiovascular Disorders in England
Authors Naser AY ![]() , Al-shehri H
, Al-shehri H ![]()
Received 6 November 2022
Accepted for publication 17 January 2023
Published 22 January 2023 Volume 2023:16 Pages 199—207
DOI https://doi.org/10.2147/JMDH.S396406
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Abdallah Y Naser,1 Hassan Al-shehri2
1Department of Applied Pharmaceutical Sciences and Clinical Pharmacy, Faculty of Pharmacy, Isra University, Amman, Jordan; 2Department of Pediatrics, College of Medicine, Imam Mohammad Ibn Saud Islamic University, Riyadh, Saudi Arabia
Correspondence: Abdallah Y Naser, Department of Applied Pharmaceutical Sciences and Clinical Pharmacy, Faculty of Pharmacy, Isra University, Amman, Jordan, Tel +962795285555, Email [email protected]
Objective: The aim of this study was to look into the rates of perinatal admissions for respiratory, cardiac, and cardiovascular diseases in England.
Methods: This ecological study was conducted in England. The Hospital Episode Statistics (HES) database in England provided the study with the publicly accessible data. The data set for this study was considered between April 01, 2012 and April 01, 2020. The HES database contains information on patients’ admissions to hospitals, notably for those hospitalised with perinatal cardiovascular and respiratory diseases. We used the chi-squared test to assess the difference between the hospital admission rates between 2012 and 2020.
Results: An increase of 15.6% was observed in hospital admissions rate during the study period [from 10,940.37 (95% CI 10,865.99– 11,014.75) in 2012 to 12,649.00 (95% CI 12,565.03– 12,732.98) in 2020 per 100,000 people, p< 0.05]. Intrauterine hypoxia, chest congestion and breathing-related respiratory distress of newborns, and other perinatal respiratory disorders accounted for 35.5%, 29.8%, and 21.3%, respectively. Males contributed for more than half of them (56.7%). The rate of hospital admission among males increased by 15.1% [from 12,227.79 (95% CI 12,118.83– 12,336.74) in 2012 to 14,074.77 (95% CI 13,952.11– 14,197.43) in 2020 per 100,000 persons, p< 0.05]. The rate of hospital admission among females increased by 17.4% [from 9,646.15 (95% CI 9,545.31– 9,747.00) in 2012 to 11,324.20 (95% CI 11,209.47– 11,438.92) in 2020 per 100,000 persons, p< 0.05].
Conclusion: The study’s findings show that the most common causes of hospital admissions for respiratory and cardiovascular disorders were intrauterine hypoxia, neonatal respiratory distress, and other perinatal respiratory issues, which were detected particularly during the perinatal period. Further research is warranted to identify risk factors of hospital admissions for respiratory and cardiovascular disorders during the perinatal period.
Keywords: admission, cardiovascular disorders, perinatal, respiratory
Introduction
In 2019, 2.4 million new-borns died in their first month of life worldwide.1 Although the frequency of deaths during this period has decreased, complications during pregnancy and delivery remain a major concern, with 75% of new-born deaths occurring during the first week of life. Congenital heart disease can be regarded a primary cause of cardiac emergencies in young children and infants,2 and acquired heart disease becomes increasingly common in infancy and early childhood.3
The neonatal phase, which includes the perinatal period, is regarded as the most critical time after delivery. It is a time of rapid change and development during which infancy behaviours such as eating and bonding are developed. This was often thought to be the most dangerous phase since there is a high likelihood of post-delivery complications or the discovery of birth defects or congenital disorders. In a recent study of 100 infants born at 23 weeks, 60 died before being discharged from the hospital, with respiratory failure being the most common cause.4 There is a growing trend to start resuscitation and therapy at a younger gestational age; nevertheless, this unexpected consequence is an increase in the proportion of children with long-term respiratory and/or neurological impairment.5 Chronic respiratory disorders are the most common reasons for new-born infants being admitted to the neonatal intensive care unit (NICU).6 Despite advances in the NICU, chronic respiratory diseases continue to be a major source of morbidity and mortality in neonates.6
CVDs affect 7.6 million people in the United Kingdom (UK) and are a leading cause of death and disability.7,8 In England, respiratory disorders impact one in every five people and are the third biggest cause of death after cancer and cardiovascular disease. Furthermore, the trend in hospital admissions for respiratory disorders in England has tripled in the last 7 years.9 In 2019, more than half of all new-borns in England died as a result of immaturity-related conditions, with the majority of patients (53.1%) suffering from respiratory and cardiovascular problems.10
Previous epidemiological research in the United Kingdom focused on a variety of acute and chronic health outcomes.11–25 To the best of our knowledge, no previous research in England in the last two decades have investigated the respiratory and cardiovascular disorders of the new-borns during the neonatal-perinatal period. Understanding the prevalence of respiratory and cardiovascular disorders admissions, particularly during perinatal period, and the underlying causes is critical for researchers and policymakers, as England has set a goal of reducing stillbirth and new-borns mortality rates by 2025 compared to 2010. As a result, the purpose of this study was to investigate the rates of perinatal hospital admissions for respiratory and cardiovascular diseases in England.
Methods
Study Design
This was a retrospective ecological study that utilized publically available data on the population level. For the current study, we used data from the Hospital Episode Statistics (HES) database in England for the period between April 01, 2012 and April 01, 2020.26 Data prior to 2012 are not specific to the new-born age group, but are reported for the age group under 14 years collectively. The HES database comprises data from patients who were admitted to the hospital with respiratory and cardiovascular diseases especially in the perinatal period. We identified respiratory and cardiovascular disorders specific to the perinatal period-related hospital admissions using the Tenth Revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) 5th Edition (used by National Health Service (NHS) to classify diseases and other health conditions).
Data Extraction
All diagnostic codes for respiratory and cardiovascular disorders specific to the perinatal period (P20 – P29; P20: intrauterine hypoxia, P21: birth asphyxia, P22: respiratory distress of newborn, P23: congenital pneumonia, P24: neonatal aspiration syndromes, P25: interstitial emphysema and related conditions originating in the perinatal period, P26: pulmonary haemorrhage originating in the perinatal period, P27: chronic respiratory disease originating in the perinatal period, P28: other respiratory conditions originating in the perinatal period, and P29: cardiovascular disorders originating in the perinatal period) were used. The Office for National Statistics (ONS) database was used to obtain mid-year population data (2012–2020) in order to assess the yearly admission trend for disorders connected to cardiovascular and respiratory disease.
Statistical Analysis
Descriptive statistics were used present categorical data as frequency and percentage. The number of respiratory and cardiovascular diseases (nominator) unique to the perinatal period-related hospitalization divided by the mid-year population (denominator) was used for this research to determine hospital admission rates with 95% confidence intervals (CIs). Similar procedure was used to estimate the admission rates stratified per gender and age group. Confidence interval was estimated using the following equation for the population proportion: p^ +/− z* (p^(1 − p^)/n)0.5. We used the chi-squared test to assess the difference between the hospital admission rates between 2012 and 2020. All analyses were conducted using SPSS version 27 (IBM Corp, Armonk, NY, USA).
Results
The total annual number for respiratory and cardiovascular disorders specific to the perinatal period hospital admissions for different causes increased by 2.9% from 74,015 in 2012 to 76,136 in 2020, representing an increase in hospital admission rate of 15.6% [from 10,940.37 (95% CI 10,865.99–11,014.75) in 2012 to 12,649.00 (95% CI 12,565.03–12,732.98) in 2020 per 100,000 persons, p<0.05] (Figure 1).
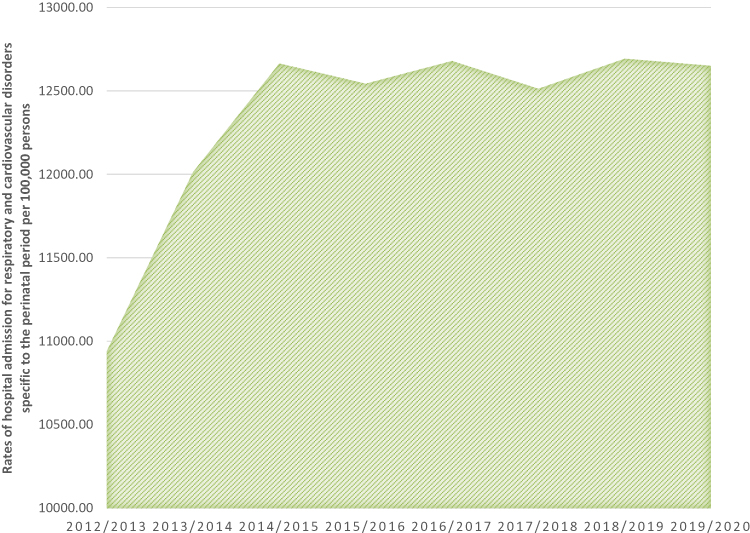 |
Figure 1 Total rates of hospital admission for respiratory and cardiovascular disorders specific to the perinatal period in England. |
The total number of admissions during the study period was 642,320 episodes. Males contributed for more than half of them (56.7%). The rate of hospital admission among males increased by 15.1% [from 12,227.79 (95% CI 12,118.83–12,336.74) in 2012 to 14,074.77 (95% CI 13,952.11–14,197.43) in 2020 per 100,000 persons, p<0.05]. The rate of hospital admission among females increased by 17.4% [from 9646.15 (95% CI 9545.31–9747.00) in 2012 to 11,24.20 (95% CI 11,209.47–11,438.92) in 2020 per 100,000 persons, p<0.05], Figure 2.
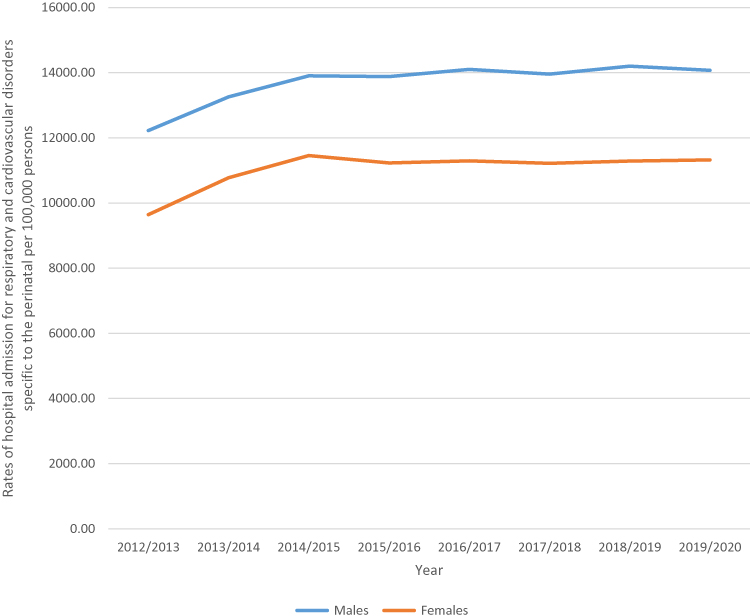 |
Figure 2 Rate of admissions stratified by gender. |
The most prevalent respiratory and cardiovascular disorders specific to the perinatal period hospital admissions causes were intrauterine hypoxia, respiratory distress of newborn, and other respiratory conditions originating in the perinatal period, which accounted for 35.5%, 29.8%, and 21.3%, respectively (Figure 3).
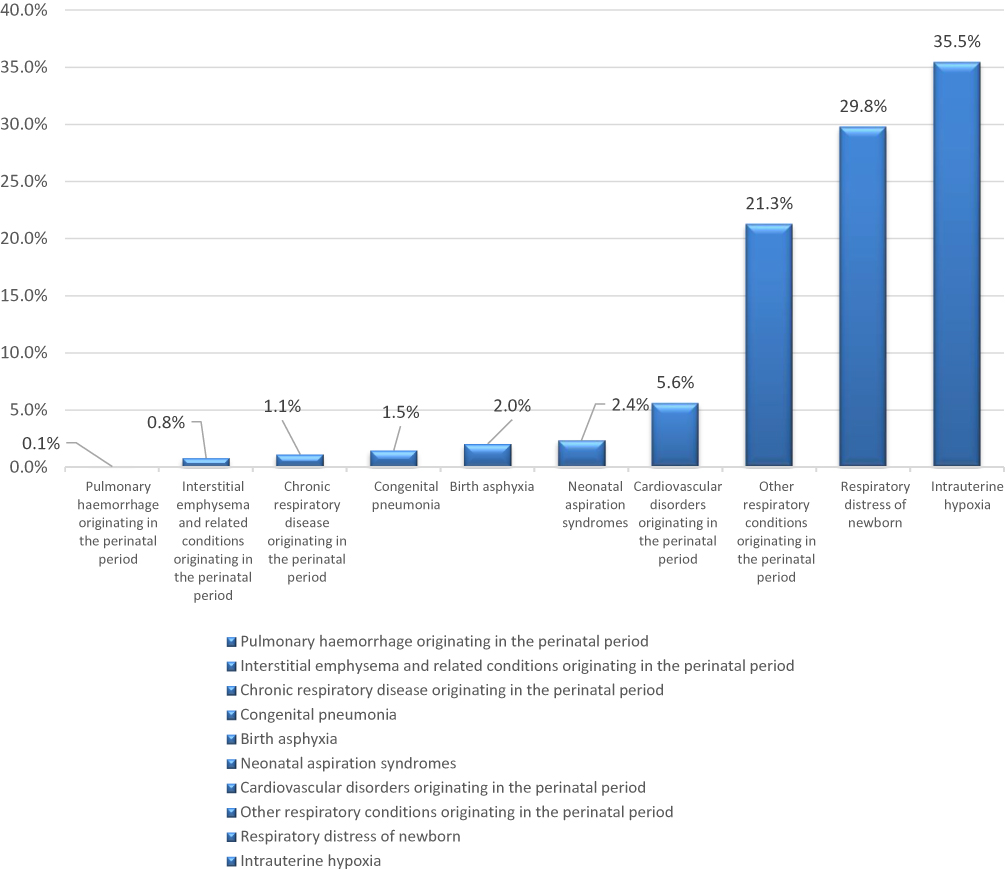 |
Figure 3 Percentage of respiratory and cardiovascular disorders specific to the perinatal period hospital admission from total number of admissions. |
Throughout the past eight years, a tremendous increase in respiratory and cardiovascular disorders specific to the perinatal period hospital admissions rate was seen in respiratory distress of newborn, chronic respiratory disease originating in the perinatal period, and pulmonary haemorrhage originating in the perinatal period with 53.2%, 36.2%, and 31.8%, respectively. However, respiratory and cardiovascular disorders specific to the perinatal period hospital admissions rate for birth asphyxia, neonatal aspiration syndromes, and intrauterine hypoxia were decreased by 60.3%, 25.0%, and 2.6%, respectively (Table 1, Figure 4).
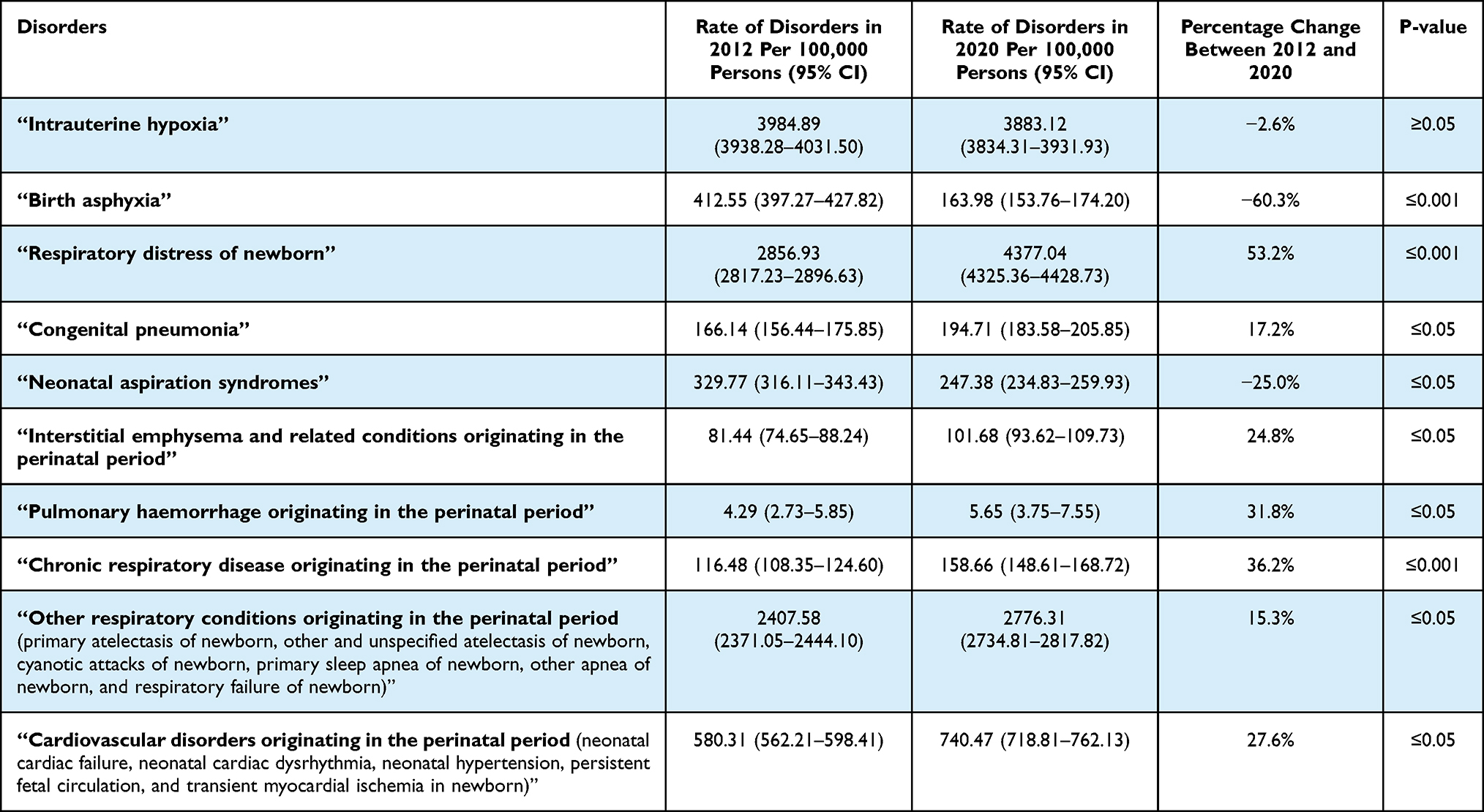 |
Table 1 Percentage Change in the Hospital Admission Rates for Respiratory and Cardiovascular Disorders Specific to the Perinatal Period Between 2012 and 2020 in England |
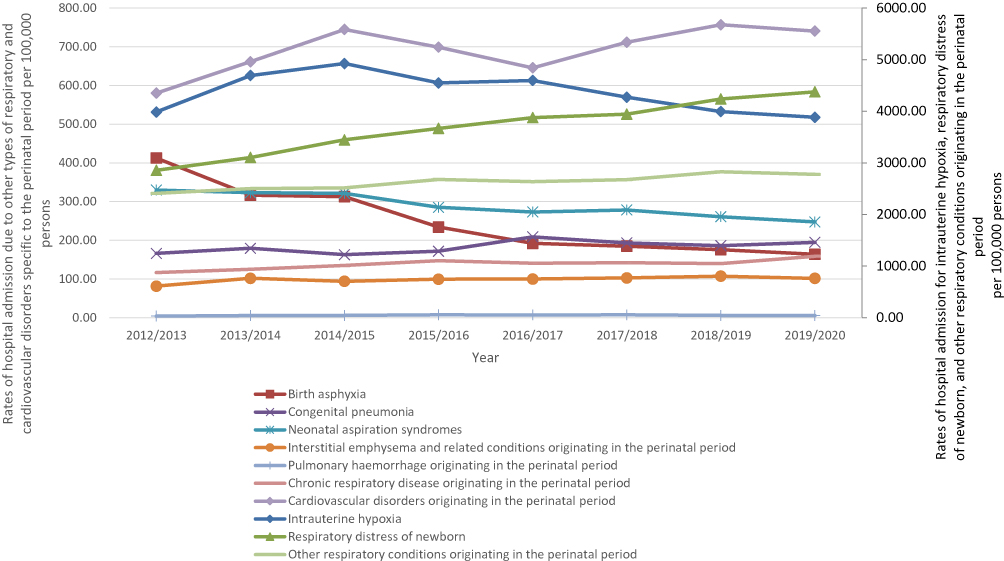 |
Figure 4 Rates of hospital admission for respiratory and cardiovascular disorders specific to the perinatal period in England stratified by type between 2012 and 2020. |
Discussion
Despite that over the past 30 years England has made significant progress in the healthcare sector, improvements in mortality rates in England have slowed in the last decade.9 Since 2014, the proportion of new-born deaths among babies born at less than 24 weeks of gestation has increased. Things to be considered, that since 2014, immaturity-related disorders or respiratory infections have been the leading cause of new-born mortality in England.9 Different reports on the health profile for England also indicate that, early detection is critical. Primary and secondary prevention, as well as promoting public health awareness, remain essential avenues for reducing the burden of risk factors and maximizing the adoption of recognized effective care in the prevention of both cardiovascular disease and prenatal respiratory disease. The goal of this study was to examine the epidemiology of hospital admissions in England due to perinatal respiratory and cardiovascular problems. The key findings of this study are: 1) during the last eight years, perinatal admission rate due to respiratory and cardiovascular disease increased, 2) intrauterine hypoxia, respiratory asphyxia of newborn, and other respiratory conditions emerged during perinatal period were the most common causes of hospital admissions “related to respiratory and cardiovascular disorders” during the perinatal period, 3) the most noticeable rise in admission rates was owing to infant respiratory distress, chronic respiratory illness arising during the perinatal stage, and perinatal pulmonary haemorrhage, and 4) admission rates were higher among males compared to females during the study period.
In our study, during the last eight years, perinatal admission rate due to respiratory and cardiovascular disease increased by 15.6%. There are several reasons that are considered for the increasing trend of hospitalisation of new-born infant as they suffered for respiratory and cardiovascular disorders. These include delayed or maladaptive adaptation to extra-uterine life, pre-existing illnesses such as surgical or congenital defects, or acquired conditions like as lung infections that occur either before or after delivery. According to a previous Italian study, 2.2% of all deliveries were complicated by a respiratory illness.27 Another study in India estimated that the rate of complications could reach 6.7%.28 According to one study, respiratory issues were the predominant reason for admission in 33.3% of all neonatal admissions at >28 weeks’ gestation, excluding children with syndromes and those with congenital or surgical disorders.29 A subsequent study reported that 20.5% of all new-born admission showed symptoms of infection.30 Respiratory problems are the most common reason for neonatal unit admission in both term and preterm new-borns.31 There are various theories as to why new-born infants are increasingly being hospitalized due to the disease like cardiovascular and respiratory issues. For example, sometimes maladaptive adaptation of the infant right after birth to extra-uterine life is the main cause found as significant element. Also, another reason mostly found is the surgical complicacy that may came from a pre-existing illness, or acquired ailments such as lung infections that arise before or after delivery.
Some research evidence also exists of increasing rates of perinatal admissions where the possible reason is found as respiratory conditions that might be an impact of maternal smoking.32 Researchers found smoking of pregnant mother can lead to the respiratory and cardiovascular disorder of new born during perinatal period. According to the Centers for Disease Control and Prevention (CDC), “maternal smoking during pregnancy” (MSDP) is a severe public health danger, affecting approximately half of all pregnant smokers.33 As a result, each year, pregnant women who are used to smoke during their pregnancy, infect almost more than 500,000 infants20 Smith, Martin, and Ventura (1999; CDC, 2004). Women those who are used to smoke during their period of pregnancy have children with altered cardiorespiratory responses,34 as well as increased asthma and wheezing.34–38 The new research from Seattle Children’s Hospital adds to the growing body of data that smoking during pregnancy can harm a baby’s heart and increase the chance of miscarriage, small new-borns, and early birth. In England, approximately 13% of pregnant women smoke. According to the same study, smoking during pregnancy could cause 1% to 2% of all heart-related diseases in new-borns.
Our research also found that most infants were admitted to the hospital due to intrauterine hypoxia, new born respiratory distress, and other perinatal respiratory disorders, accounting for 35.5%, 29.8%, and 21.3%, respectively. Furthermore, with 53.2%, 36.2%, and 31.8%, respectively, the most notable increase in respiratory and cardiovascular disorders specific to the perinatal period hospital admissions rate was seen in respiratory distress of new born, chronic respiratory disease originating in the perinatal period, and pulmonary haemorrhage originating in the perinatal period. It is a well-known fact that, fetal growth and perinatal survival are all dependent on good maternal health and appropriate placental development. Maternal exposure to a consistently hypoxic environment may result in significant organ damage. When the placenta does not function normally, it has acute and chronic impacts on the development of the fetus. As a result, it causes a variety of conditions. When the organism is deprived of oxygen, conditions such as IUGR, Intrauterine Growth Restriction, and Asphyxia occur, resulting in either unconsciousness or death. It may aggravate the disease by causing multi-organ failure, preterm labour, and perinatal death.
Hospital admissions due to birth asphyxia, new-born aspiration syndromes, and intrauterine hypoxia reduced by 60.3%, 25.0%, and 2.6%, respectively, according to our study findings. This could be linked to improvements in medical practitioners’ diagnostic abilities, allowing them to recognize certain specific anomalies early on and treat them appropriately, allowing for preterm delivery (during these periods of our research). Another reason could be that several medical science research advancements, notably on congenital heart diseases (CHD), have had a significant impact on improving the survival rate of affected patients over time.39 Many improved diagnostic procedures such as
Magnetic Resonance Imaging (MRI), genetic testing, Molecular testing of the chorionic villus sample (CVS) or aminocytes, fetal blood sample, a direct biopsy of fetal tissue, and Non-invasive prenatal diagnosis (NIPD) have also contributed to the early detection of congenital anomalies during the perinatal period. (earlier than 20 weeks of pregnancy and during the first trimester)40,41
The preceding steps play an important role in supporting early decision-making for potentially life-saving procedures. As a result, doctors have the option of terminating the pregnancy early, lowering the likelihood of delivering new-borns with hypoxia and its accompanying difficulties, as well as hospitalization.
There are certain limitations to this research. To our knowledge, our study is of a novel one to look into the epidemiology of hospital admissions in England due to perinatal respiratory and cardiovascular problems. It is difficult to demonstrate any form of causality between the variables because this is an ecological study and the database is only available at the population level. In addition, the researcher was unable to obtain sufficient information on other associated variables such as gender, age, and educational level, for example. We were unable to investigate the connection between maternal age and perinatal respiratory and cardiovascular disorders-related hospital admissions.
Conclusion
The finding of the study showed that over the research period, the epidemiology of hospitalization for prenatal respiratory and cardiovascular disorders in England has increased. The most common causes of hospital admissions related to respiratory and cardiovascular disorders specific to the perinatal period were intrauterine hypoxia, respiratory distress of newborn, and other respiratory conditions originating in the perinatal period. However, more research employing follow-up is required to investigate potential risk factors for respiratory and cardiovascular disease during the perinatal period.
Data Sharing Statement
Publicly available datasets were analyzed in this study. This data can be found here: http://http//content.digital.nhs.uk/hes.
Ethical Approval
The study was approved by the Institutional Review Board at Isra University, Amman, Jordan gave their clearance with IRB No. SREC/22/08/48. This study was conducted in accordance with the World Medical Association (WMA) Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study has not received any external funding.
Disclosure
The authors declare that there are no conflicts of interests.
References
1. World Health Organization. Newborns: improving survival and well-being; 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/newborns-reducing-mortality.
2. Alanazi AFR, Naser AY, Pakan P, et al. Trends of hospital admissions due to congenital anomalies in England and Wales between 1999 and 2019: an Ecological Study. Int J Environ Res Public Health. 2021;18(22):11808. doi:10.3390/ijerph182211808
3. Kabbani N, Kabbani MS, Al Taweel H. Cardiac emergencies in neonates and young infants. Avicenna J Med. 2017;7(1):1–6. doi:10.4103/2231-0770.197506
4. Greenough A. Long-term respiratory consequences of premature birth at less than 32 weeks of gestation. Early Hum Dev. 2013;89(2):S25–S27. doi:10.1016/j.earlhumdev.2013.07.004
5. Hillman N, Lam H. Respiratory Disorders in the newborn. In: Kendig’s Disorders of the Respiratory Tract in Children.
6. British Heart Foundation. UK factsheet. 2022; Available from: https://www.bhf.org.uk/-/media/files/research/heart-statistics/bhf-cvd-statistics-uk-factsheet.pdf?la=en.
7. England National Health Services. Cardiovascular disease (CVD); 2019. Available from: https://www.england.nhs.uk/ourwork/clinical-policy/cvd/.
8. England National Health Services. Respiratory disease; 2019. Available from: https://www.england.nhs.uk/ourwork/clinical-policy/respiratory-disease/.
9. Office for National Statistics. Child and infant mortality in England and Wales; 2022. Available from: https://cy.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/childhoodinfantandperinatalmortalityinenglandandwales/2020#:~:text=Trends%20in%20child%20and%20infant%20mortality%20There%20were,100%2C000%20population%20of%20the%20same%20age%20in%201981.
10. Al-Daghastani T, Naser AY. Hospital admission profile related to poisoning by, adverse effect of and underdosing of psychotropic drugs in England and Wales: an ecological study. Saudi Pharm J. 2022;30(9):1262–1272. doi:10.1016/j.jsps.2022.06.025
11. Alrawashdeh HM, Naser A, Alwafi H, et al. Trends in hospital admission due to diseases of the eye and adnexa in the past two decades in England and Wales: an Ecological Study. Int J Gen Med. 2022;15:1097–1110. doi:10.2147/IJGM.S344380
12. Al-shehri H, Dahmash DT, Rochow N, et al. Hospital admission profile of neonates for conditions originating in the perinatal period in England and Wales Between 1999‒2020: an Ecological Study. Int J Gen Med. 2022;15:1973–1984. doi:10.2147/IJGM.S354847
13. Hemmo SI, Naser AY, Alwafi H, et al. Hospital admissions due to ischemic heart diseases and prescriptions of cardiovascular diseases medications in England and Wales in the past two decades. Int J Environ Res Public Health. 2021;18(13):7041. doi:10.3390/ijerph18137041
14. Mustafa Ali M, Naser AY, AbuAlhommos A, et al. Hospital admissions secondary to diseases of the blood, blood-forming organs, and immune system in England and Wales. Cureus. 2022. doi:10.7759/cureus.30179
15. Naser AY, Alrawashdeh HM, Alwafi H, et al. Hospital admission trends due to viral infections characterised by skin and mucous membrane lesions in the past two decades in England and Wales: an Ecological Study. Int J Environ Res Public Health. 2021;18(21):11649. doi:10.3390/ijerph182111649
16. Naser AY, Alwafi H, Al-Daghastani T, et al. Drugs utilization profile in England and Wales in the past 15 years: a secular trend analysis. BMC Prim Care. 2022;23(1):239. doi:10.1186/s12875-022-01853-1
17. Naser AY, Alwafi H, Hemmo SI, et al. Trends in hospital admissions due to neoplasms in England and Wales between 1999 and 2019: an Ecological Study. Int J Environ Res Public Health. 2022;19(13):8054. doi:10.3390/ijerph19138054
18. Naser AY, Dahmash EZ, Al-Daghastani T, et al. An ecological analysis of hospitalization patterns for diseases of the nervous system in England and Wales over the last 20 years. Healthcare. 2022;10(9):1670. doi:10.3390/healthcare10091670
19. Naser AY, Dahmash EZ, Alqahtani JS, et al. Trends in hospital admissions for mental, behavioural and neurodevelopmental disorders in England and Wales between 1999 and 2019: an Ecological Study. Healthcare. 2022;10(11):2191. doi:10.3390/healthcare10112191
20. Naser AY, Mansour MM, Alanazi AFR, et al. Hospital admission trends due to respiratory diseases in England and Wales between 1999 and 2019: an ecologic study. BMC Pulm Med. 2021;21(1):356. doi:10.1186/s12890-021-01736-8
21. Naser AY, Wang Q, Wong LYL, et al. Hospital admissions due to dysglycaemia and prescriptions of antidiabetic medications in England and Wales: an Ecological Study. Diabetes Ther. 2018;9(1):153–163. doi:10.1007/s13300-017-0349-1
22. Sweiss K, Naser AY, Alrawashdeh HM, et al. Hospital admissions due to vasomotor and allergic rhinitis in England and Wales between 1999 and 2019: an ecological study. Ir J Med Sci. 2022. doi:10.1007/s11845-022-02996-x
23. Sweiss K, Naser AY, Samannodi M, et al. Hospital admissions due to infectious and parasitic diseases in England and Wales between 1999 and 2019: an ecological study. BMC Infect Dis. 2022;22(1):398. doi:10.1186/s12879-022-07388-1
24. Mustafa Ali S, Naser AY, Alghanemi AG, et al. Musculoskeletal system and connective tissue related hospital admission in England and Wales between 1999 and 2019: an Ecologic Study. Cureus. 2022. doi:10.7759/cureus.32453
25. Naser AY, Al-Shehri H, Altamimi N, et al. Profile of hospital admissions due to preterm labor and delivery in England. Healthcare. 2023;11(2):163. doi:10.3390/healthcare11020163
26. Health and Social Care Information Centre (HSCIC). Hospital episode statistics; 2021. Available from: http://content.digital.nhs.uk/hes.
27. Rubaltelli FF, Dani C, Reali MF, et al. Acute neonatal respiratory distress in Italy: a one-year prospective study. Italian Group of Neonatal Pneumology. Acta paediatrica. 1992;87(12):1261–1268. doi:10.1111/j.1651-2227.1998.tb00949.x
28. Kumar A, Bhat BV. Epidemiology of respiratory distress of newborns. Indian J Pediatr. 1996;63(1):93–98. doi:10.1007/BF02823875
29. Parkash A, Haider N, Khoso ZA, Shaikh AS. Frequency, causes and outcome of neonates with respiratory distress admitted to neonatal intensive care unit, National Institute of Child Health, Karachi. JPMA. 2015;65(7):771–775.
30. Qian LL, Liu CQ, Guo YX, et al.; Chinese Collaborative Study Group for Neonatal Respiratory Diseases (2010). Current status of neonatal acute respiratory disorders: a one-year prospective survey from a Chinese neonatal network. Chin Med J. 2010;123(20):2769–2775.
31. Pramanik AK, Rangaswamy N, Gates T. Neonatal respiratory distress: a practical approach to its diagnosis and management. Pediatr Clin North Am. 2015;62(2):453–469. doi:10.1016/j.pcl.2014.11.008
32. Centers for Disease Control (CDC). Smoking during pregnancy - United States, 1990–2002. MMWR Morb Mortal Wkly Rep. 2004;53(39):911–915.
33. Centers for Disease Control and Prevention (CDC). Annual smoking-attributable mortality, years of potential life lost, and economic costs--United States, 1995–1999. MMWR Morb Mortal Wkly Rep. 2022;51(14):300–303.
34. Cnattingius S. The epidemiology of smoking during pregnancy: smoking prevalence, maternal characteristics, and pregnancy outcomes. Nicotine Tob Res. 2004;6(2):125–140. doi:10.1080/14622200410001669187
35. Huang ZG, Griffioen KJ, Wang X, et al. Differential control of central cardiorespiratory interactions by hypercapnia and the effect of prenatal nicotine. J Neurosci. 2006;26(1):21–29. doi:10.1523/JNEUROSCI.4221-05.2006
36. Ebrahim SH, Floyd RL, Merritt RK, Decoufle P, Holtzman D. Trends in pregnancy-related smoking rates in the United States, 1987–1996. JAMA. 2000;283(3):361–366. doi:10.1001/jama.283.3.361
37. Janson C. The effect of passive smoking on respiratory health in children and adults. Int J Tuberc Lung Dis. 2004;8(5):510–516.
38. Stocks J, Dezateux C. The effect of parental smoking on lung function and development during infancy. Respirology. 2003;8(3):266–285. doi:10.1046/j.1440-1843.2003.00478.x
39. Smith BL, Martin JA, Ventura SJ. Births and deaths: preliminary data for July 1997-June 1998. Natl Vital Stat Rep. 1999;47(22):1–32.
40. AbdulAzeez S, Al Qahtani NH, Almandil NB, et al. Genetic disorder prenatal diagnosis and pregnancy termination practices among high consanguinity population, Saudi Arabia. Sci Rep. 2019;9(1):1–8. doi:10.1038/s41598-019-53655-8
41. Hamilton MJE, Eason J. Prenatal diagnosis of genetic disorders. Obstet Gynaecol Reprod Med. 2015;25(p):307–313. doi:10.1016/j.ogrm.2015.08.005
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.