Back to Journals » Journal of Inflammation Research » Volume 15
Adherence to the Mediterranean Diet Improved Clinical Scores and Inflammatory Markers in Children with Active Inflammatory Bowel Disease: A Randomized Trial
Authors El Amrousy D, Elashry H, Salamah A, Maher S, Abd-Elsalam SM, Hasan S
Received 23 November 2021
Accepted for publication 9 February 2022
Published 29 March 2022 Volume 2022:15 Pages 2075—2086
DOI https://doi.org/10.2147/JIR.S349502
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Doaa El Amrousy,1 Heba Elashry,2 Abeer Salamah,3 Sara Maher,4 Sherief M Abd-Elsalam,2 Samir Hasan1
1Pediatric Department, Faculty of Medicine, Tanta University, Tanta, Egypt; 2Tropical Medicine Department, Faculty of Medicine, Tanta University, Tanta, Egypt; 3Pediatric Department, Kafr Elsheikh University, Kafr Elsheikh, Egypt; 4Theodor Bilharz Research Institute, Cairo, Egypt
Correspondence: Sherief M Abd-Elsalam, Tropical Medicine Department, Faculty of Medicine, Tanta University, El-Giash Street, Tanta, 31527, Egypt, Tel +2-01147773440, Email [email protected]
Objective: The Mediterranean diet (MD) is a well-known style of diet that is full of antioxidants and may have anti-inflammatory effects. We evaluated the safety, tolerability, and effects of adherence to MD on disease activity and inflammatory markers in children and adolescents with active inflammatory bowel disease (IBD).
Methods: This prospective, randomized study included 100 IBD patients aged twelve to eighteen years with mild to moderate disease activity (PCDAI score 10– 45 or PUCAI 10– 64). The included patients were divided into two groups of 50 patients each. Group I (26 patients with active CD and 24 patients with active UC) received MD with good adherence over 12 weeks with a KIDMED 8-point score, and group II (28 patients with active CD and 22 patients with active UC) received their usual diet with a KIDMED score ≤ 7 points. Patients in both groups received treatment similar for IBD activity.
Results: Clinical remission was achieved in most of the patients after 12 weeks of treatment. Patients in the first group (adhering to an MD) showed a significant decrease in both clinical scores (PCDAI and PUCAI) and most inflammatory markers (CRP, calprotectin, TNF-α, IL17., IL 12 and IL13) compared to patients in their normal group, with earlier improvement in both PCDAI and CRP.
Conclusion: Adherence to the MD improves clinical scores and inflammatory markers in children and adolescents with mild-moderate active IBD.
Keywords: inflammatory bowel disease, Mediterranean diet, children, inflammatory markers, cytokines
Introduction
Inflammatory bowel diseases (IBD) are chronic, heterogeneous, relapsing inflammatory disorders of gastrointestinal system with multiple extra-intestinal manifestations, which severely affect growth and development and general health of children.1 In the last 50 years, the global incidence of IBD has increased, both in children and adults, and it is widely known that more than 35% of adults with IBD began experiencing symptoms before the age of 18.2
The actual pathophysiology of IBD is still unknown, but the most widely recognized ideas suggest that it is caused by a combination of a dysregulated immune system and numerous dietary and microbial variables in genetically-suited individuals.3
Exclusive enteral nutrition (EEN) has been widely accepted as first-line induction therapy around the world, with comparable efficacy to steroids but significantly fewer side effects and higher mucosal healing rates.4 Diet as a primary or adjunct therapy for IBD is not a conventional medical treatment for Crohn’s disease (CD) or ulcerative colitis (UC), with the exception of EEN. Patients with IBD regularly employ alternative and complementary therapy, including as diets, without medical supervision or guidance.5 Many diets have been reported to be beneficial, but more research is needed.6
The Mediterranean Diet (MD) is distinguished by a high proportion of vegetables, fruits, bread and other cereals, grains, beans, and nuts. It also includes virgin olive oil, moderate amounts of dairy products (essentially, cheese and yoghurt), moderate amounts of fish, moderate amounts of red meat, and wine in small amounts, usually as an aperitif. The significance of this dietary pattern stems from the fact that it is a well-balanced and diverse diet that contains the majority of the essential macronutrients in the proper proportions.7–9
New and promising data concerning the beneficial effect of MD on IBD have been reported in several adult studies but these studies are lacking in children with IBD. They reported clinical remission and mucosal healing with MD diet and attributed this effect to change in gut microbiota, lack of artificial additive, improved nutritional status, antioxidant and anti-inflammatory effects of MD components.10–15
The purpose of this randomized, parallel treatment design study is to assess the effects of MD on the clinical disease activity and biological inflammatory markers in children and adolescents with moderately active CD and UC.
Subjects and Methods
The purpose of this randomized, parallel treatment design study is to see how the MD pattern affects clinical disease activity and biological inflammatory markers in children and adolescents with moderately active CD and UC.
This prospective randomized case-controlled study was carried out at our tertiary care Tanta University Hospital, in Pediatric and Gastroenterology departments, between April 2020 and April 2021. One hundred consecutive IBD patients aged 12–18 years old were included. Patients subdivided into two groups (50 patients each), Group I received MD (KIDMED Score ≥ 8 points allover study period), and Group II on their regular diet (with KIDMED score ≤ 7 points allover study period). Pre-study period of one month for education and habituation of MD was done for group I. This study included patients with CD or UC who had mild or moderate disease activity, as measured by a PCDAI score of 10–45 or a PUCAI score of 10 to 60. Before the trial, no changes in IBD medication could be made for at least one month with immunosuppressive medicines and two months with biologics.
Assessment of Participants
All individuals were given a full history, physical examination, and laboratory testing, which included a complete blood count with differential count, CRP, ESR, albumin, serum levels of TNF-, IL17, IL10, IL12, and IL13, and stool calprotectin levels. Each study visit included the completion of standardized questionnaires such as the PCDAI or PUCAI.
Follow-up appointments are scheduled every 2, 4, 8, and 12 weeks. Patients had a physical examination, as well as ESR, CRP, and serum albumin levels, at each follow-up visit. At weeks 4 and 12, stool calprotectin, serum TNF-, IL17, IL10, IL12, and IL13 levels were measured.
Growth parameters (body weight, height and BMI) beside serum levels of calcium, PTH, vitamin D, triglycerides, cholesterol, glucose, and hemoglobin levels were measured at start as well as by the end of our study.
KIDMED Test
The KIDMED (Child and Adolescent Mediterranean Diet Quality Index) test is a technique for determining whether or not children and young adults are adhering to the MD program. Serra-Majem et al designed and validated it.13 The index is based on a 16-question test that can be self-administered or interviewed and goes from 0 to 12. Questions having a negative meaning in terms of MD are given a value of −1, while those with a positive aspect ratio are given a value of +1. Totals from the administered test are divided into three categories: 1) >8, ideal Mediterranean diet; 2) 4–7, optimization is required to align intake with Mediterranean patterns; 3) ≤3, poor adherence to MD.14
Disease Activity
The CD group’s disease activity was measured using the paediatric Crohn’s disease activity index (PCDAI), which has a score range of 0–100, with higher values indicating more active illness. Inactive disease is indicated by a score of less than 10, mild disease is shown by a score of 11–30, moderate disease is indicated by a score of 30–45, and severe disease is indicated by a score of >45. A drop of 12.5 points is considered a significant improvement. The juvenile Ulcerative Colitis Activity Index was used to assess disease activity in the UC group (PUCAI). The PUCAI score ranges from 0 to 85; a score of less than 10 indicates remission, 10 to 34 indicates mild disease, 35 to 64 indicates moderate disease, and more than 64 indicates severe disease. A PUCAI change of more than 20 is considered clinically significant. Both PCDAI and PUCAI are of excellent validity, reliability, responsiveness and feasibility.15,16
Inclusion Criteria
*Adolescents and children (12–18 years) who have CD or UC with mild or moderate disease activity, as defined by a PCDAI score of 10–45 or a PUCAI score of 10 to 64.
*Apart from having IBD, having a good health.
* There could be no changes in IBD medication(s) for a minimum of one month for immunosuppressive medicines and two months for biologics.
*Accept the invitation to take part in the research.
Exclusion Criteria
*History of GIT operation
*Pregnancy or desire to be pregnant within study period
*Systemic disorders eg cardiac, renal, pulmonary, endocrine … etc
*Psychiatric disorder
*Unable to comply with study requirements
*Unable or unwilling to consent
*Presence of alcohol or drug abuse.
Safety and Clinical Adverse Events
Every visit (at weeks 2, 4, 8, and 12), clinical and laboratory evaluations, as well as weekly phone communication with patients were assessed to ensure the safety of the patients. Regardless of withdrawal status, any subject with a suspected complaint was retained for clinical and laboratory examination.
Ethical Considerations
At the start of the study, all subjects (and care-givers) were full informed about the study, their rights and objectives of our study and signed a written consent after approval to participate in the study. The study was approved by the institutional ethical Committee of Tanta University Faculty of Medicine and the study complies with the Declaration of Helsinki. This research registered under trial number PACTR202003564365054.
Statistical Analysis
The mean and standard deviation were used to express all quantitative data. Percentage was used to express categorical variables. The Shapiro-Wilk test was used to determine if the data had a normal distribution. One way analysis of variance (ANOVA) was used to examine differences between the means of more than two groups, followed by post-hoc analysis. To compare means within the same group, a paired t test was utilized. SPSS V.20 was used for all of the analyses (SPSS, Chicago. IL, USA).
Results
This study included 100 IBD patients aged 12 to 18, divided into two groups, each with 50 patients: group I (28 males and 22 females with a mean age of 13.8±2.6 years, including 26 patients with CD and 24 patients with UC), and group II (26 males and 24 females with a mean age of 13.1±1.9 years, including 28 patients with CD and 22 patients with UC). Before the trial, group I had an average disease duration of 3.1±1.6 years while group II had an average disease duration of 3.4±1.3 years. Table 1 shows the mean demographic, clinical, and basic laboratory data of both groups, with no significant differences between them at the beginning of the trial, including activity scores and treatment.
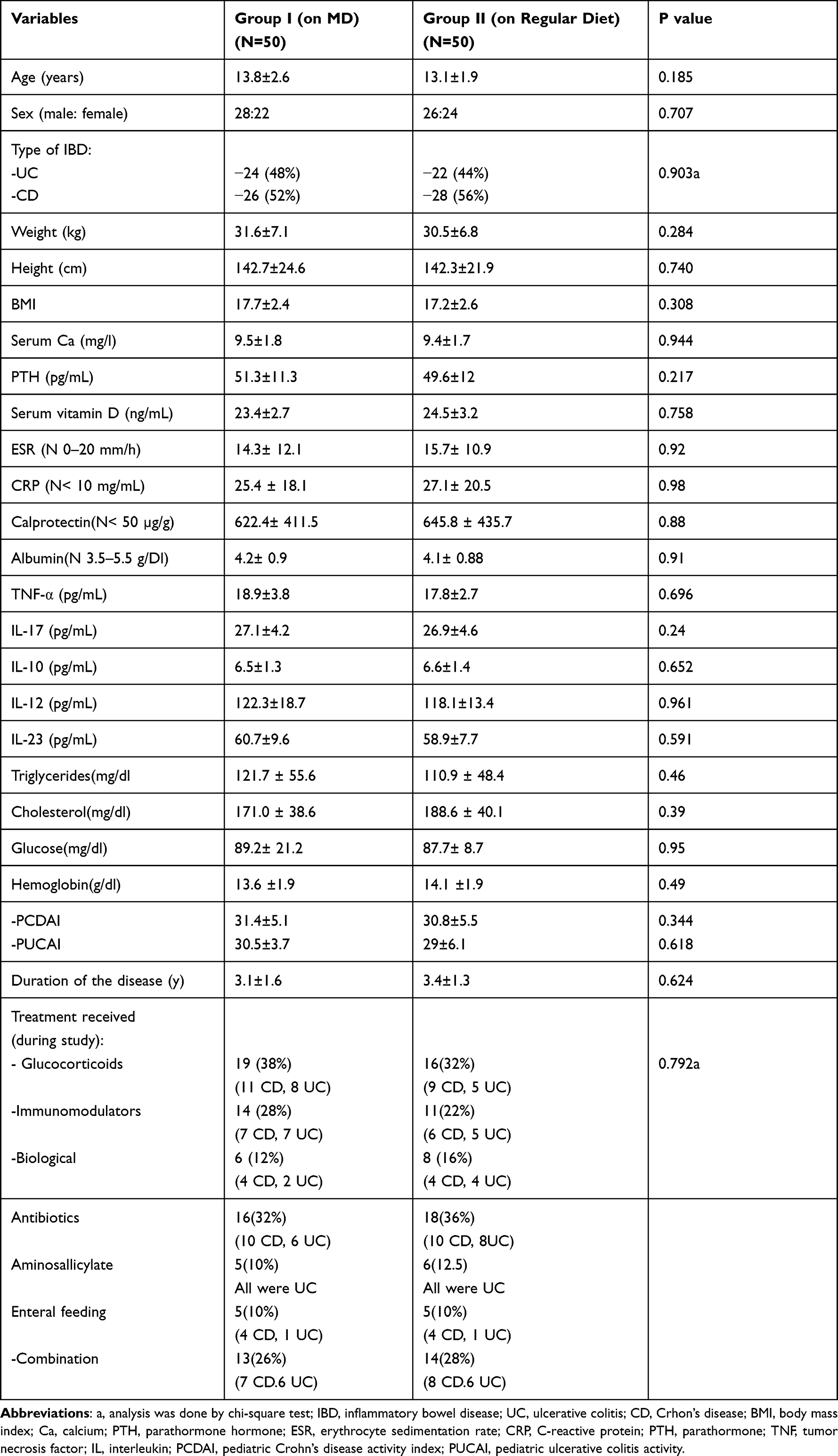 |
Table 1 Demographic, Clinical and Laboratory Data of All Patients at Start of the Study |
At time of diagnosis, Montreal classification (L1-L4 for CD; E1-E3 for UC) used for classification of patients, shown in Table 2, with exclusion of patients with fistula in our study because they may need surgical interference at any time. Clinical variables of all patients at start of the study shown in Table 3; in 54 patients with CD (in both groups) the common general presentations were weight loss (42 patients), fever (16 patients), anorexia (18 patients) growth retardations (39 patients) and lethargy (in 12 patients), while gastrointestinal presentations included abdominal pain (42 patients), diarrhea (35 patients), rectal bleeding (16 patients), nausea/vomiting (6 patients), constipation (2 patients), perianal disease other than fistula (5 patients) and mouth ulcers (2 patients). In 46 patients with UC (in both groups) the common general presentations were weight loss (37 patients), fever (4 patients), anorexia (5 patients), growth retardations (39 patients) and lethargy (in 9 patients), while gastrointestinal presentations included abdominal pain (40 patients), diarrhea (42 patients), rectal bleeding (34 patients), nausea/vomiting (1patient), constipation (1 patient), and mouth ulcers (2 patients). Most patients presented with more than one symptom.
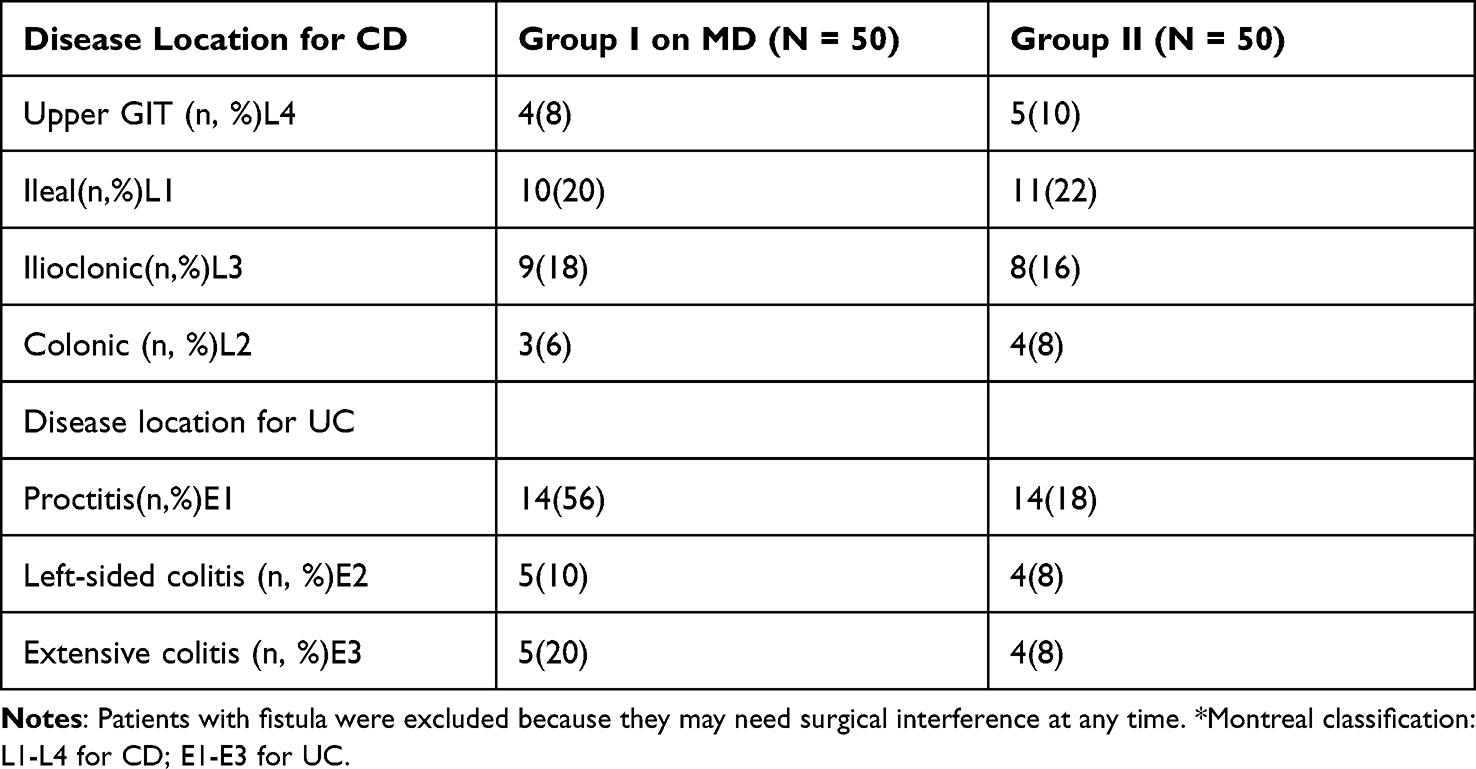 |
Table 2 Disease Location, and Montreal Classification* |
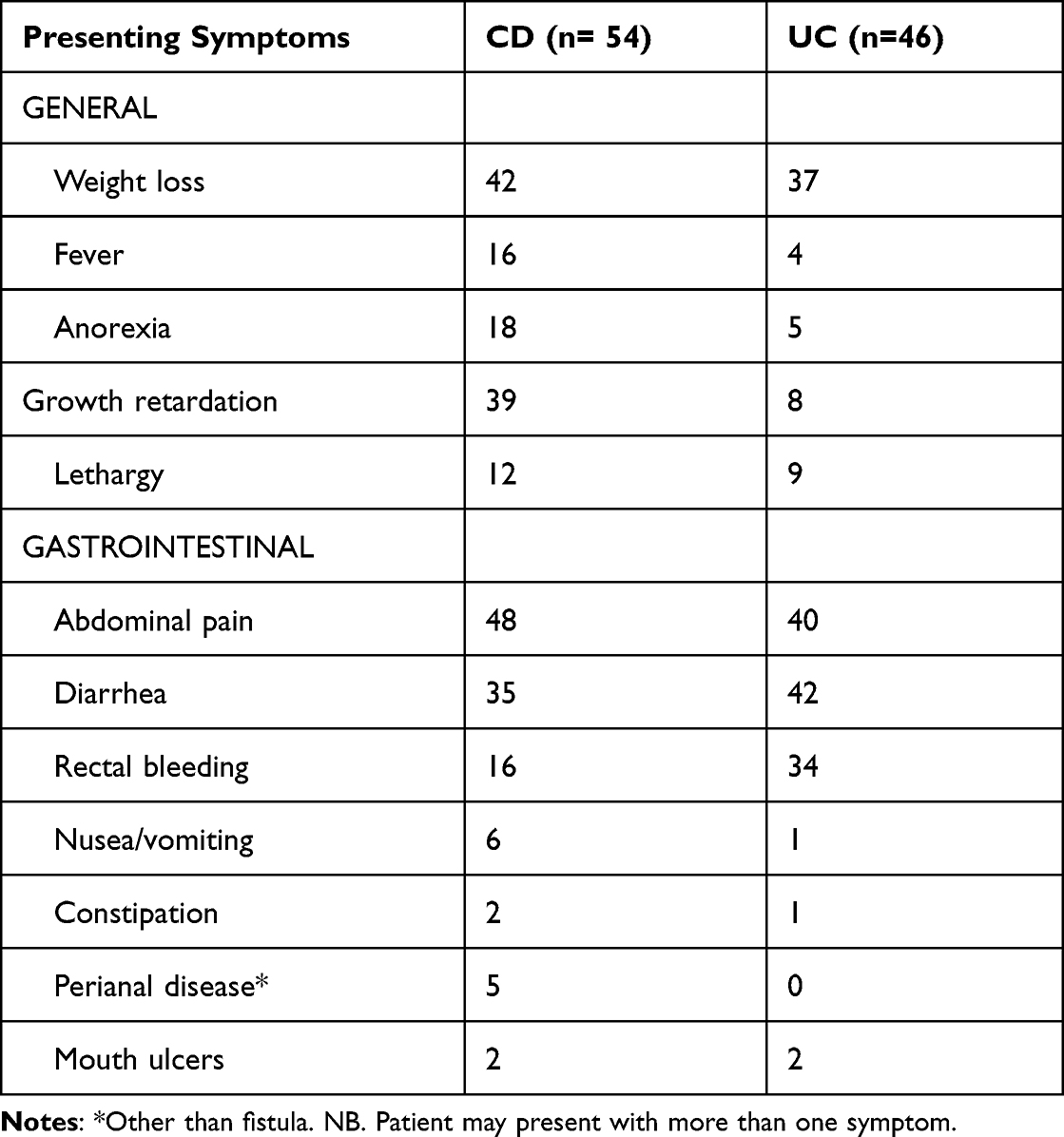 |
Table 3 Clinical Variables of Studied Patients |
No adverse events regarding MD were reported as reflected by non-significant changes in growth parameters, serum calcium, vit D, PTH, triglycerides, cholesterol, glucose and hemoglobin when compared to their values at the outset of our research (Table 4). Four patients stopped the study in group I (2 CD and 2 UC), 2 of them due to difficulty maintaining the diet (both were UC) and 2 due to failure of attendance at prescribed times. Three patients in group II (1 UC and 2 CD) stopped the study due to failure of attendance at prescribed times. All missed patients were replaced by new ones fulfilling study protocols.
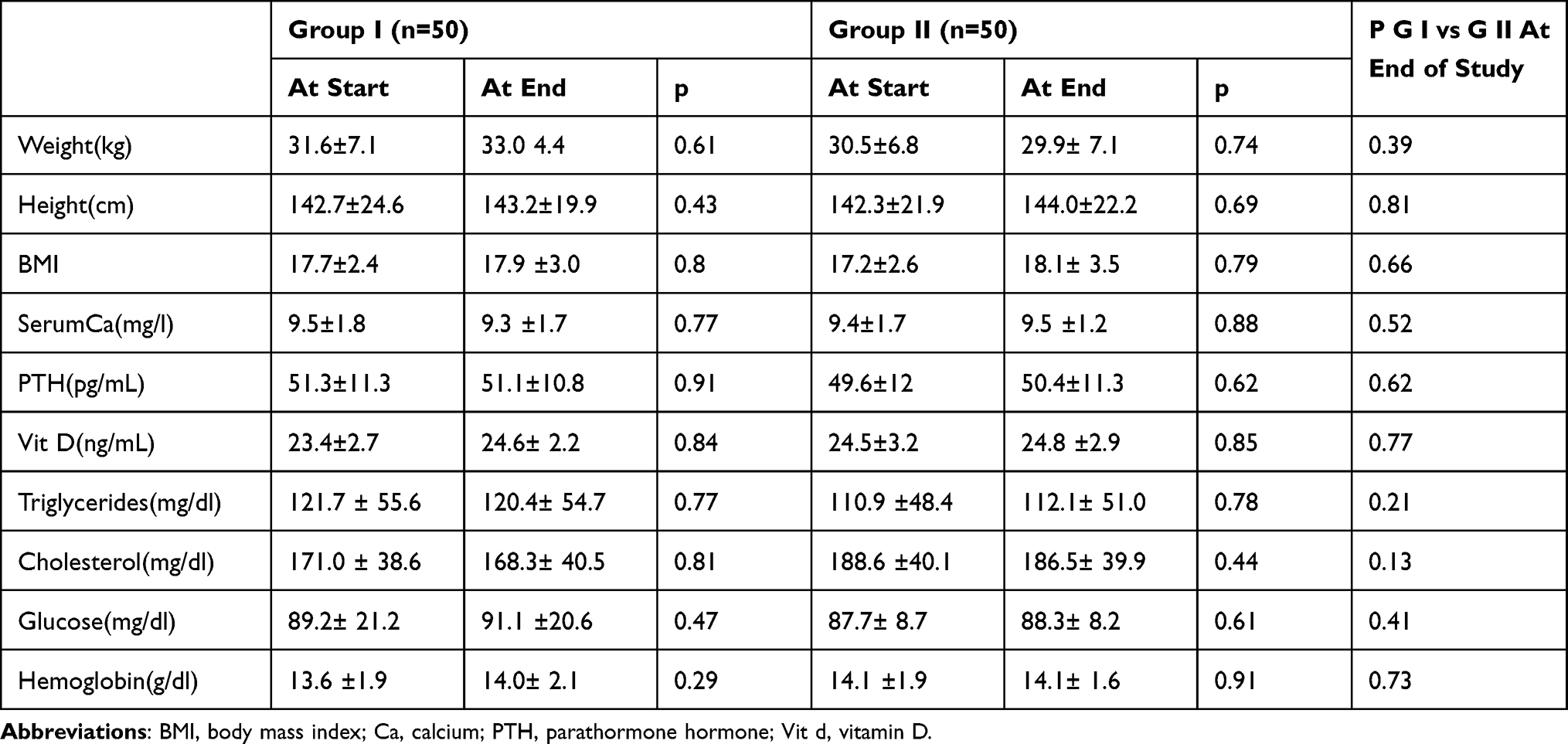 |
Table 4 Growth Parameters, Serum Calcium, Vit D, PTH Triglycerides, Cholesterol. Glucose and Hemoglobin at Start of Study vs at the End |
Two weeks after initiation of the study, 2 patients in group I (both were CD) were in clinical remission (PCDAI <10). After 4 weeks, 7 patients in group I (4 CD and 3 UC) were in clinical remission, while in group II only 3 patients (2 CD and 1 UC) were in clinical remission. At week 8; significant clinical remission in CD patients in group I (14 patients with PCDAI <10) was recorded compared to CD patients in group II (only 8 patients were in clinical remission), with mean PCDAI 9.7 ± 11.2 in group I compared to 11.3 ±10.5 in group II. Regarding UC patients at week 8; 8 patients were in clinical remission in group I versus 6 patients in group II, with mean PUCAI 8.3 ± 4.7 in group I and 10.6 ± 5.4 in group II with no significant difference between both groups. At the end of study (week 12), 24 CD patients in group I were in clinical remission while in group II 21 CD patients in clinical remission with a significant lower mean PCDAI in group I (6.4± 8.1) compared to mean PCDAI in group II (10.8 ± 7.4). In UC patients at the end of study, 22 patients in group I were in clinical remission, while in group II 18 patients in clinical remission with a significant lower mean PUCAI in group I (7.6± 11.2) compared to mean PCDAI in group II (9.2 ± 7.5). CRP was high in both groups at start of study (mean level 25.4 ± 18.1 in group I versus 27.1± 20.5 in group II), still high at second week (19.6 ±21.1 versus 22.3 ± 16.5) and fourth week (12.3± 11.3 versus 16.1 ± 14.9), with no significant differences between both groups. At 8 th week, there was significant decrease in mean CRP in group I (4.4 ± 2.7) compared to group II (8.1 ± 3.0), and this significant difference extended to end of study (3.1 ± 0.09 versus 5.8 ± 3.5). ESR was high in both groups at start of study (14.3 ± 12.1 versus 15.7± 10.9) and gradually decreased in both groups (11.7± 9.9 vs 11.9 ± 10.0 at week 2, 10.2 ± 8.8 vs 10.0 ± 7.8 at week 4, 8.3± 6.3 vs 8.2 ± 0.88 at week 8, and 6.5 ± 5.2 vs 5.8± 6.1 at the end of study) with no significant differences recorded between both groups allover our study period. Serum albumin showed normal mean values allover study period with mean value 4.2± 0.9 vs 4.1 ± 0.88 at start of study, 4.2± 0.88 vs 4.2± 0.91 at second week, 4.3± 0.78 vs 4.2± 0.77 at fourth week, 4.4 ±0.45 vs 4.3± 0.7 at 8th week, and 4.3 ±0.68 vs 4.4± 0.37 at the end of study, with no significant differences between both groups allover our study period. Fecal calprotectin was high in both groups at start of study (622.4 ± 411.5 in group I, 645.8 ± 435.7) and at fourth week (405.4± 168.8 vs 488.2 ±230.9) with no significant differences between both groups, while at the end of study, there was significant decrease in its level in group I (mean level 221.5 ± 88.5) compared to group II (mean level 395.7 ±194.4) (Table 5). Other serum inflammatory markers (TNF- α, IL17, IL10, IL 12 and IL13) were comparable in both groups at start of study. With non-significant drop in both groups at the end of fourth week (p > 0.05), while at the end of our study there were significant decrease in group I in all measured cytokines compared to group II (p ≤ 0.05) except IL10 (p = 0.1).
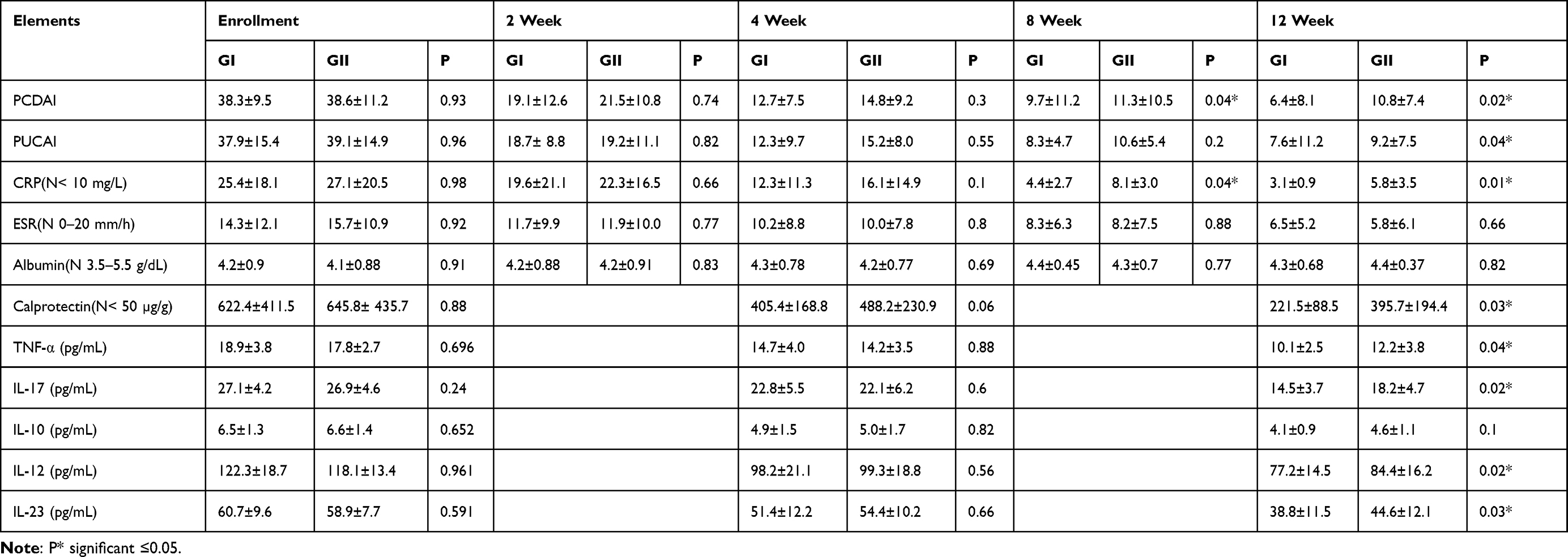 |
Table 5 Mean IBD Activity Index and Mean Inflammatory Measures for Patients During Study Period |
Discussion
What to eat? This is one of the most commonly requested questions by IBD patients. Many people also seek dietary advice, believing that diet is a better alternative to medical treatment.17 Changing a patient’s diet to treat IBD activity has long been one of the most desirable therapy methods for IBD. Unfortunately, due to a lack of high-quality evidence supporting a specific dietary intervention, patients have been forced to adopt exclusion diets with no proof of benefit or safety, particularly in pediatric age groups.18
The nutritional intervention with the most evidence for inducing clinical and endoscopic remission remission in pediatric patients with Crohn’s disease is exclusive enteral feeding (EEN).19
Many studies have been conducted in children patients with IBD using various feeding methods with variable results. Levin et al20 reported a trial involving 78 pediatric patients with mild to moderate Crohn’s disease activity who were given either a Crohn’s disease exclusion diet (CDED) with partial enteral nutrition (PEN) or PEN alone, with non-significant improvements in CRP, fecal calprotectin, and fecal microbial profile in CDED patients. Other diets that have been tested in IBD include the Food Influence on the Intestinal Microbiota diet,21 the Specific Carbohydrate Diet (SCD),22 the Anti-Inflammatory Diet,23 and the low-fermentable oligosaccharide, disaccharide, monosaccharide, and polyols (low FODMAP) diet,24 all of which have different study designs, variable end points, and/or a limited number of patients.
High intakes of plant foods (vegetables, legumes, fruits, nuts, and whole grain cereals), olive oil as the main source of fat, moderate amounts of dairy products (yoghurt and cheese), and limited to moderate amounts of fish and meat25 characterise the Mediterranean Diet (MD). The MD was listed as a Cultural Landmark for Greece, Italy, Spain, and Morocco on the UNESCO Intangible Cultural Heritage List in November 2010 (Resolution 5. COM 6.4).25 Despite the fact that different geographical locations of the Mediterranean have varied diets affected by social, cultural, religious, or economic circumstances, it is reasonable to infer that these diets are all variations of the same MD.26,27
MD has recently received a lot of attention as a potential novel treatment strategy for gastrointestinal28 and extra intestinal illnesses.29 The findings of this prospective trial suggest that MD was safe and well tolerated in paediatric and adolescent patients with active IBD. In addition, the majority of patients had clinical and objective laboratory improvements, including normalization of inflammatory markers.
Although most patients achieved clinical remission after 12 weeks of treatment, patients in group I (MD adherents) showed significant reductions in both clinical scores (PCDAI and PUCAI) and most inflammatory markers (CRP, calprotectin, TNF-, IL17, IL12, and IL13) when compared to patients on their regular diet, with PCDAI and CRP improving earlier. The protective effects of MD on IBD may be due to its individual nutritional components, which in turn affect the structure and function of the gut. Additional properties of MD potentially related to beneficial effects on the gut include the antioxidant and anti-inflammatory effects of MD components.30,31
Vegetables, fruits, seafood, and possibly grape wine are all part of a Mediterranean diet. The accumulation of nitrates/nitrites/NO•, polyunsaturated fatty acids (PUFA), and polyphenolic substances, such as resveratrol, in the human body is caused by regular consumption of these foodstuffs.31
Although the oxidation of NO• accounts for 80% of the basal plasma nitrite level (NO2), the reduction of nitrate (NO3) may also contribute to the increase of NO2.32,33
Exogenous injection of NO3- (10 mg/kg in humans) has been shown to elevate plasma NO2 concentration by up to 4–5 times in 30 minutes.34 Green vegetables such as spinach, lettuce, cabbage, radish, and beets35,36 and beef37 are the most abundant dietary sources of NO3- for the human body. Furthermore, processed meats have the same NO.37 NO2-dependent vasodilation regulates hypoxic blood flow and improves tissue microcirculation at the organ level.37
The Mediterranean diet is known for its abundance of vegetables and fish, both of which are high in PUFA (−3, 6, 9) of various types. In a nutshell, PUFAs are classified into three groups based on the position of the first methyl carbon double bond, referred to as ““: (1) −3, which includes DHA-docosahexaenoic, EPA-eicosapentaenoic, and ALA-alpha-linolenic; (2) −6, which includes LA-linoleic, GLA-linolenic, and AA-arachidonic; and (3) −9, which includes OA-oleic acid. The protective effects of EPA and DHA may be mediated via the creation of reactive lipid molecules termed resolvins, according to extensive research.38
Resolvin (E1, D1) is well-known for its anti-inflammatory characteristics, since it prevents polymorphous neutrophils (PMN) from activating and translocating to tissue.39,40 Resolvin E1 suppresses TNF-induced nuclear translocation of NF-kB and controls cytokine/chemokine production.41,42
Koenitzer et al43 identified several oxo-electrophilic derivatives of DHA and EPA that are produced in activated macrophages via the cyclooxygenase-2-dependent route. It has been discovered to have potent anti-inflammatory activities, similar to resolvin.9,43–48,49
Grape wine is a cornerstone of the Mediterranean diet, and the anti-inflammatory properties of grape wine are typically linked to its phenolic components. Antioxidants like quercetin, resveratrol, and catechins are polyphenolic chemicals. As a result, one of the preventive strategies they give could be oxidative stress inhibition.44
It should be mentioned that PUFAs increased endothelial NO production in human cells, and that the interaction between NO2/NO• and PUFAs results in the creation of nitroalkenes, further suggesting a putative interaction between NO2 and PUFAs. Nitroalkenes may also promote NO production by inducing eNOS expression, resulting in a positive feedback loop.45
In the light of our findings, we believe that MD may be a good step in the dietary management of children with IBD and could be brought more closely to pediatric patients with IBD via nutritional educational programs. However, future studies on larger sample size of patients and longer follow up is needed to confirm our results.
Our findings imply a general advantage for IBD patients in MD, although there are certain limitations to our trial. Colonoscopy was not used to measure the degree of mucosal healing in this trial, but C-reactive protein and stool calprotectin were used to objectively assess inflammation. The same study, although confirming the observed improvements in clinical disease activity, also emphasizes some of the nutritional therapy’s challenges. Due to the difficulty of sticking to the diet, two patients were unable to complete the trial.
Furthermore, while the majority of patients gained weight, some did not, and while weight and BMI for patients in MD improved overall, maintaining sufficient weight gain and nutritional adequacy is critical to ensuring good overall integration of the regimen. More research is needed to determine the long-term impact of MD on growth. Despite these limitations, this study reveals that there is a link between activity ratings and the degree of inflammation in young patients with inflammatory bowel disease and ischemic brain disease, suggesting that this could be a therapy option.
Conclusions
In children and adolescents, adhering to MD for three months at least can improve clinical outcomes and inflammatory indicators. The processes underlying this link, as well as the causal linkage between MD and IBD, require more research. If the current study’s findings are confirmed through broad nutritional evaluations, metabolic analyses and microbial assessments will be able to provide a fuller picture of the diet-health relationship.
To further understand the effects of MD and alternative feeding strategies on the clinical course, laboratory and endoscopic outcomes in young children with IBD, more research with a larger number of patients and a longer duration is needed. MD could play a role in the treatment of such a chronic disease, alongside other options.
Data sharing statement: Raw data is available on reasonable request from the corresponding author.
Abbreviations
IBD, inflammatory bowel diseases; CD, Crohn’s disease; UC, ulcerative colitis; MD, Mediterranean diet; EEN, exclusive enteral nutrition; KIDMED test, Mediterranean diet quality index for children and teenagers; BMI, body mass index; Ca, calcium; PTH, parathormone hormone; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; PTH, parathormone; TNF, tumor necrosis factor; IL, interleukin; PCDAI, pediatric Crohn’s disease activity index; PUCAI, pediatric ulcerative colitis activity.
Disclosure
The authors report no conflicts of interest in this work.
References
1. El Amrousy D, El Ashry H, Hodeib H, Hassan S. Vitamin D in children with inflammatory bowel disease: a Randomized Controlled Clinical Trial. J Clin Gastroenterol. 2021;55(9):815–820. doi:10.1097/MCG.0000000000001443
2. Weinstock JV, Elliott DE. Helminths and the IBD hygiene hypothesis. Inflamm Bowel Dis. 2009;15:128–133. doi:10.1002/ibd.20633
3. Mahida YR, Rolfe VE. Host-bacterial interactions in inflammatory bowel disease. Clin Sci. 2004;107:331–341. doi:10.1042/CS20040136
4. Critch J, Day AS, Otley A, et al. Use of enteral nutrition for the control of intestinal inflammation in pediatric Crohn disease. J Pediatr Gastroenterol Nutr. 2012;54:298–305. doi:10.1097/MPG.0b013e318235b397
5. Wong AP, Clark AL, Garnett EA, et al. Use of complementary medicine in pediatric patients with inflammatory bowel disease: results from a multicenter survey. J Pediatr Gastroenterol Nutr. 2009;48:55–60. doi:10.1097/MPG.0b013e318169330f
6. Hou JK, Lee D, Lewis J. Diet and inflammatory bowel disease: review of patient-targeted recommendations. Clin Gastroenterol Hepatol. 2014;12:1592–1600. doi:10.1016/j.cgh.2013.09.063
7. Donini LM, Serra-Majem L, Bulló M, Gil Á, Salas-Salvadó J. The Mediterranean diet: culture, health and science. Br J Nutr. 2015;113(Suppl 2):S1–3. doi:10.1017/S0007114515001087
8. Bulló M, Lamuela- Reventós R, Salas- Salvadó J. Mediterranean diet and oxidation: nuts and olive oil as important sources of fat and antioxidants. Curr Top Med Chem. 2011;11(14):1797–1810. doi:10.2174/156802611796235062
9. Nadtochiy S, Redman E. Mediterranean diet and cardioprotection: the role of nitrite, polyunsaturated fatty acids, and polyphenols. Nutrition. 2011;27(7–8):733–744. doi:10.1016/j.nut.2010.12.006
10. Vrdoljak J, Vilovic M, Živkovic PM, et al. Mediterranean diet adherence and dietary attitudes in patients with inflammatory bowel disease. Nutrients. 2020;12:3429. doi:10.3390/nu12113429
11. Khalili H, Håkansson N, Chan SS, et al. Adherence to a Mediterranean diet is associated with a lower risk of later-onset Crohn’s disease: results from two large prospective cohort studies. Gut. 2020;69(9):1637–1644. doi:10.1136/gutjnl-2019-319505
12. Papada E, Amerikanou C, Forbes A, Kaliora AC. Adherence to Mediterranean diet in Crohn’s disease. Eur J Nutr. 2020;59:1115–1121. doi:10.1007/s00394-019-01972-z
13. Serra-Majem L, García-Closas R, Ribas L, Pérez-Rodrigo C, Aranceta J. Food patterns of Spanish schoolchildren and adolescents: the enKid Study. Public Health Nutr. 2001;4:1433–1438. doi:10.1079/PHN2001234
14. Serra-Majem L, Ribas L, García A, Pérez-Rodrigo C, Aranceta J. Nutrient adequacy and Mediterranean Diet in Spanish school children and adolescents. Eur J Clin Nutr. 2003;57:35–39. doi:10.1038/sj.ejcn.1601812
15. Hyams J, Markowitz J, Otley A, et al. Evaluation of the pediatric Crohn disease activity index: a prospective multicenter experience. J Pediatr Gastroenterol Nutr. 2005;41:416–421. doi:10.1097/01.mpg.0000183350.46795.42
16. Turner D, Hyams J, Markowitz J. Appraisal of the pediatric ulcerative colitis activity index (PUCAI). Inflamm Bowel Dis. 2009;15:1218–1223. doi:10.1002/ibd.20867
17. Lewis JD, Abreu MT. Diet as a trigger or therapy for inflammatory bowel diseases. Gastroenterology. 2017;152:398–414.e396. doi:10.1053/j.gastro.2016.10.019
18. Hwang C, Ross V, Mahadevan U. Popular exclusionary diets for inflammatory bowel disease: the search for a dietary culprit. Inflamm Bowel Dis. 2014;20:732–741. doi:10.1097/01.MIB.0000438427.48726.b0
19. Narula N, Dhillon A, Zhang D, et al. Enteral nutritional therapy for induction of remission in Crohn’s disease. Cochrane Database Syst Rev. 2018;4:Cd000542. doi:10.1002/14651858.CD000542.pub3
20. Levine A, Wine E, Assa A, et al. Crohn’s disease exclusion diet plus partial enteral nutrition induces sustained remission in a randomized controlled trial. Gastroenterology. 2019;157:440–450. doi:10.1053/j.gastro.2019.04.021
21. Sabino J, Vieira-Silva S, Machiels K, et al. Therapeutic manipulation of the gut microbiota through diet to reduce intestinal inflammation: results from the FIT trial. Gastroenterology. 2017;152:S1. doi:10.1016/S0016-5085(17)30385-2
22. Cohen SA, Gold BD, Oliva S, et al. Clinical and mucosal improvement with specific carbohydrate diet in pediatric Crohn disease. J Pediatr Gastroenterol Nutr. 2014;59:516–521. doi:10.1097/MPG.0000000000000449
23. Olendzki BC, Silverstein TD, Persuitte GM, et al. An anti-inflammatory diet as treatment for inflammatory bowel disease: a case series report. Nutr J. 2014;13(1):5. doi:10.1186/1475-2891-13-5
24. Prince AC, Myers CE, Joyce T, et al. Fermentable carbohydrate restriction (low FODMAP diet) in clinical practice improves functional gastrointestinal symptoms in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2016;22:1129–1136. doi:10.1097/MIB.0000000000000708
25. Unesco. The Mediterranean diet inscribed in 2010 on the representative. List of the intangible cultural heritage of the humanity; 2010. Available from: http://www.unesco.org/culture/ich/RL/00884.
26. Bach A, Serra-Majem L, Carraco JL, et al. The use of indexes evaluating the adherence to the Mediterranean diet in epidemiological studies: a review. Public Health Nutr. 2006;9:132–146. doi:10.1079/PHN2005936
27. Sánchez-Villegas A, Martínez JA, De Irala J, et al. Determinants of the adherence to an “a priori” defined Mediterranean dietary pattern. Eur J Nutr. 2002;41:249–257. doi:10.1007/s00394-002-0382-2
28. Agakidis C, Kotzakioulafi E, Petridis D, Apostolidou K, Karagiozoglou-Lampoudi T. Mediterranean diet adherence is associated with lower prevalence of functional gastrointestinal disorders in children and adolescents. Nutrients. 2019;11:1283. doi:10.3390/nu11061283
29. Sergiy M, Nadtochiy P, Emily K. Redman.Mediterranean diet and cardioprotection: the role of nitrite, polyunsaturated fatty acids and polyphenols. Nutrition. 2011;27(7–8):733–744. doi:10.1016/j.nut.2010.12.006
30. De Filippis F, Pellegrini N, Vannini L, et al. High-level adherence to a Mediterranean diet beneficially impacts the gut microbiota and associated metabolome. Gut. 2015;65:1–10. doi:10.1136/gutjnl-2015-310043
31. David LA, Maurice CF, Carmody RN, et al. Diet rapidly and reproducibly alters the human gut microbiome. Nature. 2014;505:559–563. doi:10.1038/nature12820
32. Lundberg JO, Weitzberg E, Cole JA, Benjamin N. Nitrate, bacteria and human health. Nat Rev Microbiol. 2004;2:593–602. doi:10.1038/nrmicro929
33. Lundberg JO, Govoni M. Inorganic nitrate is a possible source for systemic generation of nitric oxide. Free Radic Biol Med. 2004;37:395–400. doi:10.1016/j.freeradbiomed.2004.04.027
34. Raat NJ, Noguchi AC, Liu VB, et al. Dietary nitrate and nitrite modulate blood and organ nitrite and the cellular ischemic stress response. Free Radic Biol Med. 2009;47:510–517. doi:10.1016/j.freeradbiomed.2009.05.015
35. Ozdestan O, Uren A. Development of a cost-effective method for nitrate and nitrite determination in leafy plants and nitrate and nitrite contents of some green leafy vegetables grown in the Aegean Region of Turkey. J Agric Food Chem. 2010;58:5235–5240. doi:10.1021/jf904558c
36. Hord NG, Tang Y, Bryan NS. Food sources of nitrates and nitrites: the physiologic context for potential health benefits. Am J Clin Nutr. 2009;90:1–10. doi:10.3945/ajcn.2008.27131
37. Ologhobo AD, Adegede HI, Maduagiwu EN. Occurrence of nitrate, nitrite and volatile Nitrosamines in certain feedstuffs and animal products. Nutr Health. 1996;11:109–114. doi:10.1177/026010609601100203
38. Van Faassen EE, Bahrami S, Feelisch M, et al. Nitrite as Regulator of hypoxic signaling in mammalian physiology. Med Res Rev. 2009;29:683–741. doi:10.1002/med.20151
39. Serhan CN, Hong S, Gronert K, et al. Resolvins: a family of bioactive products of omega-3 fatty acid transformation circuits initiated by aspirin treatment that counter proinflammation signals. J Exp Med. 2002;196:1025–1037. doi:10.1084/jem.20020760
40. Serhan CN, Clish CB, Brannon J, Colgan SP, Chiang N, Gronert K. Novel functional sets of lipid derived mediators with antiinflammatory actions generated from omega-3 fatty acids via cyclooxygenase 2-nonsteroidal antiinflammatory drugs and transcellular processing. J Exp Med. 2000;192:1197–1204. doi:10.1084/jem.192.8.1197
41. Serhan CN, Gotlinger K, Hong S, Arita M. Resolvins, docosatrienes, and neuroprotectins, novel omega-3-derived mediators, and their aspirin-triggered endogenous epimers: an overview of their protective roles in catabasis. Prostaglandins Other Lipid Mediat. 2004;73:155–172. doi:10.1016/j.prostaglandins.2004.03.005
42. Bannenberg GL, Chiang N, Ariel A, et al. Molecular circuits of resolution: formation and actions of resolvins and protectins. J Immunol. 2005;174:4345–4355. doi:10.4049/jimmunol.174.7.4345
43. Koenitzer JR, Freeman BA. Redox signaling in inflammation: interactions of endogenous electrophiles and mitochondria in cardiovascular disease. Ann N Y Acad Sci. 2010;1203:45–52. doi:10.1111/j.1749-6632.2010.05559.x
44. Groeger AL, Cipollina C, Cole MP, et al. Cyclooxygenase-2 generates anti-inflammatory mediators from omega-3 fatty acids. Nat Chem Biol. 2010;6:433–441. doi:10.1038/nchembio.367
45. Yamazaki KG, Romero-Perez D, Barraza-Hidalgo M, et al. Short- and long-term effects of (−)-epicatechin on myocardial ischemia-reperfusion injury. Am J Physiol Heart Circ Physiol. 2008;295:H761–H767. doi:10.1152/ajpheart.00413.2008
46. El Amrousy D, Abdelhai D, Shawky D. Vitamin D and nonalcoholic fatty liver disease in children: a randomized controlled clinical trial. Eur J Pediatr. 2021. doi:10.1007/s00431-021-04243-4
47. Sabino J, Lewis JD, Colombel JF, et al. Treating inflammatory bowel disease with diet: a taste test. Gastroenterology. 2019;157(2):295–297. doi:10.1053/j.gastro.2019.06.027
48. El Amrousy D, El Ashry H, Maher S, Ganna S, Hasan S. Pulmonary function test abnormalities in children and adolescents with non-alcoholic fatty liver disease. Eur J Pediatr. 2021;180(6):1693–1699. doi:10.1007/s00431-021-03941-3
49. El-Saka AM, Zamzam YA, Haydara T, Abd-Elsalam S. Immunohistochemical staining with chemokine panel of non-specific colitis predicts future IBD diagnosis. Cytokine. 2020;127:154935. doi:10.1016/j.cyto.2019.154935
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.