Back to Journals » Patient Preference and Adherence » Volume 20
Adherence to Self-Care and Associated Factors Among Patients with Type 2 Diabetes in Southwestern Iran
Authors Shojaei Z, Khasraji Z, Charkazi A, Pahlavanzadeh B ![]()
Received 21 September 2025
Accepted for publication 14 January 2026
Published 28 January 2026 Volume 2026:20 569158
DOI https://doi.org/10.2147/PPA.S569158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Zahra Shojaei,1 Zahra Khasraji,1 Abdurrahman Charkazi,2 Bagher Pahlavanzadeh3
1Student Research Committee, Abadan University of Medical Sciences, Abadan, Iran; 2Department of Public Health, Environmental Health Research Center, Golestan University of Medical Sciences, Gorgan, Iran; 3Research Center for Environmental Contaminants (RCEC), Abadan University of Medical Sciences, Abadan, Iran
Correspondence: Bagher Pahlavanzadeh, Email [email protected]
Background: Effective self-care is essential for managing type 2 diabetes and preventing complications. However, adherence remains suboptimal. This study assessed self-care behaviors and associated factors among patients with type 2 diabetes in southwestern Iran.
Methods: A cross-sectional study was conducted on 153 patients (selected from 160 invited individuals; response rate: 95.6%) in Behbahan and Susangerd between October 2023 and March 2024. Questionnaires were checked for completeness, and complete-case analysis was performed. Self-care was assessed using the Persian version of the Summary of Diabetes Self-Care Activities (SDSCA). Differences among components were tested using Cochran’s Q, and multivariate logistic regression identified factors associated with adherence, with significance set at p < 0.05. An operational cutoff of ≥ 3.5 days per week was used to define “adequate” self-care.
Results: Adherence differed significantly among components (p < 0.001). It was highest for Diabetes Diet (OR 7.57, 4.63– 12.39) and Non-Smoking (OR 5.23, 3.25– 8.41) compared with General Diet (39.2%), whereas Glucose Monitoring (OR 0.41, 0.25– 0.67), Foot Care (OR 0.07, 0.03– 0.17), and Physical Activity (OR 0.03, 0.01– 0.10) were substantially lower. Only 8.5% adhered to five or more components. Higher income, older age, longer disease duration, and being single were associated with better adherence to specific behaviors.
Conclusion: Overall self-care was suboptimal, particularly for physical activity and foot care. Targeted interventions focusing on patient education and follow-up, especially for individuals with lower income or education, are urgently needed to improve adherence and reduce diabetes-related complications.
Keywords: type 2 diabetes, self-care behaviors, adherence, physical activity, foot care, Iran, diabetes management
Introduction
Diabetes mellitus is a chronic metabolic disorder characterized by hyperglycemia and progressive organ damage. Global estimates updated in 2024 by the World Health Organization and the NCD Risk Factor Collaboration indicate that over 800 million adults are now living with diabetes worldwide.1 According to the International Diabetes Federation (IDF), an estimated 588.7 million adults aged 20–79 years were living with diabetes in 2024, a number projected to increase to 852.5 million by 2050.2 In the Middle East and North Africa region, 84.7 million adults were affected in 2024, with a projected rise of 92% by 2050.2 Despite medical advancements, a significant “treatment gap” persists, with nearly 450 million adults aged 30 and older remaining untreated worldwide.1 Unlike other noncommunicable diseases, diabetes-related mortality continues to rise, with complications now contributing to over 2 million annual deaths globally.2,3
In Iran, the burden has intensified significantly; according to the latest Institute for Health Metrics and Evaluation (IHME) profiles, the burden of attributable death and disability has risen by over 60% in the last decade.4 During the same period, diabetes-related mortality increased by 5.4 per 100,000 population, ranking it as the seventh leading cause of death decade.4 As there is no definitive cure for diabetes, emphasis on appropriate care measures is essential to prevent serious complications.5 Self-care is defined as the acquisition of knowledge and skills through an ongoing process that enables individuals to live with the complex nature of the disease within their social context.6 It is considered a cornerstone of diabetes management,7 encompassing activities such as blood glucose monitoring, dietary adherence, physical activity, medication management, foot care, and smoking cessation.8 These activities play a vital role in improving quality of life and preventing both acute and chronic complications.9
Despite the well-documented benefits of self-care, adherence to these behaviors remains low,10,11 with notable variation across different self-care domains.7,12,13 Demographic and social factors—including gender, marital status, religious beliefs,14,15 education level, income, and access to health insurance16,17—have been identified as key determinants of adherence. Khuzestan Province presents a distinctive setting for examining diabetes self-care due to its extreme climate, pronounced socioeconomic disparities, and challenges in access to healthcare services and health education in rural areas.18 These contextual challenges may influence patients’ ability to consistently engage in recommended behaviors. The present study is grounded in the Information–Motivation–Behavioral Skills (IMB) Model, which conceptualizes diabetes self-care as a function of individuals’ knowledge, motivational factors, and behavioral competencies.19 Guided by this framework, this study aims to assess the status of self-care and identify its sociodemographic predictors in southwestern Iran. We hypothesize that socioeconomic factors, particularly income and education level, will be significantly associated with higher adherence to self-care behaviors.
Methods
Study Design, Setting, and Bias Control
The present study was conducted as a cross-sectional descriptive–analytical investigation between October 2023 and March 2024. The target population comprised patients with type 2 diabetes residing in Behbahan and Susangerd, cities with populations of 139,238 and 69,594, respectively (2016 national census). These populations are served by public primary health-care centers which act as the main referral points for chronic disease management within their respective catchment areas. These centers provide outpatient preventive services, chronic disease management, and diabetes follow-up care and are centrally located to ensure high accessibility for both urban and suburban residents.
For participant recruitment, five centers in Behbahan and two in Susangerd were selected. Eligible individuals who attended these centers were consecutively enrolled based on predefined inclusion and exclusion criteria. Trained research assistants confirmed eligibility through review of medical records and brief interviews.
The study was conducted and reported in accordance with the STROBE checklist for cross-sectional studies.20 To minimize bias, recall bias was reduced by asking participants about self-care behaviors during the preceding week, selection bias was minimized through consecutive recruitment, and social desirability bias was addressed by administering questionnaires in a private setting with standardized instructions, without involvement of research staff in participants’ clinical care. Participants’ responses were anonymized and confidentiality was maintained.
Ethical Approval and Consent / Data Security
The study protocol was approved by the Ethics Committee of Abadan University of Medical Sciences (Ethics Code: IR.ABADANUMS.REC.1402.085). Participants provided implicit consent by voluntarily completing the questionnaire after receiving a full explanation of the study objectives and procedures. This procedure was approved by the Ethics Committee. The study was conducted in accordance with the guidelines and regulations of the Declaration of Helsinki. Questionnaires were completed in a private setting, with trained research staff providing standardized instructions and no involvement in participants’ clinical care. To ensure data security, all responses were anonymized, stored in password-protected files, and accessible only to the research team. All data were entered by trained research staff and subsequently checked for completeness, logical consistency, and out-of-range values prior to analysis.
Inclusion and Exclusion Criteria
Inclusion criteria consisted of a minimum of six months since diagnosis, the presence of a medical record at the selected centers, the ability to perform self-care behaviors, no hospitalization during the previous week, and the absence of speech, mental, or hearing impairments. Exclusion criteria included individuals who declined consent, a diagnosis of gestational diabetes, incomplete questionnaire responses, and inability to recall self-care behaviors during the preceding week. All participants were fully informed of the study objectives and assured of the confidentiality of their personal information. Questionnaires were completed by participants with assistance from trained research staff when needed. Research staff were not involved in participants’ clinical care. Standardized instructions were provided, and questionnaires were completed in a private setting. No personal identifiers were recorded.
Sample Size Calculation
To determine the required sample size, an a priori power analysis was performed using G*Power version 3.1.9.7 (t-tests: Mean difference from constant, one-sample case). Based on a one-tailed test, an effect size of d = 0.2, α= 0.05, and a power of 0.80, the required sample size was calculated as 156. The final sample included 153 participants, which provides a statistical power of approximately 0.79, deemed sufficient for the study’s objectives.
Participants were recruited by trained research assistants who confirmed eligibility through medical record reviews and screening interviews. The number of individuals who declined consent was recorded to ensure transparency in the recruitment process. Furthermore, individuals with gestational diabetes were excluded to maintain a homogeneous focus on the chronic management of Type 2 Diabetes, as their self-care requirements differ significantly. Missing data were documented and addressed by excluding incomplete questionnaires.
Data Collection and Measures
Data were collected using a two-part questionnaire. The first part included demographic characteristics and duration of diabetes. The second part employed the Persian version of the Summary of Diabetes Self-Care Activities (SDSCA), a validated self-report measure assessing diabetes self-care behaviors.8
The SDSCA consists of 11 items covering general diet, specific diet, physical activity, blood glucose monitoring, foot care, and smoking. For items 1–10, participants reported the number of days during the previous week they engaged in each behavior on a 0–7 scale. The second specific diet item (consumption of high-fat foods) was reverse-scored. Smoking status was assessed dichotomously (0 = yes, 1 = no), following standard scoring procedures.8
Component scores (excluding smoking) were calculated by averaging relevant items, with higher scores indicating better self-care. Due to the low correlation between dietary subcomponents, general and specific diet were analyzed separately, as recommended by the scale developers.8
The Persian SDSCA has demonstrated acceptable reliability in Iranian populations, with reported Cronbach’s alpha values ranging from 0.68 to 0.82.21–24 In the present study, internal consistency coefficients ranged from 0.34 to 0.95, with high reliability for blood glucose monitoring (α = 0.95), general diet (α = 0.85), and foot care (α = 0.83). Lower alpha values for specific diet and physical activity are consistent with previous SDSCA studies and reflect the heterogeneous nature of these short, two-item subscales.8
Self-care adherence was defined using a cutoff score of ≥ 3.5, representing engagement in the behavior on at least four days per week. Although no universal SDSCA cutoff exists, this midpoint-based threshold provides a practical and clinically interpretable classification of adherence.21,24
Analysis
Descriptive statistics, including frequency tables and figures, were used to summarize participants’ characteristics and self-care behaviors. For each self-care component, an average score of ≥3.5 was classified as “desirable,” while scores < 3.5 were considered “undesirable.” This 3.5-day threshold represents the arithmetic midpoint of the week (50% adherence), serving as a standardized criterion for clinical interpretation. Overall self-care was assessed by calculating the number and percentage of participants achieving desirable levels across the six components.
To compare the proportions of desirable self-care across the six SDSCA components, Cochran’s Q test was employed, followed by post-hoc McNemar tests with Holm correction. A heatmap plot was generated to visualize these pairwise differences.
Prior to multivariate analysis, model validation was performed using collinearity diagnostics. The Variance Inflation Factor (VIF) for all predictors ranged from 1.16 to 2.63, well below the threshold of 5, indicating no significant multicollinearity. Multivariate Firth logistic regression models were fitted separately for each self-care component to identify independent predictors, adjusting for age, gender, education, income, marital status, and disease duration. This method was chosen to provide robust estimates and address potential issues of small sample sizes in sub-categories. Model fit was assessed using the Akaike Information Criterion (AIC).
Associations were reported as adjusted odds ratios (ORs) with 95% confidence intervals (CIs). In addition to statistical significance (p < 0.05), results were interpreted for clinical relevance based on the magnitude of the ORs. To ensure the robustness of our findings, a sensitivity analysis was conducted by repeating the regression models after excluding extreme outliers in self-care scores; the results showed no significant changes in the direction or magnitude of the associations. All statistical analyses were conducted using R software (version 4.4.0) and SPSS version 27.
Results
A total of 160 individuals were initially enrolled, of whom 7 were excluded due to incomplete questionnaires, resulting in a final sample of 153 participants (completion rate: 95.6%). The mean (SD) age of the study participants was 54.11 (8.97) years, ranging from 35 to 78. Among the participants, 59 (38.6%) were ≤50 years, 50 (32.7%) were 51–60 years, and 44 (28.8%) were >60 years. Regarding gender, 112 participants (73.2%) were male and 41 (26.8%) were female. In terms of marital status, 134 (87.6%) were married, while 19 (12.4%) were single or had a deceased spouse. Concerning education level, 25 participants (16.3%) were illiterate or had only elementary education, 87 (56.9%) had completed high school or held a diploma, and 41 (26.8%) had university education.
For monthly income, 52 participants (34.0%) reported <8 million IRR, 52 (34.0%) reported 8–16 million IRR, and 49 (32.0%) reported >16 million IRR. These categories correspond approximately to below minimum wage, around 1–2× minimum wage, and above 2× minimum wage, respectively. Health insurance coverage was reported by 141 participants (92.2%), while 12 (7.8%) did not have coverage. Regarding time since diabetes diagnosis, 49 participants (32.0%) had ≤7 years, 69 (45.1%) had 7–15 years, and 35 (22.9%) had >15 years. Additional details are provided in Table 1.
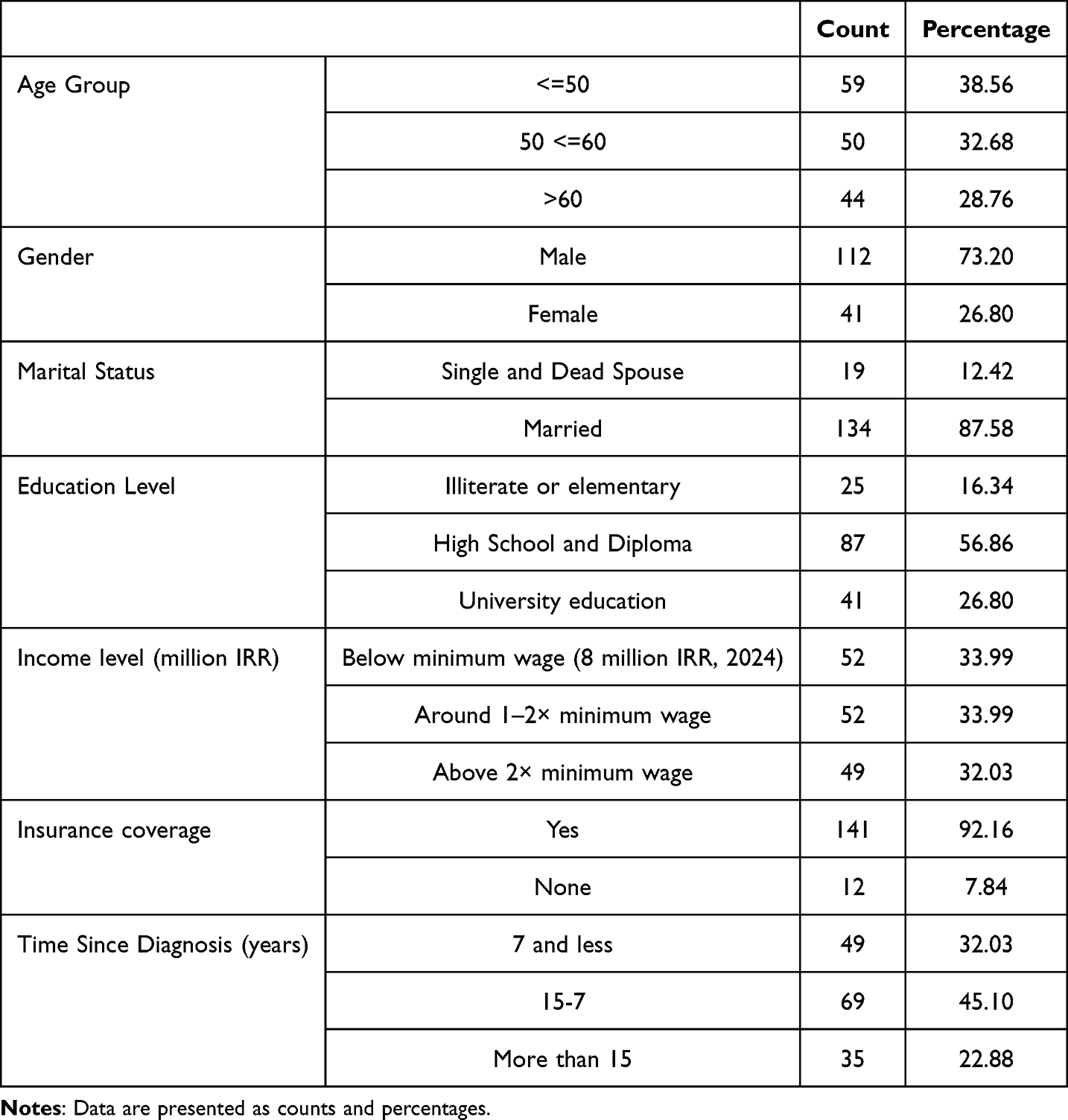 |
Table 1 Demographic, Social, and Clinical Characteristics of Participants with Diabetes (n = 153) |
Figure 1 illustrates the status of various self-care components. According to the chart, 82 participants (53.6%) of participants did not perform any foot care, 67 participants (43.8%) did not engage in physical activity, 23 participants (15.0%) did not monitor their blood glucose, and only 3 (2.0%) did not follow general dietary recommendations. In contrast, 127 (83.0%) adhered to a specific dietary regimen as recommended, and 118 (77.1%) were non-smokers. The proportion of participants with favorable self-care was 60 (39.2%) for general diet compliance and 32 (20.9%) for blood glucose monitoring. Only 7 (4.6%) and 3 (2.0%) of participants performed foot care and physical activity at desirable levels, respectively.
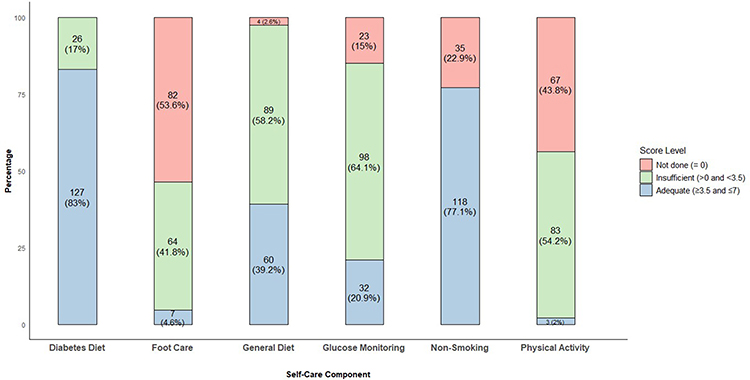 |
Figure 1 Distribution of self-care behavior levels among patients with type 2 diabetes. The stacked bar chart illustrates the percentage and frequency of patients achieving adequate (score ≥ 3.5), insufficient (>0 and <3.5), and “not done” (score=0) levels for each self-care component. The components are displayed on the x-axis, with the y-axis representing the percentage of the total sample (n=153). |
Figure 2 depicts the distribution of participants according to the number of self-care behaviors performed at a desirable level. Two participants (1.3%) did not achieve a desirable level in any self-care behavior. In contrast, 29 participants (19.0%) performed one behavior, 63 (41.2%) performed two behaviors, 46 (30.1%) performed three behaviors, 11 (7.2%) performed four behaviors, and 2 participants (1.3%) performed five self-care behaviors at a desirable level.
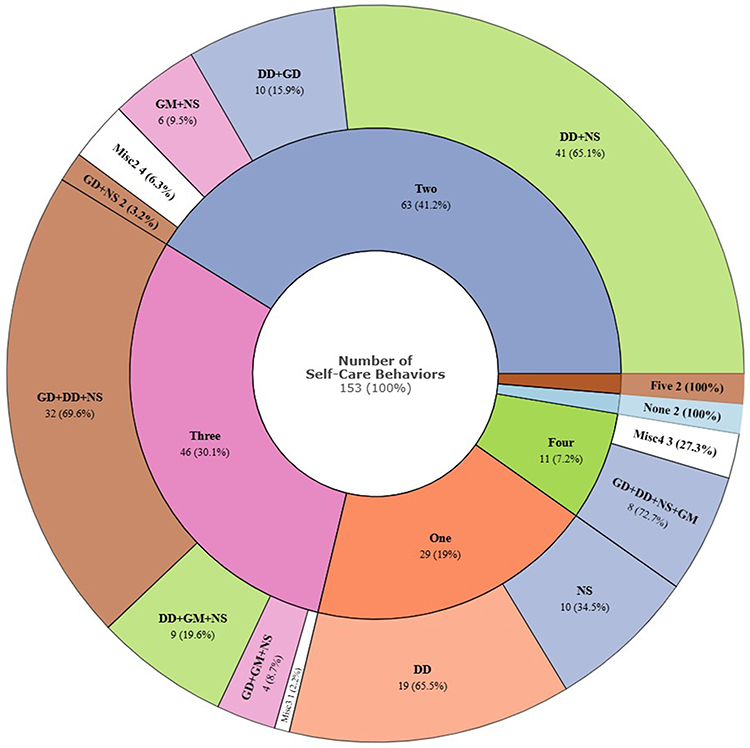 |
Figure 2 Patterns and combinations of diabetes self-care behaviors. The sunburst chart displays the distribution of the number of self-care behaviors performed by participants (inner ring) and the specific combinations of these behaviors (outer ring). Percentages are calculated based on the total sample for the inner ring and based on the respective group total for the outer ring. Abbreviations: DD, Diabetic Diet; NS, Non-Smoking; GD, General Diet; GM, Blood Sugar Monitoring; FC, Foot Care; Misc, Unique behavior combinations with low frequency. |
The sunburst diagram further illustrates the combinations of specific self-care behaviors among participants. Among participants performing only one desirable behavior, 19 adhered to a diabetic diet and 10 were non-smokers. Among participants performing two desirable behaviors, the most common combinations were: 41 participants (65.1%) following a diabetic and general diet while being non-smokers, 10 participants adhering to a diabetic diet and blood sugar monitoring, and 6 participants following general diet and non-smoking. For participants performing three desirable behaviors, the most frequent combinations included 32 participants adhering to both a specific and general diet while being non-smokers, 9 participants following a diabetic diet, blood sugar monitoring, and non-smoking, and 4 participants following other three-behavior combinations.
To examine adherence to various self-care behaviors, Figure 3 presents both the proportion of participants performing each behavior (left plot) and the pairwise differences in adherence between components (right plot).
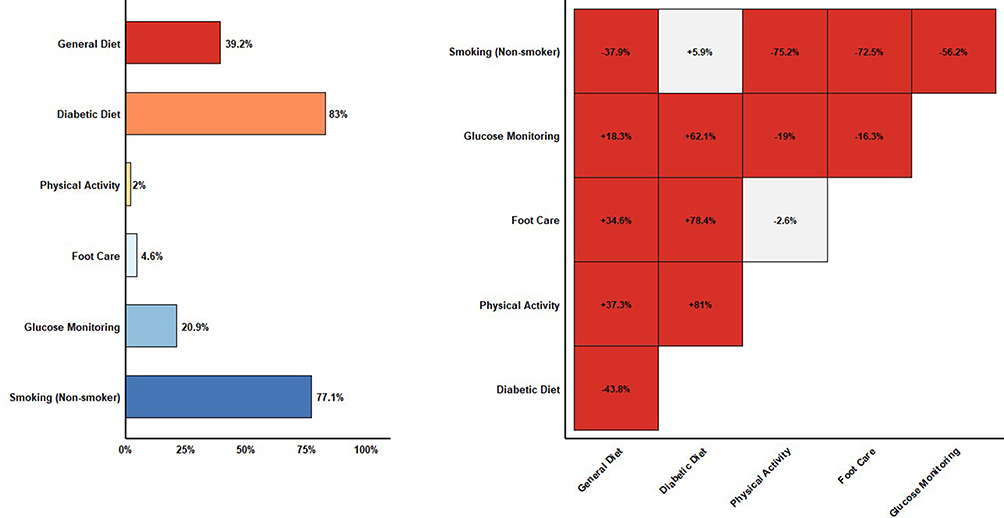 |
Figure 3 Adherence rates and pairwise statistical comparisons of self-care components. (Left) The horizontal bar chart shows the precise adherence percentage for each self-care behavior. (Right) The half-matrix heatmap displays the pairwise differences (Δ%) between components. Red cells indicate statistically significant differences (p < 0.05$) after Holm-Bonferroni adjustment using McNemar tests, while grey cells indicate non-significant differences. The Δ% values represent the difference in adherence between the column component and the row component. |
Among the components, diabetic diet adherence had the highest adherence, while physical activity had the lowest. To assess overall differences among all self-care behaviors, Cochran’s Q test was performed, which was statistically significant (p < 0.05), indicating that at least some behaviors differed in terms of adherence. This justified performing pairwise comparisons using McNemar tests.
The right panel shows a half-matrix heatmap of pairwise differences in adherence between self-care components. Most comparisons were statistically significant, indicating meaningful differences between behaviors. However, the comparisons between blood sugar monitoring and medication adherence and between diabetic diet and smoking cessation were not significant (p > 0.05), suggesting that the proportion of participants performing these pairs of behaviors was similar.
Table 2 presents the relationships between self-care components and selected demographic and social factors. Adherence to a general diet was higher among participants with a university education (p < 0.001) and those with an income greater than 8 million (p < 0.001). Adherence to a specific diet was higher in men (p = 0.018) and participants with an income above 8 million (p = 0.007). Physical activity was slightly higher among female participants (p = 0.04). Foot care was more frequent in participants over 50 years of age (p = 0.044) and those diagnosed with diabetes for more than 10 years (p = 0.05). Blood glucose monitoring was significantly higher among participants over 50 years (p = 0.013) and in men (p < 0.001). Non-smoking was significantly more common among participants aged 50 and under (p = 0.047), women (p < 0.001), and those with an income below 8 million (p = 0.001).
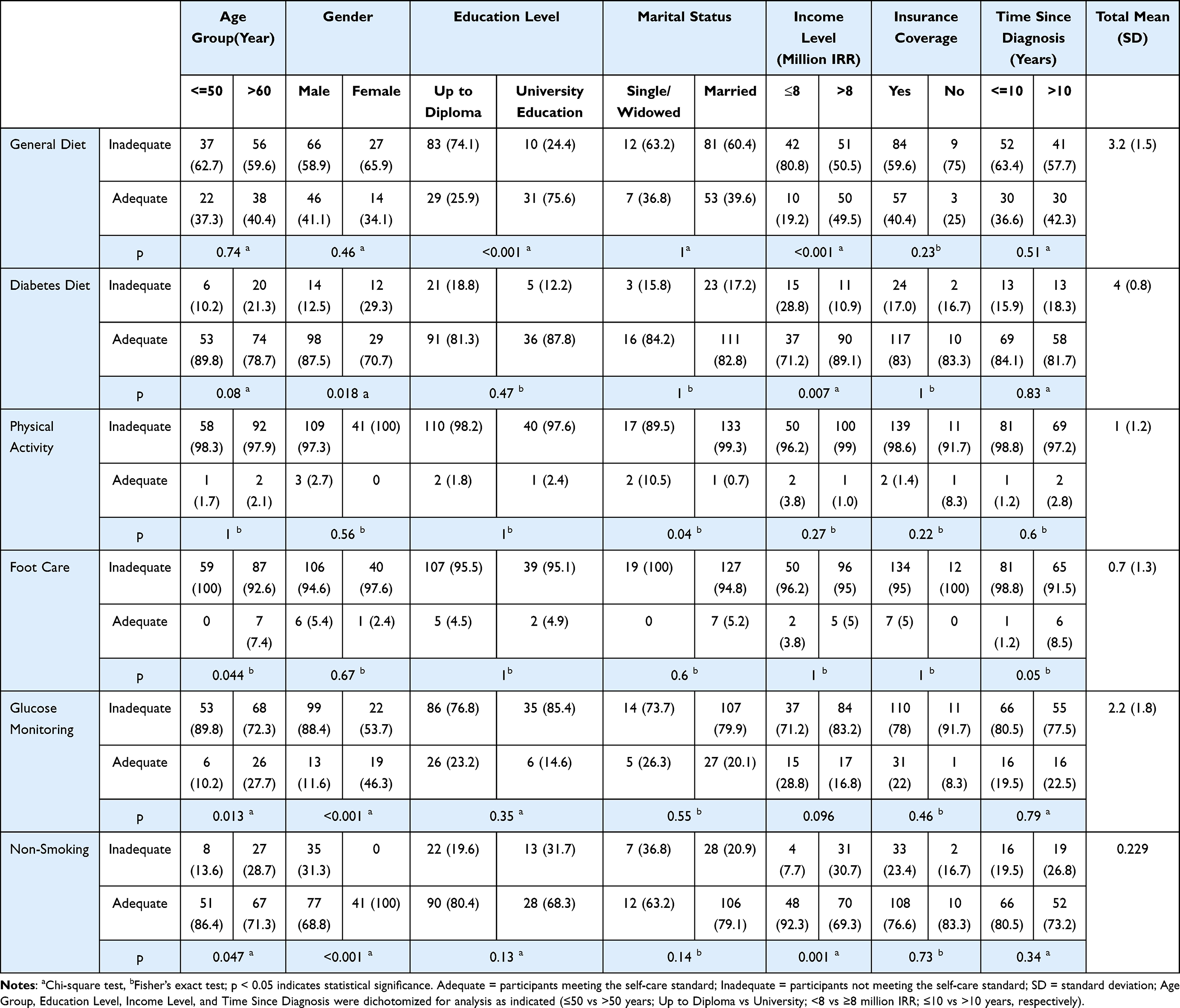 |
Table 2 Relationship Between Sociodemographic and Clinical Characteristics and Self-Care Components Among Participants with Diabetes (n = 153) |
Prior to fitting the multivariate logistic regression models, collinearity diagnostics were performed. The results confirmed the suitability of the predictors, with all VIF values < 2.7. Model fit was further confirmed using the Akaike Information Criterion (AIC).
In multivariate Firth logistic regression analyses of SDSCA self-care components (Table 3), higher education was significantly associated with better adherence to a general diet (aOR = 6.38, 95% CI: 2.75–15.73, p < 0.001). For diabetic diet, older age was associated with lower adherence (aOR = 0.31, 95% CI: 0.10–0.81, p = 0.016), while higher income showed a positive trend (aOR = 3.34, 95% CI: 0.92–11.68, p = 0.065). No significant predictors were identified for foot care, with wide confidence intervals reflecting sparse data. In glucose monitoring, older age (aOR = 6.61, 95% CI: 2.33–22.18, p < 0.001) and female gender (aOR = 11.03, 95% CI: 4.29–31.49, p < 0.001) were strong independent predictors.
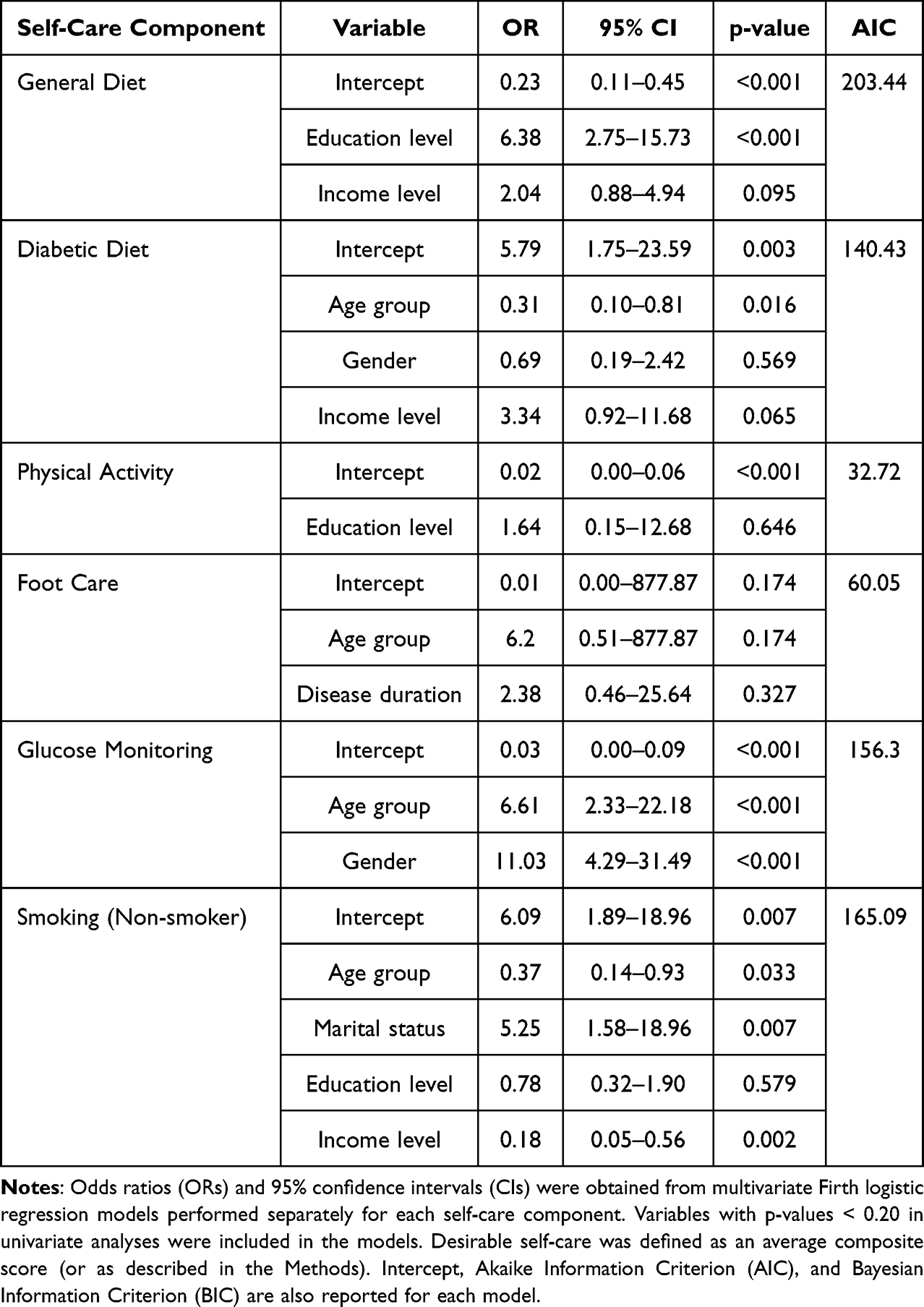 |
Table 3 Multivariate Logistic Regression Analyses Identifying Independent Predictors of Desirable Self-Care Components |
Regarding smoking behavior (non-smoking adherence), older age was associated with lower odds of being a non-smoker (aOR = 0.37, 95% CI: 0.14–0.93, p = 0.033). Similarly, higher income levels were associated with a significant decrease in the likelihood of non-smoking (aOR = 0.18, 95% CI: 0.05–0.56, p = 0.002). Conversely, marital status was a strong predictor of adherence, with married participants being over five times more likely to be non-smokers compared to those who were single or widowed (aOR = 5.25, 95% CI: 1.58–18.96, p = 0.007).
Discussion
The present study revealed that self-care behaviors among individuals with type 2 diabetes were suboptimal, with particularly low adherence to physical activity and foot care, while diet-related behaviors were relatively better. Socioeconomic factors, including income, marital status, and education, significantly influenced self-care practices, highlighting the role of regional social and economic determinants in shaping health behaviors. The clinical significance of these findings is underscored by the high magnitude of the observed effect sizes, particularly for education and gender, which represent primary drivers of adherence rather than mere correlates.
Socioeconomic and gender-related patterns appeared to shape self-care behaviors in this population. Women generally demonstrated better adherence to glucose monitoring and smoking cessation, whereas men tended to adhere more to diet-related behaviors. These patterns may reflect underlying social roles, health beliefs, and perceived risks associated with diabetes, as well as practical constraints such as workload and family responsibilities.25,26 Notably, the multivariate analysis revealed an eleven-fold increase in the odds of adhering to glucose monitoring among women compared to men (OR = 11.03). This massive disparity indicates a critical “monitoring gap” in the male population that requires urgent, gender-targeted clinical interventions to prevent long-term complications.
Physical activity showed the lowest adherence among all self-care behaviors in this population. Environmental factors, including high temperatures and limited recreational facilities in the region, may have further contributed to the low levels of physical activity observed. Overall, these findings suggest that both social and environmental determinants play an important role in influencing diabetes self-care behaviors, highlighting the need for tailored interventions that account for gender and local contextual factors.27
A systematic review by da Rocha, Silva, and Cardoso also reported low levels of physical activity among individuals with type 2 diabetes.13 Similarly, a 2024 systematic review and meta-analysis by Khosravizadeh et al, including 17 studies, found a pooled mean physical activity score of 2.12 (95% CI: 1.77–2.47).12 In 2023, Amerzadeh et al reported mean scores of 1.66 ± 1.23 and 1.58 ± 0.59 for the first and second items related to physical activity, values comparable to those observed in the present study.7 Moreover, Amerzadeh et al reported that 41.3% and 85.9% of participants did not engage in any self-care for the first and second physical activity items, respectively—percentages higher than those observed in the current study. This difference may be attributed to the older age of the sample in Amerzadeh et al’s study.
Factors such as high workload, comorbidities, financial constraints, and adverse weather conditions have been reported as barriers to physical activity.28 In Khuzestan Province, adverse weather may partially explain the low levels of physical activity observed in this study. Additionally, since the sample was drawn from individuals attending health centers, comorbidities and financial constraints may further contribute to reduced physical activity. Furthermore, as physical activity was higher among single participants than married participants, a high workload among the study population may also be a contributing factor.
Another self-care behavior that was poorly observed among the study participants was foot care. Similar to the present study, Khosravizadeh et al reported a mean score of 2.02 (95% CI: 1.05–2.98) for this component, which was lower than that for general diet.12 In the study by Amerzadeh et al, adherence to foot care was even lower, with mean (SD) scores of 1.07 (0.31) and 0.93 (0.17) for the first and second items, respectively, and 85% and 93.9% of participants reporting that they did not perform this self-care behavior at all.7
In the present study, foot care was better among older individuals and those with a longer duration of diabetes. This finding may be attributed to a higher perceived risk of diabetes-related complications in individuals with a longer disease history, as fear of complications from uncontrolled diabetes has been reported as a motivating factor for engaging in self-care behaviors.29
Although the self-care status for blood glucose testing was better than that for physical activity and foot care, the likelihood of having favorable blood glucose monitoring was less than half that of adhering to a general diet. Similarly, Khosravizadeh et al reported a low mean score for this component (1.82; 95% CI: 0.64–3.01).12 Amerzadeh et al also reported a mean score of approximately 1.97–2.06, which is comparable to the findings of the present study.7 Fear of needles has been identified as a barrier to performing this self-care behavior.28
Smoking cessation is an important component of diabetes self-care, as continued smoking increases the risk of developing diabetes-related complications. However, evidence indicates that people with diabetes are less likely to quit smoking than those without the condition.30 The difficulty of quitting in this population is partly due to characteristics of individuals with diabetes that intensify challenges during the cessation process.31 Effective smoking cessation for people with diabetes requires tailored and more intensive interventions, including close monitoring and education about the specific effects of smoking on diabetes.30,31
In this study, 77.1% of participants adhered to smoking-related self-care, meaning that 22.9% were smokers—31.3% of men and 0% of women. When compared with the age-standardized prevalence of smoking in Iran (24.4% in men and 3.8% in women),32 it appears that smoking cessation among men with diabetes has not improved in line with recommended self-care practices. This gap may reflect the absence of coherent and targeted smoking cessation programs in health centers for people with diabetes.
Similar to the present study, previous studies by Khosravizadeh et al, Tol et al, and Amerzadeh et al reported diet adherence as the best-performing self-care behavior.7,12,21 Unlike the study by Amerzadeh et al, in the present study, adherence to a specific diet—defined as avoiding high-fat foods such as red meat and high-fat dairy products and consuming five or more servings of fruits and vegetables—was the strongest aspect of diet-related self-care.7 Income level was an important determinant of adherence to both general and specific diets, with higher income associated with better compliance. This association was particularly pronounced for adherence to a specific diet. In our study, the clinical relevance of education was most striking, with university-educated patients being over six times more likely to follow a general diet (OR = 6.38). This high effect size suggests that current dietary guidelines may be too complex for patients with lower literacy, highlighting a need for simplified, visual-based nutritional counseling to bridge this adherence gap.
A key limitation in self-care research is the lack of a standard for defining “desirable” overall self-care. Using the SDSCA, an average score is calculated for each component, but no universally accepted cutoff exists. In this study, a score of 3.5 or above was considered desirable. To ensure these results were not influenced by extreme data points, a sensitivity analysis was performed by excluding outliers. The results remained consistent in both magnitude and direction, confirming the robustness of our clinical conclusions. Given the chronic nature of diabetes, expecting patients to achieve all self-care behaviors at this level may be unrealistic. Accordingly, only 8.5% of participants met the threshold if all six components were required, and even with a minimum of three components, only 38.6% met the criterion. These findings indicate that overall self-care in this population is suboptimal and underscore the need for targeted interventions to improve adherence.
Beyond methodological considerations, the observed patterns of self-care behaviors can be interpreted through established behavioral frameworks. Health Belief Model (HBM) which posits that individuals’ actions are influenced by their perceived susceptibility to complications, perceived severity of the disease, perceived benefits of adherence, perceived barriers, and self-efficacy.19 In the present study, low adherence to physical activity and foot care may reflect high perceived barriers, such as workload, comorbidities, and environmental constraints, despite awareness of potential complications. Conversely, relatively better adherence to dietary recommendations and smoking cessation could be attributed to higher perceived benefits and greater self-efficacy in these domains. Framing the findings within the HBM highlights the importance of addressing both motivational and practical barriers when designing interventions to improve diabetes self-care.
From a health-system perspective, these findings highlight opportunities to enhance self-care support within routine clinical care. Primary-care teams play a critical role in supporting diabetes self-care, as integrated care with diverse expertise has been associated with improvements in glycemic control and patient health behaviors in chronic disease management.33 Self-management support embedded within primary care helps align patient priorities with personalized care plans and facilitates structured follow-up and goal setting for behavior change.34 Frameworks such as the Chronic Care Model emphasize team-based, person-centered care that incorporates ongoing self-management support as an essential element for improving diabetes outcomes.35
In the context of Iran’s primary health-care system, particularly in provinces such as Khuzestan, strengthening policy-level support for diabetes self-care is essential. Community health-worker programs could play a key role in providing ongoing education, monitoring self-care behaviors, and addressing barriers related to workload, comorbidities, and limited access to resources. In addition, low-cost digital reminder tools (eg, SMS-based follow-ups) and culturally adapted educational materials tailored to local dietary habits and environmental conditions may enhance adherence to self-care behaviors. Integrating these approaches into existing primary-care services could support more effective and sustainable diabetes self-management.
Study Strengths
One of the main strengths of the present study is the comprehensive assessment of multiple components of self-care in people with diabetes, including general and specific diet, physical activity, foot care, blood sugar testing, and smoking cessation, which provides a detailed understanding of self-care patterns. The use of a standardized and previously validated instrument, the Persian version of the Summary of Diabetes Self-Care Activities (SDSCA), enhances the reliability and comparability of the findings. Another strength is the inclusion of a relatively diverse sample in terms of age, gender, education, and income, which allows for the exploration of demographic and social determinants of self-care behaviors. Additionally, the study employed multiple robust statistical methods, including descriptive statistics, Cochran’s Q and McNemar tests for comparing adherence across components, Fisher’s exact tests for bivariate associations, and Firth multivariate logistic regression to provide stable estimates for independent predictors. Finally, the study provides valuable local data from Khuzestan Province, which can help guide targeted interventions and inform health policy for improving diabetes self-management in similar populations.
Study Limitations
This study has several methodological limitations. Self-reported data may be subject to recall and social desirability bias, potentially affecting accuracy. The cross-sectional design precludes causal inferences, and the relatively low number of participants with optimal self-care in certain components may have limited statistical power to detect associations.
The use of convenience sampling from health center attendees may restrict the generalizability of findings to other populations or regions. Seasonal and environmental factors, such as extreme temperatures in Khuzestan Province, may have further influenced behaviors like physical activity. Potential residual confounding from unmeasured psychosocial factors cannot be excluded.
A cutoff score of 3.5 was used to define “desirable” self-care; the absence of a universally accepted threshold limits comparability with other studies, and future research could consider percentile-based or standardized z-scores for more consistent benchmarking. Finally, implicit consent procedures were used, which should be acknowledged when considering ethical implications for international readers.
Conclusion
Self-care behaviors among people with diabetes in Khuzestan Province are generally suboptimal. Adherence is relatively high for specific dietary recommendations and non-smoking, but critically low for physical activity and foot care. Factors such as age, gender, income, and education influence different aspects of self-care, highlighting social and economic determinants. Targeted educational and behavioral-support interventions addressing economic and environmental barriers are urgently required to improve adherence, particularly in the weakest components.
Future research should evaluate culturally sensitive, structured programs and integrate objective measures alongside self-report tools to enhance data accuracy and provide a more comprehensive understanding of diabetes self-management in this population.
Abbreviation
SDSCA, Summary of Diabetes Self-Care Activities.
Data Sharing Statement
Data is available from the corresponding authors on reasonable request.
Acknowledgments
The research team sincerely thanks all the individuals who provided their information and the staff of the health centers in Behbahan and Susangerd counties for their valuable support and cooperation.
Author Contributions
Author Contributions All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Vice-Chancellor of Research of Abadan University of Medical Sciences as part of a research project titled “Investigation of self-care behavior and its related factors in patients with type 2 diabetes in Behbahan and Susangerd counties in 2023–2024” (Project Code: 1675).
Disclosure
The authors declare no competing interests.
References
1. Zhou B, Rayner AW, Gregg EW, et al. Worldwide trends in diabetes prevalence and treatment from 1990 to 2022: a pooled analysis of 1108 population-representative studies with 141 million participants. The Lancet. 2024;404(10467):2077–15. doi:10.1016/S0140-6736(24)02317-1
2. Duncan BB, Magliano DJ, Boyko EJ. IDF Diabetes Atlas 11th edition 2025: global prevalence and projections for 2050. Nephrology Dialysis Transplantation. 2025;41:7–9. doi:10.1093/ndt/gfaf177
3. Network GBoDC. Global Burden of Disease Study 2023 (GBD 2023) results. Available from: https://vizhub.healthdata.org/gbd-results/.
4. Institute for Health Metrics and Evaluation. Iran (Islamic Republic of) health profile; 2023. Available from: https://www.healthdata.org/research-analysis/health-by-location/profiles/iran.
5. Stokes J, Gellatly J, Bower P, et al. Implementing a national diabetes prevention programme in England: lessons learned. BMC Health Serv Res. 2019;19(1):991. doi:10.1186/s12913-019-4809-3
6. Cooper HC, Booth K, Gill G. Patients’ perspectives on diabetes health care education. Health Educ Res. 2003;18(2):191–206. doi:10.1093/her/18.2.191
7. Amerzadeh M, Shafiei Kisomi Z, Senmar M, Khatooni M, Hosseinkhani Z, Bahrami M. Self-care behaviors, medication adherence status, and associated factors among elderly individuals with type 2 diabetes. Sci Rep. 2024;14(1):19118. doi:10.1038/s41598-024-70000-w
8. Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-care activities measure: results from 7 studies and a revised scale. Diabetes Care. 2000;23(7):943–950. doi:10.2337/diacare.23.7.943
9. Jannoo Z, Mamode Khan N. Medication adherence and diabetes self-care activities among patients with type 2 diabetes mellitus. Value Health Reg Issues. 2019;18:30–35. doi:10.1016/j.vhri.2018.06.003
10. Mogre V, Johnson NA, Tzelepis F, Shaw JE, Paul C. A systematic review of adherence to diabetes self-care behaviours: evidence from low- and middle-income countries. J Adv Nurs. 2019;75(12):3374–3389. doi:10.1111/jan.14190
11. Abate TW, Dessie G, Workineh Y, et al. Non-adherence to self-care and associated factors among diabetes adult population in Ethiopian: a systemic review with meta-analysis. PLoS One. 2021;16(2):e0245862. doi:10.1371/journal.pone.0245862
12. Khosravizadeh O, Ahadinezhad B, Maleki A, Yousefy S, Momeni Z. Diabetes self-care activities among patients with type 2 diabetes: a systematic review and meta-analysis. Int J Diabetes Develop Countries. 2024;44(1):10–19. doi:10.1007/s13410-023-01214-3
13. da Rocha RB, Silva CS, Cardoso VS. Self-care in adults with type 2 diabetes mellitus: a systematic review. Curr Diabetes Rev. 2020;16(6):598–607. doi:10.2174/1573399815666190702161849
14. Amadi K, Uwakwe R, Odinka P, Ndukuba A, Muomah C, Ohaeri J. Religion, coping and outcome in out‐patients with depression or diabetes mellitus. Acta Psychiatrica Scandinavica. 2016;133(6):489–496. doi:10.1111/acps.12537
15. Mondesir FL, White K, Liese AD, McLain AC. Gender, illness-related diabetes social support, and glycemic control among middle-aged and older adults. J Gerontol Series B. 2016;71(6):1081–1088. doi:10.1093/geronb/gbv061
16. Aliarzadeh B, Greiver M, Moineddin R, et al. Association between socio-economic status and hemoglobin A1c levels in a Canadian primary care adult population without diabetes. BMC Family Pract. 2014;15:1–9. doi:10.1186/1471-2296-15-7
17. Simons RL, Lei MK, Beach SR, et al. Economic hardship and biological weathering: the epigenetics of aging in a US sample of black women. Soc Sci Med. 2016;150:192–200. doi:10.1016/j.socscimed.2015.12.001
18. Mohammadi A, Valinejadi A, Sakipour S, Hemmat M, Zarei J, Askari Majdabadi H. Improving the distribution of rural health houses using Elicitation and GIS in Khuzestan Province (the Southwest of Iran). Int J Health Policy Manag. 2018;7(4):336–344. doi:10.15171/ijhpm.2017.101
19. Lin M, Chen T, Fan G. Current status and influential factors associated with adherence to self-monitoring of blood glucose with type 2 diabetes mellitus patients in grassroots communities: a cross-sectional survey based on information-motivation-behavior skills model in China. Front Endocrinol (Lausanne). 2023;14:1111565. doi:10.3389/fendo.2023.1111565
20. Von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. The Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
21. Tol A, Shojaeezadeh D, Eslami A, et al. Evaluation of self-care practices and relative components among type 2 diabetic patients. J Educ Health Promot. 2012;1:19. doi:10.4103/2277-9531.99219
22. Maghalian M, Jafarabadi MA, Abbasalizadeh F, Mohammad-Alizadeh-Charandabi S, Ghanbari-Homaie S, Mirghafourvand M. Validation of the Persian version of the summary of diabetes self-care activities scale (SDSCA) in pregnant women with gestational diabetes mellitus using a COSMIN methodology. BMC Endocr Disord. 2025;25(1):103. doi:10.1186/s12902-025-01931-2
23. Morowatisharifabad M, Rouhani Tonekaboni N. Perceived self-efficacy in self-care behaviors among diabetic patients referring to Yazd Diabetes Research Center. J Birjand Univ Med Sci. 2008;15(4):91–99.
24. Shamsi M, Sharifirad G, Kachoyee A, Hassanzadeh A. The effect of educational program walking based on health belief model on control sugar in woman by type 2 diabetics. Iranian Journal of Endocrinology and Metabolism. 2010;11(5):490–499.
25. Ramírez-Morros A, Berenguera A, Millaruelo L, et al. Impact of gender on patient experiences of self-management in type 2 diabetes: a qualitative study. Patient Prefer Adherence. 2024;18:1885–1896. doi:10.2147/ppa.S466931
26. Patel NR, Chew-Graham C, Bundy C, Kennedy A, Blickem C, Reeves D. Illness beliefs and the sociocultural context of diabetes self-management in British South Asians: a mixed methods study. BMC Family Pract. 2015;16(1):58. doi:10.1186/s12875-015-0269-y
27. Karimy M, Koohestani HR, Araban M. The association between attitude, self-efficacy, and social support and adherence to diabetes self-care behavior. Diabetology & Metabolic Syndrome. 2018;10(1):86. doi:10.1186/s13098-018-0386-6
28. Bukhsh A, Goh BH, Zimbudzi E, et al. Type 2 diabetes patients’ perspectives, experiences, and barriers toward diabetes-related self-care: a qualitative study from Pakistan. Front Endocrinol (Lausanne). 2020;11:534873. doi:10.3389/fendo.2020.534873
29. Jonker D, Deacon E, van Rensburg E, Segal D. Illness perception of adolescents with well-controlled type 1 diabetes mellitus. Health Psychol Open. 2018;5(2):2055102918799968. doi:10.1177/2055102918799968
30. Grech J, Norman IJ, Sammut R. Exploring the smoking cessation needs of individuals with diabetes using the information-motivation-behavior skills model. Tob Prev Cessat. 2024;10(February):1–13. doi:10.18332/tpc/181366
31. López Zubizarreta M, Hernández Mezquita MÁ, Miralles García JM, Barrueco Ferrero M. Tobacco and diabetes: clinical relevance and approach to smoking cessation in diabetic smokers. Endocrinología, Diabetes y Nutrición. 2017;64(4):221–231. doi:10.1016/j.endien.2017.05.003
32. Varmaghani M, Sharifi F, Mehdipour P, et al. Prevalence of smoking among Iranian adults: findings of the National STEPs Survey 2016. Arch Iran Med. 2020;23(6):369–377. doi:10.34172/aim.2020.29
33. Li J, Xu Z, Zhou H, Li Z, Yuan B. The involvement of specialists in primary healthcare teams for managing diabetes: a systematic review and meta-analysis. BMC Primary Care. 2025;26(1):45. doi:10.1186/s12875-025-02743-y
34. Hessler DM, Fisher L, Bowyer V, et al. Self-management support for chronic disease in primary care: frequency of patient self-management problems and patient reported priorities, and alignment with ultimate behavior goal selection. BMC Family Pract. 2019;20(1):120. doi:10.1186/s12875-019-1012-x
35. Goh LH, Siah CJR, Tam WWS, Tai ES, Young DYL. Effectiveness of the chronic care model for adults with type 2 diabetes in primary care: a systematic review and meta-analysis. Syst Rev. 2022;11(1):273. doi:10.1186/s13643-022-02117-w
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.