Back to Journals » Patient Preference and Adherence » Volume 16
Adherence to Home-Based Exercise Program and Its Predictors Among Patients Treated in Physiotherapy Outpatient Department in Amhara Region Hospitals in Ethiopia: A Prospective Cross-Sectional Study
Authors Yalew ES ![]() , Melese AZ
, Melese AZ ![]() , Guadie YG
, Guadie YG ![]() , Gashaw M
, Gashaw M ![]()
Received 29 November 2021
Accepted for publication 16 February 2022
Published 26 February 2022 Volume 2022:16 Pages 561—572
DOI https://doi.org/10.2147/PPA.S346680
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Ermias Solomon Yalew, Ashenafi Zemed Melese, Yisak Girma Guadie, Moges Gashaw
Department of Physiotherapy, School of Medicine, College of Medicine and Health Sciences, University of Gondar Comprehensive Specialized Hospital, Gondar, Ethiopia
Correspondence: Ermias Solomon Yalew, Department of Physiotherapy, School of Medicine, College of Medicine and Health Sciences, University of Gondar Comprehensive Specialized Hospital, Gondar, Ethiopia, Tel +251928991466, Email [email protected]
Background: Adherence to prescribed exercise is linked to improved treatment results for physical performance and function. Failure to adhere to the home-exercise program will adversely affect the outcome of the treatment, decrease the treatment’s efficacy, and be a cause for physiotherapists to alter treatment unnecessarily. The effectiveness of physical exercise can be determined when the patient complies with exercise therapy. Hence, this study aimed to assess patient adherence to home-based exercise programs and identify the predictors that affect the adherence of patients to home-based exercise programs.
Methods: From April 1st to May 30th, 2021, a prospective multi-institution cross-sectional study was conducted at the comprehensive specialized hospitals of Gondar University, Felege Hiwot, and Tibebe Ghion. Data from 300 participants were collected through face-to-face interviews and patient medical file reviews. Binary logistic regression was done to identify predictors of patient adherence to home exercise programs with SPSS version 20. The strength of the association was represented by the adjusted odds ratio.
Results: A 95.84% (n=300) response rate with 18– 80 years age range participated in this study. Among the study participants, 35.3% (n=106) (95% CI: 29.7– 40.3) of them were found adherent to home-based exercise programs. Age (adjusted OR 3.13 (1.031– 9.507)), gender (AOR 2.67 (1.322– 6.923)), education level (AOR 4.34 (1.101– 17.070)), occupation (adjusted OR 4.89 (1.184– 20.228)), remembering exercise (adjusted OR 2.62 (1.116– 6.161)), and patient interest in exercise (adjusted OR 3.08 (1.103– 8.574)) were independent predictors of exercise adherence.
Conclusion: The proportion of adherence to home exercise programs was relatively poor. Older age, being female, uneducated, employed, and busy work status patients had a high tendency of non-adherence. Forgetfulness, perceived exercise is boring, or no interest had negative affect on their adherence.
Keywords: adherence, home-based exercise, physiotherapy, exercise, Ethiopia
Background
Exercise therapy is usually used as a treatment prescribed by physiotherapists for patients presenting with musculoskeletal, orthopedic, and neurological conditions in physiotherapy clinics.1–3 It is the main component of the rehabilitation on the inpatient and outpatient physiotherapy service. Evidence has been reported that exercise seems to be effective in reducing pain, and promoting healing and function in various conditions.4 Exercises are mostly set individually and prearranged to be done at home as home advice.5
Home-based exercise programs (HBEPs) are an essential part of treatment for various types of musculoskeletal, orthopedic, and neurological conditions and are usually planned by physiotherapists to fit the individual desires of patients.6 This eliminates the need for the patient to deal with the illness and maintains functional improvement and continuous progress.7 Performing designed exercises is considered important for achieving a positive rehabilitation result.8 However there needs to be a change in lifestyle to include regular exercise to benefit and ensure compliance.9
Adherence is defined as “An active, voluntary, collaborative involvement of the patient, in a mutually acceptable behavior, to produce a desired preventive and therapeutic result”.10 Regarding the World Health Organization (WHO) definition, adherence is
the extent to which a person’s behavior – taking medication or intervention, following a diet, and/or executing lifestyle changes, corresponds with agreed recommendations from a health care provider.11
Exercise adherence is the degree that participants follow the clinical and home elements of the physiotherapy program. The degree to which a patient adheres to HBEP is believed to be partly involved in the success of many physiotherapy programs.8,9 Adherence to prescribed exercise is linked to improved treatment results for physical performance and function.12
In contrast, patients who did not adhere to HEPs had fewer positive results.13 Home-based exercise varies greatly in the ways of delivery, intensity, types, and contents. Studies reported that insufficient compliance to home-based exercise reduces the treatment efficiency and enhances the recurrence of the conditions. In addition, non-compliance has been reported as a cause for physiotherapists to alter treatment unnecessarily by considering that they are unsuccessful.13,14
A systematic review study which included twenty-three studies reported that the pooled prevalence of patient adherence to exercise was 21%.15 The cross-sectional study done in Nigeria showed that 24.5% of patients treated in a physiotherapy outpatient department had exercise adherence.16 Various epidemiology studies showed that age, sex, educational status, pain, forgetfulness, assuming exercise as less helpful, and tiredness had association with HBEP adherence.16–18
The physiotherapist giving treatment confronted the issue of persistently doing home-based exercise programs as endorsed, which diminishes the effectiveness of the intervention and the efficacy of the treatment. The importance of HBEP adherence in physiotherapy management has been proven by various studies, and the recognition of factors or reasons for poor adherence also served as an entry point for future intervention to increase adherence. There is a lack of evidence necessary for the proper care and effective management of physiotherapy treatment in Ethiopia. So, the purpose of this study was to assess the proportion of adherence to HBEP and the predictors that affect patient adherence.
Methods and Materials
Study Design, Period, and Setting
From April 1st to May 30th, 2021, a prospective multi-institution cross-sectional study was conducted at the comprehensive specialized hospitals of Gondar University, Felege Hiwot, and Tibebe Ghion. The centers are located in Gondar city (738 kilometers away from Addis Ababa, which is the capital of the Amhara Region’s Central Gondar Zone, Northwest Ethiopia) and Bahir Dar (565 kilometers away from Addis Ababa, and the capital city of the Amhara Regional government).
The University of Gondar comprehensive specialized teaching hospital physiotherapy outpatient clinic was established in 2002 G.C. by a Netherlands collaboration and the first physiotherapy teaching center in Ethiopia. The department of physiotherapy sees 150 patients per month and contributes physiotherapy treatment and rehabilitation programs in Gondar and surrounding catchment areas. In order to address rural areas, it participates in community-based rehabilitation programs, provides health education, and gives physiotherapy treatment. Felege Hiwot comprehensive specialized hospital was established in 1963 as a district hospital and upgraded to a referral hospital in 1994. In the physiotherapy outpatient clinic, 100 patients get the service within a month. We are now providing physiotherapy services in Bahir Dar and the surrounding area. The Tsbebe Ghion comprehensive specialized teaching hospital physiotherapy outpatient clinic was established in 2018, and 50 patients get the service within a month.
Source Population, Study Population, and Inclusion and Exclusion Criteria
Adult patients who are treated and had HBEP in an outpatient physiotherapy department were the study’s source population. All adult patients who are treated and had HBEP in outpatient physiotherapy at Gondar and Bahir Dar comprehensive specialized hospitals during the data collection period were the study population. All adult patients who had at least 1 week follow up in an outpatient physiotherapy department were included in this study.16 Whereas patients who were on physiotherapy treatment for less than 1 week and individuals with memory, comprehension, or communication deficiencies, as well as those with recognized psychological issues, were excluded from the study.
Sample Size Determination and Sampling Procedure
Based on assumptions of the single population proportion formula a sample size was calculated; 95% confidence interval, 0.245 prevalence which was a previous study done in adherence to HEP in Nigeria,16 5% precision, 10% non-response, and contingencies. The sample size was estimated as follows:
n=(za/2)2p(1–p)/d2
n=(1.96)2×(0.245)×(0.755)/(0.05)2=284.2
n=284.2 for the precision considering 10% expected contingency and the final sample size is 313.
Systematic random sampling was employed to enumerate the study subjects. Study participants were selected from three comprehensive specialized hospitals in northwest Ethiopia. To ensure representativeness, first proportional allocation of the participant was done for each comprehensive specialized hospital: 156, 104, and 53 participants were selected from UOGCSH, FHCSH, and TGCSH then “K” was calculated to be 2 (N=averagely expected number of patients come to hospital per two months of 600, n=313; K=600/313=2). Lottery method is used to draw the 1st sample of the first 2 samples and continues with every Kth interval for each outpatient physiotherapy department.
Operational Definitions
The patient adherence of the study participants was assessed by self-reported adherence to an HBEP questionnaire which is a four-point Likert scale in which the categories “Always” received a 100% rating, “Often” received a 66% rating, “Rarely” received a 33% rating, and “Never” received a 0% rating. Each participant’s total score for the four responses was calculated and divided by four to get the average and the result interpreted as adherence and non-adherence.16 Adherence: those who score 70–100% points categorized as adherent. Non-adherence: below 69% score is non-adherent.16 The pain was assessed by yes/no question if the participant answered “yes” and the intensity of pain by using visual analog scale (VAS); 0=no pain, 1–3=mild pain, 4–6=moderate, 7–10=intense pain.19 Study participants who were scored mean and above the mean in a five-point Likert scale of the person-centered therapeutic relationship in physiotherapy scale were categorized as they have high relationship and those who were scored below the mean categorized as they have low relationship with the therapist.20
Data Collection Instrument
An interviewer-administered questionnaire was utilized to assess the patients’ background information, which included a socio-demographic and socioeconomic questionnaire. Questionnaires were adapted from previously published articles with similar methodology.9,16,21,22 The questionnaire had three major components which are socio-demographic, adherence related, and clinical characteristics of the study participants (Additional File 1).
Patient–practitioner relationships were assessed by using a fifteen-item person-centered therapeutic relationship in physiotherapy scale questionnaire to identify high level of relation and low level.20 The questionnaire was first written in English by language experts and authors at the University of Gondar, who double-checked the questions for consistency. Language experts translated the English version of the questionnaire into the local language (Amharic) and then back into English. The differences between the original and translated questionnaires were compared, and the discrepancies were assessed and corrected as needed.
Face-to-face interviews and a review of patient records were used to collect the data. Three senior physiotherapists were in charge of data collection. The principal investigator (ESY) gave the data collectors a two-day intensive training on how to approach study participants, how to use the questionnaire and guideline, and data collection methodologies. The investigators kept a careful eye on the data collection procedure and checked the obtained questionnaire on a daily basis for accuracy, completeness, and consistency.
Data Analysis Procedure
Epi-data version 4.6.0.4 was used to code and enter the data, which were then exported to SPSS for Windows version 20. Data cleaning were done and missing values were checked with manually by investigators. Descriptive statistics were used to explain demographic data. Binary logistic regression was used to examine the relationships between dependent and independent variables. To control the effects of potential confounders, independent variables with p-values <0.2 in univariable analysis were exported to multivariable logistic regression analysis.
The significance of associations was computed with a P value <0.05, with adjusted odds ratio (AOR) of 95% confidence interval (CI). To check the model fitting the Hosmer–Lemeshow goodness of fit test was checked which was a P-value of >0.05.
Results
Socio-Demographic Characteristics of Participants
A 95.84% (n=300) response rate with 18–80 years age range participated in this study and it is beyond the power calculated sample size (n=284). Non-response was due to a lack of time, inadequate data, and a reluctance to participate. Among participants, more than half, 170 (56.7%), of the participants were males and the median age of the participants was 35 years with an interquartile range (IQR) of 28 to 47 years. More than one third (36.3%) of the participants were completed college and above education. Nearly two thirds (72.3%) of the participants were urban dwellers. Table 1 shows the socio-demographic characteristics of the participants.
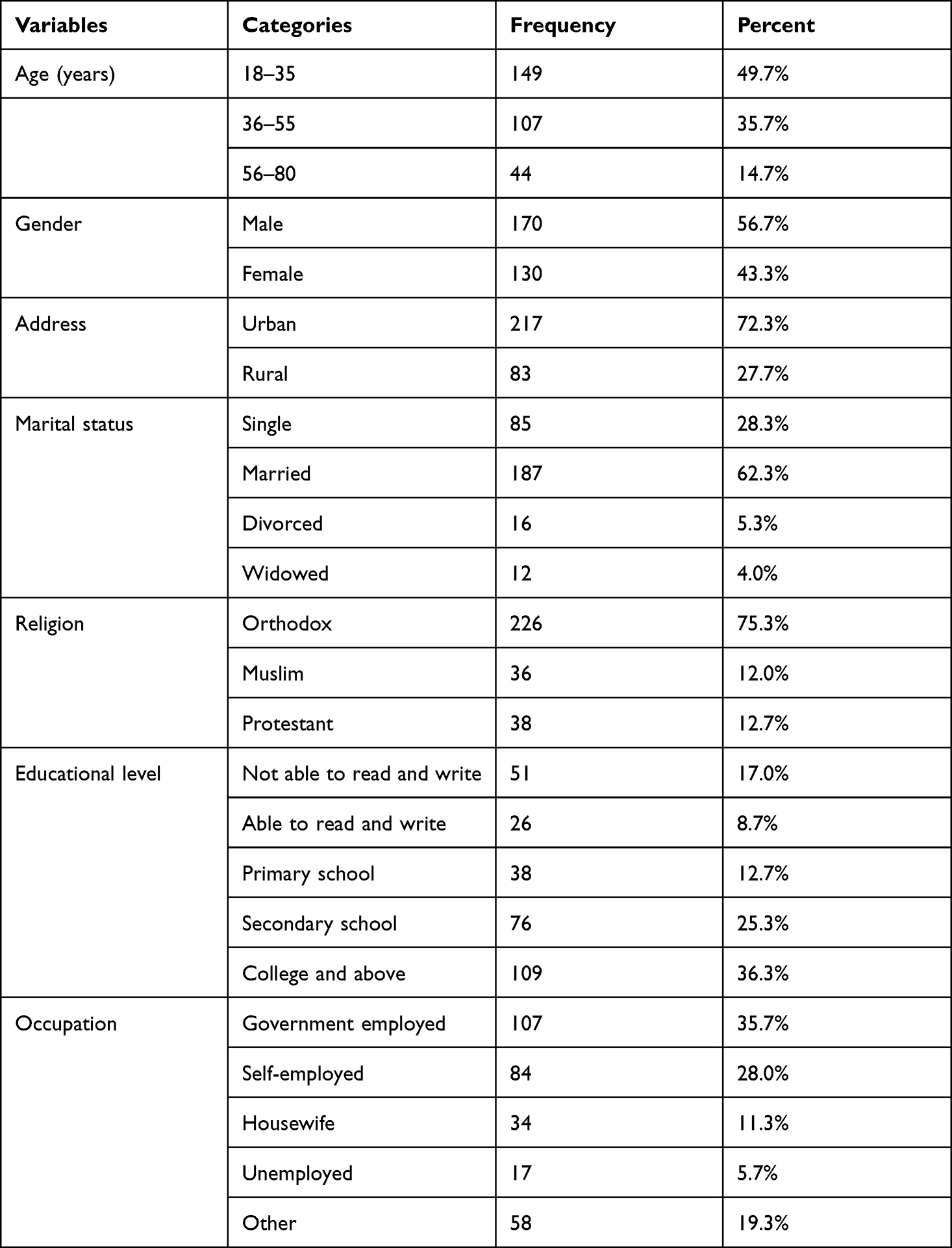 |
Table 1 Socio-Demographic Characteristics of Patients in Outpatient Physiotherapy Department at Amhara Region Hospitals, Ethiopia, 2021 (n=300) |
Patient Perceived Behavioral Characteristics of Participants
More than half (54.3%) of the participants felt tired while doing exercise and also 80 (26.7%) participants forgot their home-based exercise program (HBEP). Three quarters of the participants, 232 (77.3%), were encouraged by their family or friends during HBEP and 230 (76.7%) of the participants had interest to do exercises. Almost all, 279 (93%), of the participants believed that home-based exercise program is useful and nearly three quarters, 213 (72.7%), of the participants needed physiotherapy supervision while doing HBEP (Table 2).
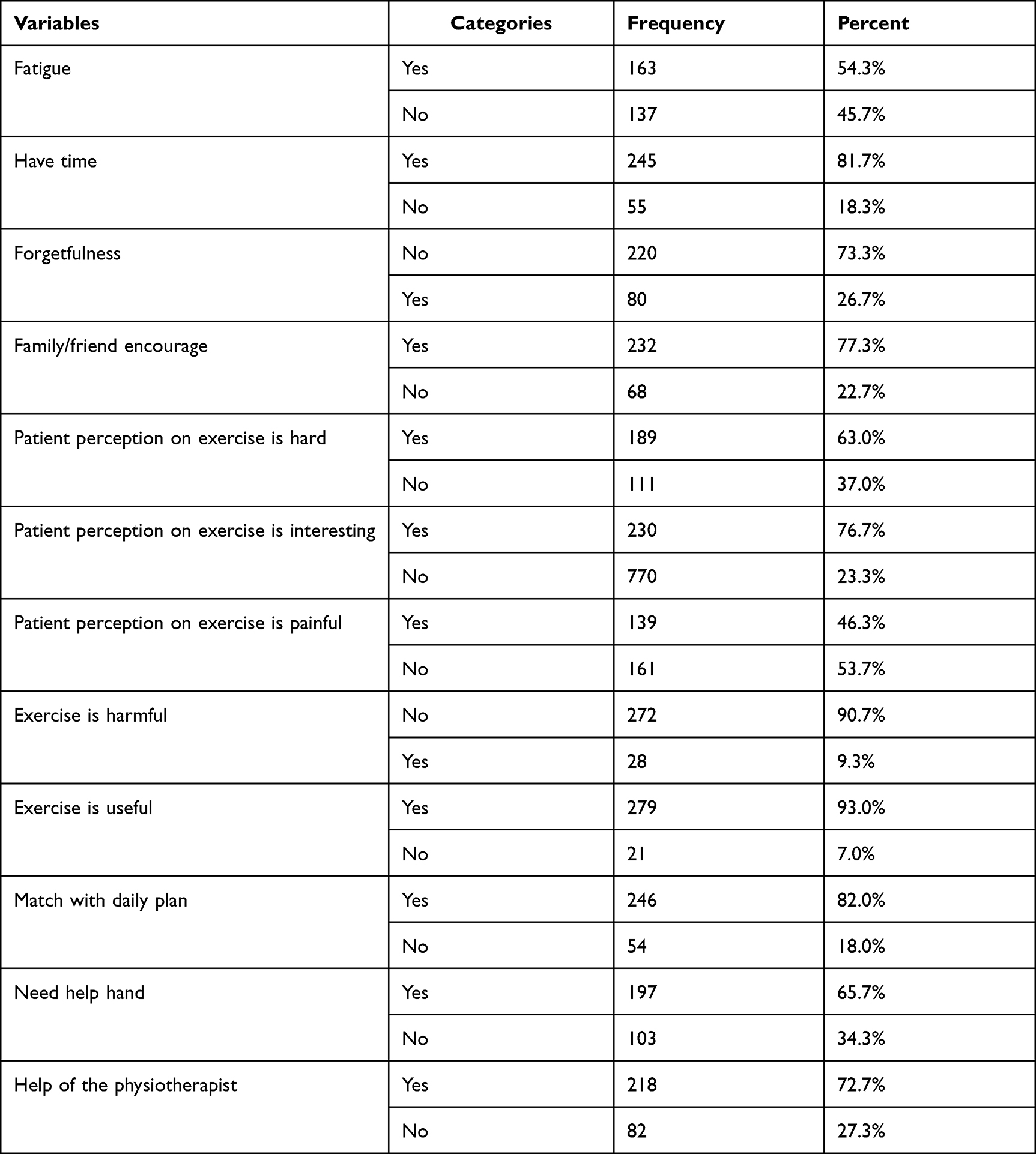 |
Table 2 Patient Perceived Behavioral Characteristics of Patients in Outpatient Physiotherapy Department at Amhara Region Hospitals, Ethiopia, 2021 (n=300) |
Clinical Characteristics of the Participants
Nearly half, 139 (46.3%), of the participants had musculoskeletal condition, and 232 (77.3%) of the participants experienced pain and among them 120 (51.7%) of the patients had moderate pain. Nearly half, 136 (45.3%), of the participants were treated 2–3 weeks in physiotherapy outpatient department. Seventy-six (25.3%) had other medical condition, among them hypertension was 23 (37.7%) and DM was 21 (34.4%).
The relationship of the patient and physiotherapist in the physiotherapy outpatient department was assessed by using a fifteen-item person-centered therapeutic relationship in physiotherapy scale questionnaire and the majority (65.70%) of the participants had a good relation with the physiotherapist (Table 3).
 |
Table 3 Clinical Characteristics of Patients in Outpatient Physiotherapy Department at Amhara Region Hospitals, Ethiopia, 2021 (n=300) |
Proportion of Adherence to Home-Based Exercise Program
The proportion of adherence among patients treated in the physiotherapy outpatient department was 106 (35.3%) (95% CI: 29.7–40.3). The highest home-based exercise program adherence was reported in those patients who perceived that exercise is useful and exercise is not harm.
Factors Associated with Adherence to Home-Based Exercise Program
A binary logistic regression analysis was done to each identified variable that is significantly associated with the proportion of adherence to HBEP of the independent variables. Age, gender, address, education level, occupation, fatigue, have time, forgetfulness, exercise is hard, exercise is interest, exercise is painful, exercise harmful, exercise is useful, matching with daily plan, need help hand (physical assistance), and patient–physiotherapy relationship was significantly associated with adherence to HBEP at P-value <0.2 in the bi-variable logistic regression. Those variables were moved into the multivariable logistic regression and further analyzed to adjust for potential confounders and to identify predictors of adherence to HBEP. In multivariable logistic regression analysis, age, gender, education level, occupation, forgetfulness, and exercise is interesting were variables significantly associated with adherence to HBEP.
Patients who were at the age ranged between 18–35 years have 3.13 higher adherence to HBEP compared with the age ranged between 56–80 years (AOR: 3.13 (1.031–9.507)). The odds of being adherent to HBEP for male patients were 2.11 times more than female (AOR: 2.67 (1.322–5.395)). Patients having educational level in primary school were 4.34 more adherence to HBEP than not able to write and read (AOR: 4.34 (1.101–17.070)) and the participants who were housewife were 4.89 times higher than other (AOR: 4.89 (1.184–20.228)).
The odds of being adherent to HBEP for the patients who had remembered home-based exercise program were 2.62 times higher than the patients who had not remembered their home-based exercise program (AOR: 2.62 (1.116–6.161)). Patients who were interested in exercise have 3.08 higher adherence to HBEP than not interested in exercise (AOR: 3.08 (1.103–8.574)) (Table 4).
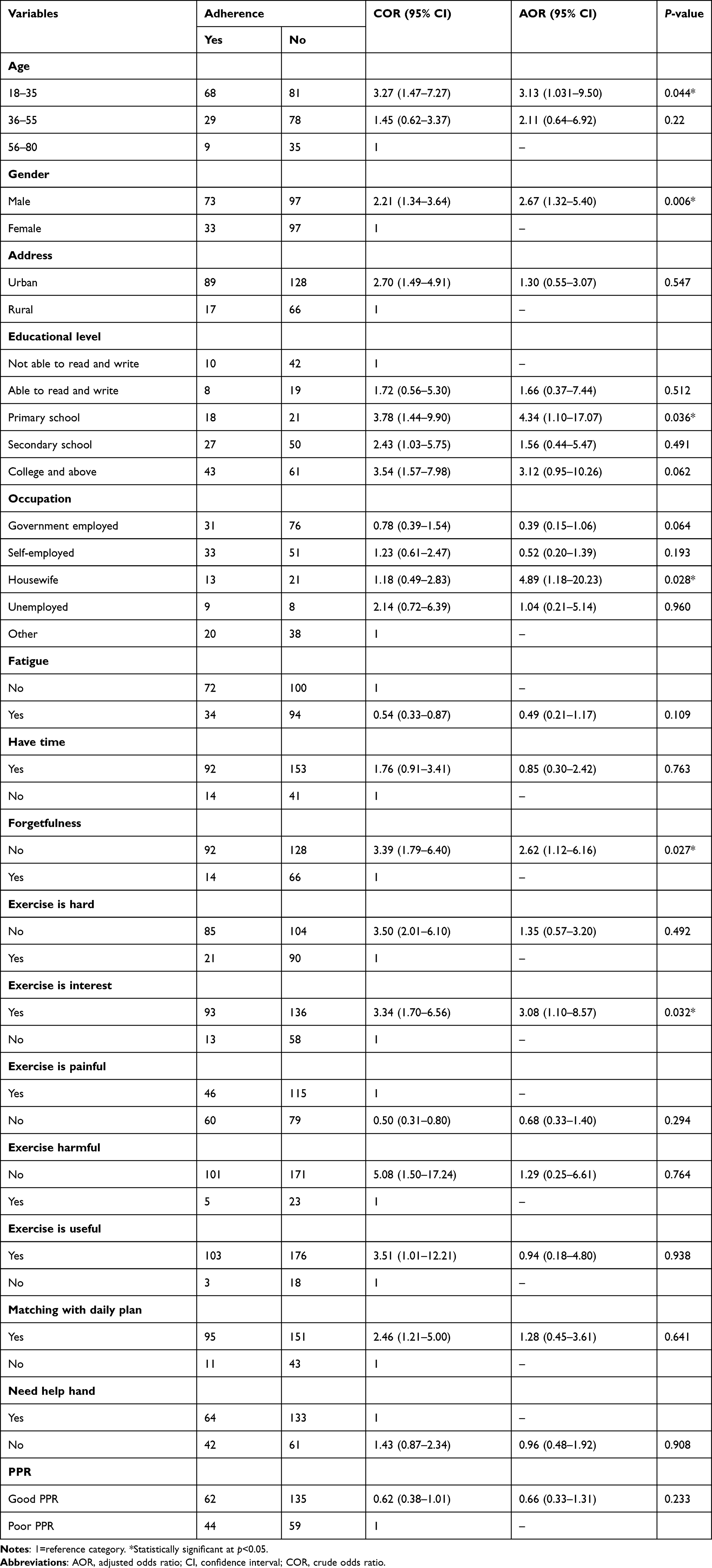 |
Table 4 Bi-Variable and Multivariable Logistic Regression Analysis on Factors Associated with Adherence to Home-Based Exercise Program Among Patients at Amhara Region Hospitals, Ethiopia, 2021 (n=300) |
Discussion
The aim of this study was to find the proportion of adherence to home-based exercise programs and its associated factors among patients treated in the physiotherapy outpatient department at Amhara regional comprehensive specialized hospitals. The overall magnitude of adherence to HBEP in physiotherapy outpatient departments was 35.3% (95% CI: 29.7–40.3). In this study, the higher adherence was reported by those participants aged 18–35 years old, who were male study participants. This could be because the frequencies of male and adult participants were higher than female and older adult participants. The magnitude of patient adherence to home-based exercise was considerably poor in the study setting. Age, gender, education level, occupation, forgetfulness, and patient interest in exercise were variables significantly associated with adherence to HBEP.
The magnitude of patient adherence to HBEP was found to be 35.3% in our study. The finding of this study is comparable with the finding of the study done by the Netherlands Institute of Primary Health Care of 35%;22 39% in general physical therapy of Hacettepe University Hospital, Ankara, Turkey;23 and 37.6% in outpatient physiotherapy clinics in Lagos State South West, Nigeria.24
In contrast, the proportion of HBEP adherence is larger than the findings from studies conducted in Nigeria: 24.5% among patients getting outpatient physiotherapy services.16 This difference may be due to methodology, the Nigerian study used convenient sampling but our study used systematic random sampling and proportional allocation is incorporated; 25.9% in stroke patients go to the Outpatient Physiotherapy Clinics of two hospitals in Kano, Nigeria.18 The possible justification for this difference may be the difference in the population studied, the above study included specifically stroke patients but this study included a patient with stroke and other conditions. Furthermore the result of this study was detected at much higher magnitude than the systematic review done in Australia with 21% pooled prevalence15 and 10% in Spain among patients.7 This variation may be the study population, the Spain study included only neck and low back pain, and used a cohort study design but our study included other condition and used a cross-sectional study design.
On the contrary, the proportion seen in this study result was lower than the studies done in Canada of 50%;25 they included only low back pain, and used a repeated measure design but our study included other condition and used a cross-sectional study design. There was 63.5% in India among stroke survivors26 and also 55.8% among stroke patients.27 This difference may be due to variation in groups which both include stroke survivors and might be different study design, sample size, and sampling procedure.
The findings of this research revealed age is significantly associated with adherence, which an inclined adherence in the younger population is 3.1 times more likely to adhere to HBEPs when compared to the elder population. The studies conducted in Egypt,21 Nigeria16 and similarly, it appears that regular physical activity/exercise decreases with age.17 Male patients were approximately three times more likely to adhere to HBEPs than female. This is because, while no precise reason can be given, the higher adherence observed by men in this study could be linked to the uniqueness of Ethiopian socio-cultural concerns.28 This fit in previous studies, men engage in more physical activity than women in Nigeria,16 USA17, and Turkey23, also implied that gender significantly associated with adherence to exercise. In contrast, the studies done in Spain7 and northwest Nigeria27 are not significantly associated. This could be sample size, study area, study participants, sampling technique, and quality of data collectors.
Regarding this study, education level is significantly associated with adherence to HBEP, whilst adherence to HBEP is more among patients with better educational status, 4.3 times more adherence than not able to write and read patients. This is related to the study conducted in Nigeria.16 Conversely, the study done in USA17 reported education is not significantly associated with exercise adherence. Accordingly, another demographic factor is the occupation of the patient. This study found that being a housewife is nearly five times higher adherence to HBEP than others. This is because employed or self-employed spend more time at work and through active travel they might not have time for HBEP.29 But in another study conducted in Egypt being employed is more likely adhere to HBEP.21 This disparity could be different population, sample size, study design, or sampling procedure.
Furthermore, significant association was found among forgetfulness and adherence to HBEP (p<0.05). The odds of remembering exercise were nearly three times more adherence to HBEP than those who forget their exercise. This result is confirmed with other studies in New Zealand9 and Nigeria,16 where the authors speculate that even though forgetfulness is an unintended process, it may have been caused by the patients' impression of barriers or lack of importance attachment to the HBEP. Exercise is interesting positively affects the adherence to HBEP, patients who were interested in exercise were the odds of three times more adherent than who perceived exercise is boring. This might be that lack of desire is one of the obstacles to do exercise.30
Conclusion
The adherence to home exercise programs was relatively poor among patients treated in a physiotherapy outpatient department. Older age, being female, uneducated, employed, and patients with a busy work schedule have a higher likelihood of non-adherence and should be given special consideration. Forgetfulness, patient perception to exercise. Based on the finding of this study, the authors recommended that clear prescription of exercise with a brief explanation given for the patient by the physiotherapist is essential to improve the adherence of the patients to HBEP.
Strength and Limitation of the Study
This is the first study in the study area as well as in the country and the study was done in multi-centers to identify further hidden burden of HBEP adherence status of the patient. Even though this is the first study to determine the prevalence of HBEP adherence among patients attending physiotherapy outpatient department in Ethiopia, it has some certain limitations. The main weakness of this study is that the study’s cross-sectional design precluded a follow-up, which would have offered a better design for detecting characteristics linked to adherence. The results also relied on patients’ self-report. This might have been subject to recall bias.
Abbreviations
AOR, Adjusted odds ratio; CI, Confidence interval; COD, Crude odds ratio; Epi Info, Epidemiological Information; FHCSH, Felege Hiwot comprehensive specialized hospital; HBEP, Home-based exercise program; HRE, Home rehabilitation exercise; LBP, Lower back pain; G.C., Gregorian calendar; OPD, Outpatient department; MPT, Masters of Physiotherapy; SPSS, Statistical Package for Social Sciences; TGCSH, Tibebe Gihion comprehensive specialized hospital; UoGCSH, University of Gondar comprehensive specialized hospital; USA, United States of America; VAS, Visual analog scale; WHO, World Health Organization.
Data Sharing Statement
The manuscript contains all of the data that are important to our findings. Requests for more information about the dataset and questions about data sharing will be handled based on a fair request to [email protected].
Ethical Consideration
This research was carried out in line with the Declaration of Helsinki. Ethical approval was secured from the Ethical Review Committee of the College of Medicine and Health Sciences, University of Gondar, Ethiopia with Ref: SOM/2035/2020. An official letter of cooperation from the college of medicine and health science was given to respective comprehensive specialized hospitals. Each study participant gave informed consent after being fully told about the study’s objective, purpose, benefits, and risks. To ensure confidentiality, no personal identifiers were recorded during the data collection period. Participants’ participation in the study was voluntary, and those who were hesitant to engage or who wanted to discontinue their participation at any time were advised that they could do so without restriction.
Acknowledgments
First and foremost, we want to thank the University of Gondar for their ethical permission and financial support. We owe a debt of thanks to the data collectors, supervisors, and study participants, without whom this study would not have been feasible.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Scott JM, Nilsen TS, Gupta D, Jones LW. Exercise therapy and cardiovascular toxicity in cancer. Circulation. 2018;137(11):1176–1191. doi:10.1161/CIRCULATIONAHA.117.024671
2. Pasanen T, Tolvanen S, Heinonen A, Kujala UM. Exercise therapy for functional capacity in chronic diseases: an overview of meta-analyses of randomised controlled trials. Br J Sports Med. 2017;51(20):1459–1465. doi:10.1136/bjsports-2016-097132
3. Hayden JA, Van Tulder MW, Tomlinson G. Systematic review: strategies for using exercise therapy to improve outcomes in chronic low back pain. Ann Intern Med. 2005;142(9):776–785. doi:10.7326/0003-4819-142-9-200505030-00014
4. Mbada C, Olawuyi A, Oyewole OO, Odole AC, Ogundele AO, Fatoye F. Characteristics and determinants of community physiotherapy utilization and supply. BMC Health Serv Res. 2019;19(1):1–10. doi:10.1186/s12913-019-3994-4
5. Richardson C, Jull G, Hides J, Hodges P. Therapeutic Exercise for Spinal Segmental Stabilization in Low Back Pain. London: Churchill Livingstone; 1999.
6. Bassett SF, Prapavessis H. A test of an adherence-enhancing adjunct to physiotherapy steeped in the protection motivation theory. Physiother Theory Pract. 2011;27(5):360–372. doi:10.3109/09593985.2010.507238
7. Medina-Mirapeix F, Escolar-Reina P, Gascón-Cánovas JJ, Montilla-Herrador J, Jimeno-Serrano FJ, Collins SM. Predictive factors of adherence to frequency and duration components in home exercise programs for neck and low back pain: an observational study. BMC Musculoskelet Disord. 2009;10(1):1–9. doi:10.1186/1471-2474-10-155
8. Kolt GS, McEvoy JF. Adherence to rehabilitation in patients with low back pain. Man Ther. 2003;8(2):110–116. doi:10.1016/S1356-689X(02)00156-X
9. Bassett SF. The assessment of patient adherence to physiotherapy rehabilitation. N Z J Physiother. 2003;31(2):60–66.
10. Meichenbaum D, Turk DC. Facilitating Treatment Adherence: A Practitioner’s Guidebook. Plenum Press; 1987.
11. World Health Organization. Adherence definition; 2003 [March 20, 2021]. Available from: https://www.who.int/chp/knowledge/publications/adherence_Section1.pdf.
12. Pisters MF, Veenhof C, Schellevis FG, Twisk JW, Dekker J, De Bakker DH. Exercise adherence improving long‐term patient outcome in patients with osteoarthritis of the hip and/or knee. Arthritis Care Res. 2010;62(8):1087–1094. doi:10.1002/acr.20182
13. Wright BJ, Galtieri NJ, Fell M. Non-adherence to prescribed home rehabilitation exercises for musculoskeletal injuries: the role of the patient-practitioner relationship. J Rehabil Med. 2014;46(2):153–158. doi:10.2340/16501977-1241
14. Turk DC, Rudy TE. Neglected topics in the treatment of chronic pain patients—relapse, noncompliance, and adherence enhancement. Pain. 1991;44(1):5–28. doi:10.1016/0304-3959(91)90142-K
15. Simek EM, McPhate L, Haines TP. Adherence to and efficacy of home exercise programs to prevent falls: a systematic review and meta-analysis of the impact of exercise program characteristics. Prev Med. 2012;55(4):262–275. doi:10.1016/j.ypmed.2012.07.007
16. Okezue OC, Nwafor GC, Ezeukwu OA, John JN, Uchenwoke CI. Adherence to home exercise programmes and its associated factors among patients receiving physiotherapy. Clin Health Promot. 2019;9(1):7–14.
17. Caspersen CJ, Pereira MA, Curran KM. Changes in physical activity patterns in the United States, by sex and cross-sectional age. Med Sci Sports Exerc. 2000;32(9):1601–1609. doi:10.1097/00005768-200009000-00013
18. Adeniyi AF, Zandam H. Association between demographic characteristics and compliance of stroke patients to prescribed unsupervised home exercise programmes. Niger J Med Rehabil. 2009;14(1and 2):20–24.
19. Aicher B, Peil H, Peil B, Diener H. Pain measurement: visual analogue scale (VAS) and verbal rating scale (VRS) in clinical trials with OTC analgesics in headache. Cephalalgia. 2012;32(3):185–197. doi:10.1177/03331024111430856
20. Rodríguez-Nogueira Ó, Morera Balaguer J, Nogueira López A, et al. The psychometric properties of the person-centered therapeutic relationship in physiotherapy scale. PLoS One. 2020;15(11):e0241010. doi:10.1371/journal.pone.0241010
21. El-Sakhy NM. Barriers of adherence to physiotherapy treatment among geriatric patients in Matrouh, Egypt. Int J Novel Res Healthcare Nurs. 2020;7(2):280–292.
22. Sluijs EM, Kok GJ, Van der Zee J. Correlates of exercise compliance in physical therapy. Phys Ther. 1993;73(11):771–782. doi:10.1093/ptj/73.11.771
23. Chan D, Can F. Patients’ adherence/compliance to physical therapy home exercises. Fiz Rehabil. 2010;21(3):132–139.
24. Odebiyi D, Fapojuwo O, Olaleye B, Olaniyan A. Correlates of non-adherence to home exercise programmes in patients with low back pain. Int J Res. 2020;8(6):280–292. doi:10.29121/granthaalayah.v8.i6.2020.443
25. L’Heureux J, Coutu M-F, Berbiche D, Larivière C. Adherence to a home exercise programme following a clinical programme for non-acute non-specific low back pain: an exploratory study. Eur J Physiother. 2020;22(5):299–308. doi:10.1080/21679169.2019.1617777
26. Babbar P, Kumar KV, Joshua PA, Chakrapani M, Misri Z. Adherence to home-based neuro-rehabilitation exercise program in stroke survivors. Bangladesh J Med Sci. 2021;20(1):145–153. doi:10.3329/bjms.v20i1.50361
27. Ogwumike OO, Badaru UM, Adeniyi AF. Factors influencing adherence to home-based exercise by stroke survivors in North Western Nigeria. Int J Ther Rehabil Res. 2014;3(1):1. doi:10.5455/ijtrr.00000023
28. Zeleke Negera G, Charles Epiphanio D. Prevalence and predictors of nonadherence to diet and physical activity recommendations among type 2 diabetes patients in Southwest Ethiopia: a cross-sectional study. Int J Endocrinol. 2020;2020:1–8. doi:10.1155/2020/1512376
29. Barr AL, Partap U, Young EH, et al. Sociodemographic inequities associated with participation in leisure-time physical activity in sub-Saharan Africa: an individual participant data meta-analysis. BMC Public Health. 2020;20(1):1–13. doi:10.1186/s12889-020-08987-w
30. Damush TM, Plue L, Bakas T, Schmid A, Williams LS. Barriers and facilitators to exercise among stroke survivors. Rehabil Nurs. 2007;32(6):253–262. doi:10.1002/j.2048-7940.2007.tb00183.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.