Back to Journals » Integrated Pharmacy Research and Practice » Volume 12
Adherence to Good Pharmacy Practices by Community Pharmacies in Lebanon and Opportunities for Quality Improvement: It is Time to Act
Authors Bou-Saba A, Kassak KM, Salameh P ![]()
Received 18 July 2022
Accepted for publication 13 January 2023
Published 27 January 2023 Volume 2023:12 Pages 25—35
DOI https://doi.org/10.2147/IPRP.S377635
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jonathan Ling
Alein Bou-Saba,1,2 Kassem M Kassak,2 Pascale Salameh3– 6
1Doctoral School of Science and Technology, Lebanese University, Hadat, Lebanon; 2Faculty of Health Sciences, American University of Beirut, Beirut, Lebanon; 3School of Medicine, Lebanese American University, Byblos, Lebanon; 4Institut National de Santé Publique d’Épidémiologie Clinique et de Toxicologie-Liban (INSPECT-LB), Beirut, Lebanon; 5Department of Primary Care and Population Health, University of Nicosia Medical School, Nicosia, 2417, Cyprus; 6Faculty of Pharmacy, Lebanese University, Hadat, Lebanon
Correspondence: Alein Bou-Saba, Doctoral School of Science and Technology, Lebanese University, Hadat, Lebanon, Tel +961 70980978, Email [email protected]
Purpose: Good pharmacy practice is an important standard that highlight the quality of services in community pharmacies. In 2018, The Order of Pharmacists in Lebanon (OPL) published their own good pharmacy practices (GPP) guidelines. The need exists for investigational studies to assess GPP implementation status and the professional conduct of on-site staff towards these standards.
Methods: Data collection was carried out between February and August 2020 using a questionnaire covering: Socio-demographic variables; Indicator A (Attitude of the Community Pharmacists); Indicator B (Services and Facilities); Indicator C (Dispensing); Indicator D (Storage). Data analysis were performed on SPSS version 25, T-Test and ANOVA were used. A significant p value of < 0.001, 95% confidence interval and variables with missing data counting less than 10% were considered.
Results: A total of 211 staffers from pharmacies were enrolled in the study, each representing one community pharmacy. The mean percent of adherence to GPP standards by community pharmacies in the South of Lebanon was below the recommended threshold of 75%. Only 65.09% adhered to all tested indicators (27% to Indicator A, 56.91% to Indicator B, 68.61% to Indicator C, 66.31% to Indicator D). Higher indicators were seen among providers who were aware of OPL standards (OR = 4.021), female (OR= 2.011) and being a licensed pharmacist (OR=3.506). Cronbach alpha of the overall score was 0.615.
Conclusion: Further steps shall be taken to improve the compliance to GPP standards. Steps shall include, identification of the core standards, such as dispensing, provision of adequate information, monitoring of storage conditions, and ensuring the presence of a licensed pharmacist. It is highly recommended that the OPL and the Ministry of Public Health develop a “Self-assessment tool” and an efficient training program to increase community Pharmacists’ awareness status. Regular assessment shall be carried to monitor the progress overtime.
Keywords: community pharmacy, good pharmacy practice, indicators, Lebanon
Introduction
Good pharmacy practice is the backbone of a strong healthcare system; related standards highlight the quality of pharmaceutical services in the community and emphasize the role of the pharmacist in optimizing the patient’s health. Pharmacists play a variety of important roles, ranging from working in hospitals and developing new drugs to regulating drug marketing and promoting community health.1,2 As healthcare systems continue to face unprecedented challenges, including the growing epidemic of non-communicable diseases, there is an increasing need for healthcare services to respond to rapid changes, including new technological developments, complex healthcare needs and financial constraints, as well as more specific challenges like an imminent health workforce crisis and increasingly comprehensive standards of practice.3,4
Furthermore, in all healthcare settings, pharmacists are increasingly being asked to play a vital role in maintaining and promoting public health,5 causing community pharmacists to place a higher emphasis on raising awareness on different healthcare issues and subjects, allow effective communication with patients, as well as enhancing health education practices offered to the general public.6 Furthermore, the current COVID-19 pandemic has driven community pharmacists to prioritize their role in disease prevention and treatment, particularly in developed countries.7 In low- and middle-income countries (LMICs), community pharmacies are also a valuable source of health advice and information.8–10
In 2011, the International Pharmaceutical Federation (FIP) and the World Health Organization (WHO) published a document entitled “Good Pharmacy Practice (GPP)”.11 However, there remains a great amount of variance in the quality of services provided by different community pharmacies, even within the same geographical area.12,13
In 2018, GPP guidelines were developed and published by the Order of Pharmacists of Lebanon (OPL). The latter is the main association in Lebanon that manage the profession of pharmacy and that Lebanese pharmacists have to register in before practicing the profession.14–16 The guidelines covered 15 aspects of pharmacy care. However, specific laws to regulate and enforce the implementation of these guidelines are not yet generated by the Ministry of Public Health (MOPH).17 The analysis of literature reported that pharmacists are dispensing prescription medication without a prescription and a low compliance to GPP standards was described by the OPL, through a pilot work published by Badro et al in 2019. Consequently, the objective of this study was to track the improvement process two years after the issuing of standards. Data collection was performed by a third party, and additional variables were addressed to assess awareness and compliance status towards GPP standards within community pharmacies in the South of Lebanon.
Methods
Participants
Data collection was carried out between February and August 2020 across 211 different pharmacies in South Lebanon constituting approximately 33% of the total number of pharmacies in the region (Figure 1). These pharmacies were randomly selected and consequently they were informed about the objective of the study. Data collection was conducted by a face-to-face interview while respecting Covid-19 safety precautions. Only one pharmacy staff was approached, regardless of his/her status (owner, employed pharmacist, or pharmacy technician). Whenever a patient went in the pharmacy, the data collector waited the pharmacist to finish his job until to continue the survey.
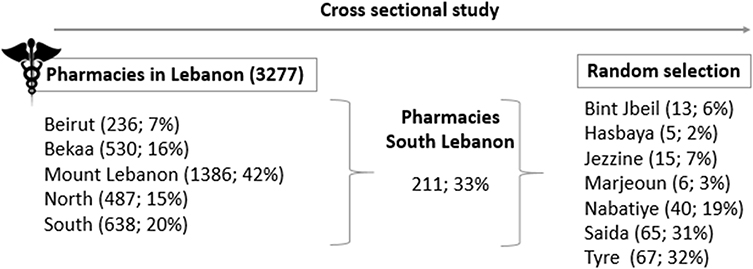 |
Figure 1 Distribution of pharmacies in Lebanon and sampling zone. |
Eligibility Criteria
Community pharmacies located in South of Lebanon were included. Respondents unwilling to participate during the data collection period were excluded from the study.
Ethical Consideration
The study was approved by the American University of Beirut – Human research protection program and Institutional Review Board, reference number (SBS-2020-0330). A written informed consent form was obtained from participants.
Data Management
Data were analyzed on SPSS version 25. For the association of variables, T-test and ANOVA were used. For the association of overall high score indicator with sex, specialty and awareness of published GPP standards a binary logistic regression was performed. P value less than 0.05 was considered significant.
GPP adherence scores were calculated for each indicator and extracted by summing the scores of the items for Indicators B, C and D. Indicator A was presented as descriptive data. For positive dichotomous variables, answers of NO are represented as zero (0) and answers of YES are represented as one (1). For negative dichotomous variables, this was reversed (ie: zero (0) for YES and one (1) for NO. The overall score was calculated as the sum of all sub-score items. Reliability of the scales was assessed by Cronbach’s alpha for Indicators B, C and D (0.586; 0.745; 0.547 respectively). For every Indicator, the participant had to demonstrate appropriate answers on more than 75% of items to be considered adherent to the GPP guidlines.11
Results
Sample Description
Of the 211 participants, most were females (57.3%), with a mean age of 35.77 ± 10.39. 61.1% held a Bachelor of Science in pharmacy (BS), while 16.6% were assistants and technicians. The highest proportion was from Tyre and Saida areas (31.8% and 30.8% respectively). Most of the respondents have more than 6 years of experience (~55%). Only 21.8% have less than 3 years of experience. Most were full-time employees, with 71.5% of them working more than 41 hours/week. Half were pharmacy owners and 32.2% were staff pharmacists. 12.3% of the respondents preferred not to reveal their family income per month. The average family size was 2.7 ±1.54 members in the same house. Approximately 50% of the pharmacies served at least 50 to 100 patients per day and more, while 34.1% had less than 50 patients per day (Table 1).
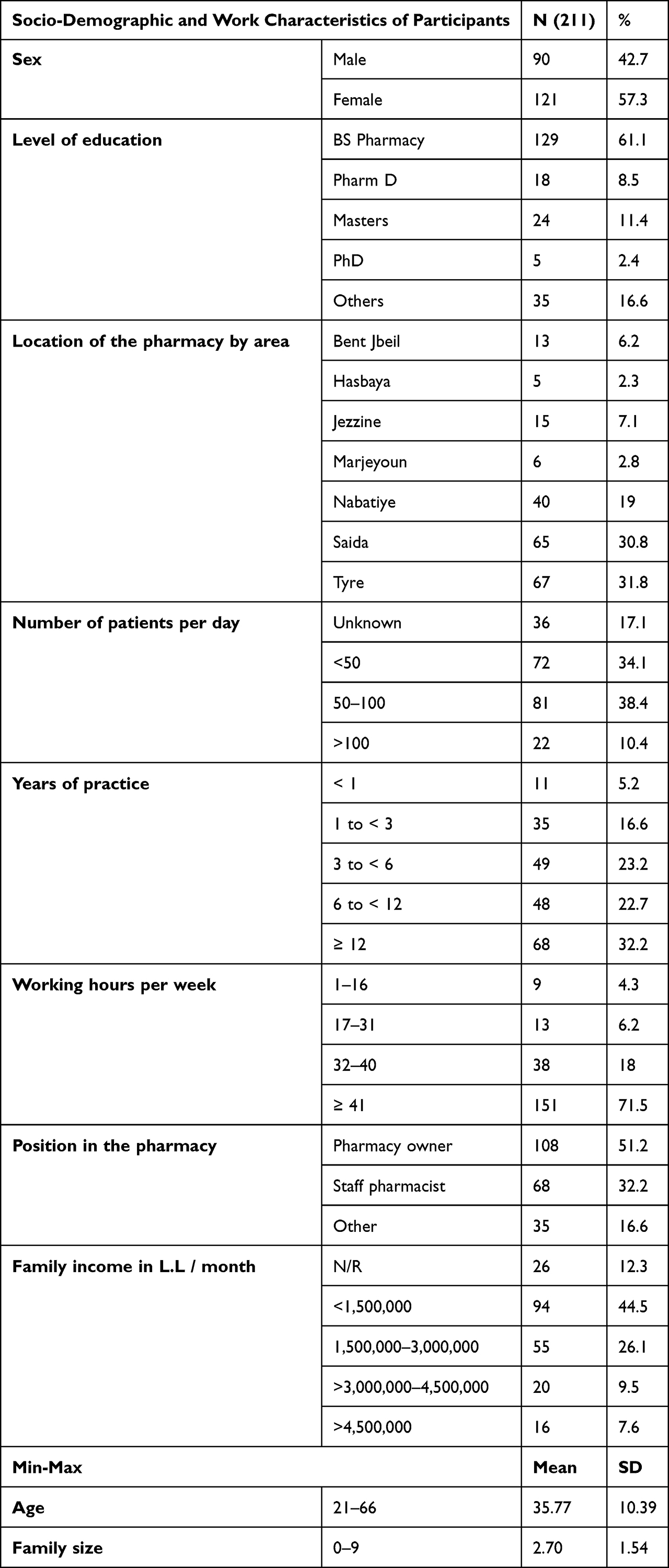 |
Table 1 Distribution of Socio-Demographic and Work Characteristics of Participants |
GPP Adherence Results
General Awareness to GPP
Only 27% of respondents were aware of the GPP standards published by the OPL. Of those, 91% agreed that the standards can be easily implemented in Lebanon (Figure 2).
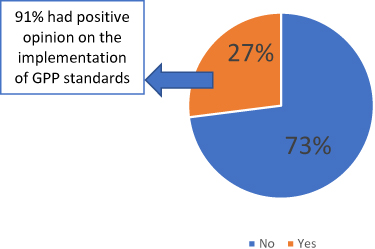 |
Figure 2 Percentage of awareness regarding the published GPP standards - Indicator A. |
Services and Facilities
The total working hours per week came to a mean of 49 ± 21.58 for the pharmacy owners and 40.85 ± 15.83 hours for other participants respectively. Owners also typically had twice the years of experience (14.03 ± 9.41) when compared to other participants (7.33 ±7.02) (Table S1).
Only 61.6% of the pharmacies had a licensed pharmacist present during all opening hours. 41.2% had a suitable space to discuss confidential information, and just 3.3% were engaged in raising awareness of community health issues, although 72% did offer information for patients (Table S2); leaflets were the most common source of information available for patients’ use in the pharmacies (59.7%) (Table S3). Height and weight measuring services were commonplace (73% and 86.3% respectively), as were options for in-pharmacy blood testing (glucose 90.5% vs cholesterol testing 2.4%), blood pressure testing (95.7%), pregnancy tests (95.3%), vaccination (88.2%), eyeglasses (41.7%) and the provision of basic comfort services like seating, drinking water and toilets for customers was startlingly low (50.2%, 0.5% and 2.4% respectively).
Dispensing Medication
While the mean percentage of patients that engage counseling time with the pharmacist was 51.61 ± 24.29, the average time per minute spent on counseling each patient was 5.98 ± 3.72. The average number of prescriptions dispensed per day was 22.71 ± 20.97, with the mean percentage of prescriptions containing mistakes being 13.62 ± 18.03 (Table S4).
The majority of drugs dispensed without prescriptions (99.1%) were Vitamins and supplements (95.3%), cosmetic preparation (90%), topical medication (81.5%), NSAIDS (89.6), antibiotics (68.7%) and gastrointestinal and endocrine medications (60.7%). Almost all the pharmacies practiced generic substitution (95.3%) and explain to the patients the purpose of the substitution and provide information to support adherence to treatment (94.8%). 87.2% provide information to reduce antimicrobial resistance (Table S5).
Regarding consultations for atypical responses to a medicine or a treatment, 94.8% acknowledged that they face such cases and 87.7% reported referring them to their doctors, while 37.9% stopped the medication and 20.4% intervened directly. 33.6% of the pharmacies did perform point-of-care testing to adjust patient therapy when needed, but few had databases on patients’ therapeutic outcomes or medication (10.4%). Most of the information resources that were present in the pharmacies (94.3%) were for staff use, and only 26.5% of pharmacies reported providing advice for patients on how to use healthcare information resources.
Out of 142 pharmacies with a pharmacist’s assistant, 17.5% said they checked prepared medication before dispensing (8.5% for counter indications, 5.2% for dosage prescribed and 3.3% for drug interactions), and 80.6% complied with requirements for a clean preparation and dispensing area (Table S6).
Storage
While 99.5% of pharmacies reported having a stable 24-hour power supply, 10.9% do have their own electric generators on site. Contingency plans for shortages were found in 86.5% of the pharmacies, but few encouraged patients to return their expired or unwanted medicines (5.2%) and, of those, only 10.9% of the pharmacies replied that they had records for expired drugs. 88.6% had separate storage for expired drugs, but only 1.9% had procedures for the disposal of expired medicines and products. 36.5% have a pest control service, and just 0.5% knew the total number of pharmaceutical items kept in stock at the time of questioning.
For the preservation of medicines, 87.2% took measures to protect medications from direct exposure to sunlight and all of them had a cooling system in the pharmacy, typically in the form of an air-conditioned room (87.2%). 85.8% also had a heating system, such as a heat pump (61.1%) or an electric heater (25.1%). All of them had refrigerators, but only 17.7% monitored and record fridge temperatures (Table S7).
71.1% of pharmacies reported keeping uncontrolled substances inside locked cupboards or locked drawers, but only 0.9% dated open bottles and 3.8% did not have appropriate lids or caps on opened bottles or containers. Storage areas were sufficient and no products were stored on the floor in 91.9% of pharmacies, with all medicines being stored on shelves in 92.4% of cases (although shelves were labeled in only 47.9% of the pharmacies). Storage of medicines using a systematic pattern was found in 95.3% of the pharmacies, and 56.9% had storage rooms with a lock. However, 7.1% were found to be keeping medicines, products, bottles or containers on the floor (Table S8).
Overall Conformity
The mean average of Indicator B, C and D calculated scores were presented in (Table 2). Comparing to 75% conformity, a discrepancy was noted of 18.09% for Indicator B, 6.39% for Indicator C and 8.69% for Indicator D. While testing the associations of Indicators B, C and D with socio-demographic and pharmacy employees’ characteristics, it was observed that female participants had higher mean scores comparing to males (14.81 ± 2.89 vs 13.87 ± 3.24 for Indicator C and 12.99 ± 1.84 vs 12.07 ± 1.95 for Indicator D). According to the results, a significant difference was found in levels of education (p<0.001). Participants that held a Pharm D or a Master’s Degree had a higher level of adherence for Indicator B, while participants with a PhD adhered higher for Indicator C. A high adherence to all indicators was also found in instances where the participant was the owner of the pharmacy. There was a significant difference between the location of the pharmacy and the adherence to Indicators B, C and D (p <0.001), showing that implementation varied from one area to another. No difference was found with respect to years of practice, working hours per week or the number of patients per day, but participants with lower family income did display higher adherence to Indicators B and D (Table 3).
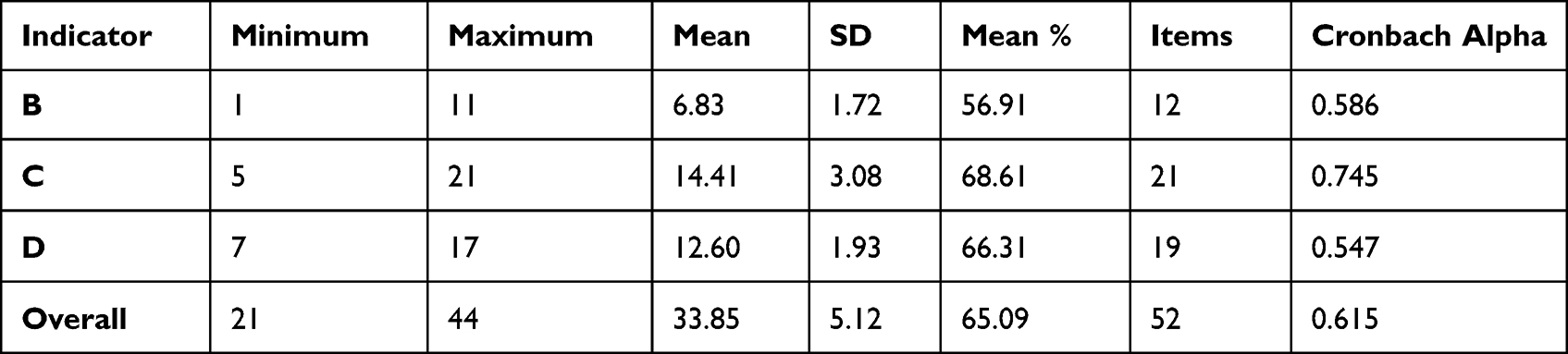 |
Table 2 Specification of Indicator B, C and D (Scores) and Their Internal Consistency Testing |
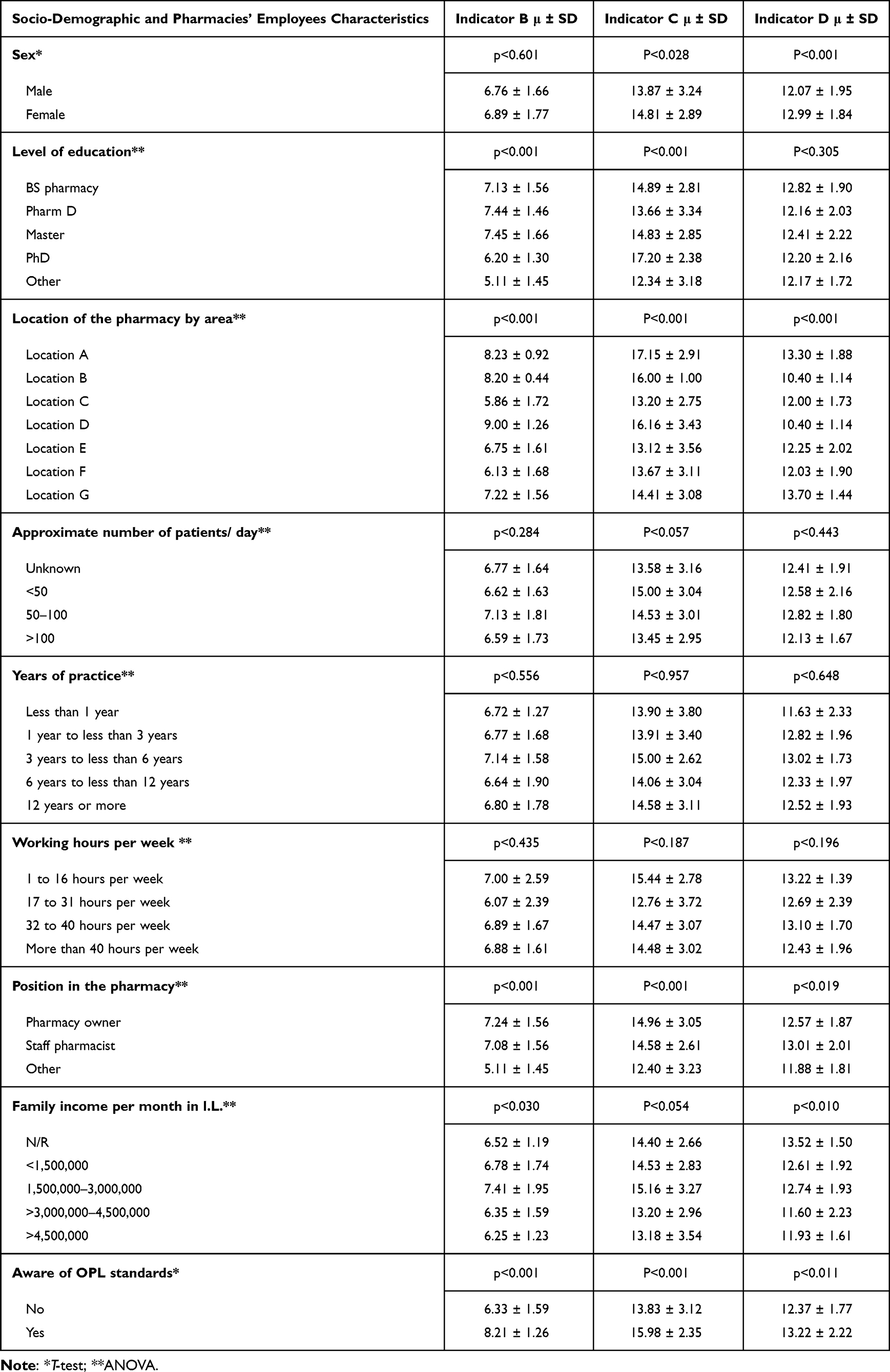 |
Table 3 Association of Indicator B, C and D with Socio-Demographic and Pharmacies’ Employees Characteristics |
Findings revealed that the level of awareness towards OPL standards was positively associated with higher scores in all indicators (Figure 3). For testing the predicting factors of higher overall score with socio-demographic characteristics a binary logistic regression was performed, those having overall higher score were found to be heavily associated with female participants, by 2 times, pharmaceutical staff by 3.5 times and awareness of OPL GPP standards by 4 folds (Table 4).
 |
Table 4 Binary Logistic Regression for the Association of Overall High Score Indicator (Model Summary Nagelkerke R Square 0.209) |
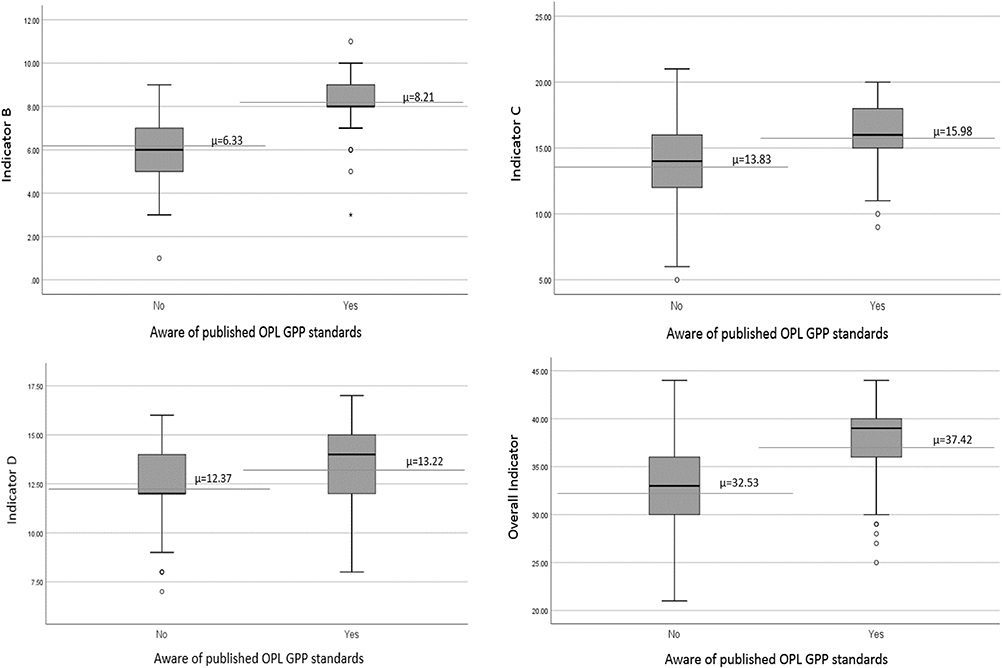 |
Figure 3 Box plot representing indicator B, C, D and overall score with level of awareness to OPL GPP standards. |
Discussion
Statement of Principal Findings
A low adherence to GPP standards was reported across South Lebanon. Very few of the participants were aware of the disseminated standards by OPL, but nevertheless responded positively regarding the feasibility of GPP implementation. The overall adherence score was below threshold level (65.09%). Women’s adherence was higher than that of men (34.70±4.85 vs 32.72±5.29); an explanation for this finding could be higher tendency of women abide by rules.
Strengths and Limitation
Because of the lengthy questionnaire, some pharmacists may have refused to participate or may have given hasty answers to questions because of that, which may increase the risk of a selection and information bias, respectively. Some of the questions might be considered as a leading, as they push respondents to answer in a specific manner and – perhaps – push them to alter their responses to match GPP standards. The study was also conducted during the COVID-19 pandemic, restricting close contact with participants due to health concerns.
A significant difference was also noted with pharmaceutical staff and those who are aware of the GPP standards, this issue has not been investigated in the similar study conducted by Badro and it could, therefore, be considered as an advantage of the present study.16
Interpretation Within the Context of the Wider Literature
Our study revealed that pharmacist dispense non-OTC drugs without any medical prescription. Compared to other studies almost same results were found in Shed et al study18 with 66.7% dispensing of antibiotics, and higher results were found in Al-Mohamadi et al, study19 in 2013, Saudi Arabia, that showed 97.9%of pharmacist handed out the antibiotic immediately 100% dispensed anti-hypertensive drugs and 89.5% gave the antipsychotic simply by following the patient’s request without even asking for a doctor’s prescription. The sale of such drugs without a medical prescription can pose adverse drug reactions and antibiotic resistance and other serious health issues as well as further investigations are recommended to ensure that appropriate and adequate assessment and counseling was undertaken before selling these drugs.
Low results were detected with regard to patient monitoring processes.In a systematic review and meta-analysis performed by Yuan et al, in 2019,20 47 studies demonstrated that community pharmacy services had positive clinical outcomes, with intervention groups displaying greater reductions in systolic BP, diastolic BP and HbA1c. Blood pressure control screenings and counseling, implemented in a generally accessible community pharmacy, was shown to help with the early detection of hypertension problems (35.6%) of the study patients were identified as having high pressure values). This lead to the initiation of more effective patient counseling by community pharmacies, resulting in earlier referral of a patient to a physician.21 It has also been shown that patient education – provided by pharmacies – helped to decrease total body weight, waist circumference and risk of weight-related complications.22 However, the importance of patient-pharmacist communication was not limited to just improving physical health; psychological improvements were also observed. In a retrospective study, medication management activities showed that 70% of patients had benefitted from pharmacy staffers delivering a community pharmacy-based mental illness and addictions program, and 20–25% of patients were receiving social support, ongoing communication and education.23
Specific focus should be given to the creation and maintenance of data bases on medication monitoring and patients’ therapeutic outcomes, an area, which was found to be severely lacking in our own.
Regarding storage, most of the low-rated elements were related to the absence of clear procedures for the disposal of expired medicines and products (98.1%). Consequently, the compliance to guidelines encouraging patients to return their expired or unwanted medicines was extremely low (5.2%). In a review by Alnahas et al, in 2020,24 studying 48 papers from 34 countries, the main issue identified was a significant lack of public awareness pertaining to the appropriate disposal of such biologically potent chemicals. Promoting medical waste disposal and implementing this culture for hospital in-patients, as well in pharmacies, should be a priority for healthcare providers, especially considering that the accumulation of pharmaceutical waste entails many ecological, economic, social and ethical concerns. For that reason, pharmacy staff should inform patients on proper pharmaceutical waste disposal and organize collection programs for unused and expired medicines. In this study, more than half of the respondents (54.5%) were unfamiliar with the concept of drug-return systems and other studies have shown that only 15.9% of patients returned expired medications to the pharmacy.24 It is also recommended to follow at least some of the different methods regarding safe disposal of unused pharmaceuticals, set in the WHO guidelines.25
Only 0.5% of our study’s participants were able to provide information on the total number of pharmaceutical items kept in stock at their pharmacies; knowing that poor stock management and expired products can have serious financial implication for pharmacies as businesses, as well as the potential risk to patient safety. It is highly recommended that pharmacies conduct stock reviews on weekly basis to check quantities and, search for expired products using software systems specifically designed report on critical threshold amounts or nearing expiration dates of stocked products.26
In addition, the vast majority (78.2%) do not monitor room storage temperatures. While in a comparable random sample of 181 community pharmacies in Riyadh 13% lacked room thermometer; 7% of the sampled pharmacies lacked refrigerator thermometers, and 33% of sample readings of the refrigerator thermometers that were in place fell outside the pre-determined accepted range.27
Concerning the protection of medicines from direct sunlight penetration, the rate of adherence (87.2%) was considerably higher in our study as compared to a study conducted in 2020, in Tripoli, Libya where approximately only (41.4%) of pharmacies reported protection from direct sunlight penetration, taking into consideration that direct penetration of sunlight leads to instability and degradation of medicines that are photosensitive.28
In our study, 16.6% of the staff working in pharmacies was not pharmacists. Therefore, it is suggested that these staffers should be regularly trained on how to act in the absence of supervision, to prevent errors and promote patient safety. In a study performed in UK, comparing the supervision in community pharmacies by pharmacists to that of other support staff, several services were found to be critical to patient safety, resulting in pharmacists being reluctant to relinquish control of those duties to the support staff, while support staff expressed reluctance to take on greater professional responsibility. While some other activities were found to be safely conducted in the absence of a pharmacist (such as the selling of general sales list medicines, the assembly of prescriptions and the provision of public health services), there was great disagreement on the safety of support staff selling pharmacy medicines and handing out checked and bagged prescription items to patients.29
Implications for Policy, Practice and Research
As learned from other countries, awareness is a well-known requirement to make changes towards better behavior and attitude and will encourage accepting more easily these practices which may lead to better results.30,31 Therefore, the first step in engaging community pharmacists is to better communicate the standards in a simple and easy manner. Particularly emphasis should also be given to the elements of prescribing and maintaining proper storage conditions, patient medication-monitoring and recalls on expired medications should be integrated into day-to-day activities, as well as the provision of appropriate information on dispensed medicine and non-OTC drugs, and adequate follow-ups with caregivers should be prioritized.
The GPP are enforced in Western countries, regular audits are conducted to ensure that the pharmacies are following the GPPs. In Lebanon, this is not done. The MOPH is required to enforce these laws and do the necessary inspections to ensure compliance and to collect data from customer’s perspective. A study conducted in Thailand revealed that assessing customer’s satisfaction towards GPP is a key requirement to ensure that customer’s needs and expectations are met since the opinion of drugstore customers may not agree with the assessment score applied by policy makers.32
Conclusions
In conclusion, very few participants were aware of the disseminated standards by the OPL; a low adherence was reported across South Lebanon. Further steps shall be taken to improve the compliance to GPP standards, thus improving the quality of pharmaceutical services and public health. Steps shall include, identification of the core GPP standards that directly influence patient safety such as dispensing process, monitoring of storage conditions, and ensuring the presence of a licensed pharmacist as long as the pharmacy is open, Proper support to improve the working conditions of pharmacists is highly recommended. An evidence-based training program should be carried out by the OPL and the Ministry of Public Health (MOPH) contextualized to the Lebanese situation and culture. It is highly recommended that the OPL be active and responsive to the enforcing of current regulations and improving them based on best practices and current knowledge and evidence. It is also recommended to develop a “GPP Self-assessment tool” to enhance the awareness status and eliminate the resistance to change, if any. These self-assessment tools shall be filled out by the community pharmacists on a yearly basis. Finally, regular assessments and monitoring of GPP performance is recommended, not only in South Lebanon, but also in all geographical areas of the country.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. The role of the pharmacist in the health care system: preparing the future pharmacist: curricular development: report of a third WHO consultative group on the role of the pharmacist, Vancouver, Canada, 27–29 August 1997 (No. WHO/PHARM/97/599). Geneva: World Health Organization; 1997. Available from: https://apps.who.int/iris/handle/10665/63817.
2. Vermeulen LC, Kolesar J, Crismon ML, et al. ASHP foundation pharmacy forecast 2018: strategic planning advice for pharmacy departments in hospitals and health systems. Am J Health Syst Pharm. 2018;75(2):23–54. doi:10.2146/sp180001
3. Bates I, John C, Bruno A, Fu P, Aliabadi S. An analysis of the global pharmacy workforce capacity. Hum Resour Health. 2016;14(1):61. doi:10.1186/s12960-016-0158-z
4. Saleem F. The need of social pharmacy: preparing future pharmacists for practice change. J Pharm Pract Community Med. 2017;3(1):01–02. doi:10.5530/jppcm.2017.1.1
5. American Society of Health-System Pharmacists. ASHP statement on the role of health-system pharmacists in public health. Am J Health Syst Pharm. 2008;65(5):462–467. doi:10.2146/ajhp070399
6. Kerr A, Strawbridge J, Kelleher C, et al. How can pharmacists develop patient-pharmacist communication skills? A realist review protocol. Syst Rev. 2017;6(1):1–7. doi:10.1186/s13643-016-0396-0
7. Zeenny RM, Dimassi A, Sacre H, et al. A cross-sectional survey on community pharmacists readiness to fight COVID-19 in a developing country: knowledge, attitude, and practice in Lebanon. J Pharm Policy Pract. 2021;14(1):1–3. doi:10.1186/s40545-021-00327-6
8. Smith F. The quality of private pharmacy services in low and middle-income countries: a systematic review. Pharm World Sci. 2009;31(3):351–361. doi:10.1007/s11096-009-9294-z
9. Brown TJ, Todd A, O’Malley C, et al. Community pharmacy-delivered interventions for public health priorities: a systematic review of interventions for alcohol reduction, smoking cessation and weight management, including meta-analysis for smoking cessation. BMJ Open. 2016;6(2):e009828. doi:10.1136/bmjopen-2015-009828
10. Hermansyah A, Pitaloka D, Sainsbury E, Krass I. Prioritising recommendations to advance community pharmacy practice. Res Social Adm Pharm. 2018;14(12):1147–1156. doi:10.1016/j.sapharm.2018.02.003
11. World Health Organization. Joint FIP/WHO guidelines on good pharmacy practice: standards for quality of pharmacy services. Geneva 2011 (No. 961). Report. Available from: https://repo.odmu.edu.ua:443/xmlui/handle/123456789/5956.
12. Azhar S, Ibrahim MI. Quality of pharmacy health services. In: Social and Administrative Aspects of Pharmacy in Low-and Middle-Income Countries. Academic Press; 2018:281–294. doi:10.1016/B978-0-12-811228-1.00018-2
13. Ranghchian M, Sehat S, Akhgari M, Mehralian G. Performance model of community pharmacies in low-middle income countries: a societal perspective. J Retail Consum Serv. 2018;40:241–248. doi:10.1016/j.jretconser.2017.10.009
14. Hallit S, Sacre H, Sarkis H, et al. Good pharmacy practice standardized for community pharmacists: the Lebanese order of pharmacists initiative. J Res Pharm Pract. 2019;8(1):29. doi:10.4103/jrpp.JRPP_18_96
15. Zeidan RK, Hallit S, Zeenny RM, Salameh P. Lebanese community-based pharmacists’ interest, practice, knowledge, and barriers towards pharmacy practice research: a cross-sectional study. Saudi Pharm J. 2019;27(4):550–557. doi:10.1016/j.jsps.2019.02.002
16. Badro DA, Sacre H, Hallit S, Amhaz A, Salameh P. Good pharmacy practice assessment among community pharmacies in Lebanon. Pharm Pract. 2020;18(1):1745. doi:10.18549/pharmpract.2020.1.1745
17. Bou-Saba A, Kassak K, Salameh P. The current trends and challenges towards good community pharmacy practice and the way forward. Explor Res Clin Soc Pharm. 2022;6:100152. doi:10.1016/j.rcsop.2022.100152
18. Shet A, Sundaresan S, Forsberg BC. Pharmacy-based dispensing of antimicrobial agents without prescription in India: appropriateness and cost burden in the private sector. Antimicrob Resist Infect Control. 2015;4(1):1–7. doi:10.1186/s13756-015-0098-8
19. Al-Mohamadi A, Badr A, Mahfouz LB, Samargandi D, Al Ahdal A. Dispensing medications without prescription at Saudi community pharmacy: extent and perception. Saudi Pharm J. 2013;21(1):13–18. doi:10.1016/j.jsps.2011.11.003
20. Yuan C, Ding Y, Zhou K, Huang Y, Xi X. Clinical outcomes of community pharmacy services: a systematic review and meta-analysis. Health Soc Care Community. 2019;27(5):e567–e587. doi:10.1111/hsc.12794
21. Waszyk-Nowaczyk M, Guzenda W, Plewka B, et al. Screening services in a community pharmacy in Poznan (Poland) to increase early detection of hypertension. J Clin Med. 2020;9(8):2572. doi:10.3390/jcm9082572
22. Moideen MM, Varghese R, Ramakrishnan P, Dhanapal CK. Patient education for overweight and obese patients on weight reduction in an urban community pharmacy and its outcome. J Pharm Biol Chem Sci. 2011;2:392–405.
23. Haslam L, Gardner D, Murphy A. A retrospective analysis of patient care activities in a community pharmacy mental illness and addictions program. Res Social Adm Pharm. 2019. doi:10.1016/j.sapharm.2019.07.003
24. Alnahas F, Yeboah P, Fliedel L, Abdin AY, Alhareth K. Expired medication: societal, regulatory and ethical aspects of a wasted opportunity. Int J Environ Res Public Health. 2020;17(3):787. doi:10.3390/ijerph17030787
25. Gray RCF, Hogerzeil HV, Prüss AM, Rushbrook P. Guideline of Safe Disposal of Unused Pharmaceuticals in and After Emergencies. Geneva, Switzerland: World Health Organization; 1999:1–31. doi:10.3390/ijerph17030787
26. Ali AK. Inventory management in pharmacy practice: a review of literature. Arch Pharm Pract. 2011;2(4):151.
27. Khojah HM, Pallos H, Tsuboi H, Yoshida N, Abou-Auda HS, Kimura K. Adherence of community pharmacies in Riyadh, Saudi Arabia, to optimal conditions for keeping and selling good-quality medicines. Pharmacol Pharm. 2013;2013. doi:10.4236/pp.2013.45061
28. Atia A, Amabrouk N. Drug storage practices in Libyan community pharmacies coinciding with the circumstances of recurrent electricity blackouts. J Hosp Clin Pharm. 2020;6(4):1–2.
29. Bradley F, Schafheutle EI, Willis SC, Noyce PR. Changes to supervision in community pharmacy: pharmacist and pharmacy support staff views. Health Soc Care Community. 2013;21(6):644–654. doi:10.1111/hsc.12053
30. Trap B, Kikule K, Vialle-Valentin C, et al. First regulatory inspections measuring adherence to good pharmacy practices in the public sector in Uganda: a cross-sectional comparison of performance between supervised and unsupervised facilities. J Pharm Policy Pract. 2016;9(1):18. doi:10.1186/s40545-016-0068-4
31. Milosavljevic A, Aspden T, Harrison J. Community pharmacist-led interventions and their impact on patients’ medication adherence and other health outcomes: a systematic review. Int J Pharm Pract. 2018;26(5):387–397. doi:10.1111/ijpp.12462
32. Yotsombut K, Parinyarux P. Customers’ satisfaction toward drugstore facilities and services based on the good pharmacy practice standard in Thailand. Pharm Pract. 2022;20(1):2601. doi:10.18549/PharmPract.2022.1.2601
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.