Back to Journals » Local and Regional Anesthesia » Volume 16
Addition of Deep Parasternal Plane Block to Enhanced Recovery Protocol for Pediatric Cardiac Surgery
Authors Ohliger S ![]() , Harb A, Al-Haddadin C, Bennett DP
, Harb A, Al-Haddadin C, Bennett DP ![]() , Frazee T, Hoffmann C
, Frazee T, Hoffmann C ![]()
Received 26 August 2022
Accepted for publication 27 January 2023
Published 16 February 2023 Volume 2023:16 Pages 11—18
DOI https://doi.org/10.2147/LRA.S387631
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Stefan Wirz
Shelley Ohliger, Alain Harb, Caroline Al-Haddadin, David P Bennett, Tiffany Frazee, Cassandra Hoffmann
Department of Anesthesiology and Perioperative Medicine, University Hospitals/Rainbow Babies and Children’s Hospital, Cleveland, OH, 44106, USA
Correspondence: Shelley Ohliger, Department of Anesthesiology and Perioperative Medicine, University Hospitals/Rainbow Babies and Children’s Hospital, 11100 Euclid Ave, Cleveland, OH, 44106, USA, Tel +1 216 844 7340, Fax +1 216 844 3780, Email [email protected]
Purpose: This study aims to evaluate if the addition of deep parasternal plane blocks to a pre-existing enhanced recovery pathway for pediatric cardiac surgery improves outcomes.
Patients and Methods: A retrospective review through an EMR query from June 2019 to June 2021 was performed for patients less than 18 years of age who underwent cardiac surgery via median sternotomy and were extubated immediately following surgery in a single academic tertiary care hospital. Patients receiving deep parasternal blocks as part of an enhanced recovery protocol were compared to similar patients from the year prior to block implementation.
Results: The primary outcome was intraoperative and postoperative opioid consumption. Secondary outcomes were pain scores, intensive care unit (ICU) length of stay and time to first oral intake. There was a statistically significant reduction in intraoperative opioid administration and pain scores in the first 24 hours post-operatively. There was also a statistically significant reduction in ICU length of stay. There was no statistically significant difference in post-operative opioid consumption and time to first oral intake.
Conclusion: Bilateral deep parasternal blocks may reduce opioid consumption, provide effective postoperative pain control, and result in decreased length of intensive care unit stay across both simple and complex pediatric cardiac procedures when added to a pre-existing enhanced recovery protocol.
Keywords: enhanced recovery after surgery, pediatric cardiac surgery, congenital heart disease, regional anesthesia, truncal blocks
Introduction
Pediatric cardiac surgery involving median sternotomy can be associated with significant postoperative pain. Poorly controlled pain following cardiac surgery has been shown to be a risk factor for increased morbidity, including severe cardiopulmonary dysfunction, hypercoagulability, and immunosuppression.1 Post-operative pain management, which provides effective analgesia, minimizes side effects and contributes to enhanced recovery after surgery, is a unique challenge in the pediatric cardiac surgery population. The ideal post-operative analgesic regimen would enable early separation from mechanical ventilation, decrease opioid consumption, and expedite discharge from the intensive care unit.
Systemic opioids and non-steroidal anti-inflammatory drugs (NSAIDs) have been the mainstay for treating pain during the perioperative period in children undergoing median sternotomy for cardiac surgery. The traditional high-dose opioid approach is associated with a decreased stress response2,3 but at the expense of prolonged mechanical ventilation, and increased opioid-related side effects. NSAIDs are effective as part of a multimodal analgesic approach, but their use can be limited due to concerns regarding coagulopathy or impairment in renal function.
Regional anesthesia is becoming increasingly popular in pediatric cardiac surgery for its opioid sparing effects. By blocking the afferent impulses from surgical sites, the need for supplemental opioids is reduced. Neuraxial catheters, while effective, are often not utilized in the setting of full heparinization and coagulopathy due to the small yet significant risk of epidural hematoma formation.4 Paravertebral blocks have similar risk and side effect profiles to neuraxial catheters and require blocks to be performed bilaterally with a posterior approach. Truncal blocks such as erector spinae plane blocks, as well as superficial and deep parasternal blocks, have been shown to provide adequate pain relief for cardiac surgery, and have been gaining popularity.5
Appropriate pain relief from a sternotomy incision can be achieved by blocking the second to sixth thoracic intercostal nerves.1 The newer ultrasound-guided deep parasternal block (previously known as transversus thoracic muscle plane (TTP) block),6 involves deposition of a local anesthetic between the internal intercostal and transversus thoracic muscles and effectively blocks the anterior branches of intercostal nerves T2-6.7 The recent American Association for Thoracic Surgery Congenital Cardiac Surgery Working Group 2021 consensus document on enhanced recovery after pediatric cardiac surgery gives mention to bilateral transversus thoracic muscle plane blocks (now deep parasternal block) as a regional anesthetic option with opioid-sparing effects but states that more data are needed to determine their efficacy.8 Here we describe the successful use of bilateral single injection deep parasternal blocks in 16 pediatric patients undergoing median sternotomy for cardiac surgery.
Materials and Methods
This was a single-center retrospective comparative study undertaken at Rainbow Babies and Children’s Hospital which is part of University Hospitals in Cleveland, Ohio. University Hospitals Institutional Review Board (IRB) approval was obtained and in accordance with the Declaration of Helsinki the ethics committee of our IRB determined that informed consent was not required due to the retrospective nature of the study and confidentiality of the data was ensured. All data collected were de-identified and stored in a password protected RedCap database to maintain anonymity and confidentiality. Our electronic medical record was retrospectively queried from June 2019 to June 2021 for patients less than 18 years of age who underwent cardiac surgery via median sternotomy and were extubated immediately following surgery. Deep parasternal blocks were instituted as part of our pediatric cardiac surgery anesthetic protocol in March 2020 for all patients that were candidates for early extubation. Our control or comparison group included patients in the year prior to implementation of the deep parasternal blocks who were extubated immediately after their procedure (Figure 1).
 |
Figure 1 Flow chart of the study. |
Patients were premedicated with oral midazolam (0.7mg/kg) or IV midazolam (0.1mg/kg) if a peripheral intravenous line (PIV) was already present. Inhalation induction was performed with incremental dosing of sevoflurane and nitrous oxide if appropriate. After PIV placement, fentanyl (1–2µg/kg) and rocuronium (1mg/kg) were administered to facilitate endotracheal intubation. If an IV was present preoperatively, patients were induced with fentanyl (1µg/kg), propofol (1–2mg/kg) and rocuronium (1mg/kg). Prior to incision bilateral deep parasternal blocks were performed. A Sonosite high frequency linear probe was used over ribs 3 and 4 in the parasagittal plane along the midclavicular line to identify the intercostal and transversus thoracic muscle (TTM) (Figure 2). A Pajunk 24G × 40mm Sonoplex needle was advanced in a caudal to cranial direction into the plane between the intercostal and TTM. Sterile saline was injected for hydro-dissection to confirm correct placement. And, 0.25% ropivacaine 0.5mL/kg + clonidine 0.5µg/kg were injected to both the right and left side in an incremental fashion (Figure 3). Blocks were performed at least 20 minutes prior to incision. During the procedure, anesthesia was maintained with sevoflurane and a dexmedetomidine infusion (0.3µg/kg/hr). As needed, bolus doses of fentanyl (1–2µg/kg) were administered when hemodynamic changes such as tachycardia and hypertension indicated painful stimulus. Acetaminophen (15mg/kg) was administered at the beginning of the case. While on cardiopulmonary bypass, isoflurane was administered via the bypass circuit and the dexmedetomidine infusion was continued. At the conclusion of surgery, ketorolac (0.5mg/kg) was administered if hemostasis was adequate. Muscle relaxation was reversed with sugammadex, and the patient was extubated when they were taking spontaneous tidal volumes of 6–8mL/kg and making purposeful movements. The dexmedetomidine infusion was continued into the post-operative period and titrated at the discretion of the intensivist. Acetaminophen (15mg/kg) and ketorolac (0.5mg/kg) were scheduled every 6 hours. Morphine (0.05mg/kg) was administered as needed for post-operative pain according to our cardiothoracic intensive care unit (CTICU) protocol. Patients were transitioned to enteral medications once tolerating oral intake.
 |
Figure 2 Deep parasternal nerve block anatomy visualized with high-frequency linear probe prior to injection, showing respectively the pectoralis muscle (PM), intercostal muscle (IM), transversus thoracic plane (TTP), and transversus thoracic muscle (TTM). |
 |
Figure 3 Injectate placed superficial to the transversus thoracic muscle (TTM) in the transversus thoracic plane (TTP), with the needle under direct guidance passing through the pectoralis muscle (PM) and intercostal muscle (IM). |
Postoperative pain scores were recorded every hour by CTICU nursing staff per policy according to age appropriate 10-point pain scales: CRIES score for age 0–1 year, FLACC score for age 1–5 years, FACES scoring for age 5–8 years, and VAS for children over the age of 8 years. Post-operative pain scores and intravenous opioid consumption were recorded for the first 24 hours after surgery.
Data Analysis
Data were reported as frequencies and percentages for categorical data, and means, standard deviations, and ranges for continuous data. Differences between groups were examined using independent t-tests for continuous data and chi-square or Fisher’s exact test for categorical data. All tests were two-tailed and ps < 0.05 was considered significant. All tests were run using R version 4.2.1 statistical software.
Results
A total of 37 patients met inclusion criteria for data analysis in the present study. Twenty-one patients underwent anesthesia for cardiac surgery without a regional anesthetic technique and 16 patients received deep parasternal blocks. There were no significant differences between groups in regards to demographics and surgical data (Table 1) although the group receiving a deep parasternal block had a slightly increased duration of cardiopulmonary bypass. In the block group the mean age was 55.8 months (range, 6−168 months) with a mean weight of 22.6 kg; (range, 6.3–112.2 kg). The mean duration of surgery was 184.1 minutes; (range, 123–277 minutes). The mean duration of cardiopulmonary bypass was 107.2 ± 39.6 minutes (range, 43–204 minutes). In the group not receiving blocks, the mean age was 76.8 months (range 21−204 months) with a mean weight of 21.3 kg (range, 4.5–79.1 kg). The mean duration of surgery was 165.3 minutes (range, 102–237 minutes). The mean duration of cardiopulmonary bypass was 81.9 ± 34.9 minutes (range, 40–161 minutes).
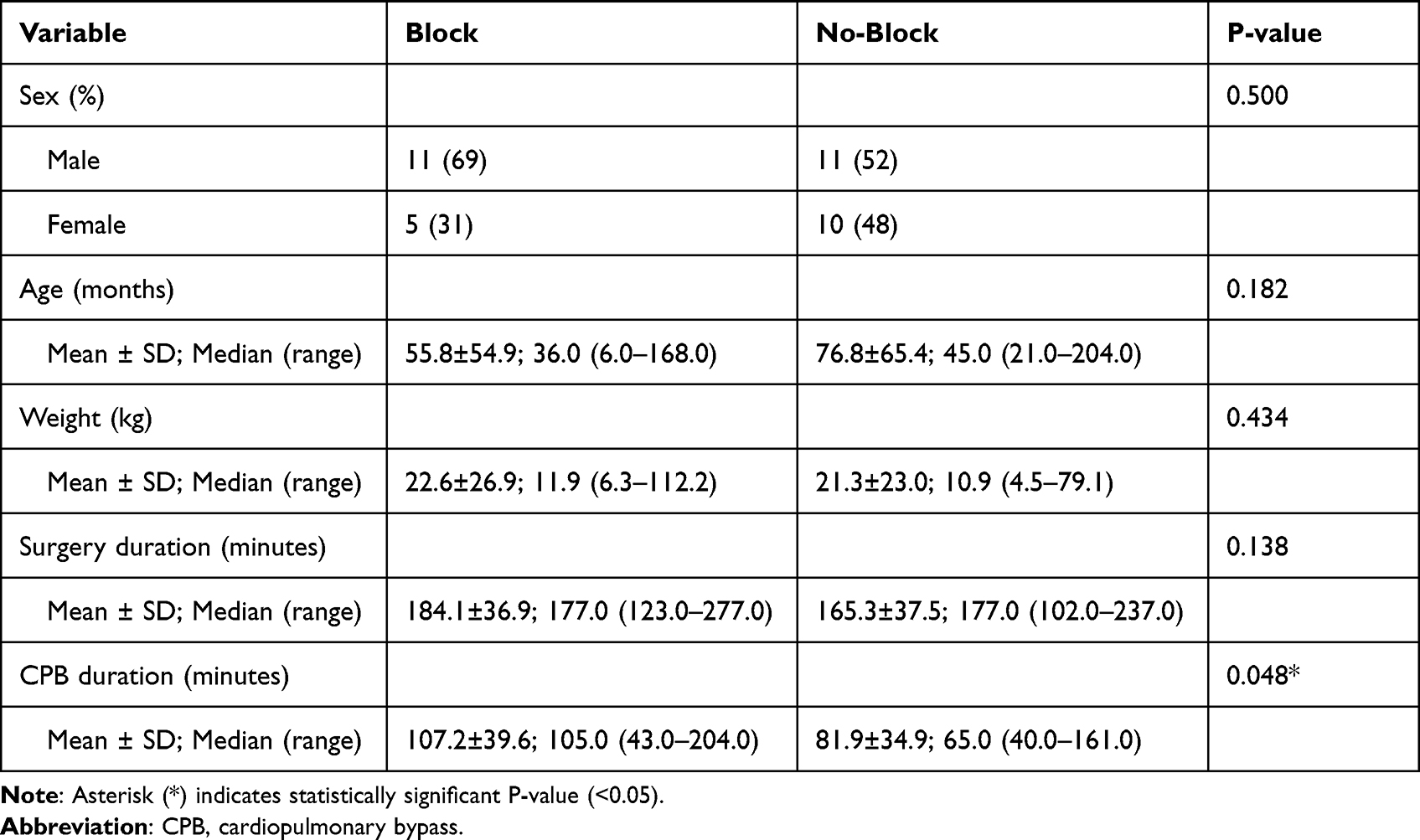 |
Table 1 Demographic and Surgical Characteristics |
The no-block group had significantly higher intraoperative opioid doses than the block group (Table 2). The average dose in intravenous intraoperative morphine equivalents was 0.63 ± 0.2 mg/kg for the control group, and 0.42 ± 0.2 mg/kg for the block group (p value 0.003). Postoperatively, the average pain scores were 3.9 ± 1.0 for the no-block group, and 2.6 ± 1.3 for the block group (p value 0.003). Postoperative length of stay in the ICU was 2.33 ± 0.58 days for the control group and it was 2.00 ± 1.59 days for the block group (p value 0.017).
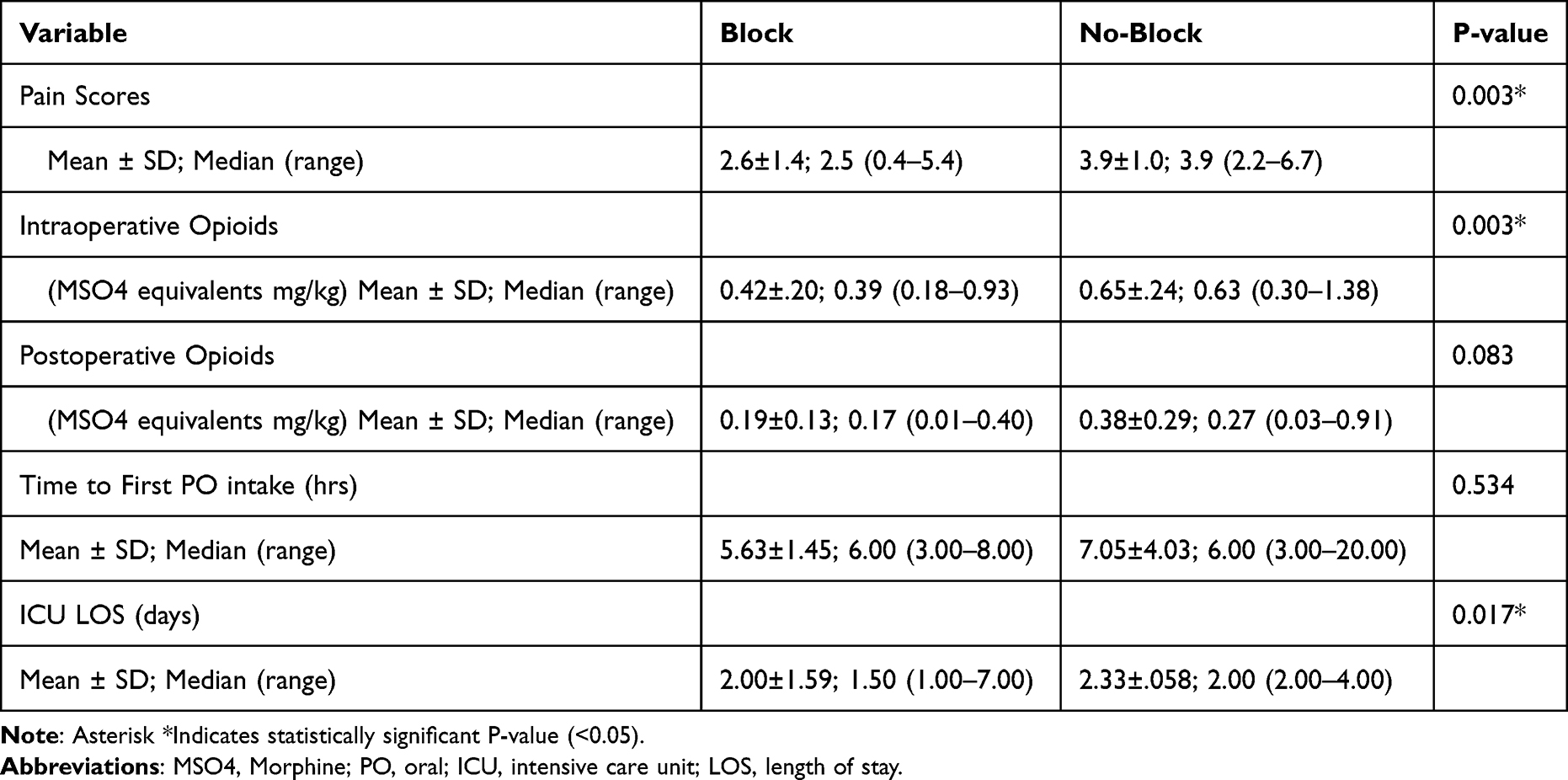 |
Table 2 Opioid Consumption and Post-Operative Outcomes |
There were no significant differences between groups in terms of time to first PO intake or post-operative opioid use. No complications with deep parasternal blocks were reported in any of the patients.
Discussion
Children undergoing cardiac surgery via median sternotomy often experience significant postoperative pain. The pain can last up to 7 days post-operatively and is often most severe on post-operative day 1.9 Opioids were traditionally the primary analgesic modality for treating postoperative pain after cardiac surgery; however, significant side effects such as sedation, pruritus, nausea, vomiting and constipation can limit their usefulness. Regional anesthetic strategies have been used in enhanced recovery protocols for colorectal surgery and adult cardiac surgery and may be able to play a role in pediatric cardiac surgery as well. Techniques such as neuraxial catheters and paravertebral blocks or catheters provide good analgesia but are not routinely used in this patient population. Newer truncal and facial plane blocks such as erector spinae and serratus anterior blocks have been shown to be useful in cardiac surgery patients as well as being safe and efficient.5,10 These techniques show promise as part of a multimodal analgesic approach that allows for early extubation and minimizes post-operative opioid consumption. The deep parasternal plane block, previously described as the transversus thoracic plane block, was first described in 2015 and has been shown to provide adequate analgesic coverage of the sternum via the T2-T6 anterior branches of the intercostal nerves. The block can be performed in the supine position, minimizing the time needed for performing the block, and it is safe to use in patients who will be undergoing systemic heparinization due to its low bleeding risk and superficial location. Our patient series describes the use of bilateral single injection deep parasternal blocks as part of a multimodal analgesic approach, providing optimal intraoperative and postoperative analgesia that decreases intraoperative opioid requirement, allows for early extubation and may decrease length of ICU stay.
Recent prospective and retrospective studies have demonstrated that the deep parasternal plane block provides effective postoperative analgesia in pediatric cardiac surgery patients.11,12 Patients receiving the parasternal blocks had lower postoperative pain scores until 24 hours after extubation, while also having significantly lower intraoperative and postoperative fentanyl requirements than control group patients. Additionally, time to extubation and length of stay in both the ICU and hospital were significantly shorter. No complications were reported in any of the patients.
Our retrospective study yielded similar results but included both simple and complex surgical procedures (Table 3), suggesting that the deep parasternal blocks may be applied to additional sternotomy candidates other than ASD and VSD closures. Specific to pediatric cardiac surgery, patients with single-ventricle physiology undergoing superior cavopulmonary anastomosis (Glenn) and total cavopulmonary anastomosis (Fontan) benefit from early extubation to eliminate the deleterious effects of positive-pressure ventilation on physiology that is dependent on a passive pulmonary circulation. Additionally, adequate post-operative pain control allows for improved respiratory mechanics which have hemodynamic benefits in these patients.
 |
Table 3 Surgical Procedures |
In our series, we also included the use of an adjuvant along with our local anesthetic in an attempt to prolong the length of the block. Bilateral injections were performed with 0.5 mL/kg of ropivacaine 0.25% with 0.5 µg/kg of clonidine to each side; this dosing provided adequate perioperative analgesia without any manifestations of local anesthetic toxicity. As an adjuvant, clonidine may extend the duration of a single injection block and provide analgesic properties with its alpha-2 effects. It has a well-established safety profile in pediatric regional anesthesia.13 Dexmedetomidine is gaining popularity as an adjuvant for local anesthetics in the pediatric population and has been shown to increase block duration.14–16 The efficacy of its use as an adjuvant for parasternal blocks has not yet been established but may prolong duration, allowing a single block to provide effective analgesia for many hours. Further studies to evaluate the effectiveness of dexmedetomidine in prolonging deep parasternal blocks are necessary.
In our experience, deep parasternal blocks provided sufficient analgesia to allow for lower intra-operative opioid dosing, improved pain scores in the first 24 hours post-operatively and may decrease ICU length of stay. The amount of intraoperative opioid administered was reduced significantly following the addition of the deep parasternal block to our practice (p-value 0.003). There was a statistically significant reduction in pain scores in the first 24 hours post-operatively in the group that received the block compared to the group that only received multimodal analgesia without a block (p-value 0.003). Most importantly, there was a decrease in ICU length of stay in the group receiving blocks (p-value 0.017) which is an important factor in decreasing hospital costs. However, there was no difference in post-operative opioid consumption or time to first PO intake. A contributing factor to this lack of difference may be that opioids are sometimes used as a first-line treatment in the ICU to treat agitation as well as to provide comfort and some sedation for patients in order to safely tolerate essential lines and tubes. This may account for the lack of statistically significant difference in post-operative opioid consumption. Additionally, our pre-existing post-operative pathway promotes early oral intake even prior to implementation of the block. No adverse outcomes were reported in any of the patients receiving the regional technique.
There are some major limitations of this study, the first being the relatively small number of cases and lack of a true control group (versus a comparison group). Additionally, while a statistically significant reduction in intraoperative opioid use was seen with the deep parasternal block group, without blinding we are unable to identify if this is a result of bias by administering less opioids to patients who were known to have had a block.
Further well-designed, large, randomized control trials in homogenous cardiac surgery populations comparing this regional block technique with other techniques are necessary to confirm efficacy and opioid-sparing effects to help make more definitive conclusions regarding the use of the deep parasternal block in routine practice.
Conclusion
When added to a pre-existing ERAS pathway, bilateral deep parasternal blocks may reduce intraoperative opioid consumption, provide effective postoperative pain control, and reduce ICU length of stay, across both simple and complex cardiac surgical procedures.
Acknowledgments
Non-Author Collaborators-Janessa Thirion, NP and Carrie Williams, NP Rainbow Babies & Children’s Hospital-Pediatric Pain Service, 11100 Euclid Ave, Cleveland, OH 44106.
Sarah DeLozier, PhD, Clinical Research Biostatistician–University Hospitals Cleveland Medical Center, Clinical Research Center, 11100 Euclid Ave, Cleveland, OH 44106.
This publication was made possible through the support of the Clinical Research Center of University Hospitals Cleveland Medical Center (UHCMC) and the Case Western Reserve University Clinical and Translational Science Collaborative (CTSC) 4UL1TR000439. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of UHCMC or NIH.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mazzeffi M, Khelemsky Y. Poststernotomy pain: a clinical review. J Cardiothorac Vasc Anesth. 2011;25(6):1163–1178. doi:10.1053/j.jvca.2011.08.001
2. Anand K, Hickey PR. Halothane‐morphine compared with high dose sufentanil for anesthesia and postoperative analgesia in neonatal cardiac surgery. N Engl J Med. 1992;326:1–9. doi:10.1056/NEJM199201023260101
3. Gruber EM, Laussen PC, Casta A, et al. Stress response in infants undergoing cardiac surgery: a randomized study of fentanyl bolus, fentanyl infusion and fentanyl‐midazolam infusion. Anesth Analg. 2001;92:
4. Mehta Y, Arora D. Benefits and risks of epidural analgesia in cardiac surgery. J Cardiothorac Vasc Anesth. 2014;28:
5. Kaushal B, Chauhan S, Magoon R, et al. Efficacy of bilateral erector spinae plane block in management of acute postoperative surgical pain after pediatric cardiac surgeries through a midline sternotomy. J Cardiothorac Vasc Anesth. 2020;34(4):981–986. doi:10.1053/j.jvca.2019.08.009
6. El-Boghdadly K, Wolmarans M, Stengel AD, et al. Standardizing nomenclature in regional anesthesia: an ASRA-ERAS Delphi consensus study of abdominal wall, paraspinal and chest wall blocks. Reg Anesth Pain Med. 2021;46:571–580. doi:10.1136/rapm-2020-102451
7. Ueshima H, Akira K. Blocking of multiple anterior branches of intercostal nerves (Th2-6) using a transversus thoracic muscle plane block. Reg Anesth Pain Med. 2015;40:388. doi:10.1097/AAP.0000000000000245
8. Fuller S, Kumar SR, Roy N, et al. The American Association for Thoracic Surgery Congenital Cardiac Surgery Working Group 2021 consensus document on a comprehensive perioperative approach to enhanced recovery after pediatric surgery. J Thorac Cardiovasc Surg. 2021;162(3):931–954. doi:10.1016/j.jtcvs.2021.04.072
9. Mueller XM, Tinguely F, Tevaearai HT, Revelly JP, Chioléro R, Von Segesser LK. Pain location, distribution, and intensity after cardiac surgery. Chest. 2000;118:
10. Bhatt HV, Hernandez N, Shariat A. Successful use of serratus and transversus thoracic plane blocks for subcutaneous implantable cardioverter-defibrillator placement. J Cardiothorac Vasc Anesth. 2018;32(1):e22–e23 . doi:10.1053/j.jvca.2017.09.019
11. Zhang Y, Chen S, Gong H, Zhan B. Efficacy of bilateral transversus thoracis muscle plane block in pediatric patients undergoing open cardiac surgery. J Cardiothorac Vasc Anesth. 2020;34(9):2430–2434. doi:10.1053/j.jvca.2020.02.005
12. Abdelbaser I, Mageed N. Analgesic efficacy of ultrasound guided bilateral transversus thoracis muscle plane block in pediatric cardiac surgery: a randomized, double-blind controlled study. J Clin Anesth. 2020;67:110002.
13. Lundblad M, Trifa M, Kaabachi O, et al. Alpha-2 adrenoceptor agonists as adjuncts to peripheral nerve blocks in children: a meta-analysis. Paediatr Anaesth. 2016;26:232–238. doi:10.1111/pan.12825
14. Shah UJ, Nguyen D, Karuppiaah N, et al. Efficacy and safety of caudal dexmedetomidine in pediatric infra-umbilical surgery: a meta-analysis and trial-sequential analysis of randomized controlled trials. Reg Anesth Pain Med. 2021;46(5):422–432. doi:10.1136/rapm-2020-102024
15. Lundblad M, Marhofer D, Eksborg S, et al. Dexmedetomidine as adjunct to ilioinguinal/iliohypogastric nerve blocks for pediatric inguinal hernia repair: an exploratory randomized controlled trial. Paediatr Anaesth. 2015;25(9):897–905. doi:10.1111/pan.12704
16. Abdellatif A, Kasem A, Bestarous J, et al. Efficacy of dexmedetomidine as an adjuvant to quadratus lumborum block for pediatrics undergoing laparoscopic pyeloplasty. A prospective randomized double blinded study. Minerva Anestesiol. 2020;86(10):1031–1038. doi:10.23736/S0375-9393.20.14298-6
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Impact of Fascial Plane Block on Postoperative Length of Stay and Opioid Use Among Colectomy Patients Within an Established Enhanced Recovery After Surgery Program: A Retrospective Cohort Study
Khersonsky J, Alavi M, Yap EN, Campbell CI
Journal of Pain Research 2025, 18:689-699
Published Date: 12 February 2025