")
Back to Journals » Psychology Research and Behavior Management » Volume 16
Adaptation of the Mental Health Inventory (MHI-38) for Adolescents - Indonesian Version
Authors Parombean AC, Abidin FA , Qodariah L , Novita S
Received 14 April 2023
Accepted for publication 6 July 2023
Published 13 July 2023 Volume 2023:16 Pages 2655—2665
DOI https://doi.org/10.2147/PRBM.S412460
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Abes Chrismayanti Parombean,1 Fitri Ariyanti Abidin,2,3 Laila Qodariah,2,3 Shally Novita4
1Postgraduate Professional Psychology Study Programme, Faculty of Psychology, Universitas Padjadjaran, Sumedang, 45363, Indonesia; 2Department of Psychology, Faculty of Psychology, Universitas Padjadjaran, Sumedang, 45363, Indonesia; 3Center for Family Life and Parenting Studies, Faculty of Psychology, Universitas Padjadjaran, Sumedang, 45363, Indonesia; 4Center for Innovations and Psychological Research, Faculty of Psychology, Universitas Padjadjaran, Sumedang, 45363, Indonesia
Correspondence: Abes Chrismayanti Parombean, Department of Psychology, Faculty of Psychology, Universitas Padjadjaran, Jl Raya Bandung-Sumedang Km. 2, Sumedang, 45363, Indonesia, Tel +62 812 7892 3493, Email [email protected]
Objective: This study validates the Indonesian version of the Mental Health Inventory-38 (MHI-38) for use among Indonesian adolescents. The adaptation process followed guidelines from the International Test Commission and involved translation, expert review, cognitive interviews, and psychometric evaluation. A total of 562 adolescents (mean age = 15.42, SD = 1.84) participated in the study.
Results: The MHI-38 demonstrated dual factors: psychological well-being and psychological distress. Internal consistency was high for the MHI-38 (α = 0.892) and its factors: psychological well-being (α = 0.894) and psychological distress (α = 0.952). Confirmatory factor analysis indicated a good fit (RMSEA = 0.048, CFI = 0.945, NFI = 0.908, TLI = 0.929). Psychological well-being correlated moderately with the Satisfaction with Life Scale (r = 0.469, p = 0.00) and positive affect (r = 0.448, p = 0.00), but negatively with the Kessler Psychological Distress Scale (r = − 0.230, p = 0.00). Psychological distress correlated strongly with the Kessler Psychological Distress Scale (r = 0.910, p = 0.00) and negative affect (r = 0.857, p = 0.00), but negatively with the Satisfaction with Life Scale (r = 0.556, p = 0.00).
Conclusion: The Indonesian version of the MHI-38 demonstrated good psychometric properties and validity, making it a reliable tool for assessing mental health in Indonesian adolescents.
Keywords: adolescents, mental health, psychological well-being, psychological distress, psychometric properties, validation
Introduction
Mental health in adolescents poses a significant challenge, especially in developing countries like Indonesia. However, the existing body of research on mental health assessment primarily originates from developed countries.1 Insufficient attention has been given to investigating adolescents’ mental health in low- and middle-income countries (LMICs), leading to a dearth of data in this area. One potential factor contributing to the limited research in this area is the lack of attention given to the distinct mental health needs of children and adolescents, which differ from those of adults. This lack of attention is particularly evident in the insufficient availability of mental health professionals and dedicated facilities specifically tailored to meet the needs of children and adolescents in many LMICs. The lack of specialized training among mental health professionals hampers their ability to provide effective services to this population. Additionally, children and adolescents are often perceived as having limited influence in politics and economics. As a result, their mental health needs are more likely to be overlooked than adult patients with mental disorders.2 It is crucial to develop diagnostic and assessment tools that consider specific regions’ unique cultural and social contexts. Tools developed in developed countries may not adequately address the cultural nuances prevalent in developing nations, thereby hampering the accurate identification and measurement of adolescent mental health issues.
In recent years, mental health problems among Indonesian adolescents have increased.3 A study by the Indonesian Psychiatric Association in 2020 found that 27% of Indonesian adolescents aged 13–18 reported experiencing mental health issues, with depression and anxiety being the most common concerns.4 Various factors contribute to mental health problems among Indonesian adolescents, including academic pressure,5 social media use,6 family conflicts,7 and exposure to violence and trauma.8 Moreover, the stigma and lack of awareness around mental health issues may prevent adolescents from seeking help. Additionally, living in a rural district and having a low-educated father was associated with a higher prevalence.1
Adolescent mental health represents a matter of significant concern, given the intricacies and challenges associated with this pivotal development period.9 Traditionally, mental health has been conceptualized within a negative framework, defined by the absence of mental illnesses such as anxiety and depression. This approach primarily focused on identifying and addressing pathological conditions.10 However, the emergence of positive psychology has ushered in a paradigm shift, wherein attention is increasingly directed towards acknowledging and understanding positive patterns and experiences, such as well-being, happiness, resilience, and flourishing. Consequently, mental health is now comprehended through a dual perspective that integrates both positive and negative dimensions.11 This contemporary approach recognizes that individuals can experience positive and negative states simultaneously, challenging the notion of an exclusive dichotomy. By adopting this comprehensive perspective, researchers and practitioners are better equipped to capture the complexity and interconnectedness of mental health, enabling a more holistic understanding of the factors that contribute to overall well-being during adolescence.
In line with the evolving understanding of mental health, the measurement tools utilized have also followed suit. Earlier assessments predominantly adhered to a negative framework, exemplified by instruments like the Kessler Psychological Distress Scale11 and Beck Depression Inventory.12 However, with the growing recognition of positive aspects of mental health, recent measurement tools have shifted their focus accordingly. Examples of this are the Brief Scale for Psychological Well-being for Adolescents (BSPWB-A),13 the Satisfaction with Life Scale (SWLS),14 and the Warwick-Edinburgh Mental Well-being Scale (WEMWBS),15 which specifically captures and evaluates positive dimensions of well-being. The most recent development shows that several measurement tools have been developed to assess multiple perspectives within mental health. For instance, the Strengths and Difficulties Questionnaire (SDQ),1 Positive Affect Negative Affect Schedule (PANAS),14 and the Mental Health Inventory (MHI-38).10
Compared to the Strengths and Difficulties Questionnaire (SDQ), which primarily focuses on strengths and difficulties in children and adolescents, and the Positive Affect Negative Affect Schedule (PANAS), which primarily focuses on affective states, the Mental Health Inventory (MHI-38) stands out for its explicit assessment of psychological distress and well-being. This characteristic makes it suitable for identifying individuals experiencing significant psychological difficulties or distress and those with higher levels of well-being. Furthermore, the MHI-38 offers the advantage of applicability across a broader age range, including adolescents and adults, in contrast to the SDQ’s specific focus on children and adolescents. This characteristic allows for longitudinal studies tracking mental health trends from adolescence to adulthood. Utilizing the MHI-38 provides researchers with insights into the stability and trajectory of mental health outcomes over time. In addition to its broad age applicability and longitudinal potential, the MHI-38 enjoys a well-established reputation as a valid and reliable instrument in mental health research. Previous studies have demonstrated its validity and reliability, enhancing its credibility and robustness as a measurement tool.
Numerous studies have reported on the psychometric properties of the MHI-38 in various languages, including the Urdu version,16 Arabian version,17 Persian version,18 and Chinese version.19 In these versions, the internal consistency yielded satisfactory reliability coefficients ranging between 0.62 and 0.96, achieved by improving or removing less satisfactory items. The factor structure consistently showed a two-factor structure: Psychological Well-Being and Psychological Distress. Confirmatory factor analysis (CFA) and exploratory factor analysis (EFA) supported this structure, confirming a good fit.
Adolescents who achieve psychological well-being demonstrate various positive conditions, such as better physical and mental health,16,20 improved quality of life and prosocial behavior, as well as reduced rates of crime, illicit drug use, and alcohol consumption,21 possess better social skills,22 perform better academically, exhibit higher levels of intrapersonal and interpersonal competence, and demonstrate the ability to cope with problems using more adaptive strategies.23 In the long term, psychological well-being in adolescence can determine psychological well-being in adulthood and enhance life expectancy.20,22,24,25 In contrast, psychological distress has significant effects on adolescents. It can manifest in various negative outcomes and impact different aspects of their lives, such as decreased educational attainment, higher rates of school dropout, impaired social relationships, and an elevated risk of substance abuse, mental health issues, and suicide.26,27 Therefore, the availability of measurement tools that can assess both conditions is highly important.
Based on the explanation, the present study aims to adapt and validate the MHI-38 as a self-report instrument for assessing the mental health of Indonesian adolescents. By utilizing the MHI-38, researchers can comprehensively understand mental health in this population, considering its multidimensional nature and potential long-term implications. This adaptation and validation process will facilitate the use of a reliable and culturally sensitive tool to measure mental health outcomes among Indonesian adolescents, ultimately enhancing the accuracy and effectiveness of mental health interventions and policies in the region. Based on the comprehensive factors measured, the well-known, and the capability to capture the mental health in adolescents and the trends until adults, the present study aims to adapt and validate the Mental Health Inventory (MHI-38) as a self-report instrument for assessing the mental health of Indonesian adolescents.
Material and Methods
Procedures
The research was conducted following the stages outlined by the International Test Commission’s guidelines,28 including 1) Obtaining permission, 2) Test development, 3) Confirmation, 4) Administration, and 5) Psychometric analysis. In the first stage, written permission was obtained from the RAND Corporation to adapt and translate the original MHI for research purposes. RAND Health Care surveys and tools are publicly available documents that can be accessed free of charge. Further information regarding the availability of the surveys can be found at https://www.rand.org/health-care/surveys_tools/mos/mental-health.html.
In the second stage, two certified Indonesian translators conducted forward translations of the MHI from English to Indonesian. Following this procedure, an online discussion was conducted with two psychology colleagues to determine the accuracy of the translation. The items were then translated back into English by one certified Indonesian translator. Two psychology colleagues then reviewed the final translated version, and three clinical psychologists were engaged to evaluate the items’ relevance, necessity, representativeness, and comprehensiveness in measuring mental health. Each expert independently rated each item on a 4-point scale (1= Not relevant, 2= Somewhat relevant, 3=Sufficiently relevant, 4= Highly relevant). The Content Validity Index (CVI) was calculated by dividing the number of experts who rated the item as 3 or 4 by the total number of experts for each item. The translation results can be seen in Appendix 1.
In the original version of the MHI, 34 items used six answer choices, while two items used five answer choices. However, modifications were made to adapt the MHI for use in the Indonesian context, where all item used five answer choices. This modification was based on the original Likert scale, which included five symmetrical and balanced options,29 and was intended to ensure the instrument’s cultural and linguistic appropriateness for Indonesian adolescents. Muhid et al recommended that the answer choices for each item should always be symmetrical, with the same proportion of positive and negative levels. They argued that using too many answer choices can blur the desired difference, potentially confusing participants who may have difficulty perceiving differences between similarly worded response options. On the other hand, using more differentiated response scales may pose important challenges to humans’ ability to make fine-grained distinctions regarding responses to relatively coarse psychological test items.30
In the third stage, we conducted cognitive interviews. Five participants reported that they found the items in the MHI-38 to be easy to comprehend. However, one participant had difficulty understanding item 18, which originally read, “How much of the time, during the past month, have you felt emotionally stable? This participant interpreted the word “emotion” as negative emotions such as anger. Therefore, the item was modified to ‘How much of the time, during the past month, your emotions and feelings are stable?’ to better reflect the intended meaning of the item.
In the fourth stage, we administered the instrument that had obtained ethical clearance from the Ethical Committee of Padjadjaran University (No. 27/UN6.KEP/EC/2022). Data collection was conducted between January and March 2022, utilizing an online questionnaire on Google Forms. Prior to participating, all participants provided their informed consent. The participants were granted ethical committee approval to provide informed consent on their own behalf, after receiving a comprehensive explanation of the data collection process. The questionnaire was completed within an estimated timeframe of 15–30 minutes.
In the fifth stage, the administered instruments were analyzed for their psychometric properties, encompassing reliability and construct validity through Confirmatory Factor Analysis (CFA). Concurrent validity was assessed by comparing the results with established measures such as the Satisfaction with Life Scale (SWLS), the Kessler Psychological Distress Scale-6 (K-6), and the Positive Affect Negative Affect Schedule (PANAS). The obtained results from the measurement adaptation were diligently recorded.
Participants
This study involved 562 Indonesian adolescents, with a mean age of 15.43 years (SD = 1.84). Convenience sampling was employed, which allowed researchers to collect information from participants who were easily accessible.31 Participants were recruited through social media platforms such as WhatsApp, Facebook, and Instagram and through personal networks of acquaintances and colleagues who met the study’s inclusion criteria. The inclusion criteria encompassed individuals aged between 12 and 18 years who were fluent in Bahasa Indonesia. An online research questionnaire was distributed to eligible participants.
Instruments
Except for the MHI-38, the Indonesian versions were available for all other questionnaire tools used, and each measurement had previously been determined to have satisfactory reliability and validity.
MHI-38
The instrument comprises 38 items that describe symptoms or states of mind, with respondents rating the frequency or intensity of symptoms or states of mind experienced during the past month. The scale consists of two components: psychological well-being and psychological distress. Psychological well-being comprises three dimensions: general positive affect (11 items, eg, During the past month, how much of the time have you been a happy person?), emotional ties (2 items, eg, During the past month, how much of the time have you felt loved and wanted?), and life satisfaction (1 item, how happy, satisfied, or pleased have you been with your personal life during the past month?), while the psychological distress component comprises three dimensions: anxiety (9 items, eg, During the past month, how much of the time have you been anxious or worried?), depression (6 items, eg, During the past month, how much of the time have you been moody or brooded about things?), and loss of behavioral/emotional control (9 items, eg, During the past month, how much of the time did you feel that you had nothing to look forward to?). The Indonesian version of the MHI-38 employed a Likert scale (1 = never, 2 = rarely), 3 = sometimes, 4 =often, and 5 = always) to capture the ratings provided by the respondents. The original version of the MHI-38 demonstrated good internal consistency, with α=0.92 for the psychological distress component and α=0.96 for the psychological well-being component.2 The Indonesian version of the MHI-38 utilized a Likert scale ranging from 1 (Never) to 5 (Always) to capture respondent ratings. The original version of the MHI-38 demonstrated good internal consistency, with α=0.92 for the psychological distress component and α=0.96 for the psychological well-being component.9
To measure the concurrent validity of MHI-38, we used the following instruments:
The Kessler Psychological Distress Scale-6 (K-6) is available and validated for use in the Indonesian context. The K-6 measures psychological distress (6 items, eg, During the past 30 days, about how often did you feel worthless?), using a 5-point Likert scale using a 5-point Likert scale (1 = never, 2 = rarely, 3 = sometimes, 4 =often, and 5 = always). In previous studies with Indonesian students, the K-6 has shown a good predictive ability for depression and anxiety disorders, with Area Under the Curve (AUCs) ranging from 0.68 to 0.88.11
The Satisfaction with Life Scale (SWLS) is also available and validated in Indonesia. The SWLS is a commonly used scale for measuring general life satisfaction (5 items, eg In most ways my life is close to my ideal), using a 7-point Likert scale (1 = strongly disagree, 2 = Disagree, 3 = Slightly Disagree, 4 = Neither Agree nor Disagree, 5 = Slightly Agree, 6 = Agree, 7 = Strongly Agree). The SWLS has demonstrated good reliability with internal consistency (α = 0.82) and a good item-total correlation ranging between 0.55 and 0.68.14
The Positive Affect Negative Affect Schedule (PANAS), is available and validated for use in the Indonesian context. The PANAS consists of two subscales measuring positive affect (10 items, eg, Interested) and negative affect (10 items, eg, Ashamed), respectively, using a 5-point Likert scale (1 = Very slightly or not at all, 2 = A little, 3 = Moderately, 4 = Quite a bit 5 = Extremely). The subscales are scored separately due to the partial independence of the two types of feelings. The PANAS has shown satisfactory internal consistency, with Cronbach’s α coefficients of 0.86 for positive affect and 0.83 for negative affect. The item-total correlation for positive affect ranged from 0.45 to 0.66, and for negative affect, it ranged from 0.41 to 0.69.14
Data Analysis
Missing values in the variable data were handled using the listwise deletion method, only analyzing respondents with complete data for the research variables.31 The psychometric properties of the adapted MHI-38 were examined in terms of reliability and validity. Internal consistency was assessed using Cronbach’s alpha, with values of at least 0.70 considered to indicate good reliability.32 Content validity was evaluated using the content validity index (CVI), which is a standard approach for evaluating content validity.33 Three clinical psychologists were involved in evaluating the items’ relevance, necessity, representativeness, and comprehensiveness in measuring mental health. The CVI was computed as the number of experts giving a rating of 3 or 4 (indicating sufficient or high relevance, respectively), divided by the total number of experts for each item. A CVI of at least 0.78 was considered acceptable.34
Construct validity was evaluated using confirmatory factor analysis (CFA) in JASP 0.14.1.1.0. Model fit was evaluated using several fit indices. The root means square error of approximation (RMSEA) was employed with a cut-off value below 0.05. The normed fit index (NFI) was utilized, with a criterion of 0.90 or higher. Similarly, the comparative fit index (CFI) and Tucker-Lewis index (TLI) were assessed, both requiring values greater than 0.90 for an acceptable fit.35 Factor loadings were evaluated to ensure that all items had a moderate correlation with the factor, with a threshold of 0.30.36 Concurrent validity was evaluated by correlating the Psychological Well-being score with the Satisfaction with Life score and Positive Affect Score, and the Psychological Distress score with the Kessler Psychological Distress Scale-6 score and Negative Affect Score. Correlation coefficients were interpreted using the criterion proposed by Dancey and Reidy: < 0.3 = weak, 0.4–0.6 = moderate, 0.70–0.9 = strong, 1 = perfect.37
Results
Characteristics of the Study Participants
The participants in our study were between the ages of 12 and 18 years, with a mean age of 15.42 (SD = 1.84). The distribution of respondents was 45.8% male and 54.2% female.
Psychometric Properties
Reliability
In the current study, the MHI-38 demonstrated relatively adequate reliability with a Cronbach’s alpha coefficient of 0.892. Additionally, both the Psychological Well-being and Psychological Distress factors showed acceptable coefficient reliability, with Cronbach’s alpha coefficients of 0.894 and 0.952, respectively, as shown in Table 1. We calculated coefficient H for both psychological well-being (coefficient H = 0.912) and psychological distress (coefficient H = 0.827) using a formula suggested by Hancock et al.38
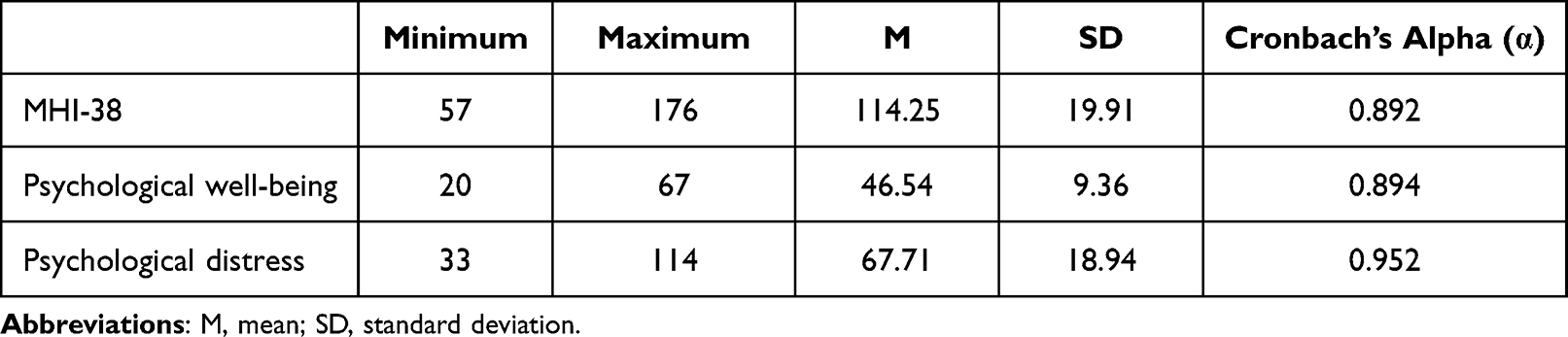 |
Table 1 Reliability of the Indonesian Version of the MHI-38 for Adolescent |
Content Validity
The content validity index (CVI) was calculated to be 1.00, indicating very good validity of the instrument based on the CVI criteria.39 Nevertheless, based on the comments and feedback provided by the experts, some item wordings were modified to improve the clarity and comprehensibility of the instrument.
Construct Validity
The Indonesian version of MHI-38 was examined using the dual-factor model in Confirmatory Factor Analysis (CFA), with the Chi-Square value (χ2 = 1217.456; p < 0.001). The results of the CFA demonstrated that the MHI-38 had a good fit (RMSEA = 0.048; CFI = 0.945; NFI = 0.908; TLI = 0.929). As shown in Table 2, the factor loadings for all items, except for items 14 and 18, were above 0.30 and statistically significant (p < 0.001). These results indicate that the items have significant relationships with their respective factors, indicating sufficient construct validity for the scale. Figure 1 presents the measurement model for the Indonesian version of MHI-38 for Adolescents.
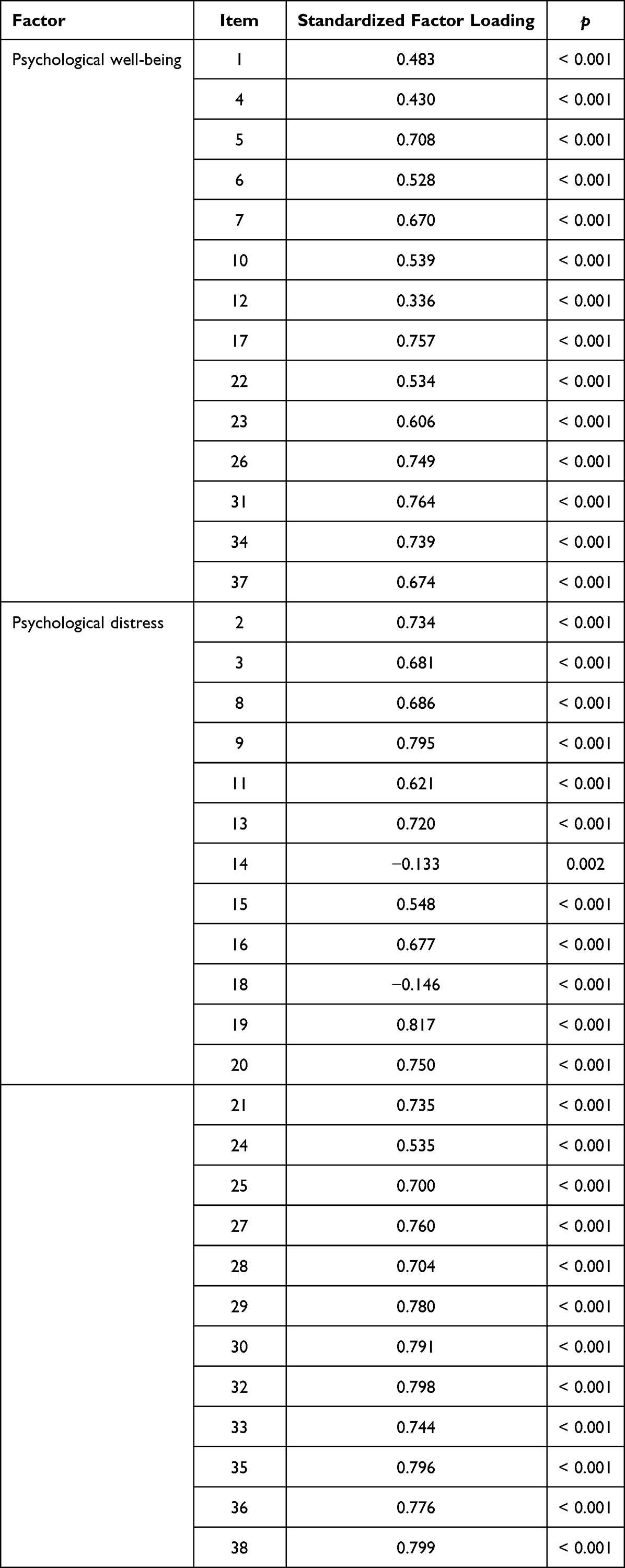 |
Table 2 Factor Loadings |
 |
Figure 1 Dual-factor model. |
Concurrent Validity
Based on the results in Table 3, the concurrent validity of the Indonesian version of MHI-38 was tested by correlating the scores of each mental health factor, namely psychological well-being, and psychological distress, with several established scales, including the Satisfaction with Life Scale (SWLS), The Kessler Psychological Distress Scale-6 (K-6), and Positive Affect and Negative Affect Schedule (PANAS). The psychological well-being factor demonstrated a moderate positive correlation with SWLS (r = 0.469, p < 0.001), and Positive Affect (r = 0.448, p < 0.001), a weak negative correlation with K-6 (r = - 0.230, p < 0.001), and Negative Affect (r = −0.165, p < 0.001). On the other hand, the psychological distress factor showed a strong positive correlation with K-6 (r = 0.910, p < 0.001), and Negative Affect (r = 0.857, p < 0.001), a moderate negative correlation with SWLS (r = −0.556, p < 0.001), and a weak negative correlation with Positive Affect (r = −0.386, p < 0.001). These results demonstrate the satisfactory concurrent validity of the Indonesian version of MHI-38.
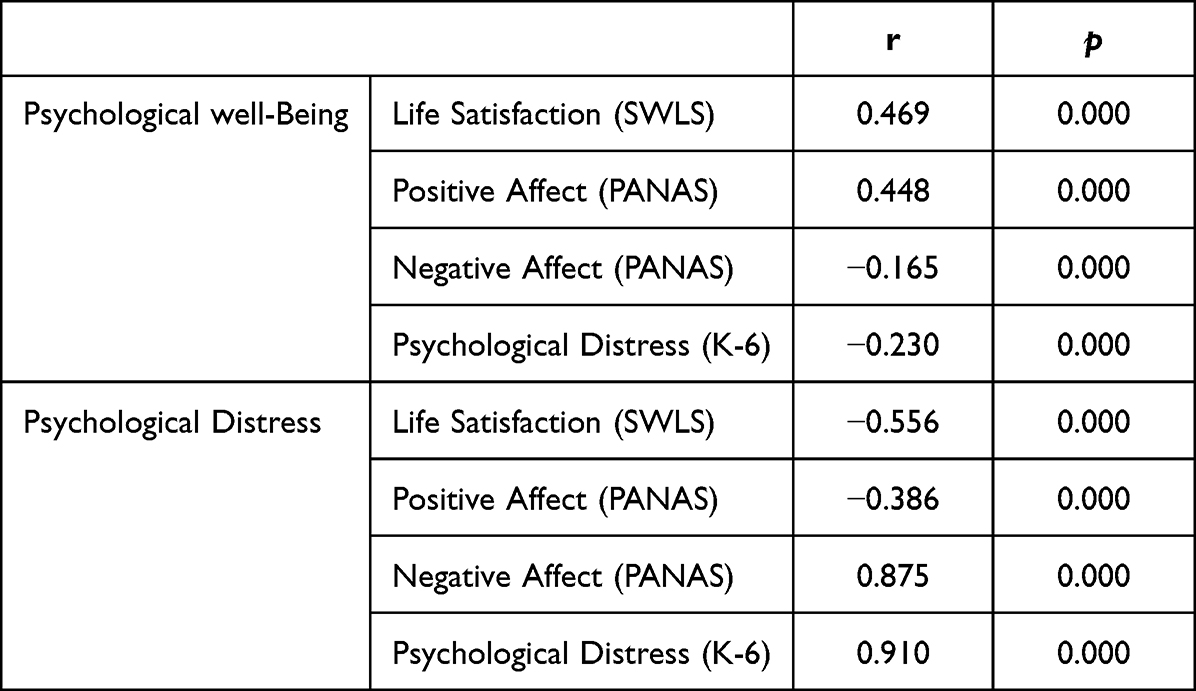 |
Table 3 Correlation Between MHI-38 and Related Instruments |
Discussion
The present study aimed to translate and test the psychometric properties of the MHI-38 in the Indonesian context using data collected from a sample of adolescents in Indonesia. The analysis of the psychometric properties of the instrument demonstrated promising results. Regarding reliability, the internal consistency of the Indonesian version of MHI-38 was found to be relatively high. Additionally, both psychological well-being and psychological distress subscales showed acceptable reliability coefficients.
Regarding the validity, the validity evidence indicated the MHI-38 as a valid scale to measure adolescents’ mental health in the Indonesia population. The Confirmatory Factor Analysis (CFA) results revealed that the Indonesian Version of the MHI-38 clustered into two different factors that were congruent with the original version of the scale. These two sub-groups were found to measure the dimensions of mental health, namely psychological well-being, and psychological distress. These findings are consistent with previous studies on the translation, adaptation, or psychometric testing of the MHI-38 in other languages, including Urdu, Arabic, Persian, and Chinese.16–19
The results of the study indicated that all items in both the psychological well-being and psychological distress factors loaded onto their respective factors, with two items (ie, 14 and 18) as exceptions. Item 14 “During the past month, have you been in firm control of your behavior, thoughts, emotions, or feelings?” seems to pose multiple questions, such as the ability to control behavior, thoughts, emotions, and feelings, with only one answer choice, making it difficult to assess each aspect separately. Conversely, the responses to these four aspects may differ for everyone. Item 18 had ambiguous phrasing. During the cognitive interview process, one participant interpreted emotion as a negative feeling, such as anger, a common understanding in Indonesian society. This understanding may have affected some adolescents’ responses, as some may have interpreted the item similarly. Peacock et al noted that individuals with limited reasoning abilities need assistance comprehending the scale’s statement items.40 Considering the factor loadings issue, we suggest that future studies carefully examine items 14 and 18 and consider excluding them from the analysis if their factor loadings do not yield satisfactory results.
Correlations between the dual mental health factors and other related psychological constructs were identified. For example, the psychological distress subscale has a high correlation with the K-6. This finding is understandable due to the same construct these scales measured. Both scales measure an individual’s emotional state over the previous 30 days. For instance, item 1 of the K-6 asks, “About how often during the past 30 days did you feel nervous?”, while the MHI-38 assesses, “How much of the time, during the past month, have you been a very nervous person?”. Similarly, item 4 of the K-6 queries, “How often did you feel so depressed that nothing could cheer you up?”, whereas the MHI evaluates, “How often, during the past month, have you felt so down in the dumps that nothing could cheer you up?”
However, there is also a correlation between the psychological well-being subscale and the K-6. However, a closer inspection revealed that such correlations were not strong enough. These findings confirm that the association was not strong enough to assume that distress and well-being are two completely different ends of one continuum.41 These results suggest that it is conceptually and methodologically incorrect to assume the presence of well-being simply by the absence of distress. The weak relationships between these various indicators suggest that the scores on the well-being scale do not strongly predict the level of distress. Individuals experiencing psychological distress may concurrently experience lower levels of well-being. Similarly, individuals with higher levels of well-being may be less likely to report distress symptoms. Thus, there may be a shared variance between distress and well-being measures, leading to a significant correlation between the K-6 and both subscales of the MHI-38.
The findings of this study demonstrate that the Indonesian Version of MHI-38 is an effective tool for assessing psychological well-being and psychological distress, two distinct aspects of mental health. The MHI-38 is a multidimensional measurement instrument that can be used to evaluate these aspects independently and collectively. Furthermore, the MHI-38 has wide-ranging applications and can contribute to promoting mental health in various settings, including clinical and non-clinical contexts. In clinical or counseling settings, the MHI-38 can be utilized to identify, screen, and diagnose mental health problems. Additionally, it is valuable for conducting pre-post assessments in intervention or prevention research studies. The MHI-38 can be employed in the educational sector to evaluate students’ mental health, providing valuable insights into their well-being and distress levels. This information can inform the development of targeted interventions and support systems to enhance student mental health. Overall, the Indonesian Version of MHI-38 offers a comprehensive and versatile approach to assessing mental health and can be applied effectively across different domains, making it a valuable resource for researchers, clinicians, educators, and other professionals working in mental health.
Study Limitations
This study makes a valuable contribution to the existing literature on mental health assessments by validating the MHI-38 in a non-adult population. The research offers novel insights into the instrument’s validity in Indonesian, particularly in its application among adolescents. Nevertheless, it is essential to acknowledge several limitations of this study. Firstly, the use of convenience samples may affect the generalizability of the findings. Additionally, relying on online self-report measures without a proctor introduces the possibility of response bias and inaccuracies in participant reporting. Another limitation pertains to the Content Validity Index (CVI), where a score of 1 for complete agreement may not fully capture diverse perspectives or identify potential content flaws. To address this limitation, we employed additional validity assessment methods, such as Confirmatory Factor Analysis (CFA).
Conclusion
The present study provides initial evidence for the psychometric soundness of the Indonesian version of the MHI-38. Our findings demonstrate that the MHI-38 effectively captures both psychological well-being and psychological distress factors, with high reliability and validity across most of its items. While two items exhibited lower reliability, the scale demonstrates adequate measurement consistency and construct validity. These results suggest that with some refinement, the MHI-38 may serve as a valuable tool for measuring mental health among adolescents in Indonesia while also acknowledging the importance of cultural and developmental factors in the evaluation of mental health.
Acknowledgments
The authors would like to express our gratitude to all participants in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pandia V, Noviandhari A, Amelia I, Hidayat GH, Fadlyana E, Dhamayanti M. Association of mental health problems and socio-demographic factors among adolescents in Indonesia. Glob Pediat Health. 2021;8:2333794X211042223. doi:10.1177/2333794X211042223
2. Zhou W, Ouyang F, Nergui OE, et al. Child and adolescent mental health policy in low-and middle-income countries: challenges and lessons for policy development and implementation. Front Psychiatry. 2020;11:150. doi:10.3389/fpsyt.2020.00150
3. Sulistiowati E, Wicaksono IR, Indrawati L. Prevalence of mental health problems among adolescents in Surabaya, Indonesia. Jurnal Psikiatri Surabaya. 2020;3(2):49–56.
4. Sari KA, Wahyuningsih DP, Rahayu E. Academic pressure and mental health among adolescents in Indonesia. Indian J Public Health Res Dev. 2020;11(2):225–229.
5. Santoso HB, Wahyuningsih DP. The relationship between social media use and mental health among adolescents in Indonesia. Indian J Public Health Res Dev. 2020;11(2):238–242.
6. Rosalina IN, Widiastuti R. Family conflict and adolescent mental health: a study on high school students in Indonesia. J Asian Behav Stud. 2020;5(14):1–7.
7. Arifin EN, Utami ND, Rahayu E. Exposure to violence and trauma and its relationship with mental health among adolescents in Indonesia. J Public Health Africa. 2018;9(1):819.
8. Blakemore SJ. Adolescence and mental health. Lancet. 2019;393(10185):2030–2031. doi:10.1016/S0140-6736(19)31013-X
9. Veit CT, Ware JE. The structure of psychological distress and well-being in general populations. J Consult Clin Psychol. 1983;51(5):730. doi:10.1037/0022-006X.51.5.730
10. Aziz R. Aplikasi model raasch dalam pengujian alat ukur kesehatan mental di tempat Kerja [The application of the Raasch model in testing mental health measurement tools in the workplace]. Jurnal Psikologi Islam. 2015;12:1.
11. Tran TD, Kaligis F, Wiguna T, et al. Screening for depressive and anxiety disorders among adolescents in Indonesia: formal validation of the center for epidemiologic studies depression scale–revised and the Kessler psychological distress scale. J Affect Disord. 2019;246:189–194. doi:10.1016/j.jad.2018.12.042
12. Gebrie MH. An Analysis of Beck Depression Inventory.
13. Viejo C, Gómez-López M, Ortega-Ruiz R. Adolescents’ psychological well-being: a multidimensional measure. Int J Environ Res Public Health. 2018;15(10):2325. doi:10.3390/ijerph15102325
14. Akhtar H. Evaluasi properti psikometris dan perbandingan model pengukuran konstruk subjective well-being [Evaluation of psychometric properties and comparison of measurement models for subjective well-being constructs]. Jurnal Psikologi. 2019;18(1):29–40. doi:10.14710/jp.18.1.29-40
15. Clarke A, Friede T, Putz R, et al. Warwick-Edinburgh Mental Well-being Scale (WEMWBS): validated for teenage school students in England and Scotland. A mixed methods assessment. BMC Public Health. 2011;11:1–9. doi:10.1186/1471-2458-11-487
16. Khan Y, Taghdisi MH, Nourijelyani K. Psychological Well-Being (PWB) of school adolescents aged 12–18 yr, its correlation with general levels of Physical Activity (PA) and socio-demographic factors In Gilgit, Pakistan. Iran J Public Health. 2015;44(6):804–813.
17. Al Mutair A, Al Mohaini M, Fernandez R, Moxham L, Lapkin S, Ham‐Baloyi WT. Psychometric testing of the mental health inventory in an Arabian context: cross‐cultural validation study. Nurs Open. 2018;5(3):376–383. doi:10.1002/nop2.149
18. Mousavi A, VaezMousavi M, Yaghobi H. Psychometric properties of the Persian version of mental health inventory (mhi-38) in elite athletes. Sport Psychol Stud. 2015;4(11):27–40.
19. Liang J, Wu SC, Krause NM, Chiang TL, Wu HY. The structure of the mental health inventory among Chinese in Taiwan. Med Care. 1992;30(8):659–676. doi:10.1097/00005650-199208000-00001
20. Ryff CD. Eudaimonic well-being, inequality, and health: recent findings and future directions. Int Rev Econ. 2017;64(2):159–178. doi:10.1007/s12232-017-0277-4
21. Rapheal J, Paul V. Psychological well-being and anxiety among adolescents’ analysis along wellness: illness continuum. Int J Innov Res Dev. 2014;3(1):395–401.
22. Gómez-López M, Viejo C, Ortega-Ruiz R. Psychological well-being during adolescence: stability and association with romantic relationships. Front Psychol. 2019;10:1772. doi:10.3389/fpsyg.2019.01772
23. Shek DT, Lin L. Personal well-being and family quality of life of early adolescents in Hong Kong: do economic disadvantage and time matter? Soc Indic Res. 2014;117(3):795–809. doi:10.1007/s11205-013-0399-3
24. Abidin FA, Koesma RE, Joefiani P, Siregar JR. Pengaruh pengasuhan orangtua, kualitas pertemanan dan iklim sekolah terhadap kesejahteraan psikologis Remaja Indonesia usia 12–15 tahun Melalui kepuasan kebutuhan psikologis dasar [The influence of parenting, quality of friendships, and school climate on the psychological well-being of Indonesian adolescents aged 12-15 years through satisfaction of basic psychological needs]. J Psychol Sci Prof. 2020;4(1):1. doi:10.24198/jpsp.v4i1.24840
25. Ben-Arieh A, Casas F, Frønes I, Korbin JE. Multifaceted concept of child well-being. Handbook Child Well Being. 2014;1:1–27.
26. Copeland WE, Angold A, Shanahan L, Costello EJ. Longitudinal patterns of anxiety from childhood to adulthood: the great smoky mountains study. J Am Acad Child Adolesc Psychiatry. 2014;53(1):21–33. doi:10.1016/j.jaac.2013.09.017
27. Hetrick SE, Cox GR, Witt KG, Bir JJ, Merry SN. Cognitive behavioural therapy (CBT), third-wave CBT and interpersonal therapy (IPT) based interventions for preventing depression in children and adolescents. Cochrane Database Syst Rev. 2016;9:8.
28. Hernández A, Hidalgo MD, Hambleton RK, Gómez Benito J. International test commission guidelines for test adaptation: a criterion checklist. Psicothema. 2020;32(3):390–398. doi:10.7334/psicothema2019.306
29. Likert R. A technique for the measurement of attitudes. Arch Psychol. 1932;1932:1.
30. Muhid A, Suhadiyanto S, Nurhidayat D. Pengembangan alat ukur psikologi; 2015.
31. Hair JF
32. Kaplan RM, Saccuzzo DP. Psychological Assessment and Theory: Creating and Using Psychological Tests. Wadsworth Cengage Learning; 2013.
33. Hendryadi H. Content validity: early stage of questionnaire development. J Manag Bus Res. 2017;2(2):259334.
34. Shrotryia VK, Dhanda U. Measuring employee engagement: perspectives from literature. IUP J Organ Behav. 2019;18(3):1.
35. Chehri A, Brand S, Goldaste N, et al. Psychometric properties of the Persian Pittsburgh sleep quality index for adolescents. Int J Environ Res Public Health. 2020;17(19):7095. doi:10.3390/ijerph17197095
36. Tavakol M, Wetzel A. Factor analysis: a means for theory and instrument development in support of construct validity. Int J Med Educ. 2020;11:245. doi:10.5116/ijme.5f96.0f4a
37. Akoglu H. User’s guide to correlation coefficients. Turk J Emerg Med. 2018;18(3):91–93. doi:10.1016/j.tjem.2018.08.001
38. Hancock GR, Mueller RO. Rethinking construct reliability within latent variable systems. Struct Equ Modeling. 2001;195:216.
39. Polit DF, Beck CT. The content validity index: are you sure you know what’s being reported? Critique and recommendations. Res Nurs Health. 2006;29(5):489–497. doi:10.1002/nur.20147
40. Peacock GG, Ervin RA, Daly EJ, Merrell KW. Practical Handbook of School Psychology: Effective Practices for the 21st Century. Guilford Press; 2009.
41. Keyes CL. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J Consult Clin Psychol. 2005;73(3):539–548. doi:10.1037/0022-006X.73.3.539
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.