Back to Journals » Pharmacogenomics and Personalized Medicine » Volume 14
ADAMTS8 Expression is a Potential Prognostic Biomarker for Postoperative Metastasis in Lymph Node-Negative Early-Stage Invasive Breast Carcinoma Patients
Authors Li Y, Yang X, Sun J ![]() , Zhao Y, Zhou Q
, Zhao Y, Zhou Q ![]() , Hua B
, Hua B
Received 23 September 2021
Accepted for publication 15 December 2021
Published 30 December 2021 Volume 2021:14 Pages 1701—1713
DOI https://doi.org/10.2147/PGPM.S339919
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Yao Li,1,* Xin Yang,1,* Jie Sun,2 Yangyang Zhao,3 Qi Zhou,3 Bin Hua1
1Breast Center, Department of Thyroid-Breast-Hernia Surgery, Department of General Surgery, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 2Graduate School of Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 3The Key Laboratory of Geriatrics, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Hua
Breast Center, Department of Thyroid-breast-hernia Surgery, Department of General Surgery, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China
Tel +86-10-85136127
Fax +86-10-65132969
Email [email protected]
Purpose: Invasive breast carcinoma (BC) is the most common malignant breast tumor. Most lymph node-negative (LN−) early-stage BC patients usually have a good prognosis, but 7% of patients still develop metastasis after surgery. It is not yet clear how to screen candidates with poorer prognosis in LN− early-stage patients, so that they can receive intensive therapy. Hence, we expect to identify a prognostic biomarker to assess postoperative metastasis in LN− early-stage BC patients.
Patients and Methods: Screening and verifying of candidate genes by gene expression profiling of LN− early-stage BC samples (n = 640) from 3 independent public datasets. Univariable and multivariable Cox regression analyses showed the relation between the candidate genes and postoperative metastasis. Distant metastasis-free survival (DMFS) analysis was performed to examine the prognostic significance. Quantitative real-time polymerase chain reaction (qRT-PCR) assays were performed to examine ADAMTS8 expression and prognostic association in our clinical samples (n = 25).
Results: In the discovery cohort (TCGA and GSE20685 datasets), we found that ADAMTS8 tend to be low expression in LN− early-stage BC, and low ADAMTS8 expression was associated with postoperative metastasis and shortened DMFS. Moreover, the above finding was confirmed in the validation cohort (GSE6538 dataset). Lower ADAMTS8 expression was related to poorer prognostic clinical stage and PAM50 subtypes and shorter DMFS. Gene enrichment analysis indicated that ADAMTS8 may be correlated with BC metastasis. qRT-PCR assays of our clinical tumor sample showed that patients with low ADAMTS8 expression seem to be prone to developing metastasis and have a shorter DMFS time.
Conclusion: Our research shows that low ADAMTS8 expression is associated with postoperative metastasis and shortened DMFS in LN− early-stage BC patients, which suggests that ADAMTS8 may be a potential prognostic marker for postoperative metastasis in LN− early-stage BC patients.
Keywords: ADAMTS8, lymph node-negative early-stage invasive breast carcinoma, distant metastasis-free survival, biomarker
Introduction
Female breast cancer is the most commonly diagnosed cancer in the world, and more than 2.3 million women are diagnosed in 2020 and are still the leading cause of cancer death.1 Invasive breast carcinoma (BC) accounts for 80–90% of breast cancer and is the most common type of pathology and is a heterogeneous disease at the molecular level.2–5 In the last decade, systemic therapy, including endocrine therapy, anti-HER2 therapy, immunotherapy and chemotherapy, has achieved success in improving the clinical outcomes of BC patients after surgery, including early-stage BC.6–9 Although most lymph node-negative (LN−) early-stage BC patients have a good prognosis,10–12 postoperative metastasis still occurs. The risk of metastasis may be underestimated in this group of BC patients. Whether to intensify treatment for LN− early-stage BC patients remains controversial.7 Hence, it is necessary to define prognostic markers to assess the risk of postoperative metastasis in LN− early-stage BC patients.
Traditional clinical and pathological characteristics, such as patient age, tumor size, histological features, lymph node status, and molecular subtypes, can predict the outcomes of breast cancer but are not accurate, which will cause over- or undertreatment.13,14 With the development of bioinformatics, all kinds of gene signatures, including intrinsic molecular subtypes, 21-gene recurrence scores (RS) and MammaPrint 70 genetic testing, were used to predict the risk of postoperative metastasis in patients with early-stage breast cancer.15–18 We found that most studies on early-stage breast cancer outcomes involve all stage I–II BC patients, according to the definition of early-stage BC,5 but few studies have focused only on LN− early-stage BC patients.9,19–21
In this study, we compared the gene expression profiles of patients (n = 640) between postoperative metastatic and non-metastatic LN− early-stage BC patients from The Cancer Genome Atlas (TCGA provisional dataset, 2021) and Gene Expression Omnibus (GEO) databases.22,23 After a series of rigorous bioinformatics screenings and analyses, we determined that low ADAMTS8 expression correlated with shortened distant metastasis-free survival (DMFS) in these patients. Furthermore, qRT–PCR assays were used to test the relationship between ADAMTS8 expression levels and DMFS in our clinical samples (n = 25) with a matched case study. Finally, we identified ADAMTS8 as a potential prognostic marker for postoperative metastasis in LN− early-stage BC, although there were several limitations in our study; for example, our clinical sample size was small.
Materials and Methods
Data Extraction
Transcriptome and clinical data from BC patients were downloaded from TCGA (https://portal.gdc.cancer.gov/), and the microarray gene expression profiles and clinical data were retrieved from the GEO (GSE20685, GSE6532) (https://www.ncbi.nlm.nih.gov/gds) database. Patients who met the following criteria were included: (1) female patients were diagnosed with BC between the ages of 20–85 years; (2) LN− status at diagnosis; (3) the size of the primary tumors was T1-T3 stage; (4) no distant metastasis; (5) patients accepted standard systemic therapy; and (6) metastatic status was recorded at the end of follow-up. Patients with only local or regional recurrence were excluded from this study. The discovery cohorts TCGA (n = 390) and GSE20685 (n = 131, Affymetrix Human Genome U133 Plus 2.0 Array (GPL570)) datasets were used as cohorts to identify common differentially expressed genes (DEGs) and detect the correlation between common DEGs and postoperative metastatic and DMFS time. The testing cohort (GSE6532 dataset; n = 119; Affymetrix Human Genome U133 (GPL96)) was used to verify the differences in expression and prognostic value of the DEGs. The detailed clinical information of the three datasets is included in Supplementary Table S1.
Data Processing
The raw counts of RNA-sequencing data from the TCGA dataset were corrected and normalized using the R package “limma”. Preprocessing procedures were used to process raw data of the Affymetrix microarray in the GSE20685 and GSE6532 datasets, including RMA background correction, and the “affy” R package was also applied to complete log2 transformation, quantile normalization and median polishing algorithm summarization. Probes were annotated by the Affymetrix annotation files. The PAM50 gene expression data in TCGA and GES20685 were extracted and applied against reference data of median gene expression to bin each sample into the intrinsic molecular subtypes of BC patients using the “genefu” R package. The detailed candidate gene screening process is shown in Figure 1. All data analyses and screening procedures referred to the RECIST criteria.24,25
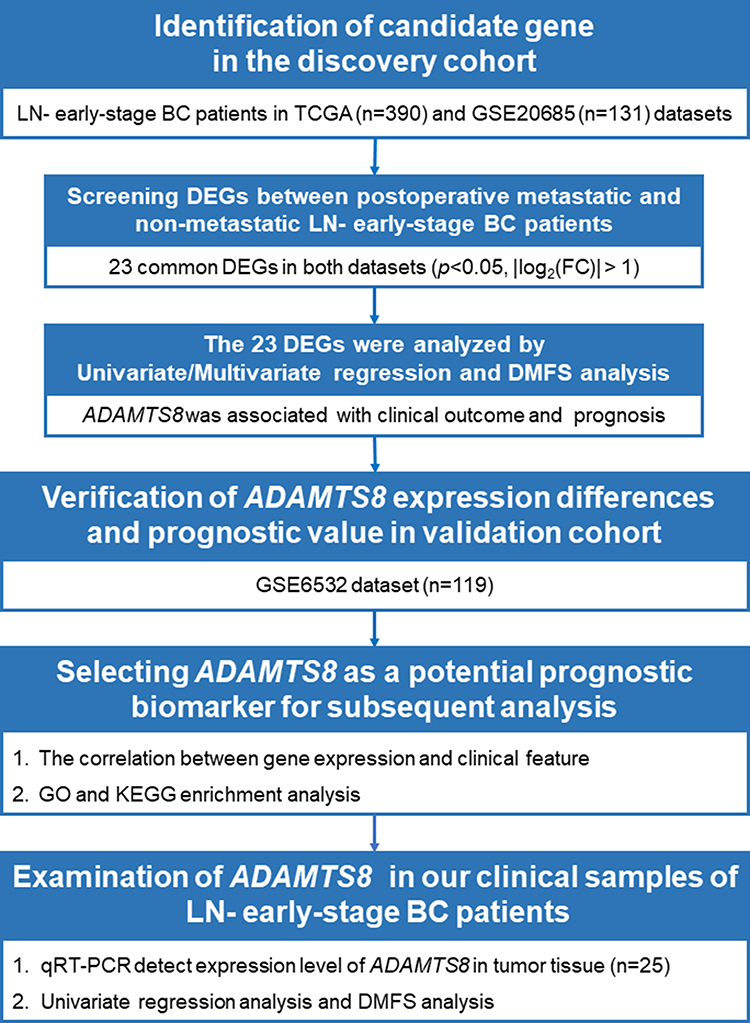 |
Figure 1 Study workflow. Abbreviations: LNN, lymph node-negative; BC, invasive breast carcinoma; DEGs, differentially expressed genes; DMFS, distant metastasis-free survival; log2(FC), log2(fold change); qRT–PCR, quantitative real-time polymerase chain reaction. |
Analysis of Differentially Expressed Genes
In the discovery cohort, the common DEGs were screened between postoperative metastatic patients and non-metastatic patients. The differences in expression of the final candidate genes were validated in the validation cohort. The filtering condition for all DEGs was p<0.05 and |log2fold change (FC)| > 1.
Univariate and Multivariate Cox Regression Analysis
The common DEGs with significant differences in univariate analysis were entered into multivariate analysis. Multivariate Cox regression with forward stepwise regression was performed to investigate the impact of independent factors on postoperative metastasis, and the hazard ratios (HRs) with 95% confidence intervals (CIs) and p values are reported.
Distant Metastasis-Free Survival Analysis
The data of postoperative metastasis in LN− early-stage patients were used to calculate DMFS. DMFS analysis was conducted to test the ability of the DEGs to predict the prognosis of LN− early-stage BC patients in the discovery cohort, in the testing cohort, and in our LN− early-stage BC tumor specimen. Kaplan–Meier survival curves were used to compare the high and low expression groups according to the hazard ratio (HR) and log-rank p value.
Gene Ontology and Pathway Enrichment Analysis
To explore the potential molecular biological functions of ADAMTS8, we used the online bioinformatic tool DAVID (https://david.ncifcrf.gov/)26 to analyze the enrichment of Gene Ontology (GO)27 and pathway (KEGG)28 between the high and low ADAMTS8 expression groups using the TCGA and GSE20685 datasets (p<0.05).
Examination in Our Clinical Tumor Specimens of LN− Early-Stage BC Patients
We examined the candidate gene expression levels in clinical tumor specimens obtained from breast tumor tissue removed during surgery and stored in liquid nitrogen in the Breast Centre of Beijing Hospital. The sample screening criteria were consistent with the patient screening criteria in the Data Extraction section. The follow-up time was from surgical resection of the tumor to May 2021.
We found 8 LN− early-stage patients who developed postoperative metastasis in our sample library. We matched each metastatic patient according to their molecular subtype, age, and date of surgery to approximately 2 non-metastatic patients as controls (n = 17). A total of 25 patient information and matching methods were showed in Supplementary Table S3.
We extracted total RNA of tumor specimens using RNAiso Plus (TaKaRa). qRT–PCR assays were performed to detect GAPDH and ADAMTS8 mRNA using the PrimeScript RT reagent Kit and SYBR Premix Ex Taq (TaKaRa). The primers for qPCR were as follows: GAPDH: forward 5ʹ-GGAGCGAGATCCCTCCAAAAT-3ʹ, reverse 5ʹ-GGCTGTTGTCATACTTCTCATGG-3ʹ; ADAMTS8: forward 5ʹ-GTGGCAGCCCGAATCYACAAGCA-3ʹ, reverse 5ʹ-AGTGTAAGCCCCCCATTGTCGGA-3ʹ. GAPDH was used as control. The relative expression levels of ADAMTS8 mRNAs were calculated and quantified using the 2−ΔΔct method.29
Statistical Analysis
DEG analysis was conducted on the TCGA datasets using the “edgeR” R package and on the GEO datasets using the “limma” R package. We used the “survival” and “survminer” R packages to draw Kaplan–Meier survival curves and compared the high and low expression groups according to the log-rank p value. Univariate and multivariate Cox regression analyses with forward stepwise regression based on the likelihood ratio test (forward LR model) were performed to investigate the impact of independent factors on DMFS, and the hazard ratios (HRs) with 95% confidence intervals (CIs) and p values are reported.
SPSS version 25 (IBMCorp, Armonk, N.K. USA) and R software version 4.0.5 (R core Team, Vienna, Austria) were used to statistically analyze the data. The chi-squared test or Fisher’s exact probability test was used to process the categorical variables, and t-test, ANOVA test or the Mann–Whitney U-test was used to process the continuous variables. Linear regression models were used to detect linear trends. A value of p < 0.05 was considered statistically significant.
Results
Data Collection
A total of 640 LN− early-stage BC patients were collected in public databases. In the TCGA dataset (n = 390), 23 patients developed distant metastasis, and 367 patients were included as a negative control. In the GES20685 dataset (n = 131), 12 patients developed distant metastasis, and 119 patients were included as a negative control. In the GSE6532 dataset (n = 119), 10 patients developed distant metastasis, and 109 patients were included as a negative control. The clinical information is summarized in Supplementary Table S1.
Identification of Candidate Gene in the Discovery Cohort
In the discovery cohort, a total of 893 and 314 DEGs were extracted from the TCGA and GES20685 datasets, respectively. Nine common DEGs were upregulated, and 14 common DEGs were downregulated in both datasets (Figure 2A and B). Twenty-three common DEGs in the GSE20685 dataset are presented as a heatmap in Figure 2C.
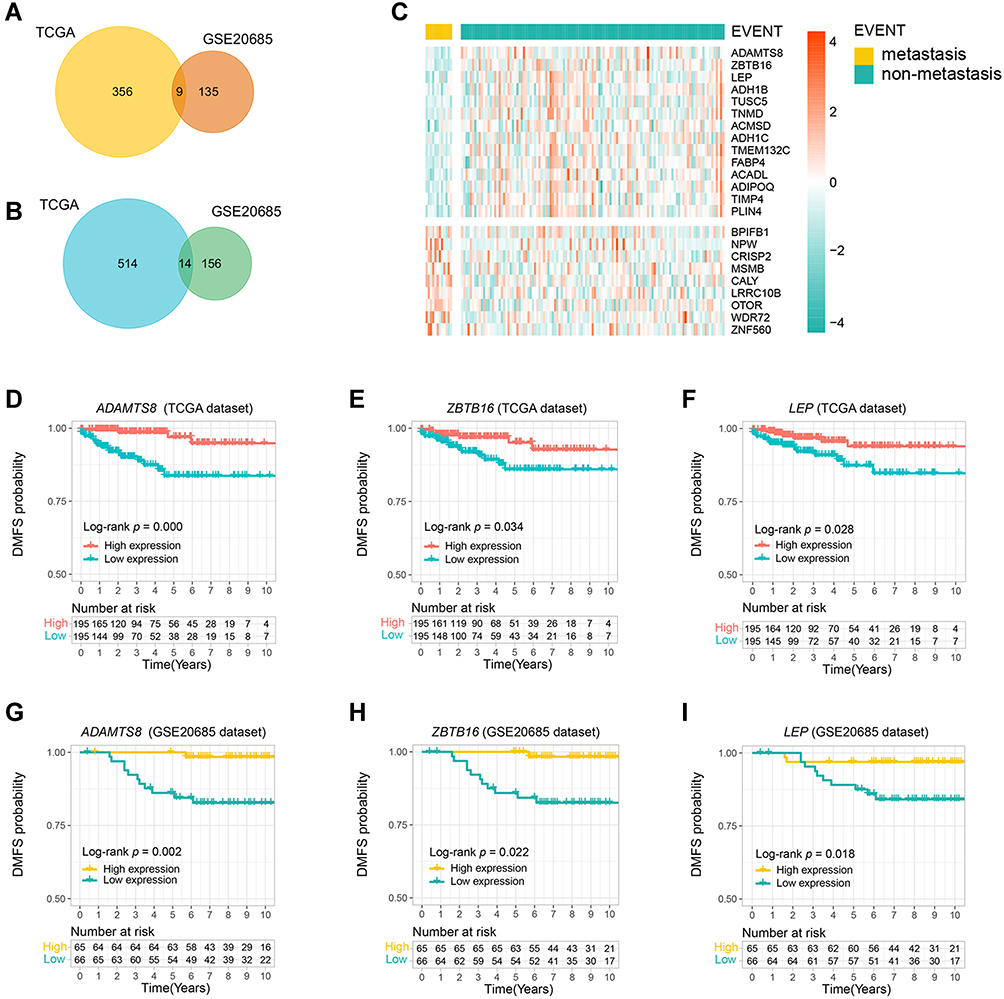 |
Figure 2 Low ADAMTS8 expression was correlated with a reduced postoperative distant metastasis-free survival (DMFS) time in LNN early-stage BC patients. (A and B) A total of 23 genes were simultaneously differentially expressed in both discovery cohorts (TCGA and GSE20685), 9 DEGs were upregulated in postoperative metastasis patients, and 14 DEGs were downregulated in postoperative metastasis patients. (C) The heatmap shows significant differences of the 23 DEGs in the GSE20685 dataset. Kaplan–Meier curves of DMFS between the high and low expression groups in the discovery cohort stratified by 3 genes: (D and G) stratified by ADAMTS8, (E and H) stratified by ZBTB16, (F and I) stratified by LEP. |
Then, Kaplan–Meier curves of DMFS analysis showed that only 3 of the 23 common DEGs were significantly associated with the prognosis, including ADAMTS8 (TCGA: log-rank p = 0.000; GSE20685: log-rank p = 0.002), ZBTB16 (TCGA: log-rank p = 0.034; GSE20685: log-rank p = 0.022), and LEP (TCGA: log-rank p = 0.028; GSE20685: log-rank p = 0.018), and their low expression suggested shorter DMFS times in both datasets (Figure 2D–I).
In addition, the 23 common DEGs were analyzed by univariate and multivariate Cox regression (Table 1). We found that low ADAMTS8 expression was a high risk factor for postoperative metastasis in both discovery datasets (TCGA: HR = 5.637 [1.915–16.595], p = 0.002; GSE20685: HR = 14.550 [1.853–114.230], p = 0.011).
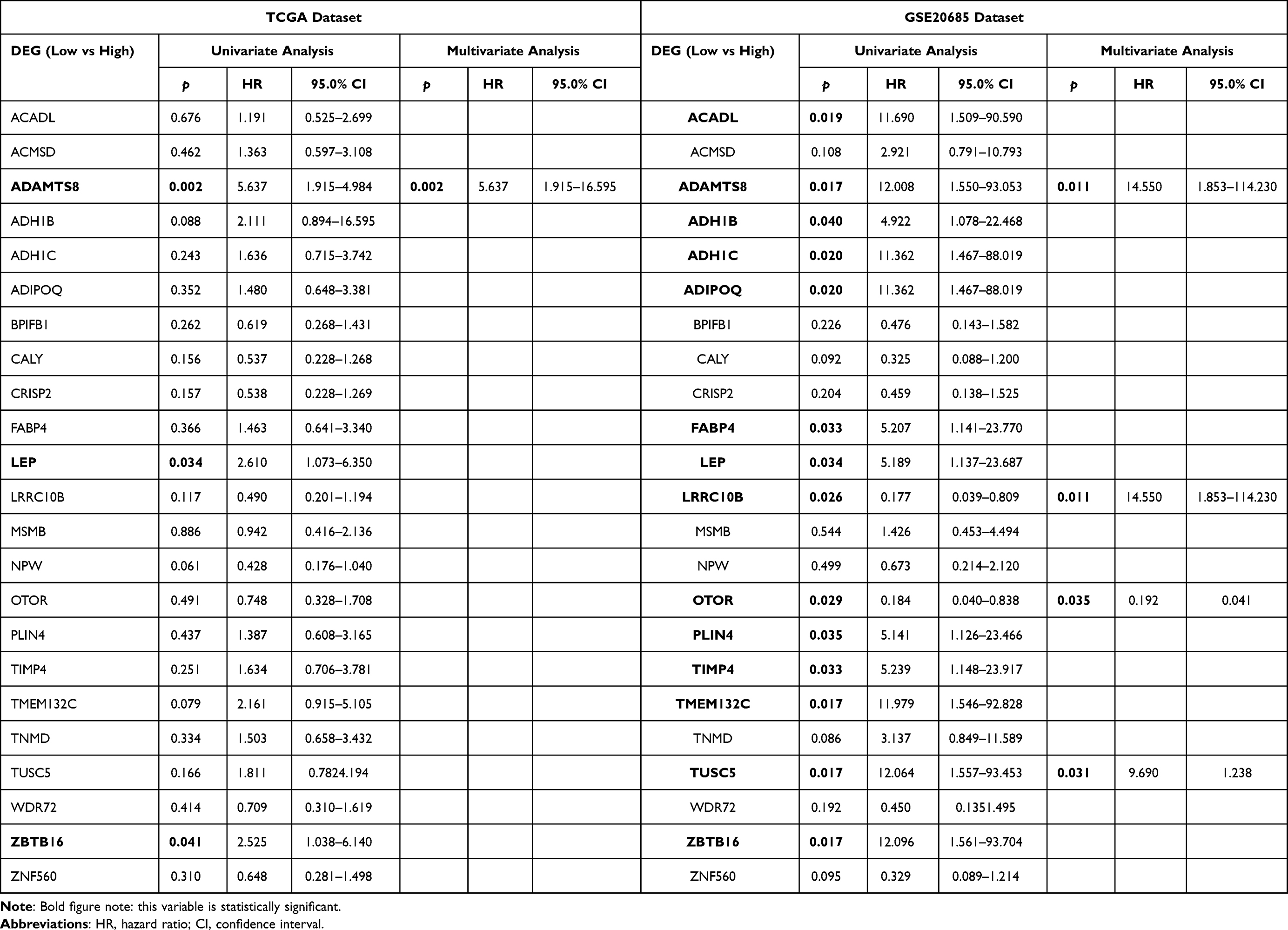 |
Table 1 Univariate and Multivariate Cox Regression (Forward LR Model) Analysis the 23 Common DEGs to Detect the Correlation Between DEGs Expression Levels and Clinical Outcome of LN− Early-Stage BC Patients |
Furthermore, we combined the expression level of ADAMTS8 and standard clinical prognostic variables (age, PAM50 and stage), regardless of their statistical significance, into the multivariate Cox regression analysis in the TCGA and GSE20685 datasets (Table 2). The results showed that the expression level of ADAMTS8 was an independent prognostic factor correlated with DMFS in both datasets (TCGA: HR = 0.136 [0.038–0.493], p = 0.002; GSE20685: HR = 0.119 [0.014–0.977], p = 0.047).
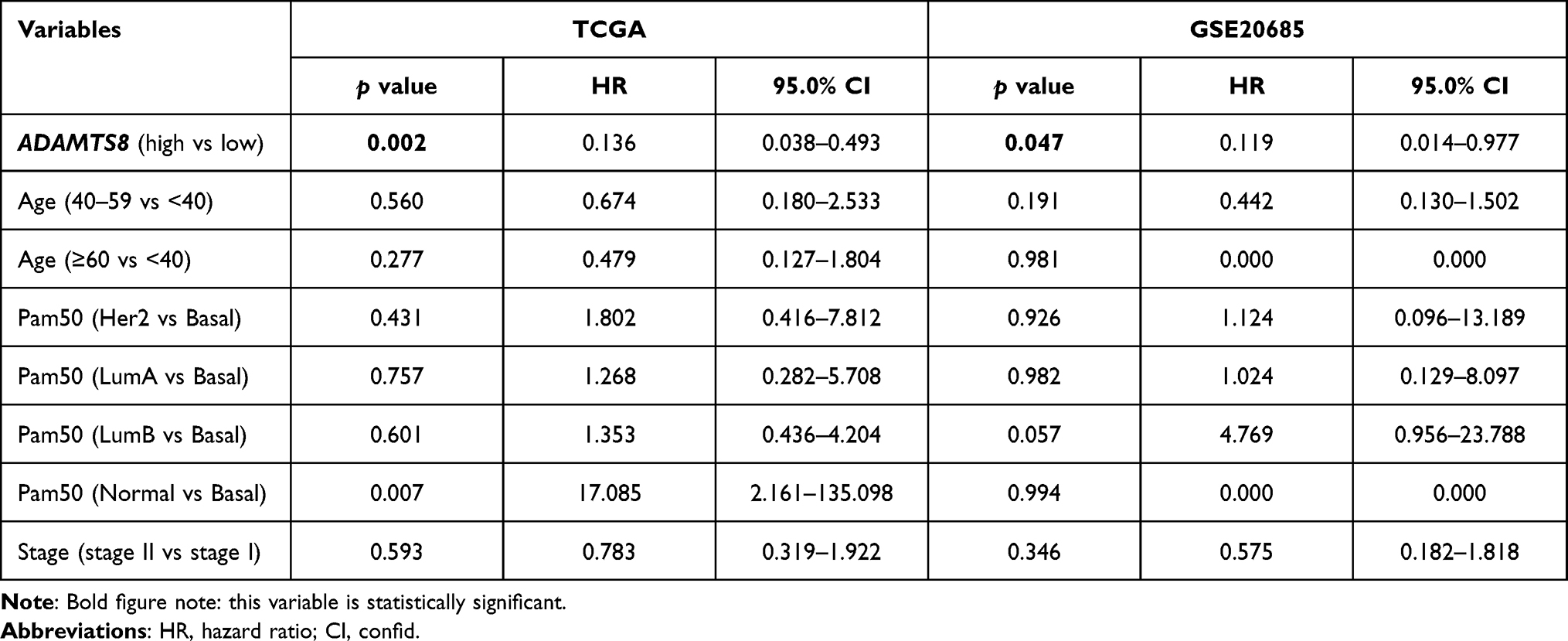 |
Table 2 Multivariable Cox Regression Analyses of ADAMTS8 in TCGA and GSE20685 Datasets |
In conclusion, we found that only ADAMTS8 appeared to be reduced in LN− early-stage BC patients with metastasis, and its low expression was associated with postoperative metastasis and shortened DMFS time. Thus, we focused attention on ADAMTS8 in this study.
Verification of Prognostic Value of ADAMTS8 in the Validation Cohort
In the validation cohort (GSE6532), we found that the expression level of ADAMTS8 was lower than that in metastatic patients (Figure 3A, log2(metastasis/non-metastasis) = −1.621, p = 0.000). Patients with low ADAMTS8 expression had an increased risk of metastasis (GSE6532: HR=9.416 [1.193–74.328], p = 0.033). In addition, the lower the ADAMTS8 expression was, the shorter the DMFS time (Figure 3B, log-rank p = 0.009).
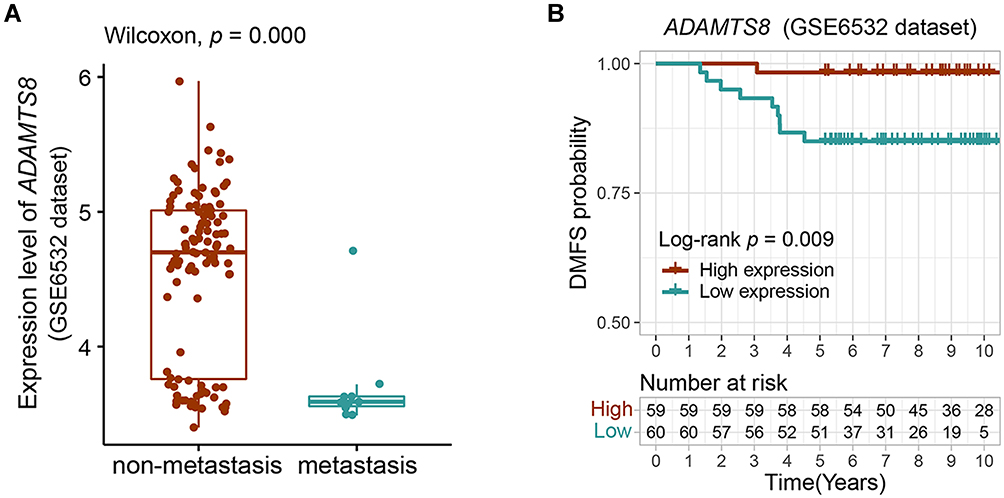 |
Figure 3 Verification of difference in expression and prognostic value of ADAMTS8 in the validation cohort. (A) The expression level of ADAMTS8 in metastatic and non-metastatic LN− early-stage BC patients. (B) Kaplan–Meier curves of DMFS between the ADAMTS8 high and ADAMTS8 low expression groups. |
The results in the discovery and validation cohorts imply the potential ability of ADAMTS8 to predict the outcomes of LN− early-stage BC patients.
Analysis of the Correlation Between ADAMTS8 Gene Expression and Clinical Features
First, we studied the difference in the distribution of clinical features, including age, tumor size, clinical stage, molecular subtypes and DMFS, between ADAMTS8 high and low expression in TCGA and GSE20685 datasets. As there were no molecular subtypes of BC patients in the datasets, we used the PAM50 gene set to define the intrinsic molecular subtypes of BC patients as luminal A (LumA), luminal B (LumB), HER2-enriched (Her2), basal-like (basal), and normal-like (normal).17 The detailed clinical data are presented in Supplementary Table S1, and the PAM50 hierarchical clustering of TCGA and GSE20685 datasets is presented by heatmaps in Figure 4A and Supplementary Figure S1A, respectively. There were obvious differences in the distribution of clinical stage, PAM50 subtypes and DMFS performance status in both datasets, but there were no common significant differences between ADAMTS8 expression and age and tumor size in both datasets at the same time. Among all patients, the expression trend of ADAMTS8 was lower in stage II patients than in stage I patients (Figure 4B; Supplementary Figure S1B), and more than half of the stage II patients (TCGA: 56.3%; GSE20685: 59.1%) had low ADAMTS8 expression (Table 3). The expression trend of ADAMTS8 was lower in the non-LumA subtype than in the LumA subtype (Figure 4C; Supplementary Figure S1C), and less than half of the LumA patients (TCGA: 24.4%; GSE20685: 41.2%) had low ADAMTS8 expression (Table 3). Next, we grouped the TCGA and GSE20685 datasets by DMFS. We identified ADAMTS8 expression in the subgroups of patients with metastasis within 3 years, metastasis after 3 years and non-metastasis. Patients with follow-up times less than 3 years were excluded. The detailed clinical data are presented in Supplementary Table S2. We found that the expression trend of ADAMTS8 between the three subgroups was significantly different, and the linear trend test p<0.05 (Figure 4D, Kruskal–Wallis p = 0.003, linear trend test p = 0.005; Supplementary Figure S1D, Kruskal–Wallis p = 0.043, linear trend test p = 0.034). The patients in the metastasis within 3 years subgroup exhibited the lowest ADAMTS8 expression trend, which implied that the lower the ADAMTS8 expression was, the shorter the DMFS time.
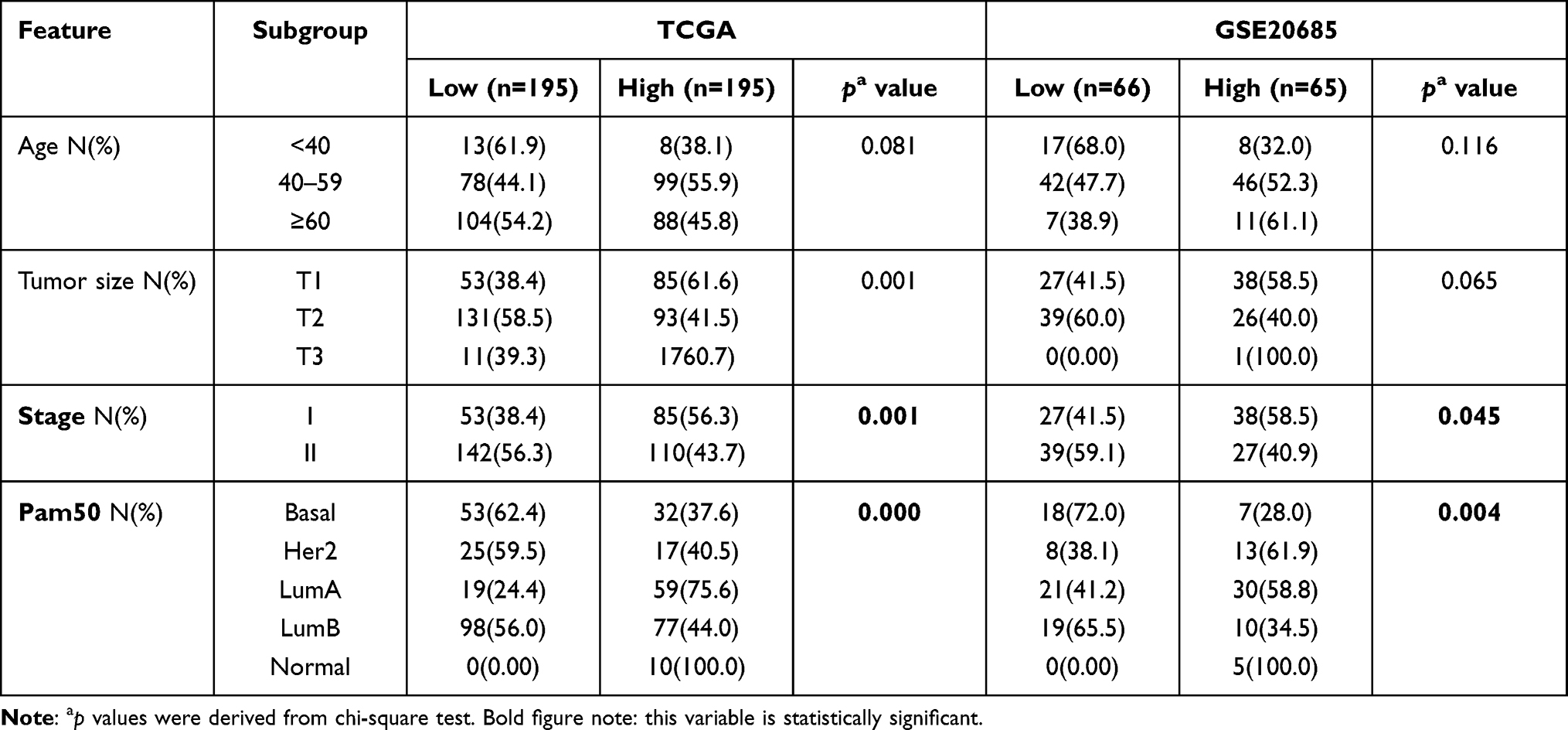 |
Table 3 Clinical Features of the Patients in TCGA and GSE20685 Datasets and Correlation of ADAMTS8 Expression in LN− Early-Stage BC Patients |
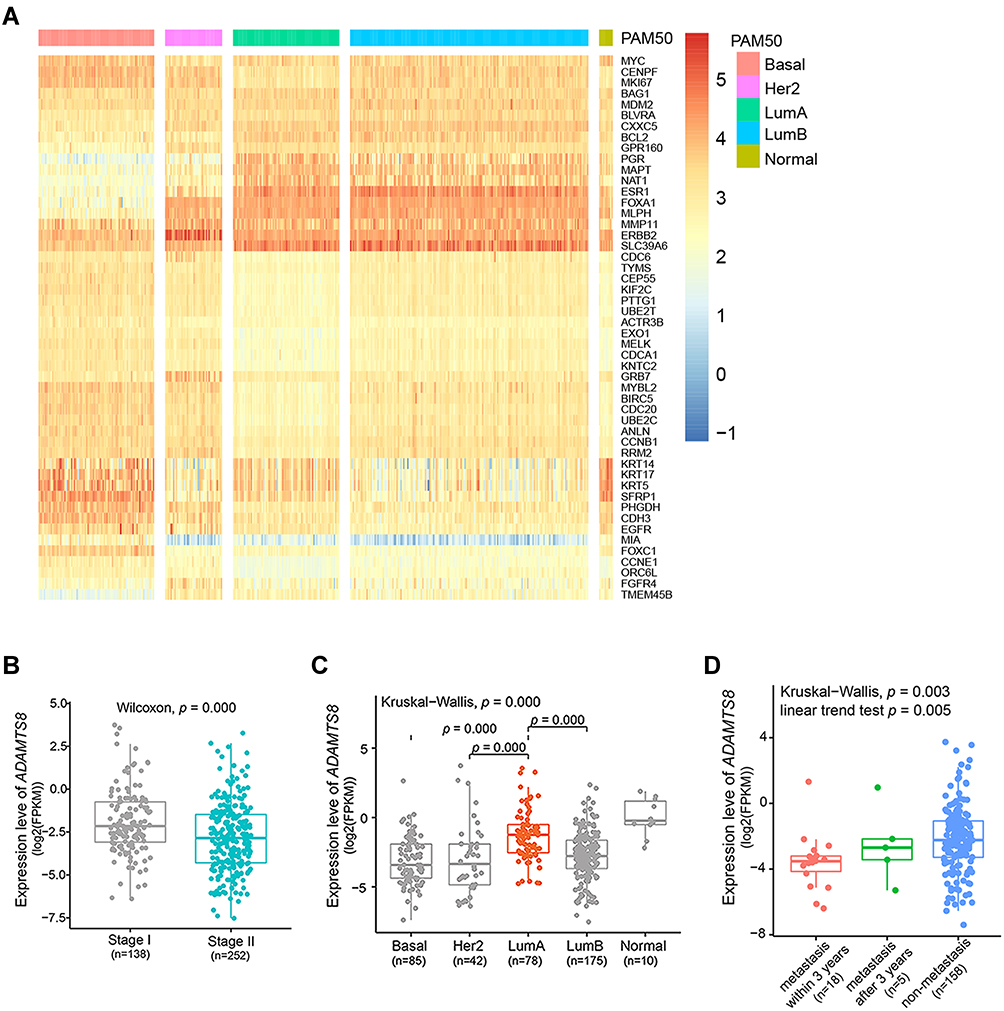 |
Figure 4 Lower ADAMTS8 expression was related to poorer prognostic clinical stage and PAM50 subtypes and shorter DMFS time in the TCGA dataset. (A) PAM50 gene expression hierarchical in a heatmap. (B–D) Boxplots showing the distribution of ADAMTS8 expression in patients stratified by clinical stage, PAM50 subtype and DMFS time performance status. |
GO and KEGG Analysis Reveals the Cell Signaling Pathways of ADAMTS8
All DEGs between the high ADAMTS8 expression groups and the low ADAMTS8 expression groups were analyzed by DAVID software and the GO and KEGG results (p < 0.05). As shown in Figure 5A–D, the DEGs were significantly enriched in GO terms and KEGG pathways, including ECM-receptor interaction, focal adhesion, angiogenesis, PI3K-AKT signaling pathway, cell proliferation and cell cycle, which showed that ADAMTS8 may participate in the development and metastasis of BC through these pathways.
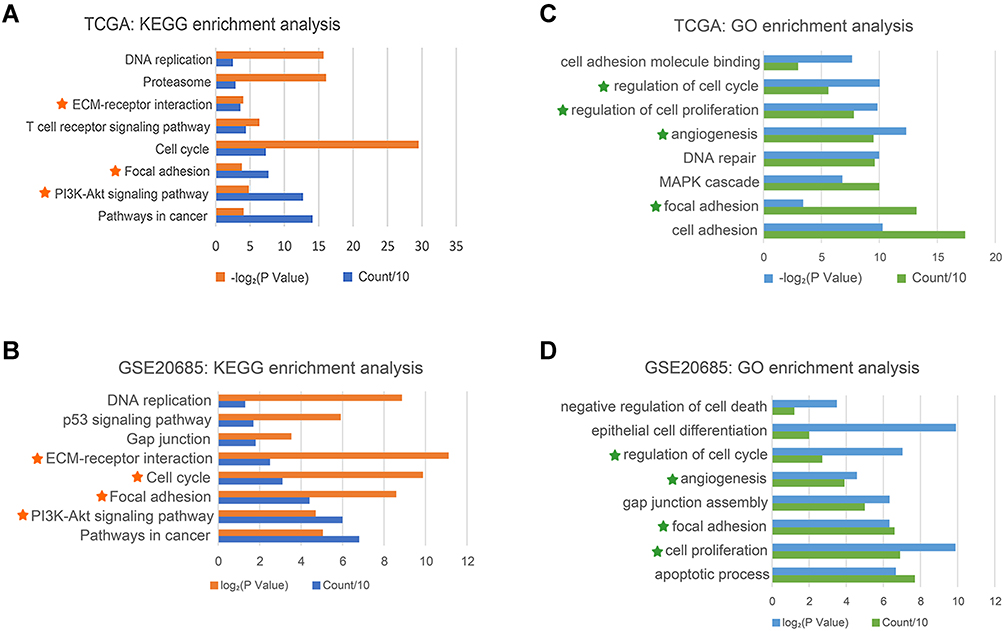 |
Figure 5 Gene ontology and pathway enrichment analysis showed that ADAMTS8 may participate in the development and metastasis of IDC. GO and KEGG analyses revealed the biological function of ADAMTS8 in the TCGA dataset (A and C) and in the GSE20685 dataset (B and D). Pentagram marks indicate simultaneous enrichment of two datasets. |
Examining ADAMTS8 Expression Level and Its Association with Prognosis in Our Clinical Specimens of LN− Early-Stage BC
The expression levels of ADAMTS8 were detected by qRT–PCR in 25 LN− early-stage BC tumor tissue samples. The median age of the enrolled patients was 59 years, the oldest 73 years and the youngest 36 years. The median distant metastasis-free survival time for 8 patients who developed metastases was 3.41 years (range: 1.17–4.92 years), and for 17 non-metastatic patients, it was 6.17 years (range: 4.92–7.83 years). All patients had undergone surgery and accepted systemic therapy. The detailed clinical information of 25 patients is included in Supplementary Table S3.
The results showed that the mRNA expression levels of ADAMTS8 were lower in patients who developed metastases (Figure 6A, WilCoxon p = 0.009). Univariate Cox regression showed that low ADAMTS8 expression was related to metastasis developed (HR = 8.639 [1.059–70.503], p = 0.044). Low expression of ADAMTS8 was related to shortened DMFS compared with high ADAMTS8 expression (Figure 6B, log-rank p = 0.015). There was no correlation between ADAMTS8 expression and clinical features except DMFS, and the metastatic patients within 3 years were all concentrated in low ADAMTS8 expression (Supplementary Table S4).
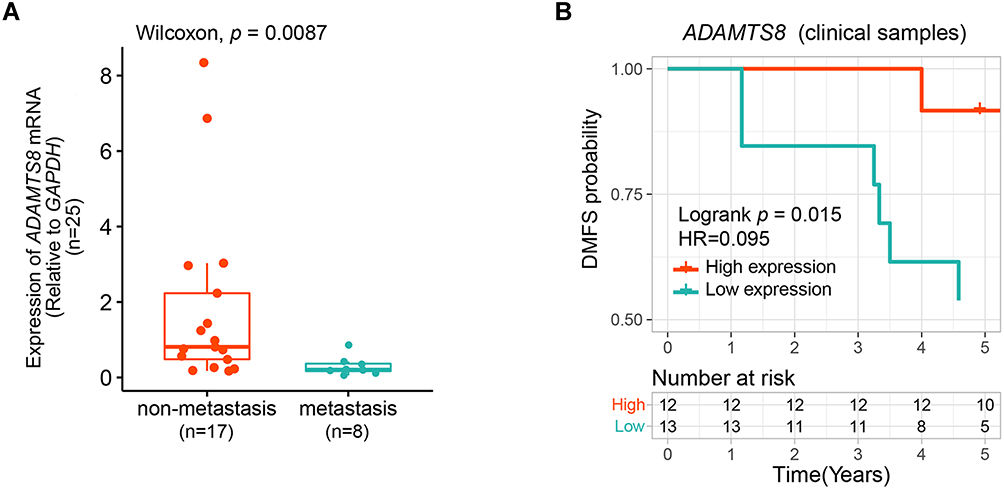 |
Figure 6 ADAMTS8 is a potential prognostic biomarker for DMFS in real clinical samples of LNN early-stage BC patients. (A) qRT–PCR assays of the expression level of ADAMTS8 in BC tumor samples. (B) Kaplan–Meier curves of DMFS between the ADAMTS8 high and ADAMTS8 low expression groups. |
Discussion
In three independent datasets, we compared the gene expression profiles of LN− early-stage BC patients between the metastatic group and the non-metastatic group to identify DEGs and found for the first time that low ADAMTS8 expression is correlated with postoperative metastasis and shortened DMFS in this group of patients. In our clinical tumor specimens, we detected ADAMTS8 expression levels in LN− early-stage BC patients by qRT–PCR. The results showed that ADAMTS8 was significantly lower in patients who developed postoperative metastases. Downregulation of ADAMTS8 was related to shorter DMFS.
ADAMTS8 is a member of the ADAMTS family known to have antiangiogenic properties. It has been shown to specifically inhibit endothelial growth factor VEGF-mediated angiogenesis in endothelial cells in vitro.30 Some studies have demonstrated that ADAMTS8 displays antitumor properties by antagonizing EGFR-MEK-ERK signaling.31 Increasing evidence has indicated that ADAMTS8 is an antioncogene in some cancers,32–35 including breast cancer. Some studies have demonstrated that ADAMTS8 inhibits cell proliferation and invasion and induces apoptosis in breast cancer (BC).36 Another study demonstrated that ADAMTS8 combined with ADAMTS15 or 16 other immune genes was associated with overall survival in BC.37,38 However, to the best of our knowledge, no studies have reported the prognostic value of the ADAMTS8 expression level for postoperative metastasis in LN− early-stage BC patients.
In TCGA and GSE20685 datasets, correlation analysis between ADAMTS8 expression and clinical features indicated that the prediction results of ADAMTS8 on patient prognosis were consistent with traditional prognostic indicators, including clinical stage, PAM50 subtypes and DMFS. In general, stage II patients are considered to have a worse prognosis than stage I patients. LN− LumA patients, which have the lowest proliferative ability of tumor cells and are sensitive to endocrine therapy, are considered to have the best prognosis.39–41 The shorter DMFS, the poorer prognosis. In our study, lower ADAMTS8 expression was related to poorer prognostic clinical stage and PAM50 subtypes and shorter DMFS. In our clinical samples, DMFS stratification of ADAMTS8 expression showed similar results, and the metastatic patients within 3 years all had low ADAMTS8 expression. No other clinical features were significantly different between high and low ADAMTS8 expression, which may be due to our small clinical sample size.
To better understand the function of ADAMTS8, we performed GO and KEGG enrichment analysis, which showed that the DEGs between ADAMTS8 low expression ADAMTS8 and high expression were significantly enriched in ECM-receptor interaction, PI3K-AKT signaling pathway,42–44 focal adhesion, and angiogenesis.45–48 The PI3K-AKT pathway is a downstream effector of the ECM-receptor pathway, and the results implied that breast tumor cell metastasis in patients with low ADAMTS8 expression could be associated with ECM-receptor interactions and PI3K-AKT pathway activation, which has never been reported. However, further experiments are needed to directly test this hypothesis.
There were several limitations await to be addressed in our study. First, the sample size was insufficient for multivariate Cox regression analysis and in the stratified analysis of clinical features in our clinical samples. Second, no further experiments explored the role of ADAMTS8 in breast cancer cell movement and metastasis.
Conclusion
In conclusion, we first found that the downregulated expression of ADAMTS8 was associated with LN− early-stage BC patients prone to developing postoperative metastasis. We validated that ADAMTS8 could be a potential biomarker for postoperative metastasis in LN− early-stage BC patients, and it is helpful to screen candidates with poorer prognosis in LN− early-stage patients so that they can receive intensive therapy.
Ethics Statement
The clinical tumor specimens from LN− early-stage BC patients were collected from the Breast Cancer Biobank of the Breast Centre at Beijing Hospital. The study protocol was approved by the Ethics Committee of Beijing Hospital on the basis of the Declaration of Helsinki (IRB Number in Ethical approval: 2017BJYYEC-086-02), and written informed consent was obtained from the patients.
Funding
Beijing Hospital Clinical Research 121 Project(Project Number: BJ-2019-191); Beijing Hospital Project (Project Number: BJ-2021-212).
Disclosure
The authors declare there are no competing interest.
References
1. Lei S, Zheng R, Zhang S, et al. Global patterns of breast cancer incidence and mortality: a population-based cancer registry data analysis from 2000 to 2020. Cancer commun. 2021;41(11):1183–1194. doi:10.1002/cac2.12207
2. Koboldt DC, Fulton R, McLellan M, et al.Comprehensive molecular portraits of human breast tumours. Nature. 2012;490(7418):61–70. doi:10.1038/nature11412
3. Waks AG, Winer EP. Breast cancer treatment: a review. JAMA. 2019;321(3):288–300. doi:10.1001/jama.2018.19323
4. Cserni G. Histological type and typing of breast carcinomas and the WHO classification changes over time. Pathologica. 2020;112(1):25–41. doi:10.32074/1591-951X-1-20
5. Harbeck N, Penault-Llorca F, Cortes J, et al. Breast cancer. Nat Rev Dis Primers. 2019;5(1):66. doi:10.1038/s41572-019-0111-2
6. Harbeck N, Gnant M. Breast cancer. Lancet. 2017;389(10074):1134–1150. doi:10.1016/S0140-6736(16)31891-8
7. Shah C, Smith BD, Royce TJ. Balancing treatment deintensification strategies in early stage breast cancer. Int J Radiat Oncol Biol Phys. 2020;107(5):959–963. doi:10.1016/j.ijrobp.2020.04.037
8. Korde LA, Somerfield MR, Carey LA, et al. Neoadjuvant chemotherapy, endocrine therapy, and targeted therapy for breast cancer: ASCO guideline. Int J Cancer. 2021;39(13):1485–1505. doi:10.1200/JCO.20.03399
9. Agostinetto E, Rediti M, Fimereli D, et al. HER2-low breast cancer: molecular characteristics and prognosis. Cancers. 2021;13(11):2824. doi:10.3390/cancers13112824
10. Pan H, Gray R, Braybrooke J, et al. 20-year risks of breast-cancer recurrence after stopping endocrine therapy at 5 years. N Engl J Med. 2017;377(19):1836–1846. doi:10.1056/NEJMoa1701830
11. Chu QD, Hsieh MC, Lyons JM, Wu XC. 10-year survival after breast-conserving surgery compared with mastectomy in Louisiana women with early-stage breast cancer: a population-based study. J Am Coll Surg. 2021;232(4):607–621. doi:10.1016/j.jamcollsurg.2020.11.011
12. Choi HY, Park M, Seo M, Song E, Shin SY, Sohn YM. Preoperative axillary lymph node evaluation in breast cancer: current issues and literature review. Ultrasound Q. 2017;33(1):6–14. doi:10.1097/RUQ.0000000000000277
13. Curigliano G, Burstein HJ, Winer EP, et al. De-escalating and escalating treatments for early-stage breast cancer: the St. Gallen International expert consensus conference on the primary therapy of early breast cancer 2017. Ann Oncol. 2017;28(8):1700–1712. doi:10.1093/annonc/mdx308
14. Harris LN, Ismaila N, McShane LM, et al. Use of biomarkers to guide decisions on adjuvant systemic therapy for women with early-stage invasive breast cancer: American society of clinical oncology clinical practice guideline. Int J Cancer. 2016;34(10):1134–1150. doi:10.1200/JCO.2015.65.2289
15. Cardoso F, Van’t Veer LJ, Bogaerts J, et al. 70-gene signature as an aid to treatment decisions in early-stage breast cancer. N Engl J Med. 2016;375(8):717–729. doi:10.1056/NEJMoa1602253
16. Albain KS, Barlow WE, Shak S, et al. Prognostic and predictive value of the 21-gene recurrence score assay in postmenopausal women with node-positive, oestrogen-receptor-positive breast cancer on chemotherapy: a retrospective analysis of a randomised trial. Lancet Oncol. 2010;11(1):55–65. doi:10.1016/S1470-2045(09)70314-6
17. Parker JS, Mullins M, Cheang MC, et al. Supervised risk predictor of breast cancer based on intrinsic subtypes. Int J Cancer. 2009;27(8):1160–1167. doi:10.1200/JCO.2008.18.1370
18. Krop I, Ismaila N, Andre F, et al. Use of biomarkers to guide decisions on adjuvant systemic therapy for women with early-stage invasive breast cancer: American society of clinical oncology clinical practice guideline focused update. Int J Cancer. 2017;35(24):2838–2847. doi:10.1200/JCO.2017.74.0472
19. Kwa M, Makris A, Esteva FJ. Clinical utility of gene-expression signatures in early stage breast cancer. Nat Rev Clin Oncol. 2017;14(10):595–610. doi:10.1038/nrclinonc.2017.74
20. Zhu Y, Wang T, Tong Y, Chen X, Shen K. 21-gene recurrence assay associated with favorable metabolic profiles in HR-positive, HER2-negative early-stage breast cancer patients. Front Endocrinol. 2021;12:725161. doi:10.3389/fendo.2021.725161
21. Kok M, Koornstra RH, Mook S, et al. Additional value of the 70-gene signature and levels of ER and PR for the prediction of outcome in tamoxifen-treated ER-positive breast cancer. Breast. 2012;21(6):769–778. doi:10.1016/j.breast.2012.04.010
22. Barrett T, Wilhite SE, Ledoux P, et al. NCBI GEO: archive for functional genomics data sets–update. Nucleic Acids Res. 2013;41(D1):D991–D995. doi:10.1093/nar/gks1193
23. Blum A, Wang P, Zenklusen JC. SnapShot: TCGA-analyzed tumors. Cell. 2018;173(2):530. doi:10.1016/j.cell.2018.03.059
24. Kern SE. Why your new cancer biomarker may never work: recurrent patterns and remarkable diversity in biomarker failures. Cancer Res. 2012;72(23):6097–6101. doi:10.1158/0008-5472.CAN-12-3232
25. Sauerbrei W, Taube SE, McShane LM, Cavenagh MM, Altman DG. Reporting recommendations for tumor marker prognostic studies (REMARK): an Abridged explanation and elaboration. J Natl Cancer Inst. 2018;110(8):803–811. doi:10.1093/jnci/djy088
26. Huang da W, Sherman BT, Lempicki RA. Systematic and integrative analysis of large gene lists using DAVID bioinformatics resources. Nat Protoc. 2009;4(1):44–57. doi:10.1038/nprot.2008.211
27. Ashburner M, Ball CA, Blake JA, et al. Gene ontology: tool for the unification of biology. The gene ontology consortium. Nat Genet. 2000;25(1):25–29. doi:10.1038/75556
28. Kanehisa M, Goto S. KEGG: Kyoto Encyclopedia of Genes and Genomes. Nucleic Acids Res. 2000;28(1):27–30. doi:10.1093/nar/28.1.27
29. Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) method. Methods. 2001;25(4):402–408. doi:10.1006/meth.2001.1262
30. Vázquez F, Hastings G, Ortega MA, et al. METH-1, a human ortholog of ADAMTS-1, and METH-2 are members of a new family of proteins with angio-inhibitory activity. J Biol Chem. 1999;274(33):23349–23357. doi:10.1074/jbc.274.33.23349
31. Choi GC, Li J, Wang Y, et al. The metalloprotease ADAMTS8 displays antitumor properties through antagonizing EGFR-MEK-ERK signaling and is silenced in carcinomas by CpG methylation. Mol Cancer Res. 2014;12(2):228–238. doi:10.1158/1541-7786.MCR-13-0195
32. Zhang X, Li D, Jia C, Cai H, Lv Z, Wu B. METTL14 promotes tumorigenesis by regulating lncRNA OIP5-AS1/miR-98/ADAMTS8 signaling in papillary thyroid cancer. Cell Death Dis. 2021;12(6):617. doi:10.1038/s41419-021-03891-6
33. Wu Z, Shi Y, Ren S, Ju Y, Hu Y, Wu J. ADAMTS8 inhibits progression of esophageal squamous cell carcinoma. DNA Cell Biol. 2020;39(12):2300–2307. doi:10.1089/dna.2020.6053
34. Li L, Yuan S, Zhao X, Luo T. ADAMTS8 is frequently down-regulated in colorectal cancer and functions as a tumor suppressor. Biochem Biophys Res Commun. 2020;524(3):663–671. doi:10.1016/j.bbrc.2020.01.020
35. Dunn JR, Reed JE, Du Plessis DG, et al. Expression of ADAMTS-8, a secreted protease with antiangiogenic properties, is downregulated in brain tumours. Br J Cancer. 2006;94(8):1186–1193.
36. Zhao X, Yang C, Wu J, Nan Y. ADAMTS8 targets ERK to suppress cell proliferation, invasion, and metastasis of hepatocellular carcinoma. Onco Targets Ther. 2018;11:7569–7578. doi:10.2147/OTT.S173360
37. Zhang Z, Li J, He T, Ding J. Bioinformatics identified 17 immune genes as prognostic biomarkers for breast cancer: application study based on artificial intelligence algorithms. Front Oncol. 2020;10:330. doi:10.3389/fonc.2020.00330
38. Porter S, Span PN, Sweep FC, et al. ADAMTS8 and ADAMTS15 expression predicts survival in human breast carcinoma. Int J Cancer. 2006;118(5):1241–1247. doi:10.1002/ijc.21476
39. Zhang Y, Schnabel CA, Schroeder BE, et al. Breast cancer index identifies early-stage estrogen receptor-positive breast cancer patients at risk for early- and late-distant recurrence. Clin Cancer Res. 2013;19(15):4196–4205. doi:10.1158/1078-0432.CCR-13-0804
40. Pu M, Messer K, Davies SR, et al. Research-based PAM50 signature and long-term breast cancer survival. Breast Cancer Res Treat. 2020;179(1):197–206. doi:10.1007/s10549-019-05446-y
41. Almstedt K, Mendoza S, Otto M, et al. EndoPredict(®) in early hormone receptor-positive, HER2-negative breast cancer. Breast Cancer Res Treat. 2020;182(1):137–146. doi:10.1007/s10549-020-05688-1
42. Gilkes DM, Semenza GL, Wirtz D. Hypoxia and the extracellular matrix: drivers of tumour metastasis. Nat Rev Cancer. 2014;14(6):430–439. doi:10.1038/nrc3726
43. Gkretsi V, Stylianopoulos T. Cell adhesion and matrix stiffness: coordinating cancer cell invasion and metastasis. Front Oncol. 2018;8:145. doi:10.3389/fonc.2018.00145
44. Aoki M, Fujishita T. Oncogenic roles of the PI3K/AKT/mTOR axis. Curr Top Microbiol Immunol. 2017;407:153–189. doi:10.1007/82_2017_6
45. Carragher NO, Frame MC. Focal adhesion and actin dynamics: a place where kinases and proteases meet to promote invasion. Trends Cell Biol. 2004;14(5):241–249. doi:10.1016/j.tcb.2004.03.011
46. Burridge K. Focal adhesions: a personal perspective on a half century of progress. FEBS J. 2017;284(20):3355–3361. doi:10.1111/febs.14195
47. Lamalice L, Le Boeuf F, Huot J. Endothelial cell migration during angiogenesis. Circ Res. 2007;100(6):782–794. doi:10.1161/01.RES.0000259593.07661.1e
48. Ma Q, Reiter RJ, Chen Y. Role of melatonin in controlling angiogenesis under physiological and pathological conditions. Angiogenesis. 2020;23(2):91–104. doi:10.1007/s10456-019-09689-7
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.