Back to Journals » Biologics: Targets and Therapy » Volume 15
Adalimumab Therapy in a Patient with Psoriasis, Down Syndrome, and Concomitant Hepatitis B Virus Infection
Authors Madani A, Almuhaideb Q ![]()
Received 8 June 2021
Accepted for publication 24 August 2021
Published 1 September 2021 Volume 2021:15 Pages 375—378
DOI https://doi.org/10.2147/BTT.S317888
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Shein-Chung Chow
Abdulaziz Madani,1 Qais Almuhaideb2
1Department of Dermatology, College of Medicine, King Saud University, Riyadh, Saudi Arabia; 2College of Medicine, King Saud University, Riyadh, Saudi Arabia
Correspondence: Abdulaziz Madani
King Saud University, Riyadh, 11451, Saudi Arabia
Tel +966 1-80 66481
Fax +966114671992
Email [email protected]
Abstract: Down syndrome is the most common chromosomal disorder and may present with a combination of dysmorphic features, congenital heart disease, and immunological deficiency. The association between Down syndrome and psoriasis is unclear. The prevalence of psoriasis in patients with Down syndrome ranges from 0.5% to 8%. The safety of biologics in the treatment of Down syndrome-related psoriasis is still debated. Down syndrome results in mild immunological abnormalities; consequently, the risk of infectious complications during immunosuppressive therapy might be higher in this group of patients. We report a case of a 33-year-old male, a case of chronic plaque psoriasis, Down syndrome (DS), asthma, and hepatitis B. The patient was started on Calcipotriene 0.005%-betamethasone 0.064% ointment, which failed to control the patient’s psoriasis; thus, adalimumab was started. His response to adalimumab was significant, where over 70% improvement of the psoriatic lesions was seen.
Keywords: adalimumab, biologics, trisomy 21, HBV
Introduction
Down syndrome (DS), also known as trisomy 21, is a genetic disorder caused by an additional copy of chromosome 21.1 DS is associated with rare dermatological conditions and an increased frequency of some common dermatoses.2 Individuals with DS have a higher prevalence of psoriasis, reaching 8%.3,4 The association between DS and the development of psoriasis and its severity is unclear.5,6 We report a case of psoriasis in a patient with DS with concomitant hepatitis B virus (HBV) infection that successfully responded to adalimumab.
Case Presentation
A 33-year-old male with chronic plaque psoriasis since 2009, DS, and asthma with atopy, presented to the Dermatology clinic at King Khalid University Hospital in Riyadh, Saudi Arabia in 2018. At his initial presentation to our clinic, over 10% of his body surface area (BSA) was covered with hyperkeratotic erythematous scaly plaques over his lower limbs, knees, and elbows (Figure 1). The patient was started on topical calcipotriene 0.005%-betamethasone 0.064% ointment daily.
 |
Figure 1 Extensive bilateral psoriatic lesions over the knee, anterior leg, and dorsum of the foot. |
Over the next months, the response to calcipotriene 0.005% betamethasone 0.064% ointment was poor and BSA remained more than 10%. The patient developed bilateral diffuse erythematous scaly plaques over the upper extremities, trunk, and left ear in addition to the bilateral hyperkeratotic plaques over the knees, legs, and foot.
The patient underwent screening to start treatment with adalimumab. The screening showed a normal complete blood count and urinalysis; the liver function test was normal except for low albumin (31.38 g/L). The interferon gamma release assay (IGRA) test was negative, and hepatitis C was not detectable by PCR. Hepatitis B screening showed positive hepatitis B surface antigen (HBsAg), hepatitis B e antigen (HBeAg), and hepatitis B core antibody (anti-HBc); negative hepatitis B surface antibody (HBsAb) and hepatitis B e antibody (HBeAb). The patient was started with entecavir 0.5 mg oral daily by the hepatology team.
Due to the extensive skin involvement and the lack of improvement with topical treatment, a decision was made to start the patient on a biologic treatment. Given the lack of biologic options in our institution, and after discussion with the hepatology team, a decision was made to start the patient on adalimumab injections.
Adalimumab was started in 2020 with a dose of 80 mg, followed by a dose of 40 mg every other week. Two months after treatment, the lesions in the trunk improved by 30% and the lesions in the upper extremities and ears completely cleared up. However, the lesions on the legs and feet did not improve. The patient did not complain of joint pain or stiffness. He had stopped using topical medications, so the topical calcipotriene-betamethasone ointment was reintroduced. Seven months into treatment, the knee, leg, and foot lesions showed an improvement of over 70% (Figure 2), and no joint pain was present. At the time of this writing, the patient was still being treated with adalimumab, entecavir, and topical calcipotriene-betamethasone ointment.
 |
Figure 2 Significant improvement in psoriatic lesions after treatment with adalimumab. |
Discussion
Psoriasis affects 2.0% to 3.0% of the world’s population, while it has been reported to reach 8% in patients with Down syndrome.3,7 The concomitant presence of the two diseases has been observed in several studies;3,4,6,8 however, the association between DS and psoriasis remains not fully understood.3,5,6
This association can be explained by the dysregulation of the interferon (IFN) system in DS patients.3,6 In psoriasis, skin immunocytes produce various cytokines, one of which is IFN-gamma, a significant culprit of psoriasis formation and severity.3,5 In DS, the percentage of T cells producing IFN-gamma and serum levels of IFN-gamma are substantially higher than healthy controls.3 Furthermore, signal transduction of IFN-gamma requires binding to its receptor interferon gamma receptor-1 (IFNGR-1) and an accessory factor, interferon gamma receptor-2 (IFNGR-2), encoded on chromosome 21. With the additional copy of chromosome 21 in DS patients, IFN sensitivity is increased.3 It is thought that individuals with DS have a greater prevalence of psoriasis secondary to both high serum levels of and enhanced sensitivity to IFN-gamma.3
Immunological alterations present in individuals with DS can increase susceptibility to infections. Therefore, a higher risk of infectious complications during immunosuppressive treatment is expected.6 It is still debated if the use of biologics in the treatment of DS-related psoriasis is safe.4 Thus, the decision to initiate systemic immunosuppressive therapy should be made carefully.6 Few studies have assessed the use of biologic treatment for psoriasis in patients with DS (Table 1).
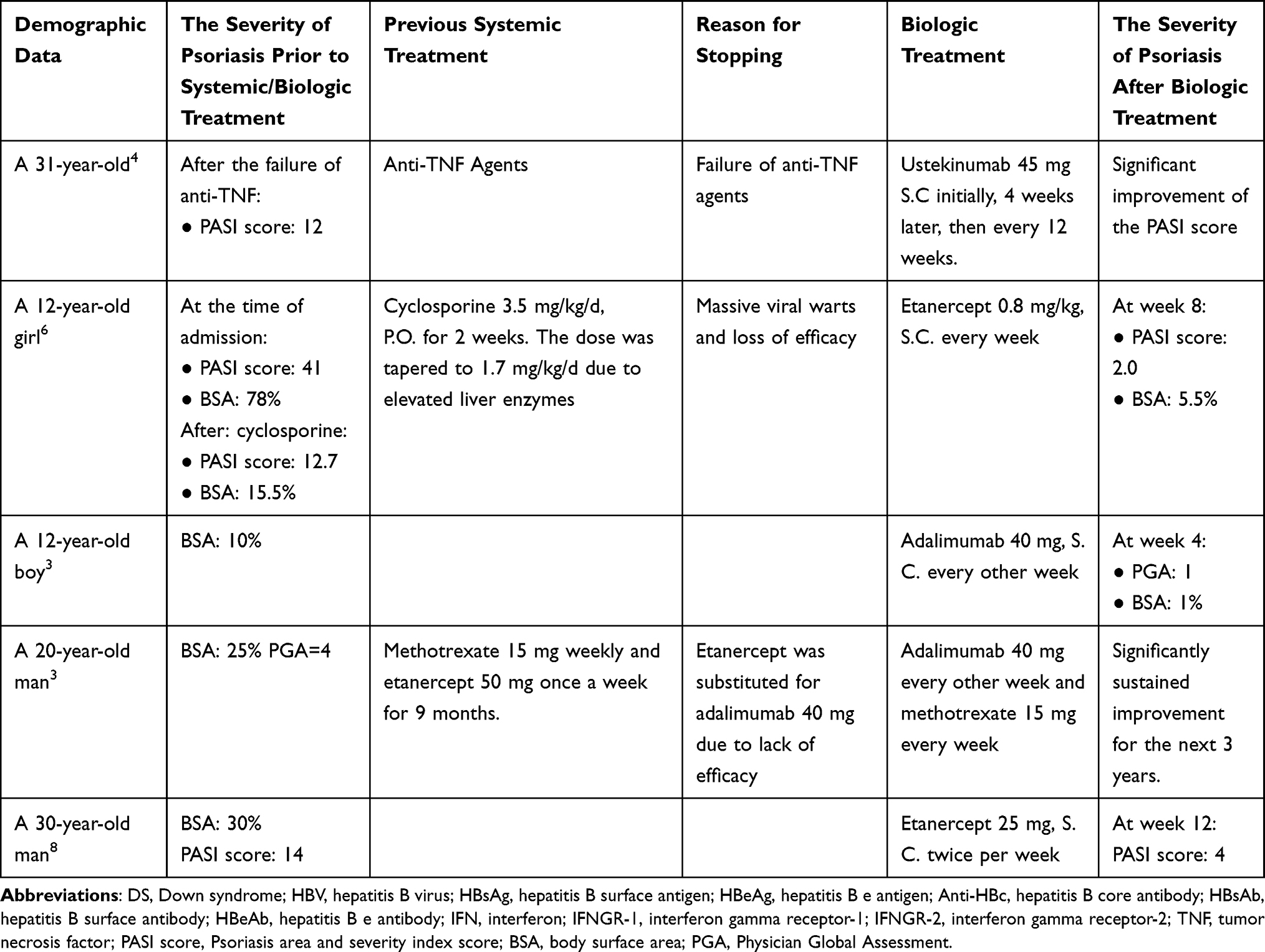 |
Table 1 Characteristics of Patients with Down Syndrome and Plaque Psoriasis Treated with Biologic Agents |
Most of the systemic agents used in the treatment of psoriasis are immunosuppressive, which poses a therapeutic challenge in patients with psoriasis and chronic infections since they are already immunosuppressed. Tumor Necrosis Factor (TNF)-α plays a fundamental role in the elimination of the hepatitis virus from infected hepatocytes. Hence, TNF-α inhibitors may lead to reactivation or exacerbation of hepatitis. A study of 257 patients with hepatitis receiving anti–TNF-α therapy showed that HBV reactivation was 39% in HbsAg positive patients compared to 5% in anti-Hbc positive patients. Furthermore, HBV reactivation was more frequent in patients who did not receive antiviral prophylaxis compared to patients who did.12
Adalimumab is a monoclonal antibody against tumor necrosis factor (TNF)-alpha, which blocks TNF interaction with its cell-surface receptors.9 Adalimumab is a known drug for treating moderate to severe chronic plaque psoriasis in adults.10 As data concerning the use of adalimumab in patients with psoriasis and concomitant viral hepatitis is lacking, little is known about the drug’s true safety in this context.11 In this case, we followed the current expert opinion, suggesting that immunosuppressive therapies should not be used during the acute stage of infection. However, biologic treatment can be started in patients with chronic or resolved hepatitis under close monitoring and collaboration with a gastroenterologist.12
Conclusion
To our knowledge, this is the first case of severe psoriasis in a patient with DS with concomitant HBV infection who successfully responded to adalimumab. Physicians should be aware of the association between DS and psoriasis. We encourage physicians to be careful with the use of biologic treatment in patients with DS. More extensive studies are needed to evaluate the efficacy and safety of adalimumab in patients with DS with psoriasis.
Consent Statement
Informed consent to publish this case was obtained from the patient’s legal guardian. Institutional approval was not required to publish the case details.
Disclosure
The authors have received honoraria for serving as a speaker for AbbVie. The authors report no other conflicts of interest in this work.
References
1. Talamonti M, Galluzzo M, Chiricozzi A, et al. Ustekinumab for treatment of plaque psoriasis in a patient with Down syndrome. J Drugs Dermatol. 2012;11(8):1000–1002.
2. Adamczyk M, Michalska-Jakubus M, Krasowska D. A 12-year-old girl with severe plaque psoriasis and Down syndrome treated successfully with etanercept. Acta Dermatovenerol Croat. 2017;25(2):155–158.
3. Patterson D. Molecular genetic analysis of Down syndrome. Hum Genet. 2009;126(1):195–214. doi:10.1007/s00439-009-0696-8
4. Madan V, Williams J, Lear JT. Dermatological manifestations of Down’s syndrome. Clin Exp Dermatol. 2006;31(5):623–629. doi:10.1111/j.1365-2230.2006.02164.x
5. Marmon S, De Souza A, Strober BE. Psoriasis and Down syndrome: a report of three cases and a potential pathophysiologic link. Dermatol Online J. 2012;18(6):13. doi:10.5070/D305M5F4BX
6. Sismour B, D’Acunto K. Down syndrome, severe psoriasis, and increased risk for cardiovascular events. J Am Acad Physician Assist. 2019;32(12):31–33. doi:10.1097/01.JAA.0000604860.71819.c1
7. Mohd Affandi A, Khan I, Ngah Saaya N. Epidemiology and clinical features of adult patients with psoriasis in Malaysia: 10-year review from the Malaysian Psoriasis Registry (2007–2016). Dermatol Res Pract. 2018;2018:1–8. doi:10.1155/2018/4371471
8. Alcaide AJ, Barrera MV, Habicheyn S, López N, Mendiola MV, Herrera E. Safety of etanercept therapy in a patient with psoriasis, Down’s syndrome and concomitant hepatitis C virus infection. J Eur Acad Dermatol Venereol. 2008;22(12):1514–1516. doi:10.1111/j.1468-3083.2008.02693.x
9. Wu JJ, Valdecantos WC. Adalimumab in chronic plaque psoriasis: a Clinical Guide. J Drugs Dermatol. 2017;16(8):779–790.
10. Burness CB, McKeage K. Adalimumab: a Review in Chronic Plaque Psoriasis. Drugs. 2015;75(18):2119–2130. doi:10.1007/s40265-015-0503-x
11. Piaserico S, Dapavo P, Conti A, Gisondi P, Russo FP. Adalimumab is a safe option for psoriasis patients with concomitant hepatitis B or C infection: a multicentre cohort study of 37 patients and review of the literature. J Eur Acad Dermatol Venereol. 2017;31(11):1853–1859. doi:10.1111/jdv.14146
12. Kaushik SB, Lebwohl MG. Psoriasis: which therapy for which patient: psoriasis comorbidities and preferred systemic agents. J Am Acad Dermatol. 2019;80(1):27–40. doi:10.1016/j.jaad.2018.06.056
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.